Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

208 Section III • The Esophagus
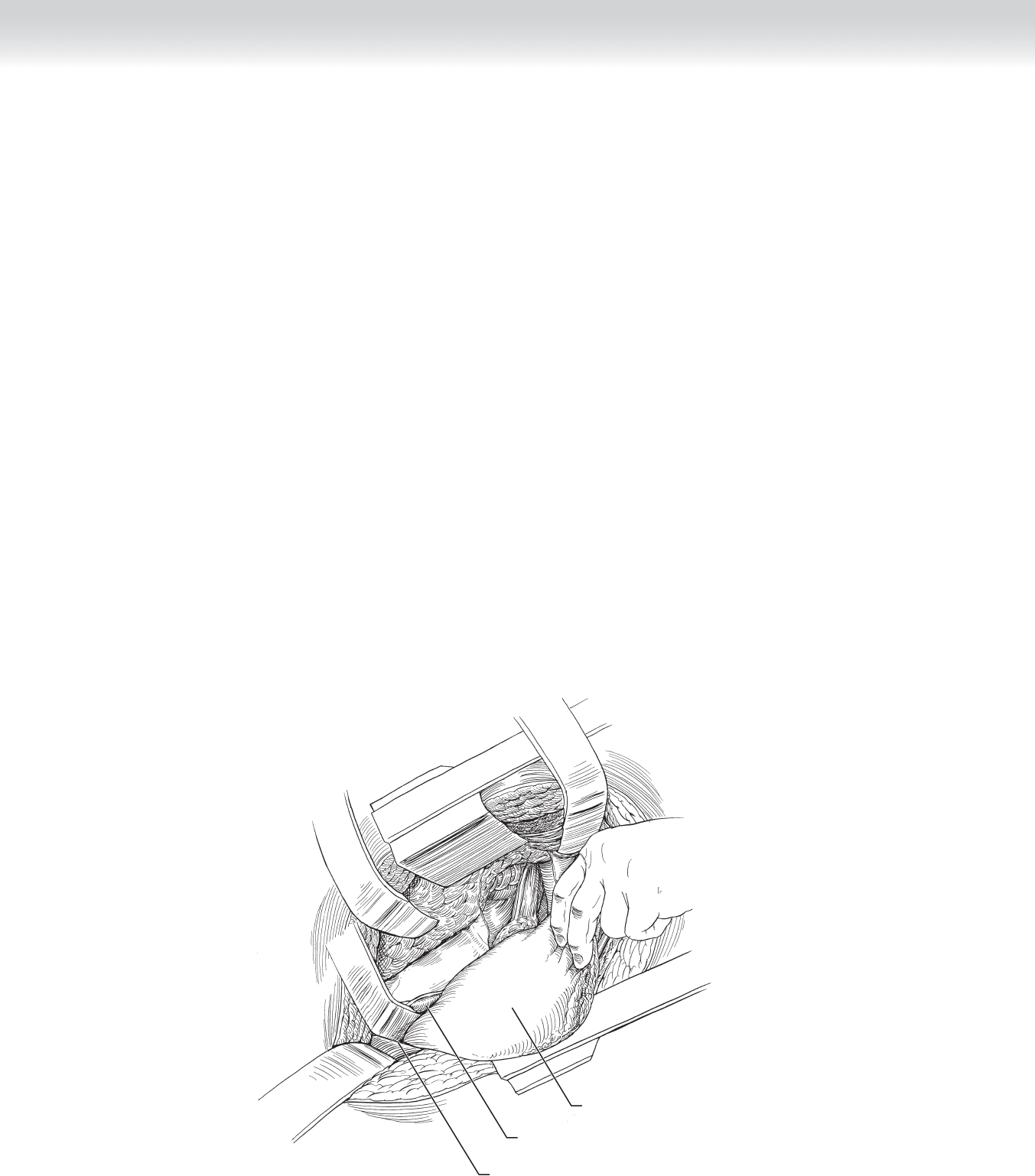
◆ Mobilization of the stomach: The mobilization of the stomach proceeds along the greater
curvature in the direction of the pylorus, with division of the omentum maintaining a 1-cm
margin from the right gastroepiploic artery and vein. Attention should be paid to avoiding
excessive traction on the omental artery arcade. The right gastroepiploic vessels should be
preserved until the extent of dissection is determined. The stomach is retracted to the right
to provide tension on the short gastric vessels. Dissection proceeds cephalad along the
greater curvature until the proximal stomach and distal esophagus are freed (Figure 18-5).
◆ The freed stomach is refl ected to visualize the celiac axis on the posterior aspect. The poste-
rior gastric artery and recurrent branch of the left inferior phrenic artery should be identi-
fi ed, ligated, and divided. Node-bearing tissue is removed from the superior aspect of the
pancreas, around the celiac axis, and along the left gastric artery for en bloc removal with
the specimen. The left gastric artery and vein are ligated.
◆ The lesser sac is examined to determine whether the pancreas or spleen is involved with the
tumor. The lesser omentum is divided and removed from the right side of the esophagus to
the pylorus, with care taken to preserve the right gastric artery and vein.
Liver
Cut edge of diaphragm
Stomach
MC
MC
FIGURE 18 –5
CHAPTER 18 • Esophagogastrectomy 209
3. SELECTION OF PARTIAL OR TOTAL GASTRECTOMY
◆ Proximal esophagogastrectomy with esophagogastrostomy should be undertaken if the tumor
can be adequately resected with a 5-cm margin by removal of the proximal stomach. The
stomach has a blood supply that is less likely to be affected by atherosclerotic disease and
requires only a single anastomosis, as opposed to using an intestinal conduit.
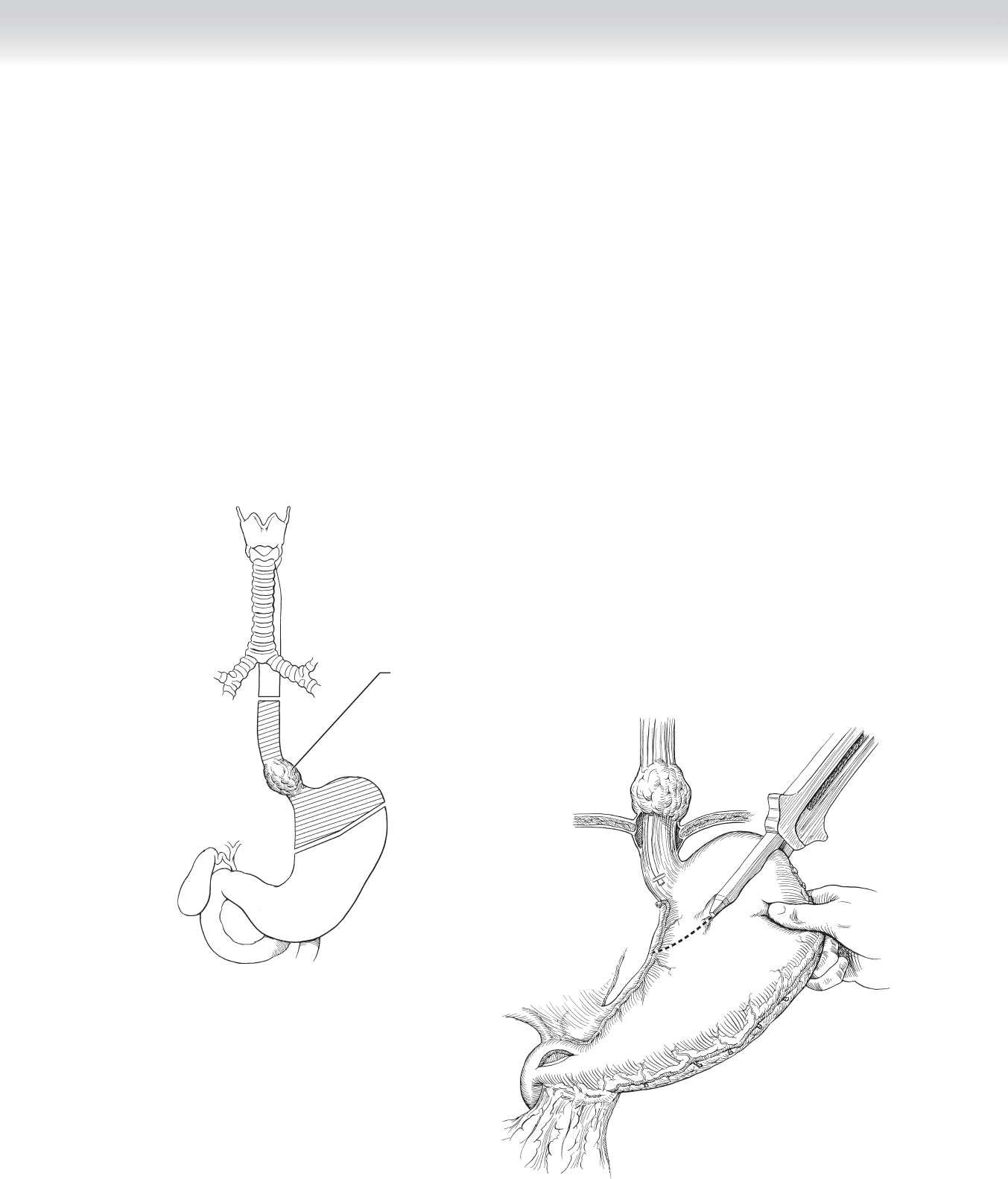
◆ Gastric remnant reconstruction: The margin of resection should be 4 to 6 cm from the
esophagogastric junction, from halfway on the lesser curvature to a medial point on the
fundus. A gastrointestinal anastomosis (GIA) stapler is placed at a right angle and transects
the proximal stomach from the lesser curvature toward the fundus. The staple line is
oversewn with inverting 3-0 suture. Care should be taken to maintain tension along the
stomach to prevent shortening of the lesser curvature. A pyloromyotomy may be necessary
to prevent gastric stasis secondary to division of the vagus nerves (Figure 18-6).
A
Tumor removed along
with portions of esophagus
and fundus of stomach
B
FIGURE 18 –6
210 Section III • The Esophagus
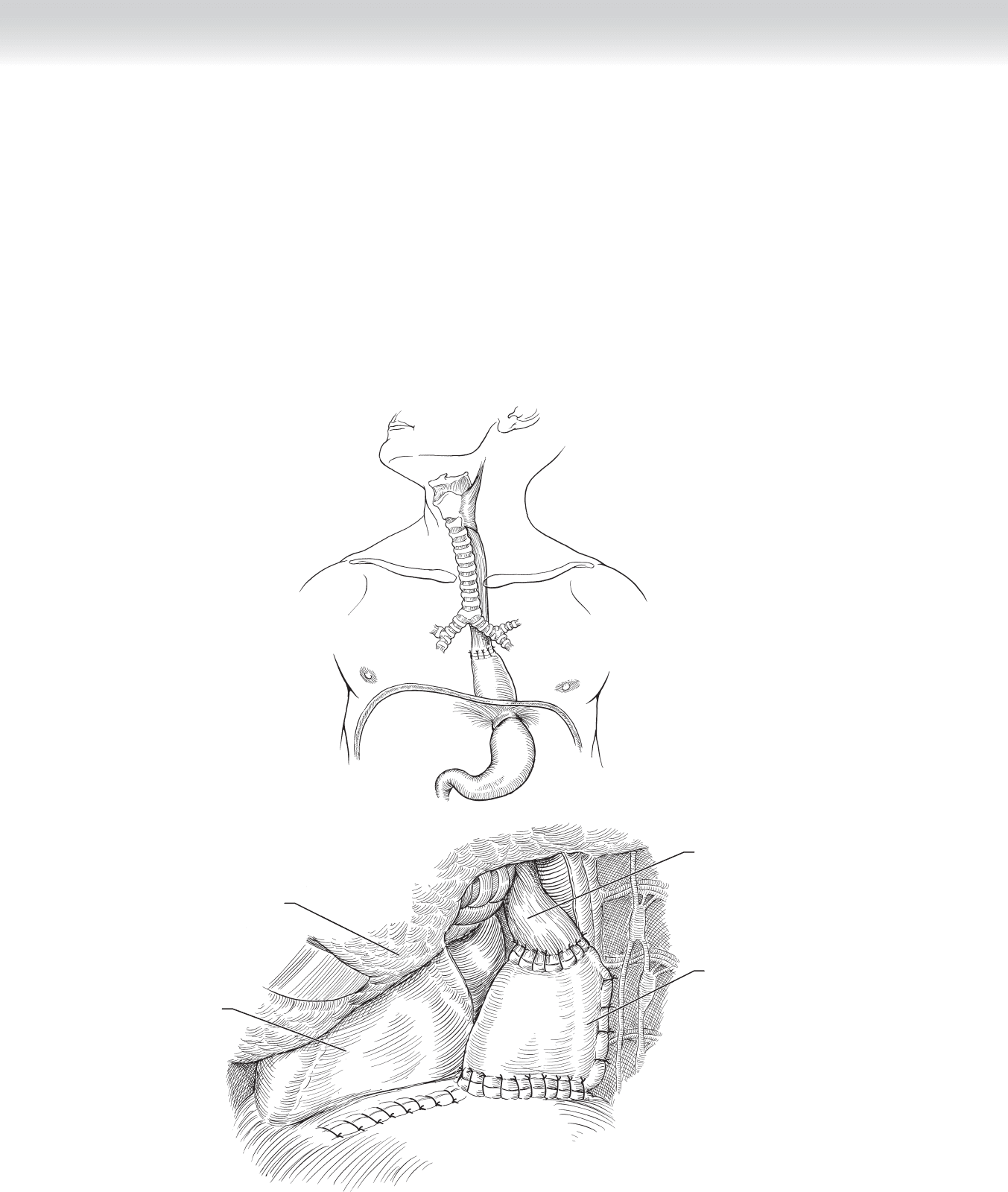
◆ The gastric remnant is brought into the thorax through the hiatus and behind the proximal
esophagus. The margin should be at least 10 cm. If the margin is adequate, the posterior
wall of the esophagus is anastomosed to the end of the gastric tube. If the margin is inade-
quate, the gastric tube length should be determined. If the length of stomach is inadequate
to achieve a clear proximal remnant, the left side of the colon can be used as an alternative
between the gastric remnant and the cervical esophagus (Figure 18-7).
A
B
Stomach
Esophagus
Left lung
Heart
FIGURE 18 –7
CHAPTER 18 • Esophagogastrectomy 211
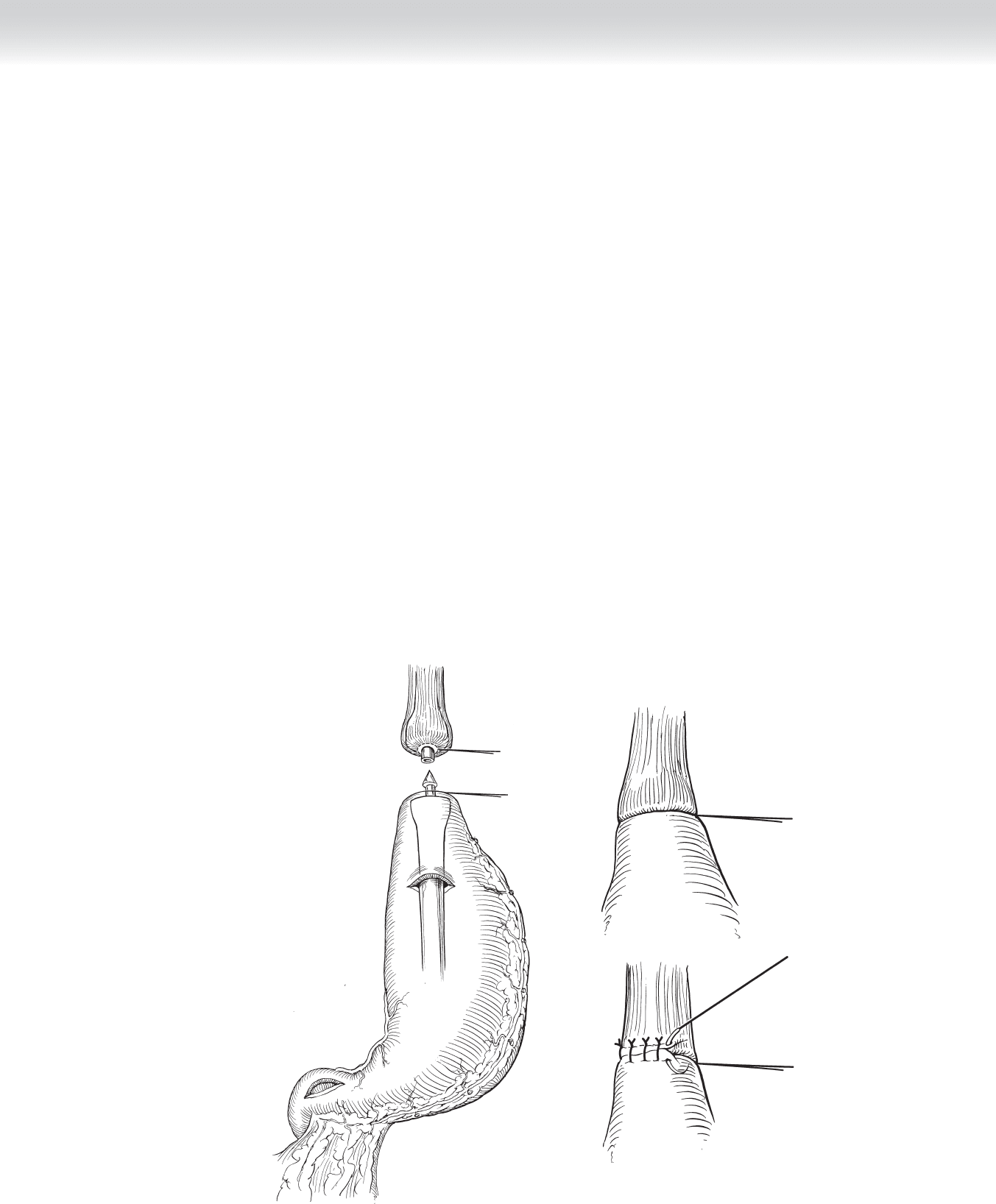
◆ Esophagogastric anastomosis: The esophagus is cut at a 45-degree angle with the ante-
rior wall longer than the posterior wall. Stay sutures should be placed with 4-0 Vicryl at
the midpoint of the anterior wall, as well as the posterior wall. A 2-cm gastrotomy is
made between the stapled end of the lesser curvature and the greater curvature. The stay
suture from the posterior esophageal wall is passed through the full thickness of the
cephalad portion of the gastrotomy. A 45-mm endoscopic GIA stapler is placed with the
thick part in the stomach and the narrow part in the esophagus. Two suspension sutures
are tied on each side of the anastomosis, one at the tip and one at the base. The stapler
is fi red to complete the posterior section of the anastomosis (Figure 18-8, A-B).
◆ Care should be paid to ensure that the staple line is adequately clear of the previous staple
line along the lesser curvature. Overlap of the staple lines could result in ischemia and a
subsequent leak.
◆ The anterior portion of the anastomosis is made in two layers: the inner layer with con-
tinuous full-thickness 4-0 inverting polydioxanone structure (PDS) and the outer layer
with interrupted sutures. Particular attention should be given to where the hand-sewn
portion intersects with the stapled portion at the corners. Start the inner layer at the cor-
ner and incorporate at least 5 mm of the staple line (Figure 18-8, C).
◆ Total gastrectomy with Roux-en-Y esophagojejunostomy is undertaken if a proximal
gastrectomy does not allow the tumor to be resected with adequate 5-cm margins on the
stomach.
A
B
C
FIGURE 18 –8
212 Section III • The Esophagus
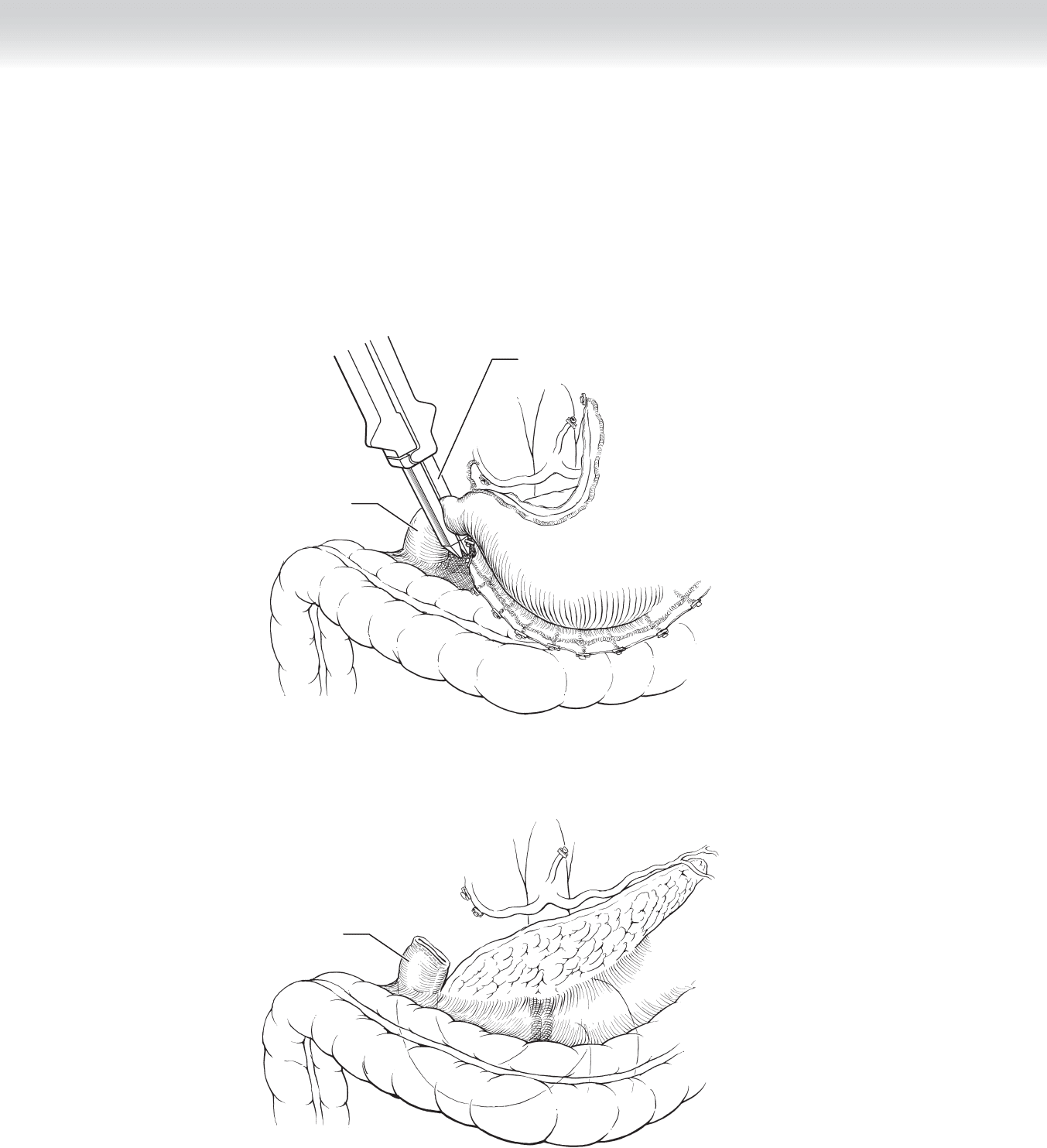
◆ The right gastroepiploic and right gastric vessels are suture-ligated and divided distal to the
pylorus. The duodenum is divided distal to the pylorus with a linear stapler. The staple line
should be inverted with interrupted 3-0 nonabsorbable sutures and covered with omentum
to prevent duodenal stump blowout (Figures 18-9 and 18-10).
Gastrointestinal
anastomosis stapler
Duodenum
FIGURE 18 –9
Duodenum
FIGURE 18 –10
CHAPTER 18 • Esophagogastrectomy 213
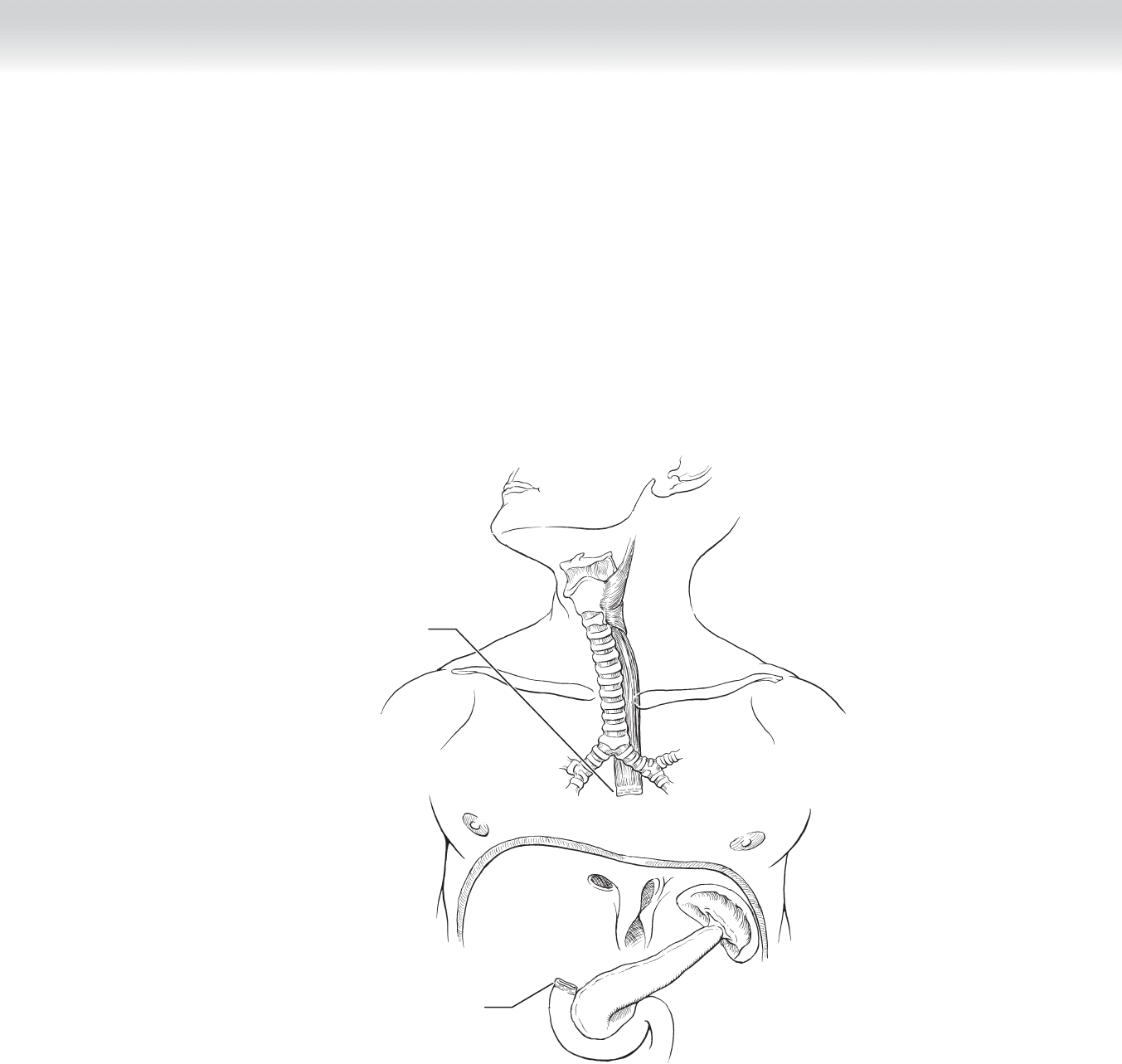
◆ The esophagus is mobilized to the level of the inferior pulmonary vein. A monofi lament
nylon purse-string suture is placed around the circumference of the proximal esophagus.
The esophageal lumen should be distended with a no. 24 Foley catheter and a 20-mL
balloon, which is advanced into the esophagus and gently infl ated (Figure 18-11).
Proximal end
of duodenum
Distal end
of esophagus
FIGURE 18 –11
214 Section III • The Esophagus
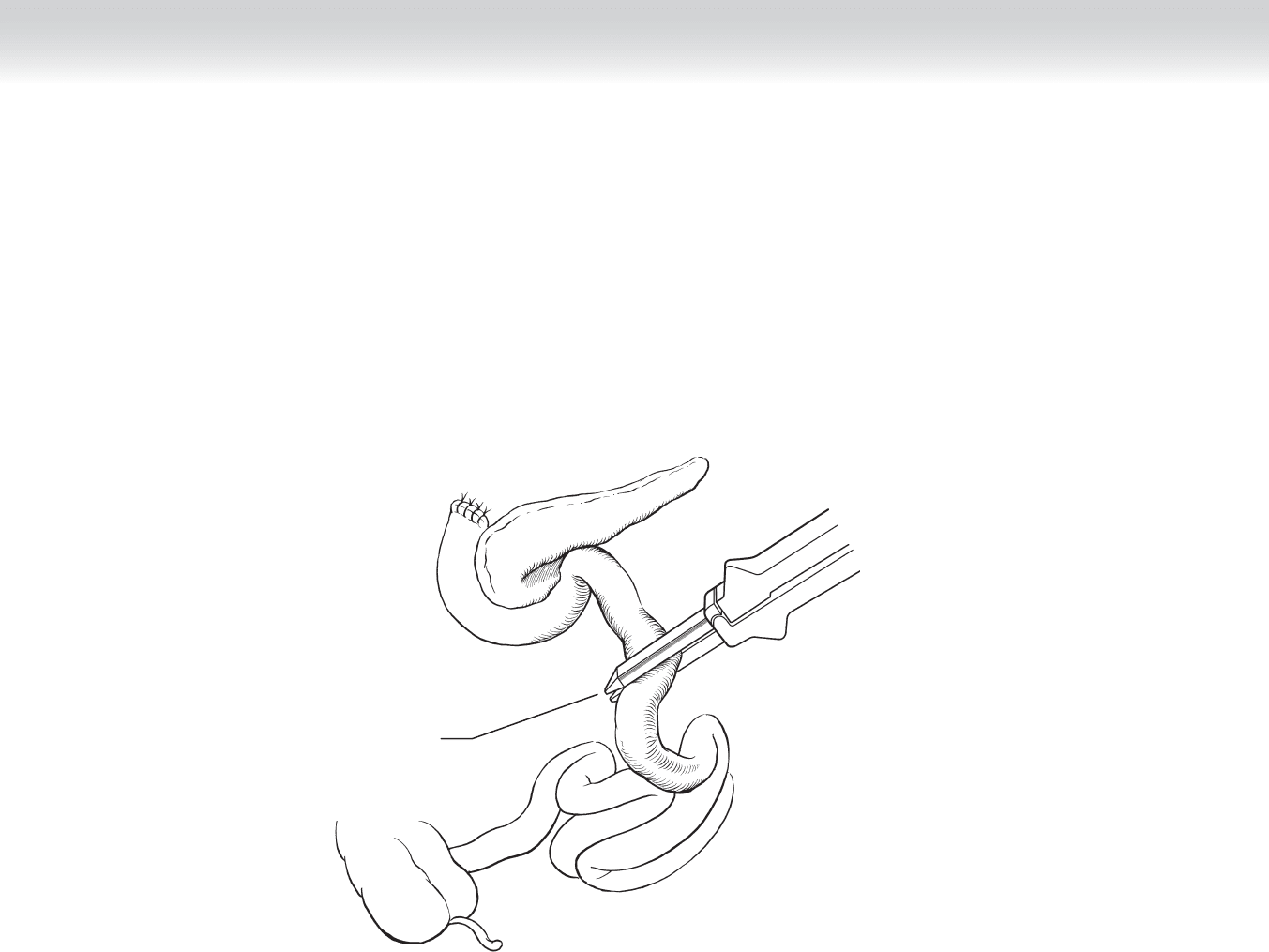
◆ A jejunal interposition is created using the Roux-en-Y technique (Figures 18-12 and 18-13).
The jejunum should be mobilized suffi ciently to permit anastomosis with the thoracic
esophagus, necessitating division of several jejunal arteriovenous arcades.
Jejunum divided
with GIA stapler
FIGURE 18 –12
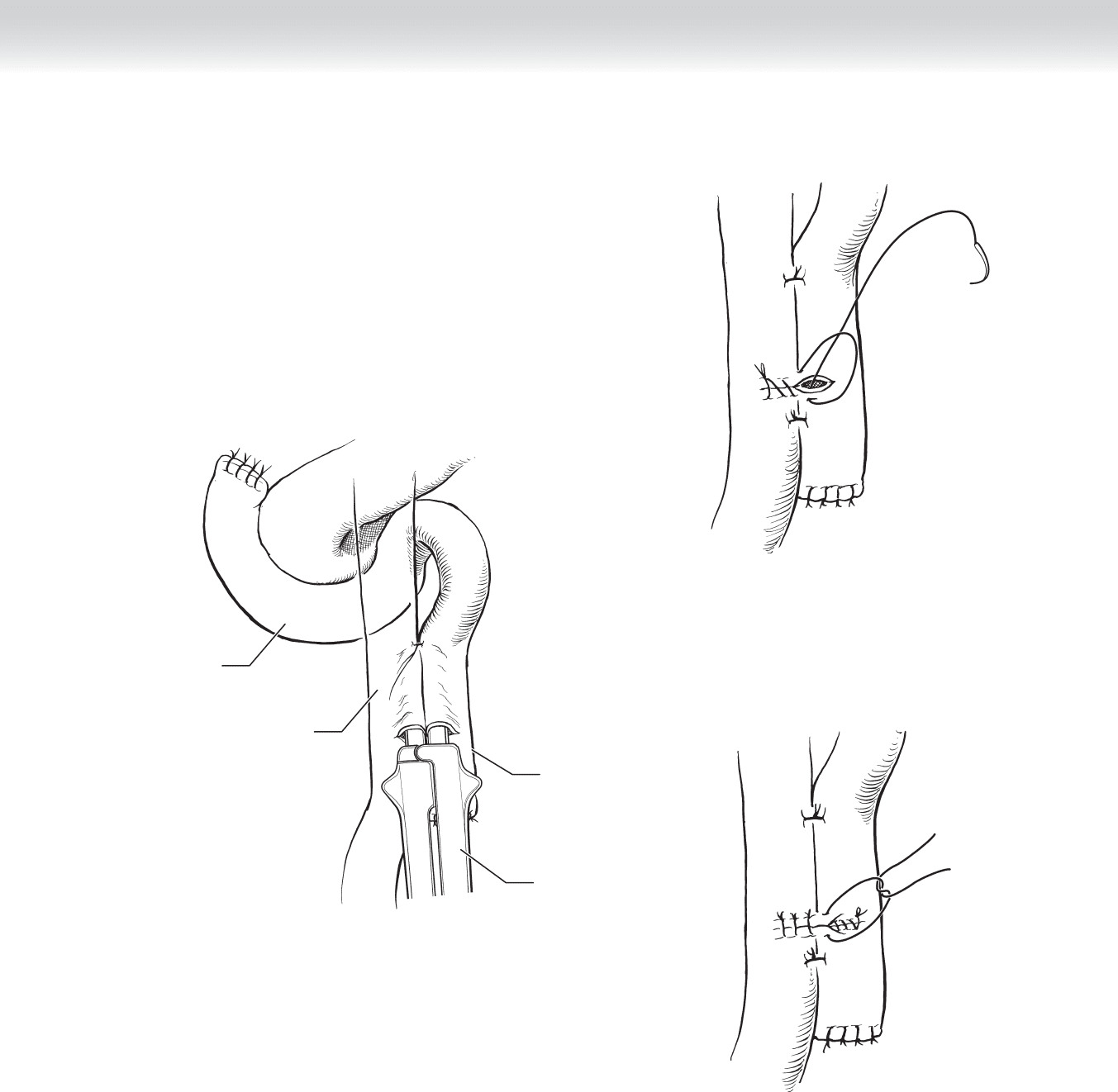
CHAPTER 18 • Esophagogastrectomy 215
GIA stapler
(Roux-en-Y anastomosis)
Duodenum
A
Jejunum
Proximal end
of jejunum
B
C
FIGURE 18 –13
216 Section III • The Esophagus
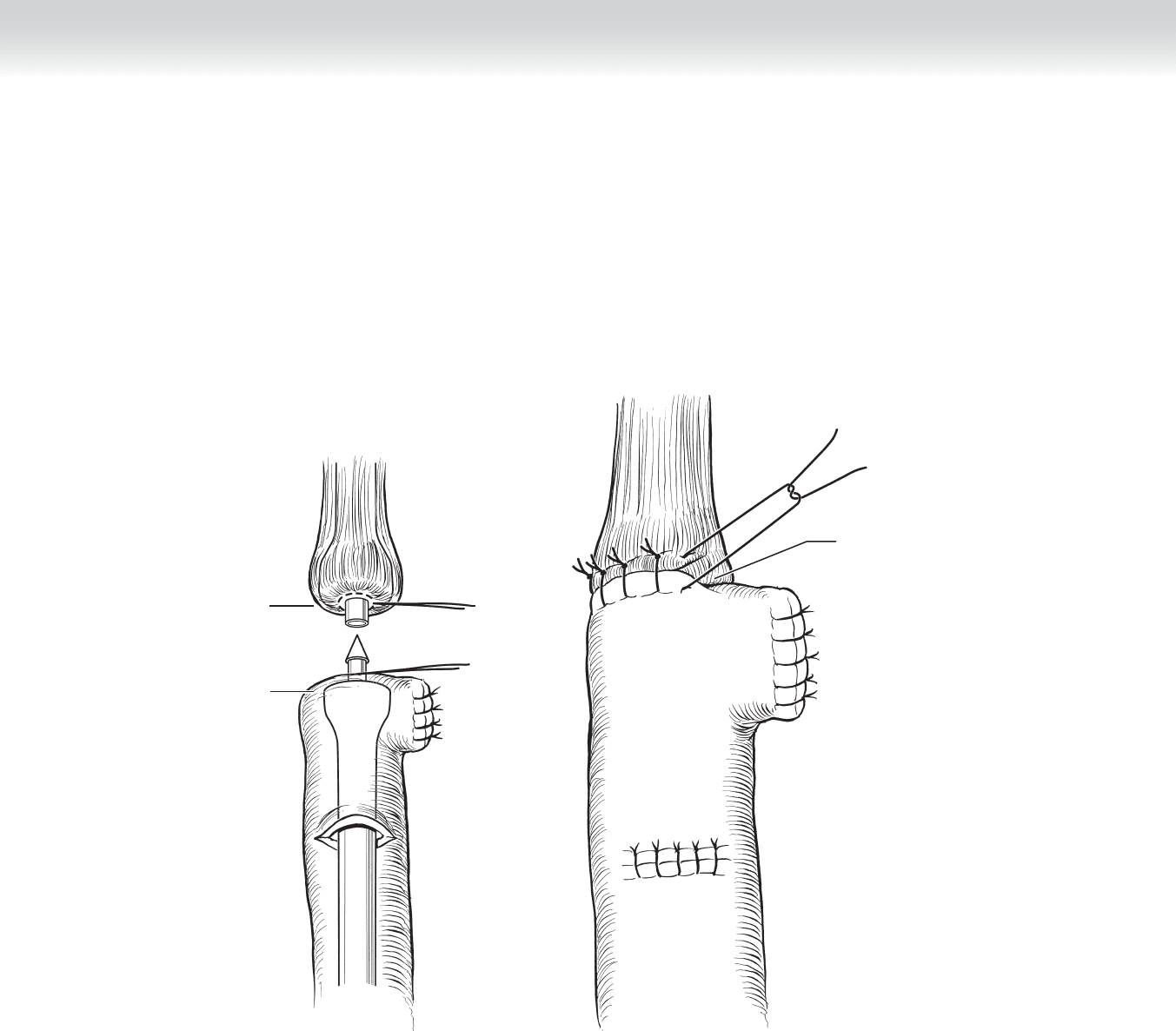
◆ Loading: An end-to-end anastomosis (EEA) stapler is passed through the jejunum into the
esophagus and fi red. The jejunum is anchored to the proximal esophagus. To minimize
bile refl ux, the surgeon should anastomose the duodenal loop to the jejunum at least
50 cm distal to the esophagojejunal anastomosis. The blind end of the jejunal loop is sta-
pled closed (Figures 18-14 and 18-15).
A
Distal end of
esophagus
Proximal end of
jejunum
Securing
anastomosis
with interrupted
sutures
B
FIGURE 18 –14
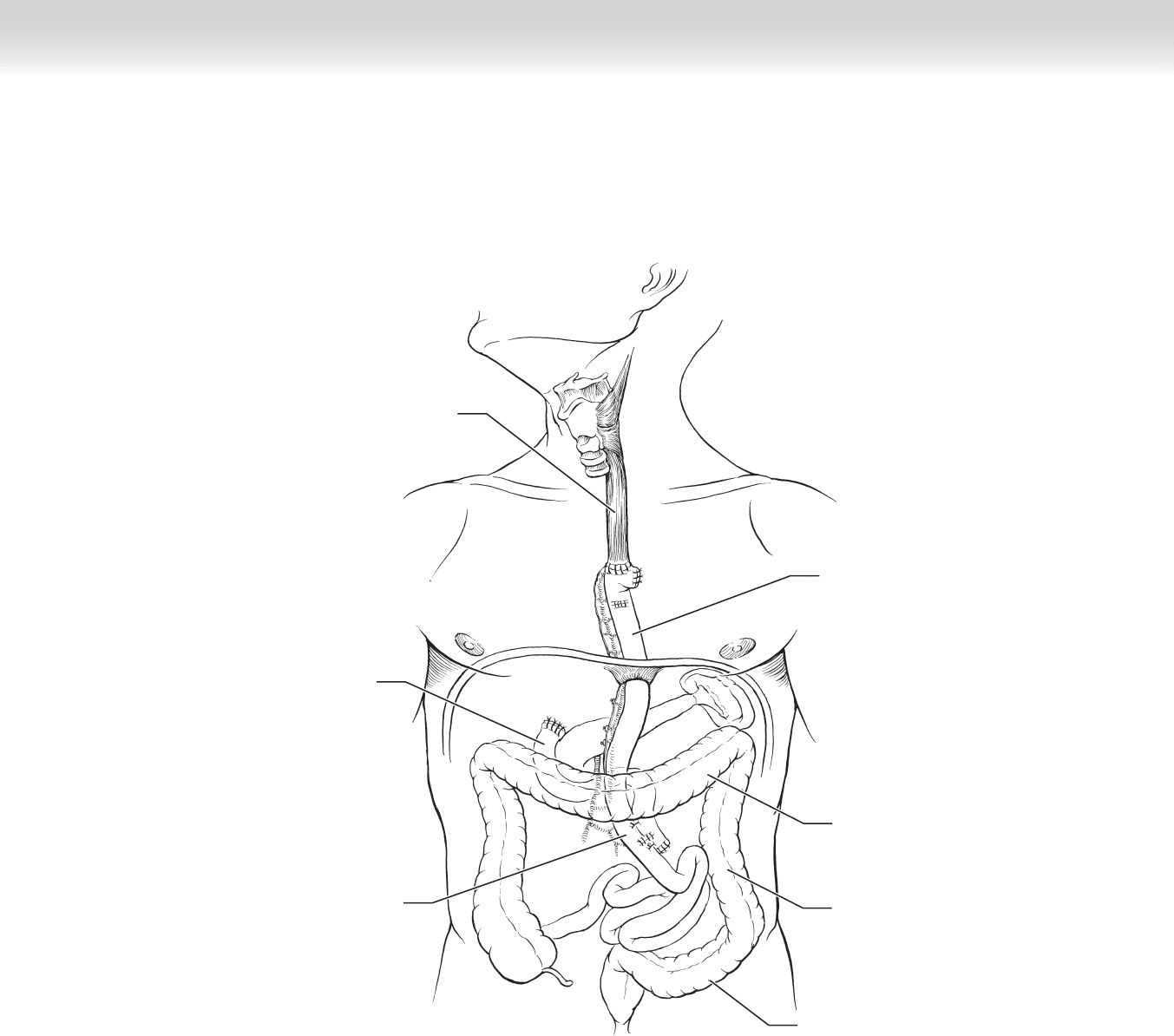
Jejunum
Esophagus
Descending
colon
Transverse colon
Sigmoid colon
Jejunum
Duodenum
FIGURE 18 –15
CHAPTER 18 • Esophagogastrectomy 217