Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

218 Section III • The Esophagus
4. CLOSING
◆ In repairing the diaphragm, the gastric or jejunal interposition is secured to the crura with
interrupted sutures. The remainder of the diaphragm is closed with interrupted mattress
sutures. A chest tube should be placed into the pleural space near the anastomosis to ensure
adequate fl uid drainage. The left lung is reexpanded and the costal cartilages are left to fl oat
free. Tissue and skin are closed according to surgeon preference.
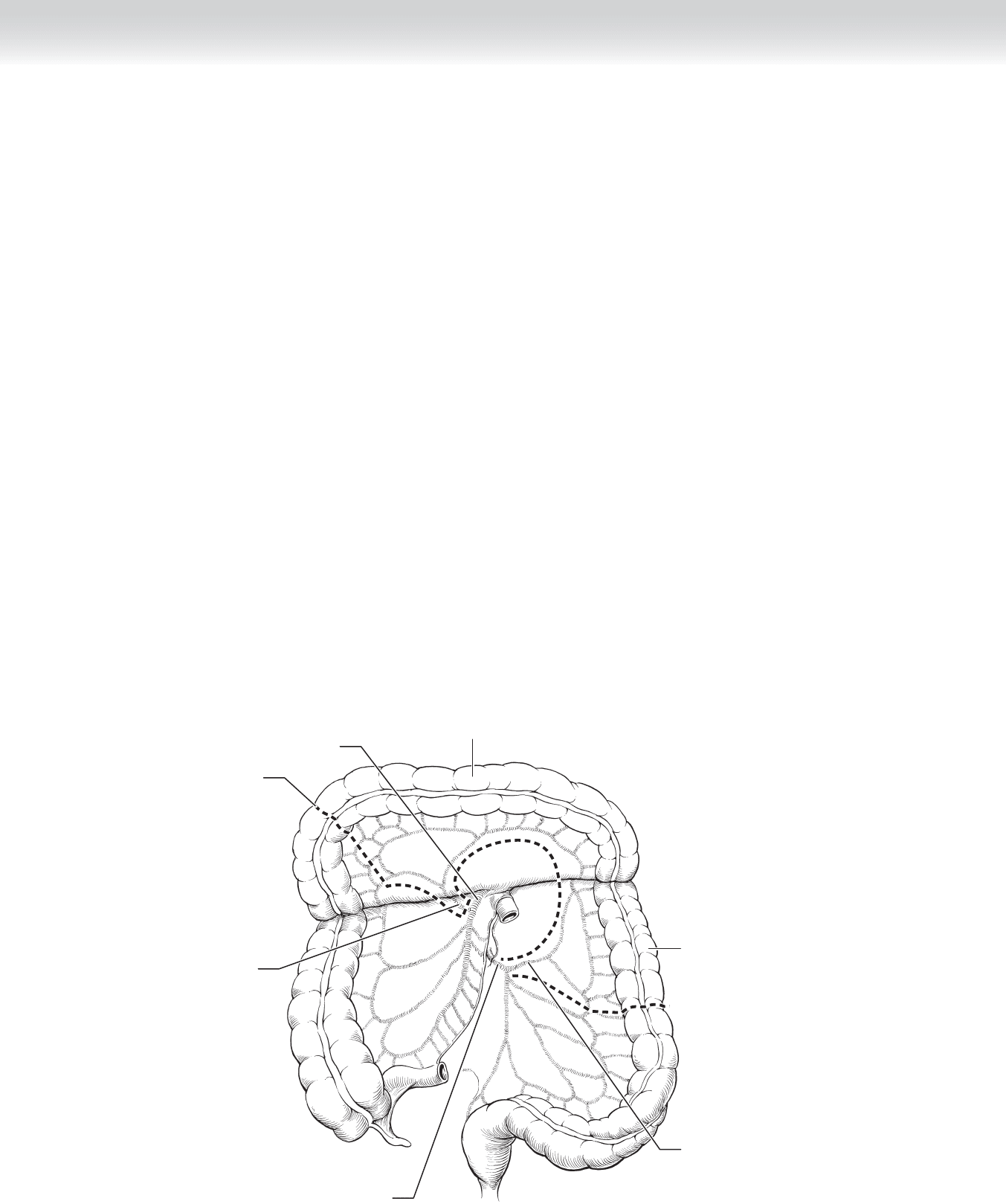
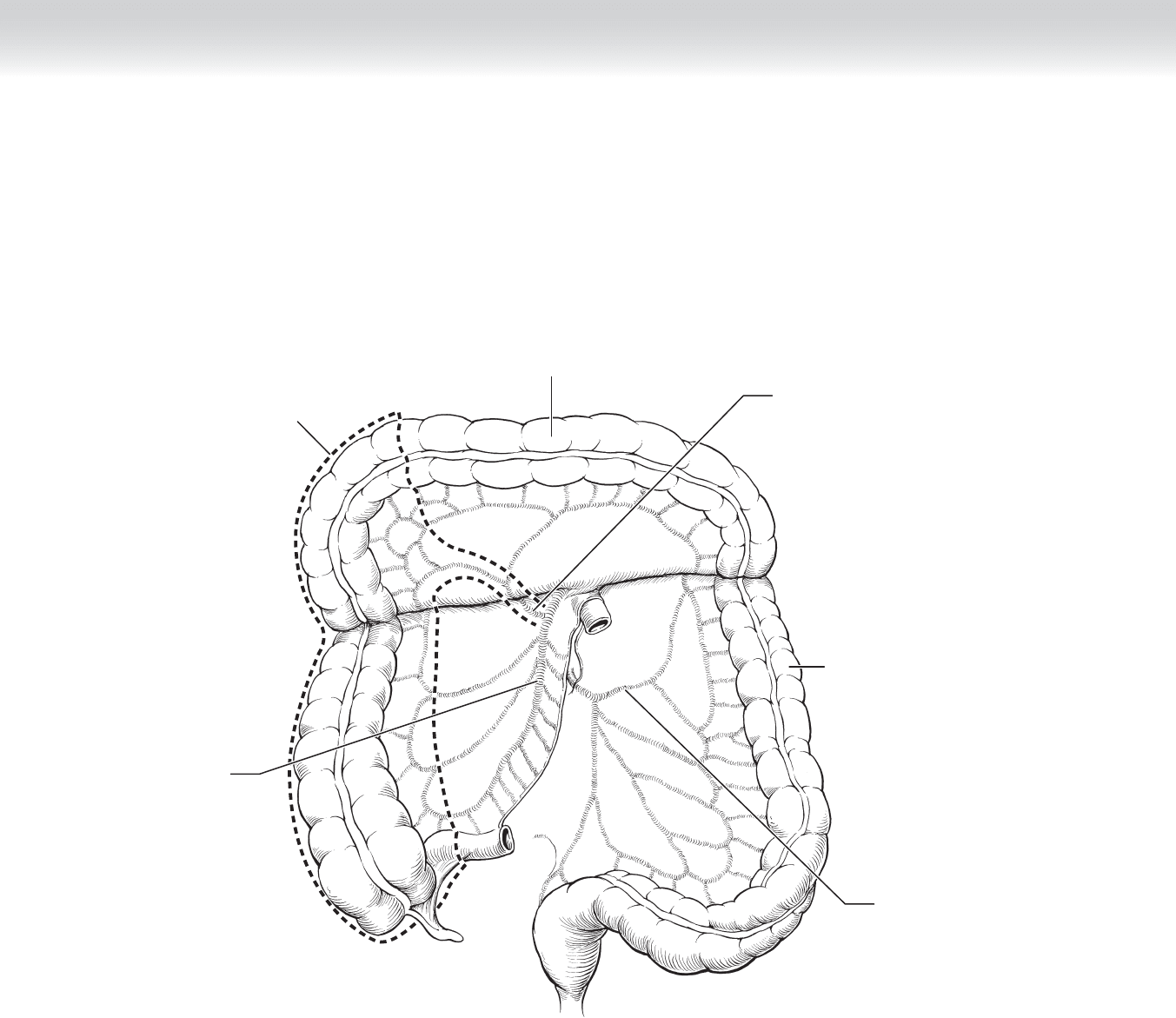
◆ Total gastrectomy with descending colon graft: Whereas the stomach is better than the colon
as an esophageal substitute, the colon may be used if the stomach is not a viable option
because of prior surgery or tumor extension. The descending colon is preferred to the ascend-
ing colon, because the smaller lumen is more similar in diameter to the esophagus. However,
the inferior mesenteric artery that supplies the descending colon is more likely to have athero-
sclerotic disease than other mesenteric vessels (Figure 18-16).
◆ After the surgeon thoroughly explores the abdomen for metastases, the length of the re-
quired graft should be measured. The middle colic artery should be clamped with a bulldog
clamp to evaluate the adequacy of collateral circulation.
◆ The descending colon is prepared by mobilizing the splenic fl exure and separating the
attached omentum. The remaining colon is reanastomosed and the mesentery is reapproxi-
mated (Figures 18-17 and 18-18).
Middle
colic artery
Transverse colon
Left
colic artery
Descending
colon
Superior
mesenteric
artery
Incision
Inferior
mesenteric
artery
FIGURE 18 –16
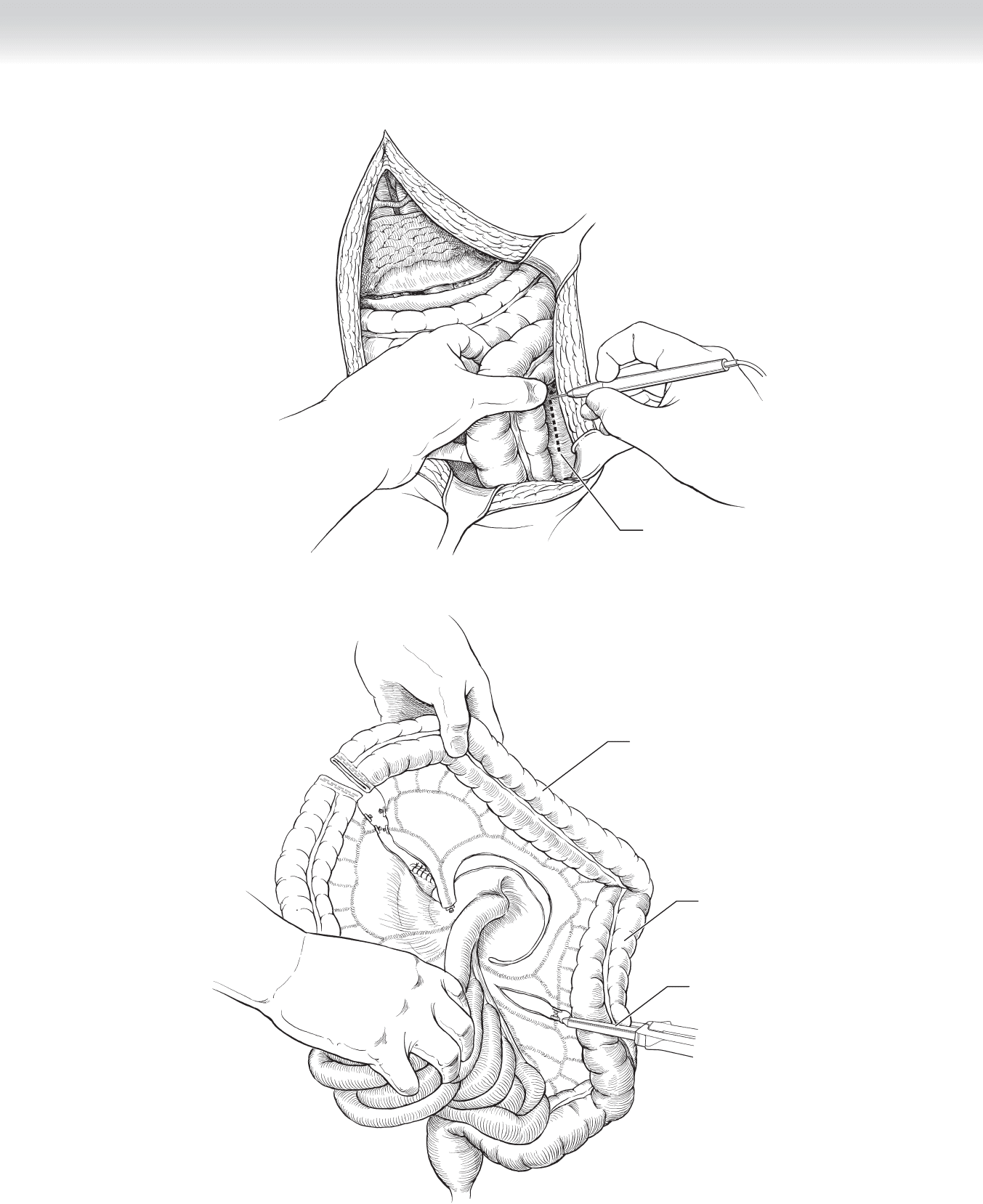
Incising lateral
peritoneum to
mobilize
descending colon
FIGURE 18 –17
CHAPTER 18 • Esophagogastrectomy 219
Dividing descending colon
with GIA stapler
Descending colon
Transverse colon
FIGURE 18 –18
220 Section III • The Esophagus
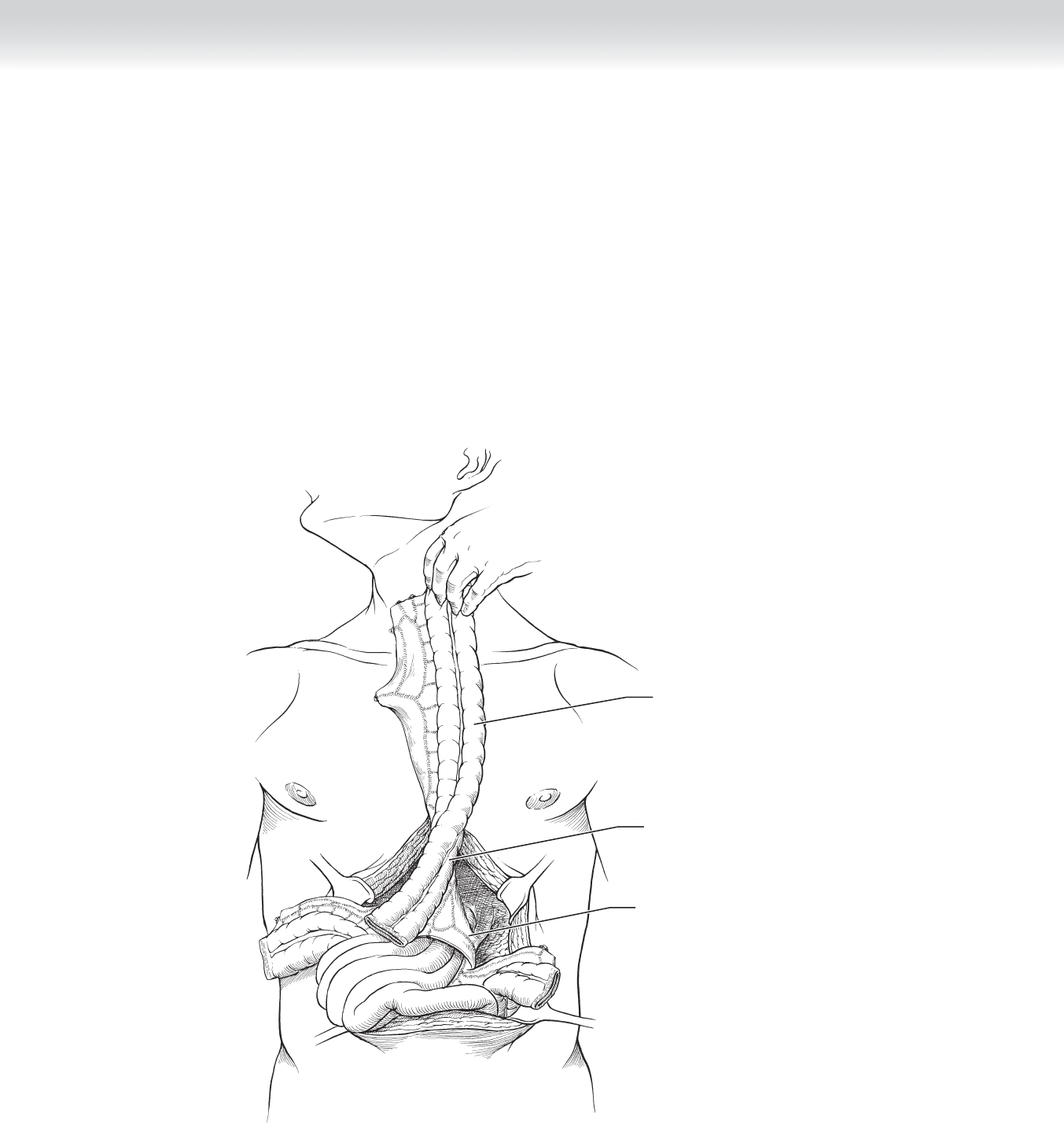
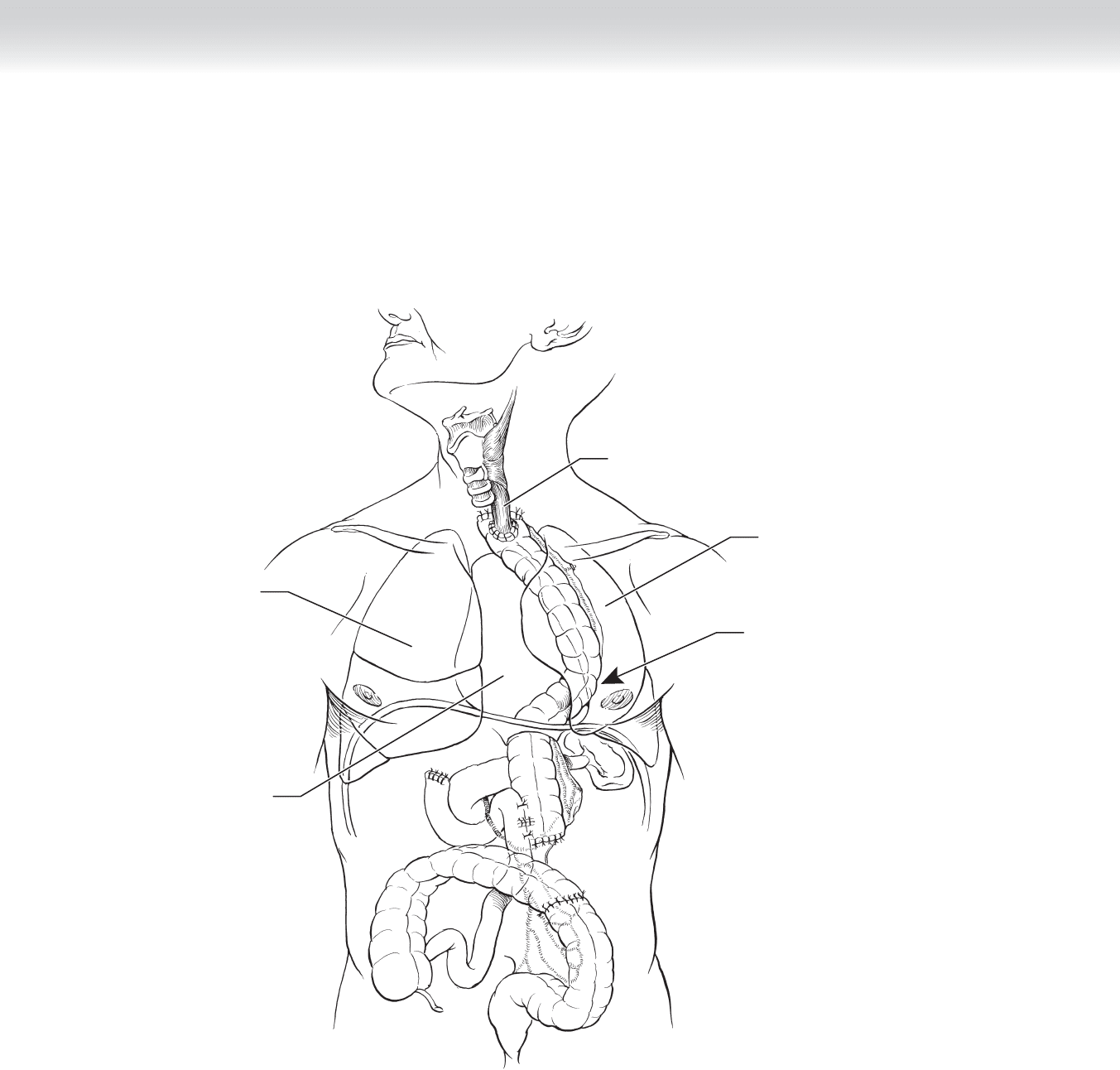
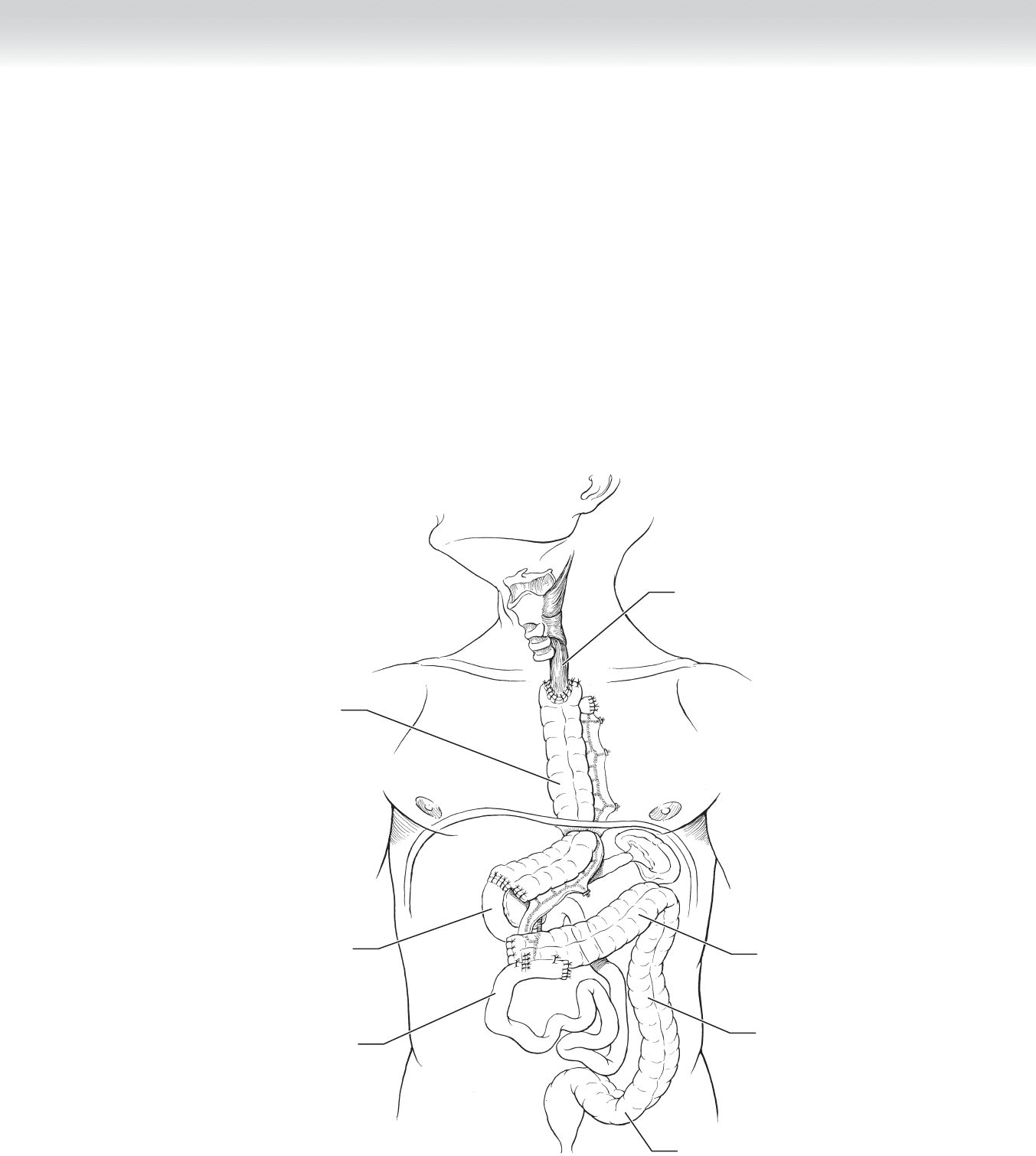
◆ The proximal end of the anastomosis may be performed fi rst to measure the length of the
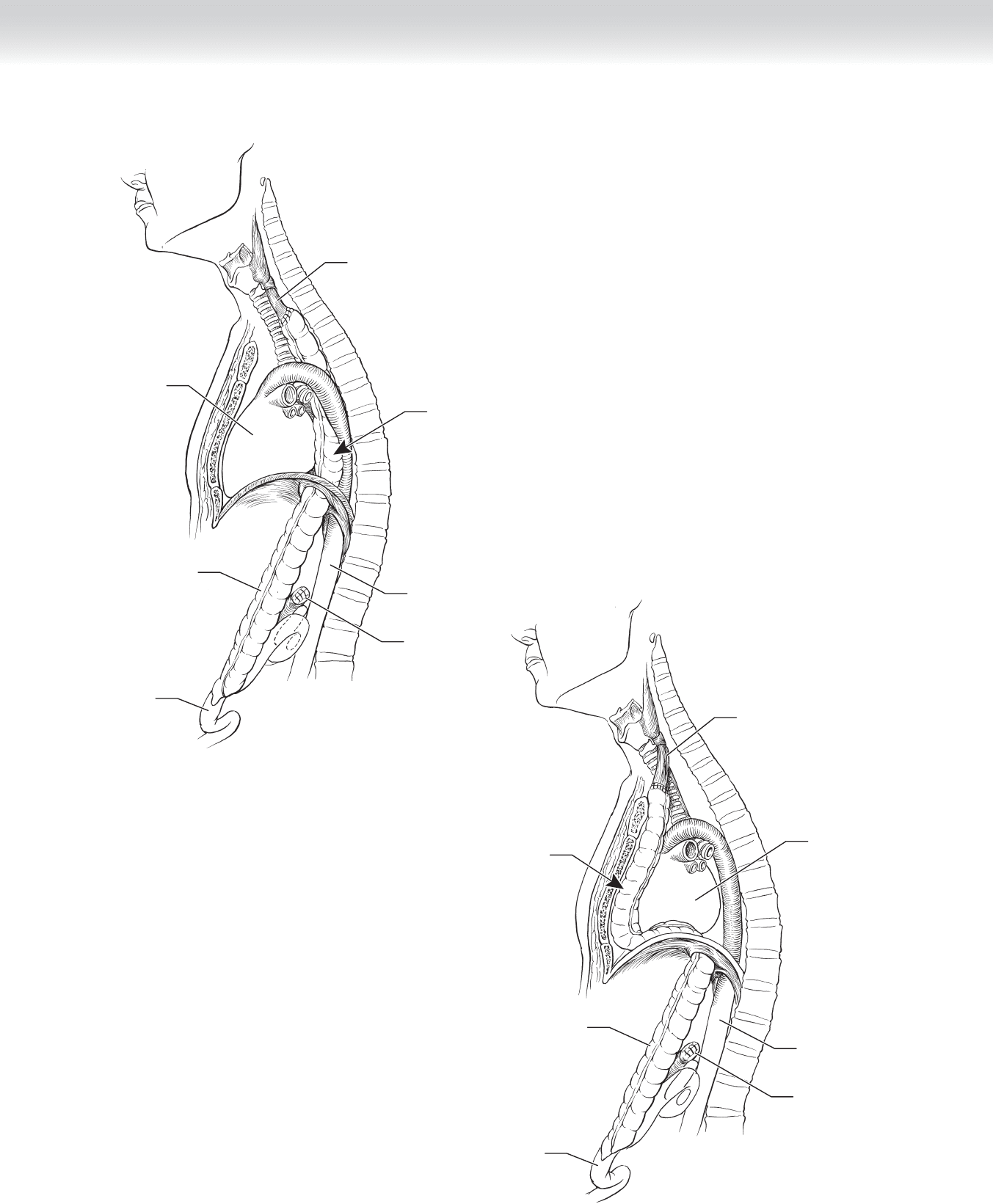
graft more accurately (Figure 18-19). The colon is passed along the posterior mediastinum,
which is the shortest route between the stomach and the esophagus (Figure 18-20). The
substernal and transpleural routes are also secondary possibilities but may result in greater
kinking of the graft and subsequent emptying problems (Figures 18-21 and 18-22). The
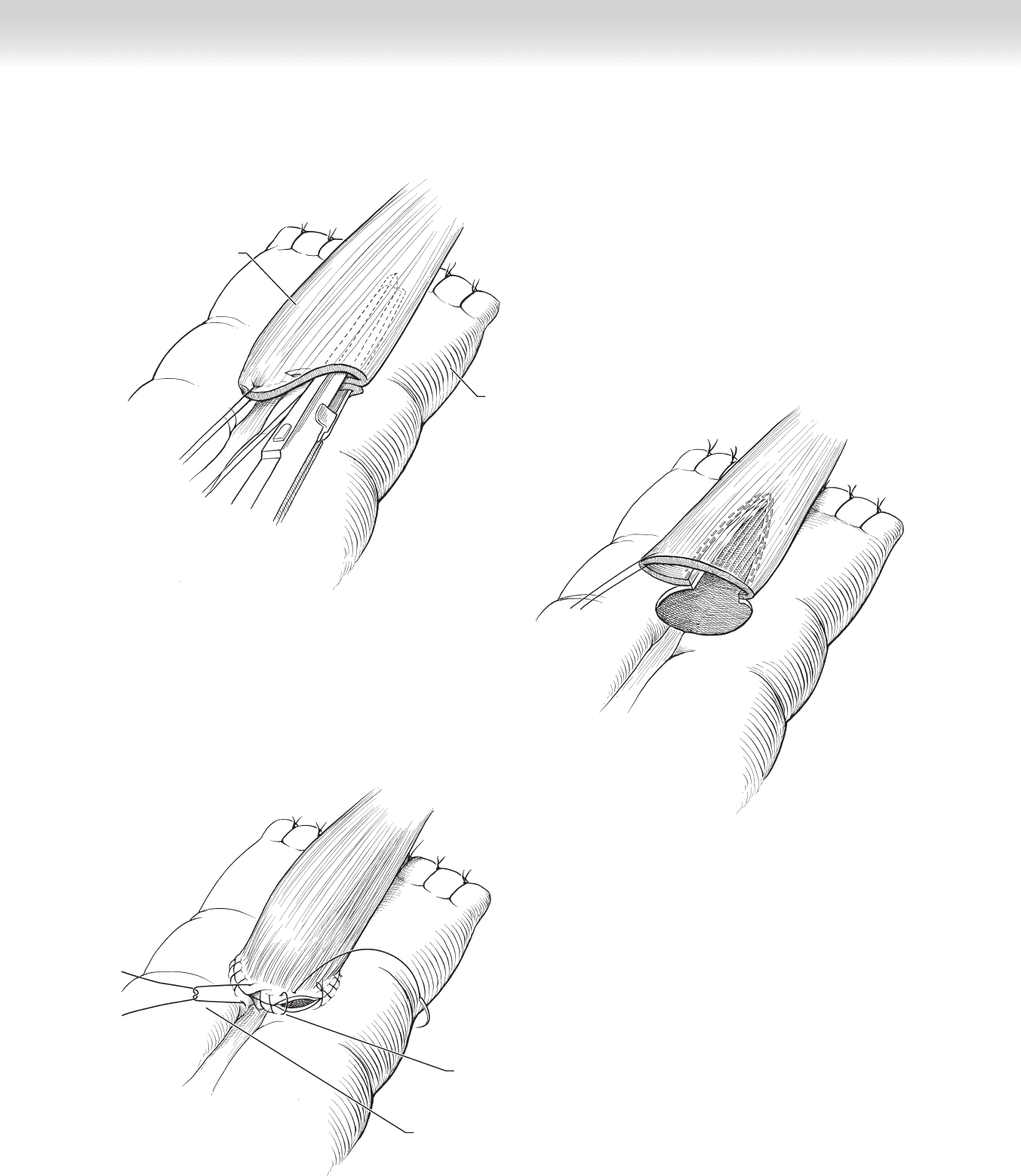
proximal anastomosis may be hand-sewn in two layers or stapled (Figure 18-23). The
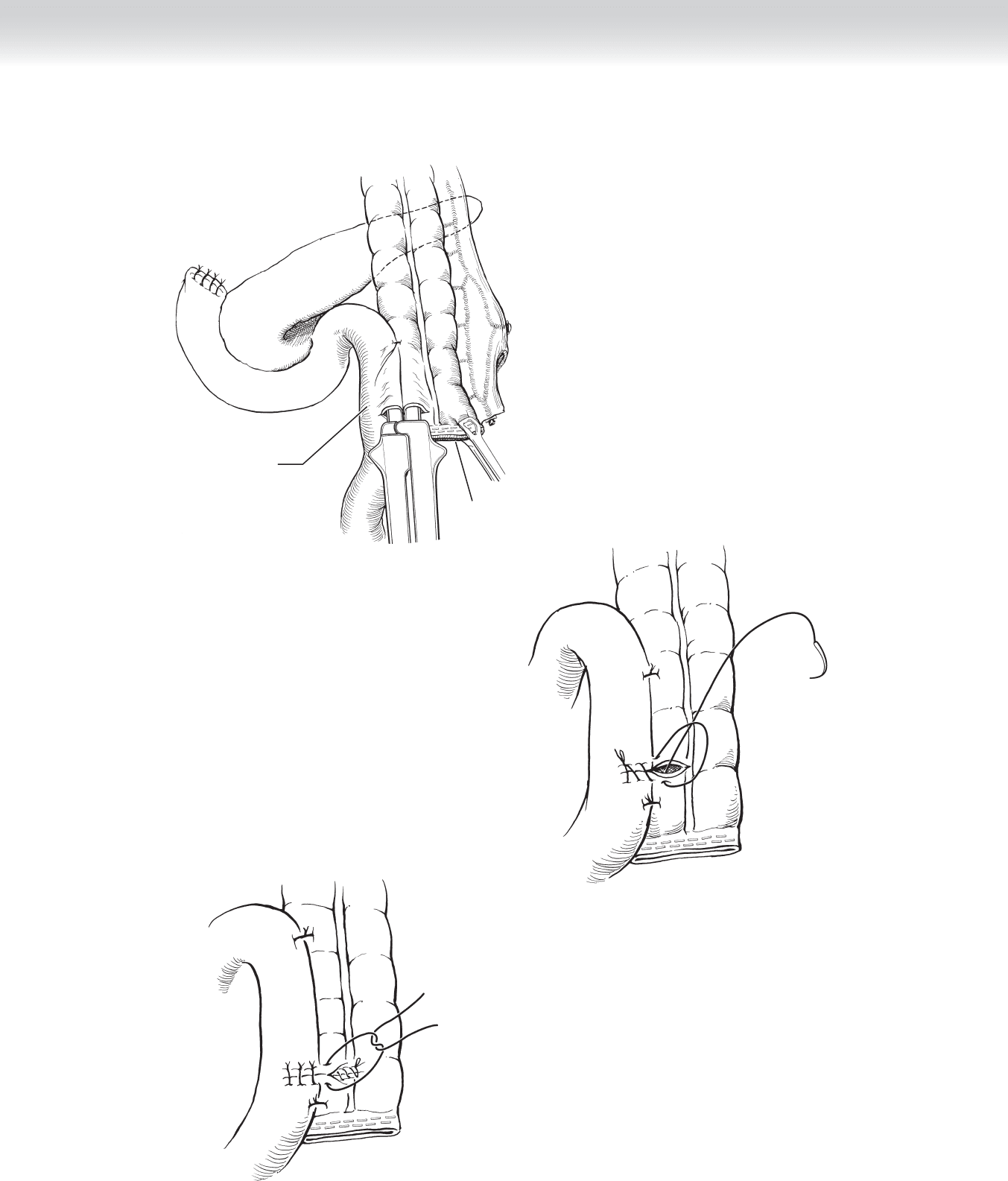
distal anastomosis between the proximal jejunum and colon is closed with an EEA stapler
(Figure 18-24).
Descending colon
Transverse colon
Left
colic artery
FIGURE 18 –19
Text continued on p. 225
CHAPTER 18 • Esophagogastrectomy 221
Heart
Esophagus
Substernal route
Abdominal aorta
Duodenum
Jejunum
Colon
Posterior
mediastinal
route
Esophagus
Heart
Abdominal aorta
Duodenum
Jejunum
Colon
FIGURE 18 –20
FIGURE 18 –21
222 Section III • The Esophagus
Left lung
Transpleural route
Esophagus
Right lung
Heart
FIGURE 18 –22
CHAPTER 18 • Esophagogastrectomy 223
B
A
Colon
Esophagus
C
Reinforcing anastomosis
of colon and esophagus
with interrupted sutures
Securing colon and esophagus
with running sutures
FIGURE 18 –23
224 Section III • The Esophagus
Proximal jejunum
A
Distal end
of colon
B
C
FIGURE 18 –24
CHAPTER 18 • Esophagogastrectomy 225
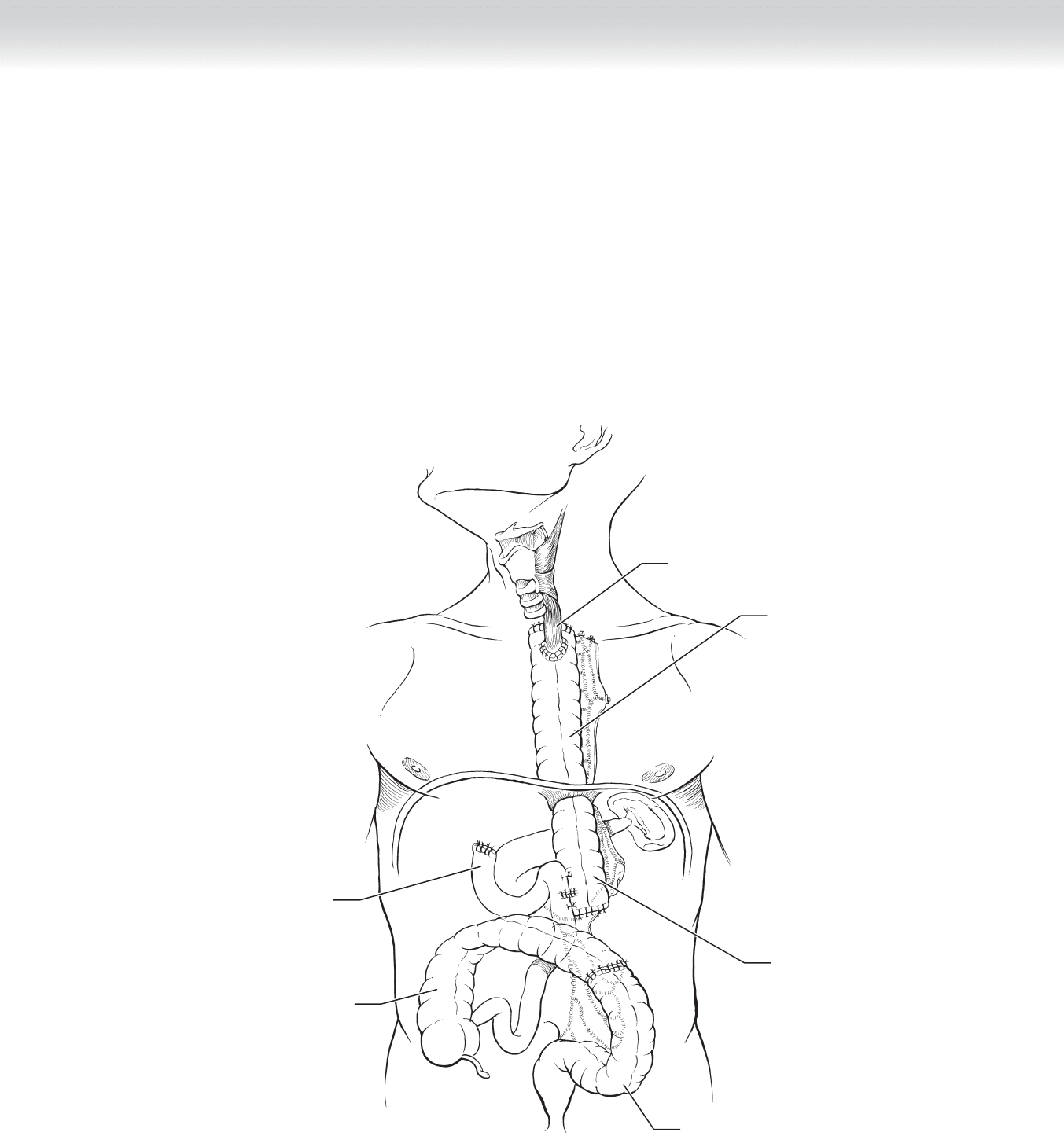
◆ The graft should be sutured to the crus of the diaphragm to avoid migration of the colon
into the thoracic cavity. The remainder of the closure is carried out as described previously
(Figure 18-25).
◆ Total gastrectomy with ascending colon graft: The ascending colon may be used if the
descending colon has been affected by severe diverticular disease, atherosclerotic disease of
the inferior mesenteric artery, or splenic vein thrombosis that extends to the inferior mesen-
teric vein.
Descending colon
Esophagus
Descending
colon
Sigmoid colon
Ascending colon
Duodenum
FIGURE 18 –25
226 Section III • The Esophagus
◆ The blood supply of the right colon from the marginal artery should be inspected by
clamping the ileocolic and right colic arteries. The ascending colon is harvested, leaving the
marginal artery intact (Figure 18-26).
Left
colic artery
Middle
colic artery
Descending
colon
Superior
mesenteric
artery
Transverse colon
Incision
FIGURE 18 –26
CHAPTER 18 • Esophagogastrectomy 227
◆ A section of ileum and the ileocecal valve may be included as part of the graft, because the
size of the ileum matches well with that of the esophagus and because the valve may pro-
vide some protection against refl ux. However, refl ux esophagitis is unusually high in the
neck and the valve may result in mild obstruction.
◆ After measuring out the length of colon needed, the surgeon divides the ascending colon
with a GIA stapler and reanastomoses the remaining colon. The graft is rotated and the
proximal end is brought into the neck for the anastomosis. The distal anastomosis can be
performed with an EEA stapler or a side-to-side stapled technique. The closure is performed
as described previously (Figure 18-27).
Ascending colon
Esophagus
Descending
colon
Transverse colon
Sigmoid colon
Ileum
Duodenum
FIGURE 18 –27