Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

188 Section III • The Esophagus
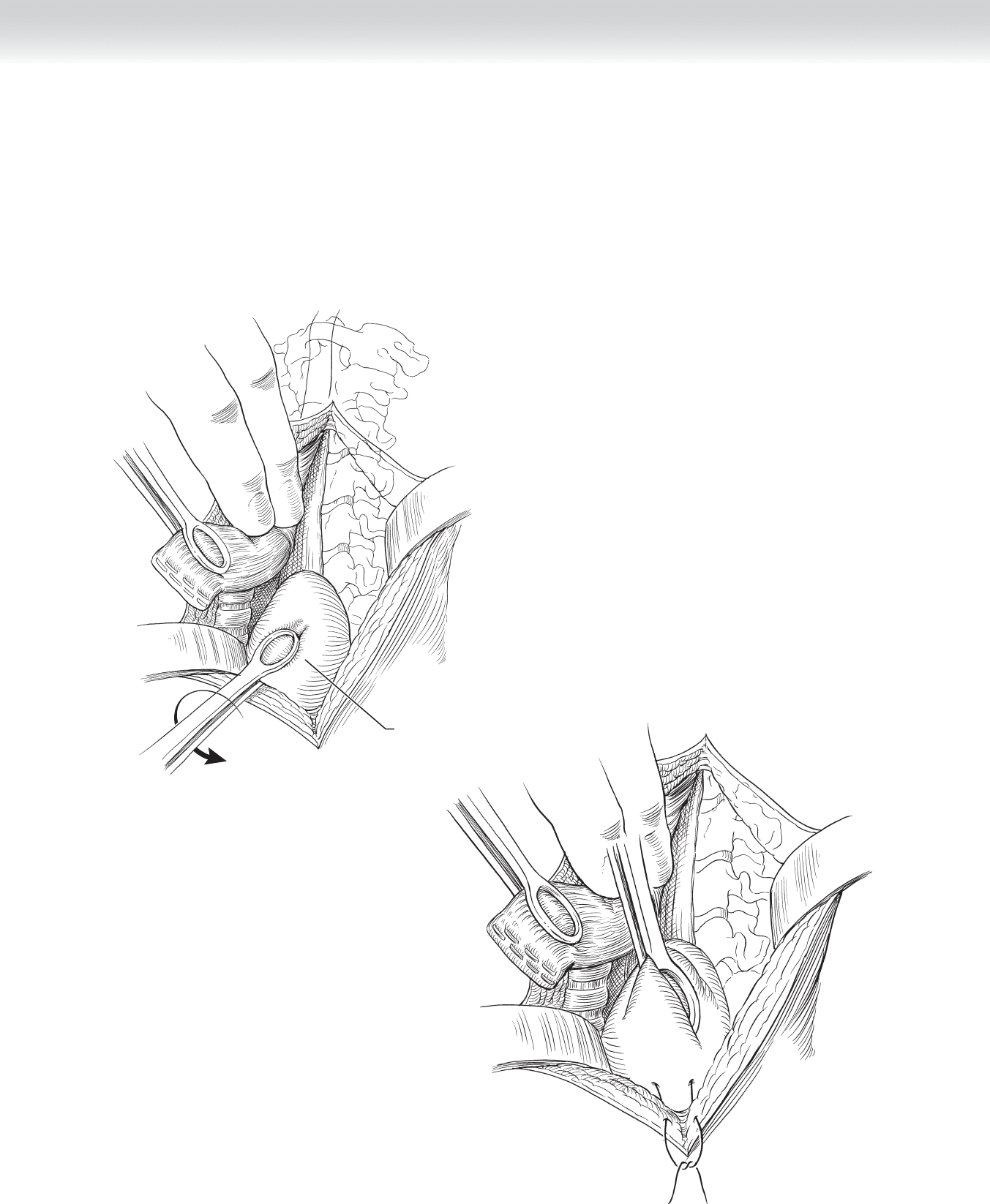
◆ Many techniques have been described to complete the cervical esophagogastric anastomo-
sis. Stapled anastomoses have shown a lower incidence of anastomotic leak over hand-sewn
anastomoses. Once an adequate length of stomach (4 to 5 cm) has been mobilized above
the clavicles, the suture line from the lesser curve is oriented toward the patient’s right, and
a traction suture is placed on the anterior wall of the stomach at the lower aspect of the
neck wound (Figures 16-21 and 16-22).
FIGURE 16 –22
Medial rotation
of stomach
FIGURE 16 –21
CHAPTER 16 • Esophagectomy—Transhiatal 189
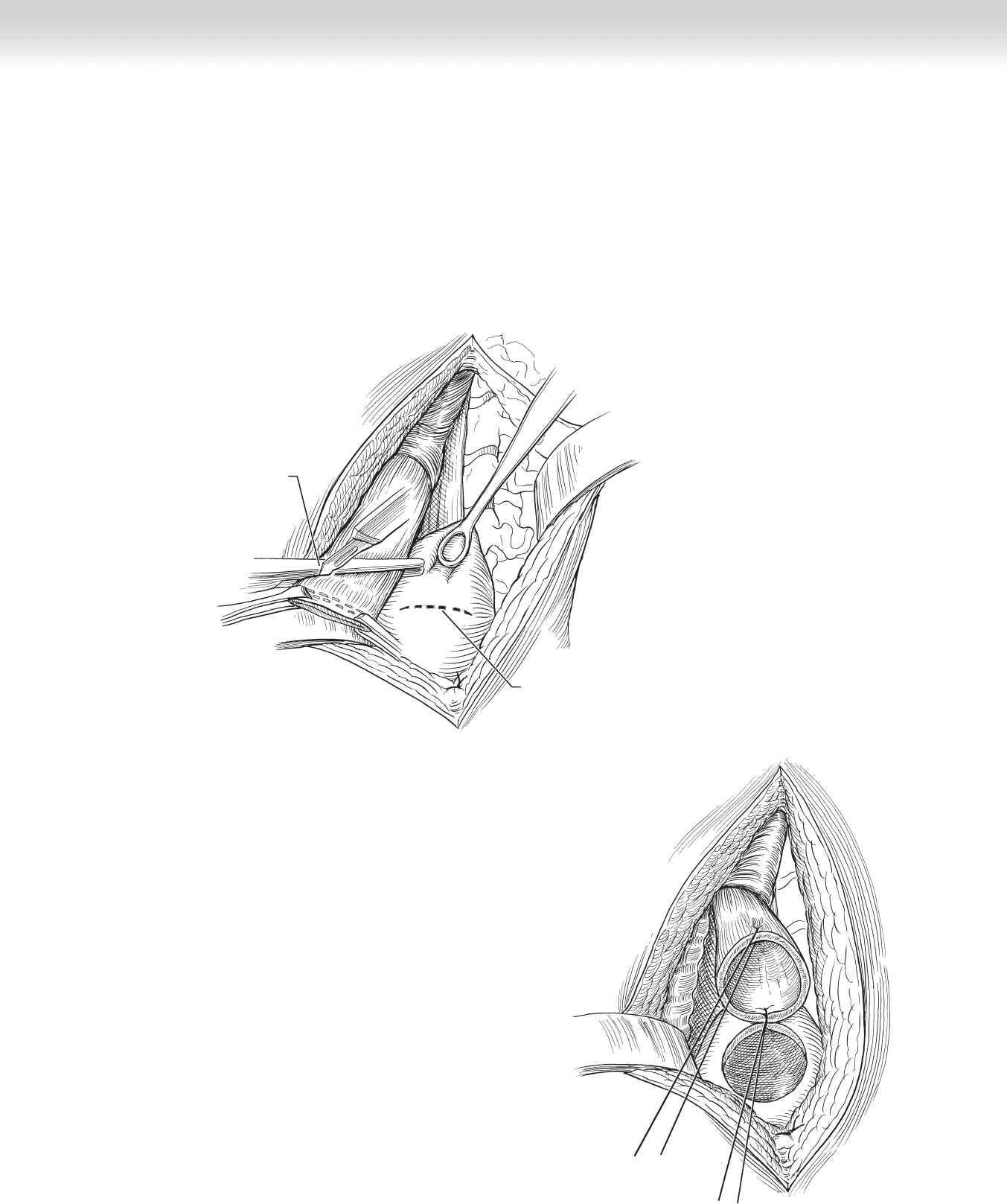
◆ A 1.0- to 1.5-cm gastrotomy is performed on the anterior gastric wall, 3 to 4 cm distal to
the tip of the fundus lying high in the neck (Figures 16-23 and 16-24).
◆ An atraumatic clamp is placed parallel to the esophageal staple line, keeping the oblique
orientation to ensure the anterior portion of the esophagus is longer than the posterior por-
tion to facilitate the anastomosis.
Incision in
stomach
Cutting esophagus
to appropriate angle
FIGURE 16 –23
FIGURE 16 –24
190 Section III • The Esophagus
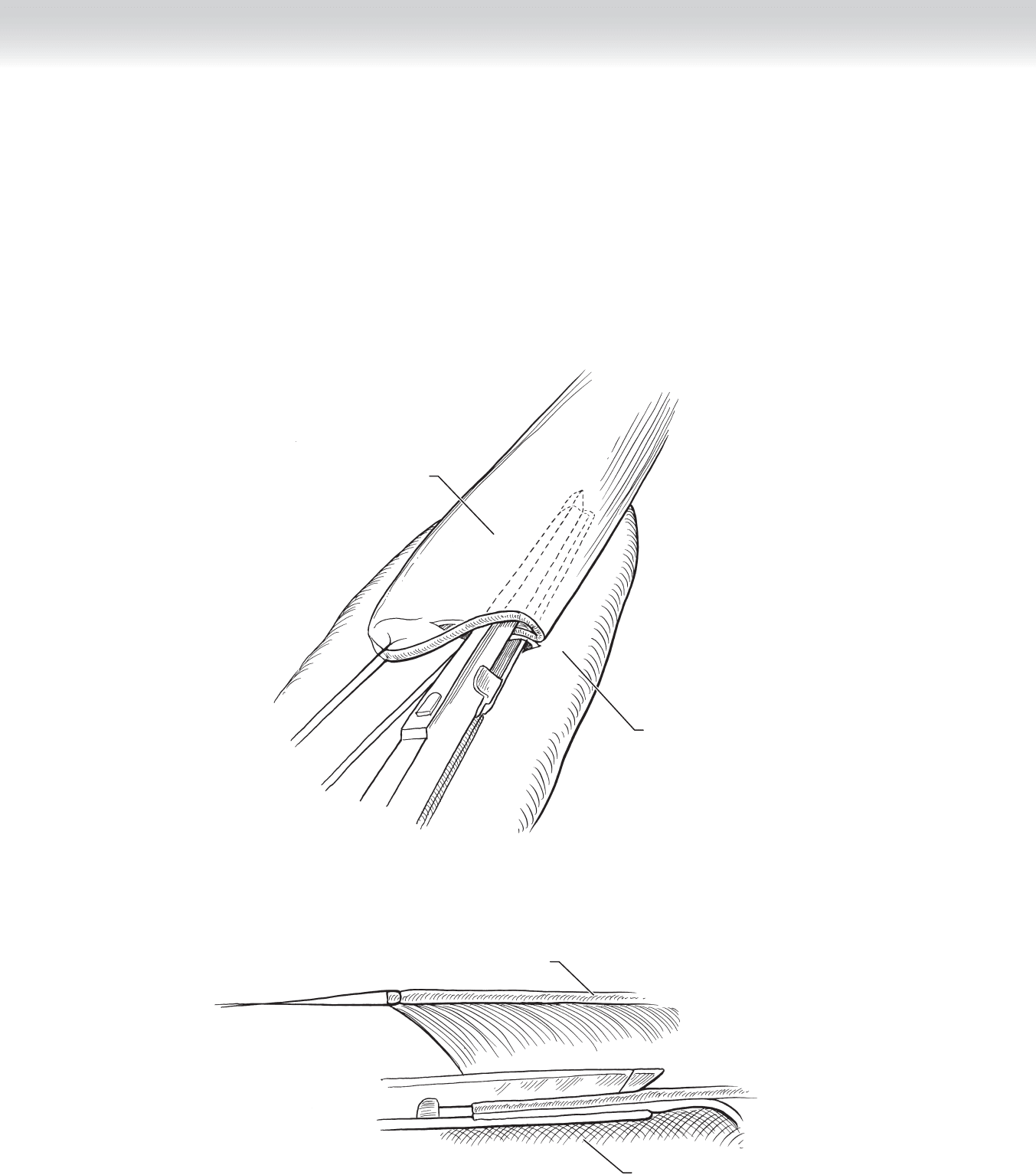
◆ A traction stitch is placed on the anterior corner of the cervical esophagus and pulled
caudad while one arm of the endoscopic gastrointestinal anastomosis (EndoGIA) stapling
device is placed through the gastrotomy toward the fundus and the other arm placed into
the esophagus along its posterior wall. The stapling device is fi red and individual 4-0
absorbable sutures are then placed at the corners of the stapled anastomosis. At this point
the anesthesiologist inserts a nasogastric (NG) tube while the surgeon guides the tube
through the partially completed anastomosis and into the distal stomach (Figure 16-25).
Stomach
Esophagus
A
Stomach
Esophagus
B
FIGURE 16 –25
CHAPTER 16 • Esophagectomy—Transhiatal 191
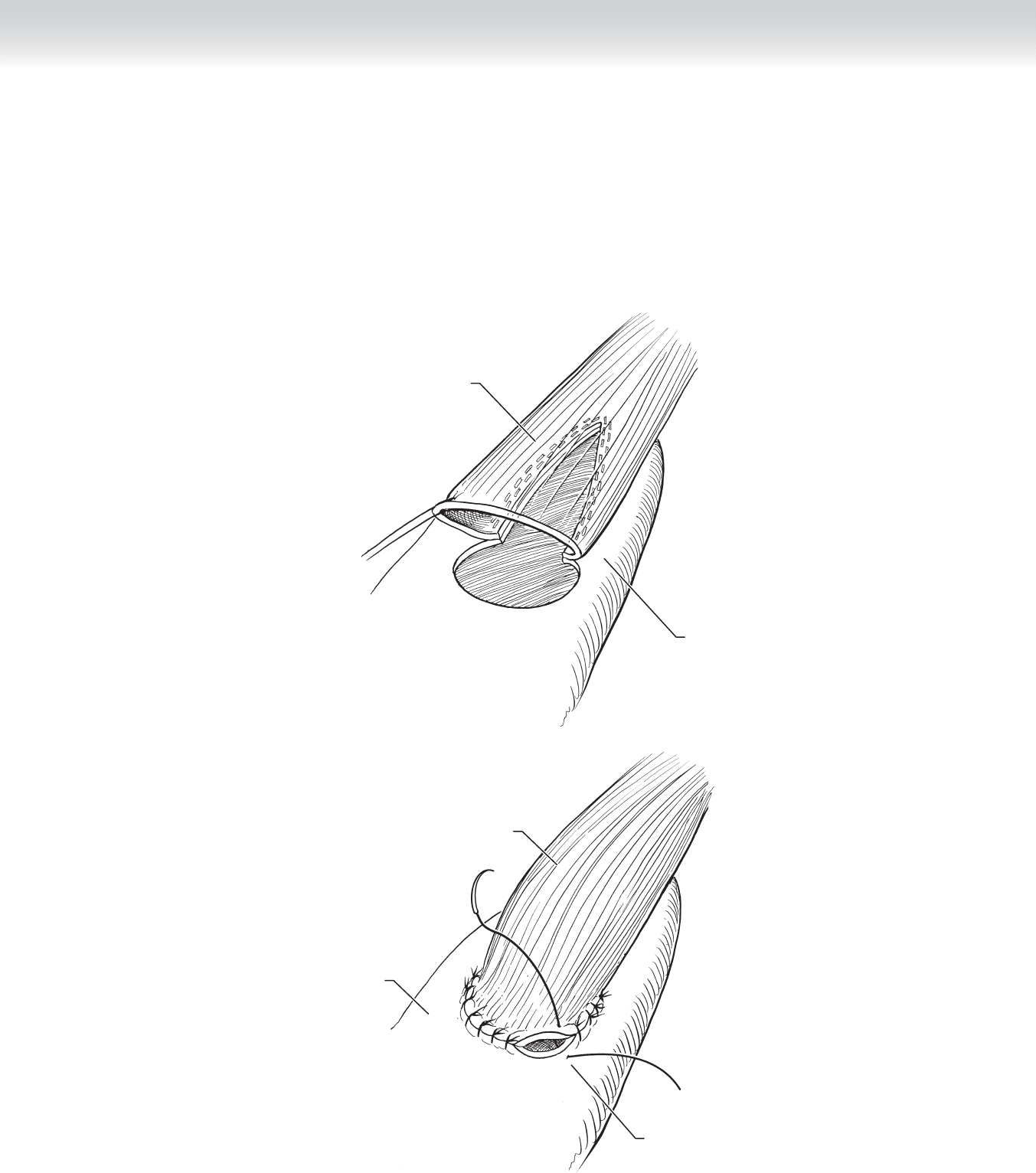
◆ The remaining small opening between the esophagus and gastrotomy is closed in two
layers. A running 4-0 absorbable suture is used for the fi rst layer followed by
interrupted 4-0 Lembert stitches to complete the anastomosis (Figure 16-26).
Stomach
Esophagus
A
Securing the stomach
and esophagus with
interrupted sutures
Stomach
Esophagus
B
FIGURE 16 –26
192 Section III • The Esophagus
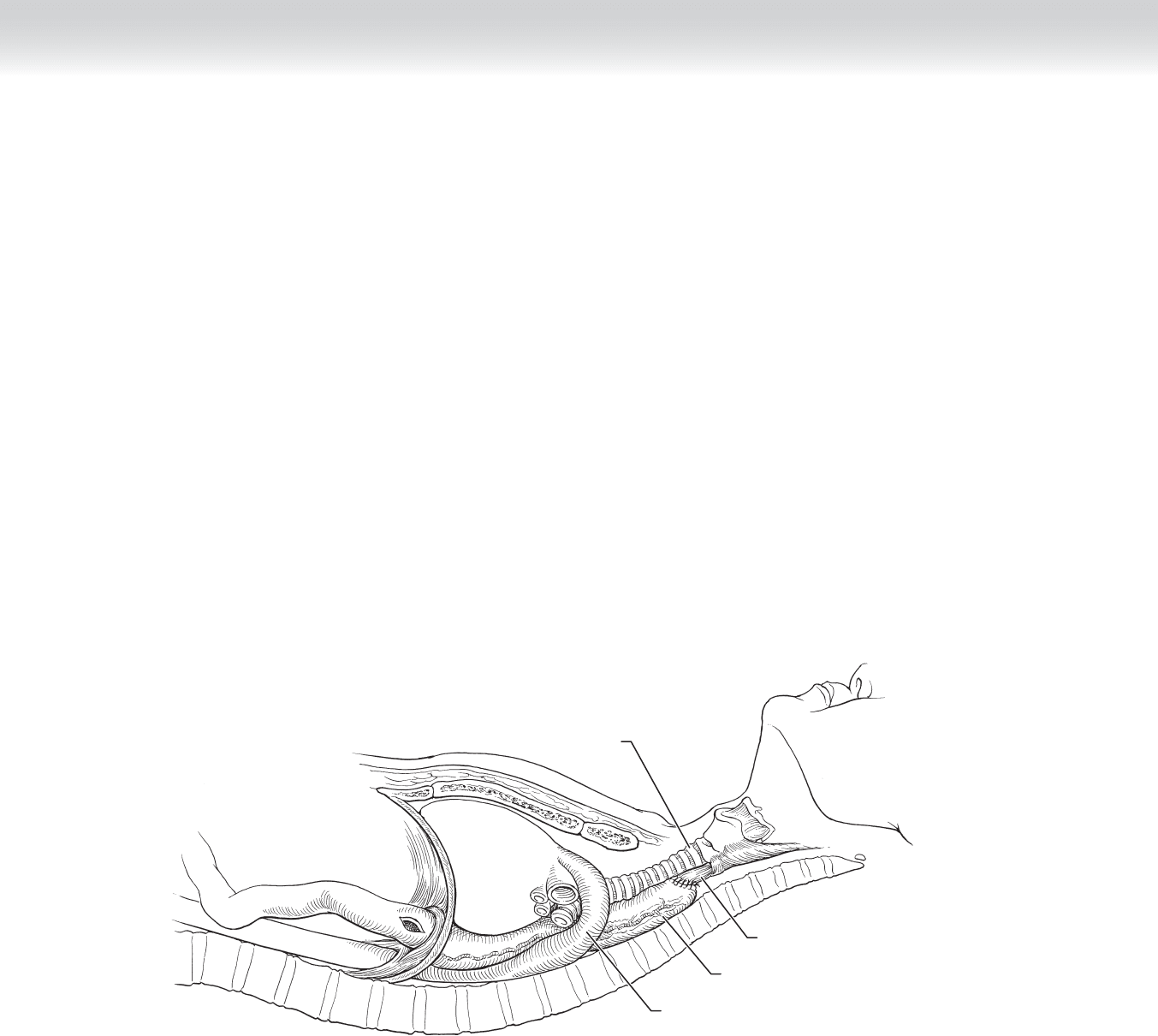
◆ The neck wound is fi lled with saline and the anesthesiologist gently introduces 50 mL of air
into the NG tube while the surgeon occludes the distal stomach and observes for air bub-
bles at the anastomosis in the neck. The completed anastomosis should lie high in the neck
without tension (Figure 16-27).
3. CLOSING
◆ Before closure, the entire stomach should be inspected for areas of necrosis. The abdominal
fascia is closed with an 0-looped running polydioxanone suture (PDS) or according to sur-
geon preference, then the skin closed with staples. In the neck, a small Jackson-Pratt drain
is placed in the surgical bed and exited through a separate stab incision in the lateral neck.
The platysma is approximated with a running 4-0 absorbable suture, then the skin closed
with a second 4-0 to 5-0 absorbable stitch. A chest radiograph should be obtained in the
operating room to ensure no pneumothorax or hemothorax is present. If pneumothorax or
hemothorax is present, appropriate chest tubes should be inserted.
Aorta
Heart
Stomach
Esophagus
Trachea
FIGURE 16 –27

CHAPTER 16 • Esophagectomy—Transhiatal 193
STEP 4: POSTOPERATIVE CARE
◆ The need for extensive postoperative monitoring in the intensive care unit (ICU) is
based on surgeon preference, patient comorbidities, blood loss, and length of procedure.
However, routine ICU care is not required postoperatively.
◆ Hallmarks to a rapid recovery lie in adequate pain control, physical therapy, and pulmonary
toilet.
◆ The esophagogastrostomy should be evaluated on postoperative day 4 or 5 with a contrast
swallow study. If no leak is present, a diet is initiated and the drain is removed as long as
the output does not increase with feeding.
◆ If an anastomotic leak occurs, the neck incision should be opened and packed with moist
gauze 2 to 3 times daily. The wound is allowed to granulate and close secondarily.
STEP 5: PEARLS AND PITFALLS
◆ Identify and preserve the right gastroepiploic and right gastric arteries during mobilization
of the stomach.
◆ Vagal fi bers around the midesophagus can be diffi cult to dissect bluntly. Using the vertebral
bodies posteriorly as an anvil against which to compress tissues can facilitate blunt dissection.
◆ Communicate with the anesthesiologist, especially during transthoracic dissection when
periods of hypotension are common.
◆ Keep dissection close to the proximal esophagus to minimize potential injury to the recur-
rent laryngeal nerves.
SELECTED REFERENCES
1. Orringer MB, Marshall B, Iannettoni MD: Eliminating the cervical esophagogastric anastomotic leak with a
side-to-side stapled anastomosis. J Thorac Cardiovasc Surg 2000;119:277-288.
2. Orringer MB, Marshall B, Stirling MC: Transhiatal esophagectomy for benign and malignant disease.
J Thorac Cardiovasc Surg 1993;105:265-276.

194
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the anatomy of the esophagus is critical before under-
taking surgical procedures on the esophagus.
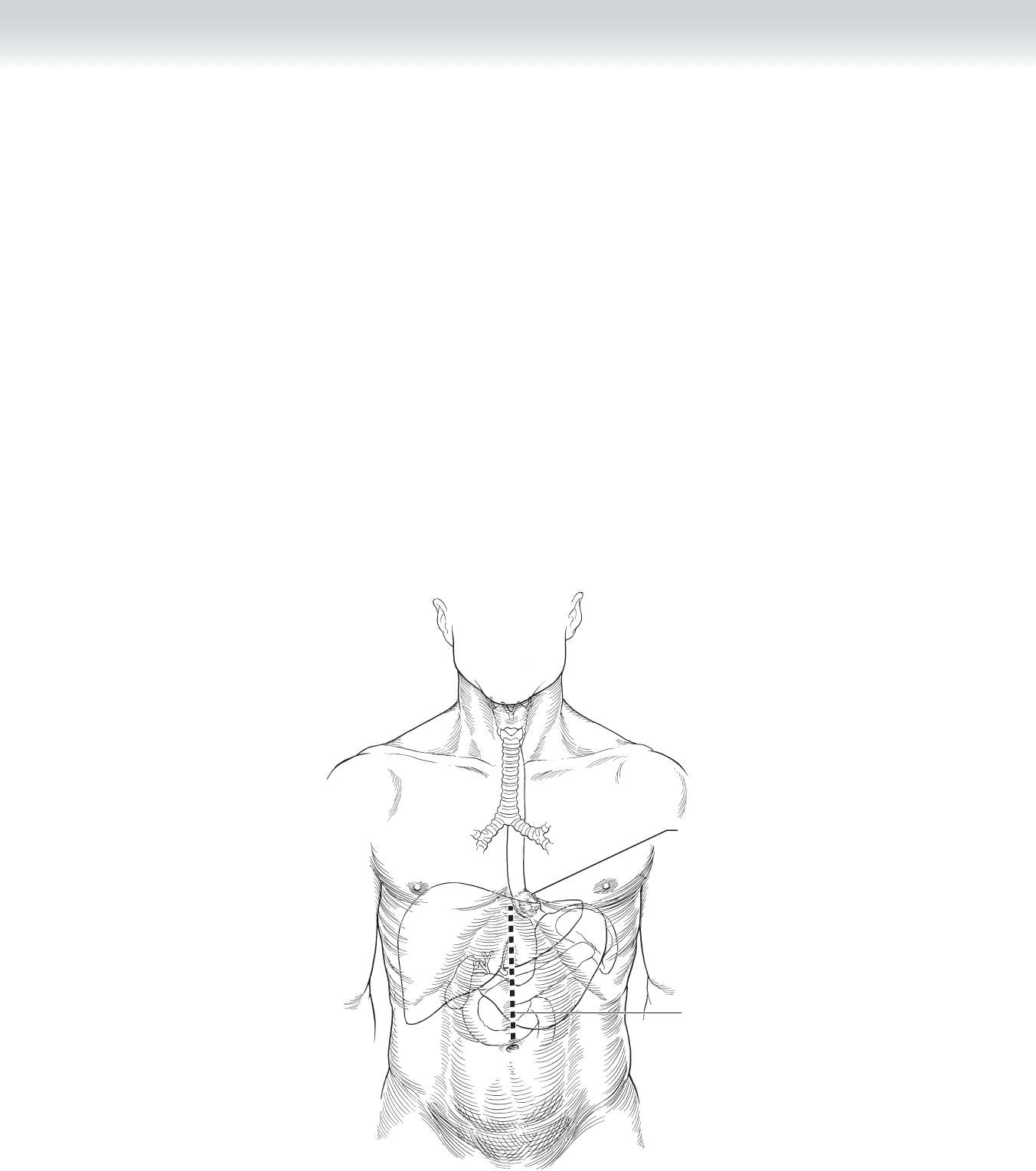
◆ Figure 17-1 demonstrates key anatomic features that should be considered before perform-
ing a transthoracic esophagectomy.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for transthoracic esophagectomy include carcinoma, caustic injury with stricture
or dysplastic mucosal changes, and other benign diseases. Most surgeons agree that benign
disease is best treated with transhiatal esophagectomy, which eliminates the risk of intrathoracic
anastomotic leak and spares the patient the discomfort of thoracotomy without compromising
outcomes. If dense adhesions are expected, a transthoracic approach can afford a safer dis-
section of the intrathoracic esophagus under direct vision and eliminate the blind dissection
and potential for massive hemorrhage, which is rarely associated with transhiatal esophagec-
tomy. For tumors of the proximal esophagus and mid-esophagus, a right thoracotomy is pre-
ferred, whereas a left thoracotomy is preferred for distal esophageal tumors.
◆ Advocates of the transthoracic approach for cancer resection point out that a more complete
lymph node dissection can be accomplished by direct visualization of the operative fi eld.
Advocates of the transhiatal approach point to a perceived overall lower morbidity rate.
Despite multiple studies over the years with trends in both directions, the aggregate experi-
ence has shown no difference in morbidity, mortality, or outcome between the transthoracic
and transhiatal approaches. The most important determining criteria are experience of the
surgeon, need for exposure, and patient selection.
◆ Informed consent is obtained and the patient is made nothing-by-mouth status at least 8
hours before the procedure. A bowel preparation can be given to the patient the day before
the procedure in case the colon is needed as a reconstruction conduit. In the operating
room, a radial artery catheter should be used for continuous blood pressure monitoring.
CHAPTER
17
Esophagectomy—Transthoracic
(Ivor Lewis)
David B. Loran and Joseph B. Zwischenberger
Central venous access is not routinely necessary. However, if access is needed, the
contralateral neck veins should be used to allow the surgeon complete access to the neck
during operation. A double-lumen endotracheal tube is used to defl ate and retract the lung
to facilitate dissection.
◆ General endotracheal anesthesia is mandatory for this procedure.
◆ The patient is placed supine on the operating table with the head slightly extended. A roll
is placed under the patient to slightly elevate the side of the patient in anticipation of a tho-
racotomy. The patient’s arm is either elevated and draped out of the fi eld or prepped into
the fi eld to allow its mobility during the procedures. Alternatively, the patient can be placed
supine during the abdominal portion of the procedure, then re-prepped and draped in the
lateral position for the thoracic portion.
◆ The skin over the entire neck, chest, and abdomen should be prepped with povidone-
iodine (Betadine).
CHAPTER 17 • Esophagectomy—Transthoracic (Ivor Lewis) 195
Tumor in
distal esophagus
Incision
MC
FIGURE 17 –1
STEP 3: OPERATIVE STEPS
1. INCISION
◆ Transthoracic esophagectomy uses two incisions: a midline abdominal incision and a thora-
cotomy. An upper midline supraumbilical incision from the xiphoid process to the umbili-
cus is used to begin the abdominal portion of the procedure. The incision should be
extended cephalad to the left of the xiphoid process to adequately expose the esophageal
hiatus. A self-retaining retractor can facilitate exposure of the upper abdomen.
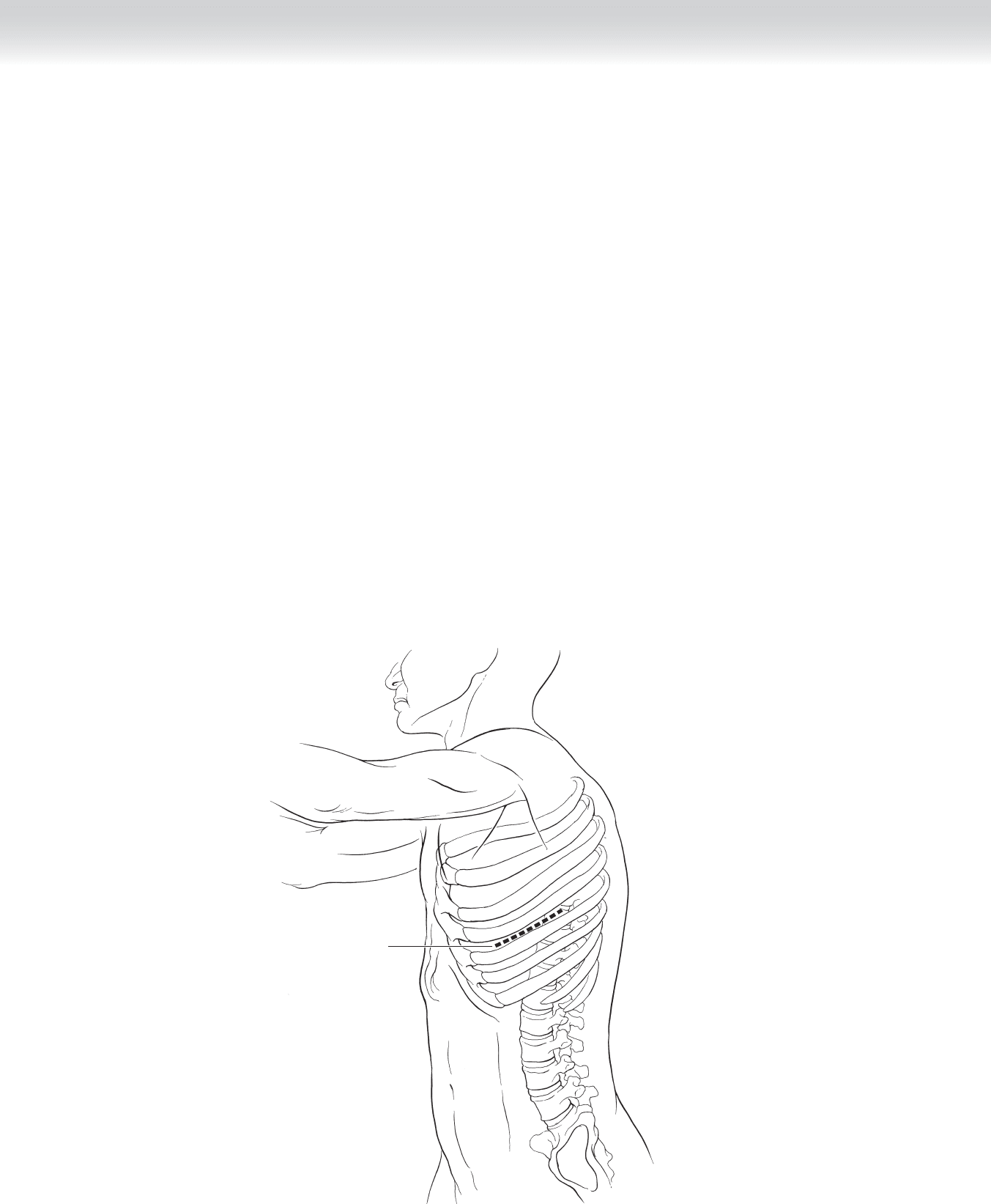
◆ A right thoracotomy is recommended for a mid-thoracic or upper thoracic cancer. A left
thoracotomy is recommended for a cancer in the lower one third of the thorax or in the
esophagus (Figure 17-2).
2. DISSECTION
◆ The stomach is completely mobilized as previously described for transhiatal esophagectomy
(Chapter 16). A lateral thoracotomy is performed in the sixth to seventh intercostal space and
the lung is retracted cephalad. If a right thoracotomy is used, the azygous vein should be iden-
tifi ed and suture ligated to better reduce the risk of postoperative hemorrhage (Figure 17-3).
Section III • The Esophagus196
Incision
FIGURE 17 –2
CHAPTER 17 • Esophagectomy—Transthoracic (Ivor Lewis) 197
Tumor in
distal esophagus
Esophageal tumor
Left lung
Heart
FIGURE 17 –3
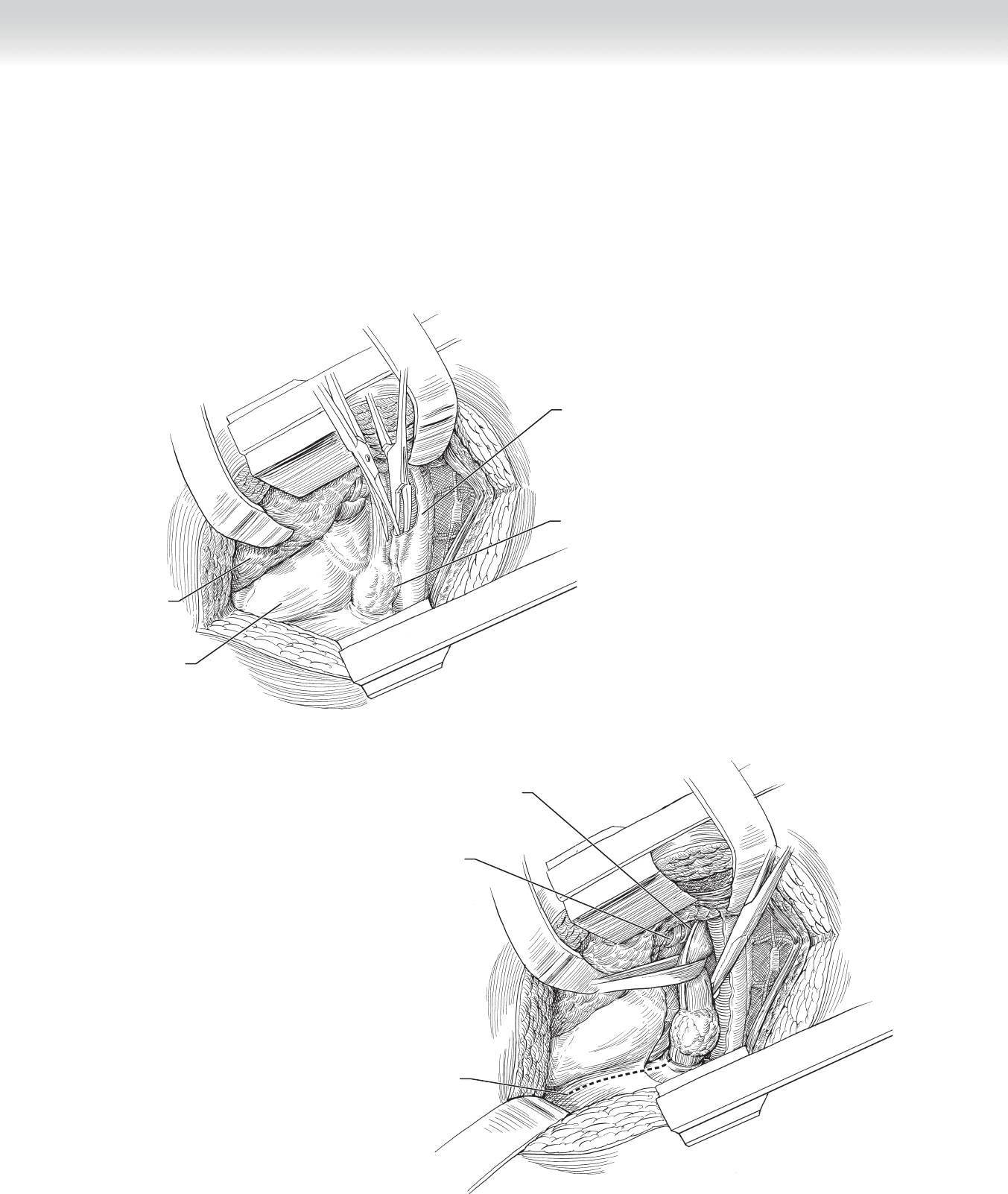
◆ The pleura overlying the esophagus is incised and the esophagus is dissected free from its
bed. A Penrose drain is used to encircle the esophagus and provide retraction during the
dissection. The surgeon should be able to include the lymph nodes surrounding the esoph-
agus in the dissection (Figure 17-4). Care must be taken not to injure the posterior mem-
branous trachea during mobilization of the esophagus or tumor or both. Once the esopha-
gus is mobilized it is transected at a point at least 4 cm proximal to the tumor.
Incision in diaphragm
Anterior vagus nerve
Left bronchus and
pulmonary vein
FIGURE 17 –4