Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

168 Section III • The Esophagus
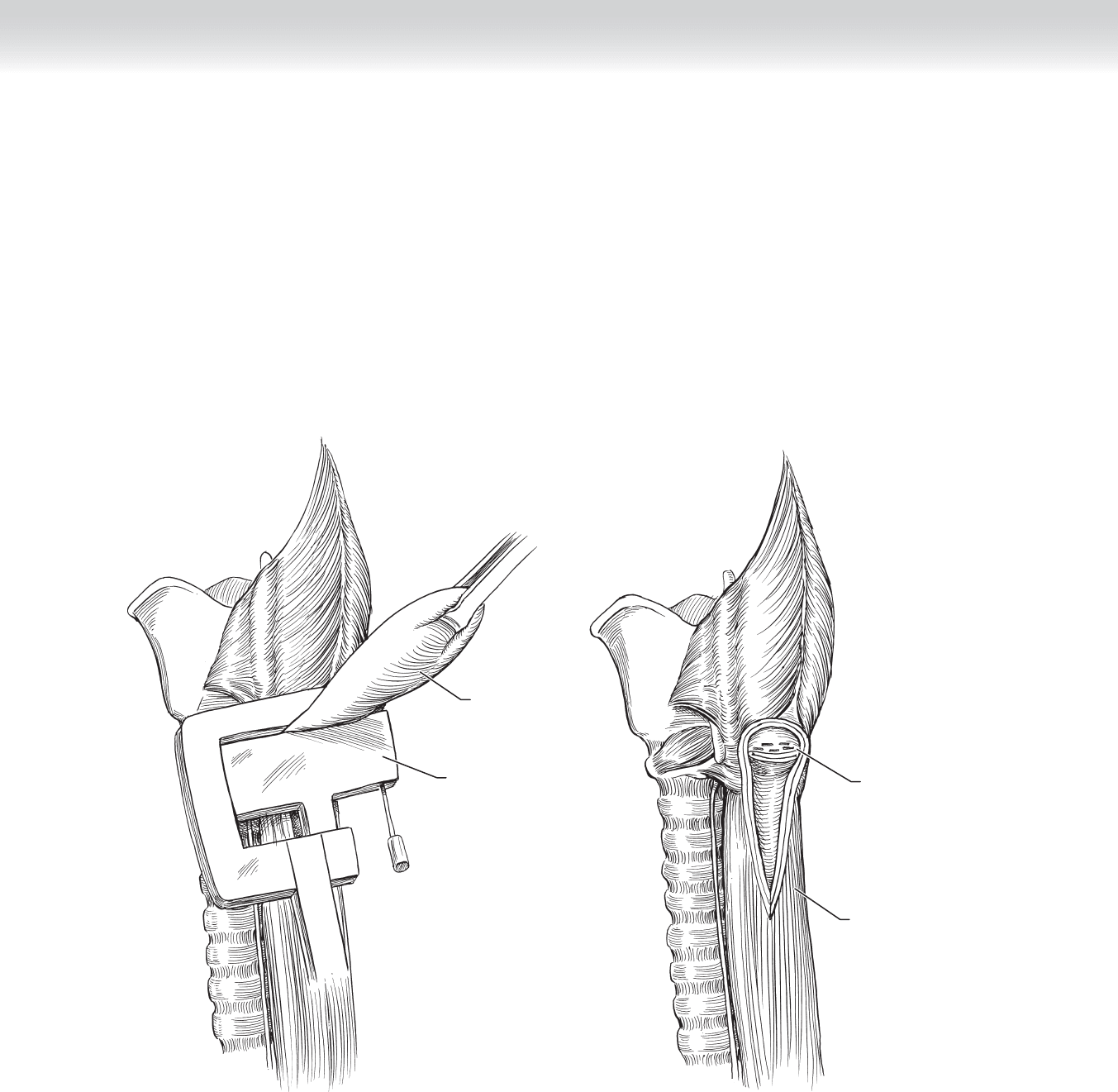
◆ A stapling device with 4.8-mm staples is oriented along the longitudinal esophageal axis
with the bougie in place and is fi red to resect the diverticulum (Figures 15-6 and 15-7).
◆ Alternatively, the diverticula can be resected with a no. 15 blade scalpel and the mucosal
defect closed with a running 4-0 absorbable suture.
Diverticulum
Stapler
FIGURE 15–6
Esophagus
Diverticulum
cut and stapled
FIGURE 15–7
CHAPTER 15 • Zenker’s Diverticula 169
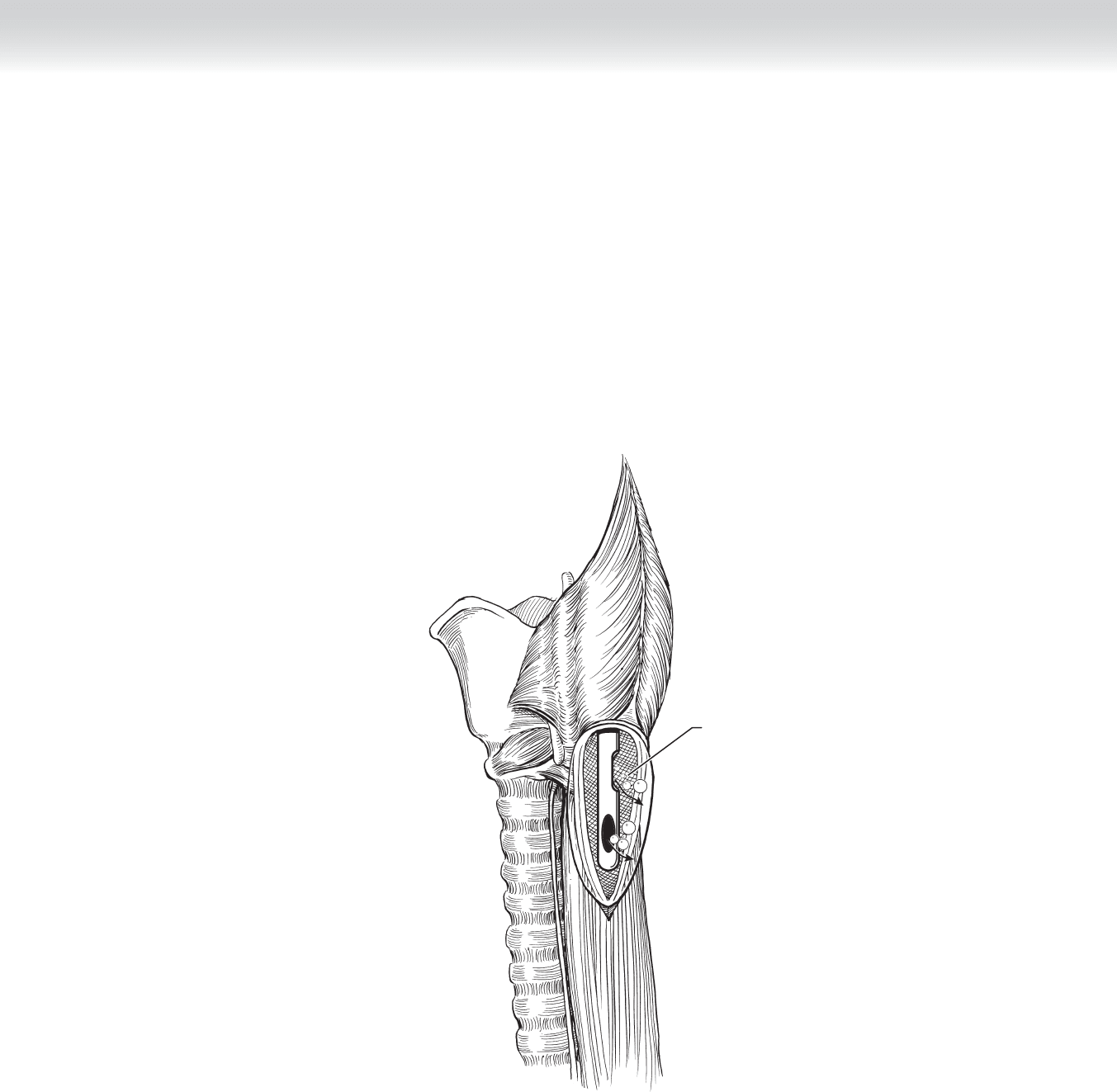
◆ The bougie is removed and the surgeon guides placement of a nasogastric (NG) tube into the
lower pharynx to check for mucosal leaks. The surgical bed is fi lled with water to cover the
suture/staple line while the anesthesiologist gently injects air through the NG tube. If no air
bubbles are seen, mucosal integrity is intact. The staple line is left uncovered and a small
Jackson-Pratt drain is placed in the surgical bed and exited through a separate stab incision
in the neck laterally (Figure 15-8). A leak can be closed primarily with fi ne interrupted
sutures and reinforced with muscle coverage.
Leak test
FIGURE 15–8
170 Section III • The Esophagus
3. CLOSING
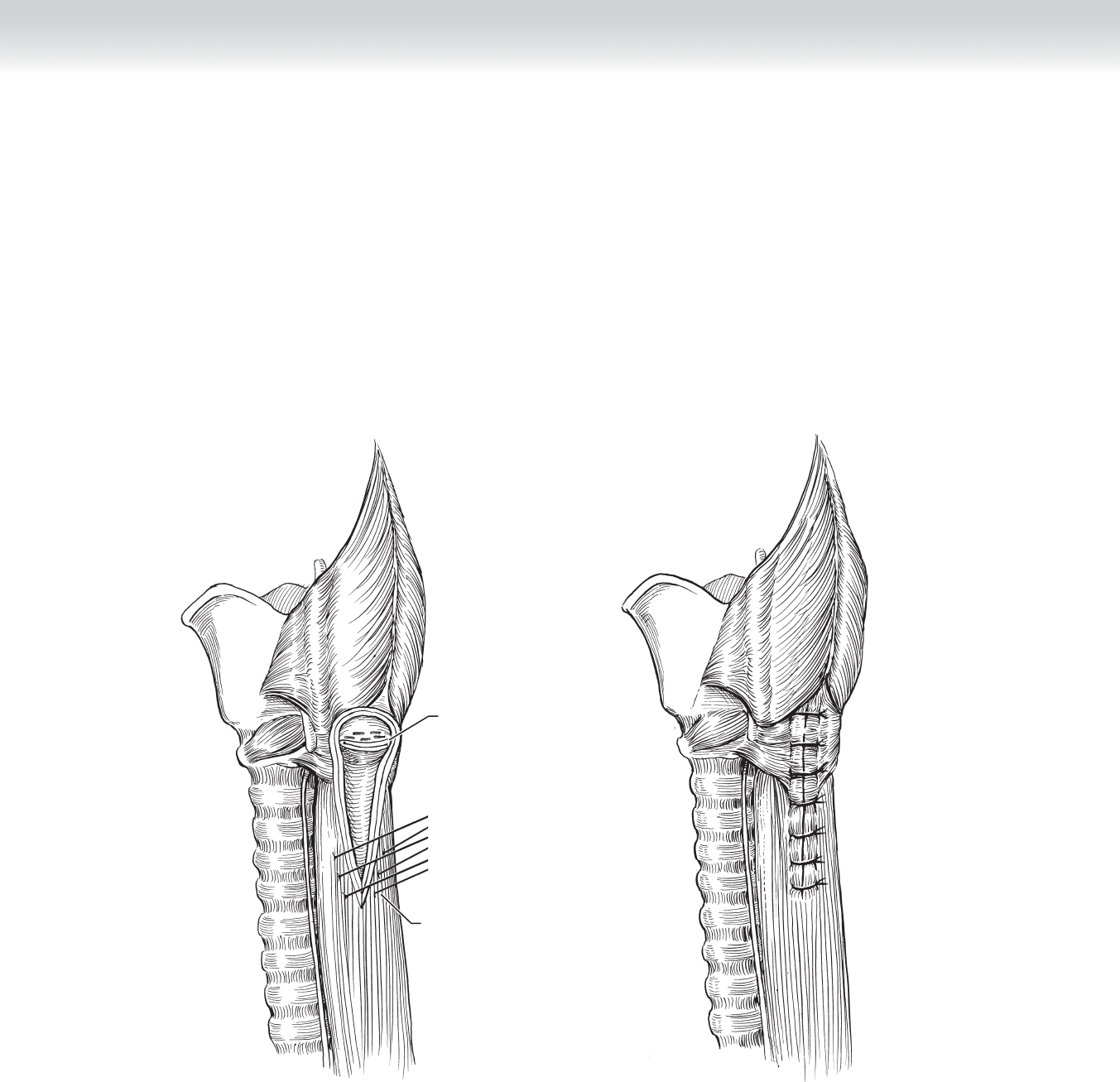
◆ Alternatively, if the muscular layers are intact they can be reapproximated. Retractors are
removed and the platysma is closed with interrupted stitches using 4-0 absorbable suture.
The drain is secured to the skin with a 4-0 silk stitch (Figures 15-9 and 15-10).
FIGURE 15–10
Interrupted
sutures
Diverticulum
cut and stapled
FIGURE 15–9

CHAPTER 15 • Zenker’s Diverticula 171
STEP 4: POSTOPERATIVE CARE
◆ After recovery from anesthesia, the patient is returned to a fl oor bed, with no food allowed
overnight. On the second postoperative day, a contrast esophageal swallow study is per-
formed and a diet started if no leak is present.
◆ The following day, the drain can be removed if no increase in output is observed after initiation
of a diet. The patient can be discharged to home by the third or fourth postoperative day.
STEP 5: PEARLS AND PITFALLS
◆ Recognize that Zenker’s diverticula are the sequelae of cricopharyngeal/esophageal dysmotil-
ity. Many patients will present with cricopharyngeal dysfunction (choking or aspiration or
both) without a Zenker’s diverticulum. The goal of the operation is to address the dysmotil-
ity in a two-step process: myotomy followed by management of the diverticulum.
◆ Recent retrospective reports with endoscopic stapler-assisted diverticulotomy and carbon
dioxide laser endoscopic diverticulotomy present alternative therapies for Zenker’s divertic-
ula. Advocates note shorter operative time, shorter hospital stay, and quicker return to diet.
The techniques have not been shown to be superior to an open procedure, with a recur-
rence rate of approximately 10%. Carbon dioxide laser endoscopic diverticulotomy is also
an alternative to open surgery, but likewise results in a higher failure rate.
SELECTED REFERENCES
1. Wirth D, Kern B, Guenin MO, et al: Outcome and quality of life after open surgery versus endoscopic
stapler-assisted esophagodiverticulostomy for Zenker’s diverticulum. Dis Esophagus 2006;19:294-298.
2. Chang CY, Payyapilli RJ, Scher RL: Endoscopic staple diverticulostomy for Zenker’s diverticulum: Review
of literature and experience in 159 consecutive cases. Laryngoscope 2003;113:957-965.
3. Chang CW, Burkey BB, Netterville JL, et al: Carbon dioxide laser endoscopic diverticulotomy versus open
diverticulectomy for Zenker’s diverticulum. Laryngoscope 2004;114:519-527.

172
STEP 1: SURGICAL ANATOMY
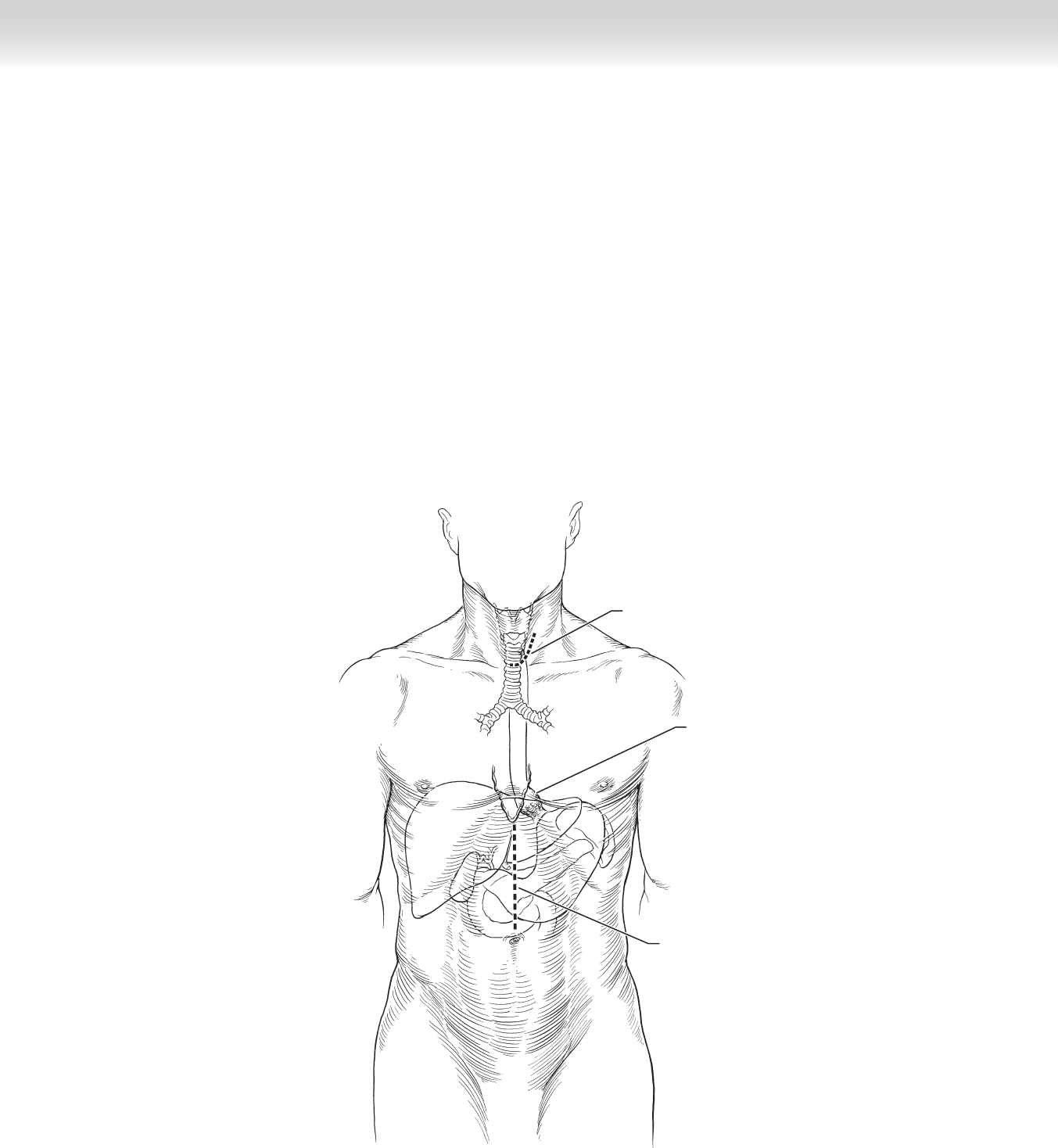
◆ A comprehensive understanding of the anatomy of the esophagus is critical before
undertaking surgical procedures on the esophagus.
◆ Figure 16-1 demonstrates key anatomic structures that must be considered before
performing a transhiatal esophagectomy.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Indications for transthoracic esophagectomy include carcinoma, caustic injury with stricture
or dysplastic mucosal changes, and other benign diseases. Most surgeons agree benign disease
is best treated with transhiatal esophagectomy, which eliminates the risk of intrathoracic anas-
tomotic leak and spares the patient the discomfort of thoracotomy without compromising
outcomes. Carcinoma at any level of the esophagus can be safely resected by transhiatal
approach. In performing a transhiatal esophagectomy, the surgeon removes accessible cervical,
intrathoracic, and intra-abdominal lymph nodes for staging, but a complete en bloc resection
of adjacent lymph node–bearing tissue is not accomplished.
◆ Transhiatal esophagectomy results in a lower incidence of pulmonary complications
compared with a transthoracic approach. Anastomotic leak rates range from 12% to 15%
but have been shown to be approximately 3% with a stapled technique. When a leak does
occur, the associated morbidity and mortality are less than that seen for leaks from an intra-
thoracic esophagogastrostomy.
◆ Informed consent is obtained and the patient is made nothing-by-mouth status at least
8 hours before the procedure. A bowel preparation can be given to the patient the day
before the procedure, in case the colon is needed as a reconstruction conduit. In the
operating room, a radial artery catheter should be used for continuous blood pressure
monitoring, because retrocardiac dissection can cause periods of hypotension. Central
venous access is not routinely necessary; however, if needed, the right neck veins should
be used to allow the surgeon complete access to the left side of the neck during opera-
tion. A standard endotracheal tube is used for intubation.
CHAPTER
16
Esophagectomy—Transhiatal
David B. Loran and Joseph B. Zwischenberger
CHAPTER 16 • Esophagectomy—Transhiatal 173
◆ General endotracheal anesthesia is mandatory for this procedure. Close cooperation and
communication between anesthesiologist and surgeon must be maintained, especially during
the transhiatal dissection when transient hypotension is expected. During this time, inhala-
tion anesthetics that can contribute to hypotension should be discontinued, and the inspired
oxygen concentration should be increased.
◆ The patient is placed supine on the operating table with the head slightly extended and
turned to the right. Arms are tucked and protected close to the patient’s body to allow the
surgeon unimpeded access to the neck, chest, and abdomen.
◆ The skin over the entire neck, chest, and abdomen should be prepped with povidone-
iodine (Betadine).
Incision
Tumor in
distal esophagus
Incision
FIGURE 16 –1
174 Section III • The Esophagus
STEP 3: OPERATIVE STEPS
1. INCISION
◆ An upper midline supraumbilical incision from the xiphoid process to the umbilicus is used
to begin the abdominal portion of the procedure. The exposure should be extended cephalad
to excise the xiphoid process to gain maximum access to the esophageal hiatus. A self-
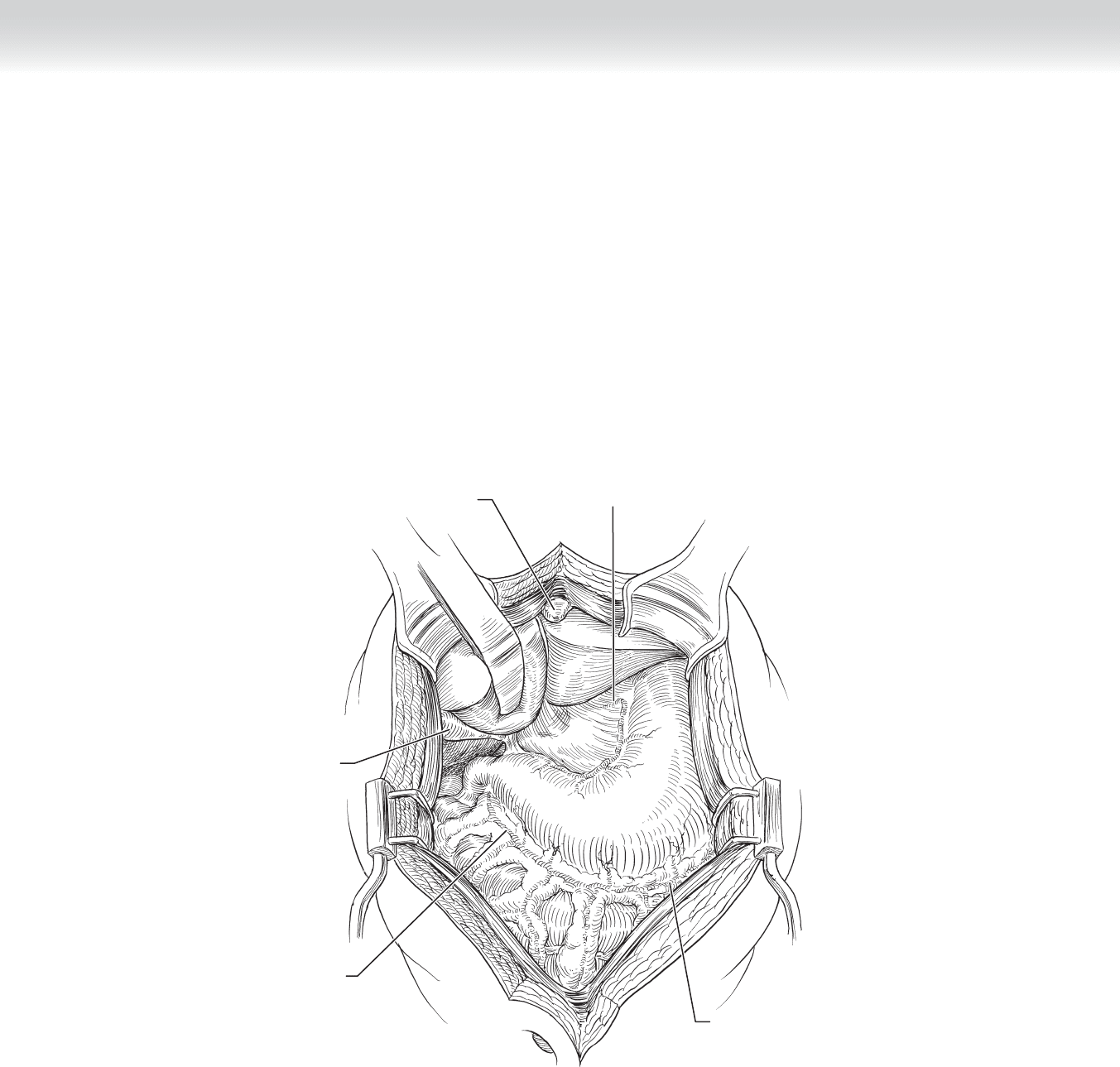
retaining retractor can facilitate exposure of the upper abdomen (Figures 16-1 and 16-2).
Right gastroepiploic
artery
Liver
Stomach
Gallbladder
Xiphoid bone
Left gastric artery
Left gastroepiploic
artery
FIGURE 16 –2
CHAPTER 16 • Esophagectomy—Transhiatal 175
2. DISSECTION
◆ Upon entering the abdomen, the surgeon should perform careful inspection to search for
metastatic disease and to ensure the stomach is free from scarring, shortening, or disease
that will preclude its use as a suitable conduit for reconstruction.
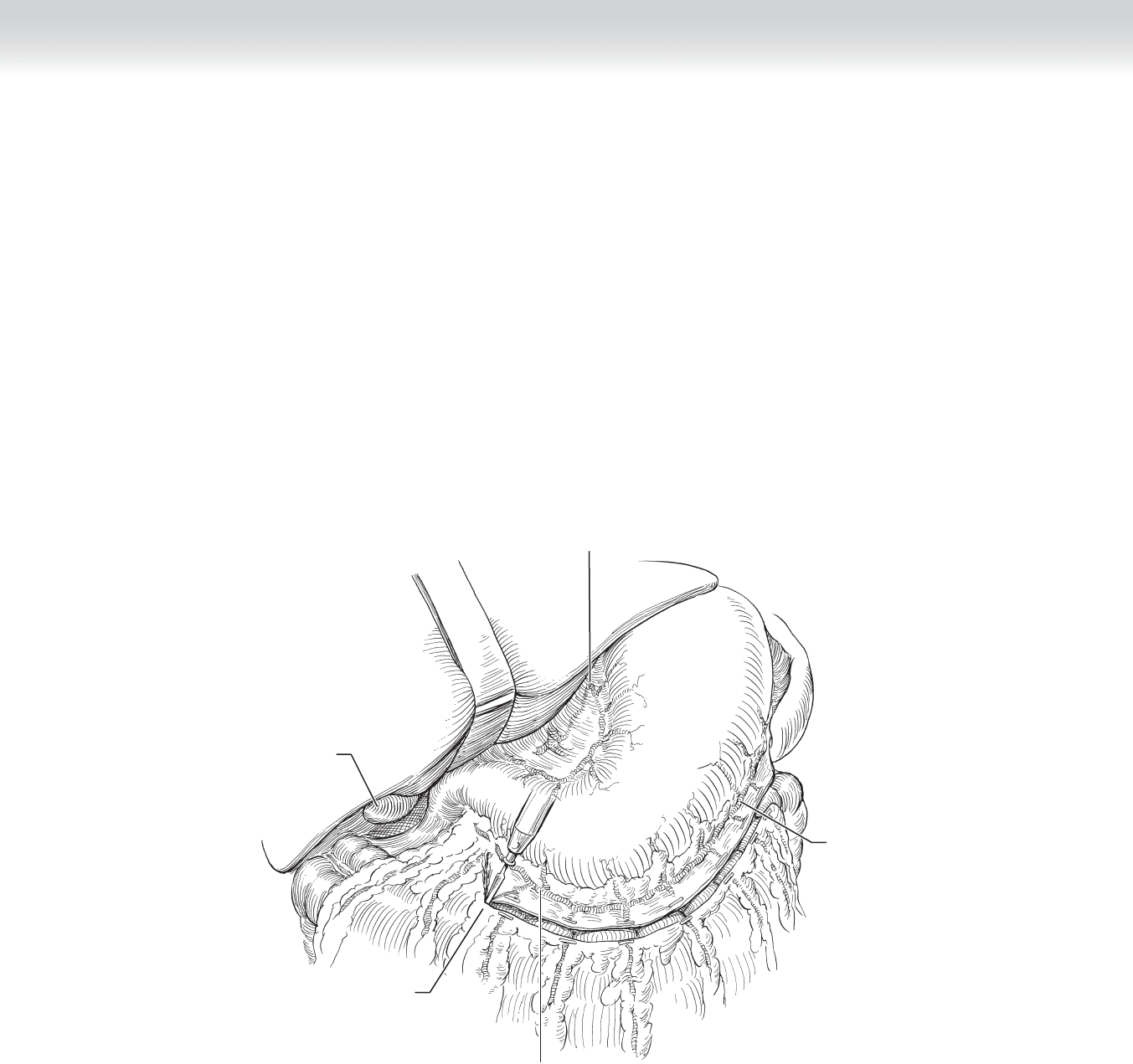
◆ The surgeon must be intimately familiar with the arterial anatomy of the upper abdomen
and early in the course of the dissection must identify the left gastroepiploic artery and
protect this artery throughout the operation (Figure 16-3).
Liver
Stomach
Omentum
Right gastroepiploic artery
Gallbladder
Left gastric artery
Left gastroepiploic
artery
FIGURE 16 –3

176 Section III • The Esophagus
◆ To begin mobilization of the stomach, the left triangular ligament is taken down and the
left liver lobe is retracted to the right. The greater omentum is separated from the greater
curve of the stomach, beginning at an avascular plane approximately at the greater curve’s
midpoint. Dissection is then carried superiorly to the esophageal hiatus, carefully ligating
the left gastroepiploic artery and all short gastric vessels. Care must be taken to avoid
pinching a portion of the stomach wall within ligature ties of the short gastric vessels,
which can later lead to necrosis and perforation of the gastric wall. Once the surgeon has
reached the esophageal hiatus, the peritoneum is incised and the distal esophagus encir-
cled with a Penrose drain to aid in esophageal retraction and dissection. The lesser omen-
tum is dissected from the lesser curve of the stomach, and the left gastric artery is ligated
because its branches supply the lesser curve. All lymph nodes in the area should be
included with the specimen. Identifi cation and preservation of the right gastric artery
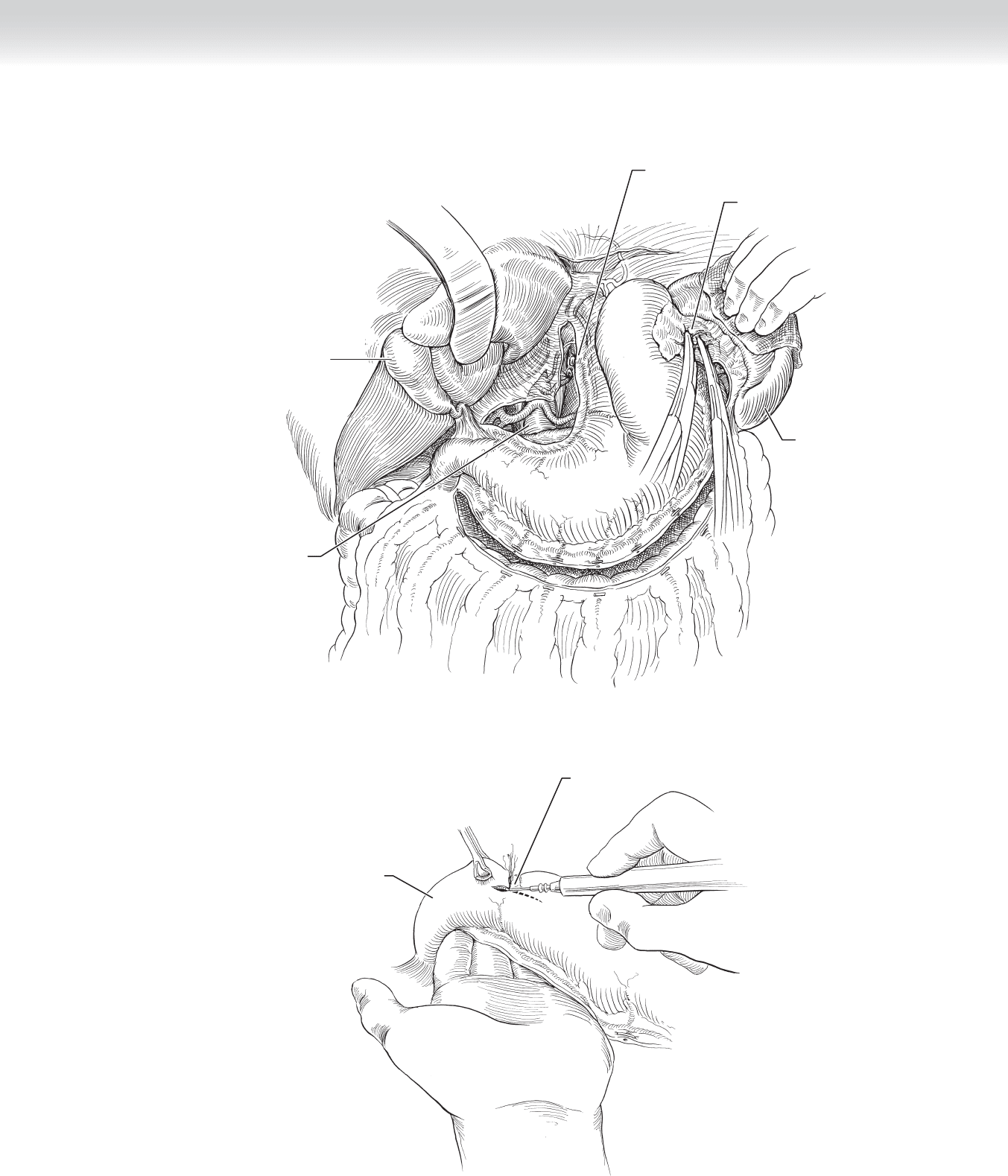
along this dissection plane is attempted (Figure 16-4).
◆ Next a pyloromyotomy is performed from 1 to 2 cm on the anterior gastric wall through
the pylorus extending approximately 0.5 to 1.0 cm onto the duodenum. We prefer to use a
fi ne-tipped hemostat and needle-tipped Bovie for careful dissection of the stomach and
duodenum muscular wall away from the underlying mucosa. The surgeon must ensure the
mucosa has not been violated. If the lumen of the bowel has been entered, the mucosal
defect is closed primarily and Heineke-Mikulicz pyloroplasty is performed (Figure 16-5).
◆ The hiatus is enlarged by small radial incisions of the crura to allow much of the esophageal
dissection under direct vision through the hiatal keyhole. To complete the abdominal por-
tion of the procedure, the Penrose drain is retracted downward, and the distal 10 to 15 cm
of esophagus is mobilized through the hiatus by blunt and sharp dissection. At this point
the surgeon must determine that the distal esophagus is free from adhesions or tumor or
both to proceed with the operation.
◆ To complete gastric mobilization, the remaining greater omentum is freed from the greater
curve again, preserving the right gastroepiploic artery, and a Kocher maneuver is performed
to ensure maximum gastric mobility.
CHAPTER 16 • Esophagectomy—Transhiatal 177
Pyloromyotomy
Duodenum
FIGURE 16 –5
Gallbladder
Stomach
Abdominal aorta
Left gastric artery
Spleen
Short gastric vessels
FIGURE 16 –4