Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

178 Section III • The Esophagus
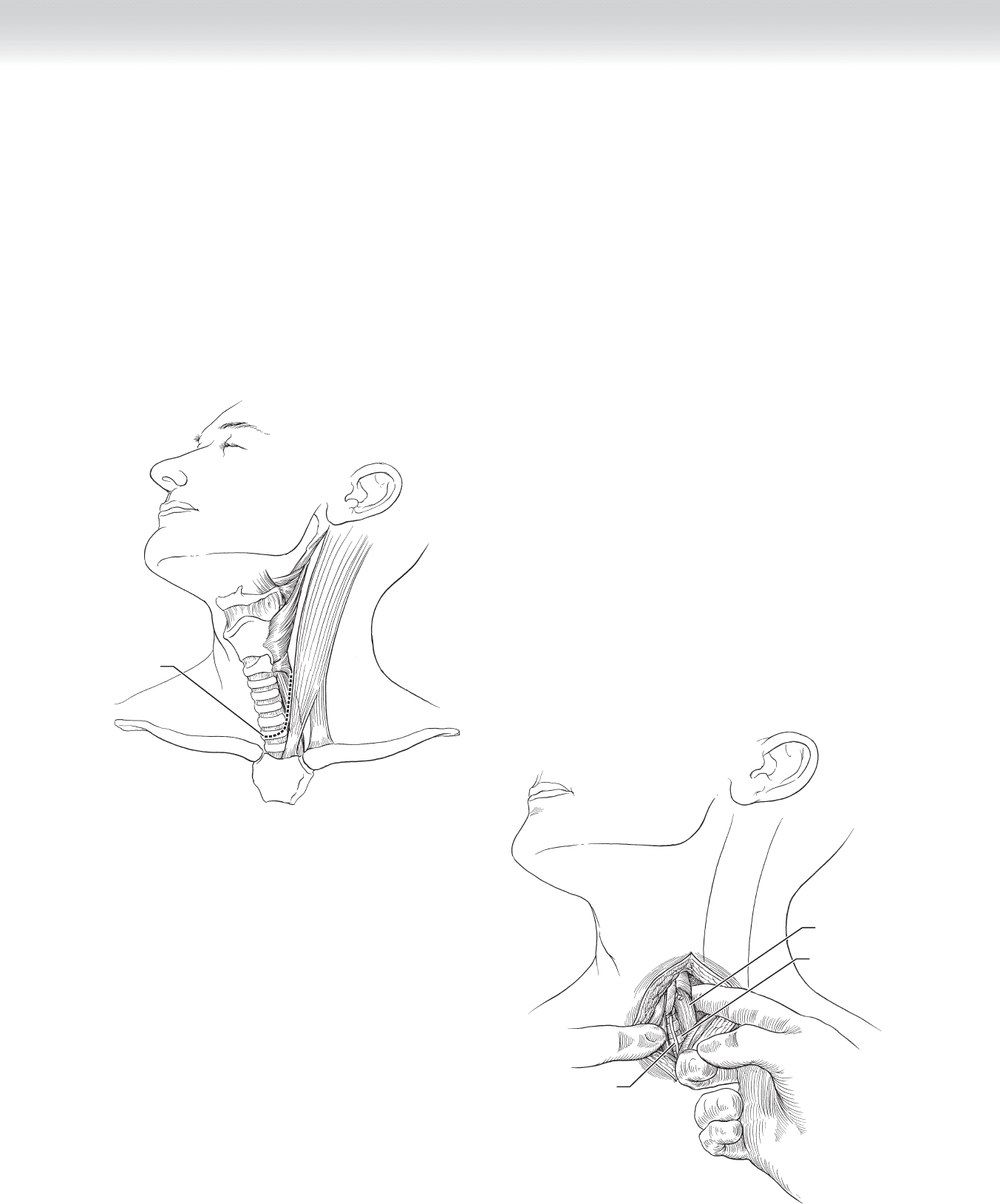
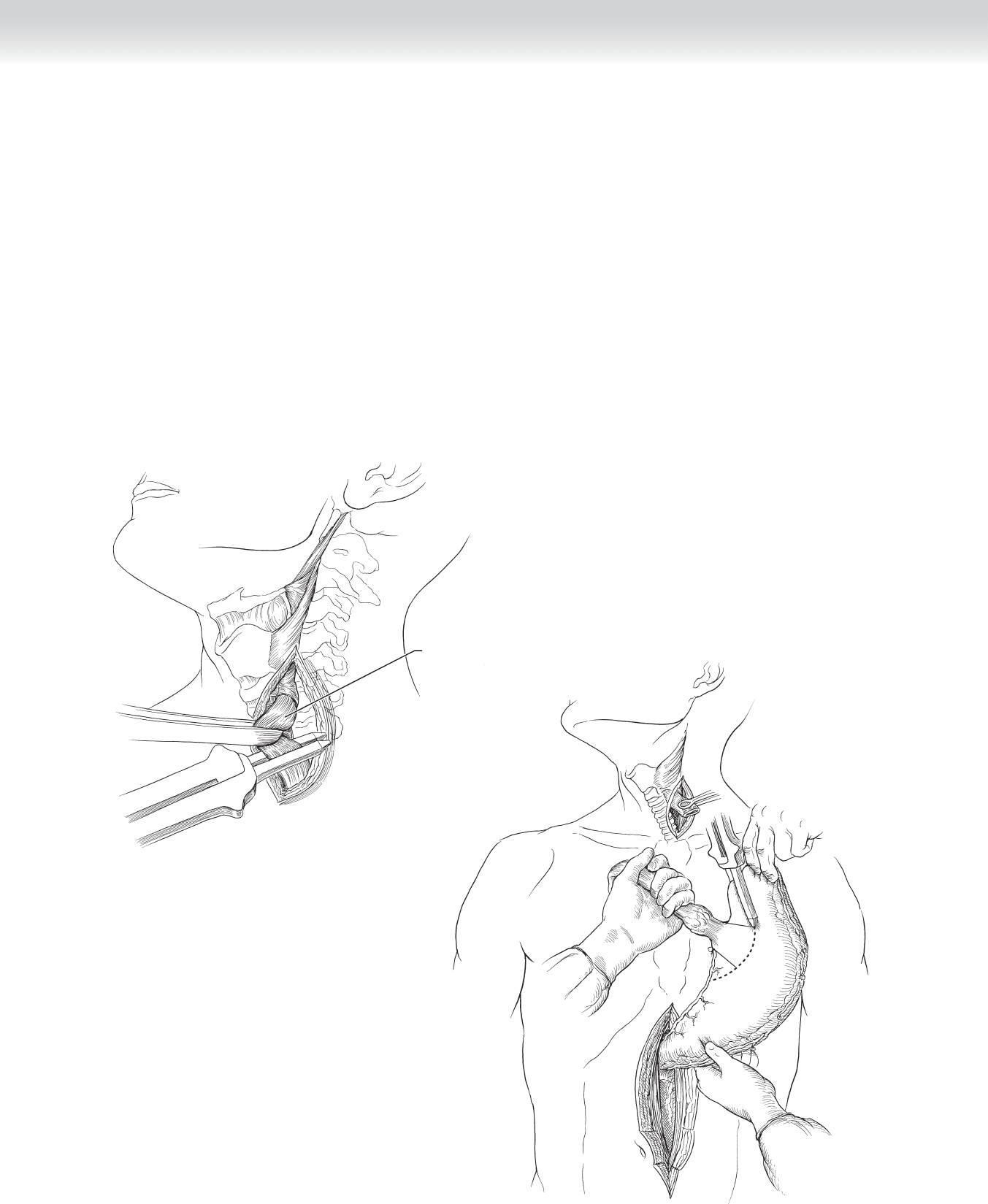
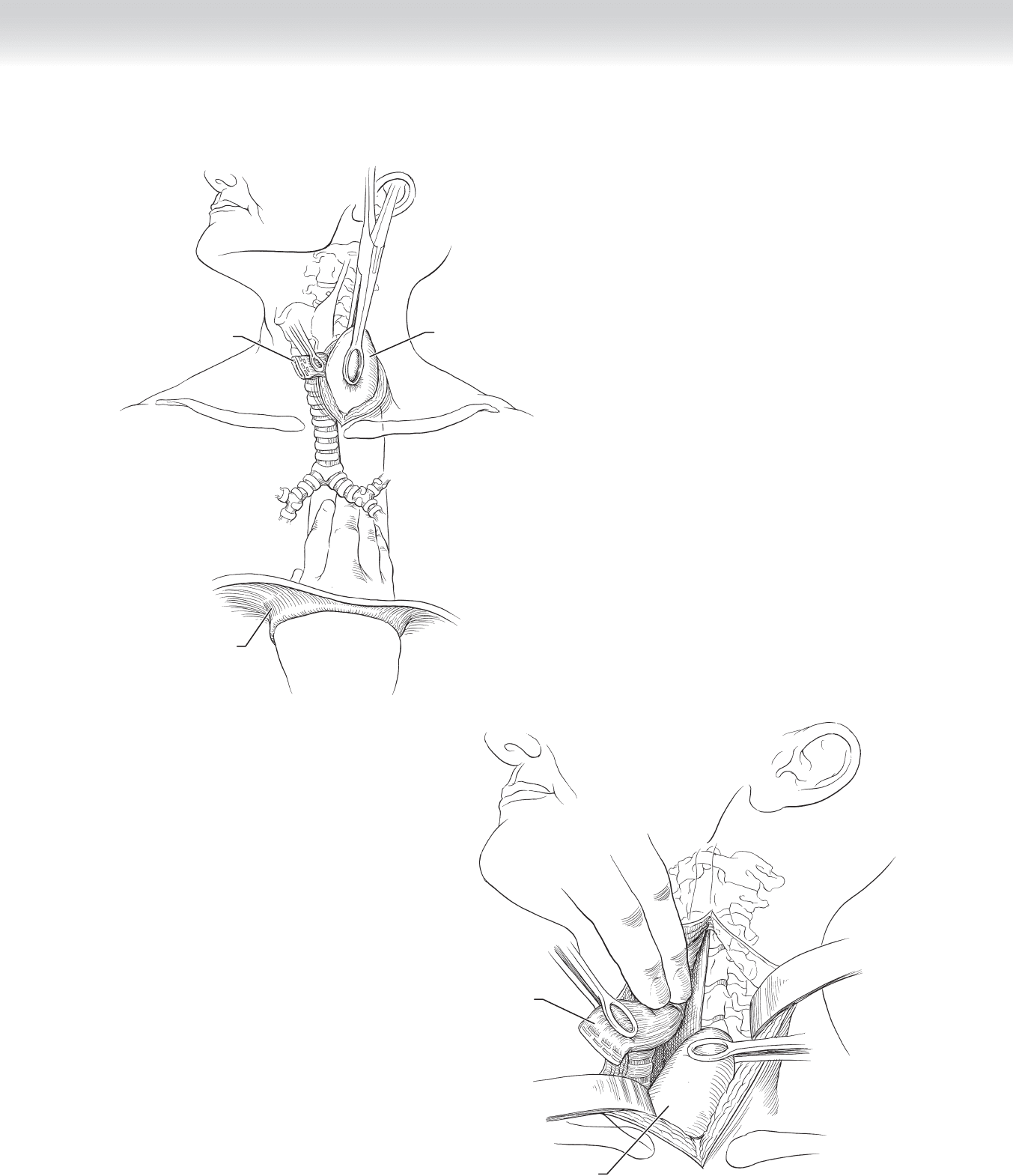
◆ The cervical dissection begins by placing an incision along the anterior border of the left
sternocleidomastoid muscle from the hyoid bone to 1 cm above the clavicle. The incision
is carried through the platysma to expose the deep cervical fascia (Figure 16-6).
◆ The sternocleidomastoid muscle and carotid sheath are retracted laterally while the thyroid
gland and trachea are retracted medially to expose the proximal esophagus. Occasionally the
middle thyroid vein and inferior thyroid artery need to be divided for adequate exposure.
Care should be taken to avoid excessive retraction or placing instruments in the tracheo-
esophageal groove, where the recurrent laryngeal nerve can be injured (Figure 16-7).
Incision
FIGURE 16 –6
Recurrent laryngeal nerve
Esophagus
Trachea
FIGURE 16 –7
CHAPTER 16 • Esophagectomy—Transhiatal 179
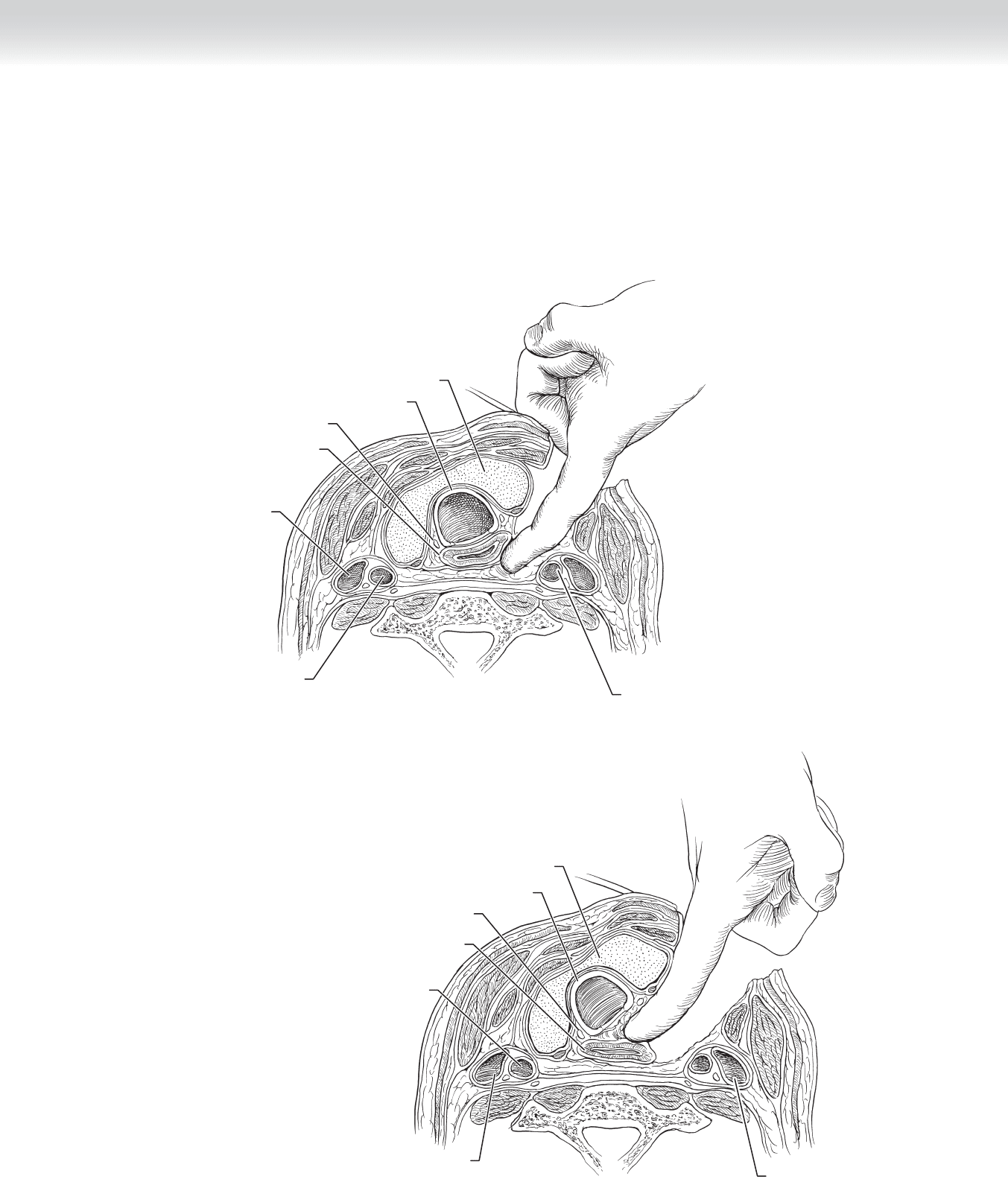
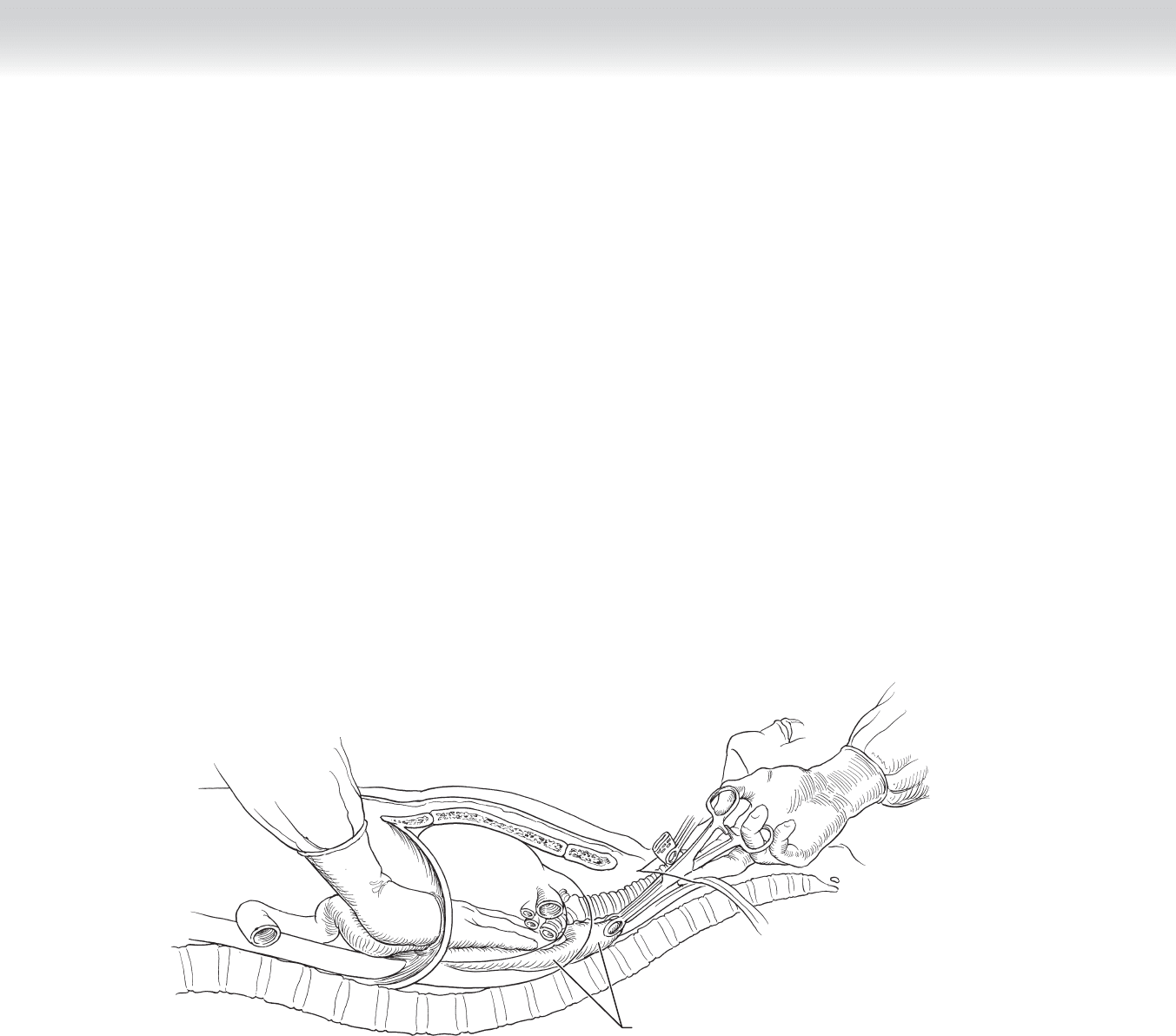
◆ The cervical esophagus is mobilized by blunt dissection, beginning in the prevertebral
space and working medially. The tracheoesophageal groove is opened with blunt dissec-
tion that is continued medially to connect with the prevertebral dissection (Figures 16-8
and 16-9).
Thyroid gland
Internal
jugular vein
Common carotid artery
Recurrent laryngeal nerve
Esophagus
Trachea
Common carotid artery
FIGURE 16 –8
Thyroid gland
Internal
jugular vein
Common carotid artery
Recurrent laryngeal nerve
Esophagus
Trachea
Common carotid artery
FIGURE 16 –9
180 Section III • The Esophagus
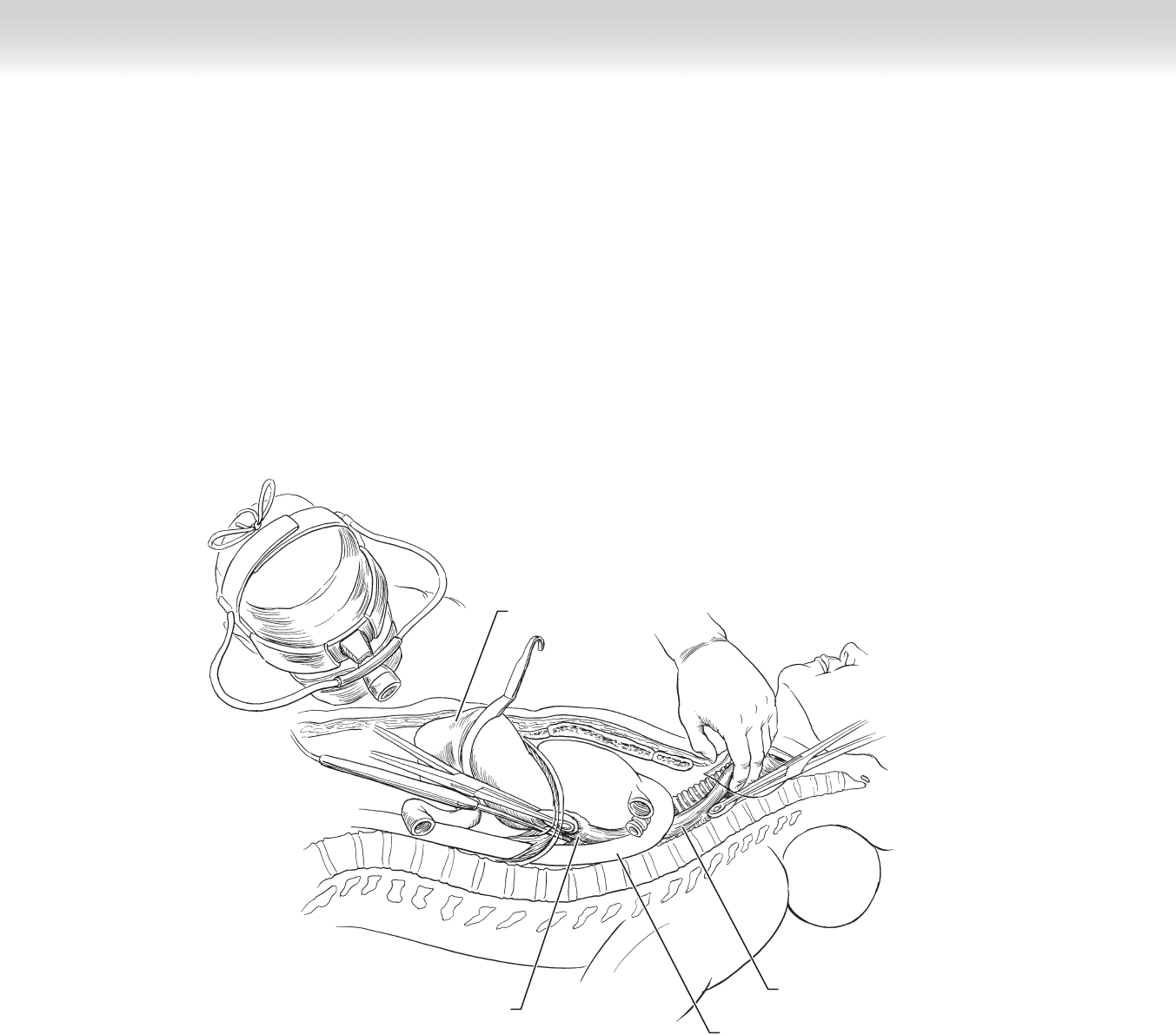
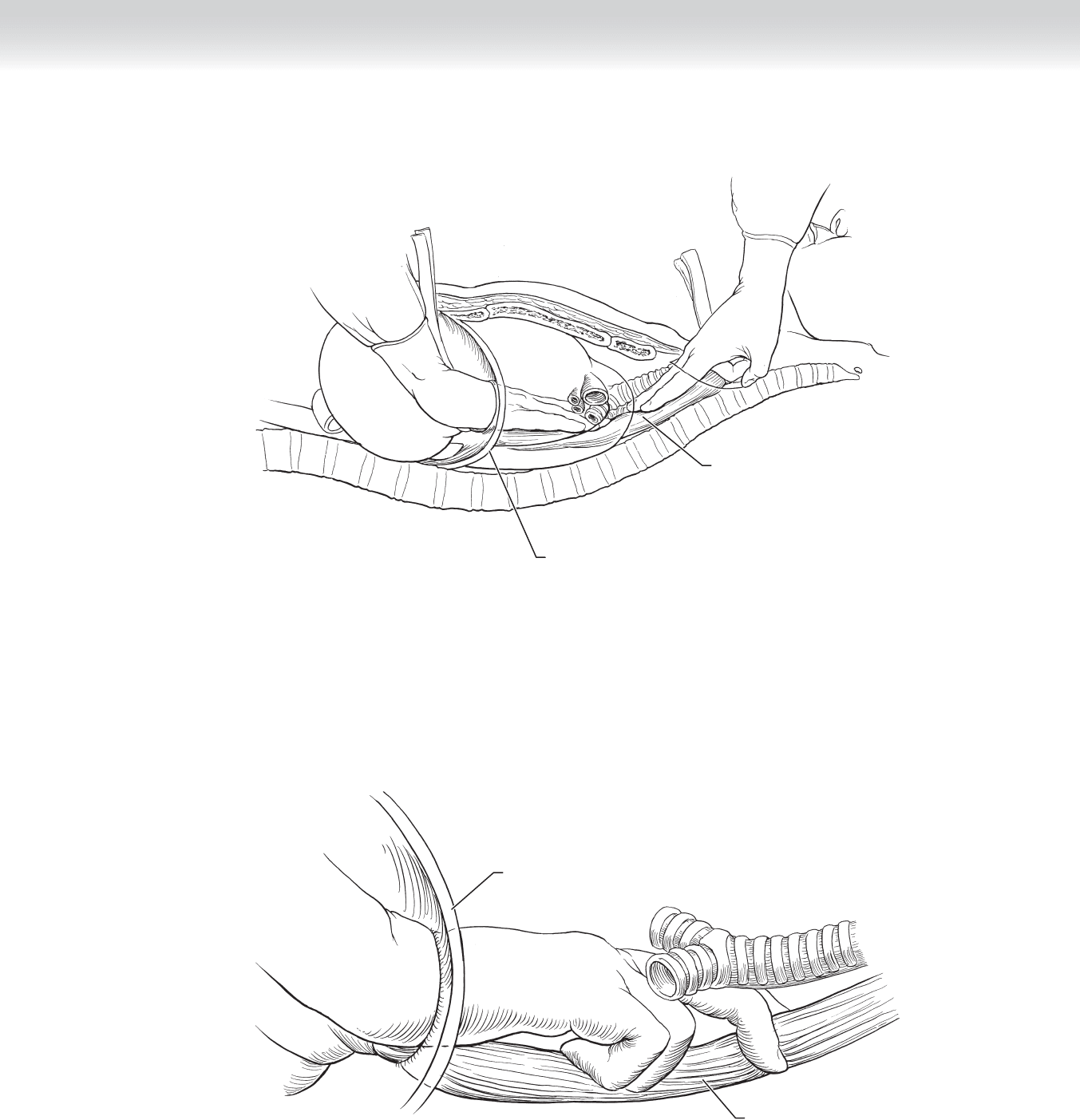
◆ Now that the proximal and distal esophagus is mobilized, the transhiatal dissection is
begun to fully mobilize the remaining esophagus is continued. Continuous traction is
placed on each of the Penrose drains encircling the ends of the esophagus while the sur-
geon bluntly develops the prevertebral plane with his or her right hand through the hiatus
and left hand through the cervical incision (Figure 16-10).
FIGURE 16 –10
Descending aorta
Esophagus
Tumor at distal end of esophagus
Stomach
Heart
FIGURE 16 –10
CHAPTER 16 • Esophagectomy—Transhiatal 181
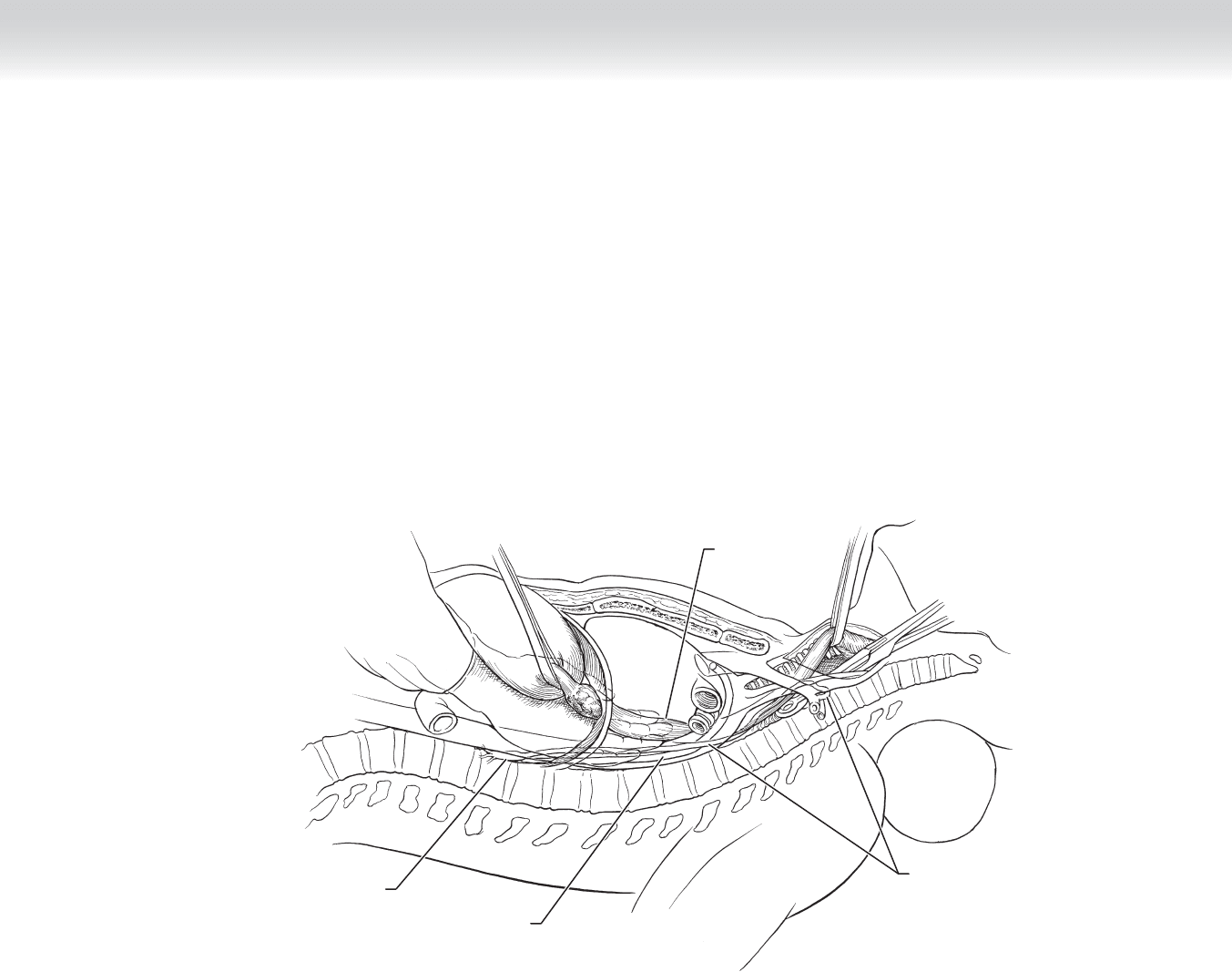
Esophagus
Thoracic duct
Azygos vein
Cisterna chyli
Heart
SVC
FIGURE 16 –11
◆ A Penrose drain is looped around the esophagus and retracted superiorly while blunt
dissection of the esophagus is continued to the level of the carina. Dissection can be
performed under direct vision through the enlarged hiatus, by blunt fi nger dissection, or
using a thoracoscope (Figure 16-11).

182 Section III • The Esophagus
◆ A sponge on a stick can help facilitate this dissection from the cervical incision. Once
the entire posterior esophagus is mobilized, the anterior section is mobilized in similar
fashion. During the anterior dissection, the surgeon must be careful not to injure the
membranous portion of the trachea. The lateral esophageal attachments can be freed
under direct vision from the hiatus with superior retraction of the chest wall. Lymph
nodes in the subcarinal area should be dissected free and removed with the specimen. If
the lateral attachments cannot be viewed, an alternative method is to insert the surgeon’s
right hand through the hiatus and pin the esophagus against the spine between the in-
dex and middle fi ngers. The lateral tissue is then stripped from the esophagus by blunt
dissection (Figures 16-12 to 16-14).
Diaphragm with
radial incisions for
enlargement
Esophagus
FIGURE 16 –12
CHAPTER 16 • Esophagectomy—Transhiatal 183
Diaphragm
Esophagus
Heart
FIGURE 16 –13
Diaphragm
Esophagus
FIGURE 16 –14
184 Section III • The Esophagus
◆ Once the esophagus is fully mobilized, the cervical esophagus is divided obliquely with a
gastrointestinal anastomosis (GIA) stapling device (Figure 16-15).
◆ The esophagus is pulled from the posterior mediastinum and delivered into the abdomen.
At this point the surgeon should inspect the surgical bed for bleeding and insert a gauze
pack into the posterior mediastinum to tamponade any minor oozing while the stomach is
prepared. The fundus and distal greater curve of the stomach are grasped and held on ten-
sion while the esophagus is pulled at a 90-degree angle. A GIA stapling device can be used
to resect a portion of the lesser curve and gastric cardia to gain a 4- to 6-cm margin from a
distal esophageal tumor. For benign disease, only the cardia is resected to maximize collat-
eral fl ow through the stomach. This process also “tubularizes” the stomach in preparation
for use as a conduit. The staple line can be oversewn with 3-0 silk interrupted Lembert
stitches (Figure 16-16).
FIGURE 16 –15
Esophagus
5 cm
5 cm
FIGURE 16 –16
CHAPTER 16 • Esophagectomy—Transhiatal 185
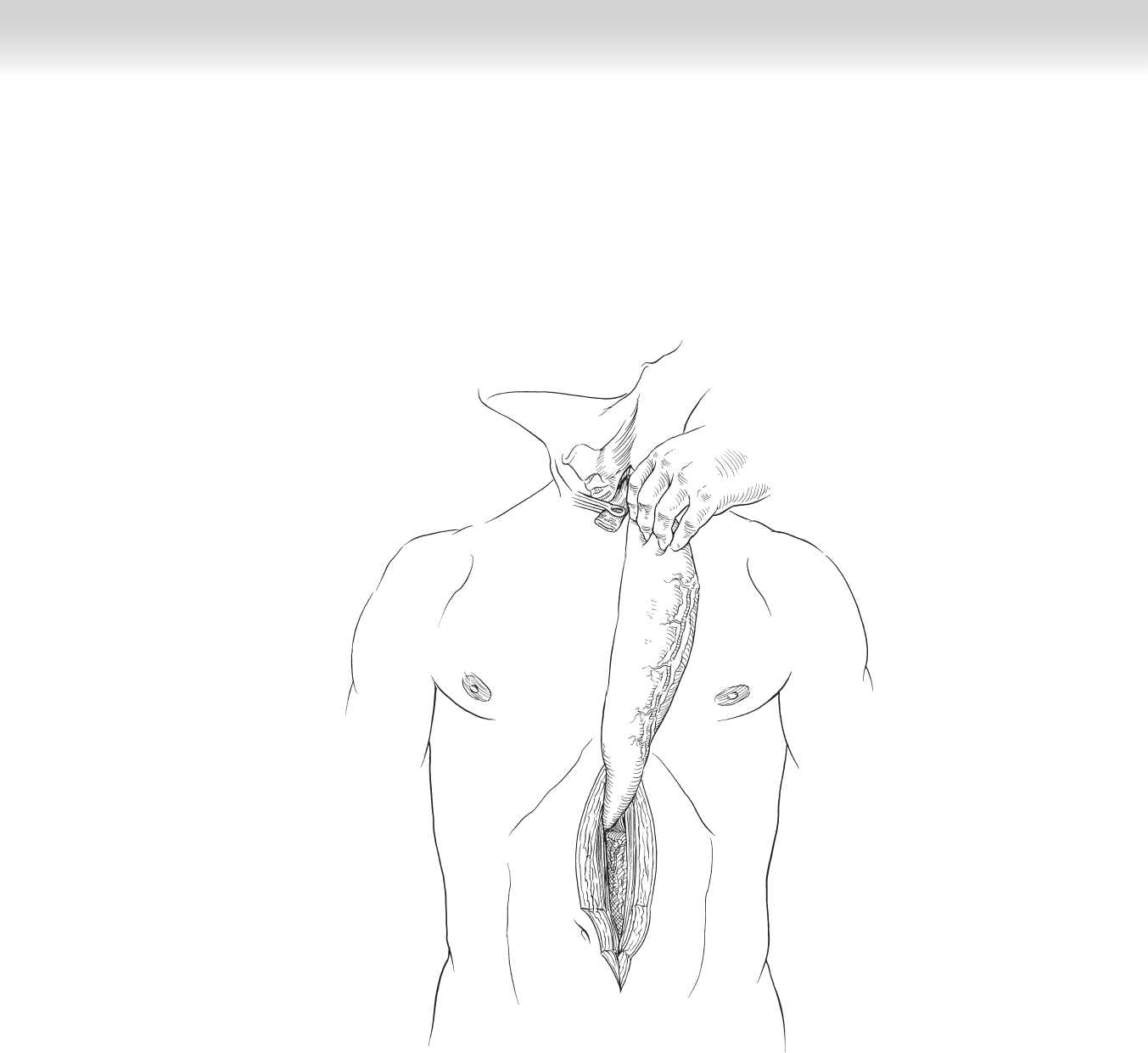
◆ The stomach is then manipulated through the enlarged hiatus to the cervical incision. A
Babcock clamp can be inserted from the cervical incision into the posterior mediastinum to
help grasp and deliver the fundus of the stomach into the neck (Figure 16-17).
FIGURE 16 –17
186 Section III • The Esophagus
◆ Alternatively, a Penrose drain can be sutured to the apex of the stomach and delivered into
the cervical incision to help provide traction. Both techniques use more pushing from the
diaphragm side rather than pulling from the neck side. The surgeon must be careful to
avoid twisting the stomach, which will compromise gastric blood fl ow and can lead to con-
duit necrosis with anastomotic breakdown (Figures 16-18 to 16-20).
◆ The abdominal portion of the procedure is completed before the cervical anastomosis is
performed. This allows time to assess the viability of the gastric conduit. In the abdomen,
the hiatus is closed by approximating the crura with 2-0 Vicryl fi gure-of-eight stitches to
easily allow 2 fi ngerbreadths between the stomach and hiatus. The stomach is also tacked
to the diaphragm with interrupted 3-0 silk stitches to prevent subsequent gastric herniation
into the chest. At this point a jejunostomy feeding tube can be placed according to surgeon
preference.
Stomach
Heart
FIGURE 16 –18
CHAPTER 16 • Esophagectomy—Transhiatal 187
Diaphragm
Stomach
Esophagus
FIGURE 16 –19
Stomach
Esophagus
FIGURE 16 –20