Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 12 • Excision of Benign Breast Lesion 147
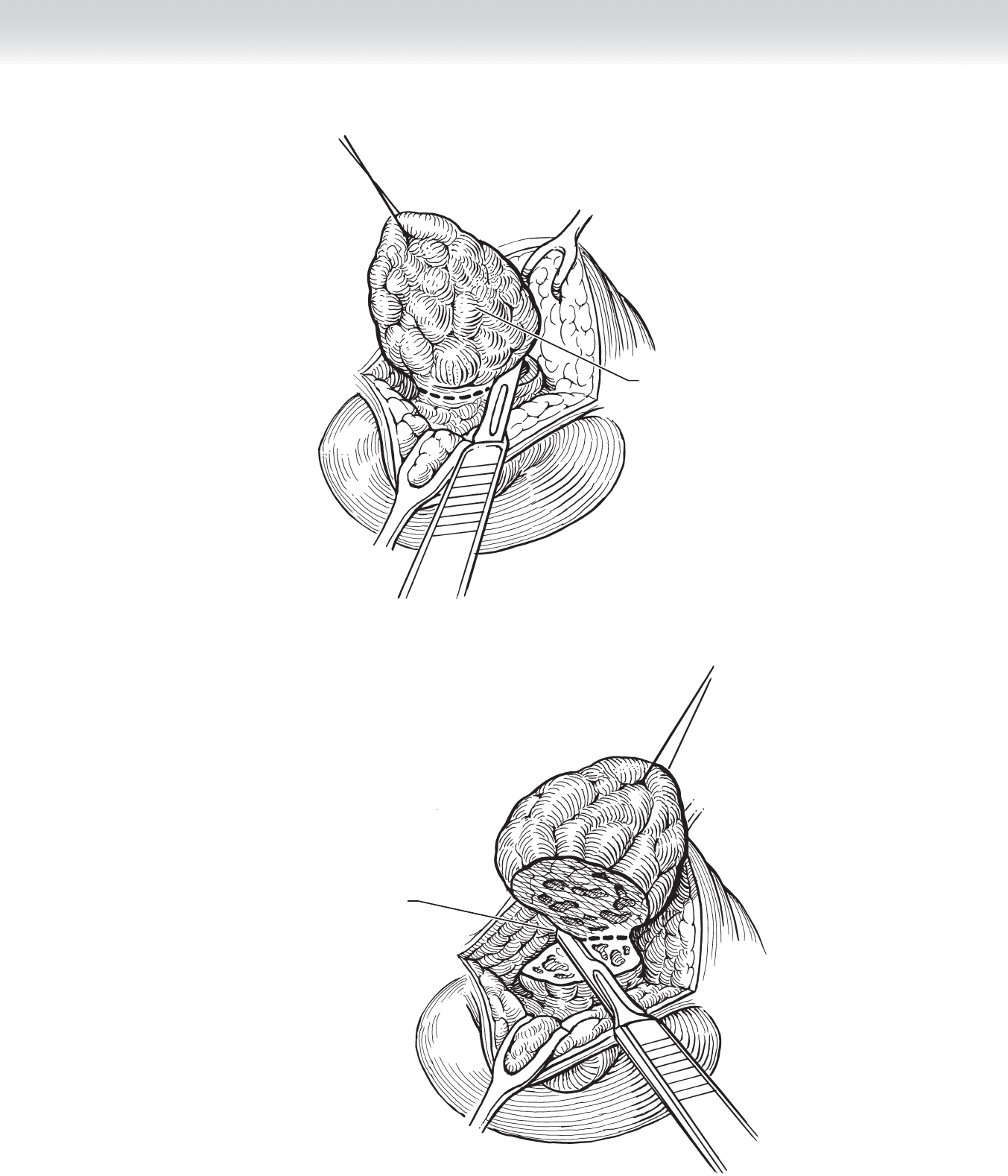
With traction,
begin excising tumor
FIGURE 12 –3
Excising remaining
portion of tumor
FIGURE 12 –4

148 Section II • The Breast
3. CLOSURE
◆ The breast tissue is not closed and the wound is closed with subcuticular absorbable
sutures (Figures 12-5 and 12-6).
◆ The wound is covered with a plastic dressing.
STEP 4: POSTOPERATIVE CARE
◆ I prefer nonopioid analgesics.
◆ An ice pack is used for the fi rst 12 to 24 hours.
◆ I recommend that the patient wear a new sports bra for support and wear it until the
discomfort has disappeared.
STEP 5: PEARLS AND PITFALLS
◆ Avoid local anesthetic in dense breasts.
◆ Avoid epinephrine if local anesthetic is to be used.
◆ Traction sutures prevent destruction of the specimen to be excised by multiple applications
of forceps or clamps. I use coagulating cautery for dissection and therefore take a more
generous margin because there may be coagulation artifact produced in the specimen.
CHAPTER 12 • Excision of Benign Breast Lesion 149
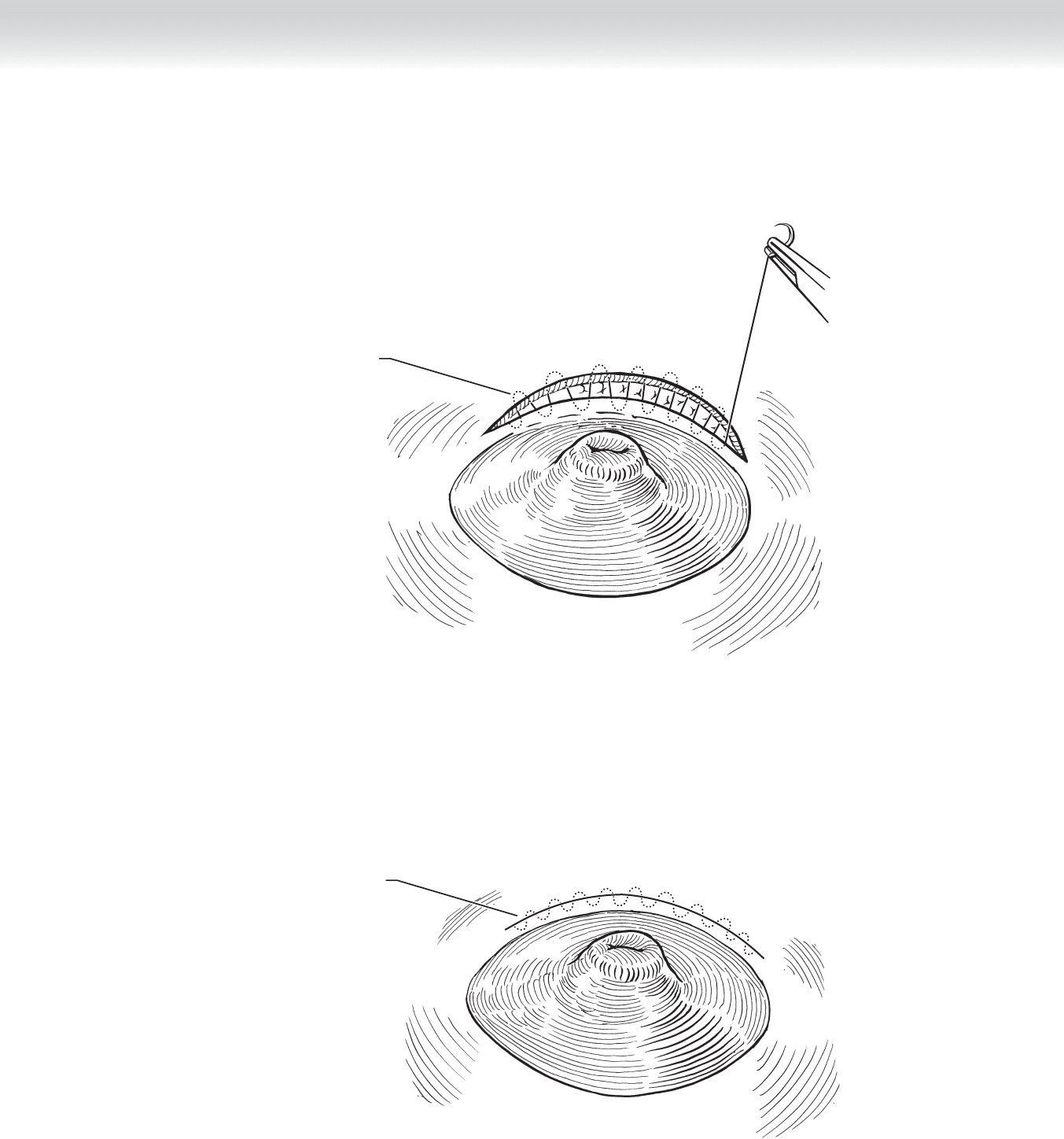
Incision site
being sutured
FIGURE 12 –5
Incision closed
with subcuticular
running suture
FIGURE 12 –6

150
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the location of the mammary gland in relation to the
chest wall musculature, the fascial boundaries, the lymphatic drainage pathways, the vascu-
lar supply to the breast and the associated supporting structures, and the innervation of the
breast and surrounding tissues is essential for appropriate surgical management.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Bilateral nipple discharge, which is usually seen in postmenopausal patients, is sometimes
suffi ciently voluminous to cause problems with soiling.
◆ Bilateral nipple discharge is rarely due to neoplastic lesions and almost always due to duct ecta-
sia. As noted, the lobes of the breast are drained by ducts that coalesce in the subareolar area
into 5 to 10 lactiferous ducts, each of which opens independently in the nipple.
◆ Diagnosis of duct ectasia is made when single-digit compression is carried out and discharge
from multiple ducts in the nipple is noted, usually bilaterally.
◆ Preoperative mammography is required for all patients.
◆ General anesthesia is used.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ When resection is required, it is performed through an areolar margin incision. The areola
is elevated from the intramammary fat and all of the ducts together can be identifi ed and
dissected free from the undersurface of the nipple (Figures 13-1 and 13-2).
CHAPTER
13
Major Duct Excision
Courtney M. Townsend, Jr.
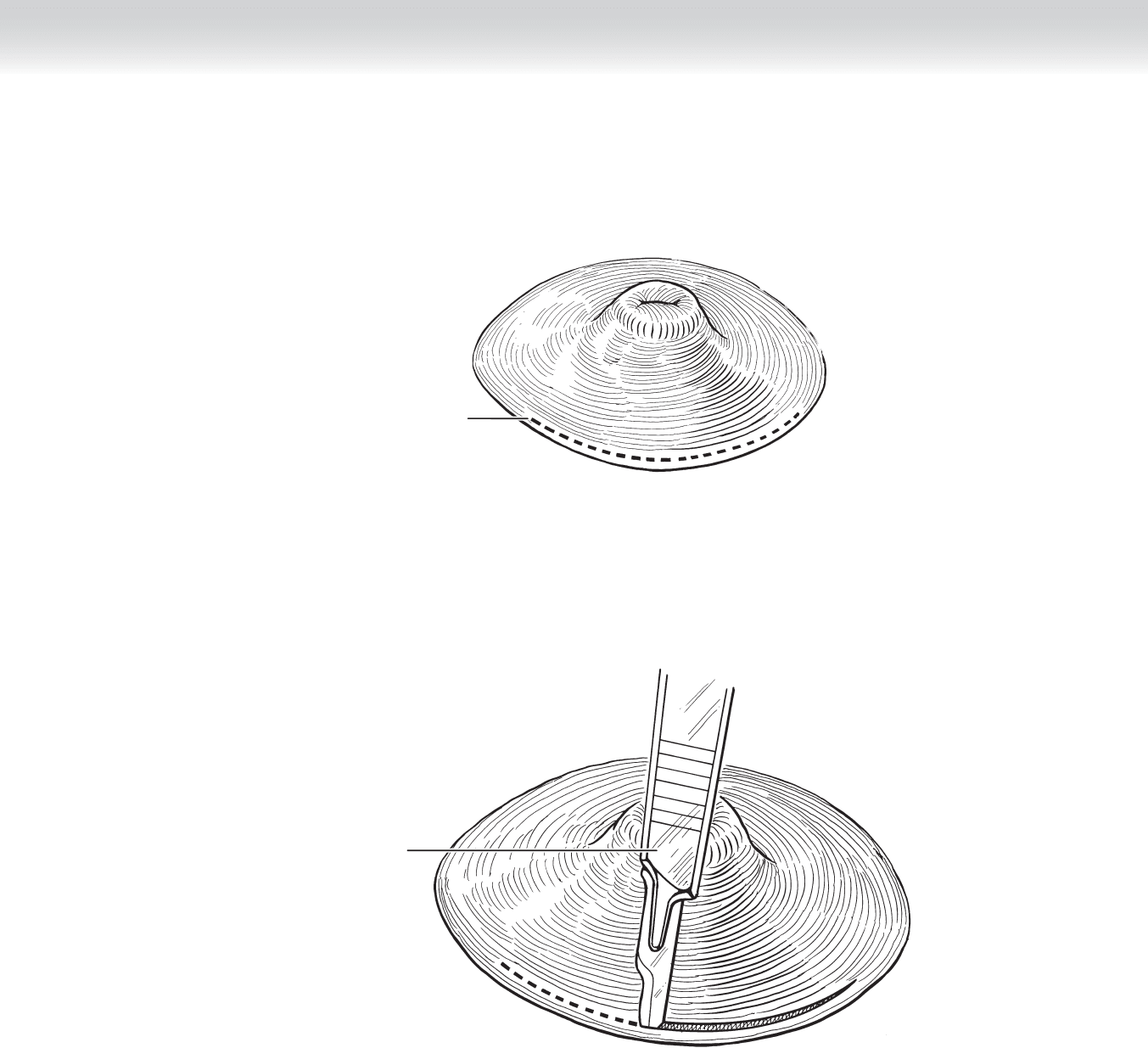
CHAPTER 13 • Major Duct Excision 151
Incision line
FIGURE 13 –1
Incising through
lower portion of
areola
FIGURE 13 –2

152 Section II • The Breast
2. DISSECTION
◆ The ducts are ligated and divided, as a group, in the subareolar area, and an inverted
cone excision removing the lactiferous ducts is carried out in a circumferential fashion
(Figures 13-3 and 13-4).
◆ Dissection and hemostasis are carried out with cautery.
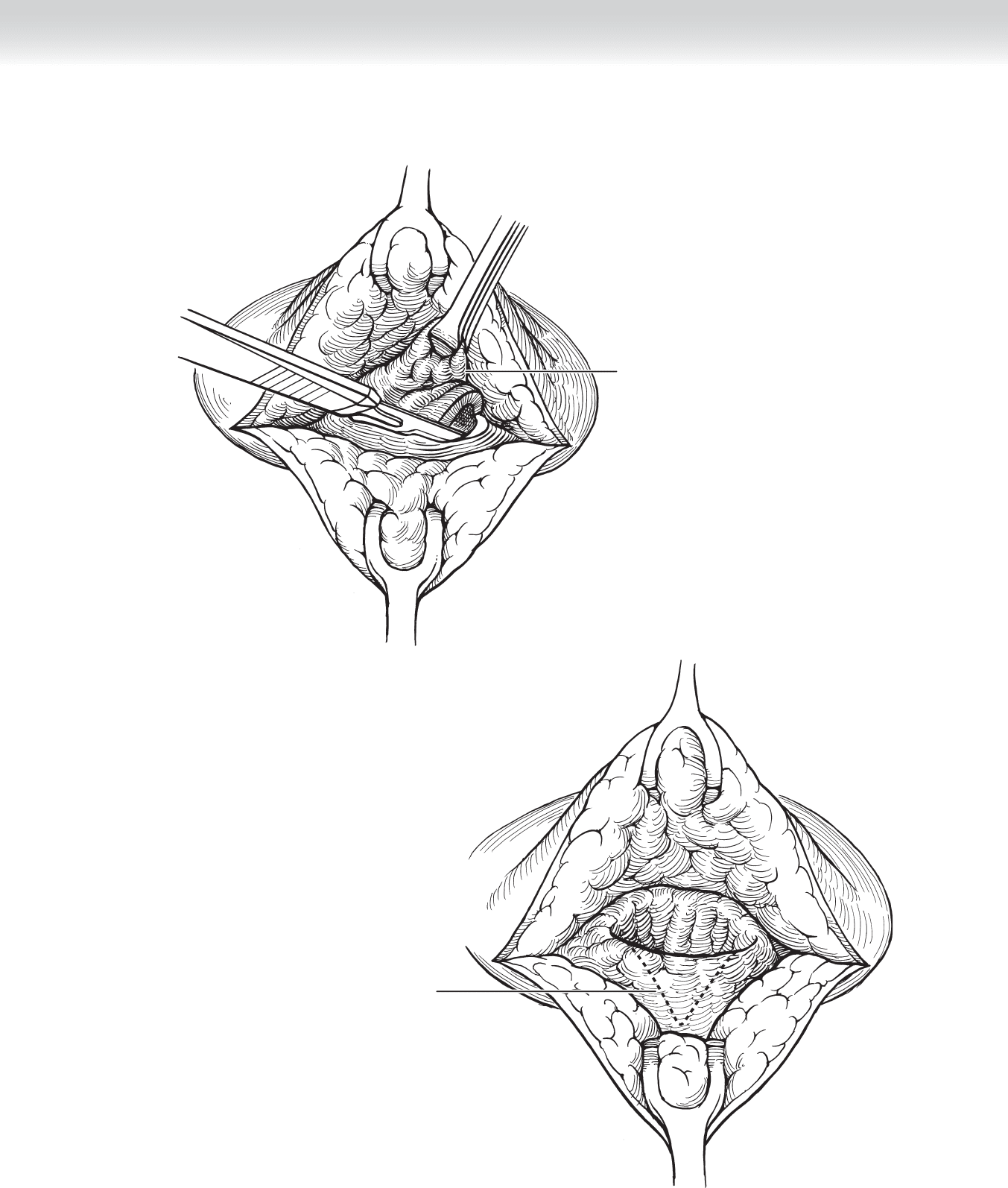
CHAPTER 13 • Major Duct Excision 153
Removing abnormal
ductal tissue
FIGURE 13 –3
Conical space
FIGURE 13 –4
154 Section II • The Breast
3. CLOSURE
◆ The breast tissue is not closed.
◆ The wound is irrigated with hydrogen peroxide and, after hemostasis is secured, the wound
is closed with running subcuticular absorbable sutures (Figure 13-5).
STEP 4: POSTOPERATIVE CARE
◆ I recommend that all patients who are going to have partial mastectomy for benign or
malignant conditions wear a new sport or jogging bra after the procedure, because it gives
good nonrigid support to the breast.
◆ An ice pack is often helpful to relieve localized pain, and one or two doses of nonopioid anal-
gesic is usually all that is required. The dressing can be removed in the bath 24 to 36 hours
after the operation and no further dressing needs to be used.
STEP 5: PEARLS AND PITFALLS
◆ I do not close the breast tissue because of the distortion that would occur.
◆ The extent of breast tissue excised is different from when resecting an area of pathologic
nipple discharge. This is a method to ablate the ducts; therefore, less extensive breast tissue
resection is required.
Incision closed with
subcuticular running suture
FIGURE 13 –5
155
STEP 1: SURGICAL ANATOMY
◆ The ducts draining the 15 to 20 lobes of the breast tissue coalesce into 5 to 10 lactiferous
ducts, each of which opens separately in the nipple.
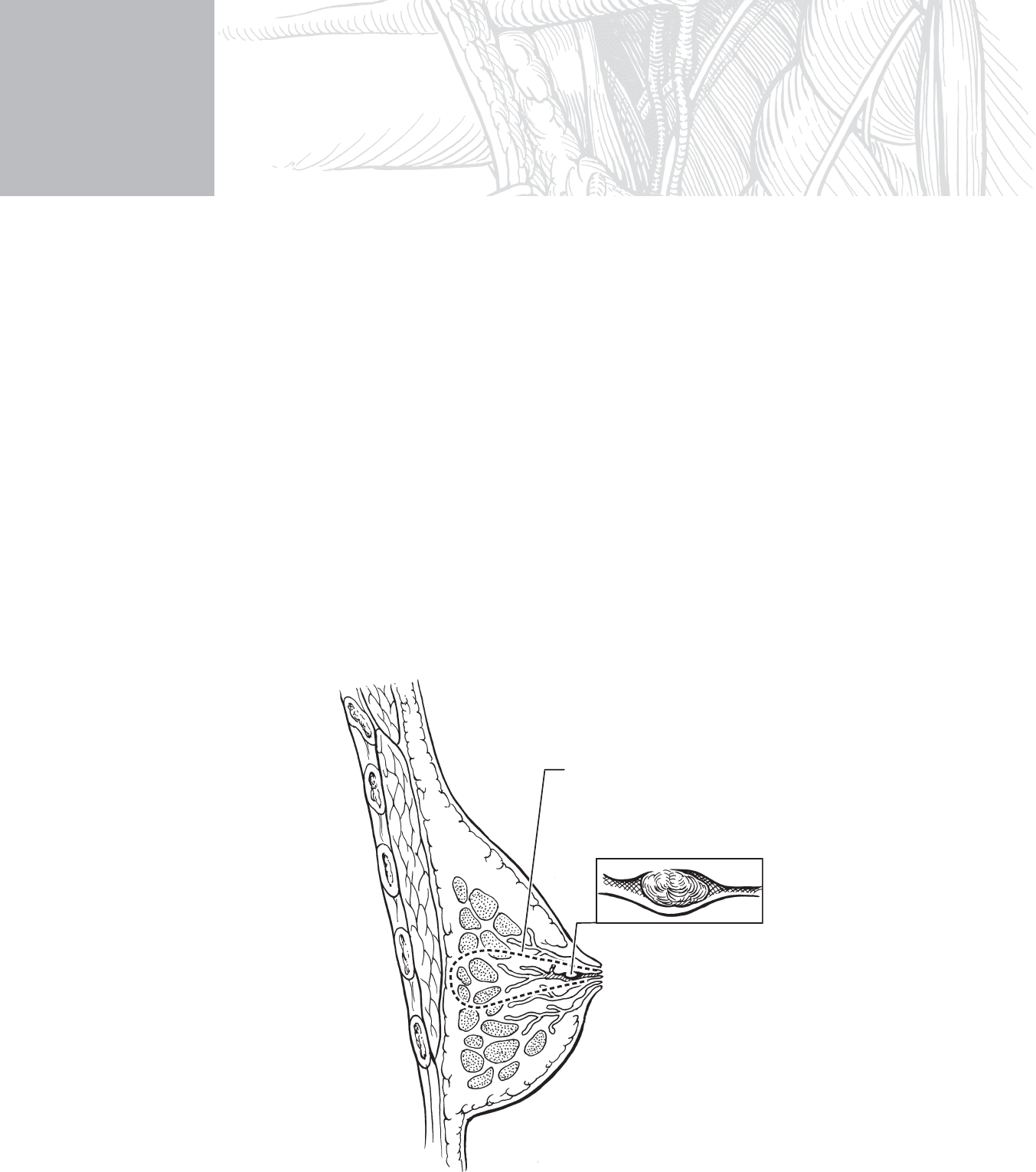
◆ Understanding that the subareolar ducts represent components from multiple glands, exci-
sion extends from the immediate area under the nipple in which the involved duct is iden-
tifi ed to encompass the tissue drained. It is excised en bloc so that the specimen is much
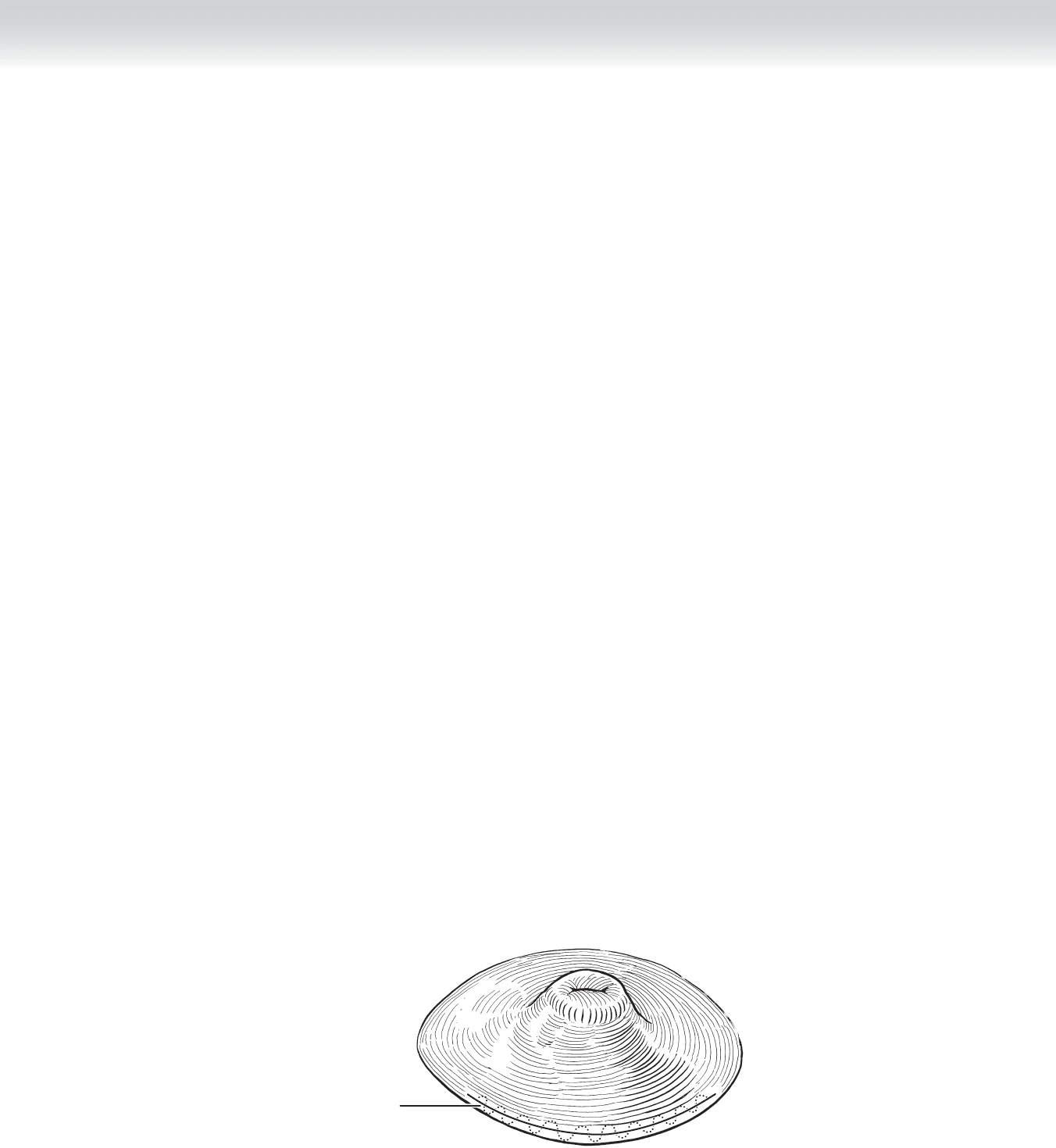
larger than simply a duct as shown in Figure 14-1.
CHAPTER
14
Intraductal Papilloma
Courtney M. Townsend, Jr.
Ductal tissue to be excised
Intraductal papilloma
FIGURE 14 –1

156 Section II • The Breast
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Pathologic nipple discharge is spontaneous, persistent, nonlactational, and unilateral. A
single-duct opening in the nipple can be identifi ed as the source of the discharge.
◆ The color and consistency of the discharge play no role in determination for resection once
the criteria for pathologic nipple discharge are met.
◆ Everyone with a breast complaint, including nipple discharge, should have a bilateral
mammogram. The object of the mammogram is not to determine whether operation for
pathologic nipple discharge will be performed but to search for occult cancer in both
breasts.
◆ Ductography is not required to identify the segment of breast to be resected.
◆ Cytologic examination of nipple discharge is not required.
◆ Pathologic nipple discharge requires resection and pathologic examination of the tissue. The
danger is that intraductal papillary cancer could be overlooked.
STEP 3: OPERATIVE STEPS
◆ I prefer that the patient has general anesthesia, although local anesthesia may be used.
1. INCISION
◆ The area of breast in which the lesion is located can be identifi ed by single-digit compres-
sion from periphery toward the areola (Figure 14-2).
2. DISSECTION
◆ The duct opening through which discharge fl ows can be identifi ed; that identifi es the area
for the excision. An areolar margin incision is used, and the areola is elevated from underly-
ing intramammary fat. The involved duct can usually be identifi ed as distended and often
containing a dark substance visible through the wall of the duct (Figure 14-3).