Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


117
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the location of the mammary gland in relation to the
chest wall musculature, the fascial boundaries, the lymphatic drainage pathways, the vascu-
lar supply to the breast and the associated supporting structures, and the innervation of the
breast and surrounding tissues is essential for appropriate surgical management.
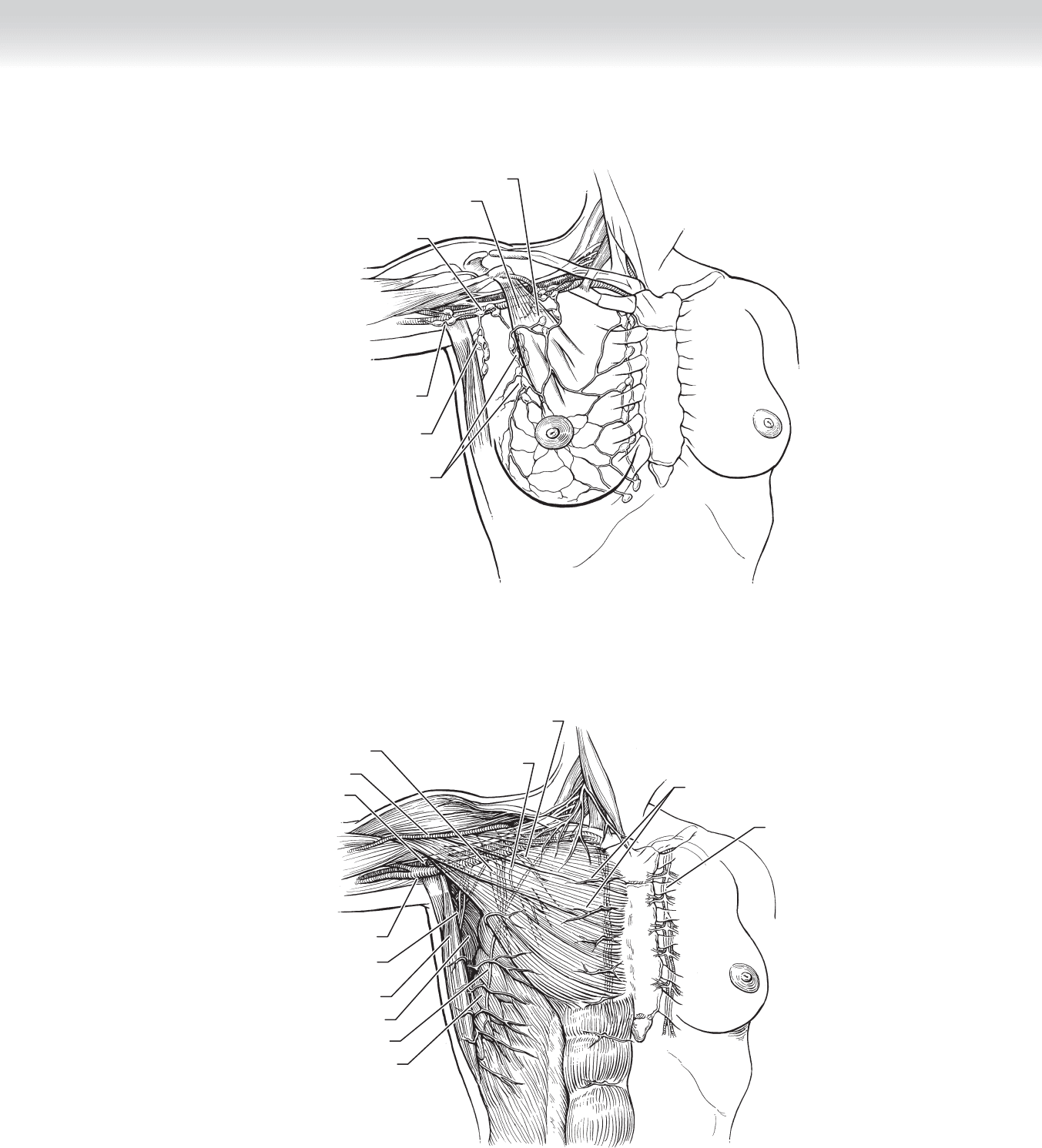
◆ Figure 10-1 demonstrates the breast gland and the rich intraparenchymal lymph channels
coursing toward the deeper major nodal reservoirs.
◆ Figure 10-2 illustrates the relationship of the nodal basins to the chest wall musculature.
The lymph nodes lateral to the pectoralis minor constitute level I nodes, those immediately
beneath the pectoralis minor level II nodes, and those medial to it level III. The interpectoral
nodes (Rotter’s nodes) are located between the pectoralis major and minor muscles and are
part of level III nodes. Internal mammary nodes are located medially along internal mam-
mary vessels beneath the sternum. Unnamed intramammary lymph nodes can be present in
all quadrants of the breast.
DEFINITION
◆ Modifi ed radical mastectomy constitutes the removal of the breast parenchyma, the nipple-
areolar complex, and levels I and II axillary lymph nodes.
◆ Other types of mastectomy procedures include the following:
◆ Total mastectomy (removal of the breast only) may be combined with sentinel node
biopsy.
◆ Patey’s modifi ed radical mastectomy includes dissection of level III nodes reached by
division or resection of the pectoralis minor muscle.
◆ Radical mastectomy further removes the pectoralis major and minor muscles.
◆ Extended radical mastectomy also eradicates the internal mammary lymph nodes.
◆ Nipple-sparing mastectomy preserves the nipple and areola.
◆ Areola-sparing mastectomy preserves the areola, usually with resection of the nipple.
CHAPTER
10
Modifi ed Radical Mastectomy
Baiba J. Grube

118 Section II • The Breast
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Selection of a surgical option for local control of breast cancer is a complex decision that is
based on tumor features, body habitus, and individual patient choice. Interdisciplinary
discussion with radiation oncologists, medical oncologists, and plastic surgeons in addition
to the oncologic surgeon provides a comprehensive understanding of the options available
to the patient.
◆ Modifi ed radical mastectomy may be an option for a diagnosis of the following:
◆ Invasive breast cancer
◆ Multicentric invasive breast cancer
◆ Invasive breast cancer after previous chest irradiation
◆ Invasive breast cancer when postoperative radiotherapy maybe contraindicated (e.g., con-
nective tissue disease, presence of a pacemaker)
◆ Invasive breast cancer in a pregnant patient
◆ Palliative resection in stage IV breast cancer for local control
◆ Lumpectomy with axillary lymph node dissection may be an alternative procedure to modi-
fi ed radical mastectomy for many women, especially in the current era of mammographic
screening and identifi cation of early stage disease, or with the use of induction chemotherapy
to reduce the size of a larger primary tumor.
◆ Discussion of the planned procedure with the anesthesiologist is critical.
◆ Long-acting paralytic agents should be avoided when an axillary dissection is planned so
that intact motor nerve function can be detected.
◆ Inhalation agents may be varied if immediate reconstruction is planned with autologous
tissue.
CHAPTER 10 • Modifi ed Radical Mastectomy 119
Interpectoral nodes
Pectoralis minor muscle
Central axillary
nodes
Subscapular axillary
pectoral nodes
Anterior axillary
pectoral nodes
Brachial axillary
nodes
FIGURE 10 –1
Serratus anterior muscle
Long thoracic nerve
Subscapular muscle
Latissimus dorsi muscle
Thoracodorsal
artery, nerve, and vein
Axillary vein
Axillary artery
Cephalic vein
Medial anterior
thoracic nerve
Medial anterior
thoracic nerve
Lateral anterior thoracic nerve
Perforating
intercostal nerves
Internal thoracic
artery and vein
FIGURE 10 –2

120 Section II • The Breast
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The patient is placed supine, close to the edge of the operating table with the arm extended
on a padded arm board, with or without a wedge. The arm may be prepped separately and
covered in a sterile stockinette to allow free rotation of the arm medially, to relax the
pectoralis major and minor muscles, and to permit better exposure of the axilla.
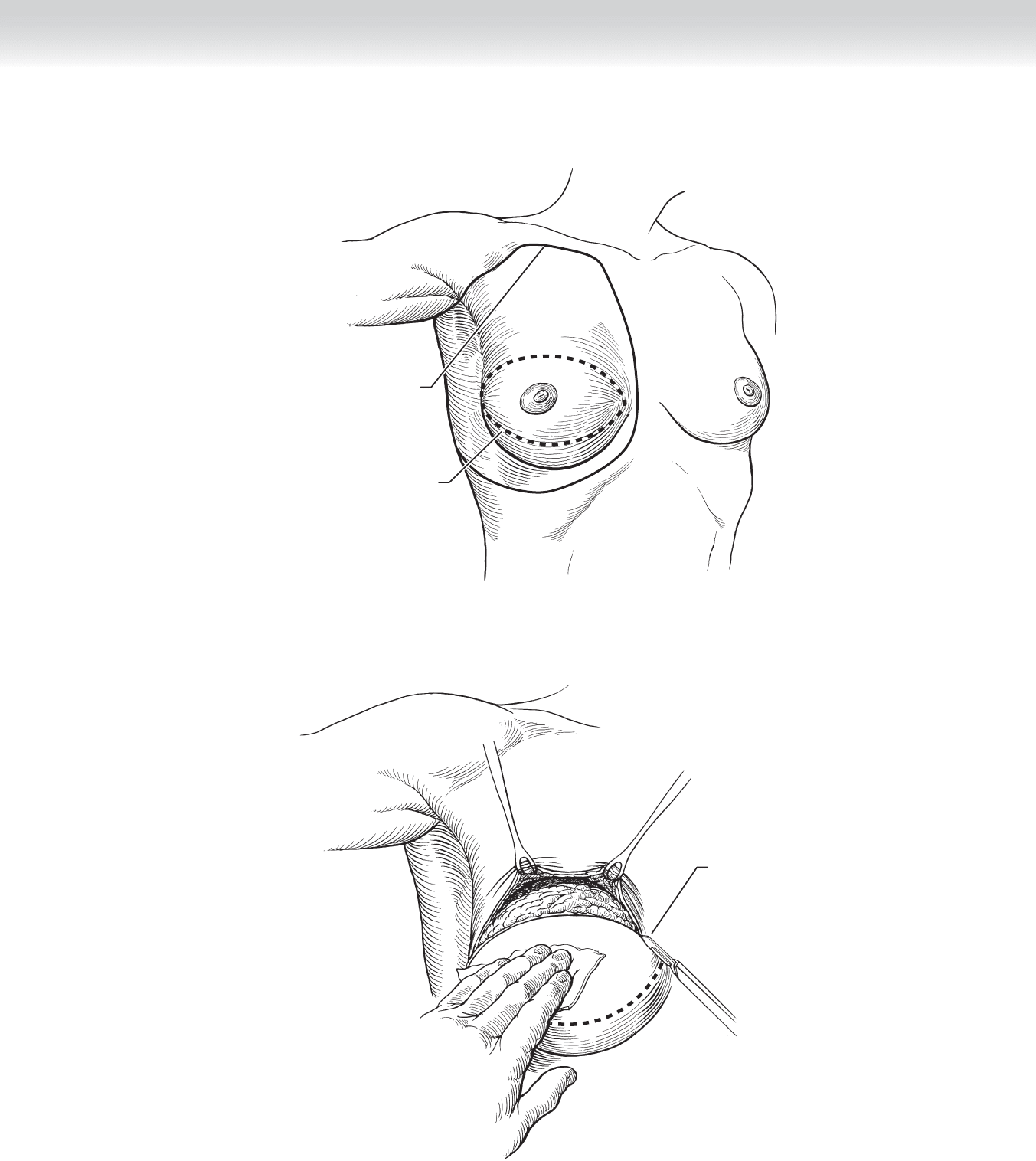
◆ The type of incision depends on whether immediate reconstruction is planned or a delayed
procedure is anticipated. If no reconstruction or a delayed procedure is planned, an
elliptical incision is made to include a previous surgical biopsy site if present (Figure 10-3).
The incision is usually placed horizontally to include the nipple-areolar complex, but in
some cases may be oriented at different angles to include a previous surgical biopsy site. If
delayed reconstruction is anticipated, the medial extent of the incision may be angled
slightly caudad to permit suffi cient skin for reconstruction of the medial cleavage and to
avoid a scar that may be visible with low décolletage. The width of skin resection should
permit a tension-free closure but avoid redundant skin folds. A good way to judge the
amount of skin to be resected is to draw a transverse or angled line through the nipple and
move the inferior fl ap upward with gentle tension and draw a mark on the skin where it
intersects the transverse line. A similar action should be performed for the superior fl ap.
◆ If immediate reconstruction is planned, discussion with the plastic surgeon for placement of
incisions is important. The most natural appearance to the native breast is a skin-sparing
mastectomy that is accomplished by resecting the nipple-areolar complex and leaving most
of the skin envelope behind. If the nipple areolar-complex is small relative to the breast, a
transverse incision can be extended laterally, resembling a tennis racquet, for a short
distance suffi cient to reach the axillary nodes.
◆ A marking pen is used to draw the planned incision. The skin is incised with a no. 15 scalpel
and extended through the dermis into the subcutaneous adipose tissue to expose the superfi -
cial investing fascia of the breast (Figure 10-4). The thickness of the fl aps will vary according
to body mass index. In very lean individuals this can be just millimeters thick and may
require subcutaneous infusion of tumescence solution for easier dissection. The breast paren-
chyma lies closest to the skin at the nipple-areolar complex and increases in thickness toward
the periphery of the breast.
CHAPTER 10 • Modifi ed Radical Mastectomy 121
Incision line for
modified radical
mastectomy
Undermined area
FIGURE 10 –3
Initial incision
being carried out
FIGURE 10 –4

122 Section II • The Breast
2. DISSECTION
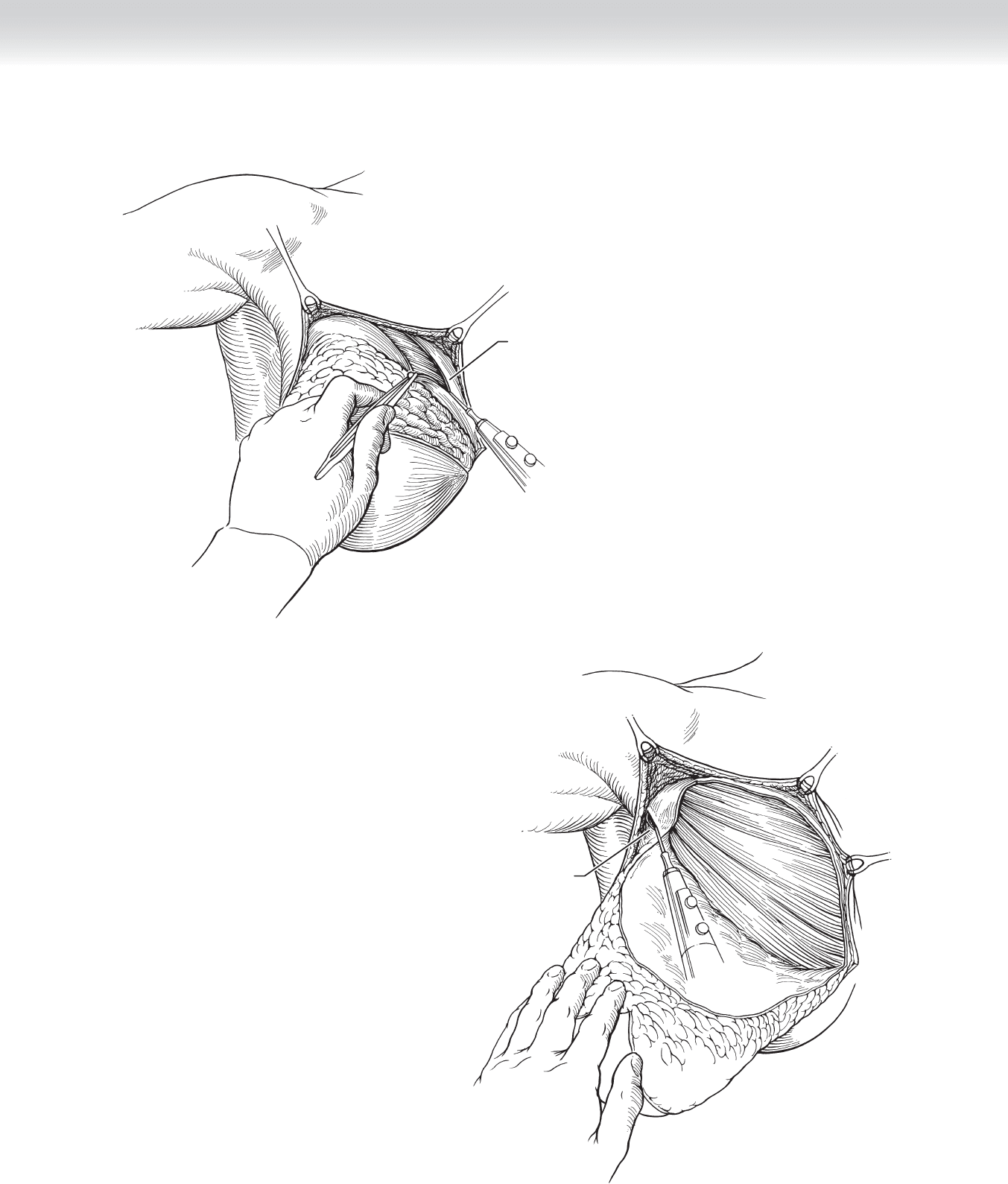
◆ Dissection is initiated by elevating the skin edges with skin hooks or Freeman rake retrac-
tors and may be performed with electrocautery as illustrated or by sharp dissection with a
no. 10 scalpel or curved Gorney scissors (Figure 10-5). If sharp dissection is undertaken,
subcutaneous injection of a dilute saline solution with epinephrine may reduce bleeding.
◆ As the fl aps are elevated, the assistant holds upward tension on the skin fl aps while the sur-
geon uses countertraction on the breast parenchyma. These counter forces help expose the
fi ne avascular areolar fascial plane separating the subcutaneous fat from breast parenchyma.
Excessive bleeding indicates that the dissection is not in the correct anatomic plane that
separates the glandular tissue from the subcutaneous adipose tissue.
◆ Dissection is continued circumferentially following the superfi cial fascia to its fusion with
the muscular fascia around the anatomic borders of the breast. These are defi ned by the
pectoralis major muscle below the clavicle superiorly, the margin of the sternum medially,
the inframammary fold overlying the rectus abdominis muscle inferiorly, and the serratus
anterior muscle to the latissimus dorsi muscle laterally. Dissection along the latissimus dorsi
muscle continues to the level of its tendinous insertion just inferior to the axillary vein.
◆ The resection of the breast off the chest wall posteriorly includes the retromammary fascia
with the investing fascia of the pectoralis major muscle.
◆ The mammary gland with the superfi cial fascia and the posterior investing fascia of the
pectoralis major muscle is resected from superomedial to inferolateral, exposing the axillary
fat pad containing the draining lymph nodes and the lateral aspect of the pectoralis major
muscle (Figure 10-6). Care should be taken to dissect the fascia in the avascular plane
parallel to the muscle fi bers to avoid transection of muscle fi bers, especially along the
sternal insertion medially and along the rectus sheath inferiorly. The fascia of the serratus
anterior muscle should be left intact if immediate implant reconstruction is planned, unless
contraindicated by disease.
◆ Perforating muscular blood vessels and intercostal vessels should be ligated with 3-0 silk
ligatures or be cauterized. Care should be taken to avoid traction on these vessels, which
have a tendency to retract and be an occasional source of postoperative bleeding. Blind
dissection for these vessels may lead to entry into the chest cavity and pneumothorax.
◆ The breast remains attached laterally exposing the axilla, the pectoralis major muscle
medially, and the latissimus dorsi muscle laterally.
◆ The boundaries of the axilla are defi ned by the pectoral muscles medially, the latissimus
dorsi muscle laterally, the axillary vein superiorly, and the subscapularis and teres major
muscles posteriorly.
CHAPTER 10 • Modifi ed Radical Mastectomy 123
Overlying fascia of
pectoralis major
muscle
FIGURE 10 –5
Incision being carried out
to include axillary region
FIGURE 10 –6

124 Section II • The Breast
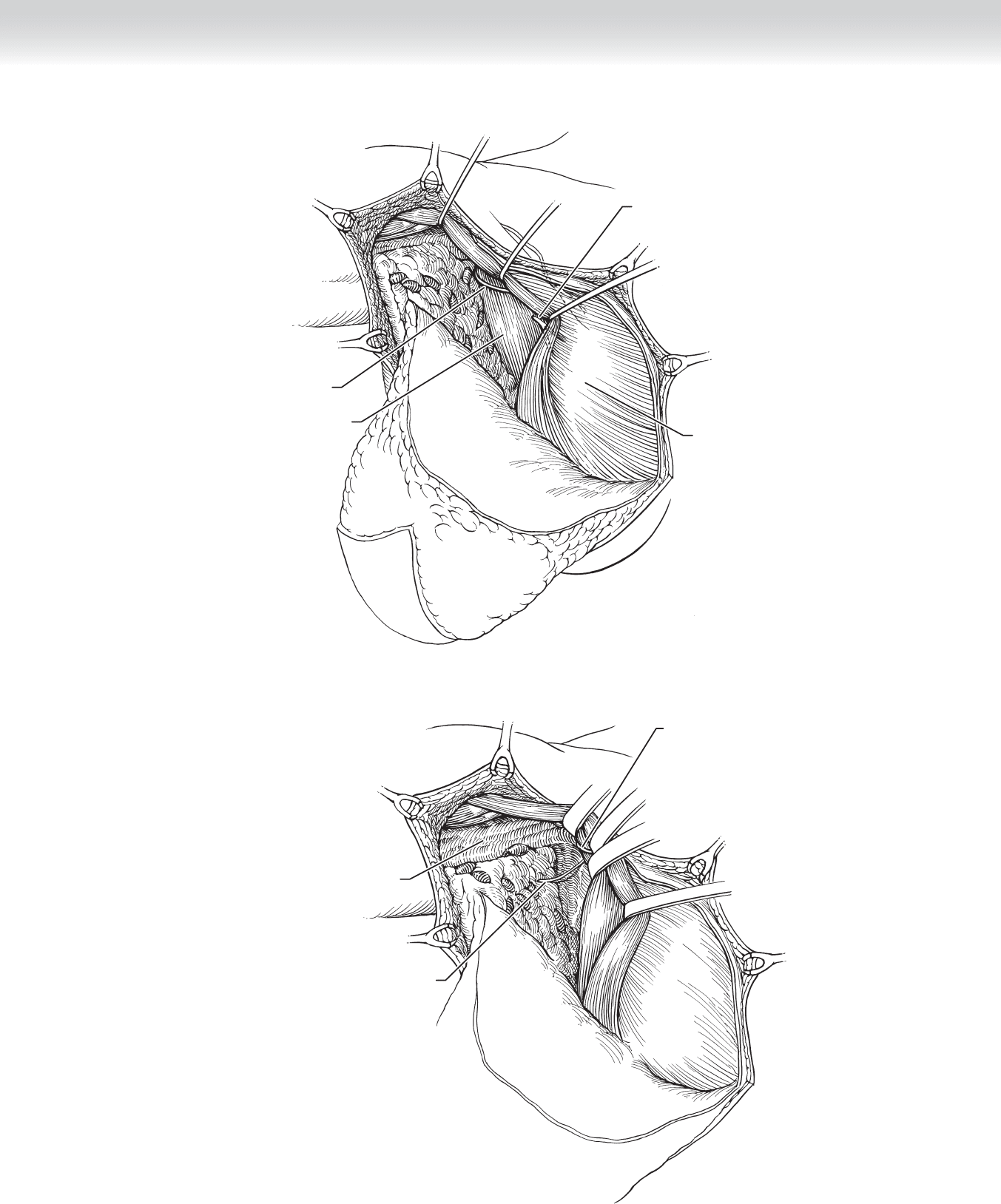
◆ Dissection of the axilla is undertaken by incising the fascia of the pectoralis major muscle
from inferior to superior (Figure 10-7). Care must be exercised to avoid injury to the
medial anterior thoracic nerve (medial pectoral nerve), which may penetrate both pecto-
ral muscles and emerge medially or may course along the lateral aspect of the pectoralis
minor muscle. Injury to this nerve may lead to atrophy of part of the pectoralis major
muscle.
◆ The fascia along the pectoralis major muscle is incised and retracted medially with a small
or medium Richardson retractor, exposing the underlying pectoralis minor muscle
(Figure 10-8). The clavipectoral fascia along the pectoralis minor muscle is then incised,
and the retractor is replaced exposing the level II nodes posterior to the pectoralis minor
muscle. The arm may now be rotated medially to take tension off the pectoral muscles and
expose the axillary contents. Care must be taken to avoid traction of the extremity and the
brachial plexus in the anesthetized patient.
◆ The intercostal brachial cutaneous nerve may be identifi ed coursing transversely below the
axillary vein and should be preserved if free of matted tumor-laden nodes to avoid bother-
some sensory dysesthesias along the medial aspect of the upper arm.
◆ Dissection medially should be cautious, with attention to the long thoracic nerve, which
lies on the serratus anterior muscle beneath the fascia. Retraction of the fascia off the chest
wall will pull the long thoracic nerve off the chest wall and place it at risk of injury. The
nerve can be identifi ed deep to the intercostal brachial nerve or higher, inferior to the
axillary vein on the chest wall, where it is less likely to have been pulled away from the
serratus anterior muscle into the axillary fat. The nerve should be protected and preserved.
The function can be confi rmed by very gentle compression and demonstration of
contraction of the serratus muscle in the unparalyzed individual. Injury to the long thoracic
nerve causes a winged scapula.
◆ Lateral dissection of the axilla is along the latissimus dorsi muscle to the tendinous inser-
tion. The axillary vein overlies the tendinous insertion, and care should be taken to proceed
cautiously from lateral to medial and from superfi cial to deep, with careful visualization of
underlying structures.
CHAPTER 10 • Modifi ed Radical Mastectomy 125
Medial anterior
thoracic nerve
(40% lateral to
pectoralis minor
muscle)
Pectoralis minor muscle
Medial anterior thoracic nerve
(60% through pectoralis minor muscle)
Pectoralis major muscle
FIGURE 10 –7
Medial anterior
thoracic nerve
Intercostal brachial nerve
Axillary artery and vein
covered by fascia
FIGURE 10 –8
126 Section II • The Breast
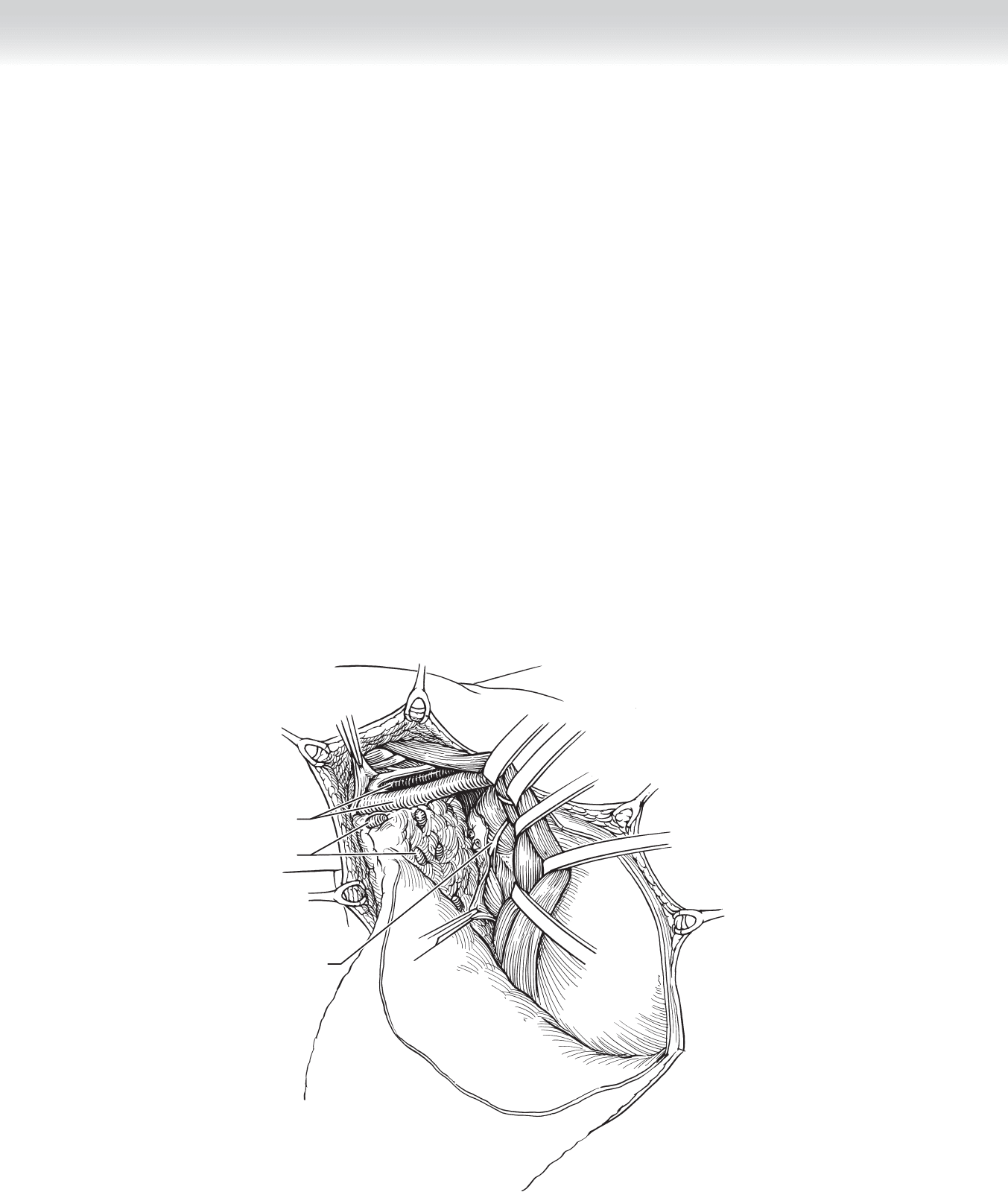
◆ The superior extent of the axillary dissection should begin approximately 5 mm below the
axillary vein to preserve the lymphatics of the arm and reduce the likelihood of upper
extremity lymphedema (Figure 10-9).
◆ Figures 10-9, 10-10, and 10-11 show dissection with exposure of the brachial plexus
above the axillary vein for anatomic orientation, but the dissection should stop just below
the vein. This tissue is rich in lymphatics and blood vessels, which should be ligated with
fi ne silk ties or Weck Hemoclips. Preservation of the lymphatics surrounding the axillary
vein reduces the risk of lymphedema.
◆ The thoracodorsal artery and vein with the thoracodorsal nerve medially will be identifi ed
in the lateral third of the axillary artery (see Figure 10-10). The thoracodorsal trunk courses
on the medial aspect of the latissimus dorsi muscle. Transection of the thoracodorsal nerve
leads to weakened shoulder adduction. Once the thoracodorsal trunk is identifi ed, lateral
dissection is safe as long as the intercostal brachial cutaneous nerve is visualized as it
emerges from the axillary fat pad, approximately halfway up the latissimus dorsi muscle
coursing toward the arm.
◆ Dissection of the axilla is carried out from superior to inferior, maintaining visualization of
the nerves at risk. As the fatty tissue is swept inferiorly, lymphatics and blood vessels are
transected.
Axillary vein
and artery
Lymph nodes
Long thoracic nerve
FIGURE 10 –9