Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 95
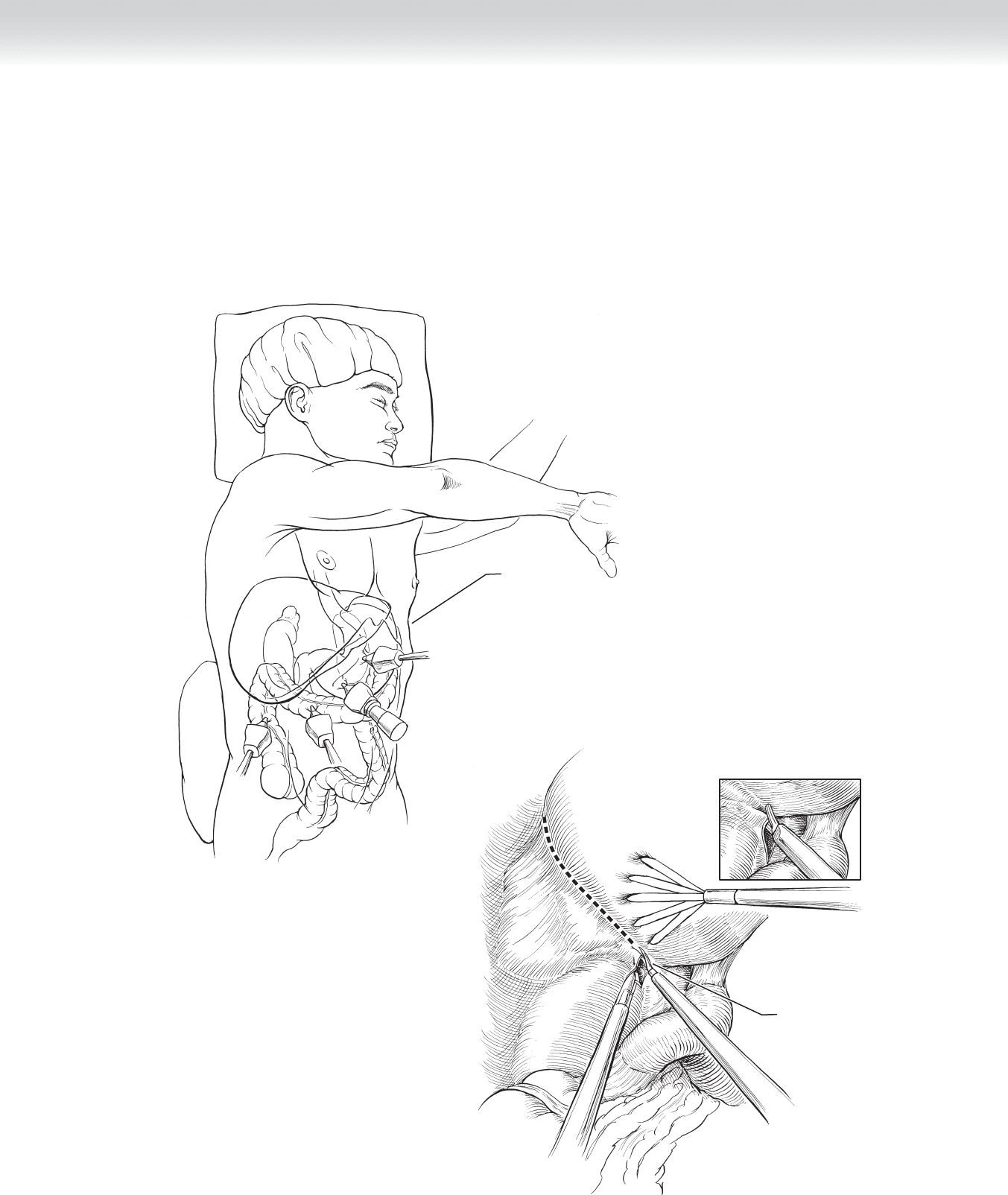
Right-Sided Laparoscopic Operation
◆ The triangular ligament of the right hepatic lobe is divided, and gravity retracts it medially
usually without the need for a specifi c liver retractor. At this time the adrenal gland is usu-
ally easily identifi ed above the kidney and lateral to the vena cava (Figure 8-5).
Patient in
right lateral
decubitus
position
A
Incising through right
triangular ligament
B
FIGURE 8 –5
96 Section I • Head and Neck and Endocrine Procedures
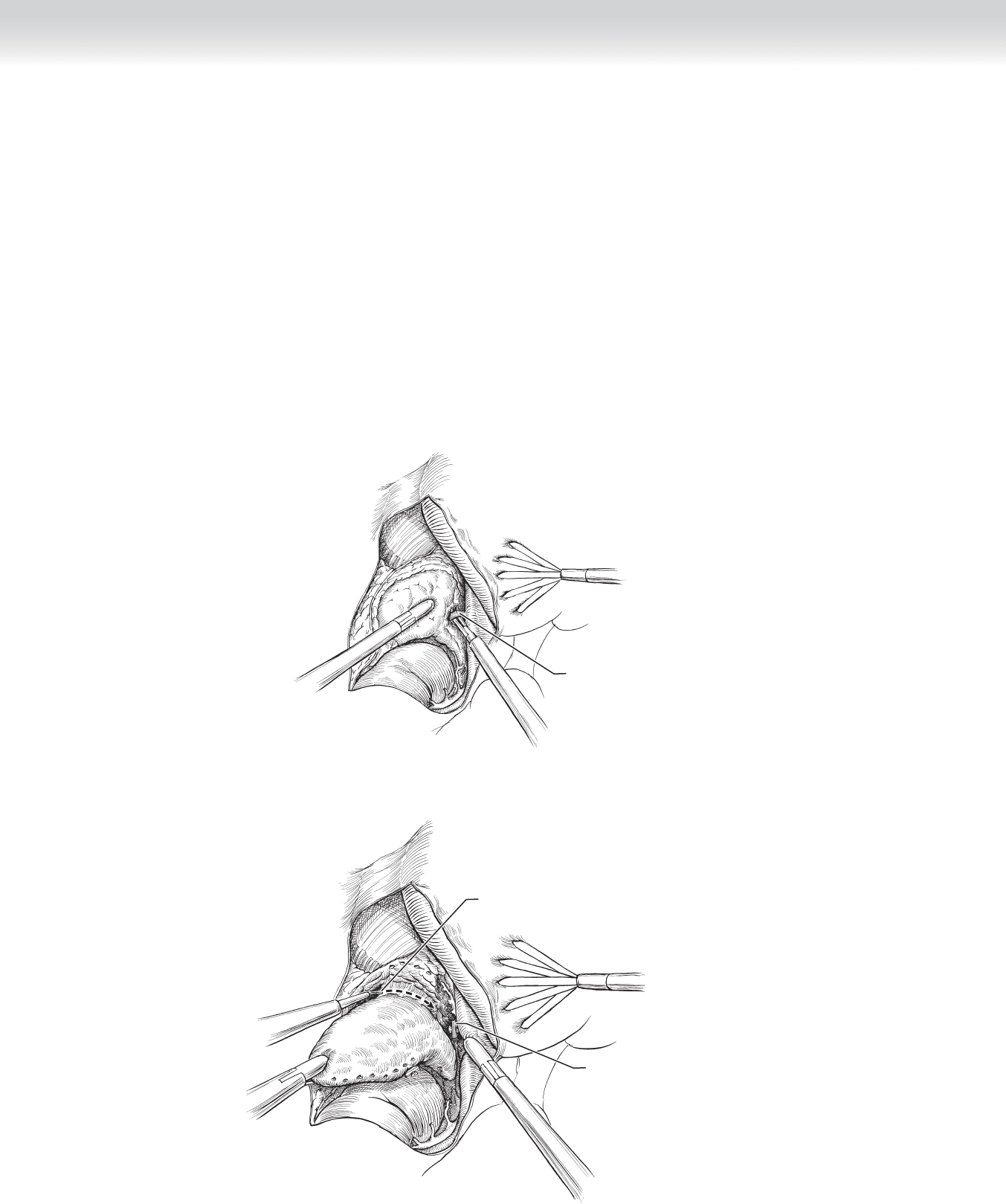
◆ Identifi cation of the adrenal vein is then pursued at the lateral aspect of the vena cava with
lateral displacement of the adrenal gland. A right-angle dissector is very useful here. Once
identifi ed, the vein is clipped and divided (Figure 8-6).
◆ The remainder of the blood vessels and attachments are easily controlled and divided with
the ultrasonic dissector (Figure 8-7). This dissection progresses medial to lateral, so the
lateral attachments provide lateral retraction until the completion of the mobilization.
◆ Once liberated from its attachments, the gland is placed in a retrieval bag and removed.
Right
adrenal vein
FIGURE 8 –6
Clip on
right adrenal vein
Removing adrenal gland
FIGURE 8 –7
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 97
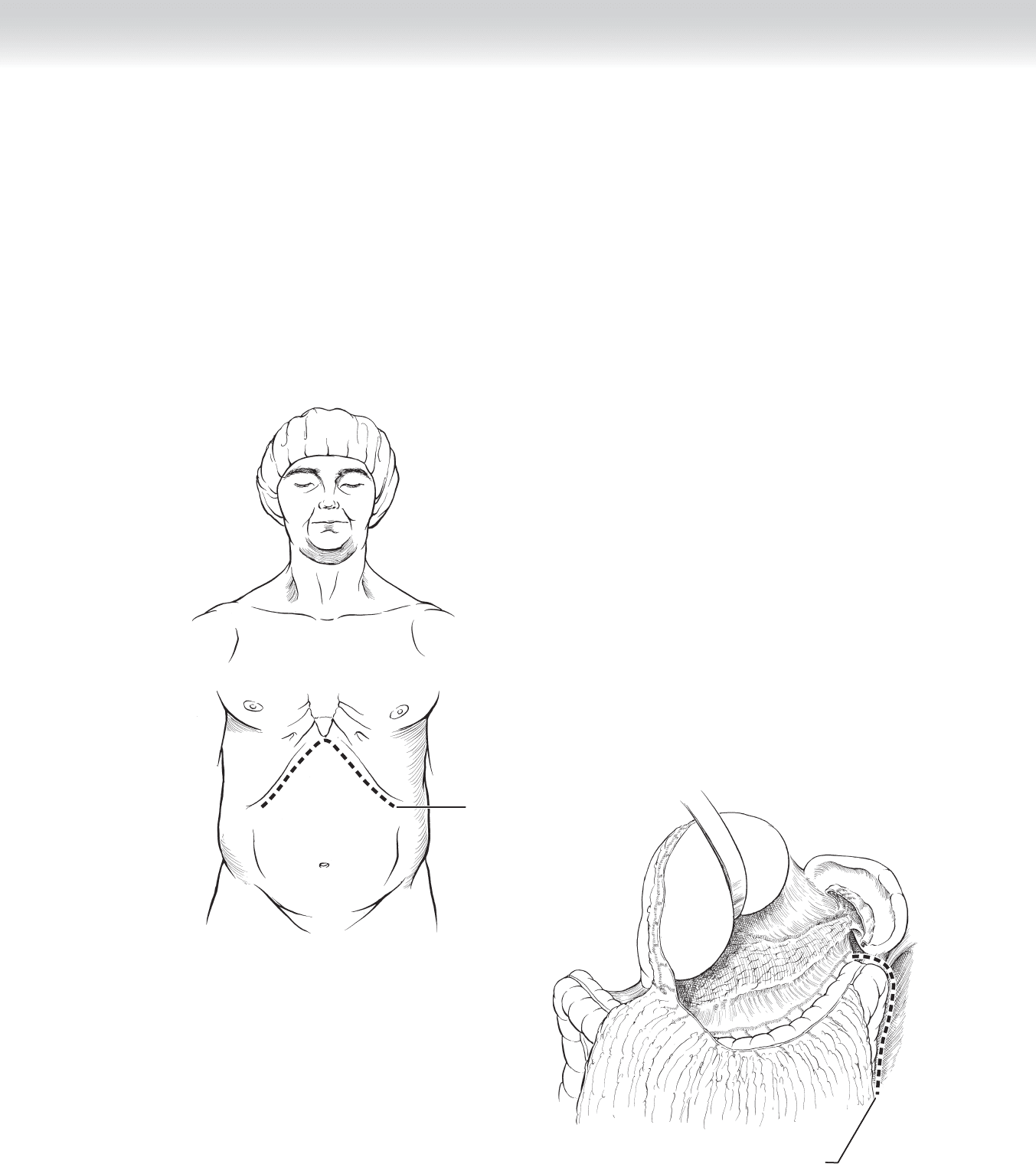
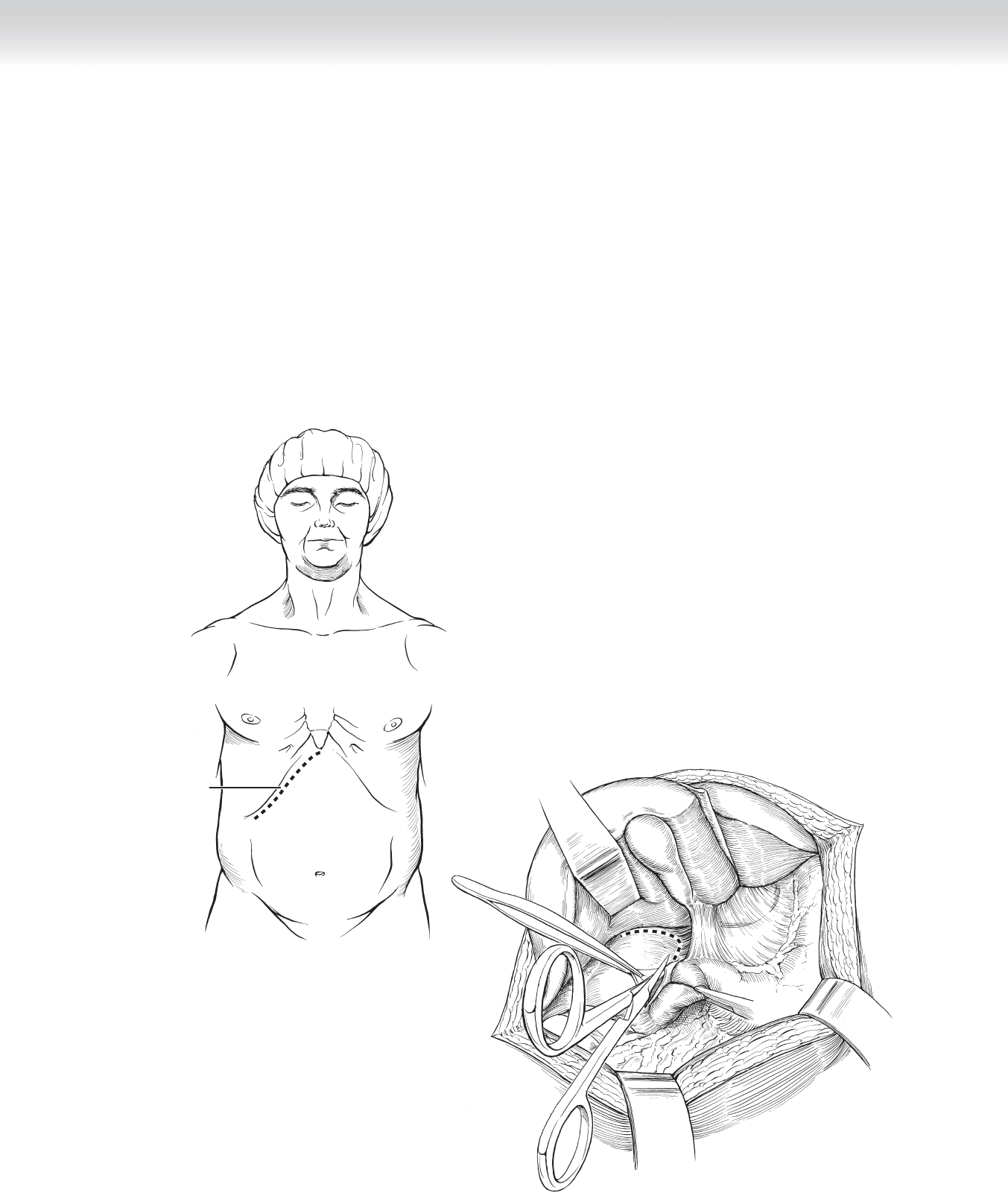
Left-Sided Anterior Open Approach
◆ One approach to left adrenalectomy is full mobilization of the splenic fl exure and
splenorenal ligament as described in the laparoscopy section.
◆ Another approach is through the lesser sac. After the abdominal incision of choice is made,
the lesser sac is opened by incision of the greater omentum at the insertion onto the left
side of the transverse mesocolon (Figure 8-8).
B
Incision to mobilize
splenic flexure
Subcostal incision
A
FIGURE 8 –8
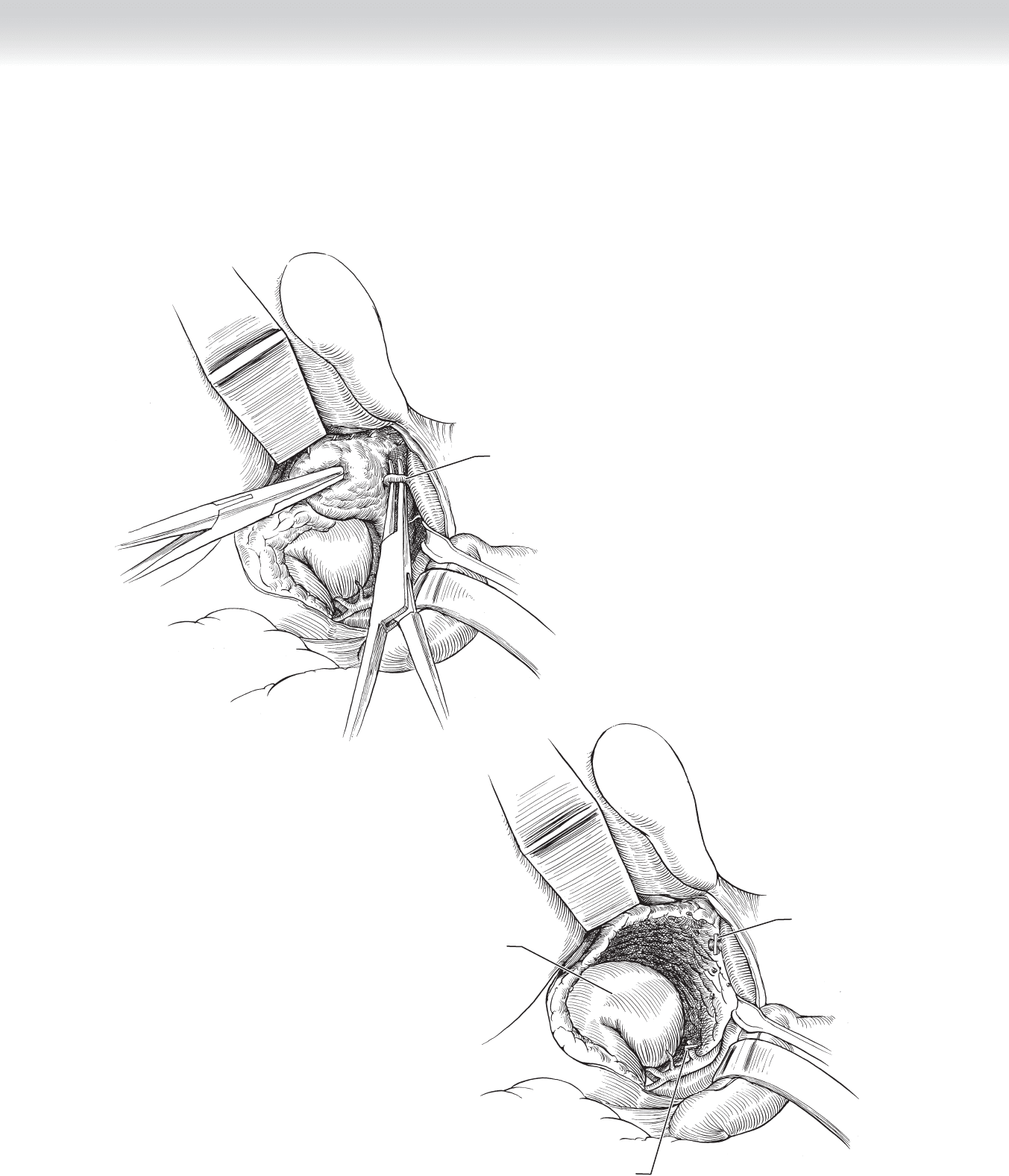
98 Section I • Head and Neck and Endocrine Procedures
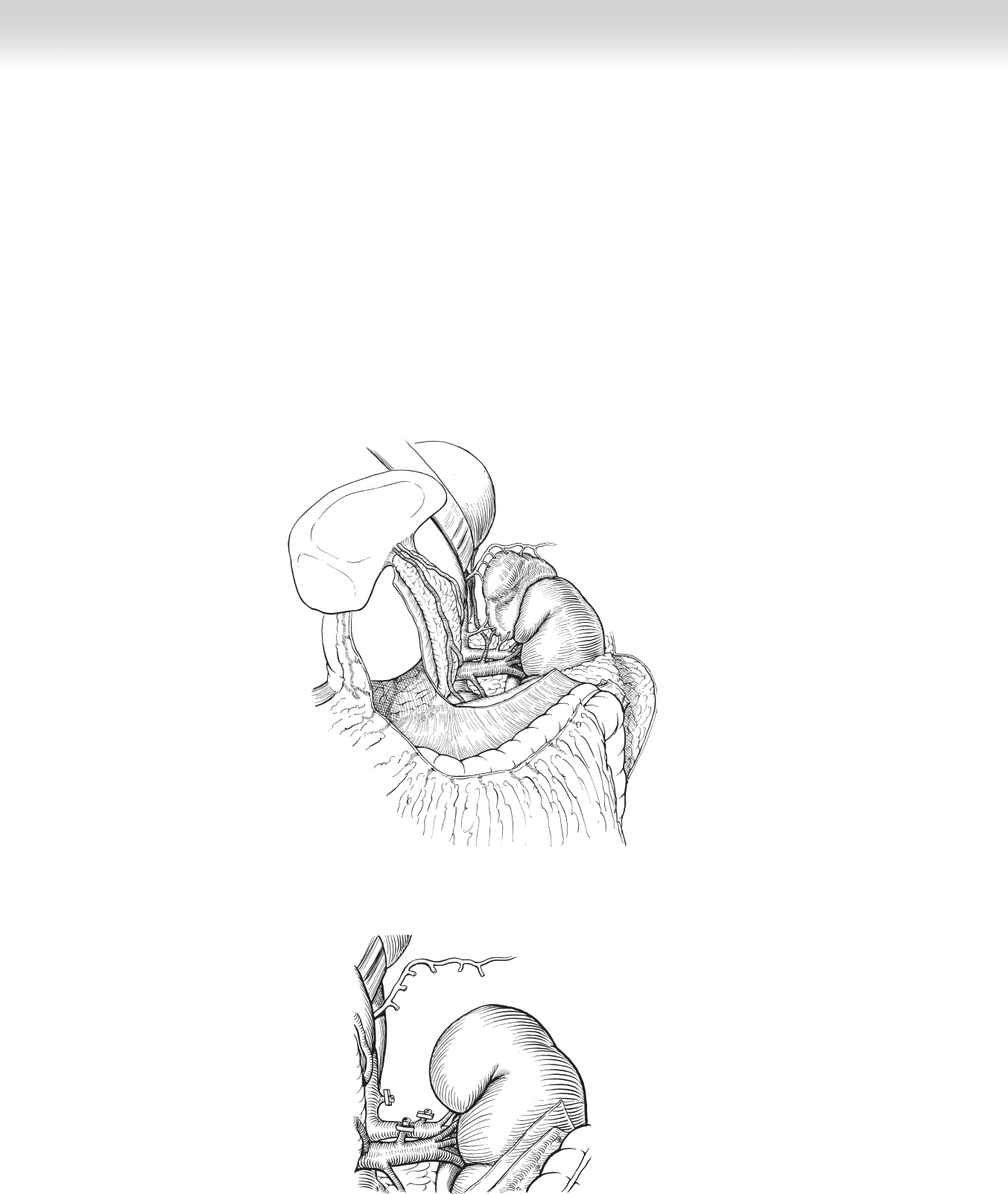
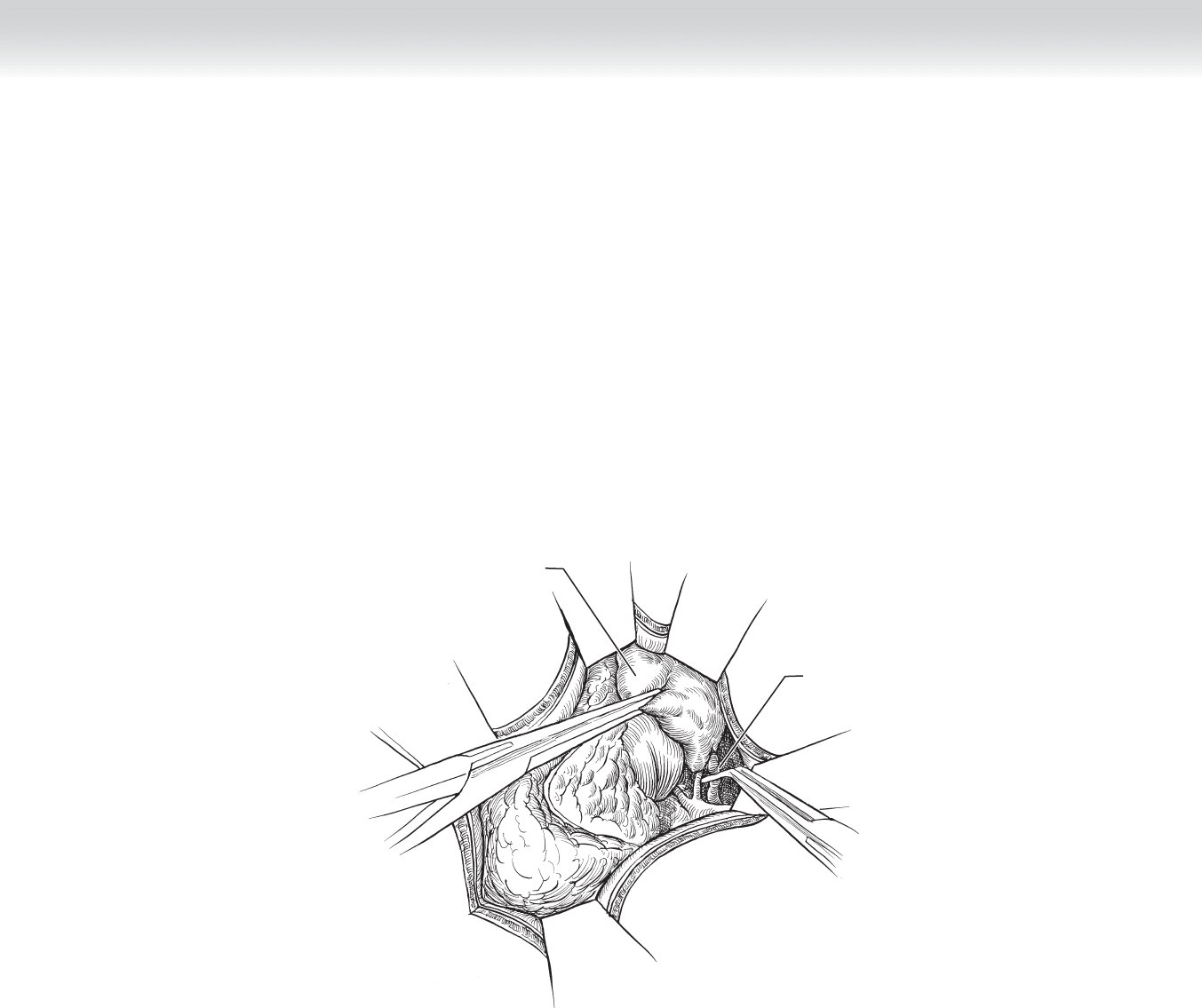
◆ The peritoneum below the tail of the pancreas is incised so that the tail of the pancreas can
be retracted superiorly (Figure 8-9).
◆ The peritoneum covering the left renal vein is opened, and the left adrenal vein is identifi ed
on the superior aspect of the left renal vein lateral to the aorta. The left renal vein is ligated
and divided (Figure 8-10).
◆ The blood vessels and tissues around the perimeter of the adrenal gland are divided
using a combination of blunt and sharp dissection and suture ligation when needed. This
dissection proceeds from medial to superior, then lateral, and fi nally inferior.
FIGURE 8 –9
FIGURE 8 –10
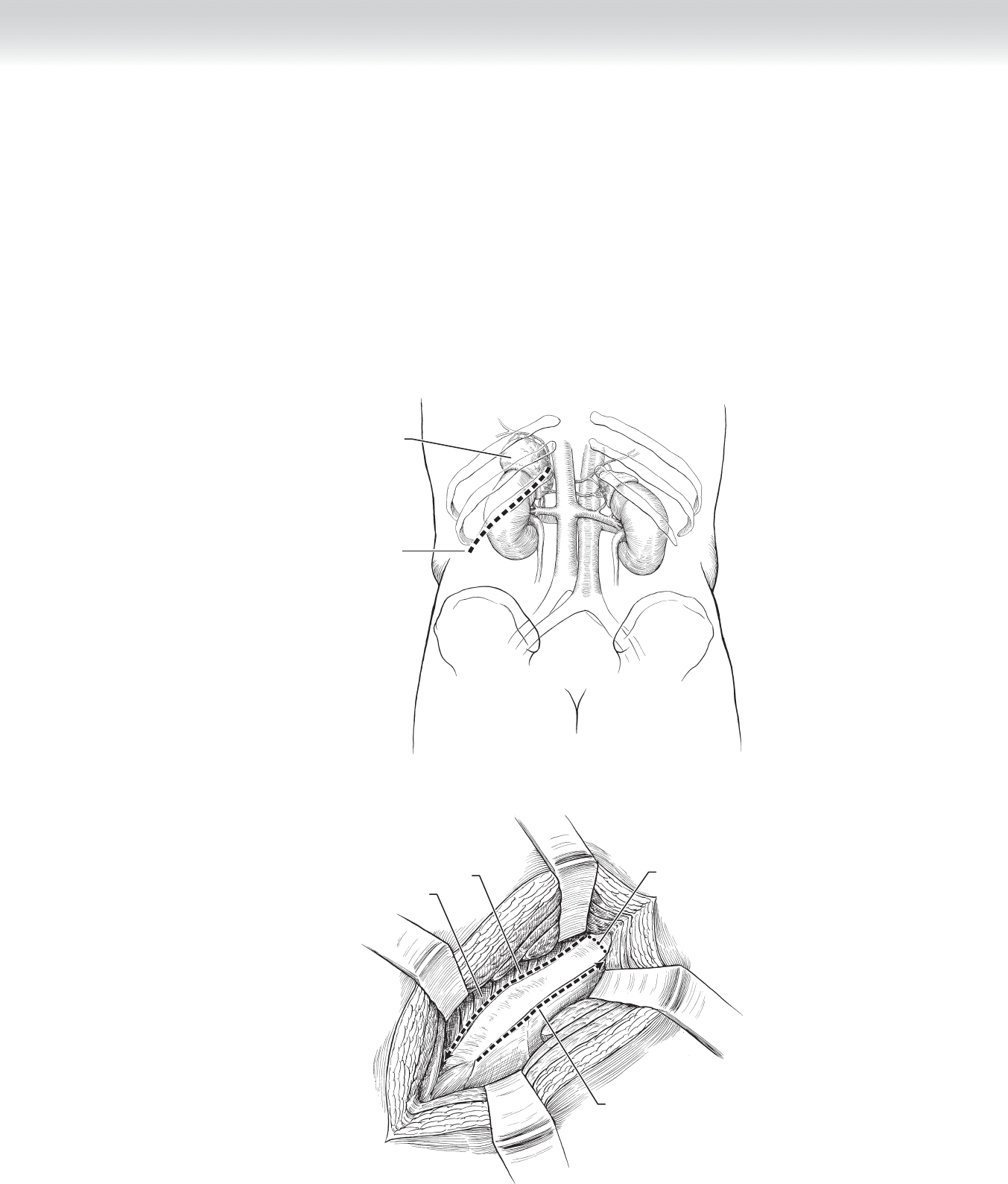
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 99
Right-Sided Anterior Open Approach
◆ The right lobe of the liver is retracted superiorly, or the triangular ligament is incised to
retract the liver medially. The kidney, vena cava, and adrenal mass should be visualized
behind the peritoneal covering. Occasionally, a Kocher maneuver may be performed to
provide better exposure.
◆ The peritoneum just lateral to the vena cava is incised. Dissection in the plane between the
vena cava and the adrenal gland will expose the right adrenal vein, which should be ligated
and divided at this time (Figure 8-11).
Subcostal incision
A
B
FIGURE 8 –11
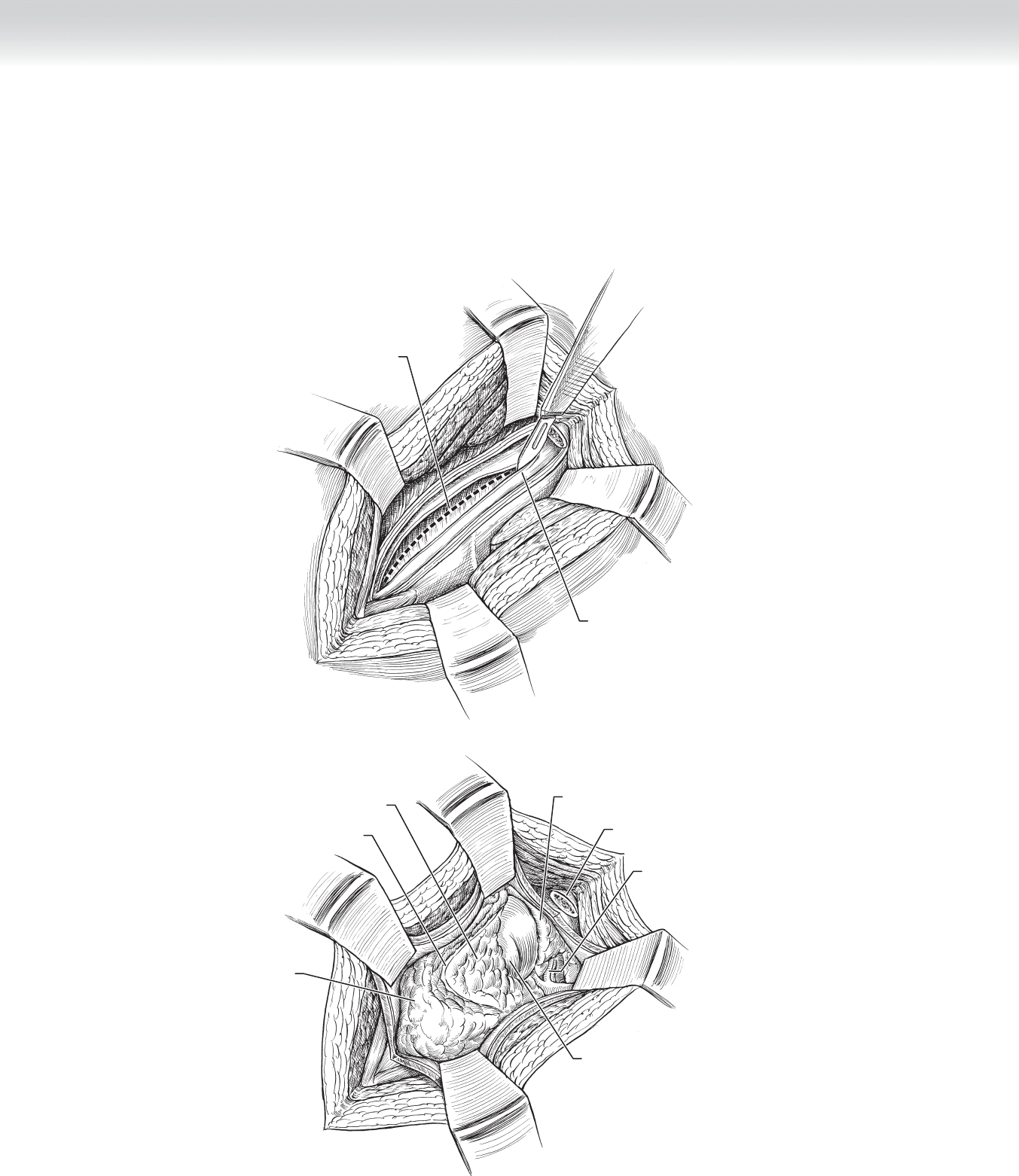
100 Section I • Head and Neck and Endocrine Procedures
◆ The remaining attachments of the adrenal gland should be divided around its perimeter
(Figure 8-12). Occasionally, for larger tumors, a large feeding vessel may be encountered,
which may require ligation, but most of this mobilization can be done with the ultrasonic
dissector.
A
Right
adrenal vein
B
Clip on
right adrenal vein
Clip on accessory
right adrenal vessel
Right kidney
FIGURE 8 –12
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 101
Posterior Open Approach
◆ The posterior approach requires appropriate positioning and padding of the patient in the
prone position.
◆ The incision over the 12th rib is deepened to the level of the periosteum, which is then in-
cised. The 12th rib is resected as far medially as reachable. A self-retaining retractor is
placed to provide exposure (Figure 8-13).
Incision over
12th rib
A
Enlarged left
adrenal gland
B
Stripping 12th rib superiorly
medial to lateral
Intercostal muscles
Stripping 12th rib inferiorly
lateral to medial
Resect rib
FIGURE 8 –13
102 Section I • Head and Neck and Endocrine Procedures
◆ The intact pleural membrane is carefully dissected from its attachments to the diaphragm,
and the diaphragm may need to be incised radially along the line of its fi bers. Care is
taken to avoid injury to the intercostal nerve, especially during subsequent retraction
(Figure 8-14).
A
Incision through diaphragm
Incise through pleura
B
Perirenal fat
Renal capsule
Perirenal fat
Left adrenal
artery and vein
Resected 12th rib
Left kidney
Left adrenal gland
FIGURE 8 –14
CHAPTER 8 • Adrenals—Anterior, Posterior (Open and Laparoscopic) 103
◆ The fascia enveloping the kidney and adrenal gland (Gerota’s fascia) is incised. A retractor
placed medially and beneath Gerota’s fascia and the diaphragm provides exposure while the
fat and adrenal gland are swept inferiorly (Figure 8-15).
◆ As with the other adrenalectomy techniques, the dissection should be aimed at careful identifi -
cation, ligation, and division of the adrenal vein early. However, the small adrenal arteries
should be ligated as they are encountered on the way to the vein. For a left adrenalectomy, the
left adrenal vein may not be visible until the gland is mobilized circumferentially.
◆ The remaining attachments are divided and the entire gland is removed.
Placing a clip on
left adrenal vein
Adrenal gland
FIGURE 8 –15

104 Section I • Head and Neck and Endocrine Procedures
3. CLOSING
◆ Port sites up to and including 12 mm do not need fascial closure if dilating tip trocars are
used in place of cutting trocars. For cutting trocars, all port sites larger than 5 mm should
be closed using a laparoscopic suture passer.
◆ Standard closure of the incision after the open approaches should be tailored to the sur-
geon’s preference.
◆ For the posterior approach, the diaphragm is closed with interrupted, horizontal mattress
polypropylene sutures. The pleural membrane should then be inspected for holes, and if
present, a small caliber drainage tube should be placed before the hole is sutured closed.
The remaining layers are closed with absorbable suture.
STEP 4: POSTOPERATIVE CARE
◆ Pain management for laparoscopic adrenalectomy is with oral analgesics, whereas the open
approaches typically require intravenous narcotics.
◆ The diet should be advanced as tolerated, with the expectation that the anterior open
approaches may result in some degree of postoperative ileus.
◆ The most common complications are the result of injury to adjacent structures. Adrenal
vein, vena cava, liver, and kidney injuries result in life-threatening bleeding during the
operation or more subtle bleeding with the development of a hematoma postoperatively. A
missed thermal or retractor injury to the intestines will cause sepsis in the fi rst week after
the operation.
◆ Acute adrenal insuffi ciency should be suspected in patients developing hemodynamic
instability postoperatively. Prompt recognition and treatment with steroids are critical to
avoid a potentially fatal outcome.
◆ Glucocorticoid stress doses are tapered postoperatively for patients with cortisol-secreting
tumors but should be administered until the function of the hypothalamic-pituitary-
adrenal axis is confi rmed with an adrenocorticotropic hormone (ACTH) suppression test.
◆ Patients having bilateral adrenalectomy should have life-long replacement of glucocorticoids
and mineralocorticoids.