Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


Hypotheses Tested by Dietary
Intervention Trials
0019 It would be a mistake to summarize the present
situation on dietary trials in CHD, as results are
constantly accumulating and the picture is changing.
Rather, intervention trials in a few areas will be
described briefly, largely in order to illustrate meth-
odological aspects.
Dietary Fat Reduction
0020 Undoubtedly, the relationship of saturated fat to fat
reduction has been more investigated in the preven-
tion of CHD than any other potential prophylactic.
The early trials focused largely on the reduction of
total fat in the diet; interest then focused on the P:S
ratio (the ratio of polyunsaturated to saturated fats)
and on monounsaturated fats. Almost all metaana-
lyses or overviews of dietary RCTs have failed to
detect any significant reduction in mortality from
dietary changes aimed at reducing cholesterol, though
several overviews have reported a significant reduc-
tion of around 20% in the incidence of nonfatal
myocardial infarctions. (See Cholesterol: Role of
Cholesterol in Heart Disease; Fats: Requirements.)
0021 An issue worth noting because of its wider rele-
vance to the drawing of conclusions from trials is
the degree to which successful trials are cited in pref-
erence to negative trials. A report of an overview of
22 RCTs in which the effect of a reduction in dietary
fat intake had been examined went on to examine
how often these trials had been cited in the general
literature. It was found that the few trials in which a
reduction in CHD had been observed had been cited
six times more frequently than the trials which had
failed to find such an effect. This positive bias in the
reporting of trials is serious bias in any overview of
the literature, whether this is based upon a formal
metaanalysis, or simply an impression gained from
reading the literature.
0022 The relevance of cholesterol level to vascular dis-
ease has been very considerably reinforced by the
results of recent RCTs of statin drugs. These drugs
substantially reduce cholesterol level, and at the same
time are associated with a reduction in vascular dis-
ease incidence and mortality. The reduction in disease
appears however to commence virtually immediately,
and this has led to the suggestion that some of the
benefit from these drugs may arise because of effects
that have been described on platelet function, on
hemostasis and on immunological mechanisms.
0023 Within the area of lipids and vascular disease, one
trial stands out. This tested the effect of the so-called
‘Mediterranean diet,’ a dietary pattern modeled on
the dietary pattern in Crete and other Mediterranean
communities. The initial finding was a 70% reduction
in all-cause mortality together with comparable reduc-
tions in nonfatal events, and these results have been
sustained in a 4-year follow-up, reported in 1999. The
diet advised in this trial was rich in fruit and vegetables,
but the group responsible for the study considered
that its most important feature was its richness in
a-linolenic acid. In the trial this last was achieved by
distributing a special margarine containing rapeseed
oil to half the subjects. At present only one RCT of a
Mediterranean type of diet has been reported. Clearly
there is an urgent need for further trials.
Fatty Fish
0024The hypothesis that fatty fish, fish oil, or eicosapen-
taenoic acid might reduce the risk of CHD emerged
from surveys of Inuit in Greenland in the 1930s.
Later, historical studies showed that changes in fish
consumption during World War II had been accom-
panied in The Netherlands and in Norway by de-
creases in heart disease mortality. Laboratory and
animal studies then examined the effects of fish oil
on various risk factors and certain mechanisms
involved in CHD. This was the background to the
setting-up of a major RCT of fish and mortality. A
total of 2033 men were randomized factorially to
three interventions, one of which was the consump-
tion of fatty fish on at least 2 days each week. The
consumption of fish was associated with a reduction
in mortality of about 30% and a saving of lives of
about 36 per 1000 men advised. Because these esti-
mates of benefit are derived from the results of a
single trial they carry a considerable uncertainty. Fur-
ther trials are required, followed, hopefully, by a
metaanalysis. It is notable, however, that this trial
gave no evidence that nonfatal infarctions were re-
duced by the fish consumption. Indeed, there were
rather more nonfatal infarctions in the men advised
(4.8%) than in the other men (3.2%). It is therefore
possible that the effect of fish is to reduce the risk of
death after infarction rather than to reduce the
incidence of infarction. Evidence consistent with
this hypothesis comes from studies of the electrical
stability of the myocardium in animals, following
experimentally induced infarction.
Fruit and Vegetables
0025It is believed that the oxidation of lipids is an im-
portant step in the development of atherosclerosis.
Oxidized low-density lipoprotein cholesterol is
potentially highly atherogenic, while antioxidants
prevent its oxidation and reduce the risk of other
oxidative damage, thus retarding the development
of atherosclerosis. There is therefore growing interest
in the protective effect of both supplements of the
1666 CORONARY HEART DISEASE/Intervention Studies

antioxidant vitamin supplements, including vitamins
E, C, and b-carotene, and in fruit and vegetables
which carry these and other antioxidants.
0026 Numerous observational studies based on commu-
nities and on individuals give supporting evidence of
benefit. In fact, the evidence is virtually totally consist-
ent that subjects and groups with high consumptions of
fruit and/or vegetables have a reduced incidence of
both digestive cancers and of CHD. Despite their con-
sistency, however, these observations are seriously open
to confounding by related social and other dietary
factors. Hence there is no substitute for RCTs.
0027 A number of RCTs have been conducted to test the
effects of supplements of vitamins E, C, and/or
b-carotene. A recent overview of these has concluded
that ‘there is no clear indication for the use of these
supplements . . . and the suggestion of potential harm
associated with b-carotene in two clinical trials
(indicates) that b-carotene in the form of additional
vitamin supplements should be avoided.’
0028 On the other hand, RCTs of fruit and vegetables
necessitate increasing consumption of these foods by
half the subjects studied, and even in a so-called
secondary preventive trial the dietary increase has
to be either large or prolonged, or both. This makes
such trials very difficult. The diets of older subjects
tend to be relatively fixed, and it is exceedingly
difficult to persuade subjects – even patients who
have already had a clinical CHD event – to increase
their consumption of any food item. In our experience
this is especially true for fruit and vegetables. (See
Antioxidants: Natural Antioxidants.)
Dietary Fiber
0029 For a very long time there has been interest in dietary
fiber. At first this focused upon ‘roughage,’ or un-
absorbed dietary material, and measures such as
fecal bulk and bowel transit time were commonly
used. Interest then focused on cereal fiber, the diseases
of possible relevance being bowel cancer and CHD.
Numerous observational studies have been reported,
but one of the uncertainties in all of these is the effect
of confounding factors. In fact, confounding is a
major source of possible confusion in all dietary stud-
ies that are dependent upon observation. The diet of
an individual is determined by a host of factors, in-
cluding lifestyle, education, social standing and
income level, educational and psychological factors.
Furthermore, the consumption of any one food or
diet factor is interrelated with a host of other foods,
and cannot realistically be considered in isolation.
For example, an increase in the consumption of
wholemeal bread will probably lead to an increase
in spreading fats; an increase in fish consumption will
probably be balanced by a reduction in meat. It will be
almost impossible to take account of all these con-
founding and interrelated factors in a study of disease
incidence in relation to a single food item or nutrient.
The final elucidation of relationships between diet and
disease must therefore be ultimately dependent upon
intervention studies, in which control over confound-
ing is achieved by randomization, and different levels
of dietary intake are achieved experimentally.
0030There has been only one RCT of dietary fiber and
CHD. This was conducted by Burr and his colleagues
in south Wales. Advice was given to 1017 men who
had already had a myocardial infarct. This led to a
mean intake of cereal fiber of 19 g per day, compared
with 9 g in 1016 controls given no advice about fiber.
After 2 years there was no significant difference in the
deaths in those given the advice about fiber (12.1%)
compared to those not so advised (9.9%).
0031Interest in fiber has however shifted again, and
attention is now being focused on soluble fiber.
This, too, is confounded and interrelated with numer-
ous other food items and nondietary items and its
importance will only be sorted out by RCTs.
Interpretation of the Results of RCTs
Relative and Absolute Risk Reduction
0032There are two important aspects of trials that should
be understood. First, the results of a controlled trial
can be expressed as ‘relative’ protection, or the ‘rela-
tive’ reduction in the outcome events, or they can be
expressed in terms of the ‘absolute’ effect of the inter-
vention. This can be very easily illustrated.
0033In the Diet and Reinfarction Trial (DART) 1015
post-myocardial infarction patients were given
advice to eat fatty fish on at least 2 days per week. A
group of 1018 other patients, selected at random, were
given no such advice. During the next 2 years 127
(12.5%) of the men advised to take fish had a CHD
event, while 149 (14.6%) given no such advice had an
event. The difference between these incident figures
implies a relative reduction in the risk of an event of
30%. On the other hand, the absolute reduction was
2% over the 2 years or one IHD event was prevented
per year in every 100 patients advised to eat fatty fish.
0034Both these figures are correct, but each expresses
rather different concepts. Thus the relative reduction,
or relative benefit, is the proportionate extent to
which the risk is reduced in a group in which there
has been an intervention, compared to a control group
with no such intervention. The absolute reduction, or
absolute benefit, is the number of events prevented.
Another way of expressing this last is the number
needed to treat (NNT) to prevent one disease event.
Clearly, for fatty fish, this is 100 patients for 1 year.
CORONARY HEART DISEASE/Intervention Studies 1667

0035 While figures of absolute benefit may at first sight
appear disappointing, they carry a wealth of infor-
mation. Thus, in the above example, one can say that,
of every 100 patients advised to eat fatty fish, a CHD
event will be prevented in one or two each year, but
about six will still die from CHD each year. About 92
will derive no benefit because, judging from the
experience of the subjects in the control group, they
would have survived anyway. No worry! They will
have enjoyed the fatty fish and will probably have
saved money on meat!
0036 Intervention with drugs has much the same protect-
ive effect (for example, antihypertensives achieve a
relative reduction in CHD event of about 25%, that
is, closely similar to the 30% achieved by fish con-
sumption in DART). However the patients who are
given drugs, and who would have survived anyway,
will have been exposed to the undesirable side-effects
of the drugs, and their therapy will have generated
considerable costs. None of this is meant to imply
that dietary intervention is a substitute for medica-
tion. Raised CHD risk factors should be treated ap-
propriately, but considerations should also be given
to dietary intervention. These are not in competition.
Overviews or Metaanalyses
0038 In the nature of things, certainty is unobtainable and
even the largest and most carefully conducted RCT
can, by chance, give a wrong answer. Firm conclu-
sions should only be based on evidence drawn from a
number of trials. The play of chance can never be
ruled out, whatever the level of statistical signifi-
cance, and consistency in a number of studies is likely
to be a better guide to truth than the results of any
single study. Further to this, the results of any single
trial cannot be extrapolated to the general population
with certainty. Conclusions from a trial are limited
by issues such as the selection of patients tested, the
diagnostic criteria used, the way the intervention was
achieved, and the possibility that the intervention
may have affected other factors of relevance to the
disease. Together, these uncertainties can make it in-
appropriate and perhaps misleading to generalize the
results from any one study to patients in general and
make them the basis of clinical recommendations.
0045 Hence the importance of overviews of studies, or
metaanalyses of data from a number of different
studies. This approach is particularly appropriate
with RCTs, but it is important that data from every
relevant RCT are included.
0039 In fact, even the most meticulous search of the
literature followed by a formal overview of all the
evidence from relevant RCTs still leaves uncertainties.
There is publication bias, and reports which report an
effect are generally more likely to be accepted by a
journal than those which show no effect. But then this
limitation affects judgments based simply on cumula-
tive reading of the literature, however carefully done.
Nevertheless, the approach in research that is likely to
get closest to the truth is clearly drawing conclusions
from all the available acceptable evidence. Cochrane,
an epidemiologist, saw this and he commented in a
Rock Carling lecture, later published as Effectiveness
and Efficiency: ‘It is surely a great criticism of our
profession that we have not organised a critical sum-
mary, by speciality or sub-speciality, adapted period-
ically, of all relevant clinical trials.’
The Cochrane Collaboration
0040This urging by Cochrane led to the setting-up of
the Cochrane Centre in Oxford, and then to the
Cochrane Collaboration, a worldwide effort coordin-
ated in 11 Cochrane Centres. The collaboration aims
to identify every RCT ever done in medical care, to
group these by clinical objective, and make them
readily available as databases. These then constitute
the basis for statistical overviews, or metaanalyses,
which draw on all the acceptable trial evidence
relevant to each clinical procedure.
Final Considerations
0041RCTs of dietary factors are immensely difficult and
before one is mounted consideration should be given
to a number of general considerations relevant to
intervention in cardiovascular disease. In summary,
there are unlikely to be any easy answers!
0042First, compliance with a dietary intervention is
likely to be poor. Trials of the effect of dietary advice
on cholesterol levels have generally shown very little
effect, and to some extent – and probably a very large
extent – this is because of the difficulties most people
find in making a significant, let alone a large, reduc-
tion in dietary saturated fats. Likewise, attempts to
increase the intake of dietary fiber or fruit and vege-
table intake have achieved relatively little change.
Results such as these have far-reaching implications
for the acceptability of prophylactic strategies in
symptomless subjects, or in the general population.
0043Second, effectiveness is likely to be low. Geoffrey
Rose defined a paradox – population preventive strat-
egies, even those with large overall potential benefit,
are likely to confer little benefit on the individual –
and he went on to describe the overall benefit/risk
balance in strategies involving the general population
as ‘worrisome.’ An overview by Davey-Smith and
Ebrahim of nine major population-based RCTs
of the effect of advice on diet, smoking, and blood
1668 CORONARY HEART DISEASE/Intervention Studies

pressure led to the conclusion: ‘The pooled effect of
intervention on multiple risk-factors is insignificant.’
0044 Third, the costs of intervention are likely to be
high. The cost of an intervention strategy that really
matters is not the cost of the change of diet, the cost
of nutritional supplements of medication in a single
subject. Rather, the cost that matters is that of
treating a sufficient number of subjects, for a suffi-
cient time to save one life, or prevent one disease
event. While this approach has been well developed
with drug therapy, the most relevant costs of a dietary
intervention are those that arise from the need for
subjects to accept a change in their diet, and for
most of us, a possible small change in the long-term
risk of a disease is far from the front of our minds
when preparing a meal.
See also: Antioxidants: Natural Antioxidants; Role of
Antioxidant Nutrients in Defense Systems; Cholesterol:
Role of Cholesterol in Heart Disease; Epidemiology;
Fats: Requirements
Further Reading
Alderson M (1983) An Introduction to Epidemiology, 2nd
edn. London: Macmillan.
Bradford-Hill A (1971) Principles of Medical Statistics, 9th
edn. London: Lancet.
Burr ML (1983) Epidemiology for nutritionists. 3. The
design of studies. Human Nutrition: Applied Nutrition
37A: 339–347.
Burr ML, Fehily AM, Gilbert JF et al. (1989) Effects of
changes in fat, fish, and fibre intakes on death and
myocardial reinfarction: Diet and Reinfarction Trial
(DART). Lancet ii: 757–761.
Cochrane AL (1971) Effectiveness and Efficiency: Random
Reflections on Health Services. London: Royal Society
of Medicine Press.
Davey-Smith G and Ebrahim S (1996) Health Promotion in
Older People for the Prevention of Coronary Disease and
Stroke. Health Promotion Effectiveness Review: Sum-
mary Bulletin 1. London: Health Education Authority.
Margetts BM and Nelson M (1977) Design Concepts in
Nutritional Epidemiology, 2nd edn. Oxford: OUP.
Muldoon MF, Manuck SB and Matthews KA (1990)
Lowering cholesterol concentrations and mortality: a
quantitative review of primary prevention trials. British
Medical Journal 301: 309–313.
Peto R, Pike MC, Armitage P et al. (1976) Design and
analysis of randomized clinical trials requiring pro-
longed observation of each patient. I. Introduction and
design. II. Analysis and examples. British Journal of
Cancer 34: 585–612; 35: 1–39.
Pocock SJ (1983) Clinical Trials: A Practical Approach.
New York: Wiley.
Ravenov U (1992) Cholesterol lowering trials in coronary
heart disease: frequency of citation and outcome. British
Medical Journal 305: 15.
Prevention
F G Huffman and S Nath, Florida International
University, Miami, FL, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001There has been a steady decline of coronary heart
disease (CHD)-related mortality in most industrialized
nations over the past few years. Despite this fact, CHD
remains the leading cause of morbidity and mortality in
adults of middle years and older (after age 65), leading
to a loss of productivity and substantial healthcare
costs in the industrialized countries. The World Health
Organization estimates that by the year 2010, CHD
would be the leading cause of death in the developing
countries as well. Therefore, prevention (both primary
and secondary) of CHD is extremely important from a
public health point of view.
0002The preceding section in this chapter highlights the
etiology of CHD that includes both modifiable and
nonmodifiable risk factors. Among all CHD risk
factors, cigarette smoking, unhealthy diet, overweight
or obesity, physical inactivity, high blood lipids (high
total cholesterol and elevated low-density lipoprotein
cholesterol), high blood pressure or hypertension, and
high blood glucose (also metabolic syndrome) are
preventable or manageable. Several prophylactic
therapies and screening of high-risk individuals also
offer potential benefits for the prevention of CHD
(Table 1).
0003Primary prevention of CHD is generally defined as
the modification of risk factors or prevention of the
development of these risk factors, with the aim of
delaying or preventing a first coronary event (angina
pectoris, myocardial infarction, or sudden death),
offers the greatest opportunity for reducing the burden
of CHD from a personal, economical, and global
aspect. The prime objective of primary prevention is
to reduce both short-term (< 10 years) and long-term
(> 10 years) risk. However, secondary prevention in-
cludes therapy or measures to minimize recurrent cor-
onary event (angina pectoris, history of myocardial
infarction, history of bypass graft or angioplasty) and
decrease mortality and morbidity in patients with es-
tablished CHD, which is not cost-effective in most
cases. The potential benefits of primary prevention
exceed those of secondary prevention, since 30%
of patients with first myocardial infarction survive
less than 3 months. The first CHD event may progress
to prolong permanent morbidity. Both primary and
secondary preventions share many common character-
istics (Figure 1). Therefore, the elements of both
CORONARY HEART DISEASE/Prevention 1669
primary and secondary preventions are addressed
simultaneously. Combining both primary and second-
ary prevention, the overall objective of CHD preven-
tion is to reduce the risk of initial or subsequent CHD
events, thereby reducing premature CHD-related mor-
bidity and mortality, and prolonging survival.
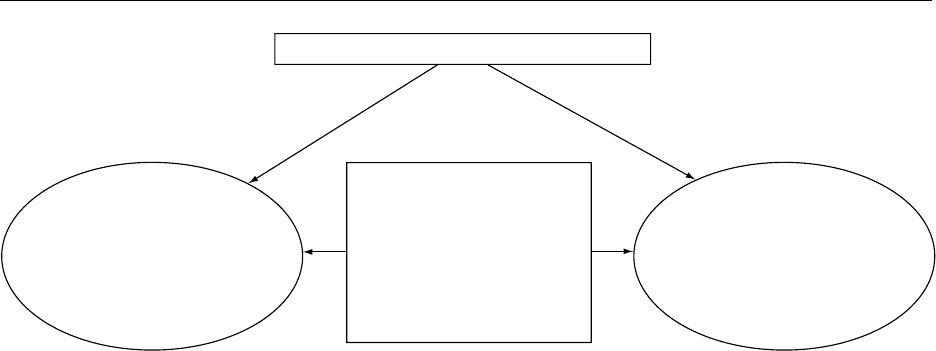
Primary and Secondary Preventive
Measures for CHD
Smoking
0004 Cigarette smoking is a convincing risk factor for
CHD, and cessation of smoking (including all forms
of tobacco) rapidly and significantly decreases the
risk for the development of CHD and CHD-related
mortality in a very cost-effective way. Smoking
cessation is a complex, multifactorial, and difficult
process. Simple brief counseling with a clear, firm,
positive, encouraging, and sympathetic attitude is
the first step in the management of smoking cessation.
Persistent smokers may require extended counsel-
ing, more than one session preferably, by a skilled
counselor or psychologist. Nicotine chewing gum or
transdermal nicotine replacement patches with a
progressively decreasing dosage can be helpful for
heavily addictive persons as an adjunct to counseling.
0005 Family support is very important in smoking cessa-
tion. Encouragement from a family or spouse is of
great help. ‘Smoke-free’ environments at home, res-
taurants, work sites, public transport vehicles, and
other public premises can greatly improve the atmos-
phere for smoking cessation attempts by smokers.
Diet
0006Diet is an important determinant for the development
of CHD by affecting the obesity, blood pressure, and
blood lipids. Therefore, it is crucial to maintain a
‘healthy diet,’ which constitutes (1) consumption of
six or more servings of whole-grain products with
25 g of fiber, especially soluble fiber; (2) consump-
tion of at least five servings of fruits and vegetables
(> 400 g per day); (3) limiting consumption of satur-
ated fat < 10% (preferably < 7%) of total daily cal-
ories, and cholesterol < 300 mg per day (preferably
< 200 mg per day); (4) consumption of polyunsatur-
ated fatty acids up to 10% of total daily calories; (5)
limiting salt intake to 6 g per day, the equivalent of
100 mmol of sodium per day; and (6) limiting alcohol
consumption to one or two standard drinks for men
per day and not more than one drink for women (a
pregnant woman should not drink) per day to prevent
or delay the development of CHD risk.
Overweight and Obesity
0007Patients who are overweight (body mass index
(BMI ¼kg m
2
) > 25 kg m
2
) or obese (BMI > 30 kg
m
2
), or with excess truncal or abdominal fat (waist
circumference > 102 cm in men and > 88 cm in
women), are at increased risk for CHD, because of
the adverse effects of fat on blood lipid levels, blood
tbl0001 Table 1 Prevention of coronary heart disease
Lifestylemodification Goals
Smoking cessation Encourage patient to stop smoking completely
Healthy diet 25 g of fiber, >400 g of fruits and vegetables; <30% fat, <10% saturated fat, poly- and monounsaturated
fat 10% each, <300 mg of cholesterol of daily calories; salt intake 6 g or less per day
Weight control Maintain a healthy BMI (18.9–24.9)
Physical activity 30–60 min aerobic activity four to six times a week
Risk factors Goal Recommendeddrugs
Blood lipid Statins
LDL cholesterol <130 mg dl
1
Total cholesterol <200 mg dl
1
Blood pressure Low-dose thiazide
Systolic 130–139 mmHg Diuretics
Diastolic 85–89 mmHg b-blockers
ACE inhibitors
Calcium antagonist
Prophylactic therapy Purpose
Aspirin (75–325 mg
per day)
For secondary prevention and maybe for primary prevention
ACE inhibitors For secondary prevention
Statins For both primary and secondary prevention
Folic acid For primary prevention
BMI, body mass index; LDL, low-density lipoprotein; ACE, angiotensin-converting enzyme.
1670 CORONARY HEART DISEASE/Prevention
pressure, and glucose tolerance. Prospective epidemi-
ological studies have shown a J-shaped association
between BMI and all-cause mortality among Western
populations. High-risk populations require profes-
sional advice on weight reduction.
0008 Successful weight reduction is not easy to manage,
often requiring long-term professional support and
encouragement, good motivation of the person, a cal-
orie-restricted lipid-lowering diet, and a suitable phys-
ical activity program. Realistic weight-reduction goals
should be based on short-term results and agreed be-
tween the physician and the patient. It is recommended
that a weight reduction of 0.5–1 kg per week is a
suitable rate until the target weight goal is achieved.
The National Heart, Lung, and Blood Institute, USA
has recommended that a person with BMI 27–35
should decrease their caloric intake by 300–500 kcal
per day, and a person with BMI > 35 should decrease
their caloric intake by 500–1000 kcal per day from
their diet to achieve a 10% weight loss in 6 months.
0009 There has been considerable concern about the
usage of drugs and their possible side-effects for
weight reduction. For example, sibutramine, a sym-
pathomimetic, reduces food intake but may cause
hypertension and tachycardia. Lipase inhibitor orli-
stat (Xenical) has significant effect on weight reduc-
tion but may cause severe gastrointestinal symptoms.
Weight loss is usually observed within 2 weeks of
initiation of therapy. However, researchers agree that
a reduction in caloric intake combined with regular
physical activity may be the most effective and safe
method in reducing excess body fat.
Physical Activity
0010 Prospective epidemiological studies have documented
that sedentary lifestyle is a strong predictor of CHD
risk, irrespective of other risk factors. Therefore, a
regular, suitable exercise program is recommended
for a sedentary person, since it has favorable effects
on body weight, blood pressure, blood lipids, insulin
sensitivity, and glucose tolerance. Epidemiological
studies have demonstrated strong evidence that aer-
obic exercise reduces the risk of CHD. Brisk walking,
jogging, cycling, mowing, swimming, aerobic dancing,
skipping, and other recreational sports that require
movement are good examples of aerobic exercise.
0011It is now recommended that everyone must perform
at least 30–60 min of physical exercise four to six times
a week. Generally, an exercise program includes a 5–
10-min warm-up by stretching and other gentle activ-
ity followed by 20–30 min endurance or aerobic
phase, and finally 5–10 min of a cool-down phase.
Physical exercise prescription (intensity and duration)
for patients with clinically established CHD must be
based on comprehensive clinical evaluation and
results of exercise testing. The Second Joint Task
Force of European and other Societies on Coronary
Prevention recommends that the intensity and dur-
ation of activity should initially be set low and grad-
ually increased according to the limits imposed by
exercise-induced symptoms. Patients recovering from
myocardial infarction and other cardiac events should
also be given advice about a suitable, gradually in-
creasing exercise program. In these patients, exercise
programs must be supervised, and ECG monitoring
should be used in the early stages.
Blood Lipids
0012CHD risk is best evaluated by measuring plasma
concentrations of total cholesterol, low-density
lipoprotein (LDL) cholesterol, and high-density lipo-
protein (HDL) cholesterol. Results from animal
experiments, epidemiological, and other studies con-
sistently demonstrate an independent, strong,
Prevention of Coronary Heart Disease
Prophylactic medications
(aspirin, β blockers,
statins, ACE inhibitors)
Secondary Prevention
Prophylactic medications
(aspirin, statins, folic
acid)
Screening for family
history
Primary Prevention
Modifiable Risk Factors
Smoking
Atherogenic diet
Overweight/obesity
Physical inactivity
Blood lipids
Metabolic syndrome
Type 2 diabetes
High blood pressure
fig0001 Figure 1 Shared preventable measures in primary and secondary prevention of coronary heart disease. ACE, angiotensin-
converting enzyme.
CORONARY HEART DISEASE/Prevention 1671
positive, and graded relationship between high total
cholesterol and elevated LDL cholesterol and the risk
of CHD development. Recently, several clinical trials
consistently showed that LDL-lowering therapy re-
duces the total mortality, CHD-related mortality,
major coronary events, and coronary artery proced-
ures in persons with established CHD and persons
with CHD risk equivalent (i.e., diabetes). Based on
the results of prospective epidemiological and clinical
trials with both angiographic and clinical end points,
an LDL cholesterol level of < 100 mg dl
1
is set as the
goal of therapy in secondary prevention. Two basic
components of LDL-lowering therapy are ‘thera-
peutic life changes’ (Table 2) and drug therapy.
0013 Therapeutic Life Changes (TLC) The Third Report
of the National Cholesterol Education Program
(NCEP) Expert Panel, USA, 2001, recommends
a multifactoral life style approach that includes:
(1) reduction of saturated fat intakes (< 7% of total
calories) and cholesterol (< 200 mg per day), (2) con-
sumption of plant sterols (2 g per day) and soluble
fiber (10–25 g per day), (3) weight reduction, and (4)
increased physical activity.
0014 Drug Therapy In order to attain the goal of LDL
cholesterol levels of < 100 mg dl
1
, many persons
with CHD and CHD risk equivalents will need LDL
cholesterol-lowering drug therapy in addition to
TLC. Low-density lipoprotein cholesterol should be
measured on admission or within 24 h in order to
decide the need for drug treatment. Currently, four
major classes of drugs are widely used to lower LDL
cholesterol effectively: hepatic hydroxymethylglu-
taryl coenzyme A (HMG CoA) reductase inhibitors
(statins), bile acid-binding resins, fibric acid deriva-
tives, and nicotinic acid. Recently, many compre-
hensive clinical trials with statins have robustly
documented that this class of drugs is the most effect-
ive in lowering LDL cholesterol from angiographical
and clinical end points. Statins also have a better
safety profile compared with other classes of drugs.
Therefore, at present, the statins are the first line of
drugs used to lower total and LDL cholesterol levels.
In some special conditions, like familial hypercholes-
terolemia, a combination of drugs (statin and resin or
statin, resin, nicotinic acid) may be used.
Blood Pressure
0015 A large number of epidemiological studies have demon-
strated that elevated arterial blood pressure is a risk
factor for CHD. The goal for blood pressure reduction
is to maintain systolic blood pressure (SBP) < 140 mmHg
and diastolic blood pressure (DBP) < 90 mmHg. The
goal can be achieved by nonpharmacological treatment
(lifestyle modification) alone or in combination with
pharmacological therapy.
0016Lifestyle modifications Several randomized clinical
trials have evaluated the effectiveness of lifestyle inter-
ventions on managing mildly elevated blood pressure
in a cost-effective way. The essential features of life-
style modifications are to: (1) maintain a healthy
weight or reduction of excess body weight based on
BMI; (2) achieve a moderate level of physical fitness
by 30–45 min of aerobic physical activity in most days
of the week; (3) reduce salt (sodium) intake moder-
ately (100 mmol per day) and not to exceed total salt
intake of 6 g per day (however, results from the meta-
analysis of randomized clinical trials presently do not
recommend a restriction of salt intake for the normo-
tensive population); (4) increase the intakes of potas-
sium (60–90 mmol per day) preferably from fruits and
vegetables; and (5) limit alcohol consumption to no
more than two standard drinks for men and one for
women per day. Table 3 demonstrates the elements of
lifestyle modification or nonpharmacological treat-
ment for elevated blood pressure.
0017Pharmacological treatment Several large-scale,
multicenter, randomized, controlled trials have cred-
ibly demonstrated that antihypertensive medications
lower CHD-related morbidity and mortality and
all-cause mortality. The decision to commence
pharmacological treatment relies on the degree of
blood pressure elevation, presence of target organ
damage (e.g., heart disease, nephropathy, peripheral
arterial disease, and retinopathy), presence of clinical
cardiovascular disease and other risk factors, or
conditions such as diabetes. A general agreement,
however, is that an individual with a ‘high normal
BP’ (130–139/85–89 mmHg) and with target organ
disease and/or diabetes should be treated with
tbl0002Table 2 Components of therapeutic life changes
a
Weight reduction Balance energy intake and
expenditure to maintain a healthy
weight (BMI 18.5–24.9)
Increased physical activity 30–60 min aerobic exercise most
days of the week
Healthy diet
Saturated fat <7% of total calories
Polyunsaturated fat 10% of total calories
Monounsaturated fat 20% of total calories
Total fat 25–35% of total calories
Carbohydrate 50–60% of total calories
Fiber 20–30 g per day
Protein *15% of total calories
Cholesterol <200 mg per day
a
Adapted from the Third Report of the National Cholesterol Education
Program (NCEP), USA, 2001.
BMI, body mass index.
1672 CORONARY HEART DISEASE/Prevention
antihypertensive medication after a trial of lifestyle
modification. Drug treatment begins with monother-
apy, low doses followed by slow titration to achieve
24-h control with once-daily medication depending
on the patient’s age, needs, and response, as well as
economic condition. The most commonly used anti-
hypertensive agents: thiazide diuretics in low dosage,
b-blockers (especially if angina is present), angioten-
sin-converting enzymes (ACE) inhibitors, calcium an-
tagonists, a-blockers, and angiotensin II receptor
blockers. Most experts prefer low-dose thiazide diur-
etics or b-blockers as a first line of antihypertensive
agents, unless contraindicated. Other preferred
choices for initial therapy are: b-blockers for hyper-
tensives with uncomplicated myocardial infarction;
ACE inhibitors for individuals with CHD and
decreased ejection fraction, with left ventricular func-
tion, diabetes with proteinuria; and thiazide,
b-blockers, or calcium antagonist (calcium channel
blocker) for isolated systolic hypertension. Isolated
systolic hypertension is a CHD risk factor, especially
for the elderly, and should be managed properly.
0018 The antihypertensive agents are not free of adverse
effects. However, the use of combinations of low
doses of two agents from different classes have been
shown to potentiate the effect of other agents without
incurring any adverse effects.
Blood Glucose
0019 Data from large numbers of epidemiological and (in-
cluding the Framingham Study) pathological studies
document hyperglycemia as an independent risk
factor for CHD. Persons with both type 1 and type 2
diabetes and diabetic women are at increased risk for
developing CHD than nondiabetics and diabetic men,
respectively. The underlying mechanisms for this
remain to be answered. In addition to hyperglycemia,
diabetics frequently have other classical risk factors
for CHD – hypertension, lack of physical activity, low
levels of HDL cholesterol, and hypertriglyceridemia–
that intensify the risk of developing CHD events.
0020 The effects of glycemic control among diabetics and
alteration in CHD risk have not been appraised con-
clusively. Results from randomized controlled trials
show that prudent insulin therapy retards the occur-
rence of microvascular events and a nonsignificant
reduction of macrovascular events in patients with
type 1 diabetes. To date, no clinical or epidemiological
evidence of the role of blood glucose control in
reducing CHD events significantly in patients with
type 2 diabetes has been documented. However,
there is general agreement that control of blood
glucose (hemoglobin A
1c
< 7.0%) among type 2 dia-
betics may minimize CHD complications. In order to
achieve an acceptable level of hemoglobin A
1c
, type 2
diabetics often need professional dietary advice (redu-
cing total calorie and fat intake), reduction of over-
weight or obesity (5–9 kg irrespective of starting
weight), and increased level of physical activity as a
first line of management. Frequent aerobic exercise (at
least 30 min most days of the week) also facilitates
blood glucose control and weight control. Oral hypo-
glycemic agents come as a second line of therapy when
a desirable hemoglobin A
1c
cannot be achieved with
lifestyle modification alone.
0021Control of blood glucose also maintains normal
plasma lipid levels in patients with type 1 diabetes
without nephropathy. Diabetic dyslipidemia (ele-
vated triglycerides, low HDL cholesterol), which is
more pronounced among type 2 diabetics, may be
corrected by normalizing blood glucose using oral
hypoglycemic agents. The primary goal of LDL chol-
esterol < 100 mg dl
1
can be achieved by moderate
caloric restriction (250–500 cal less than the average
daily intake), 30% fat, < 7% saturated fat, and
< 300 mg of cholesterol per day. Cholesterol-lowering
therapy is recommended if dietary modification fails.
The primary goal for blood pressure in diabetics is to
maintain blood pressure < 130/85 mmHg. Moderate
weight loss has also been shown to reduce dyslipid-
emia and hypertension among diabetics. Smoking
cessation is obligatory. Guidelines to reduce CHD
for diabetics are shown in Table 4.
Metabolic Syndrome
0022There is mounting recognition that many persons
have a collection of multiple major risk factors and
tbl0003 Table 3 Lifestyle modifications for high blood pressure
Lose weight if overweight or obese
Increase aerobic physical activity 30–45 min for most days of the
week
Stop smoking completely
Limit sodium intake to 6 g or less per day
Maintain adequate intake of dietary potassium
Limit alcohol intake to one or two drinks per day
tbl0004Table 4 Guidelines to reduce coronary heart disease in
patients with diabetes mellitus
Risk factors Recommendations
Smoking Complete cessation
Physical activity At least 30 min three or four times per
week
Weight reduction 5–9 kg irrespective of starting weight
Hemoglobin A
1c
Target: <7%
Fasting blood glucose Target: 80–120 mg dl
1
LDL cholesterol Target: <100 mg dl
1
Calorie restriction 250–500 kcal less than average daily
intake
Blood pressure Target: <130/85 mmHg
CORONARY HEART DISEASE/Prevention 1673

emerging risk factors for CHD; a cluster of these
conditions is known as a metabolic syndrome charac-
terized by abdominal obesity, ‘lipid triad’ (elevated
serum triglycerides, low HDL cholesterol, and high
LDL cholesterol) hypertension, insulin resistance,
and other thrombogenic risk factors. Primary preven-
tion is mainly focused on reducing body weight
through diet and by increasing physical activity. Diet-
ary modification and physical activity also effectively
normalize dyslipidemia.
Prophylactic Therapies
0023 To prevent the aforementioned classical risk factors
and other thrombogenic factors that play pivotal roles
in the CHD events, a great deal of emphasis is placed
using several prophylactic drug therapies. Likewise,
increased consumption of polyunsaturated fatty acids
(o-3 and o-6) may be used as antithrombic agents.
0024 Aspirin Compelling evidence from randomized
studies insinuates that a low dose of aspirin or acetyl-
salicylic acid (between 75 and 325 mg) daily may
considerably reduce subsequent myocardial infarction
and all-cause mortality among patients with postmyo-
cardial infarction. With regard to primary prevention,
the use of aspirin and the balance between benefits and
hazards is not lucid. However, a recent meta-analysis
has suggested that aspirin may be used as a primary
prevention agent but requires formal accurate estima-
tion of absolute CHD event risk. A maintenance dose
of 75 mg of aspirin is recommended as a secondary
prevention for all postmyocardial infarctive patients if
not contraindicated.
0025 b-blockers Results from the meta-analysis indicate
that b-blockers substantially decrease all-cause mor-
tality in patients following myocardial infarction.
Therefore, like aspirin therapy, b-blockers should be
reckoned for patients following myocardial infarc-
tion if not contraindicated.
0026 ACE inhibitors ACE inhibitors significantly reduce
all-cause mortality and the risk of progression of
heart failure among patients following myocardial
infarction and with chronic left ventricular systolic
dysfunction.
0027 Statins Although TLC is considered as the basis of
prevention to lower the high total cholesterol and
elevated LDL cholesterol, recently, several trials with
statins have documented unambiguously that statins
may be used as a method for primary prevention with-
out any substantial side-effects. Recent pharmaco-
economic analyses indicate that statin therapy may
be highly cost-effective in secondary prevention and
moderately so in primary prevention. However, the
cost-effectiveness of statins as a primary prevention
needs to be evaluated from a global perspective.
0028Estrogen Abundant observational studies strongly
and consistently attest that postmenopausal estrogen
replacement therapy (ERT) may protect against
CHD. However, recent, multicenter, randomized,
placebo-controlled secondary prevention trials have
negated this finding and documented that ERT may
increase the risk of venous thromboembolism in post-
menopausal women with CHD. Therefore, ERT is
not recommended for secondary prevention of CHD
for the postmenopausal women. The use of ERT may
be effective as a primary prevention of CHD. None
the less, ERT may be appropriate for postmenopausal
women to continue when they are already receiving
this treatment.
0029Folic acid A high level of total plasma homocysteine
(> 15 mmol l
1
) is considered as a notable risk factor
for CHD based on epidemiological studies. High
levels of homocysteine may be acquired, because of
a deficiency of folic acid, or congenital, because
of genetic mutation of a thermolabile variant of the
methylenetetrahydrofolate reductase gene. Supple-
mentation with folic acid (0.5–5.0 mg) reliably and
effectively reverses the hyperhomocysteinemia.
Screening
0030First-degree relatives (parents, siblings, and descend-
ants and other close relatives) of the patient suspected
of having familial hypercholesterolemia, or other in-
herited genetic lipid disorder, or individual with pre-
mature CHD (men < 55 years and women < 65 years)
should be regularly screened for risk factors as they
are at increased risk for CHD.
Conclusion
0031Prevention of coronary heart disease is a global public
health challenge. Given the unique and wide array of
the determinants of health (access to quality health-
care, health policies and interventions, physical and
social environments, and individual behavior and
biology) in the different geographic areas of the
world, the orderliness of preventive care for CHD
will vary from one country to another. Therefore, it
would not be pragmatic to define the aforementioned
CHD prevention as a sole model; rather, the universal
standards of prevention should be ensued and exer-
cised. The implementation of these recommendations
and emerging scientific knowledge in view of CHD
prevention should be incorporated in a person’s life-
style as well as in a healthcare provider’s professional
care. In the near future, the Human Genome Project
1674 CORONARY HEART DISEASE/Prevention

will also be able to explicate the genetic factors that
predispose to CHD.
See also: Coronary Heart Disease: Etiology and Risk
Factor; Dietary Requirements of Adults; Exercise:
Metabolic Requirements; Fats: Digestion, Absorption,
and Transport; Glucose: Maintenance of Blood Glucose
Level; Obesity: Etiology and Diagnosis; Slimming:
Metabolic Conseqences of Slimming Diets and Weight
Maintenance; Smoking, Diet, and Health
Further Reading
Assmann G, Carmen R, Cullen P et al. for the International
Task Force for the Prevention of Coronary Heart Disease
(1999) Coronary heart disease: reducing the risk. A
worldwide view. Circulation 100: 1930–1938.
Assmann G, Cullen P, Jossa F, Lewis B and Mancini M for
the International Task Force for the Prevention of Cor-
onary Heart Disease (1999) Coronary heart disease:
reducing the risk. The scientific background to primary
and secondary prevention of coronary heart disease.
A worldwide view. Arteriosclerosis, Thrombosis and
Vascular Biology 19: 1819–1824.
Barbour M (2000) Hormone replacement therapy should
not be used as secondary prevention of coronary heat
disease. Pharmacotherapy 20: 1021–1027.
Gotto A (1999) Lipid-lowering therapy for the primary
prevention of coronary heart disease. Journal of the
American College of Cardiology 33: 2078–2082.
Grundy S, Balady G, Criqui M et al. (1997) Guide to
primary prevention of cardiovascular diseases. A state-
ment for healthcare professionals from the Task Force
on risk reduction. Circulation 95: 2329–2331.
Grundy S, Balady G, Criqui M et al. (1998) Primary pre-
vention of coronary heart disease: guidance from Fra-
mingham. A statement for healthcare professionals from
the AHA Task Force on risk reduction. Circulation 97:
1876–1887.
Joint British recommendations on prevention of coronary
heart disease in clinical practice: summary (2000) British
Medical Journal 320: 705–708.
Krauss R, Eckel R, Howard B et al.(2000)AHADietary
Guidelines. Revision 2000: A statement for healthcare
professionals from the Nutrition Committee of the Ameri-
can Heart Association. Circulation 108: 2284–2299.
Liesbson P and Amsterdam E (1999) Prevention of coron-
ary heart disease. Part I. Primary prevention. Disease-a-
month 45: 500–571.
Liesbson P and Amsterdam E (2000) Prevention of coron-
ary heart disease. Part II. Secondary prevention, detec-
tion of subclinical disease, and emerging risk factors.
Disease-a-month 46: 4–123.
National Heart, Lung, and Blood Institute (1997) The Sixth
Report of the Joint National Committee on Prevention,
Detection, Evaluation, and Treatment of High Blood
Pressure. NIH Publication No. 98-4080. Bethesda,
MD: National Heart, Lung, and Blood Institute.
National Heart, Lung, and Blood Institute (2001) Third
Report of the National Cholesterol Education Program
(NCEP) Expert Panel on Detection, Evaluation, and
Treatment of High Blood Cholesterol in Adults (Adult
Treatment Panel III) Executive Summary. NIH Publica-
tion No. 01-3670. Bethesda, MD: National Heart, Lung,
and Blood Institute.
National Heart, Lung, and Blood Institute in cooperation
with The National Institute of Diabetes and Digestive
and Kidney Diseases (1998) Clinical Guidelines on the
Identification, Evaluation, and Treatment of Overweight
and Obesity in Adults. The Evidence Report. NIH Pub-
lication No. 98-4083. Bethesda, MD: National Heart,
Lung, and Blood Institute.
Ramsay L, Williams B, Johnston G et al. (1999) British
Hypertension Society guidelines for hypertension man-
agement 1999: summary. British Medical Journal 319:
630–635.
WHO (1996) Hypertension control. Report of a WHO
Expert Committee. World Health Organization Tech-
nical Report Series 862: 1–83.
Wood D, Backer G, Faergeman O et al. (1998) Prevention
of coronary heart disease in clinical practice: Recom-
mendations of the Second Joint Task Force of European
and other Societies on coronary prevention. Atheroscler-
osis 140: 199–270.
CORROSION CHEMISTRY
P Marsal, Thionville, France
This article is reproduced from Encyclopaedia of Food Science,
Food Technology and Nutrition, Copyright 1993, Academic Press.
Background
0001 For most people, the word ‘corrosion’ carries the image
of rust specific to iron-containing metals, surmising
that only iron is subject to this phenomenon. In
fact, corrosion is the general term for the damage
and destruction of most man-made metallic mater-
ials. This destructive force of corrosion has always
existed but has grown in importance only in the
modern era due to the advancement of civilization
and technology.
0002Corrosion may be considered as the deterioration
of metals and alloys made by humans, which tend to
return to their original state; thus, ‘rust’ is the natural
state of iron, as steel is obtained from iron oxides
CORROSION CHEMISTRY 1675