Markovchick Vincent J., Pons Peter T., Bakes Katherine M.(ed.) Emergency medicine secrets. 5th ed
Подождите немного. Документ загружается.

Chapter 15 HEADACHE98
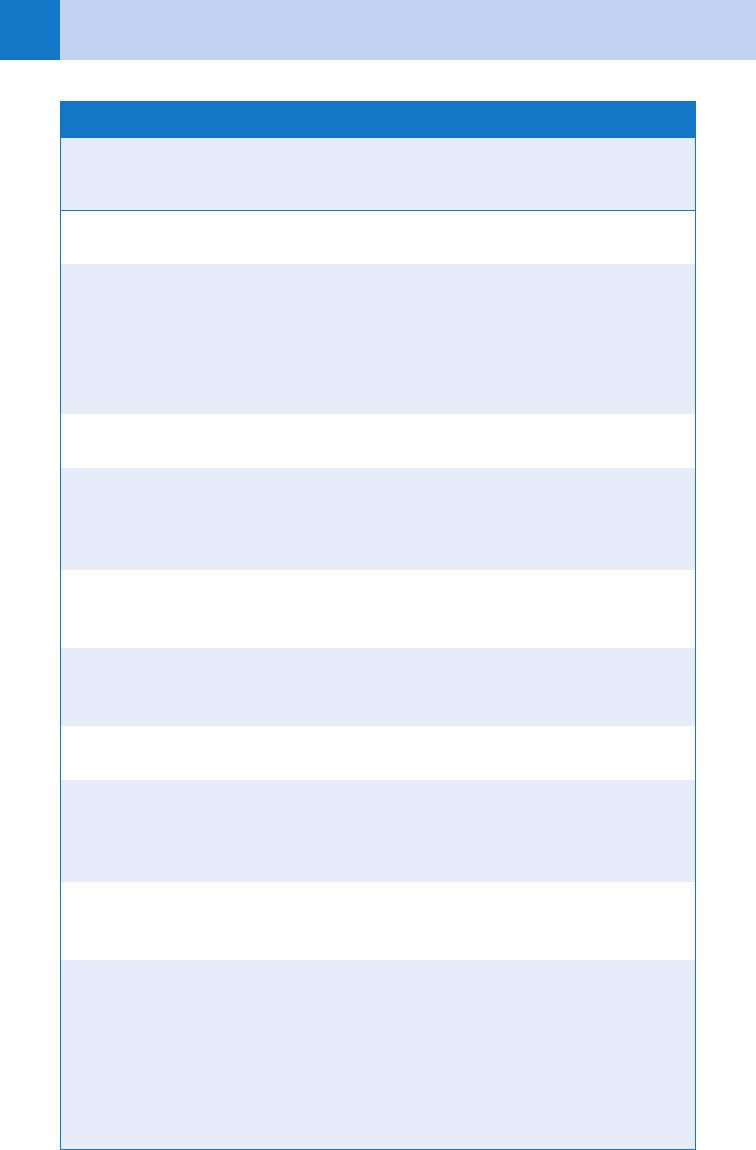
CT, computed tomography; CVST, cerebral venous sinus thrombosis; ESR, erythrocyte sedimentation rate;
LP, lumbar puncture; SAH, subarachnoid hemorrhage.
Headache Characteristics Differential Diagnosis
Possible Work-Up
(beyond history and
physical examination)
Headache begins after age 50 Mass lesion, temporal
arteritis, stroke
ESR, neuroimaging
Sudden onset of headache SAH, pituitary apoplexy,
hemorrhage into a mass
lesion or vascular malforma-
tion, mass lesion (especially
posterior fossa), vascular
dissection and CVST
Neuroimaging, LP if CT is
negative
Headaches increasing in
frequency and severity
Mass lesion, subdural hema-
toma, medication overuse
Neuroimaging, drug screen
New-onset headache in
patient who has risk factors
for HIV, cancer
Meningitis (chronic or carci-
nomatous), brain abscess
(including toxoplasmosis),
metastasis
Neuroimaging, LP if
neuroimaging is negative
Headache with fever,
meningismus, rash, or
altered mentation
Meningitis, encephalitis, Lyme
disease, systemic infection,
collagen vascular disease
Neuroimaging, LP, serology
Focal neurologic symptoms
or signs of disease (other
than typical aura)
Mass lesion, vascular
malformation, stroke,
Neuroimaging
Papilledema Mass lesion, pseudotumor,
meningitis
Neuroimaging, LP
Headache that worsens with
standing up
Spontaneous intracranial
hypotension, postdural
puncture headache
(if following an LP)
For the former—LP with
opening pressure, MRI
Headache with ocular
or visual symptoms
Pseudotumor cerebri, acute
narrow angle glaucoma,
temporal arteritis
LP for pseudotumor,
tonometry for glaucoma, ESR
and biopsy for arteritis
Headache after head trauma Intracranial hemorrhage,
subdural hematoma, epidural
hematomas, post-traumatic
headache
Neuroimaging of brain, and
possibly cervical spine
TABLE 15-1. RED FLAGS IN PATIENTS WITH HEADACHES

Chapter 15 HEADACHE 99
headaches, requires close evaluation. A sudden, severe onset, commonly described as “the
worst headache I have ever had,” is classic for a SAH. Associated fever requires evaluation for
infection, tumor, or drug use. A careful history is usually the diagnostic element that helps
decide which headaches to evaluate beyond history and physical examination. Any headache
associated with new focal neurologic signs should be investigated.
6. Why are age and context important in the history of a patient with a
headache?
Migraines most commonly begin before age 30. Tension-type headaches usually begin before
age 50. Headaches that begin after age 55 are much more likely to have a serious cause, such
as a mass lesion, giant cell arteritis, or cerebrovascular disease. Headaches occurring in the
peripartum period may be caused by cortical vein or cerebral venous sinus thrombosis. In
general, if a patient has a long history of previous similar attacks, a serious cause is less
likely. If a patient reports numerous identical attacks treated at home, it is important to
understand why this particular episode led to an ED visit.
7. What questions in the history are most important to ask in evaluating a
patient with a headache?
a. Do you get headaches frequently? Have you ever needed to go to an ED for one? Is this
current headache the same as prior ones that you have had? If not, how does it differ?
These questions are aimed at assessing the quality of pain.
b. How bad is this headache? Have you had headaches this severe in the past? These
questions assess the severity.
c. Did the headache start suddenly or gradually? If sudden, what were you doing at the time it
began? These questions go after the onset.
d. What symptoms accompany the headache? Did you vomit? Was there any fainting, seizure,
photophobia, or double vision? Did you have these same associated symptoms with prior
episodes or not? (for patients with a prior history of headache). These associated
symptoms can suggest secondary causes. For example, a patient with migraines, who has
never had photophobia or vomiting with prior episodes, and now does, ought to undergo
further evaluation. On the other hand, if this headache is similar to prior episodes, it is
most likely due to that same etiology.
e. Have you had any recent head trauma? Note that this includes even minor trauma for elderly
patients, who are more susceptible to chronic or delayed presentation subdural hematomas.
f. What treatment have you used at home and was it helpful? This can also help if a headache has
responded in the past the same as it does for the current visit. But be careful; see Question 13.
8. Does the physical examination add any information?
The history often leads to the correct diagnosis or at least a short list of possible diagnoses.
The physical findings may support or refute those diagnoses or change the likelihood of
various possibilities. Fever may reflect infection. Hypertension may cause headache, be a sign
that there is increased intracranial pressure, or simply be caused by the headache or anxiety
of an ED visit. Abnormal pulse or respiration may be due to infection or toxins.
n
Palpate the temporal arteries, sinuses (see Question 21), temporo-mandibular joints, and
the scalp for tenderness.
n
Examine the fundi for papilledema and spontaneous venous pulsations.
n
Check for nuchal rigidity and photophobia.
n
Perform a neurologic examination as indicated by the patient’s history and general physical
examination.
9. What is the sensitivity of a noncontrast, head computed tomography (CT) for
detection of a SAH?
Even with advances in imaging technology, only approximately 90% to 95% of SAHs are
detected on CT scans of the head. This number is higher in patients scanned within the first
12 to 24 hours but declines rapidly with time from the onset. This is due to cerebrospinal fluid

Chapter 15 HEADACHE100
(CSF) circulation. A lumbar puncture (LP) and CSF analysis will rule out SAH in a patient with
a normal CT scan with close to 100% sensitivity.
10. What are the CSF findings in a SAH?
As with CT, the findings on LP evolve with time. Even in the first hours after SAH, the large
numbers of red blood cells are found in the lumbar theca. Over days, these numbers fall due to the
circulation of CSF and the breakdown of the red blood cells and hemoglobin. Thus, red cells are
nearly always present early, and xanthochromia (the yellow color due to hemoglobin catabolism) is
almost always found later (until about 2 weeks post-SAH, depending on the method one uses for
detection). Measuring the opening pressure can help too because it is often elevated in SAH.
11. How do I differentiate between a traumatic tap and a SAH?
There are many tests, but none is perfect. Clearing of blood from earlier- to later-collected
tubes is commonly used and is helpful, but unless the last tube contains zero cells, SAH is
still a possibility. Wasting a few milliliters of CSF between the first and last tubes facilitates
this. An elevated opening pressure suggests a SAH and not a traumatic tap. Xanthochromia is
almost always present if blood has been in the CSF for 12 hours or longer and confirms an
intracranial bleed. As with CT, one must factor in the timing of the LP (with respect to the
onset of the headache) in interpreting the LP results.
12. If the CT and LP are both normal, do I need to pursue the diagnosis of SAH
with some form of angiography?
The data strongly support, and American College of Emergency Physicians (ACEP) clinical policy
recommends, stopping the work-up if both tests are negative. However, this assumes that SAH is
the major consideration. Rarely, an unruptured aneurysm that is acutely expanding, dissecting, or
thrombosing can cause an acute headache. Furthermore, there are other causes of acute, severe,
sudden-onset headache associated with a normal CT and LP. These include (see Table 15-2):
n
Pituitary apoplexy.
n
Cervical artery dissections.
n
Cerebral venous sinus thrombosis.
n
Posterior reversible encephalopathy syndrome (related to eclampsia).
n
Acute stroke (especially posterior fossa).
13. What are migraine headaches?
Although people may refer to any severe headache as a migraine, a migraine is a specific type of
headache. Migraines tend to be familial and affect women twice as often as men. The underlying
pathophysiology is thought to be vasogenic inflammation. The first headache usually occurs in an
individual in the teens or twenties. Headaches typically are described as unilateral, severe,
throbbing, and are commonly associated with photophobia and nausea. The headache may also
be non-throbbing. Variations on all of the symptoms occur, but each patient tends to experience a
similar constellation of symptoms with each headache. Patients who experience an aura will often
have positive symptoms (e.g., flashing lights or zig-zag patterns in vision, tingling of the face or
arm or shaking of a limb) as opposed to negative symptoms (e.g., absence of vision, anesthesia
or absence of movement of a limb), which are more common with brain ischemia or infarction.
Occasional migraine patients will have weakness, however. Patients will often use the word
migraine to describe any severe headache, so if a patient says they have a history of migraines,
get more details about their duration, frequency, and what work-up has been done. Make sure
that their headaches are truly migraines.
14. If a headache patient improves or the pain completely resolves with
sumatriptan or ketorolac, does that mean that the diagnosis is migraine
(or some other primary headache cause)?
The answer to this question is an emphatic “no.” Because the final common pathway for most
pain in the head is limited, and vasogenic inflammation probably plays a role, the response to
any analgesic or antimigraine medication is of no etiologic significance. This includes triptans,
Chapter 15 HEADACHE 101
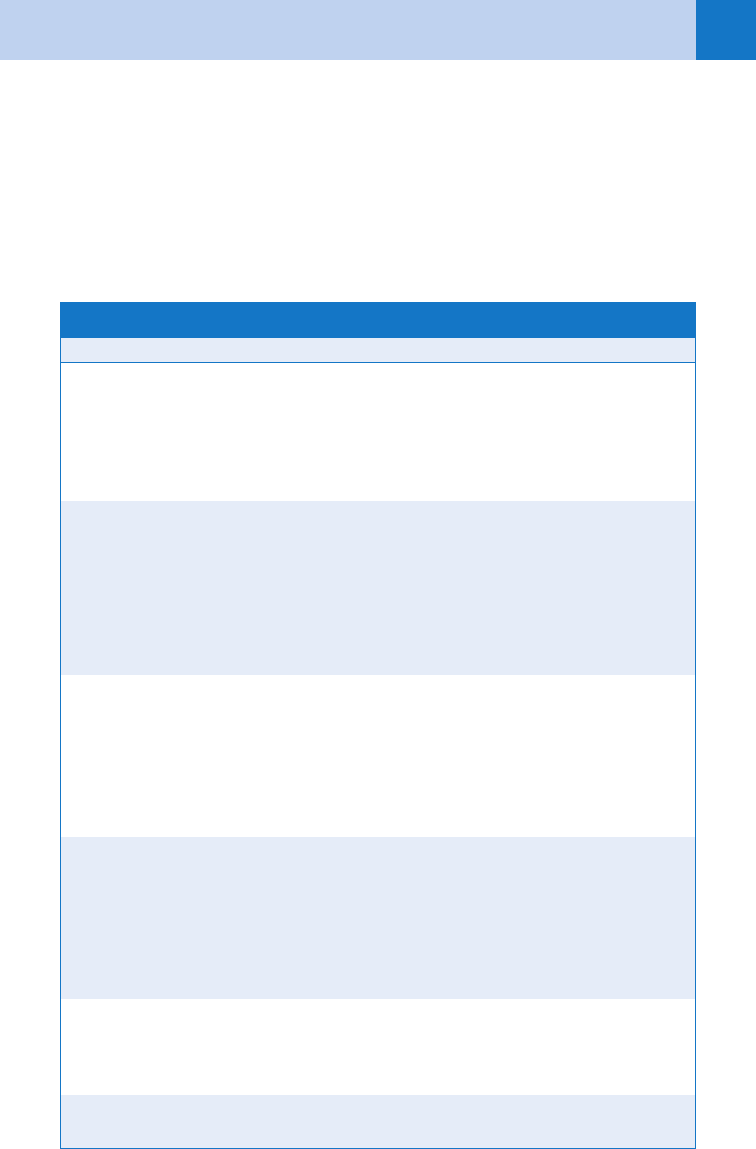
CT, computed tomography; CVA, cerebrovascular accident; LP, lumbar puncture; MRI, magnetic resonance
imaging.
Pathologic Process Clinical Characteristics Work-Up
Subarachnoid
hemorrhage
Headache worst of life CT; if normal, do LP
Headache abrupt, effort related
Normal neurologic examination to focal
deficit or coma
Cervical artery
dissections
History of trauma, Marfan syndrome,
collagen disorders
Headache is ipsilateral
Carotid: neck or head pain, Horner
syndrome, stroke
Vertebral: occipital-nuchal pain and
posterior circulation stroke
Magnetic resonance or
CT angiography
Vascular ultrasound and
conventional angiography
Intracerebral
hemorrhage
History of hypertension CT
History of brain tumor
Severe headache with signs of elevated
intracranial pressure and depressed
mental status
Cerebral venous
thrombosis (superior
sagittal sinus or
transverse sinus)
Postpartum, hypercoagulable states,
and abrupt, dull, constant headache
MRI, magnetic resonance
venography, or conventional
angiography; CT angiography
shows promise
Sixth nerve palsy, seizures
Signs of raised intracranial pressure
Pituitary apoplexy Abrupt severe headache, progressive
visual loss with subsequent signs of
pituitary insufficiency
CT or MRI with coronal views of
the pituitary
TABLE 15-2. DIFFERENTIAL DIAGNOSIS AND WORK-UP FOR ACUTE, SEVERE HEADACHE
which have been documented to improve the headaches of patients with SAH and cervical
artery dissections.
15. What specific entities must be considered in patients with a headache and a
history of cancer or immunosuppression?
In a patient with a history of cancer, consider brain metastases, or infections related to
immunosuppression. In patients who are HIV positive, especially if they have low CD4
counts or high viral loads, opportunistic infections, such as cryptococcal meningitis or

Chapter 15 HEADACHE102
toxoplasmosis, brain abscess, and primary lymphoma of the central nervous system, should
be considered.
16. What specific diagnosis should be considered in older patients with a new
onset headache and general malaise or other systemic symptoms?
Temporal arteritis is a systemic arterial vasculitis that is rare before age 50 and dramatically
increases in incidence afterward. Also known as giant cell arteritis, temporal arteritis should be
suspected in any patient older than age 50 who has a new onset headache or a change in an
established pattern of headache. It is associated with localized scalp tenderness (anywhere in the
scalp), malaise, myalgias, arthralgias, polymyalgia rheumatica, low-grade fevers, or other
constitutional symptoms. Untreated, temporal arteritis can result in blindness or stroke. Jaw
claudication, if present, is strongly suggestive of the disorder. Erythrocyte sedimentation rate
(ESR) is usually greater than 50 mm/hour, and biopsy is required to establish the diagnosis.
Treatment should be initiated in the ED, based on the clinical presumption and results of the ESR
and not delayed by biopsy. The initial doses of prednisone range from 60 to 80 mg daily. Finally,
because primary headaches start less commonly after the age of 50, many of the other serious
etiologies become more common in this age group, conditions such as stroke and tumors.
17. What is a sentinel bleed?
Up to 50% of patients with aneurysmal SAH will have experienced a warning or sentinel hemorrhage
before their catastrophic bleed. These small hemorrhages occur days to months before the major
event. These events are still characterized by abrupt onset of severe, unusual headache and, if
worked up with CT and LP, should be diagnosable in the vast majority of cases. Note that these
headaches resolve over days to weeks because of the circulation of CSF mentioned previously.
Unfortunately, these episodes are often not worked up and are misdiagnosed as migraine, sinusitis,
or tension-type headache, however, and the patients are discharged from medical care.
18. How do I treat a migraine headache?
Patients who are unable to control their headache at home often present to the ED for better
pain control or supportive therapy. The choice of treatment is based on case presentation,
prior medications used, time elapsed since onset, patient’s prior response to therapy,
existence of comorbid conditions, and severity of the current attack. Narcotics should be used
as a last resort (Table 15-3).
19. How are cluster headaches different from migraines? How are they treated?
These are nonfamilial headaches predominantly affecting men. Excruciating, unilateral pain
lasting 30 to 90 minutes occurs multiple times a day for weeks, followed by a pain-free
interval. During the attacks, autonomic signs of rhinorrhea and lacrimation frequently
occur ipsilateral to the headache. Attacks may be induced by smoking or alcohol. Oxygen
sometimes relieves 90% of cluster headaches within 15 minutes. Other treatments include
corticosteroids, calcium channel blockers, lithium, intranasal lidocaine, and methysergide.
20. How do I treat tension headaches?
If the diagnosis is secure, treatment starts with reassurance and education. Because these
headaches are usually chronic, they should be treated with nonaddictive analgesics.
Biofeedback and acupuncture may be beneficial. All patients with this diagnosis should be
screened for mood disorders because depression is a common cause of tension headaches.
21. Which toxin may bring in entire families complaining of headache?
Carbon monoxide poisoning. See Chapter 72.
22. Does sinusitis commonly cause headache? If a CT scan shows sinusitis, is
that the likely cause of a patient’s headache?
Acute bacterial sinusitis can certainly cause headache, but headache from sinusitis is not
nearly as common as some patients and doctors think. Patients will often use the term sinus
headache just as inaccurately as they use the term migraine. When sinusitis causes headache,
Chapter 15 HEADACHE 103
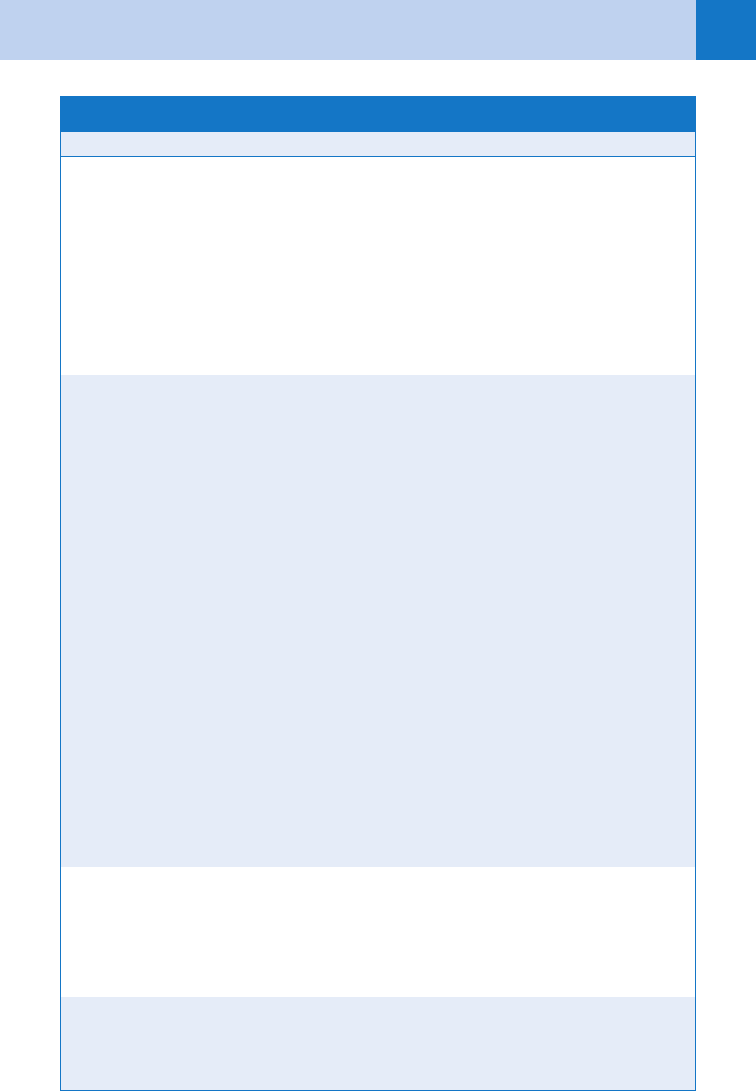
CAD, coronary artery disease; GI, gastrointestinal; HTN, hypertension; IM, intramuscularly; IV, intravenously;
PVD, peripheral vascular disease; SQ, subcutaneously.
*Assumes average-size adult patient.
Medication Dose and Route* Comments
Mild to moderate
Acetaminophen 500–1000 mg Avoid in patients with liver disease
Aspirin 650–1000 mg GI upset
Ibuprofen 600–800 mg GI upset
Naproxen sodium 275–550 mg GI upset
Indomethacin 50 mg rectal suppository
Moderate to severe
Dihydroergotamine 1 mg IV or IM May be repeated in 1 hour but not if
triptans used already
Contraindicated in HTN, PVD, CAD,
and pregnancy
Sumatriptan 6 mg SQ May be repeated in 1 hour but not if
ergots used already
Contraindicated in HTN, PVD, CAD,
and pregnancy
Metoclopramide 10 mg IV or IM Sedation and dystonic reaction
Prochlorperazine 10 mg IV or IM Sedation and dystonic reaction
Ketorolac 30–60 mg IM or 15–30 mg IV GI upset; caution in elderly and
patients at risk for renal failure
Morphine sulfate 0.1 mg/kg Opioids should be used as last resort
Hydromorphone 0.5–2 mg IV (note: 1 mg
hydromorphone 5 8–10 mg
of morphine)
Opioids should be used as last resort
Butorphanol 2 mg IV Opioids less efficacious than other
medications
Refractory attack, status migrainosus
Dihydroergotamine 1 mg IV Use in conjunction with antiemetic
Steroids Various regimens Controversial; based on anecdotal
evidence
TABLE 15-3. SELECTED MEDICATIONS FOR ACUTE MIGRAINE ATTACKS

Chapter 15 HEADACHE104
there are generally other symptoms and signs of sinusitis (e.g., nasal congestion, fever, boggy
nasal mucosae), and the pain is generally unilateral. Tenderness over a sinus is non-specific
and may be a function of how hard one is pressing. Finally and very importantly, CT findings
of chronic sinusitis, such as mucosal thickening, retention cysts, or ostial narrowing, should
never be considered the cause of a patient’s acute headache.
23. What special diagnostic considerations must be given to a patient with AIDS
and headache?
Headache is a frequent complaint among AIDS patients, occurring in 11% to 55% of patients, and
may occur in many AIDS-related conditions. Acute lymphocytic meningitis can be seen in patients
at the time of acute HIV infections, sometimes associated with fever, lymphadenopathy, sore
throat, and myalgias. Toxoplasma gondii produces multiple brain abscesses and bilateral,
persistent headaches. The diagnosis of toxoplasmosis is made by CT, magnetic resonance
imaging (MRI), or brain biopsy. Other central nervous system lesions include B-cell lymphoma
and progressive multifocal leukoencephalopathy. Cryptococcal meningitis is a common cause of
headache in AIDS patients, occurring in 10% of patients. Meningitis is characterized by fever,
headache, and nausea. The presence of meningismus, or mental status changes, is uncommon.
Patients who have HIV and who present to the ED with persistent headache usually require
neuroimaging and, if imaging is normal, LP should be done.
24. What rapidly progressive infectious entity presents with headache, fever, and
altered mental status?
Herpes simplex encephalitis, the most common form of sporadic encephalitis, is a necrotizing,
hemorrhagic infection that results in brain destruction that mandates early aggressive
treatment with antiviral therapy. LP with polymerase chain reaction of the CSF and gadolinium-
enhanced MRI are the diagnostic methods of choice. On imaging, there is a predilection for
temporal lobe involvement. Note that there are other viral encephalitides (e.g., West Nile,
Eastern Equine) but there is currently no specific treatment for them.
25. What is idiopathic intracranial hypertension, and what is the complication if
not treated appropriately?
Also known as benign intracranial hypertension or pseudotumor cerebri, this entity presents
classically in obese young women with recurrent headaches that are constant or intermittent
and that may present with bilateral papilledema and loss of spontaneous venous pulsations.
Transient pulsatile tinnitus and visual symptoms are common. Occasionally, sixth nerve palsy
is found. Note that a sixth nerve palsy has no localizing value; it is the cranial nerve with the
longest intracranial course and is thus sensitive to pressure and inflammation. Brain imaging
should be done to rule out a mass lesion and, if negative, LP is done; this not only is
diagnostic but also commonly therapeutic. High opening pressure (25 to 40 cm H
2
O) and a
suggestive clinical scenario are diagnostic. It is important to consider the diagnosis of cerebral
venous sinus thrombosis because these two entities can mimic one another. Without
treatment, there is a risk of visual loss. Treatment is with serial LPs, acetazolamide, and
diuretics such as furosemide. Optic nerve fenestration is indicated in refractory cases.
26. Which cranial nerves pass through the cavernous sinus?
Cranial nerves III, IV, V1, and V
1-2
. Cavernous sinus disease may present as only a retro-orbital
headache. Any combination of involvement of the nerves passing through the cavernous sinus is
suggestive of the diagnosis, however, and warrants further evaluation. Invasion by tumor, vascular
disease such as aneurysm or carotid cavernous sinus fistula, and clot (either bland or infection
related) are the more common causes. Patients with other cerebral venous sinus thromboses will
often present with isolated headache, seizure, and elevated intracranial pressure.
27. How common are headaches in children?
As with adults, headaches are also common in children. The history and physical examination
are paramount in sorting out who needs a work-up and who does not. Treatment can start

Chapter 15 HEADACHE 105
with acetaminophen or ibuprofen. Ruling out significant pathology is crucial in children. SAH,
primary cerebral tumors, stroke, metabolic conditions, and toxicologic causes should be
considered in the appropriate setting.
28. What is a blood patch?
One third of patients experience headaches within hours of a diagnostic LP. This is due to a
persistent CSF leak from the dural rent that results in low CSF pressure, dilation of intracranial
vessels, and traction on intracranial contents. This postdural puncture headache is worse
when the patient sits or stands up and improves with bed rest. Treatment includes bed rest,
fluids, and analgesia. Some practitioners use intravenous (IV) caffeine. If conservative
methods fail, autologous blood clot is used, the so-called blood patch. Blood is drawn from
the patient and injected into the soft tissue at the site of the LP. In most institutions, this is
performed by an anesthesiologist. Data suggest that using a small caliber LP needle and a
noncutting tip can decrease the incidence of postdural puncture headache.
29. Are there other forms of low pressure spinal headache?
In the absence of a prior LP, patients can still get a low pressure headache, a condition known
as spontaneous intracranial hypotension. The headache is positional (worse with standing,
better with lying down), similar to a post-dural puncture headache. Occasionally, patients will
develop neurological deficits. Diagnosis is by imaging and LP. This is another diagnosis, albeit
an uncommon one, that supports measuring the opening pressure when doing an LP.
30. In the pregnant (or recently postpartum) woman, are there particular causes
of headache that I should worry about?
Pregnant women can get any kind of headache that nonpregnant women can get; however,
some headache disorders that occur more commonly, or exclusively, in this situation are
cerebral venous sinus thrombosis, eclampsia, pituitary apoplexy, SAH, and posterior reversible
leukoencephalopathy syndrome (PRES). Added to this list in the postpartum patient who has
had an epidural anesthetic are postdural puncture headache and the additional complication of
a postpuncture subdural hematoma. As for imaging, MRI has certain obvious advantages
during pregnancy, but one should get the tests that are needed to make the diagnosis, trying
to balance radiation exposure with accurate diagnosis.
31. Is high blood pressure causing my patient’s headache?
One potential mistake is to diagnose hypertensive urgency in headache patients who have a
high blood pressure. Coexistent headache and hypertension can occur for several reasons.
Probably the most common is that pain and anxiety are elevating the blood pressure.
A second cause is that the problem causing the headache is also causing some degree of
raised intracranial pressure, and the body is raising the arterial blood pressure to preserve
cerebral perfusion pressure. If hypertension is primarily causing the symptoms (the third
possibility), then end organ dysfunction is occurring (in this case, the end organ is the brain).
Lowering the blood pressure about 25% below the peak in this situation, using rapidly acting,
titratable agents, will both treat and help establish the diagnosis because the headache ought
to improve dramatically. In patients with acute ischemic stroke and headache, one should be
cautious about pharmacologically treating high blood pressure because it is likely that the high
pressure is simply due to the brain autoregulating.
32. When should I be concerned about a brain tumor?
Isolated headache is rarely caused by a brain tumor. Only about half of all patients with brain
tumors have headache and the pain characteristics are not specific. The classic early morning
headache is uncommon. Localization (other than neck pain with posterior fossa tumors) does
not usually occur. One risk for patients with brain tumors is to have a headache that is
different from their previous headaches. Therefore, a careful history and physical examination
are most important in deciding which patients need a work-up for a tumor as they are for any
other secondary cause of headache.
Chapter 15 HEADACHE106
BIBLIOGRAPHY
1. Arnold M, Bousser MG, Fahrni G, et al: Vertebral artery dissection: presenting findings and predictors of
outcome. Stroke 37(10):2499–2503, 2006.
2. Bendtsen L, Jensen R: Tension-type headache. Neurol Clin 27(2):525–535, 2009.
3. Cumurciuc R, Crassard I, Sarov M, et al: Headache as the only neurological sign of cerebral venous
thrombosis: a series of 17 cases. J Neurol Neurosurg Psychiatr 76(8):1084–1087, 2005.
4. Edlow JA: Diagnosing headache in the emergency department: what is more important? Being right, or not
being wrong? Eur J Neurol 15(12):1257–1258, 2008.
5. Edlow JA, Caplan LR: Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. N Engl J Med
342(1):29–36, 2000.
6. Edlow JA, Malek AM, Ogilvy CS: Aneurysmal subarachnoid hemorrhage: update for emergency physicians.
J Emerg Med 34(3):237–251, 2008.
7. Edlow JA, Newman-Toker DE, Savitz SI: Diagnosis and initial management of cerebellar infarction. Lancet
Neurol 7(10):951–964, 2008.
8. Edlow JA, Panagos PD, Godwin SA, et al: Clinical policy: critical issues in the evaluation and management of
adult patients presenting to the emergency department with acute headache. Ann Emerg Med 52(4):407–436,
2008.
9. Edlow JA, Wyer PC: How good is a negative cranial computed tomographic scan result in excluding
subarachnoid hemorrhage? Ann Emerg Med 36(5):507–516, 2000.
10. Goldstein JN, Camargo CA Jr, Pelletier AJ, et al: Headache in United States emergency departments:
demographics, work-up and frequency of pathological diagnoses. Cephalalgia 26(6):684–690, 2006.
11. Jordan YJ, Lightfoote JB, Jordan JE: Computed tomography imaging in the management of headache in the
emergency department: cost efficacy and policy implications. J Natl Med Assoc 101(4):331–335, 2009.
12. Lewis DW: Pediatric migraine. Neurol Clin 27(2):481–501, 2009.
13. Pope JV, Edlow JA: Favorable response to analgesics does not predict a benign etiology of headache.
Headache 48(6):944–950, 2008.
14. Savitz SI, Levitan EB, Wears R, et al: Pooled analysis of patients with thunderclap headache evaluated by
CT and LP: is angiography necessary in patients with negative evaluations? J Neurol Sci 276(1–2):123–125,
2009.
15. Schankin CJ, Ferrari U, Reinisch VM, et al: Characteristics of brain tumour-associated headache. Cephalalgia
27(8):904–911, 2007.
16. Vertinsky AT, Schwartz NE, Fischbein NJ, et al: Comparison of multidetector CT angiography and MR imaging
of cervical artery dissection. AJNR Am J Neuroradiol 29(9):1753–1760, 2008.
KEY POINTS: HEADACHE
1. A response to analgesics does not exclude life-threatening causes of headache.
2. Even with modern CT, scanners will miss 5% to 10% of SAHs. LP is needed if SAH is a
major diagnostic concern.
3. HIV-positive patients presenting with headache should have a CT head scan with contrast to
exclude opportunistic infections, including toxoplasmosis.
4. A careful history and physical examination, including neurologic examination, will identify
most patients who need further evaluation.
107
CHAPTER 16
SYNCOPE, VERTIGO, AND DIZZINESS
William F. Young, Jr., MD
1. Do I need to be concerned by a complaint of dizziness?
Yes. There are over 25 million ED visits a year for dizziness; it is the most common
complaint in patients older than 75 years and may herald a stroke.
2. How do I approach this vague and ill-defined complaint?
Start your history with an open-ended question that allows the patient to describe the
symptoms. Dizzy can describe a sensation of vertigo (the illusion of motion);
lightheadedness (presyncope or frank syncope); or disequilibrium (imbalance). Those
with disequilibrium often describe imbalance while walking, especially in the dark.
3. How does one know his or her position in space?
A combination of visual clues and vestibular input determine our spatial orientation.
When they don’t agree or are asymmetric, we feel dizzy.
4. How does the vestibular system work?
The semicircular canals use the principle of liquid inertia to determine angular
acceleration. The canals, oriented in three planes to encompass all aspects of space, are
filled with a fluid, endolymph. When the head turns, the fluid stimulates hair cells in
response to this relative movement, sending impulses to the brain via cranial nerve VIII.
5. How do you define central versus peripheral vertigo?
It is an anatomical definition. Peripheral vertigo is caused by a dysfunction of the inner
ear or vestibular nerve, whereas central vertigo is from etiologies of the brain and a
brain stem. Benign paroxysmal positional vertigo (BPPV), vestibular neuritis, and
Ménière disease are common etiologies of peripheral vertigo, whereas vertebrobasilar
ischemia, multiple sclerosis, cerebellar infarction/hemorrhage, and basilar migraine are
central causes.
6. What are the characteristics of peripheral vertigo?
DR FLIP. This mnemonic reminds you that the Epley maneuver, which flips the patient,
helps BPPV.
Deafness (unilateral hearing loss)
Ringing in the ears (tinnitus)
Fatigable on repeated testing
Latency after Dix-Hallpike maneuver
Intense symptoms
Positional in nature
7. What are the characteristics of central vertigo?
Cranial nerve deficits
Vertical nystagmus (not seen in peripheral vertigo)
Ataxia (with gait impairment)
8. What are the key points for the main causes of peripheral vertigo?
See Table 16-1.