Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


Research Council (1989) attempted to set an optimal
intake level, and so recommended a higher RDA of
1000 RE per day for men and 800 RE per day for
women (the difference being due to a lower body
weight, on average). However, the most recent rec-
ommendations from the US Institute of Medicine are
calculated to maintain an adequate body pool size
and set an RDA of 900 mg of RAE for adult males,
700 mg of RAE for adult females.
Toxicity
003 3 Over600individualcasesofhumanvitaminAtoxicity
have been reported, owing to either acute (single or a
few large doses ingested over a brief period of time) or
chronic intake (moderately high doses taken fre-
quently for periods of months or years). Acute toxicity
in human adults is reported from doses of 300 000–
10 000 000 RE (1000–35 000 mmol); chronic doses of
15 000–300 000RE (50–1000 mmol) have produced
hypervitaminosis A. Symptoms include headache,
vomiting, diplopia, alopecia, dryness of mucous mem-
branes, desquamation, bone abnormalities, and liver
damage.However,singleoraldosesof60000 REinoil
have been successfully used in vitamin A intervention
programs for preschool children, with transient toxic
symptoms observed in no more than 3% of subjects.
Massive doses of b-carotene are not toxic, but may be
lessefficientlyabsorbedandusedthanvitaminAitself.
Rodent animal models have been extremely valuable
in elucidating vitamin A requirements and metabol-
ism, but the rat seems to be much less susceptible to
hypervitaminosis A than is the human.
0034 The toxic effects of high vitamin A intakes are
mediated by serum retinyl esters; retinol-RBP concen-
trations are maintained at normal levels in hypervita-
minosis A, but serum retinyl esters are markedly
elevated, bypassing the normal homeostatic controls
on vitamin A transport. Some carnivores, including
the dog, are unusual in having high fasting levels of
serum retinyl esters, presumably reflecting differences
in lipoprotein metabolism in these species; the impli-
cations of this for vitamin A metabolism and for
resistance to hypervitaminosis A are not clear.
0035 The most tragic consequences of excessive vitamin
A intake are teratogenicity (specifically, malforma-
tions of the cranium, face, heart, thymus, and central
nervous system) and embryotoxicity. Acidic retinoids
such as those that have been used in dermatology are
particularly potent, as they can attain high serum
levels and can readily pass the placental barrier. Al-
though large intakes of vitamin A itself (>7500 RE
per day, 26 mmol per day) early in human pregnancy
can cause birth defects (perhaps owing to metabolism
of retinol to retinoic acid?), serum concentrations of
retinol and retinyl esters are normally maintained at
moderate levels during pregnancy. It is assumed that
these teratogenic effects are related to the important
role of retinoids in differentiation of cells and that
these effects are mediated via the nuclear receptor
proteins. (Interestingly, the retinoid b-glucuronides
are much less teratogenic than retinoic acid.) In view
of these teratogenic effects occurring at less than
10 times the recommended daily intakes, a consensus
of several professional organizations is that women
should avoid vitamin A supplements during the first
trimester of pregnancy, and that subsequent supple-
ments, if taken at all, should be prudently limited to
8000 IU (2400 mg RE, 8.5 mmol) per day, although
10000 IU (3000 mg RE, 10 mmol) appears to be safe.
0036The previous two decades have been exciting in
retinoids research, with the disclosure of the roles of
retinoids in control of gene expression. Continuing
challenges in vitamin A research include: (1) the de-
velopment and confirmation of indirect indices of
vitamin A status; (2) elucidation of the mechanism
of control of serum retinol-RBP concentrations;
(3) more exact determination of vitamin A require-
ments for specific functions (not only growth and
prevention of blindness, but also immune function
and cell differentiation in individual tissues); and
(4) definition of the role of vitamin A in differenti-
ation in specific tissues, perhaps leading to chemical
design of distinctive retinoids to combat specific
cancers and dermatologic diseases.
Seealso: Carotenoids:Occurrence,Properties,and
Determination
Further Reading
Blomhoff R (1994) Vitamin A in Health and Disease. New
York: Marcel Dekker.
Chambon P (1996) A decade of molecular biology of reti-
noic acid receptors. FASEB Journal 10: 940–954.
Chambon P, Zelent A, Petkovich M et al. (1991) The family
of retinoic acid nuclear receptors. In: Saurat JH (ed.)
Retinoids: Ten Years On, pp. 10–27. Basel: Karger.
Clarke SD, Thuillier P, Baillie RA and Sha X (1999) Peroxi-
some proliferator-activated receptors: a family of lipid-
activated transcription factors. American Journal of
Clinical Nutrition 70: 566–571.
Collingwood TN, Urnov FD and Wolffe AP (1999) Nuclear
receptors: coactivators, corepressors, and chromatin
remodeling in the control of transcription. Journal of
Molecular Endocrinology 23: 255–275.
Dietary Reference Intakes for Vitamin A, Vitamin K, Ar-
senic, Boron, Chromium, Copper, Iodine, Iron, Manga-
nese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc
(2001), pp. 65–125. Washington, DC: National Acad-
emy Press. (available online at http://books.nap.edu/
books/0309072794/html/65.html).
4966 RETINOL/Physiology
McKenna NJ, Xu J, Nawaz Z et al. (1999) Nuclear receptor
coactivators: multiple enzymes, multiple complexes,
multiple functions. Journal of Steroid Biochemistry and
Molecular Biology 69: 3–12.
Mangelsdorf DJ, Umesono OK and Evans RM (1994) Reti-
noid receptors. In: Sporn MB, Roberts AB and Goodman
DS (eds) The Retinoids, 2nd edn, pp. 319–349. New
York: Raven Press.
Nalubola R and Nestel P (1999) The Effect of Vitamin A
Nutriture on Health: A Review, pp. 1–83. Washington,
DC: ILSI Press (available at www.ilsi.org/hnipubs.htm).
Napoli JL (1996) Retinoic acid biosynthesis and metabol-
ism. FASEB Journal 10: 993–1001.
Napoli JL (1999) Retinoic acid: its biosynthesis and metab-
olism. Progress in Nucleic Acid Research and Molecular
Biology 63: 139–188.
Ross AC (1999) Vitamin A and retinoids. In: Shils ME,
Olson JA, Shike M and Ross AC (eds) Modern Nutrition
in Health and Disease, pp. 305–327. Baltimore, MD:
Williams & Wilkins.
Sporn MB, Roberts AB and Goodman DS (eds) (1994) The
Retinoids, 2nd edn. New York: Raven Press.
Reverse Osmosis See Membrane Techniques: Principles of Reverse Osmosis; Applications of Reverse
Osmosis; Principles of Ultrafiltration; Applications of Ultrafiltration
RHEOLOGICAL PROPERTIES OF FOOD
MATERIALS
J Lefebvre, Institut National de la Recherche
Agronomique, Nantes, France
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Rheological properties of ingredients and products
are involved in all stages of food, from formulation
to consumption. Their knowledge is therefore im-
portant to many aspects of food science and tech-
nology, such as modeling of processing operations
(pumping, mixing, heat exchange, etc.), design of
the processing and packaging machines, process
control, characterization of ingredients, intermediary
and end products, and instrumental evaluation of
texture. They even concern nutrition, since foodstuffs
have to be chewed and swallowed before being
digested. The interest of food scientists in rheology
is as old as rheology itself, and some of the pioneering
work in this comparatively young discipline has been
carried out on food materials.
0002 During the last decade, the most active research
areas in food rheology dealt with the characterization
of the viscoelastic behavior of liquid, semiliquid, or
gel food systems. Whereas flow properties are of
prime importance in all aspects of processing of liquid
materials, viscoelasticity measurements often consti-
tute in practice the only feasible approach (along with
microscopy) to obtain information on the structure of
complex concentrated systems (solids and liquids)
and on how it is affected by composition, or by
physical, chemical, or biochemical treatments. They
provide a unique tool to adapt formulations or to
develop new engineered foods to meet the demands
of changing technologies and evolving consumers’
requirements.
0003However, rheometry on food systems has long been
limited to the study of flow behavior (viscometry).
Because of theoretical and practical difficulties, and
especially because of the lack of affordable rheometers
with high enough sensitivity, the viscoelastic proper-
ties of food systems have only been evaluated empiric-
ally, using an impressive variety of instruments and
methods of testing, adapted to different specific types
of materials or problems, but which did not allow the
expression of measurements in terms of relevant phys-
ical variables because of the complexity of the deform-
ations and of the mechanical sollicitation patterns they
implemented. This situation has completely changed
since the mid-1980s with the development of com-
paratively low-priced performing commercial rhe-
ometers. Viscoelasticity studies in shear are now
within the reach of the average food science labora-
tory, opening up new, exciting perspectives. But this
does not mean they are easy to carry out and to inter-
pret, and a working knowledge of the essential con-
cepts has not spread as fast and wide as the equipment.
The first purpose of this article, focused on viscoelas-
ticity, is to give an outline of these concepts.
0004Food materials display an amazing variety of rheo-
logical behavior. They can nevertheless be reduced to a
relatively small number of basic types. The main one
along the views outlined above corresponds to transi-
ent networks. It will be illustrated here with a few
examples which will also be used to point out some
RHEOLOGICAL PROPERTIES OF FOOD MATERIALS 4967
fundamental or practical problems which are espe-
cially important or critical in the case of food systems.
0005 Only behaviors in shear (more precisely, in rota-
tional geometries) will be considered, as shear is the
most important type of deformation in rheological
studies with regard to the orientations of this short
article.
Solids and Liquids: Betwixt and Between
0006 Rheology emerged as a science to describe, analyse,
and rationalize the complex mechanical behavior dis-
played by most real materials, for which the classical
Hookean elastic solid and the Newtonian viscous
fluid represent only limiting behavior, which is seldom
encountered in practice. Two types of deviation from
the ideal behavior can occur, either separately or
together: time-dependence and nonlinearity.
0007 Let us revisit briefly these classical notions with
the help of a rheological experiment which is the
retardation test (creep and recovery): a stress s is
applied suddenly at time t ¼0 and maintained till
t ¼s. Then, the sample is suddenly unloaded; the
strain g is recorded during the loading period (creep)
and after the removal of stress (recovery); the results
are expressed in terms of the compliance function
JðtÞ¼gðtÞ=s in both parts of the test.
Viscoelasticity
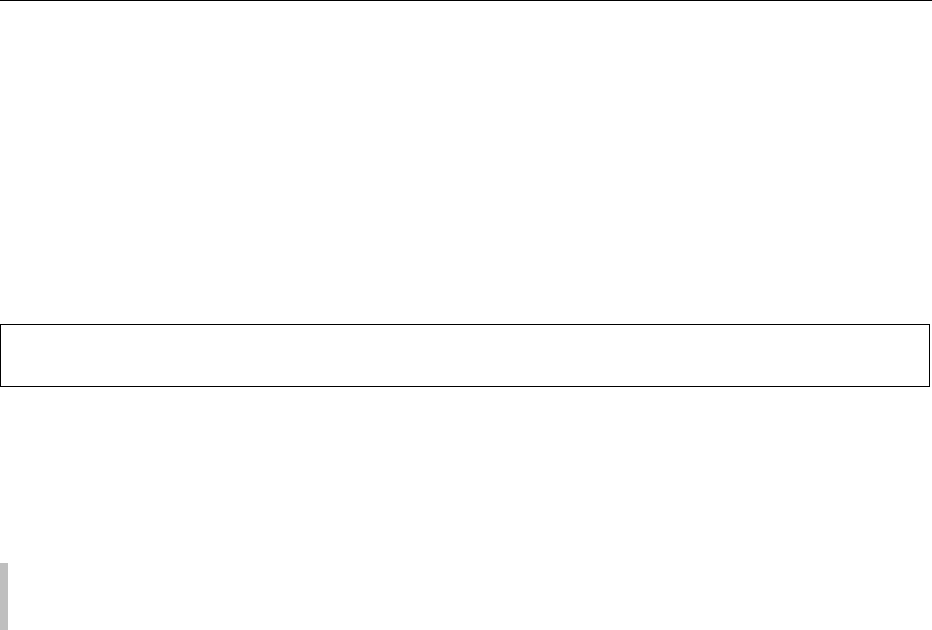
0008In time-dependent behavior, the response depends on
the duration of excitation. The general case is that of
viscoelastic behavior, illustrated schematically in
Figure 1c and d. The responses of the ideal elastic
solid and of the ideal viscous liquid are shown for
comparison (Figure 1a and b); they are instantaneous
and defined by a constant value of the compliance
J
e
¼ g
e
=s (for the solid) or the compliance rate
dJðtÞ=dt ¼ 1= (for liquid of viscosity Z). To reach
steady state (i.e. the equilibrium compliance J
e
in the
case of a viscoelastic solid, or a constant rate of
Creep
Recovery
J
e
Time t (s)
0S
(a)
0
Compliance J(t) (m
2
N
−1
)
Creep
Recovery
Slope 1/η
Time t (s)
0S
(b)
0
Compliance J(t) (m
2
N
−1
)
J(S)
Creep
Recovery
Time t (s)
0
0
S
(c)
J
e
Compliance J(t) (m
2
N
−1
)
Creep Recovery
Time t (s)
0S
(d)
Compliance J(t) (m
2
N
−1
)
1
1
2
2
t/η
t/η
S/η
S/η
J
e
o
J
e
o
J
fig0001 Figure 1 Schematic responses to a retardation test: (a) elastic solid; (b) viscous liquid; (c) viscoelastic solid; (d) viscoelastic liquid
within the linearity range. Solid curve: measured total compliance. Curve 1 (dashed line): contribution of flow. Curve 2 (dotted line):
recoverable compliance J
r
(t).
4968 RHEOLOGICAL PROPERTIES OF FOOD MATERIALS

compliance dJð tÞ=dt in that of a viscoelastic liquid)
requires a certain length of time after loading. And it
is the same after unloading for compliance to reach a
constant value. This value is zero in the case of a
viscoelastic solid: deformation is entirely reversible,
although not instantaneous. In contrast, for a visco-
elastic liquid, the strain gathered during creep is
progressively recovered after unloading, but only in-
completely; the residual compliance J
?
corresponds
to the irreversible part of the deformation, i.e., to the
contribution of flow to the total strain at the end of
the creep period: J
1
¼ S=. Flow contribution to
strain becomes dominant (J(t) becomes a linear func-
tion of time) only after a creep time t > t
m
; for t < t
m
,
elasticity dominates the response, although flow
begins as soon as stress is applied to the material. By
subtracting flow contribution t/Z from the compli-
ance in creep, the reversible contribution to the com-
pliance is obtained. This contribution similar to the
response of the viscoelastic solid is called the recover-
able compliance J
r
(t); it is identical, in the case of
linear behavior (see below), to the part of the final
compliance J(S) which is recovered during the re-
covery part of the test. The plateau value J
e
of J
r
(t)
can be taken as a gauge of the elastic character of the
liquid. The product t
m
¼ J
e
is the longest retard-
ation time of the material and corresponds to t
m
.
0009 Such behavior simultaneously displays elastic and
viscous characteristics. Elasticity dominates at short
times of observation; the behavior appears to be in-
creasingly viscous as the time scale of the experiment
broadens. Thus, a given material can display either
solid- or liquid-like behavior, depending on the time
scale of the deformation process. This scaling is rep-
resented by the Deborah number D ¼ t/, where t is
a characteristic time of material response (infinite for
an elastic solid, zero for a viscous liquid) and is a
characteristic time of the experiment. A material will
display a solid-like behavior (high D values) if it
responds slowly (large t) or if its response is observed
at short time scales (small ). Although the distinc-
tion between solid and liquid subsists in theory for
viscoelastic materials, it can be difficult to draw it in
practice. Many materials which are felt as solids in
common experience are indeed viscoelastic liquids.
Linearity and Nonlinearity
0010 The notion of linearity, which simply amounts to the
proportionality of the response to the solicitation for
the ideal solid or liquid (J
e
or Z independent of s,
respectively), has to be generalized to the time de-
pendence for viscoelastic materials. The viscoelastic
behavior is linear if the response to a sequence of
arbitrary solicitations is identical to the sum of the
responses to these stimuli if they were acting
independently. This is the Boltzmann superposition
principle which can be expressed as:
gðtÞ¼
Z
t
1
Jðt t
0
Þ
dsðt
0
Þ
dt
0
dt
0
ð1Þ
in terms of the stress history. As to the retardation
test, linearity means that:
.
0011J(t) is independent of s;
.
0012The values of the steady-state limiting compliance
J
e
and viscosity Z are the same when obtained
from the creep or from the recovery parts of the
test;
.
0013The curve of the recoverable compliance against the
recovery time (tS), obtained from recovery, super-
imposes on that of the recoverable compliance
against creep time, obtained by subtracting the con-
tribution of flow from the creep compliance.
Most real materials behave linearly only up to some
limit of strain or strain rate limit, which is a material
property. Whilst handling and processing the material
generally involves solicitations which exceed this
limit (which may be fairly low), characterization of
its viscoelastic behavior within the linearity range is a
prerequisite for studies in the nonlinear regime. In the
linear regime, the results of any of the classical rheo-
logical tests are independent of the amplitude of the
solicitation and they can also be used to predict the
behavior of the material in the other tests. Beyond
the linearity range, this is no longer the case.
Classical Rheological Tests
0014The characterization of the rheological behavior of a
material requires the study of its viscoelasticity and,
in the case of a liquid, that of its steady flow behavior.
The rheologist uses very simple ‘system of loads’
patterns and deformations. Transient regime and
dynamic tests are used to study viscoelasticity. Flow
behavior is investigated using viscometry.
0015Very often, the study of viscoelasticity is restricted
to the linear range, for the reasons hinted at above.
Although within the linearity domain all viscoelasti-
city tests are equivalent in theory and their results can
be interconverted using theoretical relations or semi-
empirical approximation methods, their respective
applications differ in practice according to the
materials and the instruments and the experimentalist
should view them as complementary.
Transient Regime Tests
0016We have already given the principle of the retardation
test (creep and creep recovery). This test corresponds
to the ‘natural’ operating mode of stress-controlled
rheometers. The transient test with strain-controlled
RHEOLOGICAL PROPERTIES OF FOOD MATERIALS 4969
instruments is the (stress) relaxation test: at time zero,
the sample is suddenly deformed to a given value of
strain which is then kept constant while the decay
of stress with time is recorded. The experiment is
analyzed using the relaxation modulus function
GðtÞ¼sðtÞ=g, which does not depend on the strain
in the linear domain of behavior. The modulus and
the compliance functions are linked in the linear
regime by the integral equation:
t ¼
Z
t
0
Jðt uÞGðuÞdu ¼
Z
t
0
JðuÞGðt uÞdu ð2Þ
so, GðtÞ6¼ 1=JðtÞ, except in the plateau regions of
these functions. Ideal elastic solids store integrally
and indefinitely the mechanical energy imput: stress
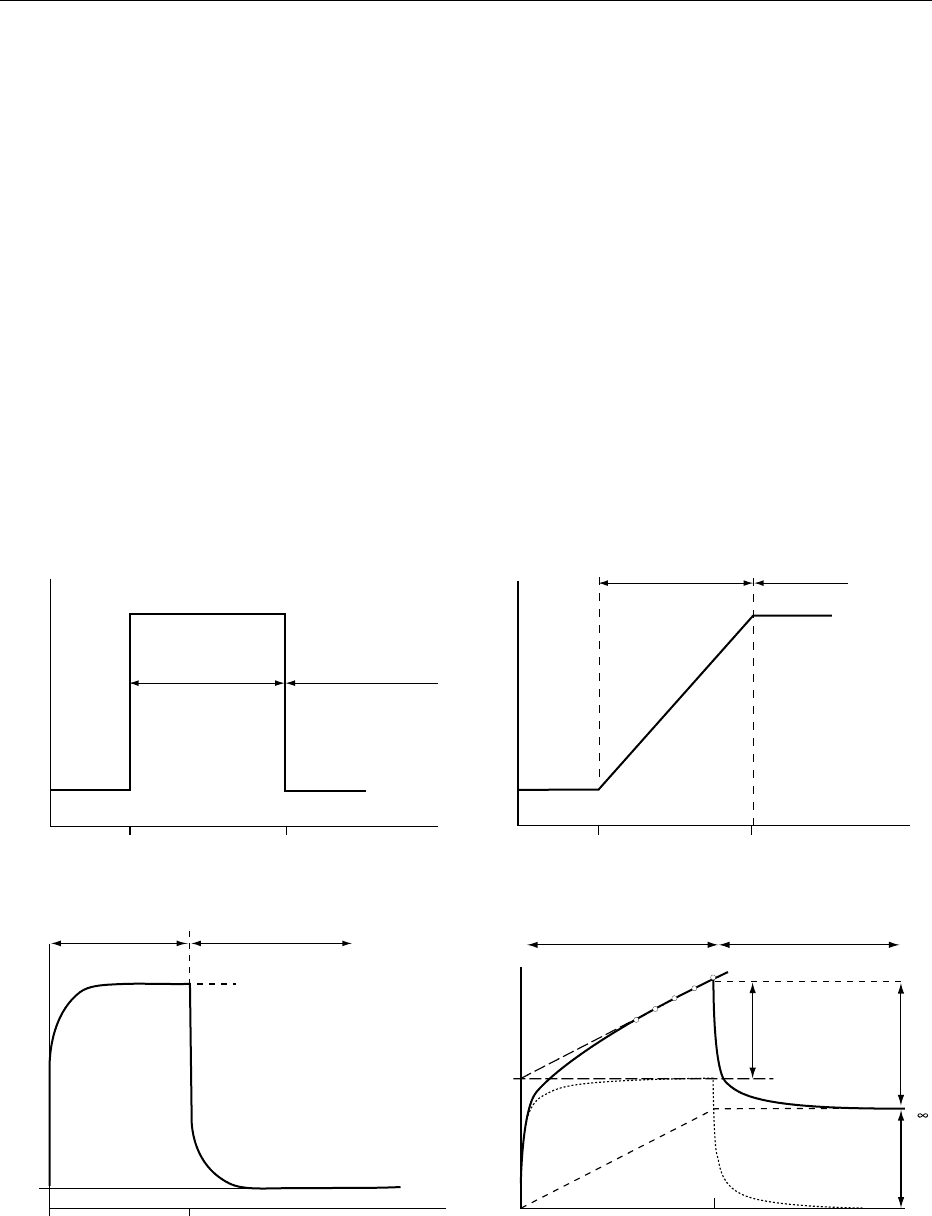
does not relax. For viscoelastic liquids, stress relaxes
gradually and vanishes after a long enough time; at
intermediate times, a region, called the viscoelastic
plateau G
N
, where the decrease of the modulus
slackens momentarily, is frequently observed on bilo-
garithmic scales (Figure 2a). Viscoelastic solids do not
relax completely: at long time values, the modulus
approaches a constant value G
e
, the equilibrium
modulus (Figure 2b).
0017 Stress relaxation tests are not easy to perform on
liquids with low elasticity or short characteristic
times. In such cases, it is preferable to submit the
material to a sudden constant shear rate
_
gg ¼ dg=dt
until an equilibrium value s
e
of stress is reached,
after which the shear rate is suddenly stopped while
stress continues to be recorded (Figure 3). Both parts of
this test can be analyzed in term of relaxation modulus:
GðtÞ¼ð1=
_
ggÞjdsðtÞ=dtjð3Þ
The retardation test is particularly interesting for vis-
coelastic liquids since the viscoelastic response can be
very simply separated from the steady flow contribu-
tion (Figure 1d), in contrast to the relaxation test; the
latter is better suited for solid materials.
0018Transient tests allow materials with very long
response times to be studied; the upper time limit
for the experiments only depends on the stability of
the material and the patience of the operator. But
since in practice the establishment or the release of a
constant value of the stress, strain, or strain rate takes
some time, transient tests do not measure correctly
the response at short times. Besides, the response
often shows at starts and stops transient damped
oscillations due to mechanical coupling between the
sample and the measuring device. These methods are
applicable to materials with characteristic times
longer than, say, 1 min.
0019Transient tests usually require relatively large
‘system of loads’ to give an accurately analyzable
response; this may be a problem for materials with a
low linearity limit.
Dynamic Measurements
0020Dynamic measurement consists of submitting the
sample to a sinusoidal ‘system of loads’ at an angular
frequency o rad s
1
. When stress is imposed, strain is
measured, and conversely: this type of test can be
performed either with stress- or with strain-controlled
G
g
G
N
8
log(t)
(s)
log(G(t))
(Pa)
(a)
G
g
G
e
log(t) (s)(b)
log(G(t))
(Pa)
fig0002 Figure 2 Schematic responses to a stress relaxation test:
(a) viscoelastic liquid; (b) viscoelastic solid.
0.002
0.001
0
010203040
Time (min)
Stress (Pa)
12
σ
e
fig0003Figure 3 Response of a 3% bovine serum albumin solution
(isoionic conditions) to the sudden application of a shear rate of
0.05 s
1
over 12 min (step 1) followed by its sudden stop (stress
relaxation: step 2).
4970 RHEOLOGICAL PROPERTIES OF FOOD MATERIALS
instruments. Within the range of linear viscoelastic
behavior, the response of the material is also sinus-
oidal with the same frequency as the excitation, but
out of phase. If a strain g ¼ g
o
cosðotÞ is imposed, the
stress will be s ¼ s
o
cosðot þ dÞ; the phase angle d
is zero for an ideal solid and p/2 for an ideal liquid.
The results are often expressed in terms of the
storage and loss moduli G
0
¼ðs
o
=g
o
Þ cosðdÞ and
G
00
¼ðs
o
=g
o
Þ sinðdÞ, which are the real and ‘imagin-
ary’ parts of the complex modulus G
ðoÞ¼G
0
ðoÞþ
iG
00
ðoÞ¼sðtÞ=gð tÞ, respectively. The viscoelastic be-
havior will be described by the variations of G
0
and
G
00
with o (the mechanical spectrum of the material);
however, the two moduli are not independent over the
frequency domain. Alternatively, the results can be
expressed in terms of the real and ‘imaginary’ com-
ponents of the complex compliance, or (for liquids
only) of the complex viscosity: J
0
¼ G
0
=ðG
02
þ G
002
Þ,
J
00
¼ G
00
=ðG
02
þ G
002
Þ, and
0
¼ G
00
=o,
00
¼ G
0
=o.
Although these representations contain strictly the
same information as G
0
, G
00
, they can prove more
interesting for viscoelastic liquids because they
weigh dissipative processes differently on the fre-
quency scale. Qualitatively, a measure at frequency
o in a dynamic test is equivalent to a measure at time t
¼ 1/o in a transient test.
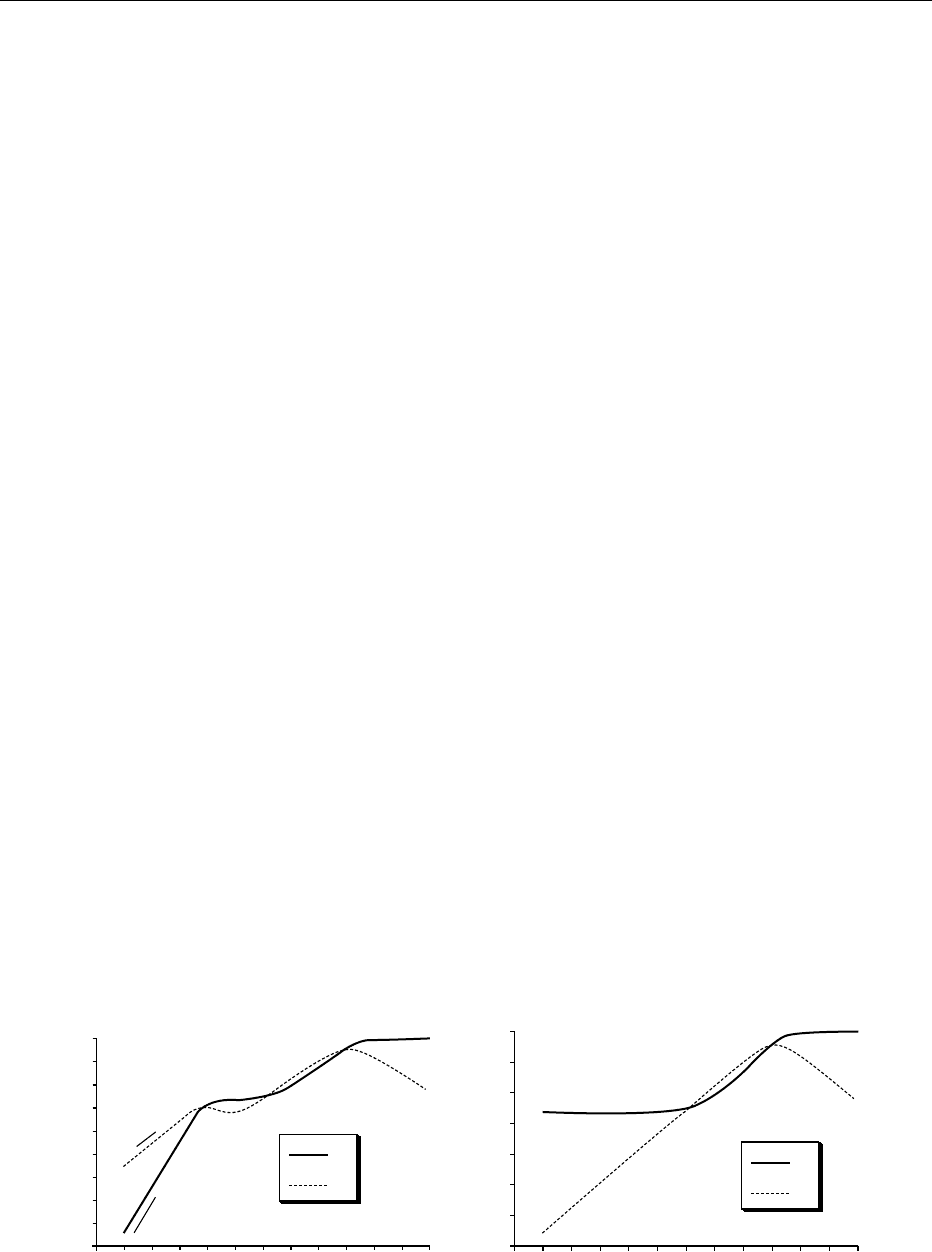
002 1 Figure 4a and b show the schematic theoretical
mechanical spectra of a viscoelastic liquid and a
viscoelastic solid, respectively. Whereas G
0
(o) is
necessarily a monotonously increasing function,
G
00
(o) shows maxima which correspond to concen-
trations of dissipative processes in the material over
certain frequency regions. Two loss peaks are visible
on the liquid-type spectrum. They encompass an inter-
mediate frequency range where G
0
> G
00
and keeps a
nearly constant value G
N
– the viscoelastic plateau;
at this time scale, when energy dissipation is showing
a relative minimum, the material is transiently quasie-
lastic. On both sides of the plateau, G
00
> G
0
and both
moduli are strongly frequency-dependent. At high
frequencies, G
0
and G
00
first both increase approxi-
mately as o
a
with a*0.5 (the transition zone); then G
0
tends towards its very high ‘glassy’ limit G
g
, whereas
G
00
drops: the ‘glassy behavior’ corresponds to solici-
tations which are too fast for the structural elements
in the material to respond. Below the viscoelastic
plateau, G
0
a o
2
and G
00
a o; this is the terminal region
of the mechanical spectrum, corresponding to flow.
For viscoelastic solids, the terminal region is not ob-
served; at low enough frequencies, G
0
reaches
a constant value – the equilibrium modulus G
e
.
Frequently, the loss peaks overlap strongly; then the
viscoelastic plateau reduces to an inflection in G
0
.
0022Dynamic measurements are very popular. They are
easy to perform, accurate even with fairly fluid ma-
terials, and cause minimal perturbation to the sample
since the amplitude of strain is controlled and can be
kept to quite low values (minimum value *0.1% on
strain-controlled instruments, but *1% on stress-
controlled ones). They permit the study of materials
with a low linearity limit.
0023However, some limitations of dynamic tests should
not be overlooked:
.
0024Beyond the linearity limit, the response signal is no
longer sinusoidal. The calculation of the real and
‘imaginary’ components of the rheological func-
tions, as outlined above, performed automatically
by the rheometer softwares, is then invalid.
.
0025The frequency range is restricted for practical
reasons. Because of mechanical problems, rota-
tional rheometers cannot operate above 200–
500 rad s
1
, but the upper limit may be as low as
* 10 rad s
1
when rather fluid materials are tested.
Instrument softwares generally permit operation
down to 10
4
rad s
1
, but below 10
3
rad s
1
measurements take an exceedingly long time. The
practical range of operation is thus 10
3
–100 rad
s
1
, corresponding to the 10
2
–10
3
s
1
time scale,
extending well below the lower limit of transient
G'
G"
log(ω) (rad s
−1
)
log(G'), log(G") (Pa)
G
g
G
e
(b)
Slope 1
Slope 2
12
3
4
G
N
⬚
G
g
log(ω) (rad s
−1
)
log(G'), log(G") (Pa)
G'
G"
(a)
fig0004 Figure 4 Dynamic measurements. Schematic mechanical spectrum of: (a) a viscoelastic liquid: 1, terminal zone; 2, viscoelastic
plateau; 3, transition zone; 4, glassy zone; (b) a viscoelastic solid.
RHEOLOGICAL PROPERTIES OF FOOD MATERIALS 4971
tests but stopping short for many materials, as will
be shown later.
Viscometry
0026 Flow behavior is usually investigated through visco-
metric experiments: a shear rate (or stress) is imposed
on the liquid and the resulting response (shear stress
or rate) is measured; viscosity is defined as ¼ s=
_
gg.
Viscometry is primarily concerned with the steady-
state response.
0027 Simple liquids and solutions of low-molecular-
weight molecules are Newtonian (constant viscosity)
over the wide shear rate range of practical interest,
which extends roughly from * 10
4
s
1
(sedimenta-
tion) to 10
4
s
1
(spraying); chewing and swallowing
or pumping and mixing involve intermediate typical
shear rate values (10
1
–10
3
s
1
). But for most mater-
ials, viscosity depends on the shear rate (or stress),
although generally it tends to be Newtonian at low
enough shear rates, and in many applications non-
Newtonian flow properties are important.
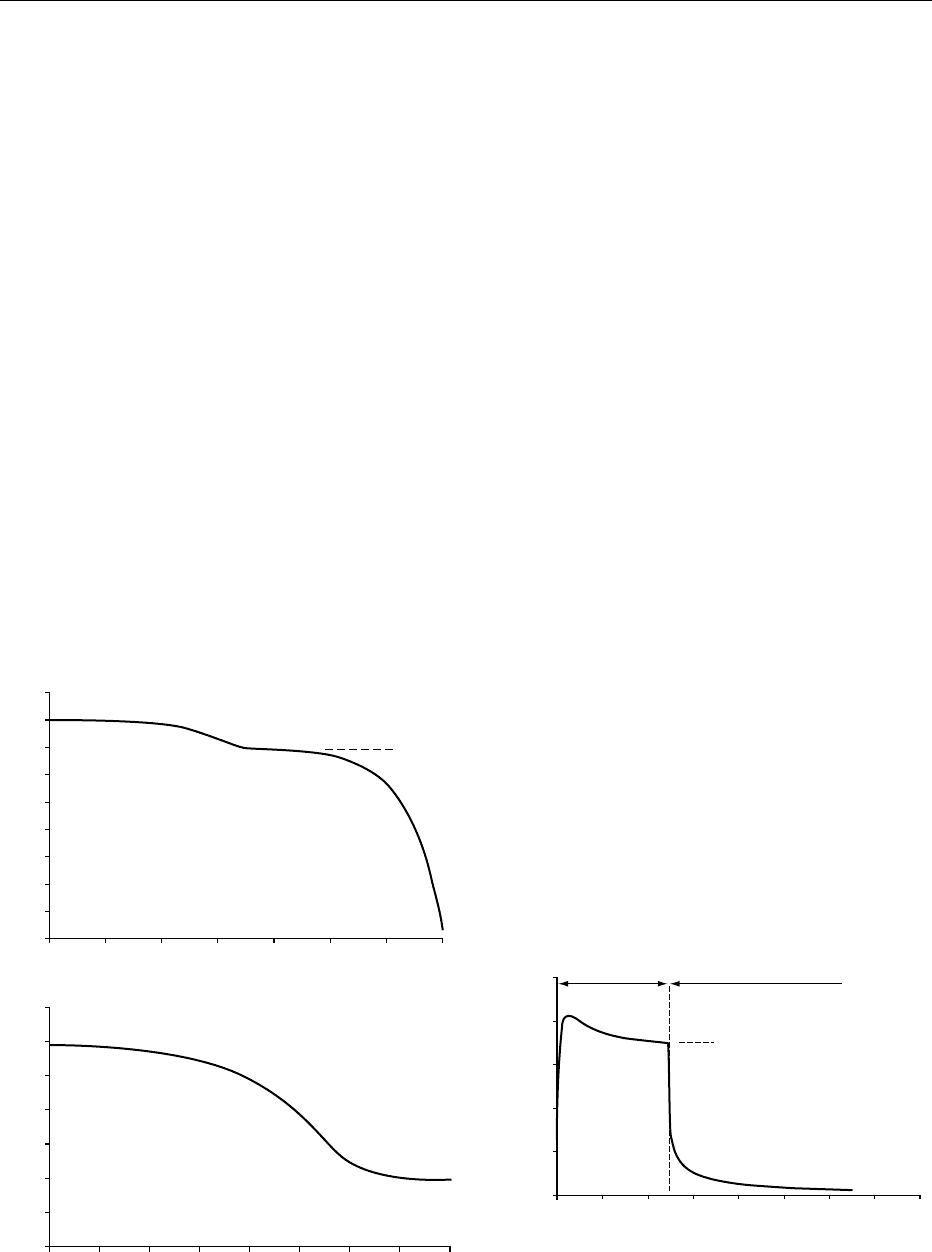
0028 The usual behavior is shear-thinning: as
_
gg increases,
Z decreases from an initial Newtonian plateau Z
o
to a final one Z
oo
; but one or both of them may often
be out of the experimental window (Figure 5). Shear-
thickening behavior is exceptional in food systems.
0029 Non-Newtonian flow curves are usually recorded
by applying shear rate (or stress) ramps. However,
artifacts can result from the inertia of the measuring
device or from the viscoelasticity of the sample. It is
better to apply a series of shear rate (or stress) steps,
waiting at each step for the steady-state response.
Performing retardation tests under different stress
values is almost the only method applicable to highly
viscoelastic liquids (Figure 6) or to very viscous
inelastic ones; it allows viscosity measurements at
very low shear rates.
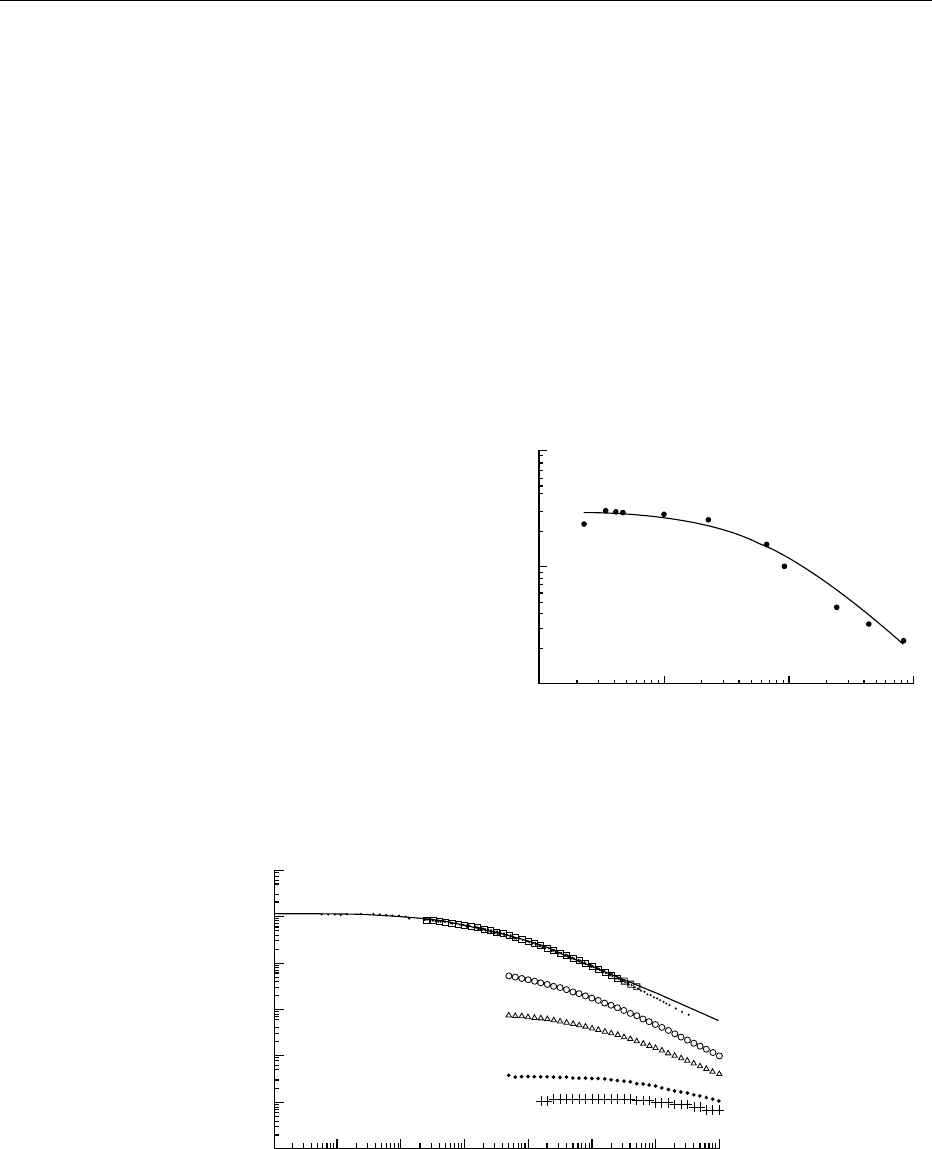
0030Many relatively inelastic shear-thinning liquids dis-
play viscosities which also depend on the duration
of shear. When viscosity decreases during shear,
the behaviour is said to be thixotropic; the reverse
case is called antithixotropy; the changes may be
completely or partially reversible. Thixotropy is a
time-dependent behavior which in principle is to be
distinguished from viscoelasticity. But in practice,
these two properties may be difficult to differentiate;
besides, thixotropic materials often show appreciable
10
−
4
10
−
3
10
−
2
2.2 g l
−
1
3.2 g l
−
1
7.4 g l
−
1
13.9 g l
−
1
22.2 g l
−
1
10
−
1
10
0
10
1
10
2
Shear rate (1/s)
Viscosity (Pa s
−
1
)
10
3
10
−
3
10
−
2
10
−
1
10
0
10
1
10
2
10
3
fig0005 Figure 5 Shear-thinning behavior. Flow curves of solutions of a high-viscosity hydroxyethylcellulose sample at different concen-
trations. Above a concentration of *2gl
1
, the solutions exhibit typical shear-thinning behavior. The master curve (dots) is built by
collapsing the different curves on the 22.2 g l
1
one by shifting them along the two axes. The continuous line shows the fit of Cross
equation: ð
1
Þ¼ð
o
1
Þ=½1 þð
_
gg=
_
gg
c
Þ
m
to the master curve data, where Z
o
¼initial Newtonian plateau viscosity; Z
?
¼high shear
rate Newtonian viscosity (taken as zero here since it is negligible compared to Z);
_
gg
c
¼ critical shear rate; and m ¼ dimensionless
exponent. The fit gives Z
o
¼ 118 Pa s
1
,
_
gg
c
¼ 0.15 s
1
and m ¼ 0.60.
10
−5
10
−4
10
−3
Shear rate (1/s)
η (Pa s
−1
)
10
−2
10
4
10
5
10
6
fig0006Figure 6 Flow curve of a toothpaste determined from the
analysis of creep tests carried out at different values of the
applied stress.
4972 RHEOLOGICAL PROPERTIES OF FOOD MATERIALS
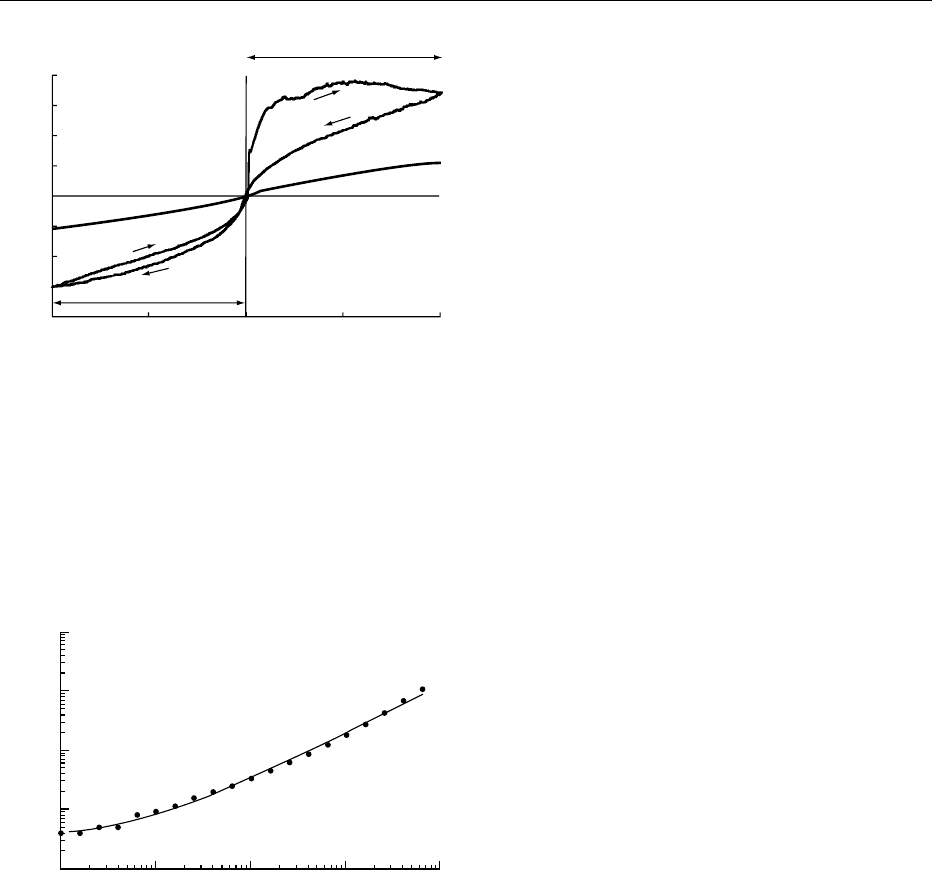
viscoelasticity at the same time. When the material is
submitted to a shear rate cycle from zero to a max-
imum and back to zero, a thixotropic loop is observed
(Figure 7). This is a popular way to spot the existence
or the apparition of thixotropy, but it only allows
comparative work; moreover, there are risks of
confusion with inertia effects or with the manifest-
ation of viscoelasticity, which also shows as loops.
The responses to sequences of step changes of shear
rate are used for thorough studies, but thixotropy is a
difficult topic.
0031Yield stress behavior or plasticity, another type of
complex flow properties, has been the subject of much
discussion. Plastic material would not flow until the
stress has exceeded a yield value s
o
, below which vis-
cosity is infinite (solid behavior). Many materials show
apparent yield stress behavior over limited ranges of
stress or shear rate (Figure 8). However, whenever it
has been possible to go down to low enough stresses
or shear rates (using creep test, for instance), such
materials were found to flow, but with the peculiarity
that viscosity drops from very high values to relatively
low ones over quite a narrow range of stress in the
region of low shear rates (Figure 9).
Problems in Rheological Characterization
of Food Systems
Structural Basis of Viscoelasticity in Food Systems
0032Viscoelasticity is the manifestation of the internal
structure of the material, i.e., the distribution in
space of the structural elements and their inter-
actions. Thixotropy and plasticity derive from flow-
induced large-scale structural changes.
0033Structural elements can be molecules, macromol-
ecules, or particles (solid particles, liquid droplets, gas
bubbles), or associations of such elements (aggre-
gates, micelles, etc.) and their combinations. The
two simplest cases to consider are the solutions of
polymer-like chain macromolecules (polysaccharides,
gelatin) and the dispersions of (quasi-)spherical par-
ticles (including globular protein solutions). When
dilute, such systems show no appreciable viscoelasti-
city in practical conditions – the longest relaxation
time of a macromolecular chain or of an emulsion
droplet is shorter than *10
2
s. Beyond a certain
polymer concentration or disperse phase volume frac-
tion in the system, an elasticity of entropic nature
develops due to topological constraints between
macromolecular chains (entanglements), or from
crowding effects between the particles which result
in a local order. Semidilute polysaccharide solutions
should normally display this type of viscoelasticity.
This is indeed the case for guar gum galactomannan
solutions; their mechanical spectrum (Figure 10)
shows in the upper region of the experimental fre-
quency range the beginning of the viscoelastic plateau
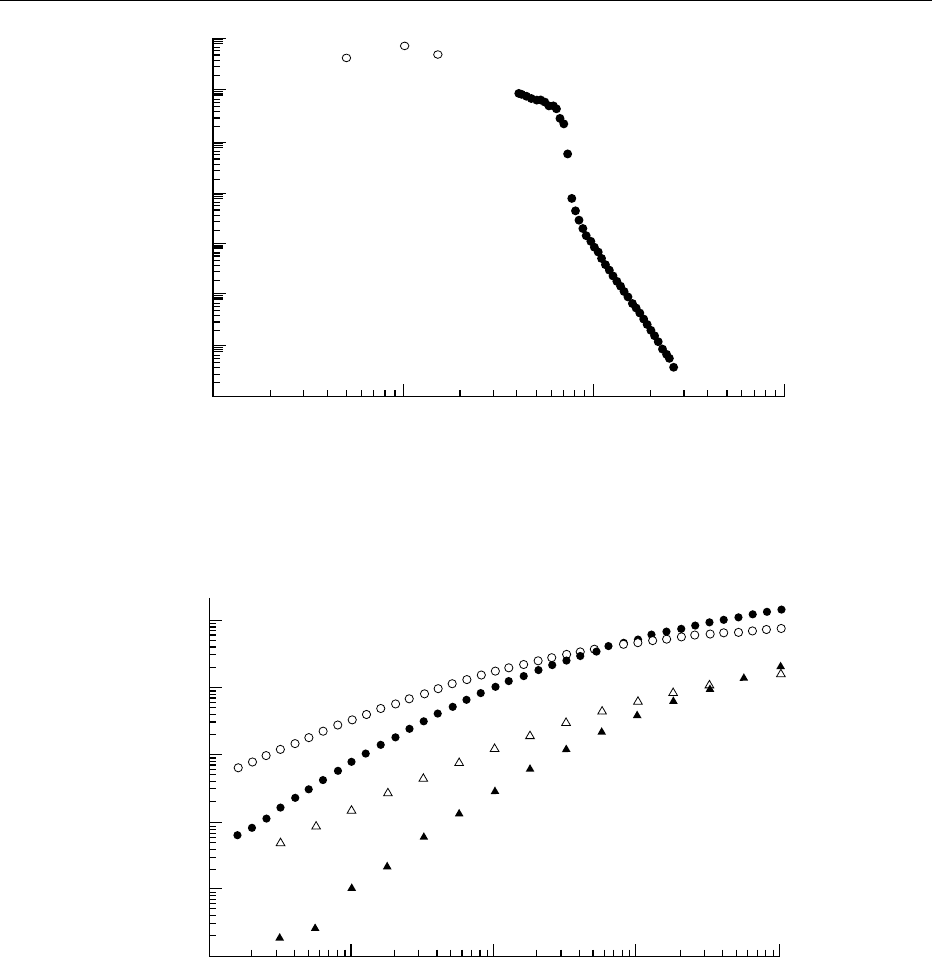
due to entanglements. But locust bean gum galacto-
mannan (LBG) solutions progressively depart from
this behavior upon aging, with the development of a
viscoelastic plateau at low frequencies (Figure 11):
the system slowly changes into a gel. This reflects
the establishment of relatively long-lived linkages
between the chains, probably due to hydrophobic
interactions between the ‘smooth’ regions (devoid of
100
20
10
0
10
20
50
2nd shear cycle
1st shear cycle
0
Shear rate (1/s)
Shear stress (Pa)
50
2
1
100
fig0007 Figure 7 Thixotropic loops. Application of two successive
shear cycles (0–100–0 s
1
) to a guar gum galactomannan/
xanthan mixture (ratio 90/10 w/w) in water at a total polysacchar-
ide concentration of 0.5% w/w (curve 1). The first cycle causes
drastic irreversible damage to the structure of the mixed system.
A residual slight thixotropic behavior is observed during the
second cycle and remains unchanged upon subsequent cycles.
No thixotropy is displayed by guar gum solutions or xanthan
solutions; the results for a 0.5% guar gum galactomannan solu-
tion are given for comparison (curve 2).
10
−1
10
0
10
1
10
2
Shear rate (1/s)
Shear stress (Pa)
10
3
10
−1
10
0
10
1
10
2
10
3
fig0008 Figure 8 Apparent yield stress behavior. Flow curve recorded
at 60
C of a wheat starch paste prepared in the presence of
sodium caseinate (concentrations 6% starch, 7.5% caseinate).
The continuous line is the fit of the Herschel–Bulkley equation:
s ¼ s
o
þ k
_
gg
n
; it gives an apparent yield stress value
s
o
¼ 0:34 Pa:
RHEOLOGICAL PROPERTIES OF FOOD MATERIALS 4973
galactose groups) of the mannose backbone, which
do not exist in the case of guar. Similarly, a 3% bovine
serum albumin (BSA) isoionic solution departs from
the purely viscous and Newtonian behavior expected
for dilute hard sphere dispersion (Figure 3), indicating
that protein molecules are strongly interacting.
0034 Because of their chemical structure and of the
specific properties of water, food macromolecules
generally interact through hydrogen and hydro-
phobic interactions. As a result, viscoelasticity of
the transient network type (noncovalent gels) can be
observed at relatively low concentrations. Transient
networks also result from partial destabilization
(flocculation) of suspensions or emulsions due to
colloidal interactions.
Monitoring Structural Transitions
0035The example of LBG solution (Figure 11) showed that
viscoelastic measurements can be used to follow
structural changes in a system. In this case, the change
10
6
10
4
10
2
10
0
10
0
10
1
10
2
10
3
Shear stress (Pa)
Viscosity (Pa s
−1
)
fig0009 Figure 9 Apparent yield stress behavior. Flow curve of a commercial mayonnaise. The filled circles correspond to the results
recorded during the imposition of a shear rate ramp, the empty circles to data obtained by application of retardation tests. The latter
data demonstrate unequivocally that the behavior is in fact shear-thinning.
10
2
10
1
10
0
10
−1
10
−2
10
−3
10
−2
10
−1
10
0
10
1
10
2
G',G" (Pa)
ω (rad s
−1
)
fig0010 Figure 10 Typical mechanical spectra of biopolymer solutions: guar gum galactomannan solutions in water (20
C) at two concen-
trations: 1.87% w/w (circles) and 1% w/w (triangles). Filled symbols, storage modulus G
0
; open symbols, loss modulus G
00
.
4974 RHEOLOGICAL PROPERTIES OF FOOD MATERIALS
was slow enough to allow viscoelasticity to be char-
acterized over a certain frequency range at different
steps of its evolution. However, structural changes are
generally rather fast, and once started, can rarely be
stopped at will. Single-frequency dynamic measure-
ments, since the time required for each individual
measure is short provided that o > 0.01 rad s
1
, are
very precious indeed to monitor the kinetics of struc-
ture changes, as exemplified in Figure 12 for milk
clotting, an instance of colloidal gel formation. But
they do not characterize rheologically the evolution
of the system. Mechanical spectra can be obtained
in the classical way only when the system remains
practically unchanged during the time necessary to
record them. However, advanced techniques which
are outside our scope require much shorter times than
with the classical frequency sweep, and allow study of
systems undergoing relatively fast structural changes.
0036In classical follow-up experiments at fixed fre-
quency, the choice of frequency may be critical.
No change would be detected in LBG solutions if
o ¼10 rad s
1
were selected to monitor aging
(Figure 11)!
The Need to Enlarge the Experimental Window
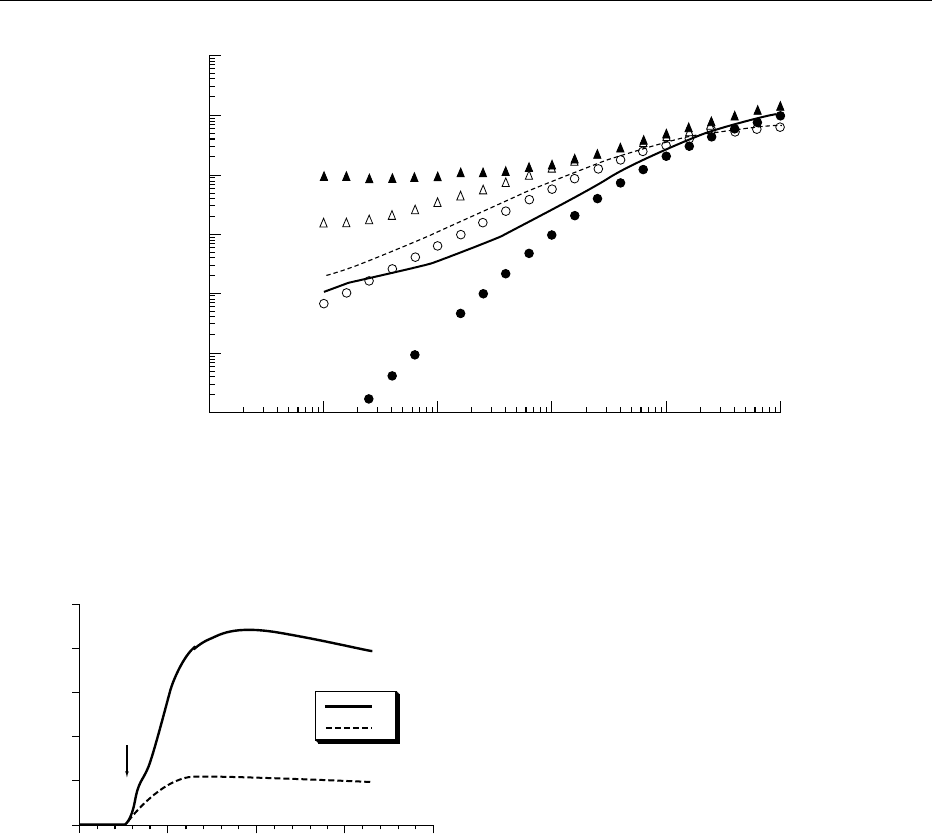
0037Figure 13 shows the mechanical spectra of food
systems we know to differ largely in nature and in
texture or consistency. Nevertheless, these spectra
are qualitatively similar; those of the commercial
mayonnaise and the 61 mg ml
1
BSA heat-set gel
even superimpose. They show the viscoelastic plateau
region of transient networks of the colloidal gel type,
with gently ascending moduli curves and with G
0
higher than G
00
over the frequency window but rela-
tively large G
00
/G
0
ratios (0.1–0.5); in the case of the
gluten sample, however, the upper end of the plateau
is visibly approached. Beyond this assignation to a
general type of structure, such flat spectra allow
only a rough estimation of the plateau modulus. But
quantitative comparison can be misleading, since the
viscoelastic plateau often extends beyond both limits
0
0
200
100
300
400
500
5 101520
pH 5.3
G'
G"
G', G" (Pa)
Time (h)
fig0012 Figure 12 Monitoring lactic acid bacteria milk clotting using
dynamic measurements at fixed frequency (40
C, o ¼ 6 rad s
1
,
strain amplitude g
o
¼ 0.02). The gelation starts after about
150 min fermentation, when the pH has decreased to 5.3. The
decline in the G
0
curve after *11 h is an artifact due to syneresis.
The experiment was performed using coaxial cylinders to minim-
ize the incidence of syneresis; with cone–plate or plate–plate
geometries, syneresis causes slippage and its effect is seen
much earlier, even when measuring devices with striated or
sanded surfaces are used.
10
−3
10
−3
10
−2
10
−1
10
0
10
1
10
2
10
3
10
−2
10
−1
10
0
10
1
10
2
G',G" (Pa)
ω (rad s
−1
)
fig0011 Figure 11 Progressive departure from the solution state during aging of a locust bean gum galactomannan solution (concentration
10 g l
1
;20
C). Mechanical spectra of the freshly prepared solution (circles), of the system after 6 days’ aging (lines), and of the system
after 15 days’ aging (triangles). Filled symbols and solid line, G
0
; open symbols and interrupted line, G
00
.
RHEOLOGICAL PROPERTIES OF FOOD MATERIALS 4975