Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 2 • Modifi ed Radical Neck Dissection Preserving Spinal Accessory Nerve 35
A
Accessory nerve
2nd Cervical rootlets
3rd Cervical rootlets
IJV
Ansa cervicalis
(inferior root)
Lymphatic pedicle
Vagus nerve
Thyrocervical trunk
B
C
Lymphatic pedicle
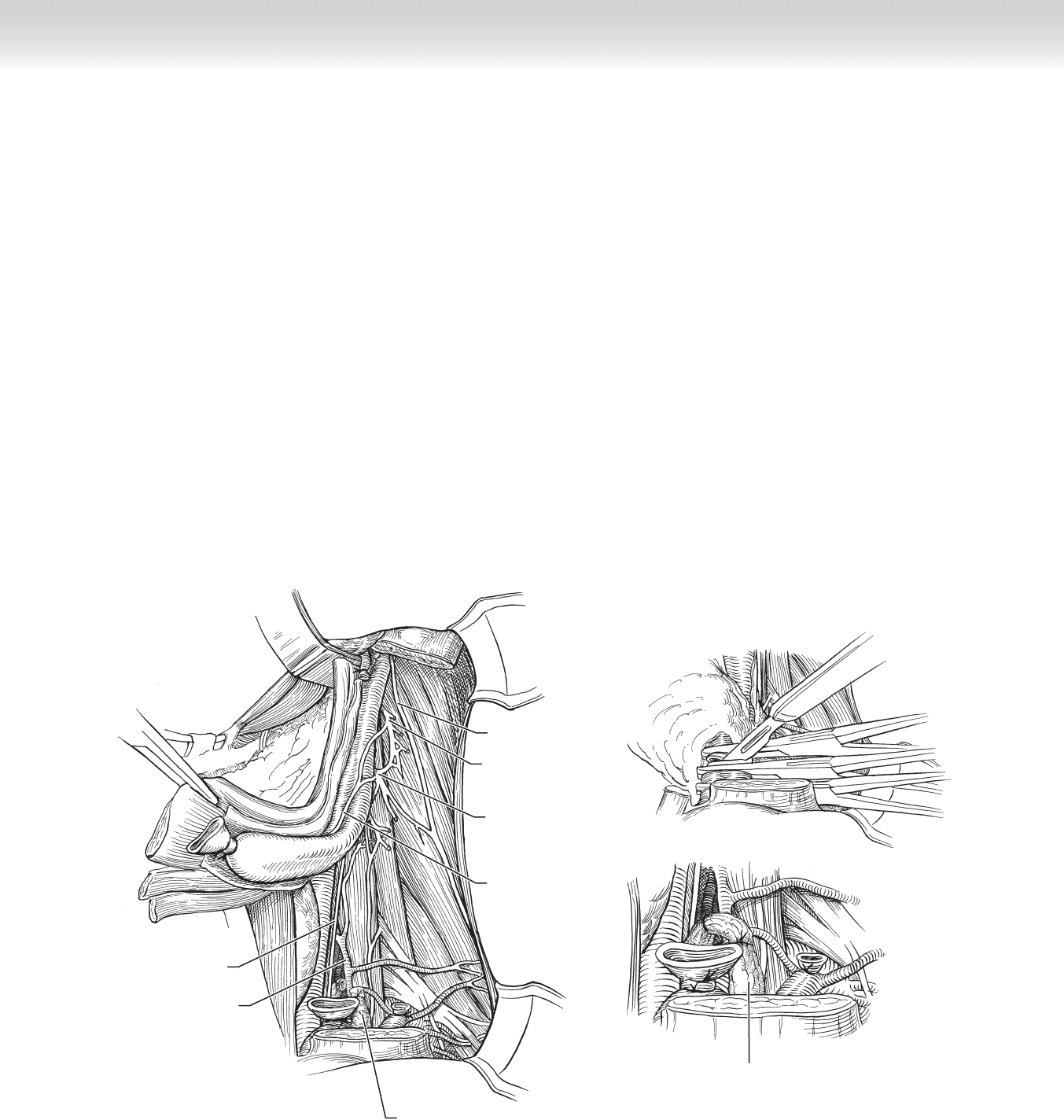
FIGURE 2 –21
◆ At this time, the IJV and the lymphatic pedicle containing the thoracic duct (accessory duct
on the right) are isolated and ligated. When clamping these structures, care is taken to
avoid dividing the vagus nerve (Figure 2-21, A).
◆ Careful circumferential dissection of the IJV inferiorly is done both sharply and bluntly to
avoid injury to the vein itself, the carotid artery, the sympathetic chain, and the vagus and
phrenic nerves. The proximal end of the vein is doubly clamped, and a single clamp is
placed on the distal end. The vein is transected between the second and third clamps, and
the proximal end is ligated using a 2-0 silk tie and a 2-0 silk suture ligature. The other end
is ligated with a single 2-0 silk tie (Figure 2-21, B).
◆ The thoracic duct can typically be seen at the lower lateral aspect of the IJV. It is very thin
walled, and extreme care in isolating the lymphatic pedicle is necessary to avoid inadver-
tent injury with chyle leak. The lymphatic pedicle is isolated and ligated (Figure 2-21, C).
A Valsalva maneuver at this time will assess for a leak.

36 Section I • Head and Neck and Endocrine Procedures
◆ The dissection now proceeds in a cephalad direction in a plane between the IJV and the
carotid sheath. The dissection also proceeds medially and superiorly along the anterior belly
of the omohyoid muscle. The hypoglossal nerve (located approximately 2 cm superior to
the carotid bifurcation) and the descendens hypoglossi branch are visible in the course of
dissection. Following the descendens hypoglossi branch superiorly will help in identifi ca-
tion of the hypoglossal nerve. Retraction of the posterior belly of the digastric muscle is
needed for visualization (Figure 2-22).
◆ The ranine veins lie lateral to the hypoglossal nerve and require ligation to avoid meddle-
some bleeding. Ligation of these vessels is done with the hypoglossal nerve under direct
visualization to avoid inadvertent injury to and/or transection of the nerve.
◆ The surgical specimen is now pedicled on the upper end of the IJV. The specimen is
fl ipped into its anatomic position, and the IJV is doubly clamped, transected, and ligated
using a 2-0 silk tie (Figure 2-23).
Cut ansa
hypoglossi
Hypoglossal
nerve
FIGURE 2 –22
Internal jugular vein
Retractor
Hypoglossal nerve
Omohyoid muscle
Posterior belly of
digastric muscle
FIGURE 2 –23
CHAPTER 2 • Modifi ed Radical Neck Dissection Preserving Spinal Accessory Nerve 37
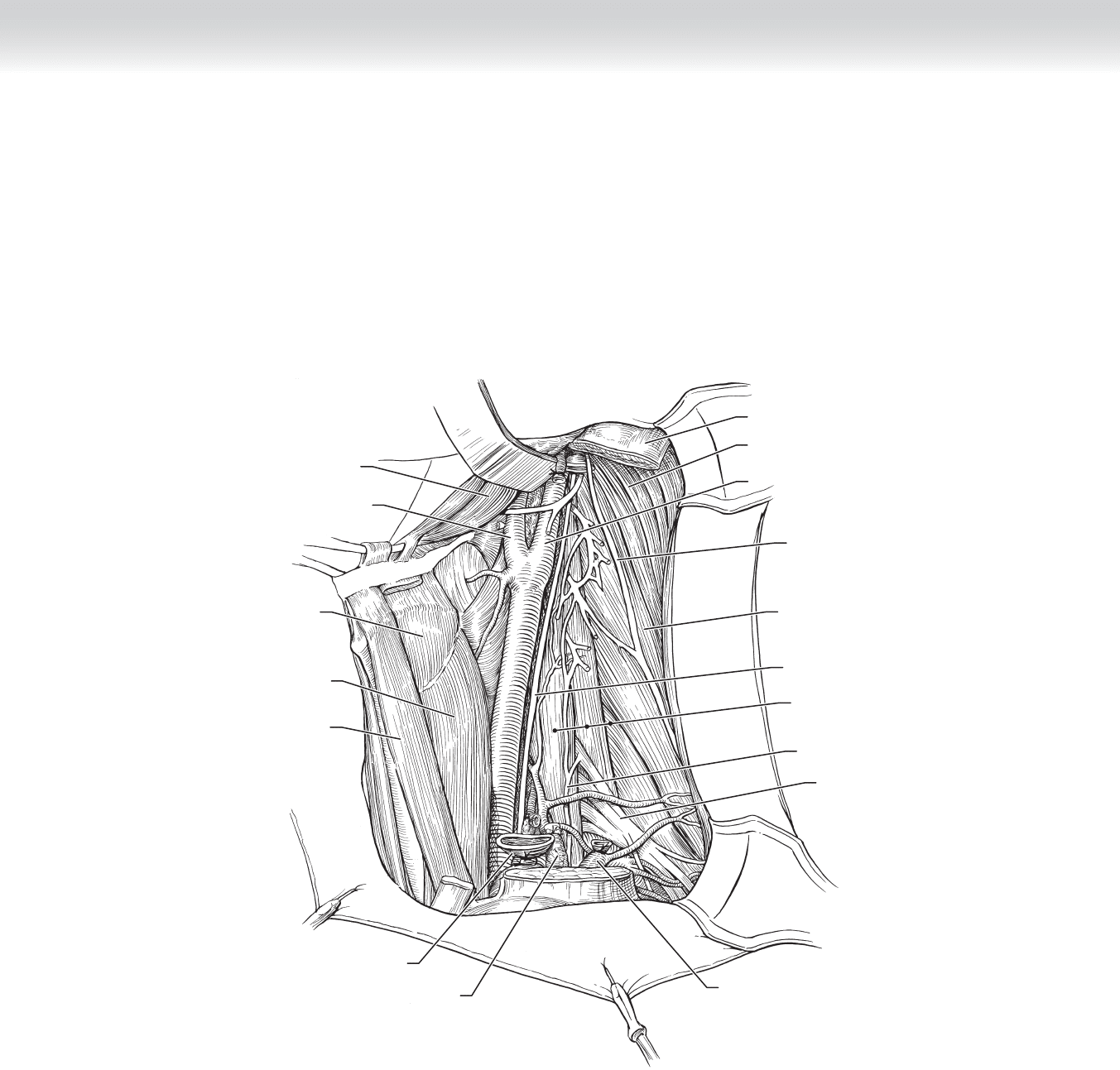
◆ As seen here, the SCM muscle, IJV, omohyoid muscle, and nodal levels 1-5 have been
removed, preserving the SAN (Figure 2-24).
◆ The surgical specimen is removed from the surgical fi eld, and each level of nodal dissection
is labeled for the pathologists.
Scalene muscle
Internal carotid artery
Sternocleidomastoid muscle
Accessory nerve
Levator scapulae muscle
Vagus nerve
Phrenic nerve
Scalene muscles
(anterior, middle, posterior)
Brachial plexus
External jugular vein
Sternothyroid
muscle
Sternohyoid
muscle
Thyrohyoid
muscle
External carotid artery
Digastric muscle
(posterior belly)
Internal jugular vein
Lymphatic pedicle
FIGURE 2 –24

38 Section I • Head and Neck and Endocrine Procedures
3. CLOSING
◆ A Valsalva maneuver is performed to check for a chyle leak.
◆ Meticulous hemostasis is obtained.
◆ The wound is copiously irrigated with normal saline.
◆ Two 10-mm Jackson-Pratt drains are placed into the wound through separate stab inci-
sions; one is placed posteriorly in the neck along the trapezius muscle and the other is
placed anteriorly in the neck, parallel to the strap muscles. To prevent suction on the
carotid artery, the drains may be loosely sewn to the fascia of the deep muscles of the neck
using an absorbable suture to hold them in place.
◆ The incision is closed in two layers; the platysma is tightly closed using an absorbable
stitch, and the skin is closed using surgical staples or suture.
◆ Antibiotic ointment only is applied to the incision. A pressure dressing is not applied (my
preference), because this increases risk of IJV occlusion in the contralateral neck.
STEP 4: POSTOPERATIVE CARE
◆ Perioperative antibiotics are given for 24 hours only if the upper aerodigestive tract was entered.
◆ Head of bed is elevated to 45 degrees to reduce edema.
◆ Neck drains are placed on low continuous wall suction for 2 days, then switched to bulb suc-
tion. The nursing staff is required to “strip” the drains every shift to prevent occlusion of the
drain from fi brinous debris.
◆ Neck incision is cleaned twice daily (bid) and as needed (prn) with half-strength hydrogen
peroxide and saline. Following this, antibiotic ointment is then applied to the neck incision
bid. This is discontinued after 3 days.
◆ Drains are individually removed when output is 20 mL or less per 24 hours.
◆ Routine tracheotomy care is performed if one is present (see Chapter 5).
◆ Physical therapy is initiated following drain removal. Exercises for range of motion in neck
and upper extremities and strengthening exercises for upper extremities are ordered.
◆ Speech and swallowing evaluation is particularly important for patients who underwent
tracheotomy, resection of the primary tumor, and/or previous radiation therapy.
◆ Staples are removed on postoperative day 7. If the patient has previously received radiation
therapy, the staples remain for 10 to 12 days.

CHAPTER 2 • Modifi ed Radical Neck Dissection Preserving Spinal Accessory Nerve 39
STEP 5: PEARLS AND PITFALLS
◆ Posterior belly of the digastric muscle is considered the “resident’s friend”; there are no
important structures lateral to it, and the contents of the carotid sheath are deep to it.
This is a very important landmark.
◆ The omohyoid muscle lies lateral to the carotid sheath, brachial plexus, and phrenic nerve.
It is also considered the “resident’s friend” and is a very important landmark.
◆ The skin fl aps in a previously irradiated patient should be raised sharply, or a Shaw knife
should be used to decrease chance of skin necrosis.
◆ The marginal mandibular nerve is most commonly injured where it courses near the angle
of the mandible.
◆ If there is a question intraoperatively as to whether the tumor can be dissected off of the
carotid artery, proximal and distal control of the vessel should be obtained and vessel
loops placed before dissection of the area in question.
INTRAOPERATIVE COMPLICATIONS
◆ “Button hole” of posterior skin fl ap
◆ Injury to brachial plexus (sensory and motor defi cits in upper extremity) and cranial
nerves: marginal mandibular (weakness in lower lip), hypoglossal (weakness/atrophy
hemitongue), vagus (aspiration, dysphonia), phrenic (elevated hemidiaphragm, respiratory
compromise), and spinal accessory (shoulder droop, chronic pain)
◆ Injury to cervical sympathetic chain (Horner syndrome)
◆ Chyle leak: If this occurs, the thoracic duct is ligated and fi brin glue and Gelfoam are
placed over the repair. Loupe magnifi cation is helpful in this situation.
◆ Laceration of the IJV: Small laceration of the vein can typically be repaired with a vascular
suture of 6-0 nylon. If the laceration is too large to repair, the vein is sacrifi ced. This causes
a problem in the case of bilateral neck dissections only if the contralateral IJV must be
sacrifi ced because of tumor. If laceration of the vein occurs at the skull base, bleeding can
be stopped by packing the area with Gelfoam and applying pressure or suturing the stump
to the digastric muscle. If laceration occurs near the thoracic inlet, the assistance of a
thoracic surgeon may be necessary to control the bleeding, and an air embolus may occur.
◆ Injury to the subclavian vein
◆ Air embolus through open cervical veins is rare (“gurgle” heard via precordial stetho-
scope and blood pressure drops). If this occurs, the patient is immediately placed in the
left lateral position and the central line is aspirated. If a central line is not present, one
should be immediately placed. If there is no time, direct left ventricular puncture should
be attempted.

40 Section I • Head and Neck and Endocrine Procedures
◆ Hemorrhage resulting in transfusion
◆ Bradycardia due to carotid dissection/retraction: If this occurs, all dissection stops and 1%
plain lidocaine is injected into the adventitia in the area of the carotid bulb.
◆ CVA: Many patients with head and neck cancer also suffer from atherosclerotic disease,
with plaque noted in the carotid arteries on preoperative imaging. Careful retraction of the
carotid artery during neck dissection will lessen the risk of an embolic event and CVA.
◆ Carotid artery injury resulting in CVA or death: This type of injury is rare and can occur
when tumor is closely dissected from the artery, or when the artery is ectatic in its course
(particularly in the elderly).
POSTOPERATIVE COMPLICATIONS
◆ Hematoma
◆ Seroma
◆ Visible scar on neck
◆ Blood loss anemia
◆ Wound infection
◆ Chyle fi stula: Milky drainage in the suction bulb or high output drainage is indicative of a
chyle leak. Drain fl uid can be sent for triglyceride level if necessary to confi rm the diagnosis.
This is treated with a pressure dressing and a medium-chain triglyceride diet. Intravenous
hyperalimentation may be necessary. If high output continues, neck exploration is indicated.
◆ Weakness and chronic shoulder pain
◆ Skin fl ap necrosis, with or without carotid artery exposure
◆ If the carotid artery is exposed, immediate coverage using a fl ap is mandatory to prevent
carotid “blowout.” A pectoralis major myocutaneous fl ap is typically used.
◆ Carotid blowout: This occurs when the carotid artery becomes exposed because of skin
necrosis or if it is bathed with saliva from a fi stula that develops following resection of
the primary tumor. The ABCs of resuscitation are as follows: If the patient is stable, a
bilateral carotid artery arteriogram is obtained and the artery may be embolized or
stented radiographically. An unstable patient is taken immediately to the operating room
for ligation of the carotid artery. Carotid blowout is often preceded by a “herald” bleed.
A herald bleed is manifested by sudden onset of bright red blood coming from the neck
wound or the tracheotomy site that is brief in duration. This is a warning and allows the
surgeon time to assess the carotid artery system via arteriogram.
◆ Persistent/recurrent tumor

CHAPTER 2 • Modifi ed Radical Neck Dissection Preserving Spinal Accessory Nerve 41
SELECTED REFERENCES
1. Eibling DE: Neck dissections. In Myers EN (ed): Operative Otolaryngology Head and Neck Surgery.
Philadelphia, Saunders, 1997, pp 676-718.
2. Peters GE, Price JC, Johns ME: Cervical lymphadenectomy. In Johns ME, Price JC, Mattox DE (eds): Atlas
of Head and Neck Surgery. Philadelphia, BC Decker, 1990, pp 378-411.
3. Crile G: Excision of cancer of the head and neck with special reference to the plan of dissection based on
132 operations. JAMA 1906; 47:1780.
4. Head and neck sites. In Greene FL, Page DL, Fleming ID, et al (eds): AJCC Cancer Staging Manual,
6th ed. New York, Springer, 2002, pp 17-22.
5. Martin H, Del VB, Ehrlich H, Cahan WG: Neck dissection. Cancer 1951; 4:441.

42
CHAPTER
3
Parathyroidectomy
B. Mark Evers
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the anatomy of the neck is critical (see Figure 1-1). In
addition, a thorough knowledge of the embryology and development of the parathyroid
glands is important to understand where in the neck or mediastinum the parathyroid gland
may lie, based on normal embryologic descent of the superior and inferior glands.
◆ Whereas bilateral neck explorations are still being performed for hyperparathyroidism,
more endocrine surgeons are choosing to localize the abnormal gland before surgery as a
result of improvements in imaging techniques over the past decade. Several noninvasive
preoperative localization modalities are available including Technetium-99m sestamibi
scintigraphy, ultrasonography, computed tomography (CT), magnetic resonance imaging
(MRI), and most recently, four-dimensional CT and positron emission tomography. These
studies have been used with great success for parathyroid localization preoperatively. This
allows for more directed operation and a smaller incision. Figure 3-1 illustrates an
abnormally enlarged right inferior parathyroid gland.
Normal superior left
parathyroid gland
Normal inferior left
parathyroid gland
Normal superior right
parathyroid gland
Abnormally enlarged
inferior right
parathyroid gland
FIGURE 3–1
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Criteria for surgical referral, as noted by the National Institutes of Health workshop in
2002, include: serum calcium concentration greater than 1 mg/dL above the upper limits of
normal, 24-hour urinary calcium greater than 400 mg, creatinine clearance reduced by
greater than 30% in comparison with age-matched subjects, bone density greater than
2 standard deviations below peak bone mass, all individuals with hyperparathyroidism and
age younger than 50 years, and patients for whom medical surveillance is either undesir-
able or impossible. In addition, all patients who are symptomatic from their hypercalcemia
should be referred for surgical management.
◆ Preoperative localization is imperative before primary exploration if unilateral exploration
is desired. As noted previously, this can be accomplished by one of several noninvasive
techniques.
STEP 3: OPERATIVE STEPS
1. INCISION
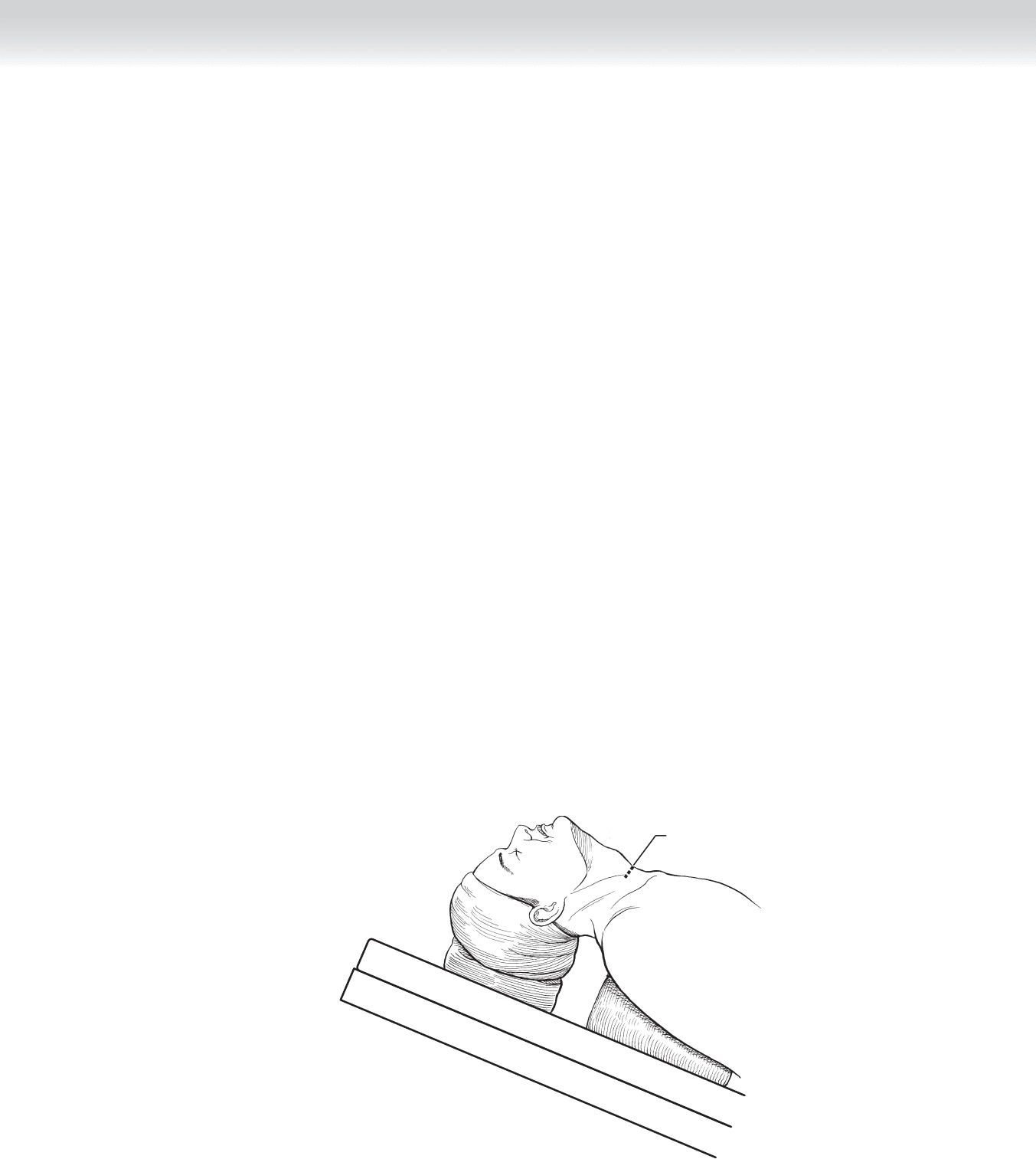
◆ Proper positioning of the patient is critical for adequate exposure. This is normally
accomplished by hyperextension of the neck using a rolled sheet between the shoulder
blades. The head is supported with a foam rubber doughnut-shaped ring. In addition, the
patient is usually placed in the semierect (semi-Fowler) position (Figure 3-2).
Incision
MC
FIGURE 3–2
CHAPTER
3
• Parathyroidectomy 43
44 Section I • Head and Neck and Endocrine Procedures
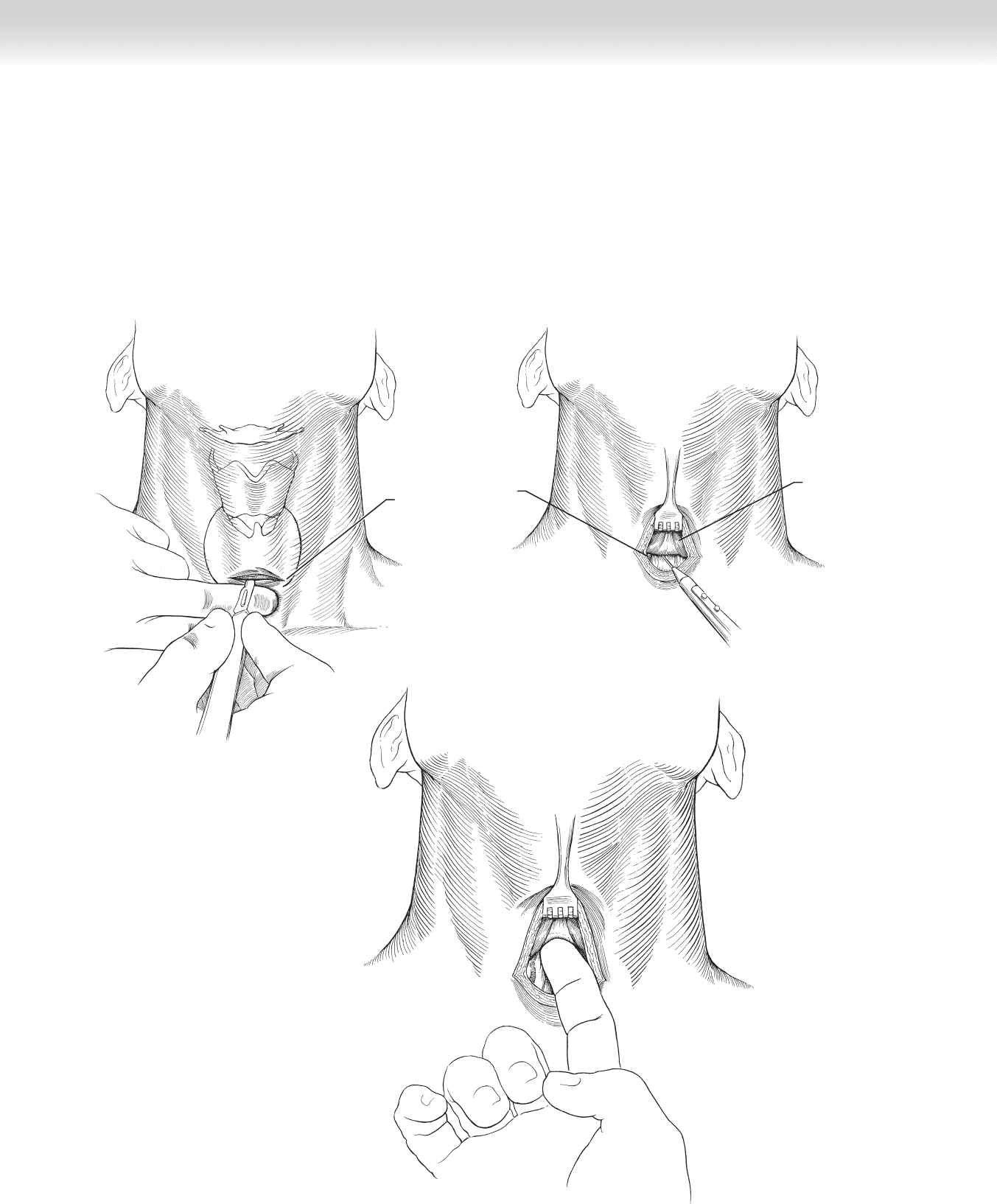
◆ If unilateral dissection is planned, the incision can be smaller than required for bilateral
exploration. The incision extends through the subcutaneous tissue, and the platysma
muscle is divided using electrocautery (Figure 3-3). Flaps are then mobilized superiorly
and inferiorly using the cautery, as well as blunt dissection, just deep to the platysma
muscle (Figures 3-4 and 3-5). The fl aps do not need to be extended superiorly and inferi-
orly as one would do for a thyroid resection, but only enough to allow adequate exposure
and placement of retraction.
Platysma muscle
Right anterior
jugular vein
Incision
FIGURE 3 –3
FIGURE 3 –4
FIGURE 3 –5