Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

CHAPTER 39
Procedures Used to Augment
the Deficient Alveolar Ridge
MASSIMO SIMION
General considerations
Case reports
Alveolar ridge augmentation for single tooth
restoration in the anterior maxilla
Alveolar
ridge augmentation for implant
restoration in
the anterior maxilla
Alveolar ridge augmentation for implant
restoration
of multiple adjacent maxillary teeth Vertical ridge
augmentation in the anterior area of
the mandible
Vertical ridge augmentation to allow implant
placement in the posterior segments of the
mandible
A variety of surgical techniques used for horizontal
and vertical ridge augmentation have been described
by different authors (e.g. Buser et al. 1990, 1993, 1995,
1996, Nevins & Mellonig 1992, 1994, Mellonig & Tri-
plett 1993, Lang et al. 1994, Rominger & Triplett 1994,
Simion et al. 1994, 1998, Tinti et al. 1996, Tinti &
Parma-Benfenati 1998). Such procedures often include
the use of autogenous bone grafts or grafts including
different biomaterials as well as the placement of bar-
rier membranes (guided bone regeneration (GBR), see
Chapter 38). In the present chapter, ridge augmenta-
tion techniques will be described that can be per-
formed either before or in combination with implant
placement and that include the use of autogenous
bone grafts.
GENERAL CONSIDERATIONS
All ridge augmentation procedures should be per-
formed in a proper surgical setting and in patients
with a dentition free of signs of destructive periodon-
titis. Before the surgical session, the perioral skin must
be cleaned with the use of a disinfectant. The patient
must rinse his or her mouth for 2 minutes with a 0.12
-
0.2% solution of chlorhexidine gluconat. The patient
is subsequently covered with sterile sheets to mini-
mize bacterial contamination from extraoral sites. The
surgical procedure is in most cases performed on a
lightly sedated patient and under local anesthesia.
Flap design
A full thickness crestal incision is placed within the
keratinized mucosa of the edentulous ridge. In a par-
tially dentate patient the crestal incision is extended
into an intrasulcular incision — mesially and/or dis-
tally — to involve one or two adjacent teeth. Vertical
releasing incisions are made at the mesial and distal
ends of the crestal incision. In order to get proper
access to the surgical site the releasing incisions are
frequently made in buccal as well as in lingual (pala-
tal) direction.
Initial preparation of the recipient site
A meticulous preparation of the recipient site is crucial
for the successful outcome of a ridge augmentation
procedure. Thus, following placement of the incisions,
the buccal and palatal (lingual) flaps are reflected with
the use of an elevator, to allow a proper exposure of
the surgical site. During flap elevation care must be
taken not to damage the palatine artery, and the men
-
tal nerve in patients with a severely reabsorbed max-
illa and/or mandible. Further, the soft tissue flaps
must be handled gently to minimize trauma and to
avoid perforations and lacerations.
Once exposed, the cortical bone at the recipient site
is curetted with a chisel to remove all remnants of
granulation tissue and portions of adherent pe-
riosteum.

898 • CHAPTER 39
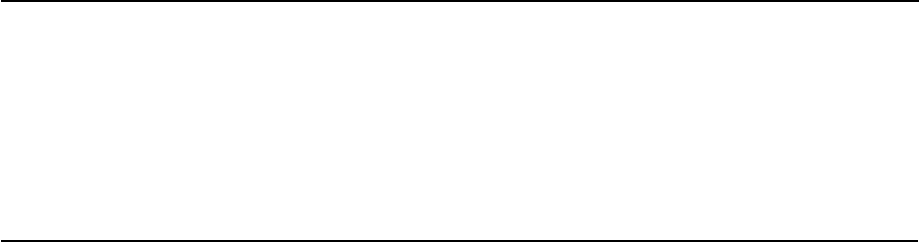
Fig. 39-1. A full thickness flap was elevated in the ra
-
mus of the mandible. The osteotomy was performed
with the use of trephines.
Positioning of the barrier membrane
The barrier membrane most frequently used in ridge
augmentation procedures is made of expanded
polytetrafluoroethylene (e-PTFE; Gore-Tex, W.L. Gore
Ass., Flagstaff, AZ, US) and often the titanium rein-
forced variety of the e-PTFE membrane (TR GTAM;
Gore-Tex, W.L. Gore Ass., Flagstaff, AZ, USA) is
placed to obtain optimal stability of the wound in the
recipient site.
Mini-screws made of stainless steel (or titanium)
are often used to support the membrane in the center
of the defect. The mini-screws are, thus, positioned in
the recipient site and left to protrude from the bone
surface at the intended height of the new bone. As an
alternative to the use of mini-screws, a block of auto-
genous bone can be placed to stabilize the membrane.
The bone block must be firmly anchored to the bone
of the recipient site with fixation screws.
Before the placement of graft material, the cortical
bone of the recipent site must be perforated with a
round bur to expose the cancellous bone and induce a
bleeding hard tissue surface (Rompen et al. 1999).
When a titanium reinforced e-PTFE membrane is
used, the barrier is adjusted with the use of pliers and
adapted to the intended shape of the augmented
ridge. The membrane is trimmed with scissors and
adjusted to extend at least 4-5 mm beyond the margins
of the defect.
Once positioned at the surgical site, the membrane
is fixed to the
lingual/palatal
aspect of the bone crest
with mini-screws. This will allow the graft to be placed
in the recipient site from a buccal direction.
Fig. 39-2. The bone samples were collected with a Molt
curette.
Preparation of the donor site
Both
extraoral
and
intraoral
sites have been proposed
as possible donor sites for the harvesting of auto-
genous bone.
The use of
extraoral
sites, including the iliac crest,
the tibia and the calvaria, allows the harvesting of
large volumes of bone. The use of such donor sites,
however, (1) increases the morbidity associated with
the procedure, and (2) requires general anesthesia and
often the hospitalization of the patient
The most frequently used
intraoral
donor sites in-
clude:
1.
the ramus (the retromolar region)
2.
the symphysis of the mandible.
Before bone is harvested, a comprehensive clinical
and radiographic examination (a panoramic radio-
graph is generally, but not always, sufficient) of the
intraoral donor site must be performed. In this exami
-
nation the following issues must be considered:
1.
the position of the alveolar nerve in relation to the
bone crest
2.
the position of the mental foramen in relation to an
obvious landmark (e.g. a neighboring tooth)
3.
the length of the roots and the position of the apices
of the mandibular incisors in relation to the lower
border of the mandible
4.
the volume of bone that can be harvested.
Surgical procedure in the region of the ramus
Bone collection from the mandibular ramus is nor-
mally performed only when the third molar is missing
PROCEDURES USED TO AUGMENT THE DEFICIENT ALVEOLAR RIDGE •
8
99
and when only a limited amount of bone is required
to
graft the recipient site.
A crestal incision is made. The incision should start
about 2-3 mm distal of the second molar and be ex-
tended in distal and lateral direction following the
lateral margin of the ramus. A vertical releasing inci-
sion is made at the mesial aspect of the crestal incision.
After the elevation of a full thickness flap, the osteo-
tomy can be accomplished with the use of trephines
or
thin carbide burs. Bone harvesting must be carried out
in a gentle and careful manner and during irriga
tion
of the surgical site with sterile saline (Figs. 39-1,
39-2).
The dimension (amount) of the bone graft that
can be
harvested is dependent on (1) the buccal-lin
gual
dimension of the ramus, and (2) the position of the
inferior alveolar nerve. Thus, at least 3 mm of intact
bone must remain over the alveolar nerve to
avoid
neurological complications. It is also essential
not to
penetrate the lingual wall of the ramus region
and
thereby sever blood vessels in this region.
When a particulate bone graft is harvested, the
round osteotomies — prepared with a trephine —
should overlap in order to reduce the size of each
individual hard tissue block, and to facilitate their
collection and grinding. After the bone collection pro-
cedure is completed, the flaps are replaced and closed
with interrupted sutures.
Surgical procedure in the region of the
symphysis of the mandible
An incision is placed about 10 mm below the muco-
gingival junction and is extended between the distal
aspect of the two mandibular canines. A full thickness
flap is elevated with a periosteal elevator and is re-
flected from the incision line to the inferior border of
the mandible.
When the intention is to prepare a particulate bone
graft, the osteotomy can be accomplished with me-
dium-sized trephines (8 mm diameter). During bone
sampling the surgical site is irrigated with saline. The
circular osteotomy cuts should overlap to facilitate the
removal of the bone tissue (see above). The depth of
each cut (<— 5-6 mm) must consistently be related to the
buccal-lingual dimension of the donor site (Figs. 39-3,
39-4). The apical limit of the bone harvesting is located
5 mm coronal to the inferior border of the chin. The
coronal limit of the osteotomy is 5 mm apical of the
apex of the anterior teeth, and the lateral limit is 5 mm
mesial to the mental foramen (Hunt & Jovanovic
1999). The bone harvesting is normally made with a
curette. The small hard tissue portions are subdivided
into small bone chips.
When the intention is to harvest a block of bone, a
bone saw can be used to prepare a rectangular shaped
graft of desired dimensions (Figs. 39-5, 39-6).
Before wound closure, a collagen sponge is placed
as hemostatic agent in the donor site. This sponge will
reduce postoperatory swelling and hematoma forma-
Fig. 39-3. Round osteotomies were made with the use
of an 8 mm diameter trephine. The cuts overlapped
and reached a depth of 5-6 mm.
Fig. 39-4. The bone samples were removed and the can
-
cellous bone was collected with the use of a surgical
spoon.
Fig. 39-5. A rectangular cut was performed with a bone
saw to collect a large bone block.
Fig. 39-6. The bone block was removed and additional
round cuts were prepared with the trephine. The round
bone samples will be ground with the use of a bone
mill to obtain bone chips.

900 • CHAPTER 39
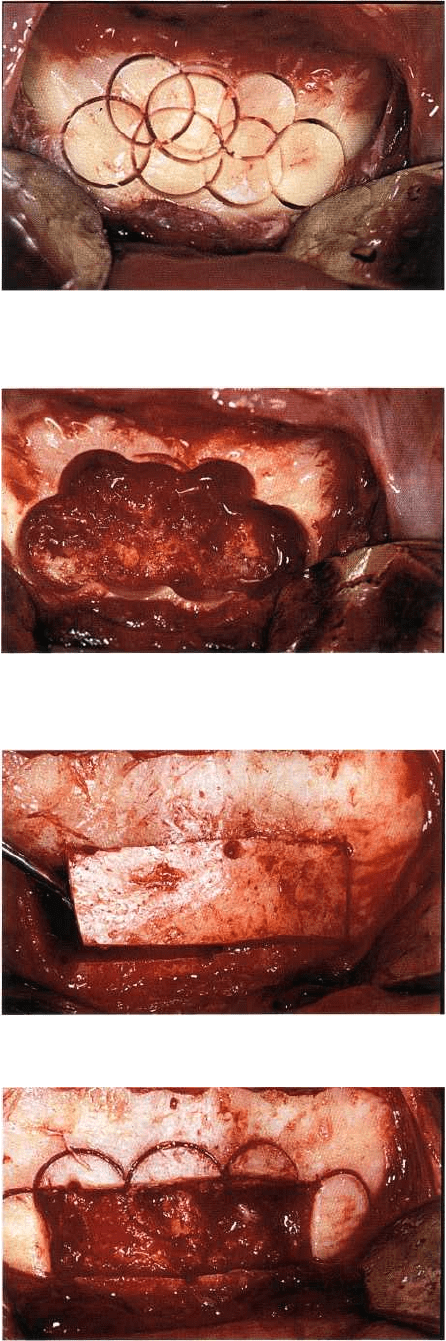
Fig. 39-7. (a) 39-year-old patient exhibiting an implant-supported restoration of tooth 21. The esthetic appearance
was compromised by the
"
overcontoured" crown. (b) Palatal aspect of the same crown.
tion. The closure of the flaps includes a two-layer
suturing technique, one internal and one external su-
ture. For the internal suture a resorbable suture mate
-
rial is used. The internal suture often has the design of
a horizontal mattress and is intended to close the
periosteum and the severed muscles. For the external
suture, that is intended for closure of the incision
wounds, a non-resorbable material is used. A continu
-
ous or an interrupted suturing technique may be
adopted.
During the immediate post-operative period (10
days) most patients will experience some swelling and
discoloration of the chin area. Paresthesia of the lower
anterior tooth region can persist for periods exceeding
6 months.
Positioning of the bone graft in the recipient
site
The barrier membrane is first anchored to the lingual
bone wall of the defect with mini-screws. After the
harvesting of the small bone blocks and the prepara-
tion of bone chips (particulated graft), the graft parti-
cles are packed on the perforated hard tissue surface
of the bone crest of the recipient site. The membrane
is subsequently adjusted to cover the graft and is
finally anchored to the buccal bone wall with mini-
screws placed at the mesiobuccal and distobuccal
rims. This will provide optimal stability of the mem-
brane and ideal protection of the grafts.
In regions where the recipient site is located close
to a natural tooth, a 2 mm wide zone of crestal bone
next to the tooth must be left uncovered by the mem-
brane so that the graft and the membrane will not
interfere with the periodontal tissues of the natural
tooth.
Closure of the recipient site
Releasing incision
Before the wound is closed, a releasing incision must
be made in the periosteum at the base of the buccal
flap (sometimes also of the lingual/palatal flap) to
facilitate soft tissue management and to achieve a
tension-free soft tissue adaptation. The periosteal in-
cision must join the vertical releasing incisions at the
mesial and distal margins of the flap. Particular atten
-
tion must be paid when such releasing incisions are
placed in the lower jaw in order to avoid damage of
the
inferior alveolar nerve at its exit from the mental
foramen. Moreover, the incisions at the lingual aspect
of the mandible must be placed so as to avoid damage
of the vascular plexa at the floor of the mouth.
Suturing
Wound closure is often accomplished with horizontal
mattress sutures, alternated with interrupted sutures.
Horizontal mattress sutures are applied to achieve
proper flap position. Interrupted sutures are placed
between the mattress sutures and to close the vertical
releasing incisions.
Postoperative care
After the completion of the procedure, the patient
should receive an antibiotic to prevent infection and
an anti-inflammatory agent to reduce edema and
swelling, for a period of about 1 week.
Chemical plaque control including the use of chlor-
hexidine mouth rinses (0.12% solution twice a day) is
instituted for 2 weeks. The sutures are removed after
12-15 days. The e-PTFE membrane is usually removed
after 6 months of healing. Implants may then be
placed in the augmented ridge, according to direc-
tions provided in the manual for the different implant
systems used.
PROCEDURES USED TO AUGMENT THE DEFICIENT ALVEOLAR RIDGE • 901
CASE REPORTS
Patient 1 - Alveolar ridge augmentation for
single tooth restoration in the anterior
maxilla
The 39-year-old man expressed concern about the
esthetic outcome of an implant-supported restoration
that had been placed in the maxillary left central inci-
sor region. The patient also complained about the
bulky palatal surface of the same restoration (Fig.
39-
7a,b). The patient was in good general health and was
a non-smoker.
Initial examination
The patient's natural dentition was in good condition
and he had a comparatively good oral hygiene status.
Tooth 21 presented with an implant-supported crown
made of porcelain fused to metal that was overcon-
toured both at its buccal and lingual aspects (Fig. 39-8).
The peri-implant mucosa exhibited signs of inflam-
mation.
The reason why the restoration had been overcon-
toured by the prosthodontist was, most likely, the
improper position of the implant in the ridge between
the natural teeth. In fact, during surgery the implant
had been placed too far palatally as compared to the
position of the adjacent teeth. The gingiva at the buccal
aspect of tooth 11 and tooth 22 exhibited modest re-
cession (Fig. 39-7a).
Treatment planning
During treatment planning different options were
considered:
1.
removal of the implant and placement of a conven-
tional three-unit bridge
2.
placement of a Maryland bridge restoration
3.
removal of the implant, reconstruction of the soft
and hard tissues at site 21 and subsequently
de novo
implant installation and crown restoration.
The different treatment options were explained to the
patient. Option 3 was selected.
Treatment
Initial therapy
The patient was instructed in proper plaque control
procedures. After flap elevation, the implant in site 21
was removed with the use of a calibrated trephine. The
flap was repositioned coronally and closed with inter-
rupted sutures.
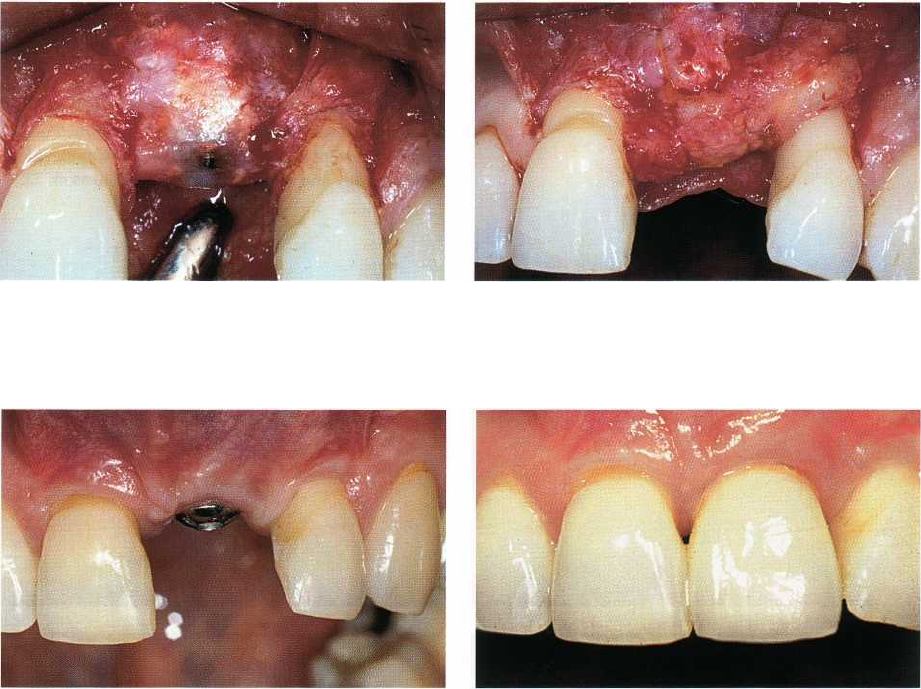
Implant placement and bone regeneration
After 2 months of healing following implant removal,
buccal and lingual full thickness flaps were elevated.
The flaps extended from tooth 11 to tooth 22 (Figs. 39-
9, 39-10) and were released with vertical incisions
Fig.
39-8.
The artificial crown was removed. It was pos
-
sible to recognize the "overcontoured" surfaces on both
the buccal and the palatal aspect of the crown.
Fig.
39-9. After implant removal and 2 months of heal
-
ing, the site demonstrated the presence of a deep defect
in the bone. Also the soft tissue was compromised.
Fig.
39-10.
A full thickness flap was reflected both buc
cally and palatally, extending from tooth 11 to tooth
22.
placed at the distal line angle of teeth 11 and 22. The
bone surface was carefully curetted and all residual
soft tissue was removed from the defect.
An implant (13 mm long) was placed in a proper
position with the implant shoulder 3 mm apical of the
free gingival margin of the adjacent teeth. This re-
sulted in an implant exposure outside the buccal bone
housing of about 8 mm (Fig. 39-11).
A reinforced e-PTFE membrane was adapted and
fixed palatally with the use of titanium pins. A par-
ticulated bone graft was collected from the retromolar
902 • CHAPTER 39
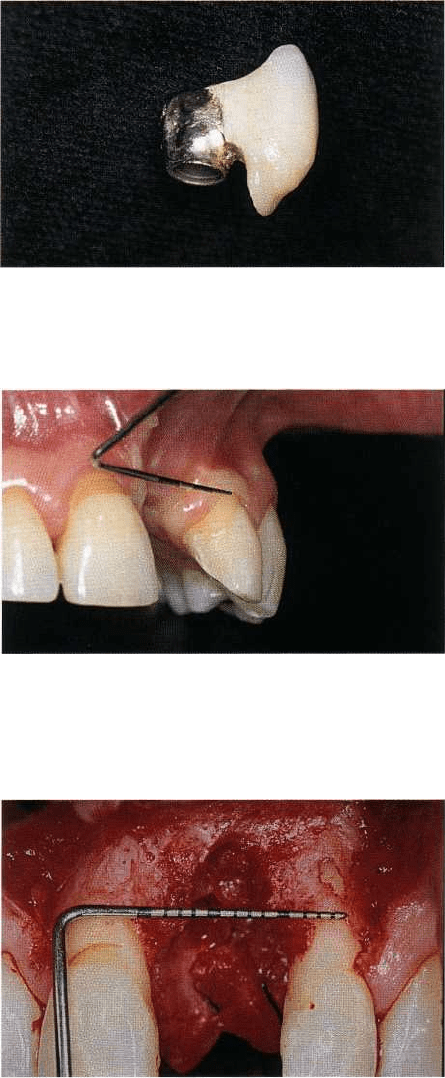
Fig. 39-11. An implant was placed with the shoulder lo-
cated 3 mm apical of the free gingival margin of the ad-
jacent teeth. This resulted in an implant exposure out-
side the buccal bone of about 8 mm.
Fig. 39-12. A particulated bone graft was collected from
the retromolar area in the mandible and was packed
into the bone defect.
Fig. 39-13. A titanium reinforced e-PTFE membrane
was placed and stabilized buccally and palatally with
titanium pins.
Fig. 39-14. The periosteum of the buccal flap was in-
cised and released in order to augment the flap mov-
ability before wound closure.
Fig. 39-15. The wound closure was performed with
horizontal mattress and interrupted suture.
Fig. 39-16. After 6 months of uneventful healing, the e
-
PTFE membrane was removed.
area in the mandible and was packed into the bone
defect (Fig. 39-12). The membrane was then anchored
to the buccal bone wall with two titanium pins (Fig.
39-
13).
The periosteum of the buccal flap was released in
order to augment the movability of the flap before the
wound was closed with horizontal mattress and inter-
rupted sutures (Figs. 39-14, 39-15).
Membrane removal and abutment connection
After 6 months of healing, the e-PTFE membrane was
removed and a connective tissue graft was placed on
top
of the regenerated bone to increase the thickness
of the
mucosa (Figs. 39-16, 39-17, 39-18). After another
2
months, the cover screw was exposed and connected to
a regular abutment (Fig. 39-19).
Restorative therapy
A provisional acrylic crown was prepared and in
serted
after one additional month of healing. The
emergence
profile of the crown was modified repeat
edly during the
next 6 months to condition the soft
PROCEDURES USED TO AUGMENT THE DEFICIENT ALVEOLAR RIDGE • 903
Fig. 39-17. A thin layer of connective tissue could be
seen on the surface of the regenerated bone.
Fig. 39-18. A connective tissue graft was placed on top
of the regenerated bone to increase the thickness of the
mucosa.
Fig. 39-19. After 2 months the cover screw was exposed
and connected with a regular abutment.
Fig. 39-20. A Procera® made full porcelain crown was
inserted.
tissue, and finally a "Procera® crown" (Nobel Biocare,
Gothenburg, Sweden) was fabricated and inserted
(Fig.
39-20).
Concluding remarks
This case showed that GBR techniques can also be
effectively used for the treatment of peri-implant bone
defects in the anterior region of the maxilla. The treat-
ment included a series of surgical and prosthetic steps
but resulted in proper function and an optimal esthetic
outcome.
Patient 2 - Alveolar ridge augmentation for
implant restoration in the anterior maxilla
A 22-year-old man had been involved in a motorcycle
accident in which the two upper central incisors, to-
gether with the associated buccal bone plate had been
lost. The patient was otherwise in good general health
and was a non-smoker.
Initial examination
The patient presented with his natural dentition in
good condition. There were no clinical signs of perio-
dontitis and dental caries. The clinical findings were
confirmed in the radiographic examination. The oral
hygiene examination revealed the presence of modest
amounts of soft and hard supragingival deposits.
The upper central incisors were missing and the
edentulous ridge in this region was insufficient, both in
width and height, for implant installation. The
upper
lateral incisors were vital, exhibiting minute
crown
fractures that had been restored with compos
ite.
Treatment planning
The patient was informed about the lack of sufficient
bone tissue in the upper front tooth region. The differ-
ent treatment modalities that were available were de-
scribed. These included bone augmentation, implant
installation and crown restoration. Further, the antici-
pated long-term result and alternative treatment op-
tions were discussed.
After having evaluated the options, it was decided
that a ridge augmentation procedure including GBR
should be performed with subsequent implant place-
ment and prosthetic reconstruction.
Treatment
Initial therapy
This treatment included patient information, oral hy-
giene instruction and professional tooth debridement
904 • CHAPTER 39
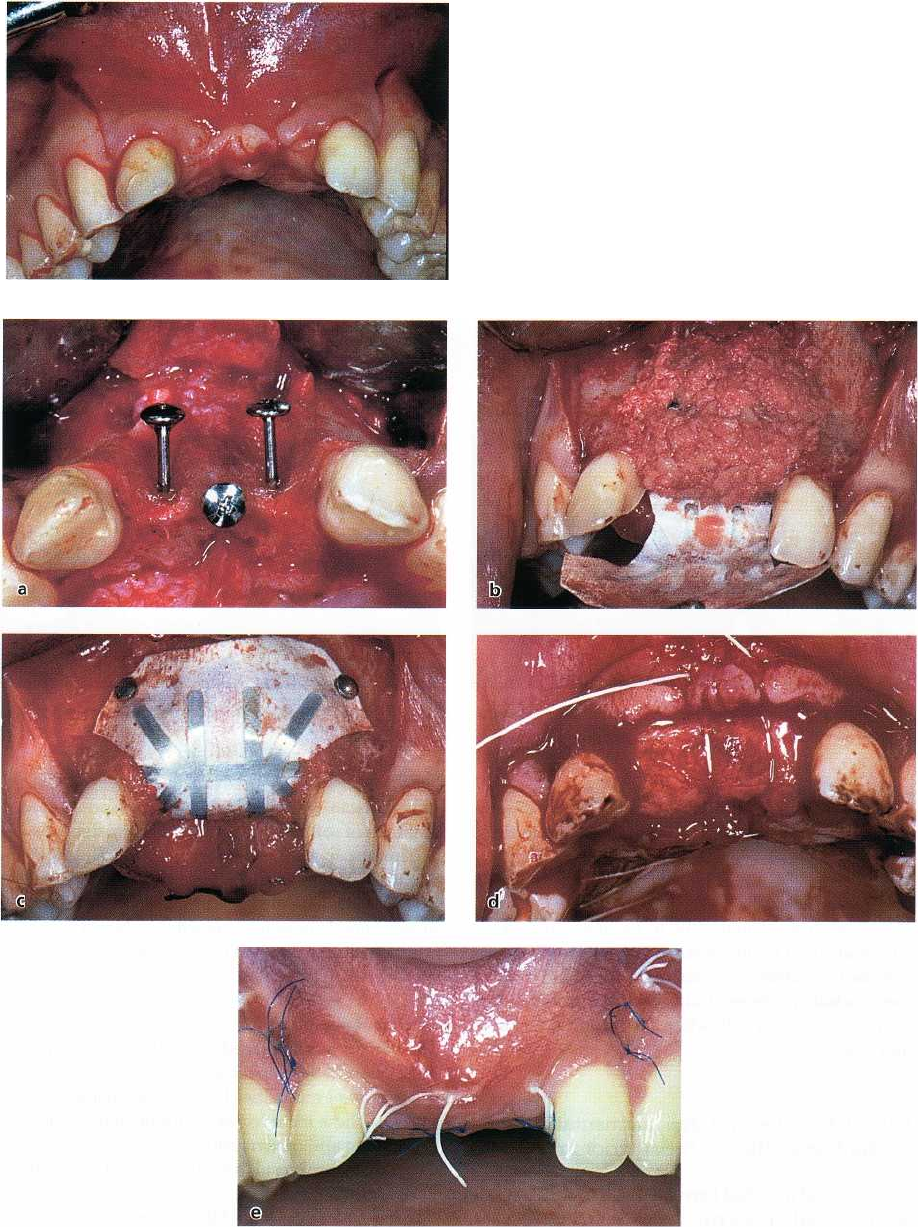
Fig. 39-21. A 22-year-old man had a motorcycle acci-
dent and the two upper central incisors and the buccal
bone plate were lost. A full thickness flap was elevated
both buccally and palatally from tooth 12 to tooth 22.
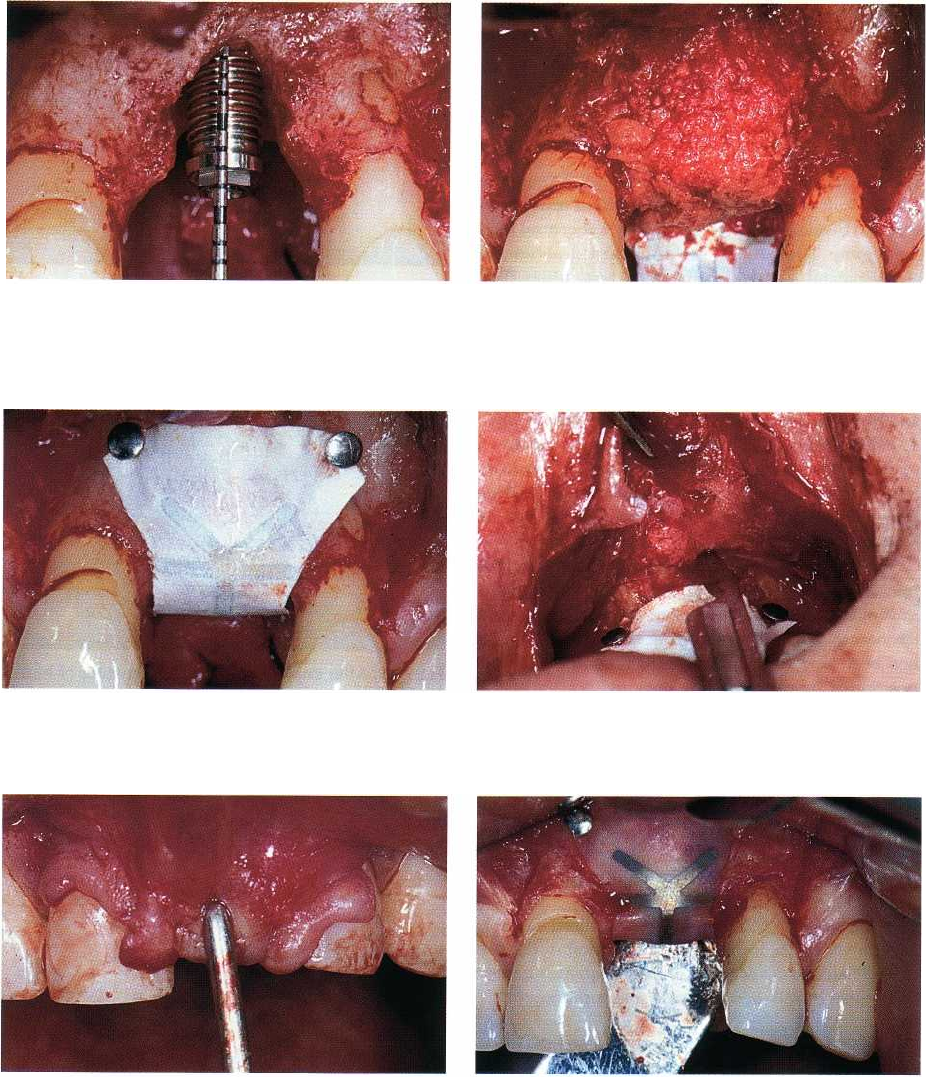
Fig. 39-22. (a) Three mini-screws were applied to the buccal defect and on top of the bone crest in order to support
a
membrane and to avoid its collapse into the defect. (b) A titanium reinforced e-PTFE membrane was adapted and
fixed to the palatal aspect of the edentulous bone crest with titanium pins. A particulate autogenous bone graft was
packed into the defect. (c) The membrane was anchored buccally with two titanium pins. (d) A connective tissue
graft
was harvested from the palate and positioned on top of the crest to augment the thickness of the mucosa. (e)
The
flaps were closed with horizontal mattress and interrupted sutures.
PROCEDURES USED TO AUGMENT THE DEFICIENT ALVEOLAR RIDGE • 905
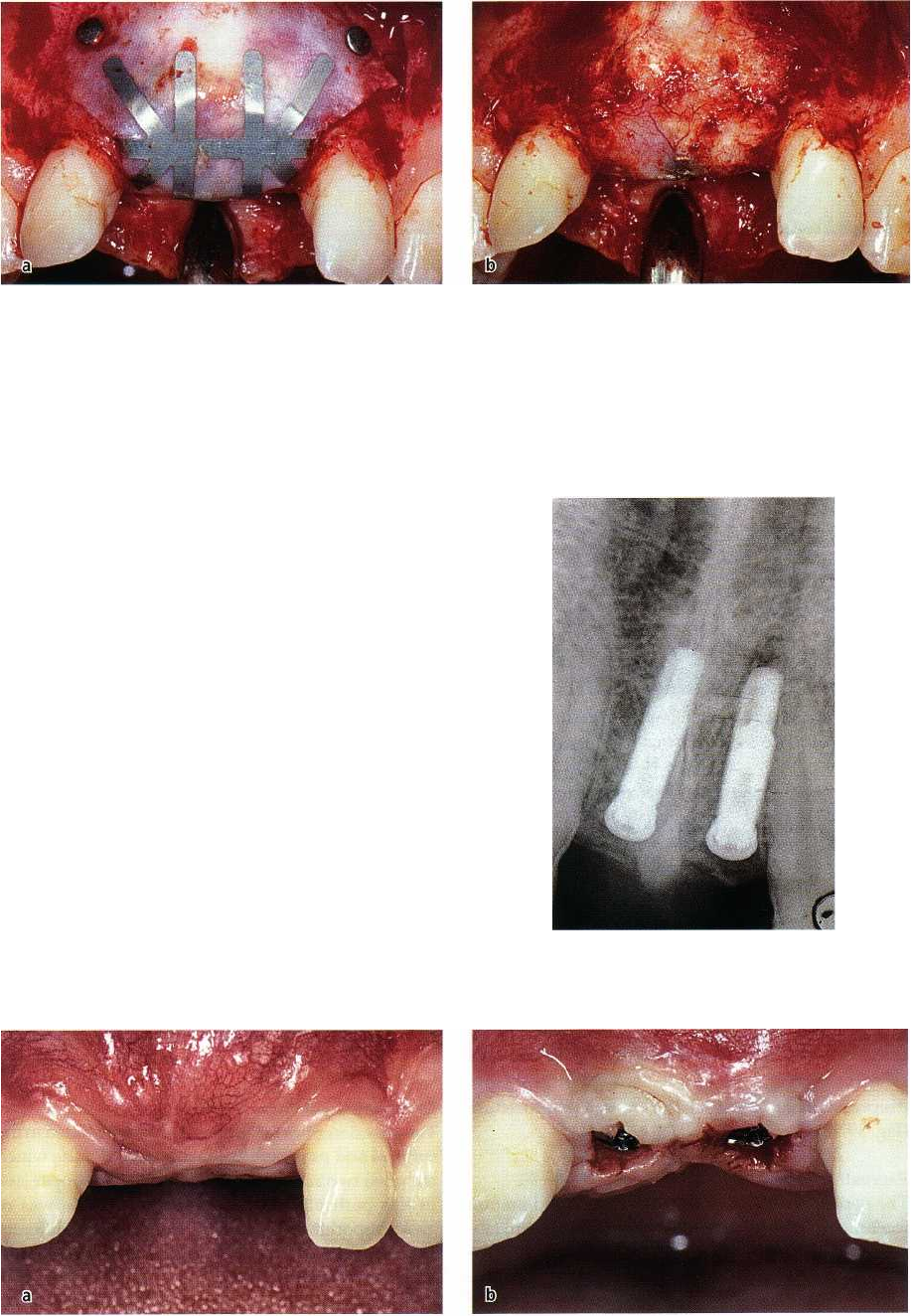
Fig. 39-23. (a) After 6 months of uneventful healing, a full thickness flap was elevated and the membrane exposed.
(
b) The membrane was removed. The mini-screws appear embedded in the regenerated bone.
A Maryland bridge was fabricated and inserted as a
provisional restoration in the upper incisor region.
Ridge augmentation
A full thickness flap was elevated both buccally and
palatally and extended from tooth 12 to tooth 22 (Fig.
39-21). A titanium reinforced e-PTFE membrane was
adapted and fixed to the palatal aspect of the edentu-
lous bone crest with titanium pins. Three mini-screws
were applied to the buccal defect and on top of the
bone crest in order to support the membrane and to
avoid its collapse into the defect (Fig. 39-22a). A par-
ticulated bone graft was collected from the mandibu-
lar symphysis region and placed in the ridge defect
(
Fig. 39-22b). The membrane was then fixed buccally
with two titanium pins (Fig. 39-22c). A connective
tissue graft was harvested from the palate and posi-
tioned on top of the crest to augment the thickness of
the soft tissue (Fig. 39-22d). Releasing incisions were
placed in the periosteum and the flaps were closed
with horizontal mattress and interrupted sutures (Fig.
39-22e). The sutures were removed after 2 weeks.
Membrane removal and implant placement
After 6 months of uneventful healing, a full thickness
flap was elevated and the membrane, pins and screws
were removed (Fig. 39-23a,b). Two 13 mm long im-
plants were placed in region 11 and 21 (Fig. 39-24).
After 6 months, abutment connection was per-
formed (Fig. 39-25a,b). In addition, the fornix was
Fig. 39-24. Two 13 mm long implants were placed in re
gion 11 and 21.
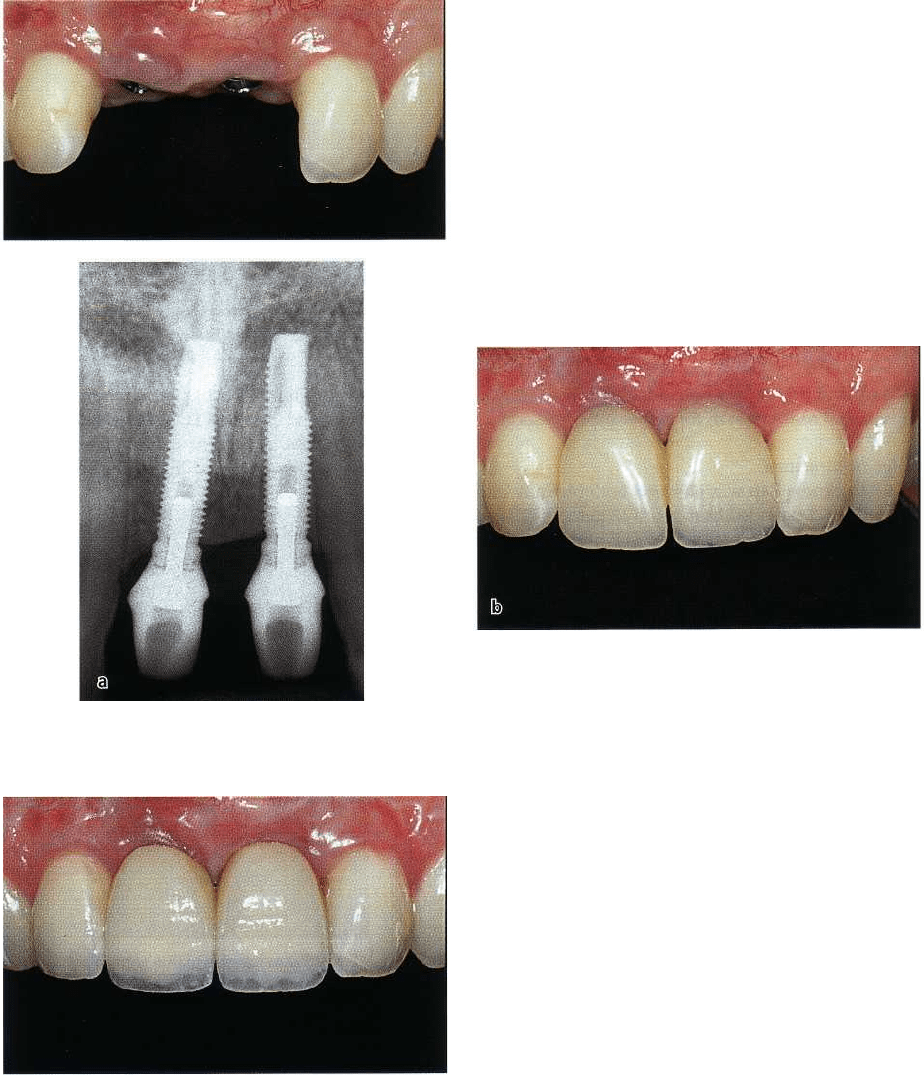
Fig. 39-25. (a)After 6 months of healing, the abutment connection was performed. (b) Two healing abutments were
placed.
906 • CHAPTER 39
Fig.
39-26.
The fornix was deepened with a partial
thickness flap. After one month the mucosa had healed.
Fig.
39-27.
(a) Periapical radiograph demonstrating the amount of new bone formation as well as the provisional
restoration. (b) Two acrylic crowns were inserted.
Fig.
39.28.
The final prosthetic restoration including
two independent (porcelain fused to metal) crowns,
was placed after 4 months of soft tissue
conditioning.
deepened using a partial thickness flap procedure
(Fig.
39-26).
Restorative therapy
The peri-implant tissues were left to heal and mature
for 1 month before two provisional crowns were fab-
ricated and inserted (Fig. 39-27a,b). The final pros-
thetic restorations, including two single crowns (por-
celain fused to metal), were placed after 4 months of
soft tissue maturation (Fig. 39-28).
The patient was incorporated in a supportive care
program that included recall appointments every 6
months.
Concluding remarks
This case describes the different phases included in the
surgical and prosthetic reconstruction of a site which
included two adjacent missing teeth in the upper jaw.
In this particular case the esthetic outcome was of
great importance. Therefore, a number of different
procedures were required to reconstruct both the hard
and the soft tissues.