Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

CHAPTER
29
Treatment of
Furcation-Involved Teeth
GIANFRANCO CARNEVALE, ROBERTO PONTORIERO AND JAN LINDHE
Therapy
Scaling and root planing
Furcation plasty
Tunnel preparation
Root separation and resection (RSR)
Regeneration of furcation defects
Extraction
Prognosis
Terminology
Anatomy
Diagnosis
Differential diagnosis
Detailed knowledge of the morphology of the multi-
rooted teeth and their position in the dental arch is a
fundamental prerequisite for a proper understanding
of problems which may occur when such teeth be-
come involved in destructive periodontal disease. The
first part of this chapter therefore includes a brief
description of some important anatomic features of
the root complexes and related structures of premolars
and molars.
TERMINOLOGY
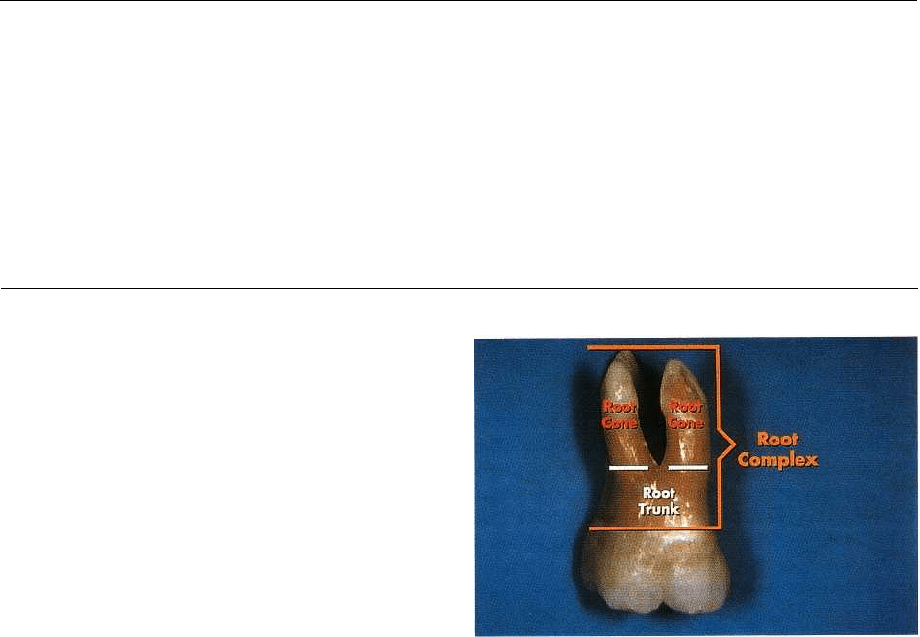
Root complex
is the portion of a tooth that is located
apical of the cemento-enamel junction (CEJ), i.e. the
portion that normally is covered with a root cemen-
turn. The root complex may be divided into two parts:
the
root trunk
and the
root cone(s)
(Fig. 29-1).
The
root trunk
represents the
undivided region
of the
root. The height of the root trunk is defined as the
distance between the CEJ and the separation line (fur
-
cation) between two root cones (roots). Depending on
the position of the separation line the height of the root
trunk may vary from one surface to the next in one
given molar or premolar.
The
root cone is
included in the
divided region
of the
root complex. The root cone (root) may vary in size
and position and may at certain levels be connected to
or separated from other root cones. Two or more root
Fig. 29-1. Root complex of a maxillary molar. The root
complex is separated into one undivided region: the
root trunk, and one divided region: the (3) root cones.
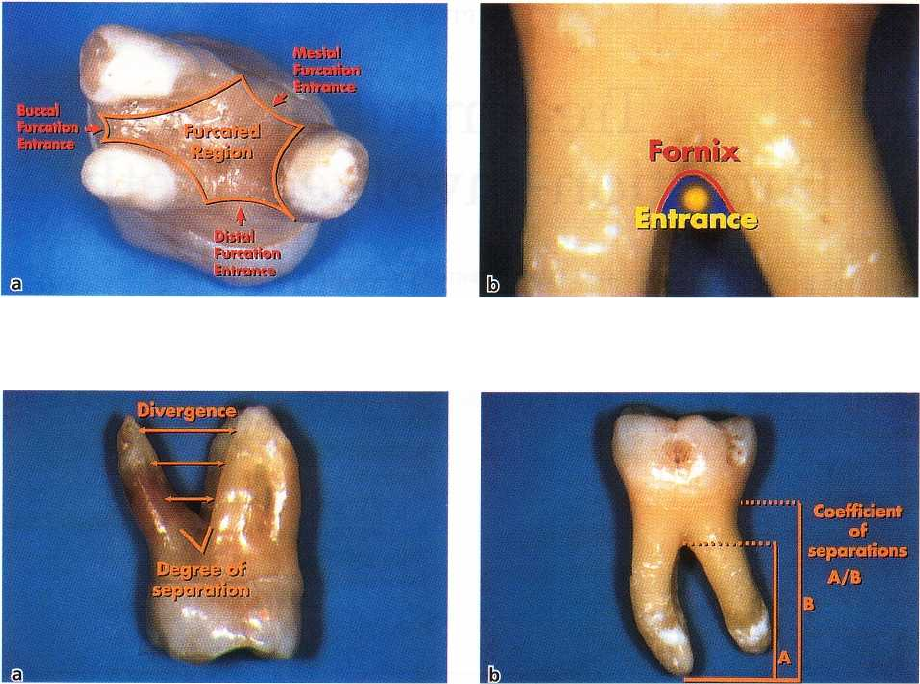
cones make up the
furcated region
of the root complex
(Fig. 29-2a).
The
furcation
is the area located between individual
root cones.
Furcation entrance:
the transitional area between the
undivided and the divided part of the root (Fig. 29-
2a,
b).
Furcation fornix:
the roof of the furcation (Fig. 29-2b).
Degree of separation:
the angle of separation between
two roots (cones) (Fig. 29-3a).
Divergence is
the distance between two roots; this
distance normally increases in apical direction (Fig.
29-3a).
706 • CHAPTER 29
Fig. 29-2. Apical-occlusal view of a maxillary molar where the three root cones make up the furcated region and the
three furcation entrances (a). A buccal view of the furcation entrance and of its roof (b).
Fig. 29-3. Photographs illustrating the angle (degree) of separation and the divergence between the mesiobuccal
and the palatal roots of a maxillary molar (a). The coefficient of separation (A/B) of the illustrated mandibular mo
lar is 0.8 (A = 8 mm; B = 10 mm).
Coefficient of separation:
the length of the root cones
in relation to the length of the root complex (Fig.
29-3b)
.
Fusion between divergent root cones may occur.
The fusion may be complete or incomplete. In the case
of an incomplete fusion, the root cones may be fused
in the area close to the CEJ but separated in a more
apical region of the root complex.
ANATOMY
Maxillary molars
As a general rule the maxillary first molar, in all re-
spects — crown and individual roots — is larger than the
second molar, which in turn is larger than the third
molar.
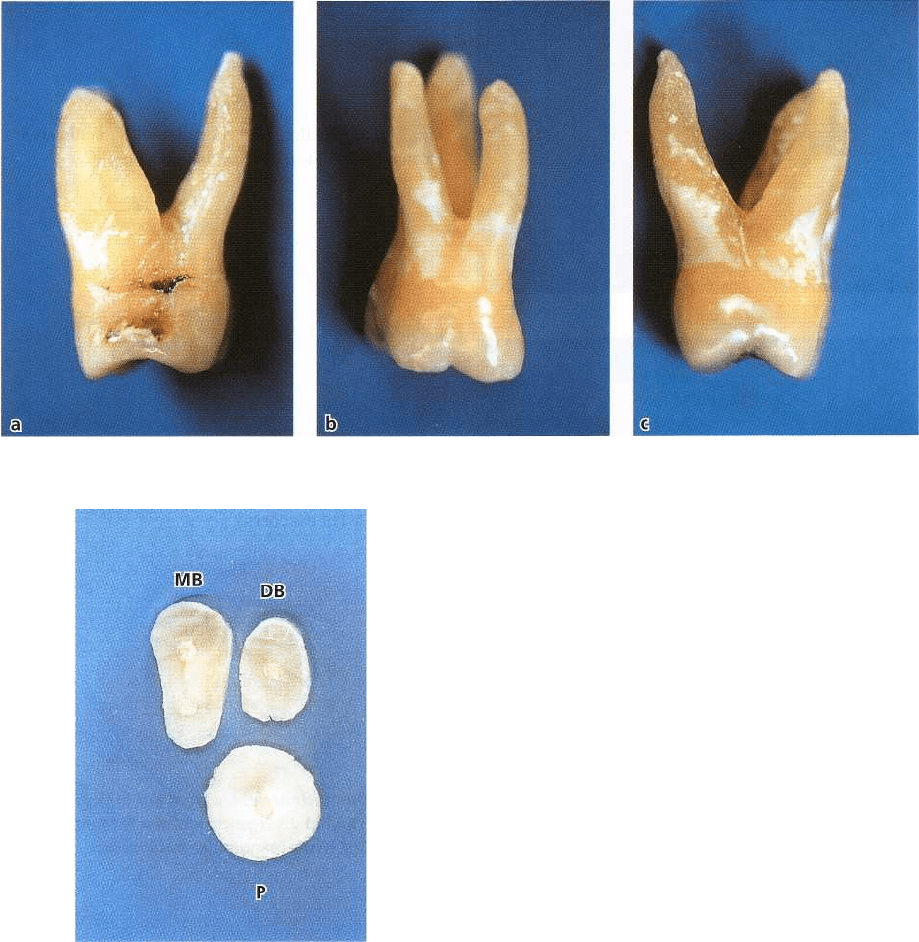
The first and second molars most often have three
roots; one mesiobuccal, one distobuccal and one pala-
tal. The mesiobuccal root is normally vertically posi-
tioned while the distobuccal and the palatal roots are
inclined. The distobuccal root projects distally and the
palatal root projects in palatal direction (Fig. 29-4a-c).
The cross-sections of the distobuccal and the palatal
roots are generally circular. The palatal root is gener
ally wider in mesiodistal than in buccopalatal direc-
tion. The distal surface of the mesiobuccal root has a
concavity which is about 0.3 mm deep (Bower
1979a,
b). This concavity gives the cross-section of the
mesiobuccal root an "hour-glass" configuration (Fig.
29-5).
The three furcation entrances of the maxillary first
and second molars vary in width and are positioned at
varying distances apical of the CEJ. As a rule, the
first
molar has a shorter root trunk than the second
molar.
In the first molar the mesial furcation entrance is
located about 3 mm from the CEJ, while the buccal
is
3.5 mm and the distal entrance about 5 mm apical
of
CEJ (Abrams & Trachtenberg 1974, Rosenberg
1988).
This implies that the furcation fornix is inclined;
in the
mesiodistal plane the fornix is comparatively
close to
CEJ at the mesial but closer to apex at the distal
surface.
The buccal furcation entrance is narrower
than its
distal and mesial counterparts.
The degree of separation between the roots and
their
divergence decreases from the first to the second,
and
from the second to the third maxillary molar.
The mesiobuccal root of the first molar is frequently
located more buccally in the arch than the distobuccal
root. If the buccal bone plate is thin, the mesiobuccal
root frequently projects through the outer surface of
TREATMENT OF FURCATION-INVOLVED TEETH •
707
Fig. 29-4. Furcation entrances (a, mesial; b, buccal; c, distal) and the position of the roots of a maxillary first molar.
Fig. 29-5. Root-shape of a maxillary first molar in a
horizontal cut at the level of the coronal third of the
cones. Note the circular shape of the palatal root in
comparison with the mesiodistally compressed shape
of the mesiobuccal root, which also exhibits a concav
-
ity in the distal aspect.
the alveolar bone and bone fenestrations and/or de-
hiscences may occur.
Maxillary premolars
In about 40% of cases the maxillary first premolars
have two root cones — one buccal and one palatal, and
hence a mesiodistal furcation. A concavity (about 0.5
mm deep) is often present in the furcation aspect of
the
buccal root. The furcation is in many cases located
in
the middle or in the apical third of the root complex (
Fig. 29-6). The mean distance between CEJ and the
furcation entrance is about 8 mm. The width of the
furcation entrance is about 0.7 mm.
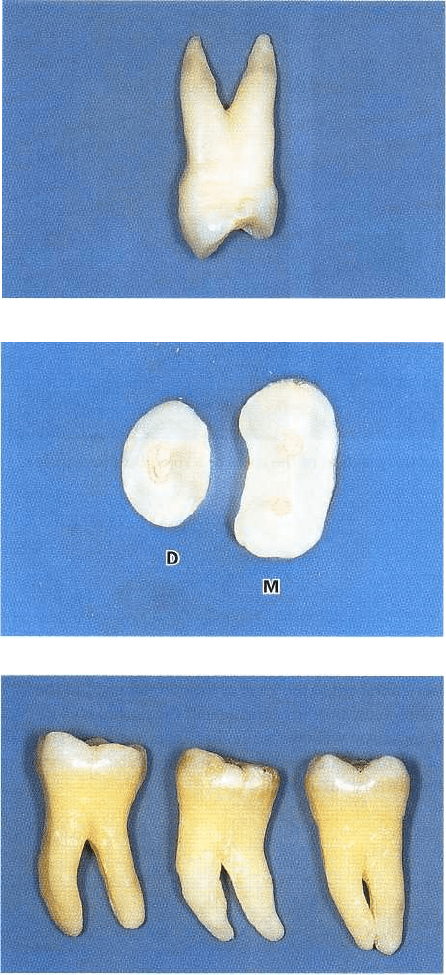
Mandibular molars
The mandibular first molar is larger than the second
molar, which in turn is larger than the third molar. In
the first and second molars the root complex almost
always includes two root cones, one mesial and one
distal. The mesial root is larger than the distal. The
mesial root has a position which is mainly vertical
while the distal root projects distally. The mesial root
is
wider in the buccolingual direction and has a larger
cross-section area than the distal root. The cross-sec-
tion of distal root is circular while the mesial root has
an "hour-glass" shape. In addition, on the distal sur-
face of the mesial root, furrows and concavities often
occur (Fig. 29-7). The distal concavity of the mesial
root
is more pronounced than that of the distal root
(Bower
1979a,b, Svardstrom & Wennstrom 1988).
The root trunk of the first molar is often shorter than
the trunk of the second molar. The furcation entrances
of the mandibular first molar, similar to those of the
maxillary first molar, are located at different distances
from the CEJ. Thus, the lingual entrance is frequently
found more apical of CEJ (> 4 mm) than the buccal
708 •
CHAPTER
29
Fig. 29-6. A maxillary first premolar with the furcation
located in the apical third of the root complex.
Fig. 29-7. "Hour-glass" shape of the mesial root — with
a
concavity in the distal aspect — and the circular shape
of the distal root (horizontal section at the level of the
coronal third of the cones).
Fig. 29-8. From left to right, differences in degree of
separation and in divergence between the root cones
from the first to the mandibular third molar.
entrance (> 3 mm). Thus, the furcation fornix is in-
clined in the buccolingual direction. The buccal furca-
tion entrance is often < 0.75 mm wide while the lingual
entrance is > 0.75 mm in most cases (Bower 1979a,b).
The degree of separation and divergence between
the
roots decreases from the first to the third molar
(Fig. 29-
8).
It should also be observed that the buccal bone plate
is thinner outside the roots of the first than of the
second molar. Bone fenestrations and dehiscences are,
as a consequence, more frequent in the first than in the
second molar region.
Other teeth
Furcations may be present also in teeth which nor-
mally have only one root. In fact, two-rooted incisors
(Fig. 29-9a), canines (Fig. 29-9b) and mandibular pre-
molars may exist. Occasionally three-rooted maxillary
premolars (Fig. 29-10a) and three-rooted mandibular
molars can be found (Fig. 29-10b).
DIAGNOSIS
The presence of furcation-involved teeth in a peri-
odontal patient will influence the treatment plan (see
Chapter 19). The selection of procedures to be used in
the treatment of periodontal disease at multirooted
teeth
can first be made when the presence and depth
of
furcation lesions have been assessed. In this exami-
nation traditional measures of periodontal disease are
used (see Chapter 18) but special attention is paid to
TREATMENT OF FURCATION-INVOLVED TEETH •
709
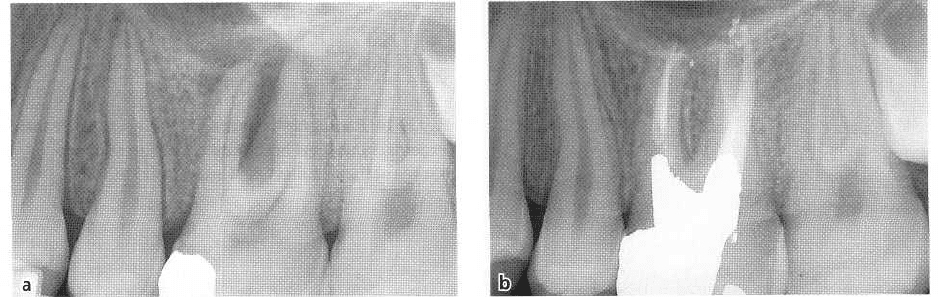
Fig. 29-9. Radiographs illustrating
morphologic variations repre-
sented by two-rooted (a) maxil-
lary lateral incisor and (b)
mandibular canine.
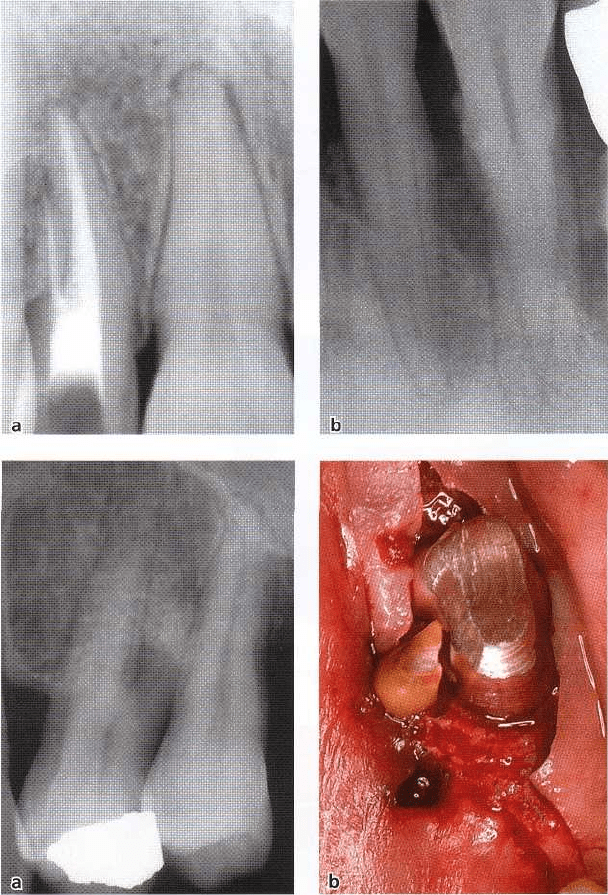
Fig. 29-10. Anatomic variation rep
-
resented in a radiograph of a
three-rooted mandibular first pre
-
molar (a). Clinical photograph il-
lustrating, during surgery, the
separation — before extraction — of
an "abnorma
l
"
second mesial root
of a mandibular molar (b).
findings from clinical
probing
and analysis of
radio-
graphs
from the premolar-molar regions.
The classification description of the involved furca-
tion is based on the amount of periodontal tissue
destruction that has occurred in the interradicular
area, i.e. degree of "horizontal root exposure" or at-
tachment loss that exists within the root complex.
Hamp et al. (1975) has suggested the following classi-
fication of the involved furcation:
•
Degree I: Horizontal loss of periodontal support not
exceeding
1
/3
of the width of the tooth (Fig. 29-11a).
•
Degree II: Horizontal loss of periodontal support
exceeding
1
/3
of the width of the tooth, but not
encompassing the total width of the furcation area
(Fig. 29-11b).
•
Degree III: Horizontal "through and through" de-
struction of the periodontal tissues in the furcation
area (Fig. 29-11c).
It is important to understand that each furcation en-
trance must be examined and each entrance must be
classified according to the above criteria.
Probing
The buccal furcation entrance of the
maxillary molars
and the buccal and lingual furcation entrances of the
mandibular molars
are normally accessible for exami-
nation using a curved graduated periodontal probe
(
Fig. 29-12a,b), an explorer or a small curette. The
examination of approximal furcations is more diffi-
cult, in particular when neighboring teeth are present.
Large contact areas between the teeth further impair
access to approximal furcation entrances.
In maxillary molars the mesial furcation entrance is
located much closer to the palatal than to the buccal
tooth surface. Thus, the mesial furcation should be
probed from the palatal aspect of the tooth (Fig. 29-13).
The distal furcation entrance of
a maxillary molar is
generally located midway between the buccal and
palatal surfaces and, as a consequence, this furcation
710 • CHAPTER
29
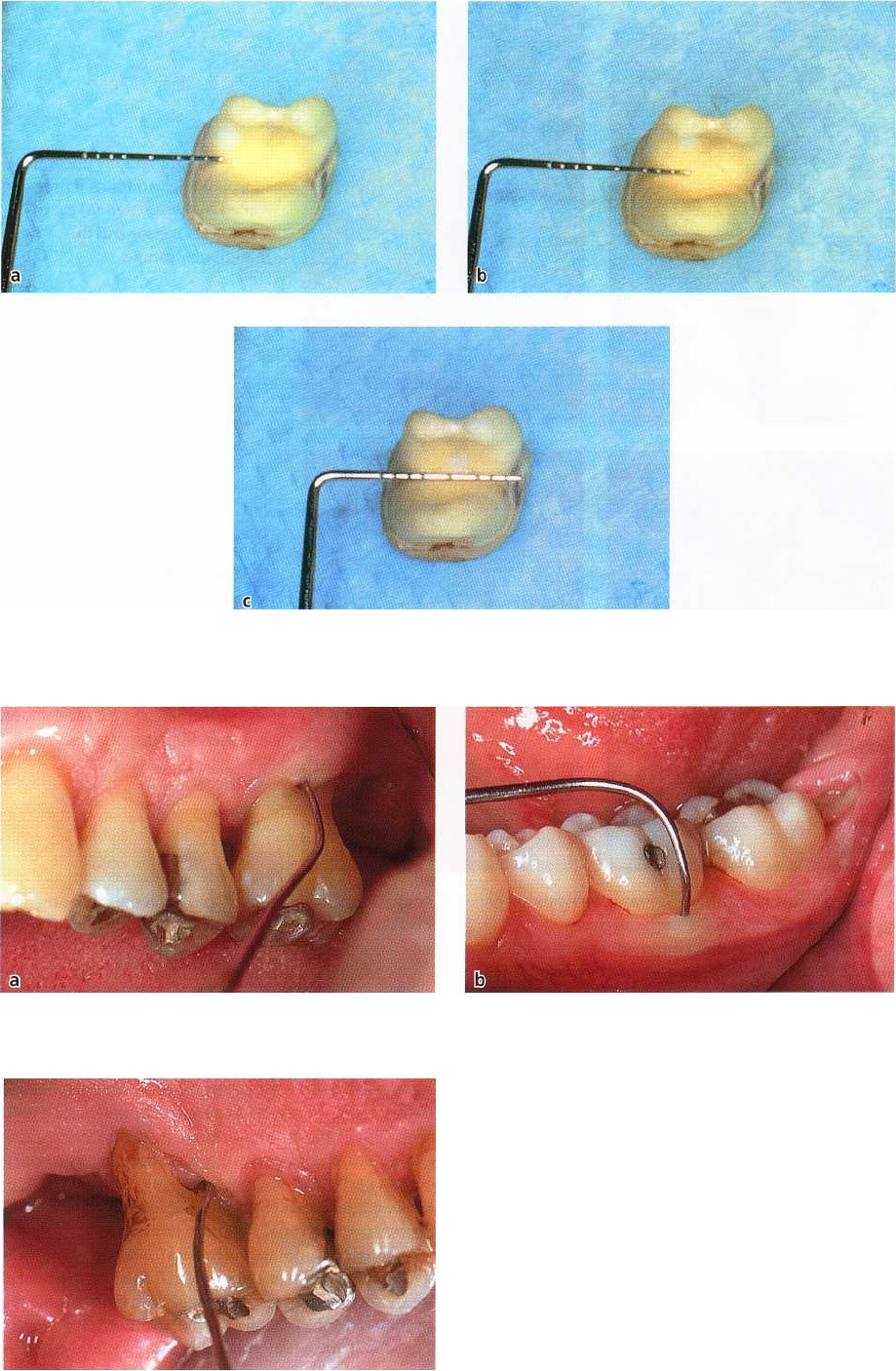
Fig. 29-11. Different degrees of furcation involvement in relation to the probe (penetration/superimposition) in the
interradicular space of a mandibular molar. (a) degree I; (b) degree II; (c) degree III.
Fig. 29-12. Easily accessible vestibular furcation entrances for probing of a (a) maxillary molar and (b) mandibular
molar.
Fig. 29-13. Common access for probing of a mesial fur-
cation entrance of a maxillary molar. The mesial furca-
tion entrance is generally located at the palatal aspect
of the tooth, while the distal entrance is located mid-
way between the buccal and the palatal surface.

TREATMENT
OF
FURCATION-INVOLVED
TEETH • 711
Fig. 29-14. Radiograph showing the location of the in
-
terdental bone level in relation to the furcation en-
trances of the maxillary first and second molar.
Fig. 29-15. Radiographs of the right maxillary molar region where, with a normal bisecting projection, the
furcation
defect of the first molar is not evident (a). It is, however, easily identified in a bitewing radiograph (b).
could be probed from either the buccal or the palatal
aspect of the tooth.
In
maxillary premolars
the root anatomy often varies
considerably. The roots may also harbor irregularities
such as longitudinal furrows, invaginations or true
furcations, which may open at varying distances from
the CEJ. Due to the above variations and due to the
limited access, the clinical assessment of a furcation
involvement in maxillary premolars is often difficult.
In some patients, a furcation involvement may, in such
teeth, first be identified after the elevation of a soft
tissue flap.
Radiographs
Radiographs must always be obtained to confirm
findings made during probing of a furcation-involved
tooth. The radiographic examination should include
both paralleling "periapical" and vertical "bite-wing"
radiographs. In the radiographs the location of the
interdental bone as well as the bone level within the
root complex should be examined (Fig. 29-14). Situ-
ations may occur when findings from clinical probing
and from the radiographs are inconsistent. Thus, the
localized but extensive attachment loss which maybe
detected within the root complex of a maxillary molar
with the use of a probe, will not always appear in the
radiograph. This may be due to the superimposition
in the radiograph of the palatal root and of remaining
bone structures (Fig. 29-15a). In such a case, additional
radiographs with different angles of orientation of the
central beam should be used to identify bone loss
within the root complex (Fig. 29-15b).
DIFFERENTIAL DIAGNOSIS
A lesion in the interradicular space of a multirooted
tooth may be associated with problems originating
from the root canal or be the result of occlusal over-
load. The treatment of a furcation-involved tooth,
therefore, should not be initiated until a proper differ
-
ential diagnosis of the lesion has been made.
Pulpal pathosis
may sometimes cause a lesion in the
periodontal tissues of the furcation (see Chapter 14).
The radiographic appearance of such a defect may
712 • CHAPTER 29
Fig. 29-16. Radiographs demonstrating a destruction of interradicular hone and the presence of periapical
defects
at the mesial and distal roots of a maxillary first molar (a). Radiographic appearance of complete healing
of the interradicular and periapical lesions after endodontic treatment (b).
have some features in common with a plaque-associ-
ated furcation lesion. In order to differentiate between
the two lesions the vitality of the affected tooth must
always
be tested. If the tooth is vital, a plaque-associ-
ated lesion should be suspected. If the tooth is non-vi
-
tal, the furcation involvement may have an endodon-
tic origin. In such a case, proper endodontic
treatment
must
always
precede periodontal therapy.
In fact, en
dodontic therapy may resolve the
inflammatory le
sion, soft and hard tissue healing
occur and the furca
tion defect disappear (Fig. 29-16a,
b). If signs of healing
of a furcation defect fail to
appear within 2 months following endodontic
treatment, the furcation in
volvement is probably
associated with marginal peri
odontitis.
Trauma from occlusion
Forces elicited by occlusal interferences, e.g. bruxers
and clenchers (see Chapters 15, 30), may cause inflam
mation and tissue destruction or adaptation within
the interradicular area of a multirooted tooth. In such
a tooth a radiolucency may be seen in the radiograph
of the root complex. The tooth may exhibit increased
mobility Probing, however, fails to detect an involve-
ment of the furcation. In this particular situation, oc
-
clusal adjustment must always precede periodontal
therapy. If the defects seen within the root complex are
of "occlusal" origin, the tooth will become stabilized
and the defects disappear within weeks following
correction of the occlusal overload (Fig. 29-17a,b).
THERAPY
Treatment of a defect in the furcation region of a
multi-rooted tooth is intended to meet two objectives:
1.
the elimination of the microbial plaque from the
exposed surfaces of the root complex
2.
the establishment of an anatomy of the affected
surfaces that facilitates proper self-performed
plaque control.
Different methods of therapy are recommended:
Furcation involvement degree I
Recommended therapy: Scaling and root planing.
Furcation plasty.
Furcation involvement degree II
Recommended therapy: Furcation plasty. Tunnel
preparation. Root resection. Tooth extraction. Guided
tissue regeneration at mandibular molars.
Furcation involvement degree III
Recommended therapy: Tunnel preparation. Root re-
section. Tooth extraction.
Scaling and root planing
Scaling and planing of the root surfaces in the furca-
tion entrance of a degree I involvement in most situ-
ations result in the resolution of the inflammatory
lesion in the gingiva. Healing will re-establish a nor-
mal gingival anatomy with the soft tissue properly
adapted to the hard tissue walls of the furcation en-
trance (Fig. 29-18a,b).
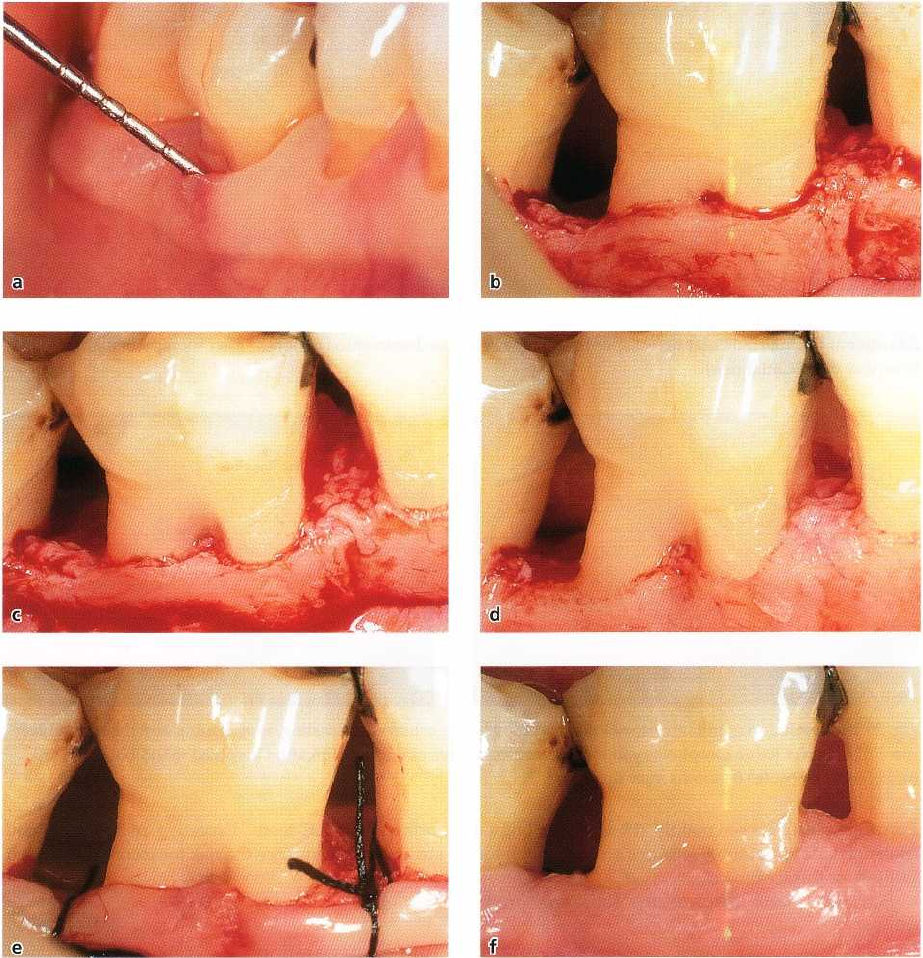
Furcation plasty
Furcation plasty (Fig 29-19a-f) is a resective treatment
modality which should lead to the elimination of the
interradicular defect. Tooth substance is removed
(
odontoplasty) and the alveolar bone crest is remod-
eled (osteoplasty) at the level of the furcation entrance.
TREATMENT OF FURCATION-INVOLVED TEETH • 713
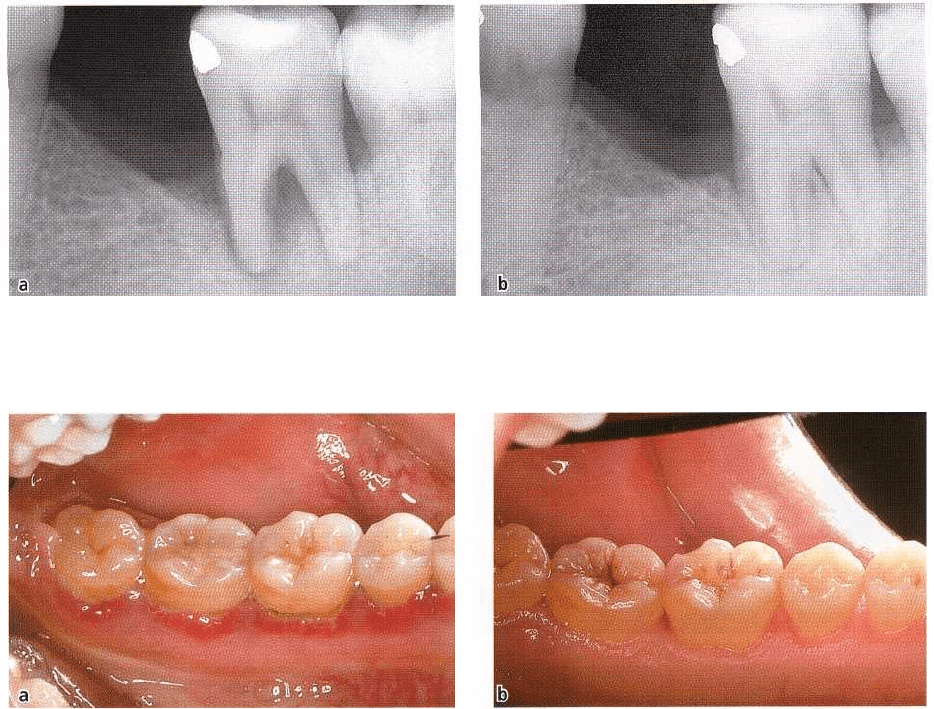
Fig. 29-17. Radiographic appearance of a defect in the furcation area caused by occlusal overload (a). After occlusal
adjustment the interradicular defect spontaneously healed, as documented 6 months after therapy in a
radiograph
(courtesy of M. Cattabriga).
Fig. 29-18. Resolution of inflammatory lesions in the gingiva achieved by scaling, root planing and the re-establish
-
ment of a correct tissue morphology in the interradicular area of degree I furcation involved mandibular molars.
(
a) Before therapy, (b) 6 months after therapy
Furcation plasty is used mainly at buccal and lingual
furcations. At approximal surfaces access is often too
limited for this treatment.
Furcation plasty involves the following proce
dures:
•
The dissection and reflection of a soft tissue flap to
obtain access to the interradicular area and the sur
-
rounding bone structures.
•
The removal of the inflammatory soft tissue from
the
furcation area followed by careful scaling and
root
planing of the exposed root surfaces.
•
The removal of crown and root substance in the
furcation area (odontoplasty) to eliminate or reduce
the horizontal component of the defect and to widen
the furcation entrance.
•
The recontouring of the alveolar bone crest in order
to reduce the buccal-lingual dimension of a bone
defect in the furcation area.
•
The positioning and the suturing of the mucosal
flaps at the level of the alveolar crest in order to
cover the furcation entrance with soft tissue. Fol-
lowing healing a "papilla"-like tissue should close
the
entrance of the furcation.
Care must be exercised when odontoplasty is per-
formed on vital teeth. Excessive removal of tooth
structure will enhance the risk for increased root sen-
sitivity.
Tunnel preparation
Tunnel preparation is a technique used to treat deep
degree II and degree III furcation defects in mandibu-
lar molars. This type of resective therapy can be of-
fered at mandibular molars which have a short root
trunk, a wide separation angle and long divergence
between the mesial and distal root. The procedure
includes the surgical exposure and management of the
entire furcation area of the affected molar.
Following the reflection of buccal and lingual mu-
cosal flaps, the granulation tissue in the defect is re-
moved and the root surfaces are scaled and planed.
The furcation area is widened by the removal of some
of the interradicular bone. The alveolar bone crest is
recontoured and to obtain a flat outline of the bone,
some of the interdental bone, mesial and distal to the
tooth in the region, is also removed. Following hard
tissue resection enough space has been established in
the furcation region to allow access for cleaning de-
vices to be used during self-performed plaque control
714 •
CHAPTER
29
Fig. 29-19. Furcation plasty performed at the buccal aspect of a mandibular molar. (a) Initial degree II furcation in
-
volvement. (b) After flap elevation, removal of the granulation tissue and scaling of the exposed root surfaces. (c)
After odontoplasty. (d) After osteoplasty. (e) Apical position of the flap managed by periosteal sutures. (f) Healing
resulting in the elimination of the furcation defect and in the establishment of a proper soft tissue morphology.
measures (Fig. 29-20a,b). The flaps are apically posi-
tioned to the surgically established interradicular and
interproximal bone level.
During maintenance the exposed root surfaces
should be treated by topical application of chlor-
hexidine digluconate and fluoride varnish. This sur-
gical procedure should be used with caution, because
there is a pronounced risk for root sensitivity and for
carious lesions developing on the denuded root sur-
faces within artificially prepared tunnels (Hamp et al.
1975).
Root separation and resection (RSR)
Root separation
involves the sectioning of the root com-
plex and the maintenance of all roots.
Root resection
involves the sectioning and the removal of one or two
roots of a multirooted tooth.
RSR is frequently used in cases of deep degree II
and degree III furcation involved molars.
Before RSR is performed the following factors must
be considered:
The length of the root trunk
In a patient with progressive periodontal disease a
tooth with
a
short
root trunk may have an early in-
volvement of the furcation (Larato 1975, Gher & Vern-