Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 625
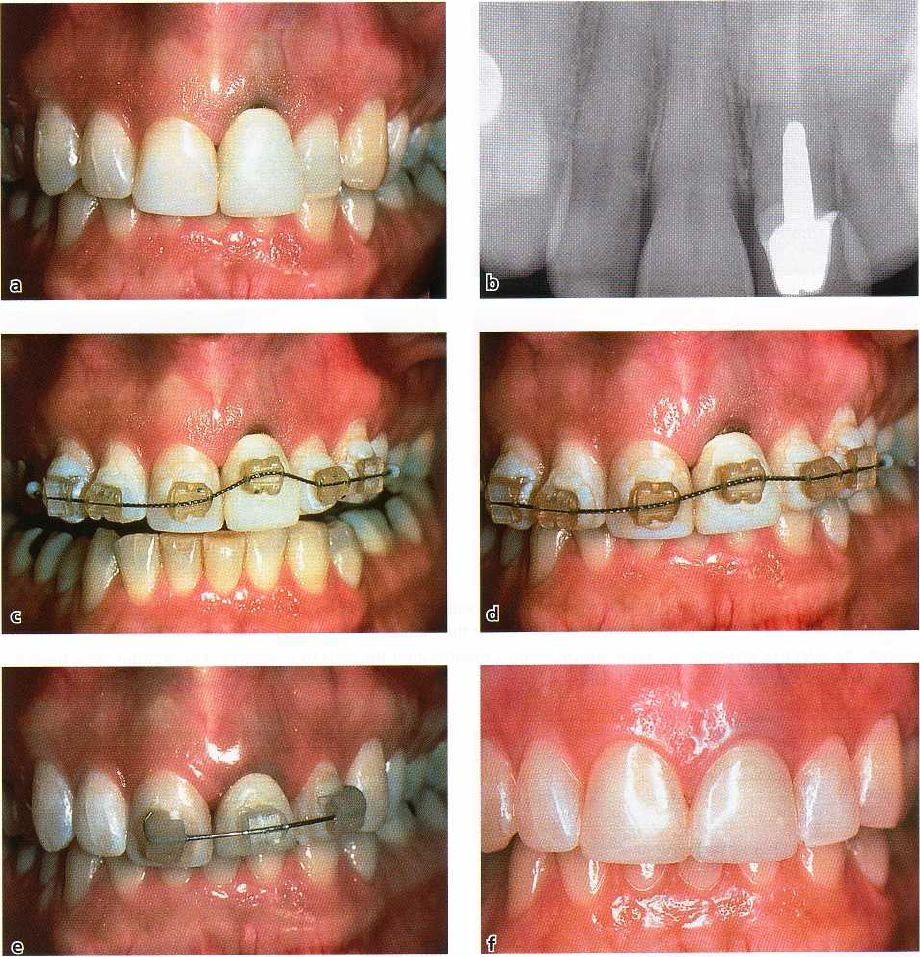
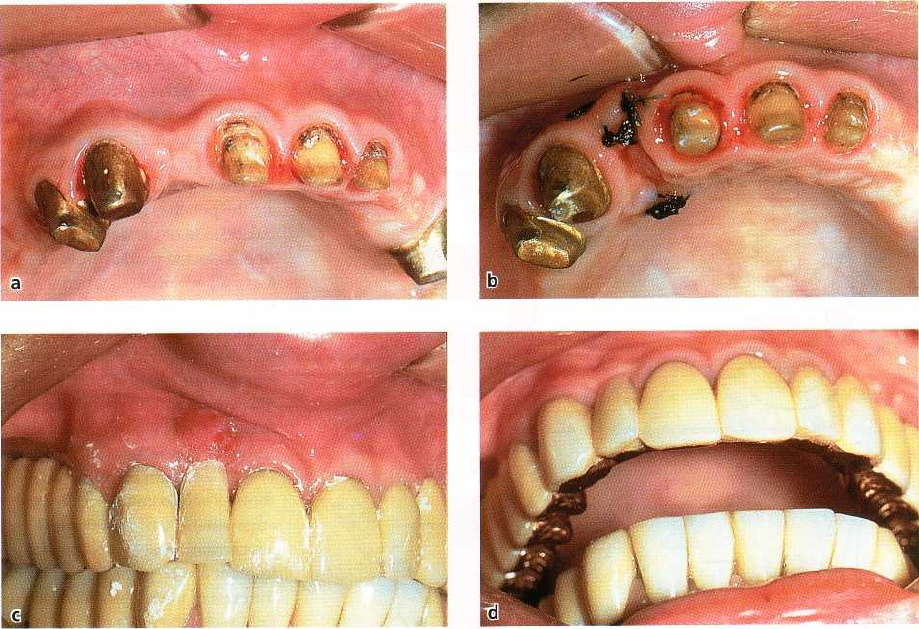
Fig. 27-65. Forced tooth eruption (slow method) used to level gingival margins, treat recession on a single tooth and
create esthetic harmony. (a-b) Recession on the left central incisor exposed the root surface darkened from root ca
nal
treatment. The uneven gingival margins and dark root surface detracted from an otherwise attractive smile. (c)
A
nitol wire with an offset bracket was used to slowly extrude the incisor. (d) Occlusal adjustment was done on the
lingual side of the crown to create room for the tooth to erupt. This view, at 1 month in tooth movement, shows the
gingival tissues moving with the root of the tooth. (e) Sufficient eruption had occurred by 3 months to level the gin
-
gival margins. The orthodontic brackets were used for temporary stabilization and a new crown was prepared. (f)
The new crown masked the show-through of the dark root. The even gingival margins and beautiful crown created
esthetic harmony. Courtesy of Dr J. Ingber, Philadelphia, PA.
Forced tooth
eruption
Orthodontic tooth movement can be used to erupt
teeth
in adults (Reitan 1967, Ingber 1974, 1976, Potash
-
nick
& Rosenberg 1982). If moderate eruptive forces
are
used, the entire attachment apparatus will move in
unison with the tooth. The tooth must be extruded
a
distance equal to or slightly longer than the portion
of
sound tooth structure that will be exposed in the
subsequent surgical treatment. After the tooth has
reached the intended position and has been stabilized,
a
full thickness flap is elevated and bone recontouring
is
performed to expose sound root structure. For es
thetic
reasons it is important that the bone and soft
tissue
levels at adjacent teeth remain unchanged.
Forced tooth eruption can also be used to level and
align gingival margins and the crowns of teeth to
obtain
esthetic harmony. Instead of using surgical
procedures
to apically position the gingival margins
626 • CHAPTER 27
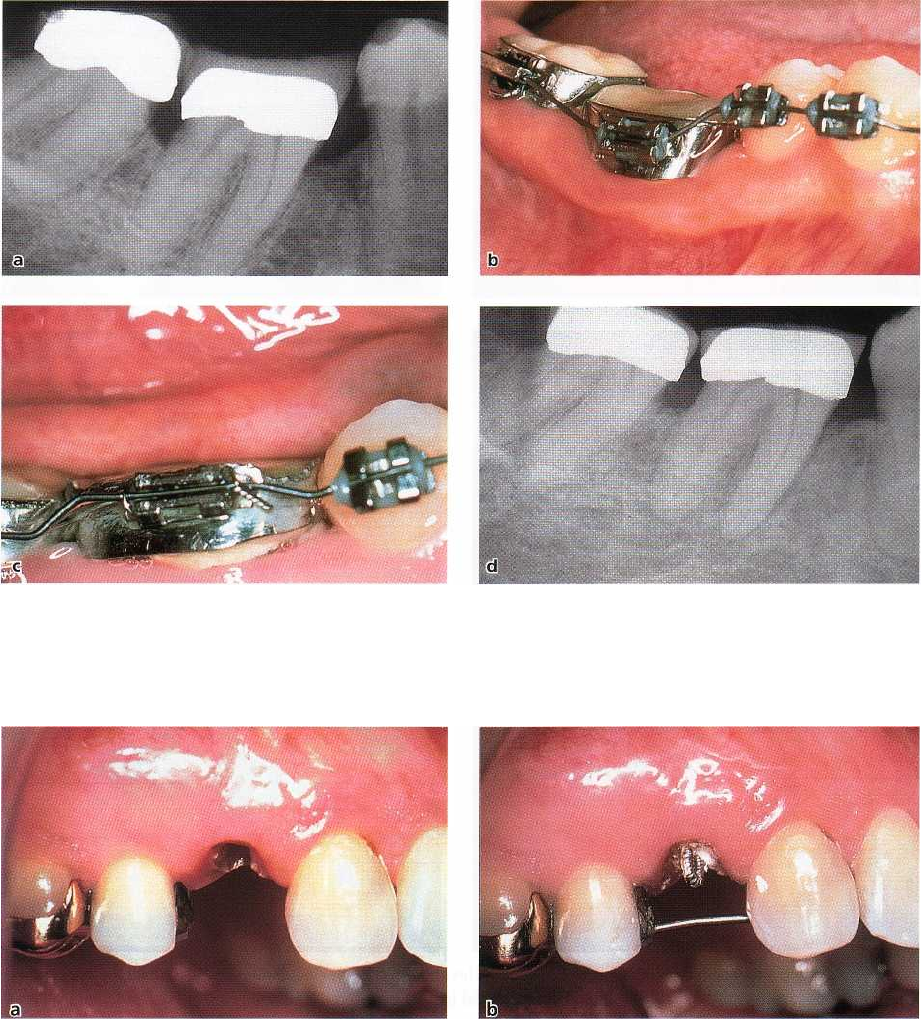
Fig. 27-66. Slow tooth eruption procedure used to level cemento-enamel junctions and angular bone crests. (a) Pre
-
treatment radiograph. (b) A nitol wire was used to erupt the molar. (c) The crown was shortened over a period of 4
months by selective grinding. (d) Radiograph taken 8 months after the start of treatment. The angular bone defects
were leveled. Courtesy of Dr J. Seibert, US.
Fig. 27-67a-b. Rapid tooth eruption procedure in conjunction with fiberotomy procedure. (a) Buccal view, the frac
ture
on the first premolar extended subgingivally. (b) Soft tooth structure was excavated and a twisted wire with an
occlusal hook was temporarily cemented in the root canal. A bar was placed into the amalgam restoration on the
premolar and bonded to the lingual surface of the canine.
of unaffected normal teeth to the level of a tooth with
recession or orthodontic malalignment, the tooth that
is
malpositioned or has sustained recession is erupted
to
the level of the normally positioned teeth. The entire
attachment apparatus and dentogingival junction will
follow the root of the tooth as it is moved coronally
(Fig.
27-65).
Indication:
Crown lengthening at sites where removal
of
attachment and bone from adjacent teeth must be
avoided. The forced eruption technique can also be
used as a means of reducing pocket depth at sites with
angular bony defects (Brown 1973, Ingber 1974, 1976).
The angular bony defect at the problem tooth can be
reduced while the attachment level at the adjacent
tooth
surface remains unchanged (Fig. 27-66).
Contraindication:
The forced eruption technique re-
quires
the use of fixed orthodontic appliances. Thus, in patients
who have only a few teeth remaining, an alternative
approach for crown lengthening has to be
selected.
Technique:
Orthodontic brackets are bonded to the pro-
MUCOGINGIVAL THERAPY - PERIODONTAL PLASTIC SURGERY • 627
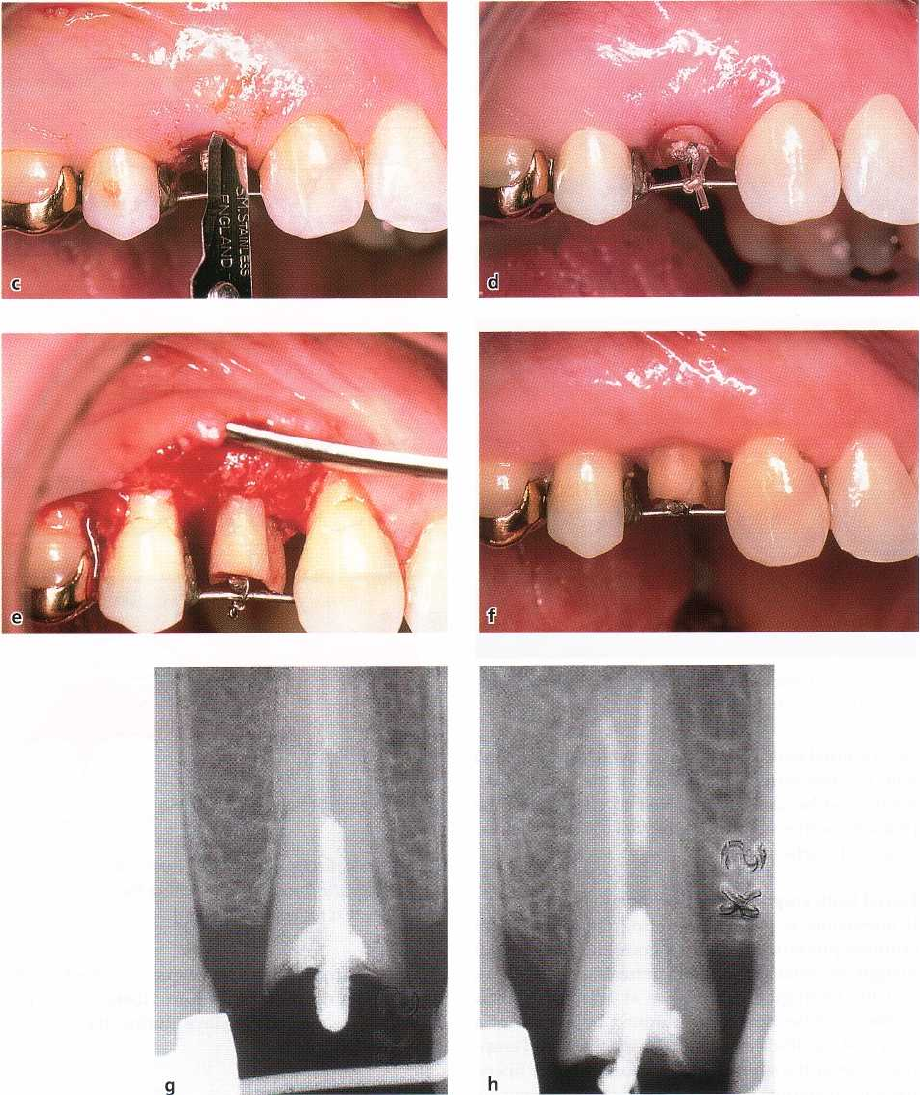
Fig. 27-67c-h. (c-d) Sulcular fiber resection was performed at the mesial half of the tooth to the level of the bone
crest. The distal half remained as a control surface. The fiber resection was repeated once a week during the 3-week
eruption phase. (e) The tooth was stabilized for 6 weeks, and at that time a full-thickness flap was raised. The bone
crest had a "positive
"
angulation at the distal surface and remained unchanged at the
"
test
"
mesial surface. Osse-
ous
resection was used to level the bony septum on the distal surface. (f) Ample crown lengthening was obtained
and
the gingival margins healed to their former shape and location. (g) Pretreatment radiograph enlarged to show the
normal shape of the crests of the interdental septae. (h) Enlargement of the posteruption radiograph (3 weeks of
rapid eruption and 6 weeks of stabilization) to show the "positive" angular crest on the "control
"
distal side and
the unchanged crest on the mesial "test" side. Courtesy of Dr R. Pontoriero, Milan, Italy
blem tooth and to adjacent teeth and are combined problem tooth. A power elastic is tied from the bracket
with
an arch wire. Another type of mechanical system to the arch wire (or the bar), which pulls to tooth can be utilized
by placing a heavy gauge bar or wire coronally. If most of the crown structure is lost, root
in grooves prepared in
the adjacent teeth and over the canal therapy is required. A post placed in the root
628 •
CHAPTER
27
a
b
c
Fig. 27-68. Ectopic tooth eruption. The permanent tooth
is erupting close to the mucogingival junction.
canal is fitted with a power elastic, which is also joined
with the arch wire. The direction of the tooth move-
ment must be carefully checked to ensure that the
problem tooth is not tilted or moved toward the adja-
cent tooth surfaces.
Forced tooth eruption with fiberotomy
If fiberotomy is performed during the forced tooth
eruption procedure the crestal bone and the gingival
margin are retained at their pretreatment locations,
and the tooth-gingiva interface at adjacent teeth is
unaltered. Fiberotomy is performed by the use of a
scalpel at 7 to 10-day intervals during the forced erup
-
tion to sever the supracrestal connective tissue fibers,
thereby preventing the crestal bone from following the
root in coronal direction. In the case presented in Fig.
27-67, fiberotomy was performed only at the mesial
half of the root. Radiographs obtained after 9 weeks
demonstrate that crestal bone migration has occurred
at the distal but not at the mesial surface of the erupted
tooth (Pontoriero et al. 1987).
Indication:
Crown lengthening at sites where it is im-
portant to maintain unchanged the location of the
gingival margin at adjacent teeth.
Contraindication:
Fiberotomy should not be used at
teeth associated with angular bone defects.
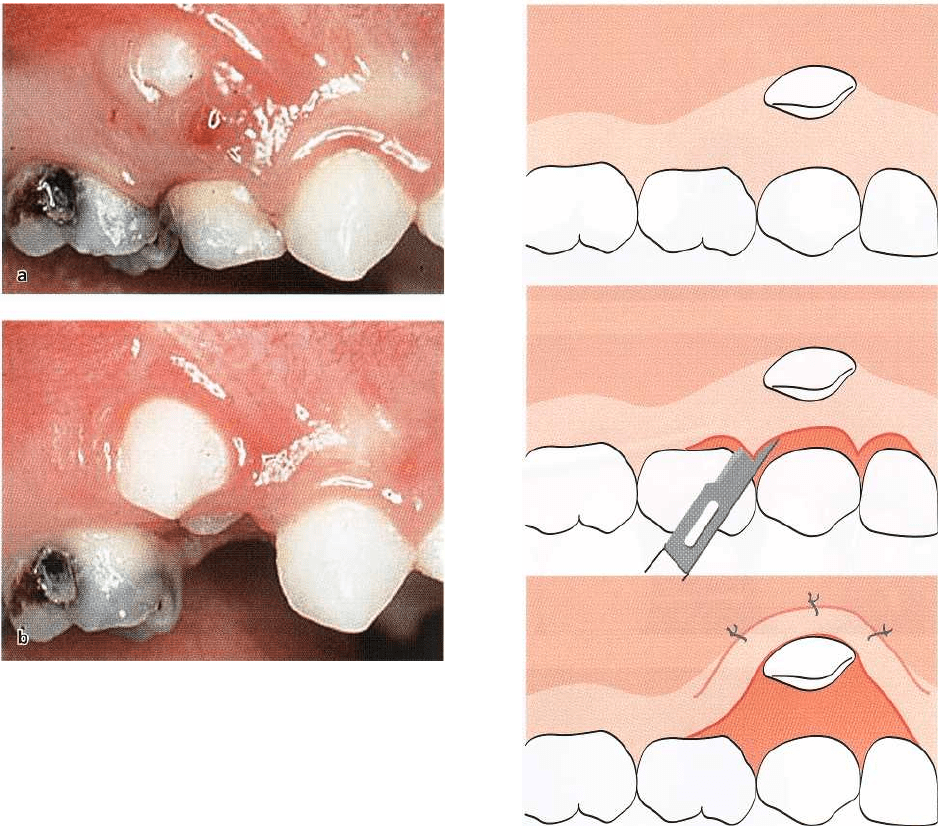
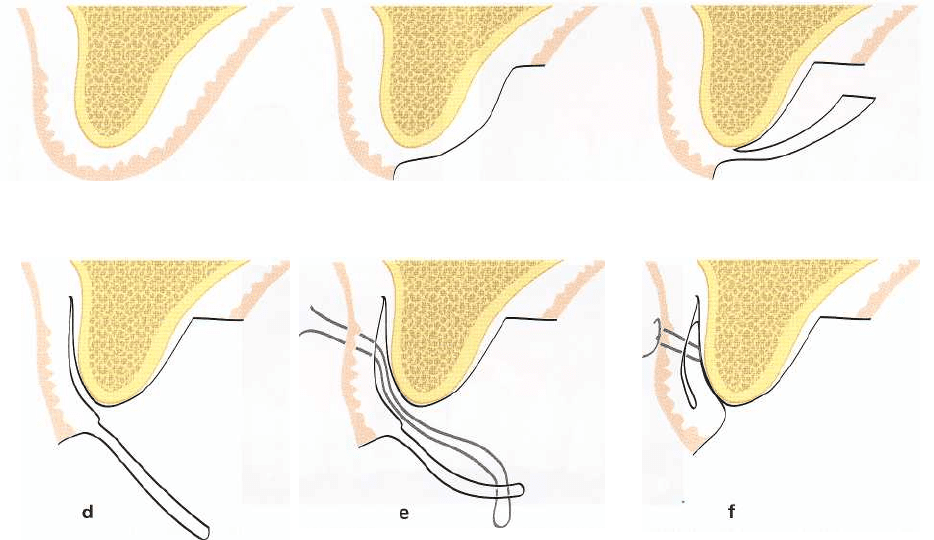
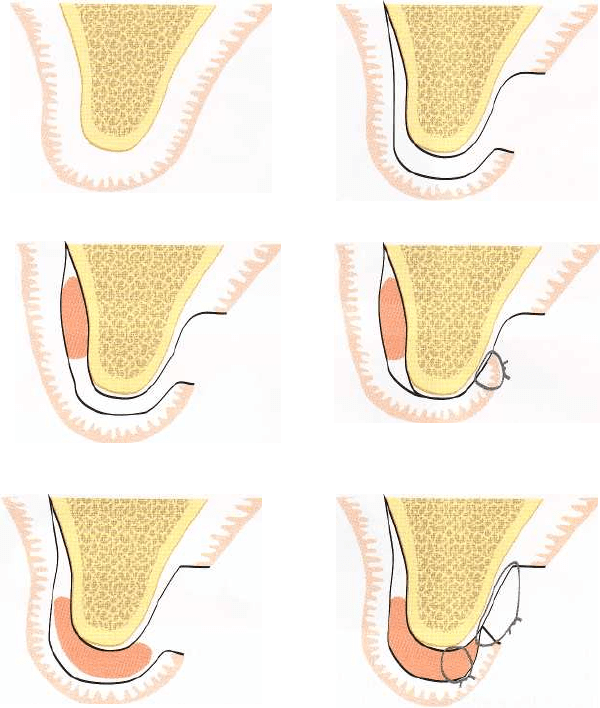
Fig. 27-69a-c.
Ectopically erupting tooth – double pedicle
graft.
Schematic drawings illustrating the surgical tech
-
nique (see text for explanation).
Technique:
Similar to the technique described for the
forced tooth eruption procedure. Fiberotomy is per-
formed once every 7-10 days during the phase of
forced tooth eruption.
Ectopic tooth eruption
Surgical intervention is often indicated for teeth erupt
ing ectopically, i.e. having an eruption position facial
to the alveolar ridge (Fig. 27-68). To create a satisfac
-
tory width of the gingiva for the permanent tooth, the
tissue entrapped between the erupting tooth and the
deciduous tooth is usually utilized as donor tissue
(
Agudio et al. 1985, Pini Prato et al. 2000b).
Three different techniques have been described for
the interceptive mucogingival treatment of buccally
erupting teeth, depending on the distance from the
donor site (entrapped gingiva) to the recipient site
MUCOGINGIVAL THERAPY - PERIODONTAL PLASTIC SURGERY • 629
Fig. 27-70a-c.
Ectopically erupting tooth — apically posi-
tioned flap.
Schematic drawings illustrating the surgical
technique (see text for explanation).
(area located facially-apically to the erupting perma-
nent tooth) (Agudio et al. 1985, Pini Prato et al. 2000b):
Double pedicle graft (Fig. 27-69):
This flap procedure is
indicated when the permanent tooth erupts within the
zone of keratinized tissue but close to the mucogingi-
val junction. An intrasulcular incision is performed at
the deciduous tooth and extended laterally to the
gingival crevice of the adjacent teeth and apically to
the erupting permanent tooth. By mobilization of the
flap apical to the mucogingival line, the entrapped
gingiva can be elevated and transposed for position-
ing apically to the erupting tooth. Sutures may be
placed to secure the position of the gingival tissue
facial to the erupting tooth.
Apically positioned flap (Fig. 27-7W:
When the perma-
nent tooth is erupting apical to the mucogingival junc
-
tion, vertical releasing incisions have to be placed to
allow for apical positioning of the keratinized tissue.
Fig. 27-71a-c.
Ectopically erupting tooth — free gingival
graft.
Schematic drawings illustrating the surgical tech
-
nique (see text for explanation).
Two lateral releasing incisions are made and extended
apically beyond the mucogingival junction. An in-
trasulcular incision is performed at the deciduous
tooth and a partial thickness flap is elevated beyond
the ectopically erupting tooth. The mobilized gingival
flap is moved apical to the erupting tooth and secured
in position by sutures.
Free gingival graft (Fig. 27-71):
If the tooth is erupting
within the alveolar mucosa distant to the mucogingi-
val junction, a free gingival graft procedure may be
selected. The entrapped gingiva is removed by a split
incision and used as an epithelialized connective tis-
sue graft. The free gingival graft is placed at a pre-
pared recipient site facial/apical of the erupting tooth.
Careful suturing is performed to secure a close adap-
tation of the graft to the underlying connective tissue
bed.
All the described procedures have been proven to
be effective in establishing a facial zone of gingiva
630 • CHAPTER
27
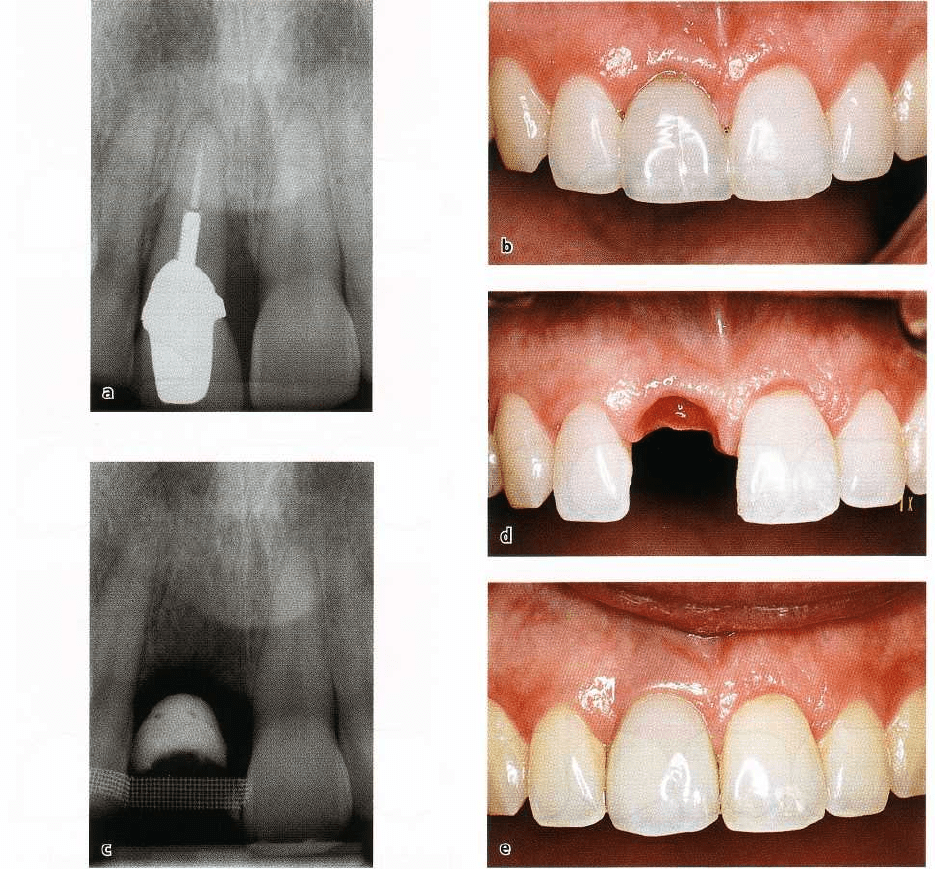
Fig. 27-72. (a) A central incisor that cannot be maintained because of root fracture which also caused pronounced
periodontal destruction. (b) Immediately following tooth extraction, an ovate pontic was inserted to support the fa
-
cial and proximal soft tissues. (c-d) Radiographic and clinical view of the area 6 weeks after tooth extraction. (e)
Fol
low-up 1 year after the placement of permanent prosthetic recontruction (single implant).
following the alignment of teeth erupting in an ectopic
position (Pino Prato et al. 2000b,c).
THE DEFORMED EDENTULOUS
RIDGE
A partially edentulous ridge may retain the general
shape of the alveolar process. Such a ridge is tradition-
ally refered to as a normal ridge. Even though this
normal ridge has retained the buccolingual and api-
cocoronal dimensions of the alveolar process, it is not
normal in many other respects; the eminences that
existed in the bone over the roots are no longer present
and the interdental papillae are missing.
The smooth contours of the normal ridge create
problems for the restorative dentist. In a fixed bridge
the pontics (1) frequently give the impression that they
rest on the top of the ridge rather than emerge from
within the alveolar process, (2) lack a root eminence,
and (3) lack marginal gingivae and interdental papil-
lae. Dark triangles, which almost always interfere
with
dentofacial esthetics, are present in the embra
sure
area between the pontics and between the abutments
and the pontics. In other words, in the presence
of a
normal ridge it may be difficult or impossible to
produce a fixed prosthesis which truly restores the
esthetics and function of the natural dentition.
Prevention of soft tissue collapse following
tooth extraction
Following extraction of a tooth, the topography of the
surrounding soft and hard tissues will be altered. The
MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 631
Fig. 27-73. (a) A 26-year-old female patient who had a trauma against the maxillary central incisors. Due to root
fracture and endodontic complications both central incisors had to be extracted. (b) A Rochette bridge with ovate
pontics was fabricated as a temporary replacement for the incisors. (c) Clinical view of the front tooth region
8
weeks after tooth extraction and placement of the resin bonded temporary bridge.
soft tissue margin will collapse and the height of the
adjacent papillae will be reduced. This soft tissue
collapse may be prevented by immediate post-extrac-
tion placement of an ovate pontic to support the soft
tissues. Fig. 27-72 illustrates such a situation where a
central incisor had to be extracted due to root fracture.
With the immediate placement of the pontic the facial
soft tissue margin and the papillae were maintained
almost unchanged following the healing of the extrac-
tion site. Also, in situations where several adjacent
teeth have to be extracted, insertion of ovate pontics
may facilitate the preservation of the outline of the soft
tissue ridge (Fig. 27-73).
Prevention of ridge collapse due to alveolar bone
resorption following tooth extractions must also be
considered. Borghetti & Laborde (1996) recommended
means for prevention of bone ridge collapse after
tooth extraction in any case of:
1.
fracture of the vestibular osseous plate during
tooth extraction or due to trauma
2.
resorption of the vestibular osseous plate
3.
presence of a thin vestibular bone plate.
Among procedures proposed for prevention of ridge
collapse in conjunction with tooth extractions are (1)
flap elevation for complete soft tissue closure of the
extraction sites (Borghetti & Glise 2000), (2) placement
of connective tissue grafts over the extraction sites
(
Nevins & Mellonig 1998), (3) placement of bone grafts
(
Becker et al. 1994), and (4) utilization of barrier mem
-
branes (Lekovic et al. 1997). Procedures for preserva-
tion of the bone dimensions following tooth extraction
are discussed in Chapter 28.
Correction of ridge defects by the use of soft
tissue grafts
A deformed ridge may result from tooth extractions,
advanced periodontal disease, abscess formations,
etc. The deformity that exists in the ridge is directly
related to the volume of root structure and associated
bone that is missing or has been destroyed. According
to Seibert (1983), ridge defects can be divided into
three classes:
Class I: Loss of buccolingual width but normal apico-
coronal height
Class II: Loss of apicocoronal height but normal buc-
colingual width
Class III: A combination of loss of both height and
width of the ridge.
Ridge augmentation procedures should be preceded
by a careful surgical-prosthetic treatment planning by
joint consultations involving the surgeon and the re-
storative dentist in order to attain an optimal esthetic
result. The following factors should be determined
prior to the initiation of therapy:
•
Volume of tissue required to eliminate the ridge
deformity
•
Type of graft procedure to be used
•
Timing of various treatment procedures
632 • CHAPTER 27
a
b
c
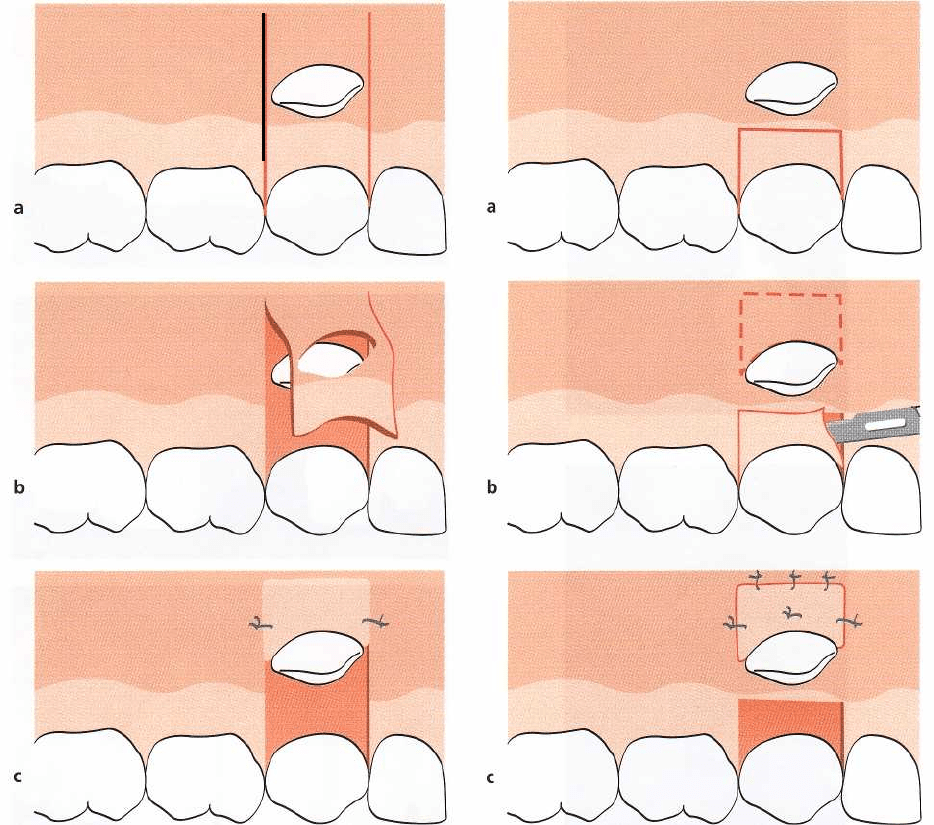
Fig. 27-74. Sequence of steps in the
"roll
flap
procedure".
(a) Cross section of the residual edentulous ridge prior to
treatment. (b) The removal of the epithelium. (c) The elevation of the pedicle. (d) The pouch is created. (e) Sutures
are placed at the mucogingival junction to catch the tip of the pedicle flap and pull it into place in the pouch. (f)
The flap is secured. A convexity in the ridge was created.
•
Design of the provisional restoration
•
Potential problems with tissue discolorations and
matching tissue color.
Ideally, a provisional restoration should be made prior
to surgery. The shape of the teeth in the provisional
restoration, the axial inclination and emergence pro-
file of the teeth and the embrasure form should be an
exact prototype of the final prosthesis that is to be
constructed. It is the task of the clinician performing
the surgery to augment the tissues to meet the provi-
sional prosthesis in the most exact manner possible. If
a gingival flange of pink-colored acrylic is used
around
single or multiple pontics on a temporary
removable
partial denture, the flange must be cut
away in order
to avoid pressure on the graft and give
the tissues
room to swell during the immediate post-
surgical phase
of healing. The soft tissue at the surgi
cally treated
recipient site for a graft will undergo
considerable
swelling during the early phase of heal
ing and the
tissues will conform to the tissue-facing surfaces of
the bridge or partial denture. The prosthe
sis is thus
used to help in shaping the outline of the
augmented
ridge to the desired form. The location and
shape of
interproximal embrasure areas in the provi
sional
bridge will determine where the "papillae"
created in
the ridge will be located.
Surgical procedures for ridge augmentation
Numerous
surgical graft and implant procedures with
the
attempt to reconstruct a partially edentulous ridge
or
ridge defect have been described in the literature
over the years. The procedures may be grouped ac-
cording to the means used for ridge augmentation as
(1) soft tissue augmentation procedures and (2) hard
tissue augmentation procedures. In this chapter only
soft tissue augmentation procedures will be ad-
dressed, while hard tissue augmentation procedures
are covered in Chapter 28. To illustrate various ap-
proaches for utilization of soft tissues for ridge aug-
mentation, the following procedures will be dis-
cussed:
Pedicle graft procedure
•
Roll flap procedure
Free graft procedures
•
Pouch graft procedure
•
Interpositional graft procedure
•
Onlay graft procedure
Studer et al. (1997) proposed the use of the pedicle
graft procedure for correction of a single-tooth ridge
defect with minor horizontal and vertical loss,
whereas
in cases of larger defects submerged free
connective
tissue graft procedures should be selected.
The onlay
full thickness graft procedure is indicated
for ridge
augmentation primarily in the presence of
additional
mucogingival problems such as insuffi
cient gingival
width, high frenum, gingival scarring,
or tattoo.
These recommendations were based on
short-term
evaluation of the obtained volumetric in-
crease of the
edentulous ridge following various aug
mentation
procedures, which demonstrated superior
results
with the use of submerged connective tissue
MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY •
6
33
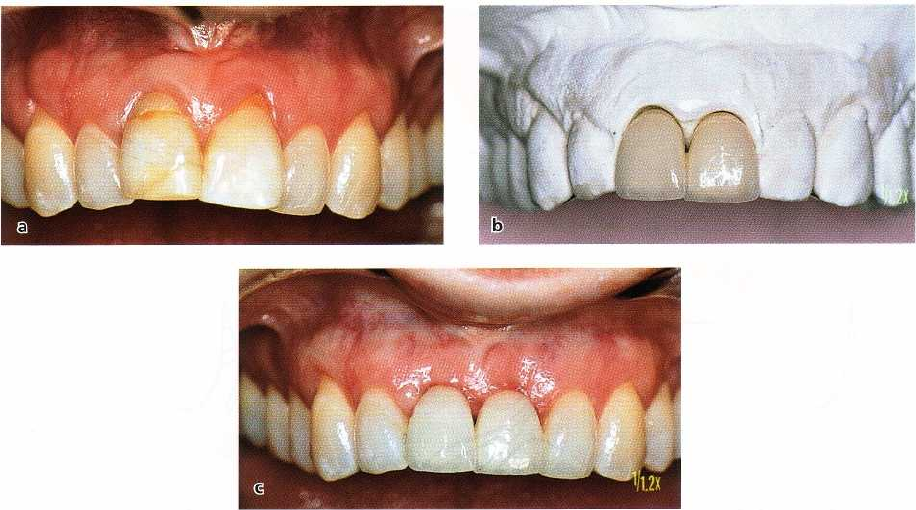
Fig.
27-75. "Roll flap procc(IlIre" .
(a) Pretreatment view of a Class I ridge defect in the area of the right lateral
incisor.
Note the marked concavity in the ridge. (b) This view shows the surgical site 1 week after surgery and
prior to the
removal of the sutures. (c) The tissue surface of the pontic was relined with autopolymerizing resin. (
d) Final pros
-
thesis in place. Note the illusion of a root eminence and a free gingival margin apical to the lateral
incisor pontic
tooth. Courtesy of Dr L. Abrams, Philadelphia, PA.
grafts compared to the use of full-thickness grafts (
Studer et al.
2000).
The "roll flap procedure"
Surgical concept:
The "roll flap procedure" (Abrams
1980) involves the preparation of a de-epithelialized
connective tissue pedicle graft, which is subsequently
placed in a subepithelial pouch (Fig.
27-74).
This pro-
cedure is used in the treatment of small to moderate
Class I ridge defects, primarily in cases with a single-
tooth space. The technique enables the surgeon to
augment tissue apically and labially to the cervical
area of a pontic and to give the recipient site the
appearance of a normal tooth-gingiva interface.
Hence, a buccolingual ridge concavity can be con-
verted into a ridge convexity resembling the eminence
produced by the roots of the adjacent teeth (Fig.
27-75).
Technique (Fig. 27-74):
A rectangular pedicle of connec
-
tive tissue is prepared on the palatal side of the defect.
The length of the pedicle must match the amount of
apicocoronal augmentation that is planned. This, in
turn, is related to the amount of root eminence that
exists on either side of the defect. If a two or three-
tooth pontic space is treated with the "roll technique",
two or three separate pedicles are raised. Each of these
pedicles will form a new "root-cervical margin".
The epithelium on the palatal surface of the donor
site is first removed. A maximum amount of suprape-
riosteal connective tissue is raised from the palate
using sharp dissection. The void that is produced at
the donor site will gradually fill in with granulation
tissue. Caution must be exercised in dissecting the
pedicle flap so that tissue perforation is avoided when
the plane of dissection approaches the facial (labial)
surface. A pouch is made in the supraperiosteal con-
nective tissue at the facial (labial) surface of the ridge.
In order to preserve as much connective tissue and
blood supply as possible at the recipient site, the
dissection must be made as close as possible to the
periosteum of the facial bone.
The pedicle is tucked into the pouch as a try-in
procedure. Adjustment of pedicle size should now be
made. Once the pedicle fits as desired, it is made ready
for the stabilizing suture. The suturing scheme is illus
-
trated in Fig. 27-74. The suture must be positioned
close to the mucobuccal fold. This enables the surgeon
to pull the pedicle to the apical portion of the pouch.
The suture should not be tightly tied, since it only
serves as a positioning and stabilizing device. The use
of a resorbable suture material is recommended.
Adjustment of pontic contours:
Measures used to adapt
the tissue surface of the pontic to the contour of the
634 • CHAPTER 27
A
C
E
B
D
F
Fig.
27-76.
Sequence of steps in
the
"pouch
graft procedure"
utiliz-
ing a free graft of connective tis-
sue (CT) to expand the ridge. (A)
Cross-section of the residual eden
-
tulous ridge prior to treatment.
(
B) The horizontal incision to cre-
ate the pouch is made well to the
palatal side of the defect. The inci
-
sion is started partial-thickness to
leave CT to suture to when the
flap is closed. The dissection is
made supraperiosteal on the la-
bial side of the ridge to (1) ensure
an adequate blood supply within
the pedicle and
(2)
permit the flap
to expand labially or labially and
coronally free of tension. (C-D)
The CT graft can be placed as
shown for maximal buccolingual
augmentation. (E-F) If vertical
augmentation is desired, the CT
implant can be placed closer to
the crest of the ridge. As is shown
in D and F, the more the flap is
stretched or expanded to gain aug
-
mentation, the more difficult it is
to gain primary flap closure.
surgically treated ridge are common to all soft tissue
ridge augmentation procedures in patients with fixed
bridgework. A light contact is maintained between the
pedicle graft and the tissue surface of the pontics. The
postoperative swelling will cause the tissue to con-
form to the shape of the pontic. This enables the
clinician to shape the soft tissue into a form that is
intended for the augmented site. Autopolymerizing
resin is added to the tissue surface of the pontics and
is allowed to cure until the resin reaches a dough-like
state. The bridge is then seated and pressed into the
grafted site. When the resin has set to a firm consis-
tency, the bridge is removed and placed in hot water
to complete the process of polymerization (Fig.
27-75).
The tissue surface of the pontics and the embrasure
areas are then carved to the shape that is intended for
the final bridge. The surface of the pontic is polished
and the bridge put in place using an appropriate
temporary cement.
Postoperative care:
A periodontal dressing is placed
over
the donor site. No dressing should be placed over
the
facial (labial) surface of the grafted area where
swelling will occur. The dressing at the donor site
should be changed at weekly intervals and main-
tained until wound healing has progressed to a point
where the tissue is no longer tender to touch.
Pouch graft procedures
Surgical concept:
A subepithelial pouch is prepared in
the area of the ridge deformity, into which a free graft
of connective tissue is placed and molded to create the
desired contour of the ridge. The entrance incision and
the plane of dissection may be made in different ways
(
Kaldahl et al.
1982,
Seibert
1983,
Allen et al.
1985,
Miller
1986,
Cohen
1994):
•
Coronal-apically: the horizontal incision is made on
the palatal or lingual side of the defect and the plane
of dissection carried in an apical direction (Fig.
27-
76)
•
Apical-coronally: the horizontal incision is made
high in the vestibule near the mucobuccal fold and
the plane of dissection is carried coronally to the
crest of the ridge
•
Laterally: one or two vertical entrance incisions are
started from either side of the defect (Fig.
27-77).
The
plane of dissection is made laterally across the span
of the deformity.
Indication:
The technique is used to correct Class I
defects. Patients with large volume defects may have
thin palatal tissues which are insufficient to provide
the volume of the donor tissue necessary to fill the
deformity. In such cases, various procedures for hard
tissue augmentation may be selected (see Chapter
28).