Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 615
Fig.
27-51.
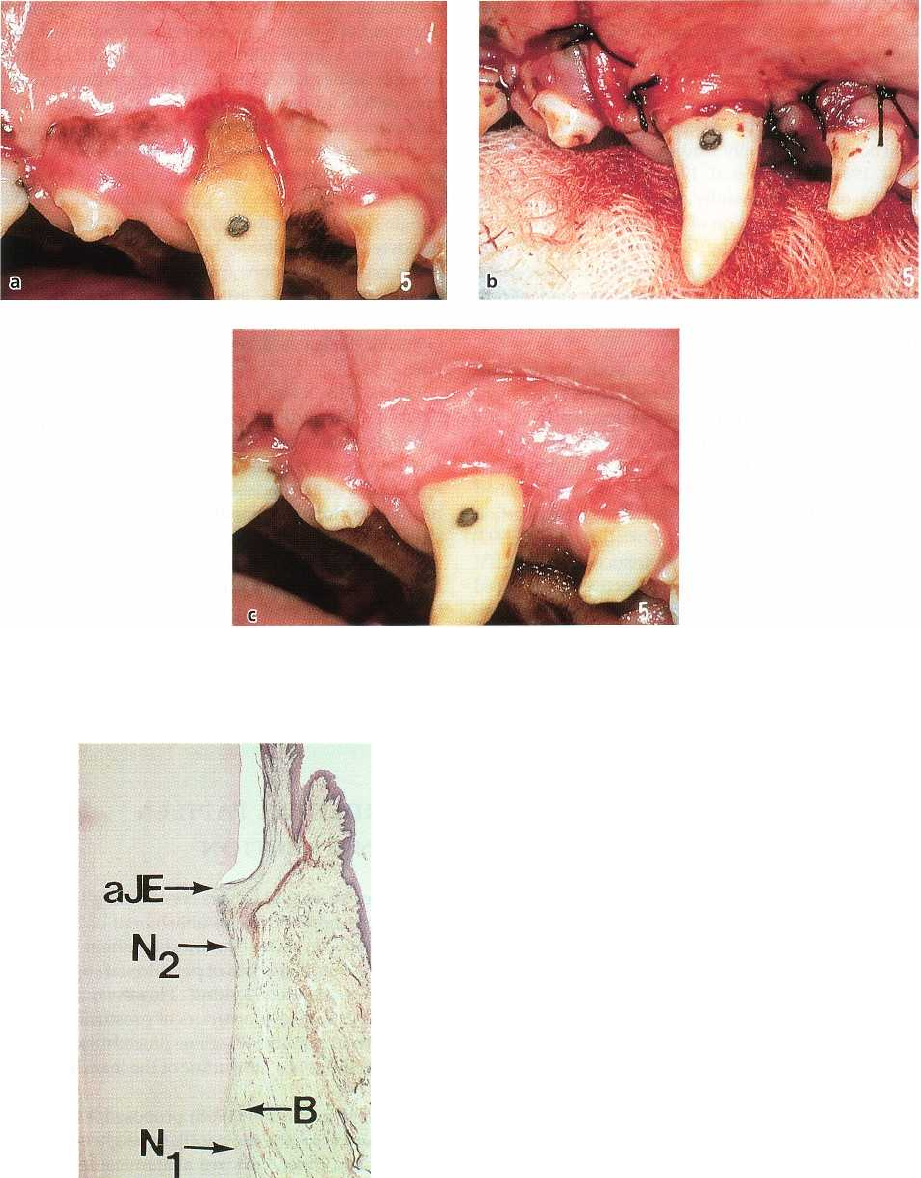
Clinical photographs illustrating the treatment of an experimentally induced localized recession defect
in a dog with a coronally displaced flap. Presurgical appearance of the localized recession defect (a). The site fol
-
lowing flap closure of the defect (b) and after 3 months of healing (c).
attachment of the same height had formed in the soft
tissue covered portion of the defect, i.e. about 50% of
the successfully covered defect showed new connec-
tive tissue attachment.
Gottlow et al. (1986) examined the result of healing
following treatment of experimentally produced re-
cession type defects with a coronally advanced flap in
dogs (Fig. 27-51). The histologic analysis after 3
months of healing disclosed that on average 20% of
Fig.
27-52.
Microphotograph of the healing following a
coronally displaced flap in the dog as illustrated in Fig.
27-51. A
new connective tissue attachment is formed
and extends coronally from the apical border of the
notch prepared at the bottom of the bone dehiscence
(
N
I
) to the apical termination of the epithelium (aJE) lo
-
cated within the notch indicating the presurgical level
of the soft tissue margin (N
2
). B: alveolar bone crest.
the apicocoronal length of the original defect had been
exposed due to recession during healing (i.e. about
80% root coverage was achieved), 40% was covered
by
epithelium and 40% demonstrated new connective
tissue attachment (Fig. 27-52). Determining factors for
the type of healing result were the size and the shape
of the defect. The possibility of achieving a new con-
nective tissue attachment in the apical portion of the
defect seemed to be considerably better in narrow
616 • CHAPTER 27
recession defects than in wider ones, most likely be-
cause the periodontal ligament at the lateral parts of
the defect will serve as a source of granulation tissue
from which a new connective tissue attachment can
develop.
The healing following pedicle graft procedures has
also been histologically studied in monkeys (Caffesse
et al. 1984, Gottlow et al. 1990), and in these studies
38-44% of the successfully covered recession defects
demonstrated formation of new connective tissue at-
tachment. The study by Gottlow et al. (1990) also
showed that the use of a GTR membrane between the
root surface and the pedicle graft generated signifi-
cantly more new connective tissue attachment (79% of
the covered recession defect).
Some case reports with human block sections pro-
vide evidence that new connective tissue attachment
with cementum formation may be formed following
pedicle graft procedures. Histologic evaluation of two
teeth treated with a laterally positioned flap revealed
that connective tissue attachment was re-established
in the apical fourth of the successfully covered portion
of the root (Sugerman 1969). Cortellini et al. (1993)
examined histologically a tooth treated with the GTR
procedure and showed that connective tissue faced
74% of the length of the recession defect. New cemen
-
turn with inserting collagen fibers, i.e. new connective
tissue attachment, covered 48% of the distance be-
tween the apical border of the root instrumentation
and the soft tissue margin.
Healing of free soft tissue grafts
Survival of a free soft tissue graft placed over a de-
nuded root surface depends on diffusion of plasma
and subsequent revascularization from those parts of
the graft that are resting on the connective tissue bed
surrounding the dehiscence. The establishment of col
-
lateral circulation from adjacent vascular borders of
the bed allows the healing phenomenon of "bridging
"
(
Sullivan & Atkins 1968a,b). Hence, the amount of
tissue that can be maintained over the root surface is
limited by the size of the avascular area (Oliver et al.
1968, Sullivan & Atkins 1968). Other factors consid-
ered critical for the survival of the tissue graft placed
over the root surface are that a sufficient vascular bed
is prepared around the dehiscence and that a thick
graft is used (Miller 1985b).
Another healing phenomenon frequently observed
following free graft procedures is "creeping attach-
ment", i.e. a coronal migration of the soft tissue mar-
gin. This occurs as a consequence of tissue maturation
during a period of about 1 year post-treatment.
Histologic evaluations of the nature of the attach-
ment established to the root surface following the use
of free grafts for root coverage are few. Sugerman
(
1969) reported from a histologic evaluation of a hu-
man tooth treated with a free soft tissue graft that new
connective tissue attachment was found in the apical
fourth of the successfully covered recession defect.
Pasquinelli (1995) harvested a human block biopsy of
a premolar for histologic evaluation 42 weeks after
treatment of a narrow recession defect with root bio-
modification (tetracycline HC1) and an epithelialized
free soft tissue graft. The root coverage amounted to 5
mm, or 83% of the original recession. The epithelial
lining was found to terminate 2.6 mm below the gin-
gival margin, and the most coronally positioned new
cementum with inserting connective tissue fibers was
seen 3.4 mm apical to the gingival margin. No his-
tologic reference for the apical extension of the origi-
nal defect was available, but the author estimated,
based on extrapolations from pre-treatment probing
assessments, that 3.6 mm of new attachment had
formed, corresponding to 51% of the apicocoronal
height of the covered, previously detached root por-
tion.
On the other hand, Harris (1999) and Majzoub et al.
(2001), each reporting the histological outcome of free
connective tissue grafts in two cases, found only mini
-
mal amounts of new cementum formation in the most
apical part of the recession defect and that healing
resulted in a long junctional epithelium occupying the
interface between the covering soft tissue and the
root.
Thus, the limited histological information available
from humans on the healing of free soft tissue grafts
indicates that a healing pattern similar to the one
discussed above following pedicle graft procedures
may result, namely that connective tissue attachment
may be established in the most apical and lateral parts
of the recession defect, but that an epithelial attach-
ment is formed along the major portion of the root.
INTERDENTAL PAPILLA
RECONSTRUCTION
There may be several factors contributing to the loss
of papilla height and the establishment of "black tri-
angles" between teeth. The most common reason in
the adult individual is loss of periodontal support due
to plaque-associated lesions. However, abnormal
tooth shape, improper contours of prosthetic restora-
tions and traumatic oral hygiene procedures may also
negatively influence the outline of the interdental soft
tissues.
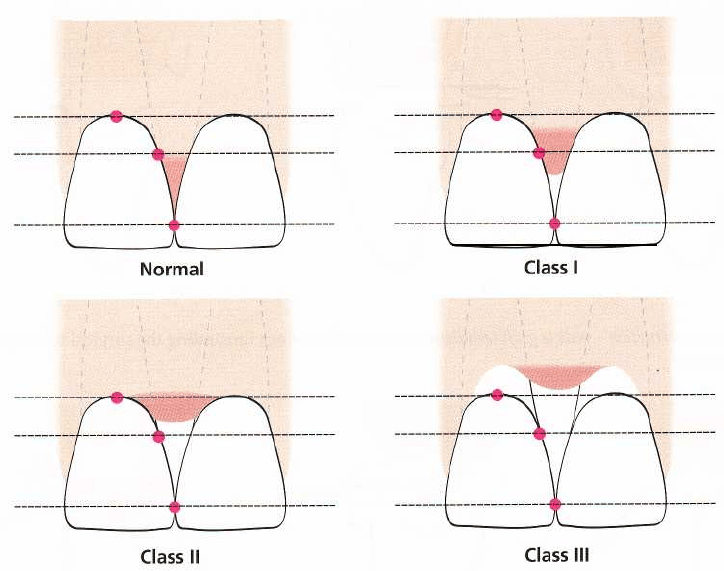
Nordland & Tarnow (1998) proposed a classifica-
tion system regarding the papillary height adjacent to
natural teeth, based on three anatomical landmarks:
the interdental contact point, the apical extent of the
facial cemento-enamel junction (CEJ), and the coronal
extent of the proximal CEJ (Fig. 27-53).
•
Normal:
the interdental papilla occupies the entire
embrasure space apical to the interdental contact
point/area.
•
Class I:
the tip of the interdental papilla is located
between the interdental contact point and the level
of the CEJ on the proximal surface of the tooth.
•
Class
II:
the tip of the interdental papilla is located
MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 617
Fig. 27-53. Schematic drawing illustrating the classification system for papilla height (Nordland & Tarnow 1998),
at or apical to the level of the CEJ on the proximal
surface of the tooth but coronal to the level of the
CEJ mid-buccally.
• Class
III:
the tip of the interdental papilla is located
at or apical to the level of the CEJ mid-buccally.
In an observational study in humans, Tarnow et al.
(
1992) analyzed the correlation between the presence
of interproximal papillae and the vertical distance
between the contact point and the interproximal bone
crest. When the vertical distance from the contact
point to the crest of bone was 5 mm or less, the papilla
was present almost 100% of the time, whereas if the
distance was 6 mm or more most commonly only
partial papilla fill of the embrasure between the teeth
was found. Considering that a supracrestal connective
tissue attachment zone of approximately 1 mm is
normally found (Gargiulo 1961), the observation indi-
cates that the biological height of the interdental pa-
pilla may be limited to about 4 mm. This interpretation
is supported by the observation that in interdental
areas denuded following an apically repositioned flap
procedure, an up-growth of around 4 mm of soft tissue
had taken place 3 years after surgery (Van der Velden
1982). Hence, before attempts are made to surgically
reconstruct an interdental papilla, it is important to
carefully assess both (1) the vertical distance between
the bone crest and the apical point of the contact area
between the crowns, and (2) the soft tissue height in
the interdental area. If the distance bone crest-contact
point is 5 mm and the papilla height is less than 4
mm, surgical intervention for increasing the volume
of the papilla could be justified in order to solve the
problem of an interdental "black triangle". However,
if
the contact point is located > 5 mm from the bone
crest, because of loss of periodontal support and/or
an inappropriate interdental contact relationship be-
tween the crowns, means to apically lengthen the
contact area between the teeth should be selected
rather than a surgical attempt to improve the topog-
raphy of the papilla.
If loss of papilla height is caused by soft tissue
damage only from oral hygiene devices, the inter-
proximal hygiene procedures must be initially discon-
tinued to allow soft tissue recovery and then succes-
sively modified in order to eliminate/minimize the
traumatic injury to the papillae.
Surgical techniques
Several case reports have been published regarding
surgical techniques for reconstruction of deficient pa-
pillae (e.g. Beagle 1992, Han & Takei 1996, Azzi et al.
1998). However, the predictability of the various pro-
cedures has not been documented and no data are
available in the literature providing information on
the long-term stability of surgically regained interden
-
tal papillae.
Beagle (1992) described a pedicle graft procedure
utilizing the soft tissues palatal of the interdental area.
Technique
(Fig. 27-54):
A split-thickness flap is dis-
sected on the palatal aspect of the interdental area. The
flap is elevated labially, folded and sutured to create
the new papilla at the facial part of the indental area.
A periodontal dressing is applied on the palatal aspect
only, in order to support the papilla.
Facial CEJ
Interproximal CEJ
Interdental
contact point
Facial CEJ
Interproximal CEJ
Interdental
contact point
618 • CHAPTER 27
a
b
c
Fig. 27-54a-c.
Papilla reconstruction – pedicle graft technique.
Schematic drawings illustrating the surgical technique
(
see text for explanation).
a
b
c
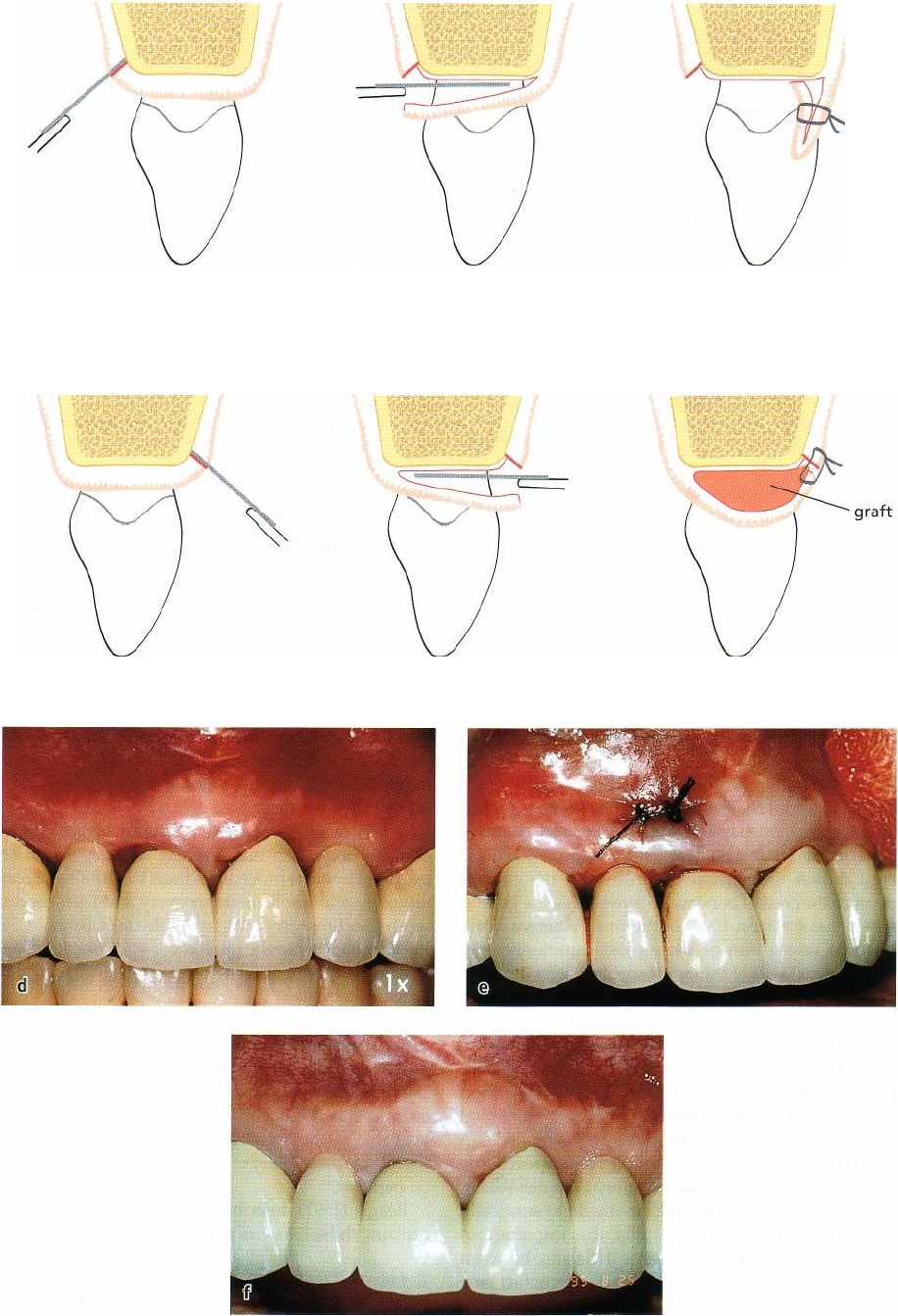
Fig. 27-55.
Papilla reconstruction – the
"
semi-lunar coronally repositioned papilla" technique. (a-c)
Schematic drawings
illustrating the surgical technique (see text for explanation). (d-f) Reconstruction of papillae distal to the central
incisors with the use of the semi-lunar coronally repositioned papilla technique in a patient with a fixed bridge
reconstruction.
MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 619
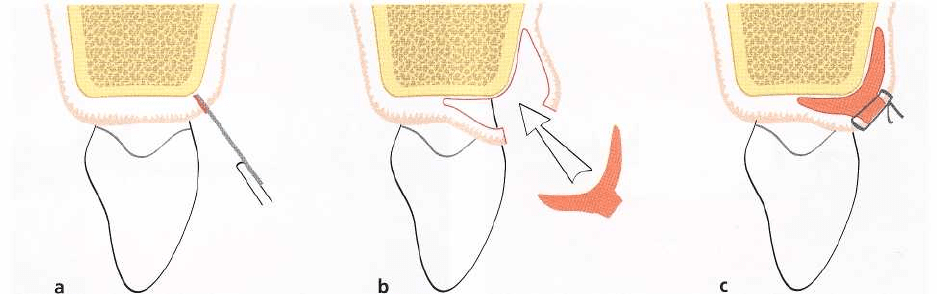
Fig. 27-56a-c.
Papilla reconstruction — "envelope" technique.
Schematic drawings illustrating the surgical
technique
(see text for explanation).
Han and Takei (1996) proposed an approach for
papilla reconstruction ("semi-lunar coronally reposi-
tioned papilla") based on the use of a free connective
tissue graft.
Technique (Fig. 27-55):
A semi-lunar incision is placed
in the alveolar mucosa facial to the interdental area
and a pouch-like preparation is performed into the
interdental area. Intrasulcular incisions are made
around the mesial and distal half of the two adjacent
teeth to free the connective tissue from the root sur-
faces to allow a coronal displacement of the gingival-
papillary unit. A connective tissue graft, taken from
the palate, is placed into the pouch to support the
coronally positioned interdental tissue.
Azzi et al. (1998) described a technique in which an
envelope-type flap was prepared for coverage of a
connective tissue graft.
Technique (Fig. 27-56):
An intrasulcular incision is
made at the tooth surfaces facing the interdental area
to be reconstructed. Subsequently, an incision is
placed across the facial aspect of the interdental area
and an envelope-type, split-thickness flap is elevated
into the proximal site as well as apically to a level
beyond the mucogingival line. A connective tissue
graft is harvested from the tuberosity area, trimmed
to adequate size and shape and placed under the flaps
in the interdental papilla area. The flaps are brought
together and sutured with the connective tissue graft
underneath.
CROWN LENGTHENING
PROCEDURES
Excessive gingival display
In most patients, the lower edge of the upper lip
assumes a "gum-wing" profile which limits the
amount of gingiva that is exposed when a person
smiles. Patients who have a high lip line expose a
broad zone of gingival tissue and may often express
concern about their "gummy smile" (Fig. 27-57a). The
form of the lips and the position of the lips during
speech and smiling cannot be easily changed, but the
dentist may, if necessary, modify/control the form of
the teeth and interdental papillae as well as the posi-
tion of the gingival margins and the incisal edges of
the teeth. In other words, it is possible by a combina-
tion of periodontal and prosthetic treatment measures
to improve dentofacial esthetics in this category of
patient.
As a base for treatment decisions, a careful analysis
of the dentofacial structures and how they may affect
esthetics should be performed and should include the
following features:
•
Facial symmetry
•
Interpupillary line — even or uneven
•
Smile line — low, median or high
•
Dental midline in relation to facial midline
•
Gingival display during speech and during broad,
relaxed smile
•
Harmony of gingival margins
•
Location of gingival margins in relation to the ce-
mento-enamel junctions
•
Tooth size and proportions/harmony
•
Incisal plane/occlusal plane.
If excessive gingival exposure is due to insufficient
length of the clinical crowns, a crown lengthening
procedure is indicated to reduce the amount of
gingiva exposed, which in turn will favorably alter the
shape and form of the anterior teeth. To select the
proper treatment approach for crown lengthening, an
analysis of the individual case with regard to crown-
root-alveolar bone relationships should also be in-
cluded.
In the young adult with an intact periodontium the
gingival margin normally resides about 1 mm coronal
to the cemento-enamel junction. However, some pa-
tients may have a height of free gingiva that is greater
than 1 mm, resulting in an unproportional appearance

620 • CHAPTER 27
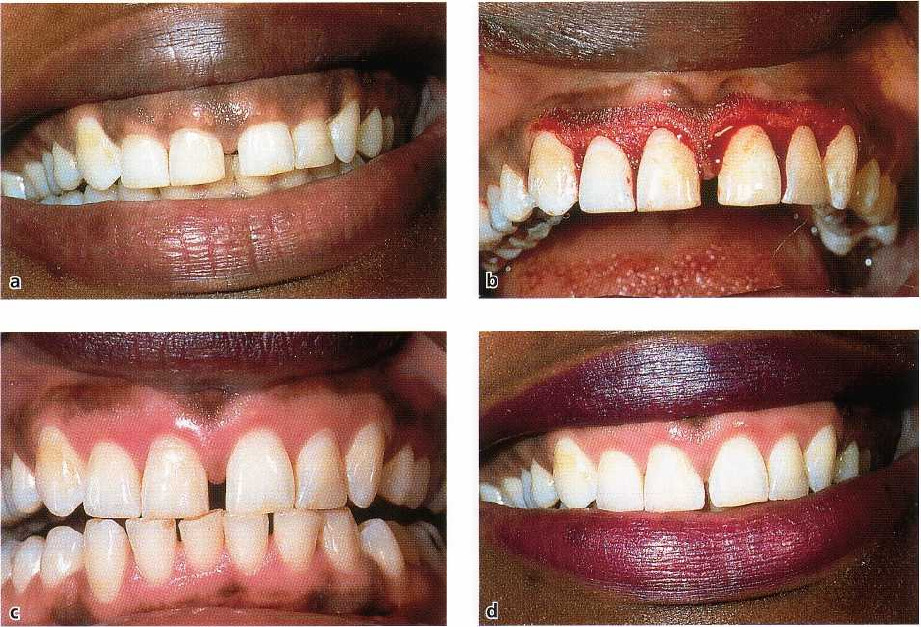
Fig.
27-57.
Crown lengthening procedure. (a-b)
Pretreatment views. The clinical crowns are considerably shorter than
the anatomical crowns. The lateral incisors were congenitally missing and orthodontic treatment had been carried
out
to move the posterior teeth anteriorly. The canine teeth in the position of the lateral incisors added to the es
thetic
disharmony. (c) A gingivectomy was performed to expose the anatomical crowns of the teeth. (d) One month
post-
surgery. At this appointment, the canine and first premolar teeth were reshaped and bonded. (e) Tooth form
and
proportional balance were improved by bonding. (f) At 3 years post-treatment, the gingival tissues exhibited
no
rebound and retained the architectural form sculpted into the tissue at the time of the surgical procedure. Cour
tesy
of Dr J. Seibert, US.
of the clinical crown. If such a patient complains about
their "small front teeth" and the periodontium is of a
thin
biotype, full exposure of the anatomical crown
can be
accomplished by a gingivecomy/gingivo
plasty
procedure (Fig.
27-57).
An assessment should also be made regarding the
amount and pattern of pigmentation existing within
the
gingival tissues, and the patient's desire to maintain or
lessen the pigmentation contained within the
tissues.
The externally beveled path of incision that is
usually
employed in a gingivectomy procedure will
remove the pigmentation and produce pink gingival
tissue upon initial healing (Fig.
27-58).
The surgically
induced color change in the tissues comes about rap-
idly, and markedly affects esthetic values. For this
reason, an externally beveled gingivectomy proce
dure
should not be terminated at the midline in pa
tients that
have pigmented gingival tissues. It should be extended
across the midline to the premolar area to
avoid a color
mismatch in the esthetic zone of the
anterior teeth. The
color change may be permanent or
the pigmentation
may slowly return over a period of
MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 621
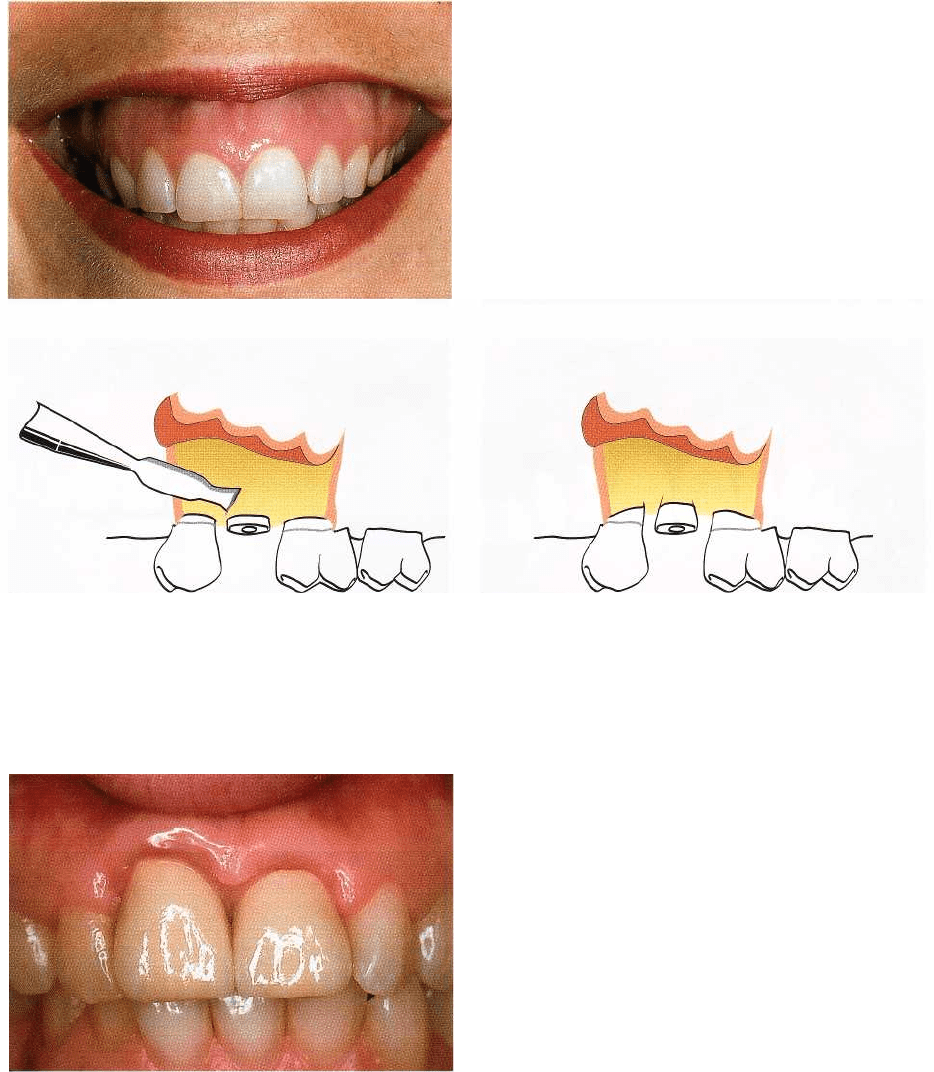
Fig. 27-58. (a) Pretreatment view. The patient disliked her "small front teeth" and diastema. Radiographs and prob
ing indicated the gingival tissues were covering the cervical one third of the crowns. Crestal bone was thin and in
normal relationship to the cemento-enamel junctions. The patient preferred "pink gum
s
"
if she could possibly have
them. (b) A long externally beveled path of incision was used to accomplish the gingivectomy. (c) This view shows
the color changes and pleasing architecture produced in the anterior gingiva at 2 months post-surgery. The di-
astema was partially closed by direct bonding at this time. (d) Post-treatment view showing the enhancement of es
thetic values for the patient. Courtesy of Dr J. Seibert, US.
a year or more. Patients should be informed of the
changes in tissue color that will occur and should be
allowed to make a choice as to the color of the tissue
they will have postsurgically. If they wish to maintain
their pigmentation, an internally beveled path of inci-
sion (internal gingivectomy) should be employed
(Fig.
27-59).
If the periodontium is of the thick biotype and there
is a bony ledge at the osseous crest, an apically posi-
tioned flap procedure (see Chapter 25) should be per-
formed. This will allow for osseous recontouring (Fig.
27-60).
More extensive bone recontouring is required to
solve esthetic problems found in patients who do
indeed have short anatomical crowns in the anterior
section of the dentition. In this category of patients,
prosthetic measures must be used after resective peri-
odontal therapy to increase the apicocoronal dimen-
sion of the crowns (Fig. 27-61). Patients who are can-
didates for this kind of resective therapy can be di-
vided into two categories:
1. Subjects who have normal occlusal relationships
and incisal guidance. In this category the incisal
line
of the front teeth must remain unaltered but the
clinical crowns can be made longer by surgically
exposing root structure and by locating the cervical
margins of the restorations apical to the cemento-
enamel junction (Fig. 27-61).
2. Subjects who have abnormal occlusal relationships
with excessive interocclusal space in the posterior
dentition when the anterior teeth are in edge-to
edge
contact. In this category of patients the length of the
maxillary front teeth can be reduced without
inducing posterior occlusal interferences. In addi-
tion, the marginal gingiva can be resected or relo-
cated to an apical position before crown restora-
tions are made.
In some individuals having excessive display of
gingiva, the size and shape of the teeth and the loca-
tion of the gingival margins may be perfectly normal.
The excessive display of gingiva in these cases is often
caused by vertical maxillary excess and a long mid-
face
(Fig. 27-62). Periodontal crown lengthening pro
cedures
will not suffice to solve their problems, but
rather the
maxilla must be impacted by major maxil
lofacial
surgical procedure. The risk-benefits and cost ratios
must be thoroughly evaluated before recom-

622 • CHAPTER 27
Fig. 27-59. Pretreatment view. This patient disliked the looks of her "small front teeth
"
; she sought consultation to
have her teeth made longer by crowning them. Probing and radiographs revealed normal osseous morphology and
a
wide zone of attached gingiva that covered the cervical one third of the incisors. It was explained to the patient
that
a surgical solution was preferred to restorative procedures to make her teeth longer. The patient made a re-
quest
that the color of her gingival tissues remain unchanged. (b) An internally beveled path of incision was used
to
effect an "internal gingivectomy" to maintain the pigmentation in the tissues. This created mini flaps in the areas
of
the papillae. (c) 5-0 gut sutures were used to stabilize the papillae. (d) The crown lengthening that was achieved
with maintenance of color harmony can be seen in this view at 3 months post-surgery. Courtesy of Dr E. Saacks,
Pennsylvania, PA.
mending this type of surgical therapy to correct es-
thetic problems.
Exposure of sound tooth structure
Crown lengthening procedures may be required to
solve
problems such as (1) inadequate amount of tooth
structure for proper restorative therapy, (2) subgingi
val
location of fracture lines, and (3) subgingival loca
tion of
carious lesions.
The techniques used to accomplish crown length-
ening include (1) apically positioned flap procedure
including bone resection, and (2) forced tooth erup
tion
with or without fiberotomy.
Apically positioned flap with bone recontouring
The apically positioned flap technique with bone re-
contouring (resection) may be used to expose sound
tooth structure. As a general rule, at least 4 mm of
sound tooth structure must be exposed at time of
surgery. During healing the supracrestal soft tissues
will
proliferate coronally to cover 2-3 mm of the root
(Herrero
et al. 1995, Pontoriero & Carnevale 2001), thereby
leaving only 1-2 mm of supragingivally lo
cated sound
tooth structure. When this technique is
used for crown
lengthening it must also be realized
Fig. 27-61. Crown lengthening by surgical and prosthetic procedures. (a) Pretreatment view. The patient displayed
"
short front teeth" and a broad exposure of gum tissue. The full anatomical crown is exposed in this case and the
surgically induced recession will expose root structure. (b) The patient had an unusually wide zone of attached
gingiva. The gingival margins were positioned apically by making an internally beveled flap with a submarginal
entrance incision as outlined in red ink. The crest of the bone was reduced in height. (c) After the tissues had ma
-
tured following surgery, individual crowns were prepared for each of the anterior teeth. Crown lengthening was
achieved and the patient no longer exposed a broad expanse of gum tissue. Courtesy of Dr D. Garber, Atlanta, GA.

MUCOGINGIVAL THERAPY — PERIODONTAL PLASTIC SURGERY • 623
Fig.
27-60.
(a) Pretreatment view. The patient, a dentist, requested crown lengthening to lessen his "gummy smile
"
and give him a more masculine appearance. The patient had a wide zone of attached gingiva and thick crestal
bone.
Palpation indicated bony exostoses. (b) An apically positioned flap and osseous resective surgery, from sec
ond
premolar to second premolar, were used to lengthen the teeth. The surgery was confined to the labial surfaces.
This
view shows one half of the surgery completed. (c) Vertical mattress sutures were utilized to hold the flap api
cally. (d)
Three years post-treatment. Note that the gingival tissues retain the morphology created at the time of sur
gery.
Courtesy of Dr J. Seibert, US.
624 • CHAPTER 27
Fig. 27-62. This patient displays a large expanse of gin
-
gival tissue when smiling or speaking. The patient has
a
long mid-face and vertical maxillary excess. The gin-
gival margins reside 1 mm coronal to the cemento-
enamel junction and the anatomical and clinical
crowns are approximately equal.
a
b
Fig. 27-63. (a-b) Surgical resective therapy for crown lengthening cannot be confined to the tooth in need of treat-
ment. The principles of osseous resection require that bone be removed from the adjacent teeth to create a gradual
rise and fall in the profile of the osseous crest. This causes a loss of attachment apparatus and recession on the
adja
cent teeth as well.
Fig. 27-64. A deformity which interfered with dento-
facial esthetics was created at the right central incisor
by using a surgical crown lengthening procedure at
one
single tooth to expose sound tooth structure. The
soft
tissues cannot follow the abrupt and steep changes
in
the osseous profile. The crown preparation invaded the
zone of normal supracrestal connective tissue. This
created a chronic periodontal pocket and adversely af-
fected esthetics. Courtesy of Dr A. Winnick, Toronto,
Canada.
that gingival tissues have an inherent tendency to
bridge abrupt changes in the contour of the bone crest.
Thus, in order to retain the gingival margin at its new
and more apical position, bone recontouring must be
performed not only at the problem tooth but also at
the
adjacent teeth to gradually reduce the osseous
profile (
Fig. 27-63). Consequently, substantial
amounts of
attachment may have to be sacrificed
when crown
lengthening is accomplished with an
apically positioned
flap technique. It is also important to remember that, for
esthetic reasons, symmetry of
tooth length must be
maintained between the right
and left side of the dental
arch. This may, in some
situations, call for the inclusion of even more teeth in
the surgical procedure.
Indication:
Crown lengthening of multiple teeth in a
quadrant or sextant of the dentition.
Contraindication:
Surgical crown lengthening of single
teeth in the esthetic zone (Fig. 27-64).
Technique:
The apically positioned flap technique and
methods used for bone recontouring are discussed in
Chapter 25.