Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

ENDODONTICS AND PERIODONTICS • 323
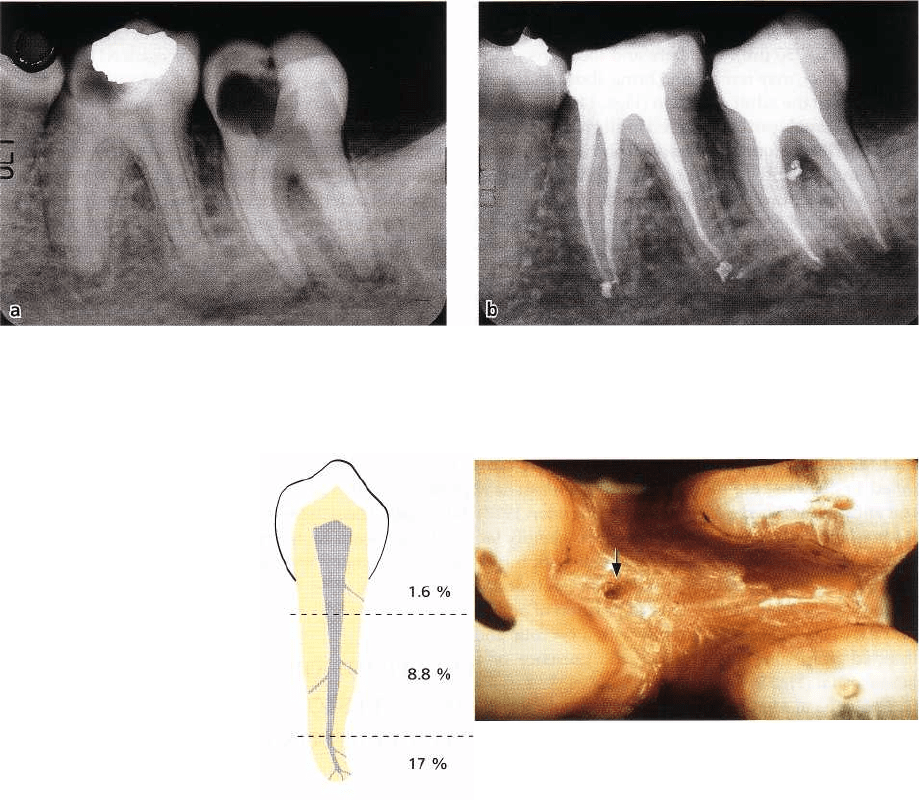
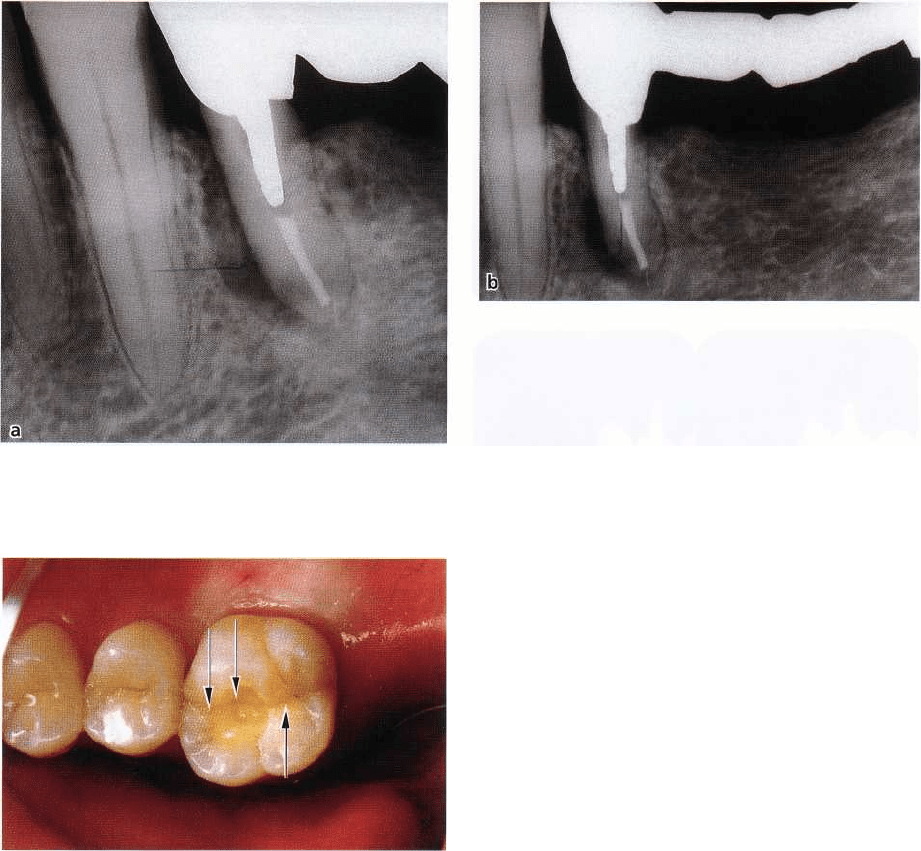
Fig. 14-6. (a) Destruction of alveolar bone is observed in the furcal region of the second lower left molar. (b)
Upon endodontic treatment a lateral became filled suggesting that the furcal lesion had an endodontic origin.
Courtesy of Dr Pierre Machtou.
Fig. 14-7. Frequency of accessory canals at different
lev- els of the root. The data are average values
obtained from De Deus (1975). Observations were
made after the teeth had been rendered transparent and
the root- canal system filled with China ink. The
figures for the coronal portion of the root include those
of the bi- and trifurcations.
Fig. 14-8. Photograph of the furcation area of an ex-
tracted maxillary molar with cut roots demonstrating
the opening of an accessory canal (arrow). Scanning
electron microscopic observations indicate that the fre-
quency of such furcation foramina is great (Burch &
Hulen 1974, Koenigs et al. 1974), whereas the number
of openings at the pulpal floor is small (Perlich et al.
1981). This suggests that furcation foramina at the ex-
ternal surface of the root do not necessarily represent
patent communications with the pulpal chamber. Cour-
tesy of Dr Robert C. Bowers.
volve the marginal periodontium, unless they are de-
veloping close to the bone margin. A potential path-
way for infectious elements in root canal in such in-
stances may be lateral canals.
Manifestations of endodontic lesions in the
marginal periodontium from lateral canals
Endodontic lesions, where bacterial elements reach the
periodontium by way of lateral canals, may, except for
lateral aspects of roots (Fig. 14-5), appear in furcation
areas of two and three-rooted teeth (Fig. 14-3). If there
is an existing periodontal lesion, the two soft tissue
lesions may merge and in the radiograph appear as
one lesion (Fig. 14-5a). Although, clinically, one may
be able to bring a probe through both lesions, it
is important from a therapeutic point of view to un-
derstand that the coronal part is directed towards an
infection in the marginal periodontium, and the apical
part to an infection emanating from the root canal
system. This means that in order to obtain healing,
elimination of both the sources of infection is required (
see further below).
Lateral canals normally harbor connective tissue
and vessels, which connect the circulatory system of
the pulp with that of the periodontal ligament. Such
anastomoses are formed during the early phases of
tooth development. During the completion of root
formation, several anastomoses become blocked and
reduced in width by continuous deposition of dentin
and root cementum. This may explain why endodontic
lesions are rarely seen in furcal areas of the adult
dentition, while in primary and young permanent
324 • CHAPTER 14
molars such lesions often are the first sign of an in-
fected pulp necrosis. Patent communications of vary-
ing sizes (10-250 1m), numbers and locations in the
root, however, may remain and bring about endodon-
tic lesions in the adult dentition (Figs. 14-3, 14-6).
Lateral canals can be observed in all groups of teeth.
The majority are found in the apical portion of the root.
In the middle and cervical root portions, the preva-
lence is small. In a study of 1140 extracted human teeth
from adult subjects, De Deus (1975) reported lateral
canals in 27%. These canals were distributed at vari-
ous levels of the root as depicted in Fig. 14-7.
The frequency of lateral canals in the furcation area
of two and three-rooted teeth has been determined in
numerous studies of extracted human teeth (Fig. 14-8).
A variety of techniques have been employed, which
may explain the divergent results obtained. While
some studies found furcation canals in between 20%
and 60% of examined teeth (Lowman et al. 1973, Ver-
tucci & Williams 1974, Gutmann 1978), others have
failed to demonstrate the presence of such canals at
furcation sites (Pineda & Kuttler 1972, Hession 1977).
Radiographically, it is seldom possible to identify lat-
eral canals unless they have been filled with a con-
trasting root-filling material following endodontic
therapy (Figs. 14-5, 14-6). A lateral position of a radi-
olucency associated with a tooth with a necrotic and
infected pulp may also indicate the presence of a
lateral canal (Fig. 14-5a).
The clinical significance of lateral canals for the
dissemination of infectious elements from an infected
pulp to the periodontium is not well established. In
fact, there is no documention as to how often such
lesions occur. It is conceivable that the wider the
lateral canal, the greater is the likelihood for a lateral
lesion to develop. Although clinical observations
demonstrate their occurrence (Figs. 14-3, 14-5 and
14-6), the
rate at which endodontic lesions appear in the mar-
ginal periodontium seems to be low.
In this context, it should be recognized that there is
little evidence suggesting that infectious products
from a necrotic pulp can affect the periodontal tissue
through intact walls of dentin and cementum. Even if
the width of the dentinal tubules is large enough to
allow passage of both bacteria and their components,
an intact outer layer of cementum evidently acts as an
effective barrier against such penetration. Once ce-
mentum has been damaged, for example by root re-
sorption, inflammatory periodontal lesions may be
sustained by an active root canal infection (see below,
Fig. 14-26).
Conclusion
Inflammatory lesions may develop from a root canal
infection at the lateral aspects of the root and in furca-
tion regions of two and multirooted teeth. In these
instances, the lesions may be induced and maintained
by bacterial products, which reach the periodontium
through lateral canals. These types of lesions appear
to be rare and do not seem to emerge at a rate that
corresponds to the frequency with which lateral ca-
nals occur in teeth.
MANIFESTATIONS OF ACUTE
ENDODONTIC LESIONS IN THE
MARGINAL PERIODONTIUM
Inflammatory lesions in the periodontal tissue, in-
duced and maintained by root canal infection, often
have a limited extension around the apex of the tooth (
Fig. 14-2) or at the orifice of a lateral canal (Fig. 14-3).
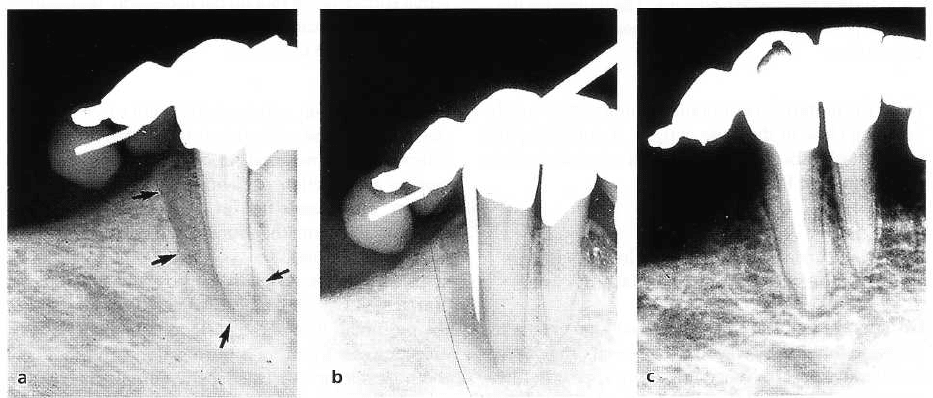
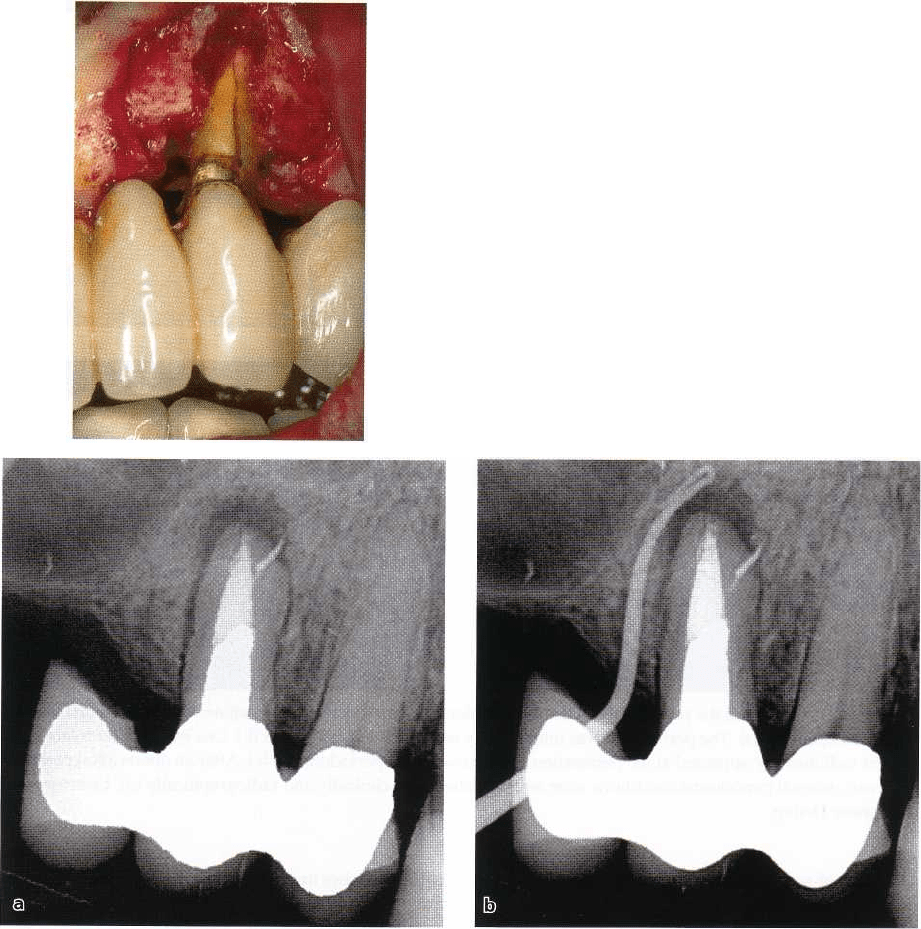
Fig. 14-9. Angular bone defect is observed along the distal root surface of a mandibular canine (a). Apical-
marginal communication was confirmed by periodontal probing (b). Endodontic treatment resulted in complete
reestablishment of the periodontal structures, demonstrating that the periodontal defect in this case was the result
of endodontic infection only. Courtesy of Dr Ralph Milthon.
ENDODONTICS AND PERIODONTICS • 325
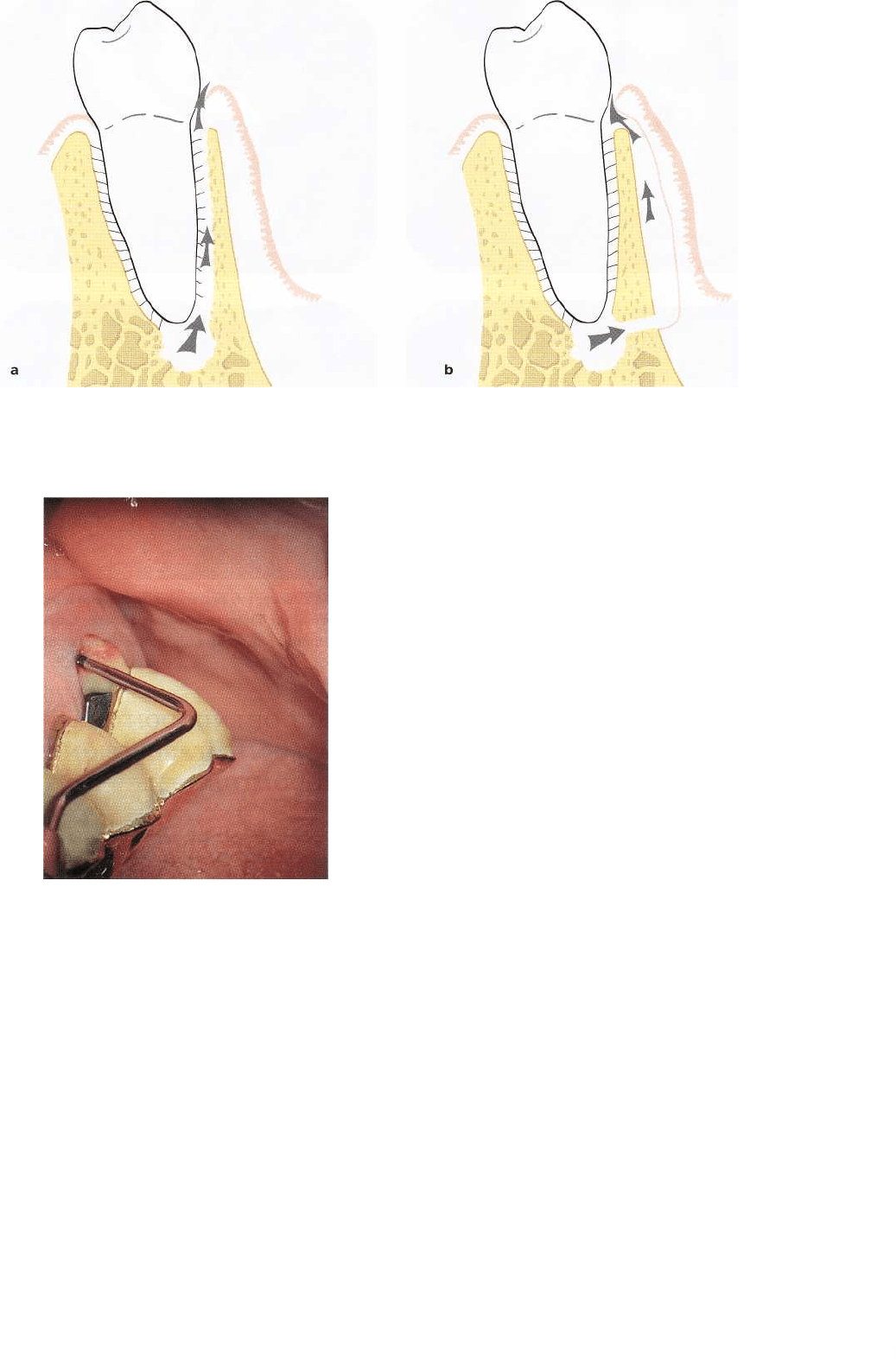
Fig. 14-10. Schematic illustration demonstrating possible pathways for drainage of a periapical abscess into the gin-
gival sulcus/pocket. (a) periodontal ligament fistulation. (b) extraosseous fistulation.
Fig. 14-11. Drainage of pus from probing a periodontal
ligament fistulation of an endodontic lesion associated
with an upper molar.
In conjunction with the initial expansion of an endo-
dontic lesion, the periodontal tissue support can be
lost to the extent that an apical-marginal communica-
tion emerges, in particular when there is already a
substantial loss of periodontal tissue support due to
periodontal disease (Fig. 14-5). Following the exacer-
bation of an established lesion, the subsequent abscess
formation may cause the destruction of the support-
ing tissue structures along the entire root length (Fig.
14-9). This may occur even in a tooth with a normal
height of the attachment apparatus.
The emergence of these processes may or may not
be associated with clinical signs of acute inflammation
including throbbing pain, tenderness to percussion
and apical palpation, increased tooth mobility and
swelling of the marginal gingiva. Note that the same
symptoms are typical of a periodontal abscess due to
either periodontal disease, root fracture, root resorp-
tion or iatrogenic root perforation (see also Fig. 14-27).
In general, drainage of endodontic abscesses into
the sulcus/pocket follows one of two routes (Fig. 14-
10):
1. The suppurative process may cause a sinus tract
along the periodontal ligament space (periodontal
ligament fistulation; Fig. 14-10a). This usually re-
sults in only a narrow opening of the fistula into
the gingival sulcus/pocket and may not be de-
tected unless careful probing of the sulcus is carried
out at multiple sites. Such a fistula may readily be
probed down to the apex of the tooth (Fig. 14-9b), where
no increased probing depth otherwise exists around the
tooth. In multirooted teeth a periodontal ligament
fistulation can drain off into the furcation area (Fig.
14-11). The resulting lesion may then resemble a "
through and through" furcation defect from peri-
odontal disease (Fig. 14-12).
2. A periapical abscess can also perforate the cortical
bone close to the apex and elevate the soft tissue
including the periosteum from the bone surface,
and drain into the gingival sulcus/pocket (Fig. 14-
10b). This type of drainage will result in a wide
opening of the fistula into the sulcus/pocket (ex-
traosseous fistulation), and is most often seen at the
buccal aspect of the tooth. Since this type of fistula
is not associated with loss of bone tissue at the inner
walls of the alveolus, a periodontal probe cannot
penetrate into the periodontal ligament space.
326 • CHAPTER 14
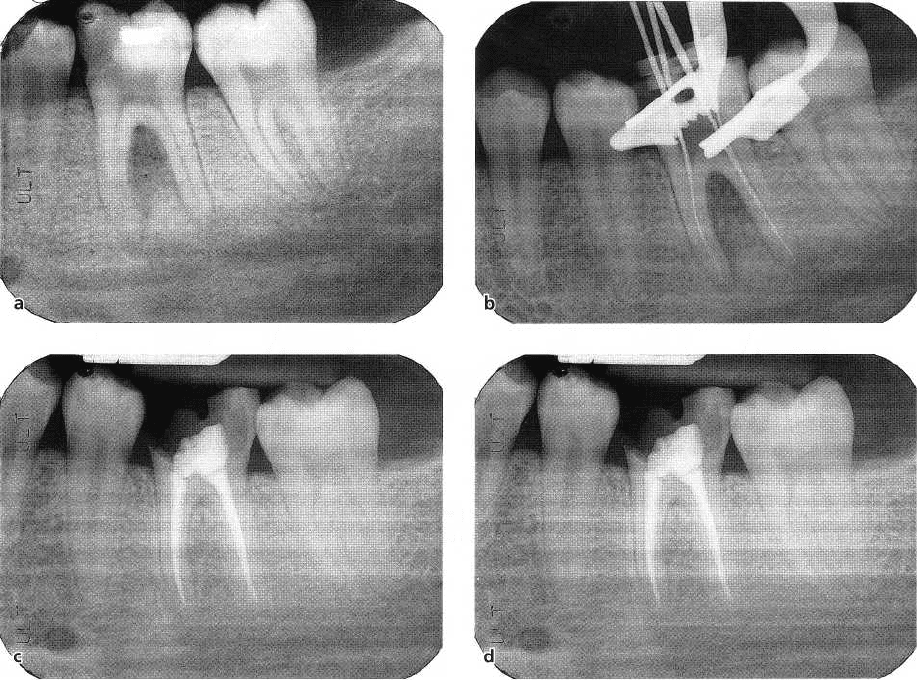
Fig. 14-12. A large radiolucent area is seen in the furcation region of the lower left first molar (tooth #36)
mimicking what potentially could be a through and through furcation involvement (a). There is, however, a
distinct caries lesion and the pulp is necrotic. Upon endodontic therapy (b,c) the 18-month follow-up
radiograph demonstrates complete bone fill in the region (d). Courtesy of Dr Kevin Martin.
It is important to realize that the lesions described are
strictly of endodontic origin. Therefore, following
conventional endodontic therapy, directed to elimi-
nate the root canal infection, both types of marginal
communications should, following proper treatment,
heal rapidly without a persistent periodontal defect (
Figs. 14-5, 14-12 and 14-13). Thus, there is generally
no need for adjunctive periodontal therapy. The endo-
dontic treatment of the involved tooth should be per-
formed without delay to prevent repeated exacerba-
tions and the establishment of a permanent apical-
marginal communication.
Conclusion
Acute manifestations of root canal infections can re-
sult in rapid and extensive destruction of the attach-
ment apparatus. Abscesses may drain off in different
directions of which (1) a sinus tract along the peri-
odontal ligament space and (2) an extraosseous fistu-
lation into the gingival sulcus/pocket warrant par-
ticular attention from a differential diagnostic point of
view. Following proper endodontic therapy, these le-
sions should be expected to heal without a persistent
periodontal defect.
IMPACT OF ENDODONTIC
TREATMENT MEASURES ON THE
PERIODONTIUM
When breakdown of periodontal tissue is associated
with a root-filled tooth, endodontic etiology should be
taken into account, particularly if the root filling is of
poor quality. From unfilled spaces in the root canal,
sustaining bacterial growth, infectious products may
emerge into the periodontium along the very same
pathways as in an untreated tooth with infected pulp.
Clinical observations suggest that such infections may
contribute to increased probing depth (Jansson et al.
1993) and results of clinical follow-ups have shown
retarded or impaired periodontal tissue healing sub-
sequent to periodontal therapy of endodontically
treated teeth with periapical pathology (Ehnevid et al.
1993a,b). From these observations, it follows that en-
dodontic retreatment may be considered as an adjunct
to periodontal therapy whenever a root canal filling is
defective and/or displays signs of periapical inflam-
mation. Root-filled teeth in general, however, do not
seem to be associated with an impaired periodontal
status (Miyashita et al. 1998).
ENDODONTICS AND PERIODONTICS • 327
Fig. 14-13. Facial swelling associated with tooth #46 as a result of a periapical abscess (a). Patient had experienced
pain and tenderness in the area for 1 week. Periodontal probing disclosed a deep facial pocket along the mesial
root (b). Radiographically, the lesion circumscribed the mesial root with marginal extension in the furcation (c).
It was not possible to determine the condition of the pulp by conventional pulp-vitality tests. Test cavity
preparation revealed a necrotic pulp that was endodontically treated including intracanal dressing with calcium
hydroxide. Obvious reduction in lesion size was observed 3 months after treatment (d). Gingival lesion resolved
leaving no abnormal probing depth (e), although radiographically a small bone defect remained in the furcation
area (d, f) Endodontic treatment was completed by filling the root canals with gutta-percha. Twelve months after
root filling complete resolution of the bone defect had occurred (f). Diagnosis and treatment of this case was
carried out by one of the authors (G.B.) in collaboration with Dr David Simpson.
Periodontal inflammatory lesions may also result hand, strong antiseptic drugs used for root canal dis-
from mechanical as well as chemical irritation initi- infection and pulp devitalization cause severe dam-
ated by root canal treatment. However, medicaments age if they leak into the periodontal tissue (Fig. 14-
for canal irrigation and disinfection as well as materi- 14a,b).
als for filling used in modern endodontics are comparatively
well tolerated by the connective tissue of the periodontium, even
if, during treatment, they are forced into the periodontal
ligament. On the other
328 • CHAPTER 14
Fig. 14-14. (a) Clinical photograph showing a periodontal defect at the mesial aspect of tooth #46. The pulp of the
tooth had been subjected to a treatment with paraformaldehyde applied in order to cause its devitalization.
Leak-age of the agent along a defect temporary restoration had obviously occurred as indicated by the loss of
proximal bone and presence of a bone sequestrum (b).
Root perforations
During endodontic treatment, and in conjunction with
preparation of root canals for the insertion of posts,
instrumentation can accidentally cause perforation of
the root and wounding of the periodontal ligament (
Alhadainy 1994). Perforations can be made through
the lateral walls of the root or through the pulpal
floor in multirooted teeth. At the site of perforation,
the subsequent inflammatory reaction can result in
the formation of a periodontal pocket, if the
perforation is located close to the gingival margin (
Lantz & Persson 1967, Stromberg et al. 1972, Peters-
son et al. 1985). Other complications include exacer-
bation of a preexisting periodontal lesion and devel-
opment of clinical symptoms, similar to those of a
periodontal abscess, e.g. acute pain, swelling, drain-
age of pus from the pocket, increased tooth mobility
and further loss of fibrous attachment (Fig. 14-15).
Early detection of the complication is crucial to
provide reasonable conditions for successful treat-
ment. Diagnosis may be based on the occurrence of
sudden pain and bleeding during preparation of root
canals coronal to the working length. Such signs are
likely to be less distinct if the perforation occurs dur-
ing a procedure conducted under local anesthesia. In
such cases bleeding may not invariably be provoked.
For example, when post preparations are carried out
by means of a machine-driven instrument, a smear
layer is formed that may clog up the blood vessels.
Thus, in many instances no bleeding will be noticed
until the following visit, when granulation tissue is
formed and has proliferated into the root canal space
from the site of perforation. These granulations some-
times bleed profusely on attempts to remove them,
which in turn may jeopardize adequate placement of
an internal perforation seal. For this reason treatment
of a root perforation should be initiated once discov-
ered.
The series of radiographs in Fig. 14-16 demon-
strates the successful outcome of a treatment of a
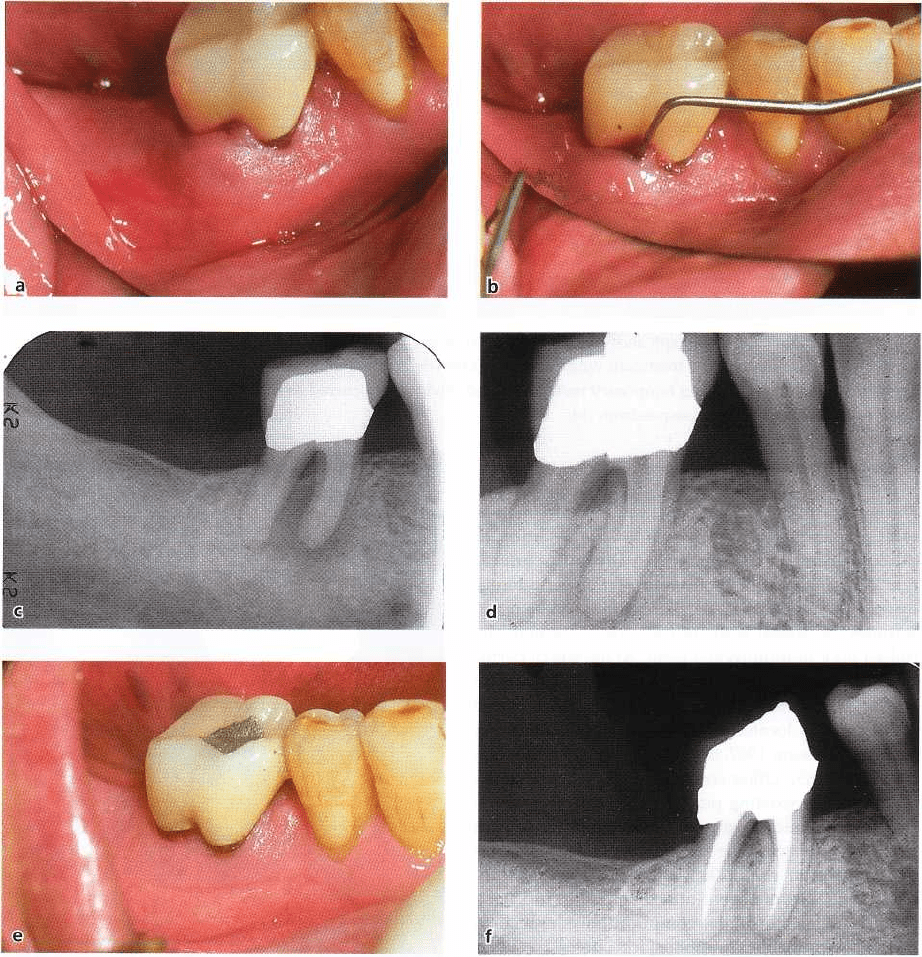
Fig. 14-15. Angular bone defect at the distal root sur-
face of a mandibular premolar (arrows). The root is per
forated. Conceivably, this occurred in conjunction with
preparation of the root canal for a post and core. Clini-
cal symptoms included drainage of pus from the
pocket and increased tooth mobility. The tooth was ex
tracted.
perforation made in the furcation of a mandibular
molar. Healing of the lesion in the periodontium de-
pends largely on whether bacterial infection can be
excluded from the wound site by a tight seal of the
perforation (Beavers et al. 1986). If the perforation is
close to the sulcus area, or conducted through the floor
of a multirooted tooth, the inflammatory response
may induce the proliferation of sulcular epithelium to
form a deepened periodontal pocket (Petersson et al.
1985).
ENDODONTICS AND PERIODONTICS • 329
Fig. 14-16. Perforation of the pulpal floor of the mandibular first molar occurred in conjunction with a search
for root canal openings (a). The perforation was immediately sealed with gutta-percha (b). One month after
treatment a slight radiolucency appeared at the perforation site (arrow) in the periodontium (c). After an
observation period of 2 years, normal periodontal conditions were re-established both clinically and
radiographically (d). Courtesy of Dr Gunnar Heden.
Repair of root perforations is unpredictable and a
questionable prognosis of treatment should be antici-
pated (Petersson et al. 1985). Major reasons are that
perforations frequently are difficult to access for a
proper seal. Furthermore, the perforation is often
made at an oblique angle in the lateral wall of the root
and the artificial canal may then have an oval-shaped
orifice into the periodontium. Obturation of such de-
fects with gutta-percha, for example, can result in a
poor seal and a risk of subsequent bacterial irritation
of the periodontal tissue.
Over the years a large number of therapeutic agents
and methods have been proposed for the manage-
ment of root perforations (Alhadainy 1994). Materials
suggested for sealing include amalgam, zinc oxide
and eugenol cements, calciumhydroxide-containing
pastes both chemically cured and light cured and
plaster of Paris. More recently, mineral trioxide aggre-
gate (MTA) has come into vogue by virtue of promis-
ing clinical results (Arens 8z Torabinejad 1996,
Schwartz et al. 1999) and by observation in animal
experiments of cementum depositions against the ma-
terial (Torabinejad et al. 1997, Holland et al. 2001).
For mid-root and cervical perforations, non-surgi-
cal approaches including placement of an internal seal
are preferable to surgical procedures as the latter often
results in pocket formation and furcation involve-
ment. Furthermore, surgical approaches are not al-
ways feasible because of the inherent difficulty in
accessing many perforation sites. In such cases, as a
last resort, extraction followed by repair and re-im-
plantation of the tooth has been attempted. In multi-
rooted teeth, hemisection and extraction of one or two
roots may be the treatment of choice.
Conclusion
Inflammatory lesions in the marginal periodontium as
manifested by increased probing depth, suppuration,
increased tooth mobility and loss of fibrous at-
tachment may result from an undetected or unsuc-
cessfully treated root perforation. If an iatrogenic root
perforation occurs during instrumentation of root ca-
nals, filling of the artificial canal to the periodontium
should be carried out immediately. Outcome of treat-
ment depends on how well the wound site can be
sealed and protected from infection. The closer the
perforation is to the marginal gingiva, the greater the
330 • CHAPTER 14
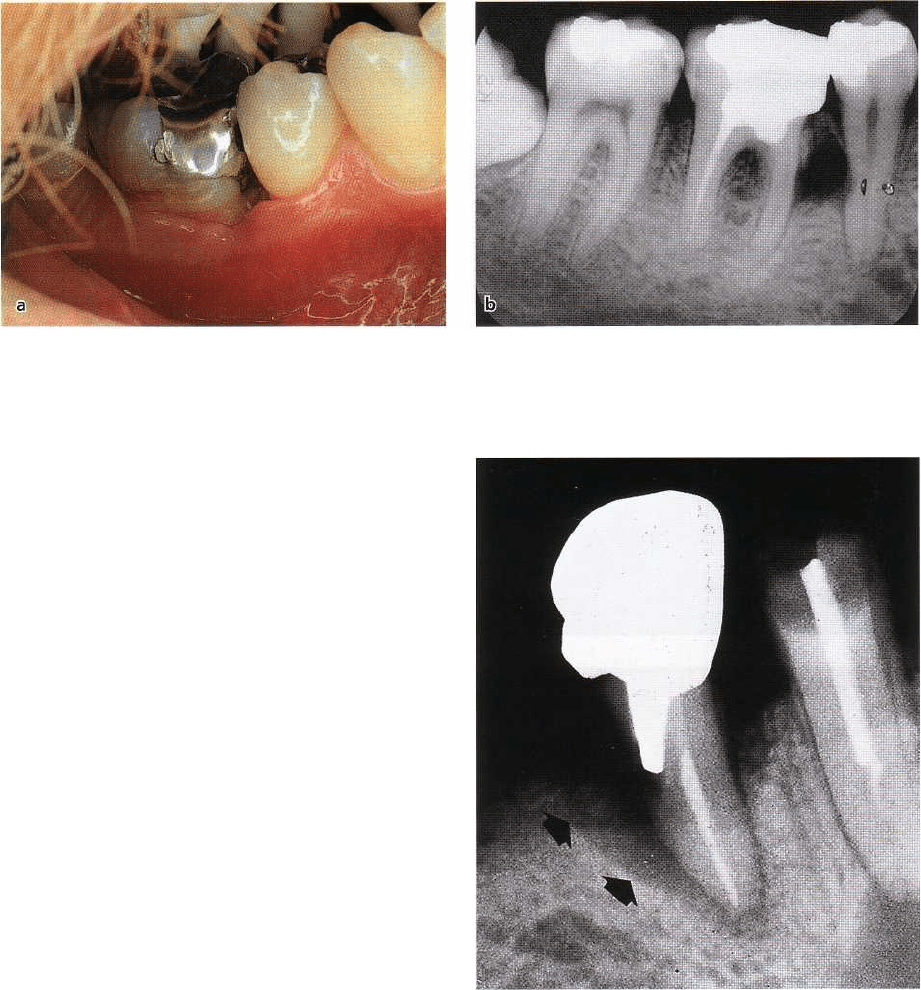
Fig. 14-17. Vertical root fracture of a maxillary root-
filled upper canine included as abutment in a pros-
thetic reconstruction. Due to the inflammatory break-
down, alveolar bone facial to the root surface is
absent.
Fig. 14-18. Periapical radiolucency associated with an upper second premolar (a) which turned out to be caused by
a longitudinal root fracture. There was a buccal deep pocket probing depth. (b) A gutta-percha point has been in-
serted in a fistulous tract. The widely prepared root canal and the cantilever most likely contributed to the risk for
fracture in this case. Courtesy of Dr Tomas Kvist.
likelihood of proliferation of sulcular epithelium to
the perforation site.
Vertical root fracture
Clinical symptoms that are typical for endodontic and
periodontal lesions may also appear at teeth with
vertical root fractures. A vertical root fracture is de-
fined as a fracture of the root that is longitudinally
oriented at a more or less oblique angle towards the
long axis of the tooth (Fig. 14-17). It can traverse the
root in different directions mesially/distally or
facially/lingually and may or may not involve the
pulpal chamber. A vertical root fracture can extend the
entire length of a tooth and involve the gingival sul-
cus/pocket area but may also be incomplete and con-
fined to either the coronal or apical ends. Furthermore,
it should be noted that even though vertical root frac-
tures usually involve opposite sides of the root, occa-
sionally only one aspect of the root is involved.
As a result of bacterial growth in the fracture space,
the adjacent periodontal ligament will become the seat
of an inflammatory lesion, which causes breakdown of
connective tissue fibers and alveolar bone (Fig. 14-17)
. Breakdown can manifest itself radiographically in a
number of different ways (Figs. 14-18, 14-19c, 14-20).
Thus, the radiographic defect may be similar to those
found at endodontic and periodontal lesions. In other
situations the appearance may be atypical of

ENDODONTICS AND PERIODONTICS • 331
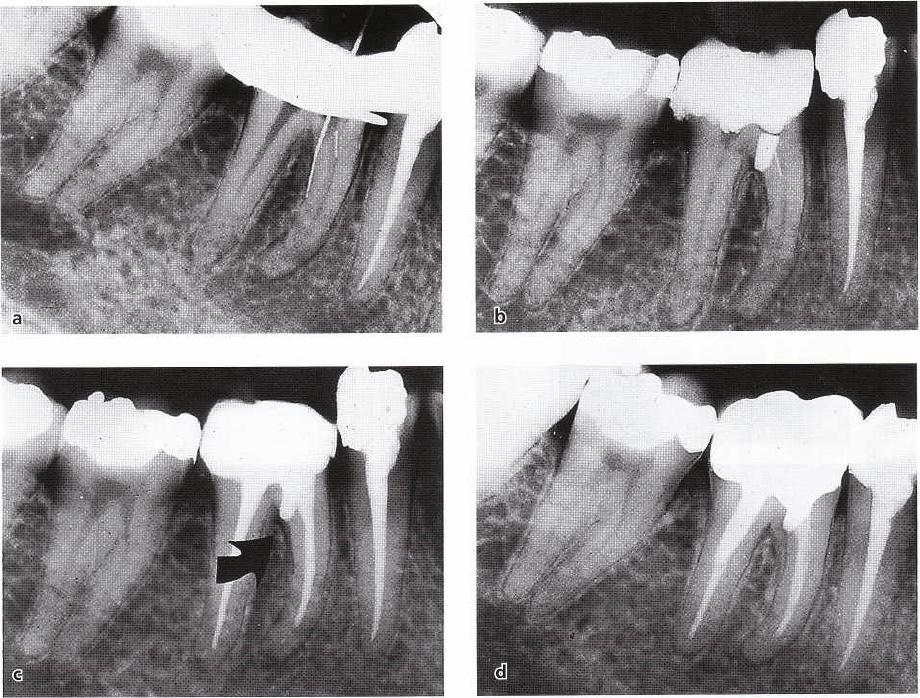
Fig. 14-19. A typical case of root fracture. The first maxillary premolar had been asymptomatic for 20 years after
completion of endodontic treatment and bridge work. Patient sought treatment because of suddenly occurring pain,
tenderness and facial swelling (a). A deep periodontal pocket can be probed at the buccal aspect of the tooth (b),
while other sites showed no abnormal probing depths. Radiographs (c) revealed a radiolucent area along the
rnesial aspect of the tooth. A set of radiographs taken 6 months earlier at a recall session (d) showed no such lesion.
The elevation of a mucoperiosteal flap (e) revealed substantial loss of marginal bone at the buccal aspect of the root
and a fracture in a mesiodistal direction could be confirmed. Following removal of bone, the root was separated
from the crown (f) and extracted.
these disorders. A widening of the periodontal liga- fracture (Pitts & Natkin 1983, Testori et al. 1993, Tamse
ment space along one or both of the lateral root sur- et al. 1999a).
faces may indicate the presence of a root fracture. A Clinical symptoms associated with vertical root
thin halo-like apical radiolucency is another example fractures show a varying character. Occasionally, there
of a radiographic lesion suggestive of a vertical root may be pronounced pain symptoms and abscess for-
mation – symptoms similar to those occurring with
33
2
• CHAPTER 14
Fig. 14-20. Mandibular premolar included in a 4-unit bridge showing a bone lesion at the mesial aspect. In one of
the projections there is no evidence of fracture (a) while in another radiograph, taken with a slight shift of angula
tion, a fracture line is clearly visible (b). Courtesy of Dr K-G. Olsson.
Fig. 14-21. Unrestored, cracked left maxillary first
molar causing symptoms of pulpitis. The patient, a
47-year-old male, had complained of pain in the TMJ
-region. Following the preparation of a test cavity a
clear split line was observed at the bottom of the cavity,
confirming the cause of the pain symptoms. Courtesy
of Dr H. Suda.
periodontal or endodontic abscesses. In other in-
stances, a narrow, local deepening of a periodontal
pocket (Fig. 14-19), associated with the fracture, may
be the only clinical finding. Other clinical symptoms
occurring in conjunction with root fractures are ten-
derness to mastication, fistulous tract, mild pain and
dull discomfort. The diagnosis of a vertical root frac-
ture is often difficult because the fracture is usually not
readily detectable by clinical inspection unless there
is a clear separation of the root fragments. By radio-
graphic examination the central X-ray beam has to be
parallel to the fracture plane to give a radiographic
appearance (Fig. 14-20). The suspicion of a vertical
root fracture is often inferred from a pocket probing
depth in an aberrant position, for example at a buccal
or lingual aspect of a tooth in a dentition which other-
wise is free from symptoms of periodontal disease (Fig
14-18). Another strong indication is the sudden ap-
pearance of clinical symptoms and/or radiographic
lesion on a root-filled tooth that has remained asymp-
tomatic and without lesion for many years (Fig. 14-
19a-d).
A number of diagnostic procedures can be under-
taken to confirm the diagnosis. Application of various
dye solutions, e.g. methylene blue or iodine tincture,
on to the crown and the root surface can sometimes be
indicative. As the dye enters the fracture space, it will
show up as a distinct line against the surrounding
tooth substance. Indirect illumination of the root, us-
ing fiber-optic light, can also be of value. The fiber-op
tic probe should then be placed at various positions
on the crown or the root, whereby the fracture line
may clearly present itself. The surgical microscope or
an endoscope, providing both enlargement and di-
rected light, are other valuable tools to detect a frac-
ture.
In premolars and molars the diagnosis may be
supported from observation of varying pain sensa-
tions elicited by loading facial and lingual cusps. The
procedure includes asking the patient to bite down on a
Burlew disc or a specially designed plastic stick (
FracFinder). Separate loading of either buccal or lin-
gual cusps eliciting pain sensation from one, but not
the other, loaded portion indicates the potential of a
fracture. Often the diagnosis of a vertical root fracture
has to be confirmed by surgical exposure of the root