Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.


DIFFERENTIAL DIAGNOSES: PERIODONTAL TUMORS AND CYSTS • 303
b
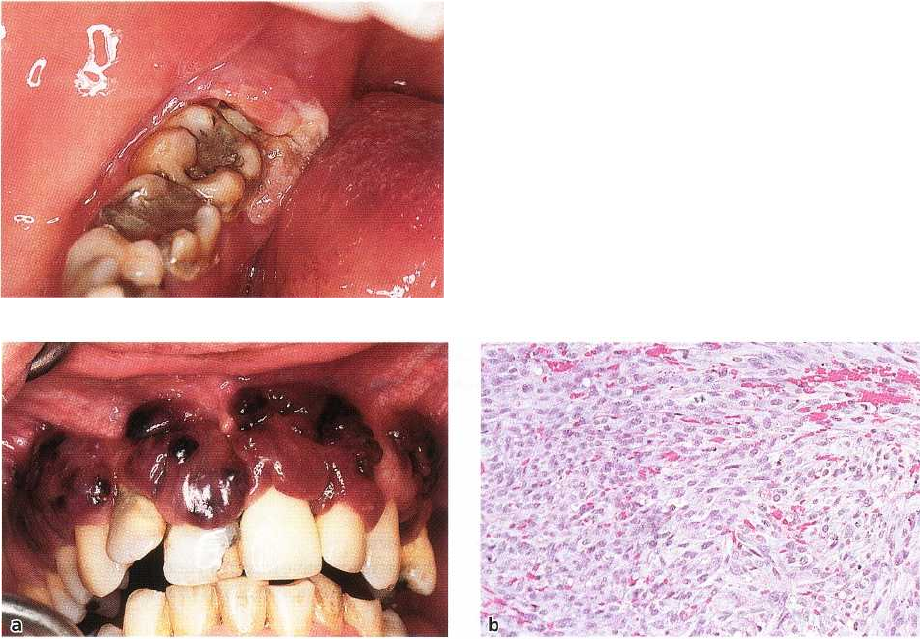
Fig. 13-8. (a) Hemangioma of alveolar mucosa at right maxillary canine. The lobulated blue lesion is a cavernous
type of hemangioma as shown in (b).
mandibular incisors are the most commonly affected
and the lesions are more frequent in women than in
men. They occur most often between the fourth and
the fifth decade. There are usually no symptoms.
Radiographical findings depend on the develop-
mental phase of the lesion, varying from well-circum-
scribed periapical radiolucencies (Fig. 13-7a), an inter
-mediate phase with irregular radiopacities within the
radiolucent zones, to a late phase with well-circum-
scribed periapical radiopacities bordered by distinct
radiolucent zones. The significance of the lesion is the
differential diagnostic problem in distinguishing it
from periapical granuloma and radicular cyst.
Histopathology
The lesion develops from an osteolytic phase in which
periapical bone is replaced by cellular fibroblastic
tissue through a cementoblastic phase in which a
cementum-like tissue is formed within the fibrous
tissue (Fig. 13-7b). In the late phase the lesion consists
of dense, irregular cementum-like material. The his-
tology resembles that seen in cemento-ossifying fi-
broma and fibrous dysplasia.
Therapy
Periapical cemental dysplasia is innocuous and needs
no surgical treatment as it is usually self-limiting.
Radiographic follow-up examination every fifth year
may be considered.
BENIGN NEOPLASMS OF
PERIODONTAL SOFT TISSUES
Most of the soft tissue tumors that occur in various
sites of the body can be seen in the oral mucosa as well.
Examples are neoplasms derived from peripheral
nerves (neurilemoma ("schwannoma") and neurofi-
broma), blood vessels (hemangioma) and smooth
muscle (leiomyoma) (Pindborg 1992, Neville et al.
1995). None of them, however, have a special propen-
sity to occur on the gingiva and usually they are
clinically indistinguishable from focal fibrous hyper-
plasias or other non-neoplastic lesions. Exceptions are
hemangiomas and nevi, which are described below.
Furthermore, squamous papilloma and verruca vul-
garis are dealt with in this section.
Hemangioma
Clinical features
Hemangiomas show a predilection for the head and
neck region and are rather frequent tumors of the oral
mucosa. There is a predilection for women (Neville et
al. 1995). Several authors doubt whether hemangi-
omas are true neoplasms and suggest they be classi-
fied as hamartomas or developmental anomalies.
Most cases are present at birth or occur shortly there-
after, although some cases develop in adults. Some of
them may undergo regression. Hemangiomas present
as flat or raised, sometimes lobulated, soft lesions of
blue to red color (Fig. 13-8a). They are usually asymp-
tomatic but may bleed when traumatized. Typically,
they blanch on pressure and the color returns shortly
after releasing the pressure. This is not the case with
other bluish lesions such as mucous cysts.
Histopathology
Hemangiomas are divided into capillary and cavern-
ous types (Fig. 13-8b) depending on the size of the
vessels. Mixed types are not uncommon. Especially in
the capillary type, sheets of proliferating endothelial
cells are common. Some hemangiomas resemble pyo-
genic granulomas but ulceration and an inflammatory
component are not typical of hemangiomas.
Treatment
Hemangiomas may give rise to severe bleeding if
treated with conventional surgery and cryosurgery
may be the treatment of choice where treatment is
necessary and possible. Large tumors which are not
suitable for surgery may be embolized or injected with
agents to induce fibrosis. Episodes of bleeding at eat-
ing and toothbrushing are common indications of
treatment.
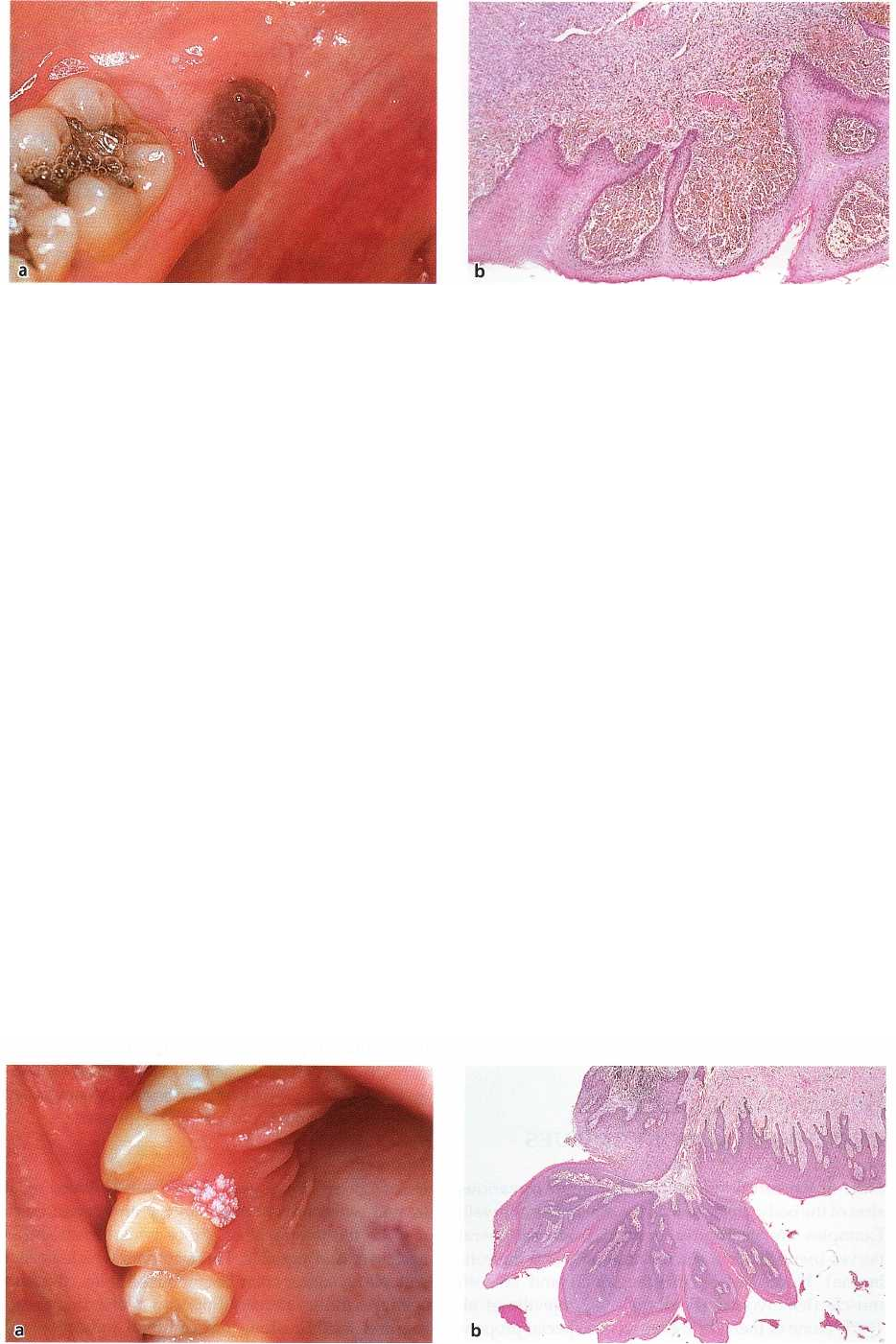
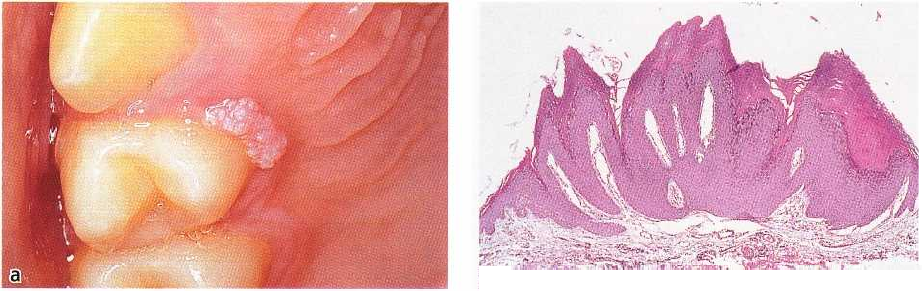
Fig. 13-10. (a) Gingival papilloma of right maxillary first premolar region. (b) Photomicrograph of lesion in (a).
304 • CHAPTER 13
Fig. 13-9. (a) Nevus of lower right mandibular retromolar area. Histopathologic examination showed that the ne
vus cells were solely located in the subepithelial connective tissue (b), which is why the lesion is an
intramucosal nevus. Note melanin formation by the nevus cells.
Nevus
Clinical features
The term "nevus" is used for a variety of lesions of the
skin and oral mucosa. Here it will be used synony-
mously with a pigmented lesion containing nevus
cells (brown or nevocellular nevus) or a lesion contain-
ing melanocytes in the connective tissue (blue nevus).
Nevus cells are derived from the neural crest and are
related to melanocytes. Nevus cells are capable of
producing melanin pigment, although they do not
invariably do so.
Nevi are very common on the skin but rare in the
oral mucosa. They usually develop during childhood
and they are more common in women than in men.
Most intraoral nevi are seen on the palate but the
gingiva is not an uncommon location (Buchner &
Hansen 198Th). They can present as flat, slightly raised
lesions or even as a tumor (Fig. 13-9a). They are usu-
ally brown or black or they may show little or no
pigmentation. The blue nevus should be differenti-
ated from an amalgam tatoo.
Histopathology
Nevocellular or brown nevus contains nests of nevus
cells located along the basal cell layer of the epithelium
(junctional activity, junctional nevus), solely in the
connective tissue (intramucosal nevus) (Fig. 13-9b), or
in both locations (compound nevus). The nevus cells
may or may not contain melanin pigment. In blue
nevus, dendritic, melanin-producing melanocytes oc-
cur in the connective tissue (Neville et al. 1995).
Treatment
Some malignant melanomas of the skin seem to de-
velop from nevi. Especially in adults, nevi with junc-
tional activity should be viewed with caution. In the
oral mucosa little is known about malignant transfor-
mation of nevi. Excision of oral nevi is generally rec-
ommended (Buchner et al. 1990).
Papilloma
Clinical features
The term papilloma covers four or five different types
of benign epithelial proliferations: squamous and fili-
form papilloma, verruca vulgaris, condyloma and fo-
cal epithelial hyperplasia (FEH). Malignant transfor-
mation is very rare or non-existing and usually there
are no symptoms. Human papilloma virus (HPV) is
commonly found in these lesions and a causative role
of HPV in the development of at least some of these
lesions is strongly suggested (Pindborg & Prtorius
1987, Garlick & Taichman 1991). Generally, a relation-
ship between the histomorphology and distinct HPV
b
DIFFERENTIAL DIAGNOSES: PERIODONTAL TUMORS AND CYSTS • 305
Fig. 13-11. (a) Gingival verruca vulgaris of left maxillary first premolar region. Clinically, it resembles the lesion
shown in Fig. 13-10 but histopathologic examination of the surgically removed lesion showed characteristics typi
cal of verruca (b).
types, of which about 70 are known, can be establ-
ished. Verruca vulgaris is dealt with separately and
condyloma and FEH will not be mentioned further
here.
Squamous papilloma and filiform papilloma can be
distinguished by detailed clinical and histologic fea-
tures (Prxtorius, personal communication). Here,
however, they will be dealt with together. They are
exophytic, pedunculated or sessile lesions with a red-
dish/normal or whitish/gray color and a granu-
lar/moruloid or filiform/digitated surface (Fig. 13-
10a). They are mainly seen in the third to fifth decade,
in contrast to verruca vulgaris, which is usually seen
in younger age groups. The soft palate is the most
common location. It is often difficult to differentiate
clinically between verruca vulgaris and squamous
and filiform papillomas.
Histopathology
Squamous and filiform papillomas are covered by
squamous epithelium with deep crypts in the surface.
The epithelium is keratinized or non-keratinized with
irregular rete ridges which cover sometimes ramified
connective tissue papillae (Fig. 13-10b).
Treatment
Surgical excision, including the base of the lesion, is
the treatment of choice. Recurrence is uncommon.
Verruca vulgaris
Clinical features
Verruca vulgaris is common on the skin. In the oral
mucosa verrucae are less common and are often seen
as a result of autoinoculation in children with warts
on the fingers. The majority are located on the lips and
in the palate and 10-20% are located on the gingiva (
Green et al. 1986, Pindborg & Prxtorius 1987). Ver-
ruca vulgaris seems to be associated with HPV type 2
and 4.
Clinically the lesions are sessile, exophytic or raised
with a whitish surface with angulated verrucous pro-
jections (Fig. 13-11a).
Histopathology
Histologically, they show a papillomatous surface
with hyperkeratinization and elongated rete ridges (
Fig. 13-11b). Characteristically, the rete ridges bend
inward at the margins of the lesion, pointing toward
a center below the lesion (Prtorius-Clausen 1972).
Treatment
Some verrucae disappear spontaneously, especially in
children. Treatment usually consists of surgical exci-
sion. Recurrence occurs in some cases.
Peripheral odontogenic tumors
Clinical features
Odontogenic tumors primarily occur as intraosseous
growths but sometimes they present in a peripheral
location in the gingiva (Buchner & Sciubba 1987, Pind-
borg 1992). The following entities may occur as a
gingival tumor: ameloblastoma, squamous odonto-
genic tumor, ameloblastic fibro-odontoma, adenoma-
toid odontogenic tumor, calcifying odontogenic cyst,
calcifying epithelial odontogenic tumor (Fig. 13-12a,b)
and odontogenic fibroma. Peripheral odontogenic tu-
mors usually present as non-ulcerated sessile or pen-
dunculated gingival lesions. The clinical features,
thus, are nonspecific, resembling focal fibrous hyper-
plasias or other non-neoplastic lesions (Buchner &
Sciubba 1987). Most examples are rather small.
Histopathology
Generally, these lesions show histopathologic features
similar to the intraosseous forms of the tumors (Fig.
13-12b).
Treatment
Due to the rather small number of reported cases and
the varying behavior of the different odontogenic tu-
mors mentioned above, general guidelines will not be
306 • CHAPTER 13
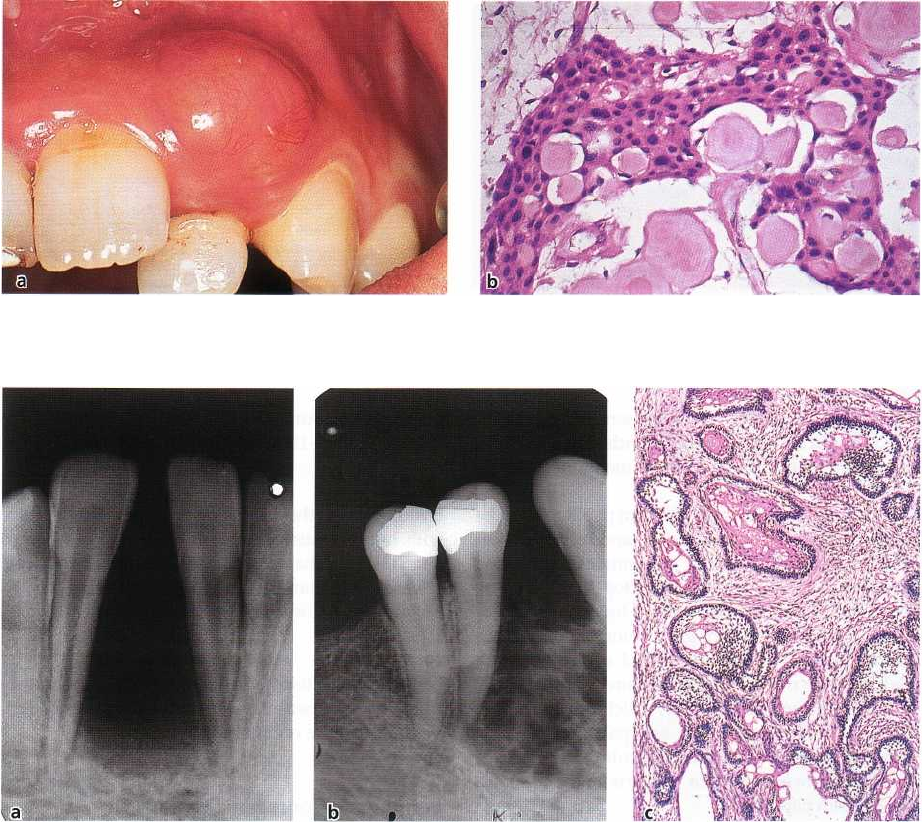
Fig. 13-12. (a) Gingival swelling of left maxillary lateral incisor region. The tumor was surgically removed and the
histopathologic examination revealed a calcifying epithelial odontogenic tumor (b).
Fig. 13-13. (a) Radiograph shows well-demarcated loss of alveolar bone between displaced mandibular incisors. Af
ter surgical removal and histopathologic examination (c) the lesion was diagnosed as an ameloblastoma. (b)
Radio-graph with irregular radiolucency with scalloped periphery in alveolar bone of mandibular premolar and
canine region. The teeth are displaced. Biopsy revealed an ameloblastoma.
given. Apparently an innocuous clinical behavior is
characteristic of most reported cases, showing a dif-
ferent biologic behavior than their intraosseous coun-
terparts (Buchner & Sciubba 1987). However, some
examples of recurrence have been reported.
It should be mentioned here that odontogenic tu-
mors or hamartomas are frequently detected his-
tologically in the soft tissue in operation specimens
from exposure of molars delayed in eruption for no
obvious clinical cause (Philipsen et al. 1992). The fate
of these lesions, had the surgical exposure not been
performed, is unknown.
BENIGN NEOPLASMS OF
PERIODONTAL HARD TISSUES
Ameloblastoma
Clinical features
The ameloblastoma is a benign but locally invasive
neoplasm derived from odontogenic epithelium (Kra-
mer et al. 1992). It occurs most commonly between 20
and 40 years of age and affects women and men
equally. The most common location is the molar re-
gions, with most tumors being localized in the man-
dible (van der Waal 1991, Reichart et al. 1995). The
tumors grow slowly and sometimes reach excessive
sizes before symptoms arise. Such symptoms may be
expansion of cortical bone and displacement of teeth.
The alveolar nerve usually remains undisturbed even
in cases of large tumors in the mandible, but roots of
DIFFERENTIAL DIAGNOSES: PERIODONTAL TUMORS AND CYSTS • 307
Fig. 13-14. (a) Squamous odontogenic tumor demonstrating substantial diffuse radiolucency of alveolar bone in left
maxillary incisor region. The diagnosis was revealed by biopsy showing features presented in (b).
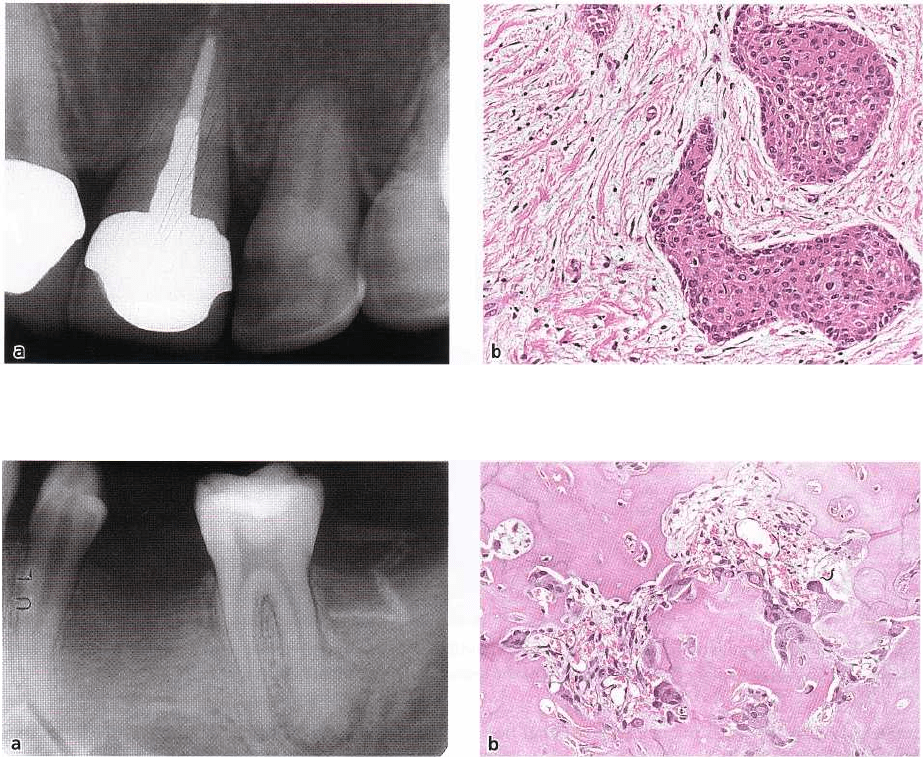
Fig. 13-15. (a) Radiographic presentation of a benign cementoblastoma in a 20-year-old man. The periapical lesion
of the mandibular second molar shows an almost circular radiopacity surrounded by a radiolucent margin. Part of
the root is resorbed and replaced by lesional tissue. The tumor is composed of cementum-like tissue (b).
adjacent teeth are sometimes resorbed. Intraosseous
ameloblastomas rarely demonstrates mucosal in-
volvement in the form of gingival tumor. Radiog-
raphically, the ameloblastoma demonstrate unilocular
or multilocular radiolucency, which is usually well-
circumscribed. The radiographic features may be in-
distinguishable from jaw cysts but may also resemble
loss of bone due to marginal periodontitis (Fig. 13-13a,
b).
Histopathology
The general histopathologic features consist of islands
and/or strands of odontogenic epithelium in a mature
collageneous stroma (Fig. 13-13c). Columnar or cuboi-
dal epithelial cells resembling ameloblasts surround
loosely arranged epithelial cells resembling the stel-
late reticulum of the enamel organ.
Treatment
Conservative and radical surgery are equally common
types of treatment, and recurrences are common fol-
lowing both treatment modalities (Reichart et al.
1995). This is probably due to difficulties in removing
the proliferating cords of tumor tissue in the marrow
spaces at the periphery of the tumor. In general, more
radical treatment of maxillary ameloblastomas than of
mandibular ones is recommended (Reichart et al.
1995).
Squamous odontogenic tumor
Clinical features
This odontogenic tumor was first described in 1975 (
Pullon et al. 1975) and very few examples have been
reported. However, as the tumor seems to develop
from the periodontal ligament, presumably from the
epithelial rests of Malassez, and is most often associ-
ated with the lateral root surface of an erupted tooth,
it is important to include it here as an example of a
periodontal tissue reaction.
Squamous odontogenic tumor has been found in
almost all age groups and does not seem to have a
predilection for any site or gender. Radiographically,
the findings are not specific (Fig. 13-14a). They often
show a triangular radiolucent defect between the

308 • CHAPTER 13
Fig. 13-16. Gingival squamous cell carcinoma of left mandibular canine and premolar region. (a) Facial aspect. (b)
Mesial and lingual aspect. (c) Photomicrograph of the lesion showing carcinoma in right half.
roots of two teeth which may suggest vertical bone
loss (Neville et al. 1995).
Histopathology
The characteristic findings are islands of squamous
epithelium in a mature collageneous stroma (Fig. 13-
14b). There are no columnar peripheral cells or stellate
reticulum-like cells as in the ameloblastoma.
Treatment
Local excision or enucleation is the most common type
of treatment. There seems to be some tendency for
recurrence.
Benign cementoblastoma
Clinical features
Benign cementoblastoma is a slow-growing neoplasm
forming hard tissue around the apex of a tooth (Kra-
mer et al. 1992). It is most common in the mandibular
premolar and molar region, is almost equally common
among men and women, and is most often seen in the
second decade (Ulmansky et al. 1994). The tumor is
slowly growing and may cause swelling and pain.
Radiographically, a periapical radiopacity typically
surrounded by a radiolucent margin of uniform width
is seen (Fig. 13-15a) (Ulmansky et al. 1994). The tumor
may obscure the apex of the involved tooth and root
resorption with fusion of the tumor with the tooth is
characteristic. The involved tooth is usually vital.
Histopathology
The tumor is built up of cementum-like tissue with
numerous reversal lines, the tissue being attached to
the tooth. Between the cementum-like areas the tissue
is cellular, and in the periphery it is unmineralized (
Fig. 13-15b). A small biopsy of this tumor may be
difficult to differentiate from osteosarcoma.
Treatment
Surgical enucleation is the treatment of choice, al-
though this may be difficult due to the relationship
between the tumor and the related tooth.
MALIGNANT NEOPLASMS OF
PERIODONTAL SOFT TISSUES
Squamous cell carcinoma
Clinical features
In the literature it is rare to see a distinction main-
tained between gingival cancer and cancer developed
on the edentulous alveolar ridge. Thus, many reports
deal with cancer of the "gums". In most of these cases
men have dominated, and only older people are af-
DIFFERENTIAL DIAGNOSES: PERIODONTAL TUMORS AND CYSTS • 309
Fig. 13-17. Metastasis from adenocarcinoma of lung.
The neoplasm affects lingual gingiva of right mandibu
lar second molar and mucosa covering semi-
impacted third molar.
Fig. 13-18. (a) Gingival Kaposi's sarcoma of the maxilla in 33-year-old man with AIDS. (b) Histopathologic features
of Kaposi's sarcoma shown in (a).
fected (Pindborg 1980). In England a marked shift in
male/female ratio has been observed, since the ratio
was 5:1 in 1932-39, but 1:1 by 1960-69 (Easson & Pal-
mer 1976). Most gingival cancers affect the mandible
and 60% are located posterior to the premolars. In an
American study it has been shown that dentists play
an important part in the early recognition of gingival
cancer; 60% of these patients are first seen by a dentist
(Cady & Catlin 1969). Gingival cancer commonly be-
gins as a nodular lesion (Fig. 13-16a,b) often with
ulceration and surrounding leukoplakia. It infiltrates
rapidly in depth, frequently extending along the peri-
odontal membrane with osseous involvement and
destruction of the supporting bone. Pain and loosen-
ing of teeth is common. In the American study, gingi-
val cancer had exceeded 3 cm at admission in 44% of
the referred cases and regional lymph-node metasta-
sis on admission was found in 37%.
Histopathology
Squamous cell carcinoma of the gingiva does not dif-
fer histologically from squamous cell carcinomas else-
where in the oral mucosa. Islands and cords of malig-
nant epithelial cells are seen infiltrating underlying
tissues (Fig. 13-16c). Varying amounts of horn pearls
are formed and usually a strong inflammatory reac-
tion is found in the stroma.
Treatment
Gingival squamous cell carcinomas are usually
treated by surgery, irradiation or combinations of
these. When irradiation therapy is required, extraction
of involved teeth is often necessary before irradiation
is instituted if the teeth suffer from severe periodonti-
tis. This is due to an increased risk of osteoradione-
crosis after extraction of teeth situated in irradiated
bone as the result of permanently reduced vasculari-
zation (Beumer et al. 1984).
Metastasis to the gingiva
The majority of metastases to the oral region are in-
traosseous. The gingiva (including the alveolar mu-
cosa) is most often the seat of soft tissue metastasis in
the mouth. In the oral regions, soft tissue metastases
from lung cancer (Fig. 13-17) is encountered most
frequently in men, while metastases from breast can-
cer account for most soft tissue metastases in women.
About 20% of oral soft tissue metastases were mani-
fested before the primary tumor was diagnosed. Fur-
thermore, in 90% of the cases the clinical manifestation
resembled a hyperplastic or reactive lesion (Hirshberg
et al. 1993). These observations emphasize the need
for a histologic examination of all such tumors.
Histopathology
The histology resembles the tumor of origin. Most
cases are carcinomas and sarcomas rarely metastasize
to the oral region.
310 • CHAPTER 13
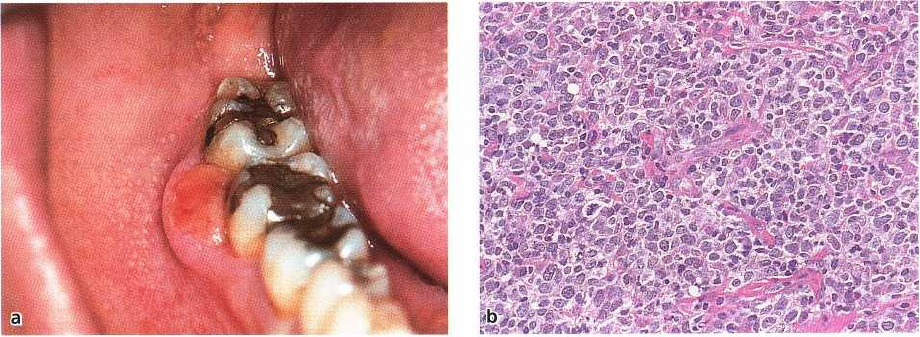
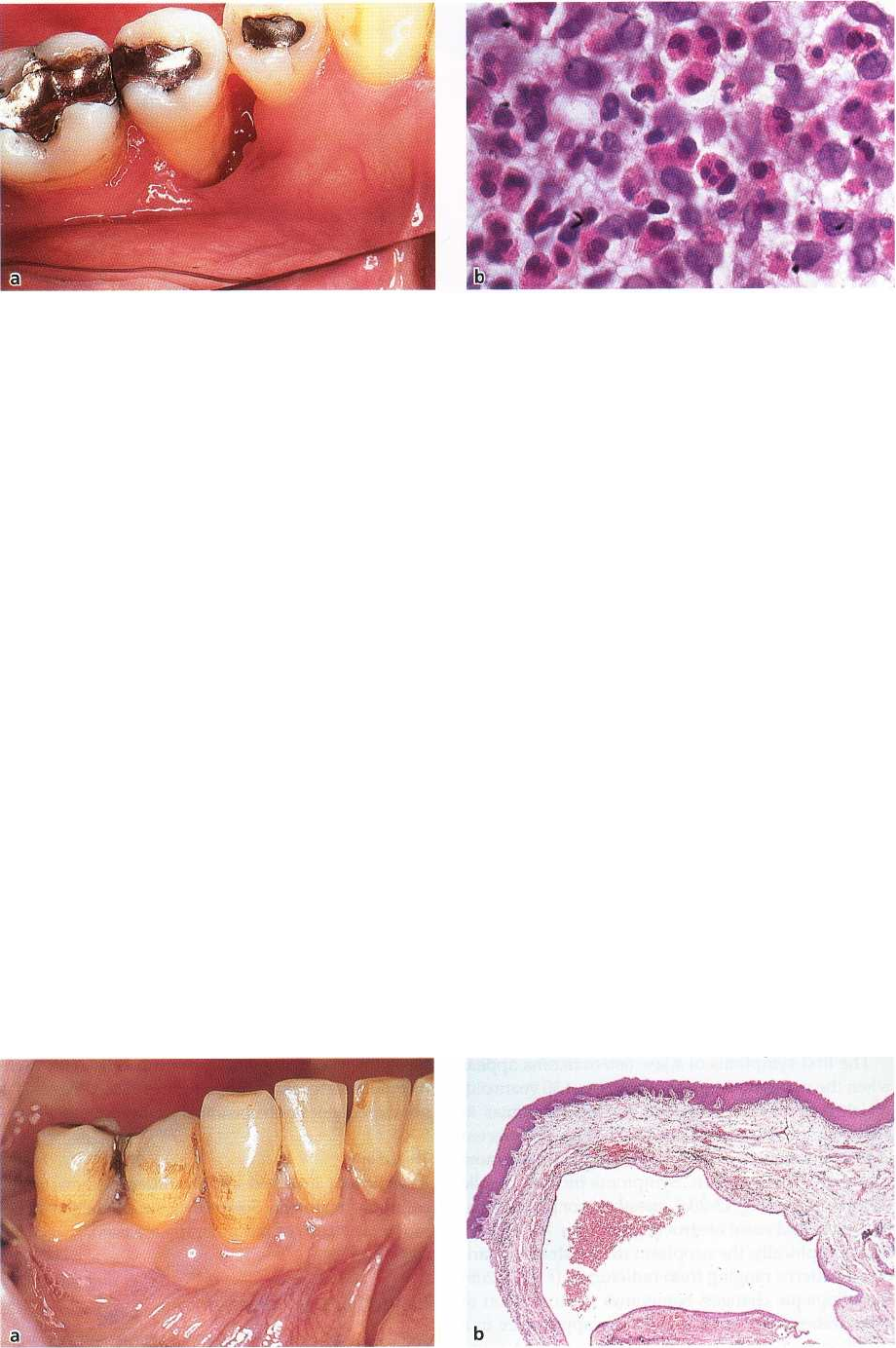
Fig. 13-19. (a) Malignant lymphoma of HIV-infected 36-year-old man. The gingival neoplasm in the right mandibu-
lar molar region resembles a pyogenic granuloma, but histopathologic examination revealed a malignant lym-
phoma shown in (b).
Kaposi's sarcoma
Clinical features
In 1872, Kaposi described what he called "multiple
idiopathic hemorrhagic sarcoma", which later came to
bear his name. Most of his patients were Jews, espe-
cially Ashkenazim. Later it was reported that Kaposi's
sarcoma occurred among people living around the
Mediterranean.
Then, in the middle of the 1950s, reports came from
Sub-Saharan Africa that Kaposi's sarcoma was a
prevalent malignant tumor in that area, but oral mani-
festations of Kaposi's sarcoma in Jews and Africans
were rare.
It was later recognized that Kaposi's sarcoma some-
times occurred in individuals who had been treated
with immunosuppressive drugs after kidney trans-
plantation.
The latest phase in the occurrence of Kaposi's sar-
coma is among individuals suffering from the ac-
quired immunodeficiency syndrome (AIDS). The ap-
pearance of a Kaposi's sarcoma is one of the criteria
for the development of AIDS in patients infected with
human immunodeficiency virus (HIV). In most in-
stances, Kaposi's sarcoma will first manifest as skin
lesions followed by oral lesions. In rare cases, oral
manifestations may be the first sign of Kaposi's sar-
coma. Gingival location is the second most frequently
observed after the palate (Pindborg & Reichart 1995).
The typical appearance is that of single or multiple
blue, violet or red slightly raised lesions. Ulceration is
common and with time the tumors can reach mon-
strous proportions (Fig. 13-18a).
Histopathology
The typical features are a lesion with bundles of spin-
dle-shaped cells and many thin-walled vascular lumi-
nae, often lined by plump endothelial cells (Fig. 13-
18b). There are usually a number of mitotic figures of
which some are atypical. There is general agreement
that the cell of origin of Kaposi's sarcoma is the endo-
thelial cell.
Treatment
There is no curative treatment but palliative treatment
includes both cytostatics and irradiation.
Malignant lymphoma
Clinical features
A primary malignant lymphoma is rare in the oral
cavity. When it occurs, it is most commonly seen in the
palate and gingiva (Takahashi et al. 1989). It presents
as a diffuse swelling which is usually ulcerated. The
diagnosis may be quite difficult to arrive at as the first
manifestations may resemble a non-specific periodon-
titis, pyogenic granuloma (Fig. 13-19a) or pericoroni-
tis (Maxymiw et al. 1991).
In HIV-infected patients non-Hodgkin's lymph-
omas occur with increased frequency (Holmstrup &
Westergaard 1994). Occasionally, a gingival tumor
may be the first manifestation of a non-Hodgkin's
lymphoma in an HIV-infected patient (Fig. 13-19a).
Histopathology
Histomorphologic features, immunologic and genetic
markers are used to diagnose and classify malignant
lymphomas. The lesions contain lymphocytic-appear-
ing cells (Fig. 13-19b); in low-grade tumors the cells
are well-differentiated small lymphocytes, whereas
high-grade tumors contain less differentiated cells.
Common to all lymphomas are infiltrative growth as
characteristically seen in all malignant tumors.
Treatment
Depending on the extension and spread of the tumor,
surgical removal, irradiation, cytostatics and combi-
nations of these may be the treatment of choice.
DIFFERENTIAL DIAGNOSES: PERIODONTAL TUMORS AND CYSTS • 311
Fig. 13-20. (a) A swelling between
the right mandibular canine and
lateral incisor was associated with
tooth mobility, displacement, and
loss of supporting periodontal
bone as seen in the radiograph (b).
The biopsy showed osteosarcoma
(c).
MALIGNANT NEOPLASMS OF
PERIODONTAL HARD TISSUES
Osteosarcoma
Clinical features
Osteosarcoma is the most common primary malig-
nant tumor of bone. About 7% of all osteosarcomas
occur in the jaws.
The first symptoms of a jaw osteosarcoma appear
when the patients are, on average, about 30 years old,
which is a decade older than for osteosarcomas in
other bones. The maxilla and mandible are affected
with about equal frequency. Men are affected more
commonly than women. Symptoms include mobile
teeth, swelling (Fig. 13-20a), anesthesia or paresthesia,
toothache and nasal obstruction (van der Waal 1991).
Radiographically, the neoplasm demonstrates a vari-
ety of patterns ranging from radiolucent (Fig. 13-20b)
to radiopaque changes. Sometimes the formation of
bony trabeculae results in a sunray appearance in a
direction perpendicular to the outer surface. A num-
ber of jaw osteosarcomas will have, as their first mani-
festation, a widening of the periodontal membrane (
Garrington et al. 1967).
Histopathology
A variety of histologic appearances can be seen (
Neville et al. 1995). Some osteosarcomas are primar-
ily osteoblastic, with production of irregular osteoid
and bone (Fig. 13-20c). In others, production of carti-
lage (chondroblastic osteosarcomas) or the presence
of fibroblastic cells (fibroblastic osteosarcomas) are the
dominant histologic features. Common to all these
types are the malignant-appearing cells with pleo-
morphic nuclei and mitotic figures. The prognosis is
not dependent on the histologic subtype.
Treatment
Resection of involved and surrounding bone is the
common treatment. Sometimes supplementary che-
motherapy and/or radiotherapy are used.
Langerhans cell disease
Clinical features
Langerhans cell disease, formerly named histiocytosis
X, is a proliferation of histiocyte-like cells that have
312 • CHAPTER 13
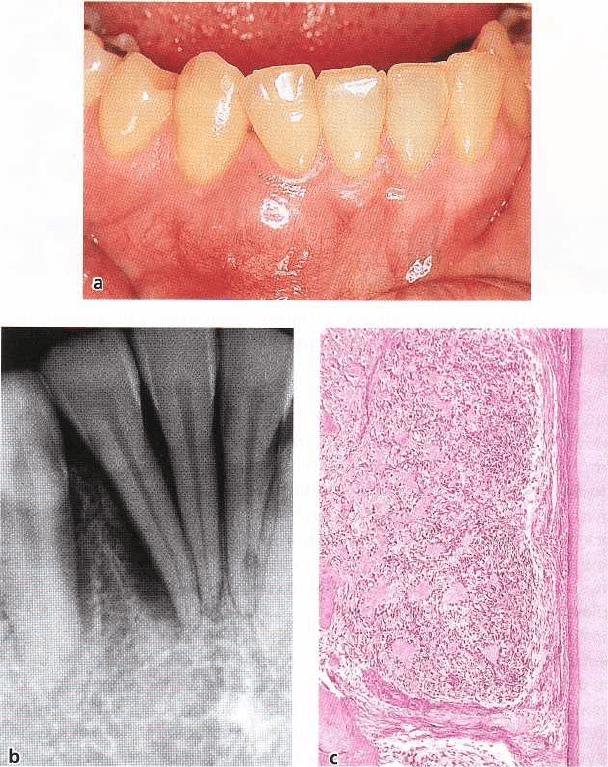
Fig. 13-21. (a) Eosinophilic granuloma of alveolar bone in the mandibular premolar region showed progressive loss
of supporting periodontal tissue in a 33-year-old woman. The lesion was biopsied and characteristic features
of Langerhans cell disease were revealed (b). Note the numerous eosinophils.
been shown in recent years to be Langerhans cells.
Langerhans cells are blood marrow-derived cells nor-
mally present in the skin, mucosa, lymph nodes and
blood marrow. The disease is difficult to classify as the
etiology and pathogenesis are unknown and due to
the fact that it is characterized by clinical heterogene-
ity and an unpredictable course. Some classify this
disease, or at least some of its manifestations, as a
malignant systemic disorder/neoplastic disease while
others classify it as a reactive, proliferative disease.
Traditionally, the disease has been divided into three
subtypes: a disease with solitary or multiple bone
lesions (eosinophilic granuloma), a chronic multi-
organ disease associated with considerable morbidity
(Hand-Schuller-Christian syndrome) and an acute
multi-organ disease occurring mainly in infants and
with a common fatal outcome (Letterer-Siwe disease).
There are overlapping clinical features between
these subtypes.
Manifestations in the jaws are seen in 10-20% of all
cases. Swelling, tenderness, pain and loosening of
teeth (Fig. 13-21a) are frequent symptoms. The jaw
lesions often appear as punched-out radiolucencies
but ill-defined radiolucencies are also seen, sometimes
mimicking periodontal disease (Neville et al. 1995,
van der Waal 1991).
Histopathology
The lesions are characterized by a diffuse infiltration
of rather large mononuclear cells representing Lang-
erhans cells with varying numbers of eosinophilic
granulocytes and other inflammatory cells (Fig. 13-
21b). Identification of Langerhans cells by electron
microscopy or immunohistochemical methods is
sometimes used to confirm the diagnosis.
Treatment
The prognosis for patients with jaw lesions in the
absence of visceral involvement is generally good.
Such lesions are usually treated surgically, sometimes
with supplementary radiotherapy. Recurrence and
progression of the disease can be seen. Chronic and
acute disease with multiorgan involvement is usually
treated with chemotherapeutic agents and the prog-
nosis is generally moderate or poor.
CYSTS OF THE PERIODONTIUM
The origin of jaw cysts is either developmental or
inflammatory and the background of the frequent
occurrence of these cysts is the abundance of epithelial
remnants residing within the jaws (Shear 1992, 1994).
Fig. 13-22. (a) Gingival cyst between right mandibular first premolar and canine. (b) Characteristic histopathologic
features of a cyst lined by a thin non-keratinized squamous epithelium.