Cui Dongmei. Atlas of Histology: with functional and clinical correlations. 1st ed
Подождите немного. Документ загружается.

CHAPTER 19
■
Female Reproductive System
375
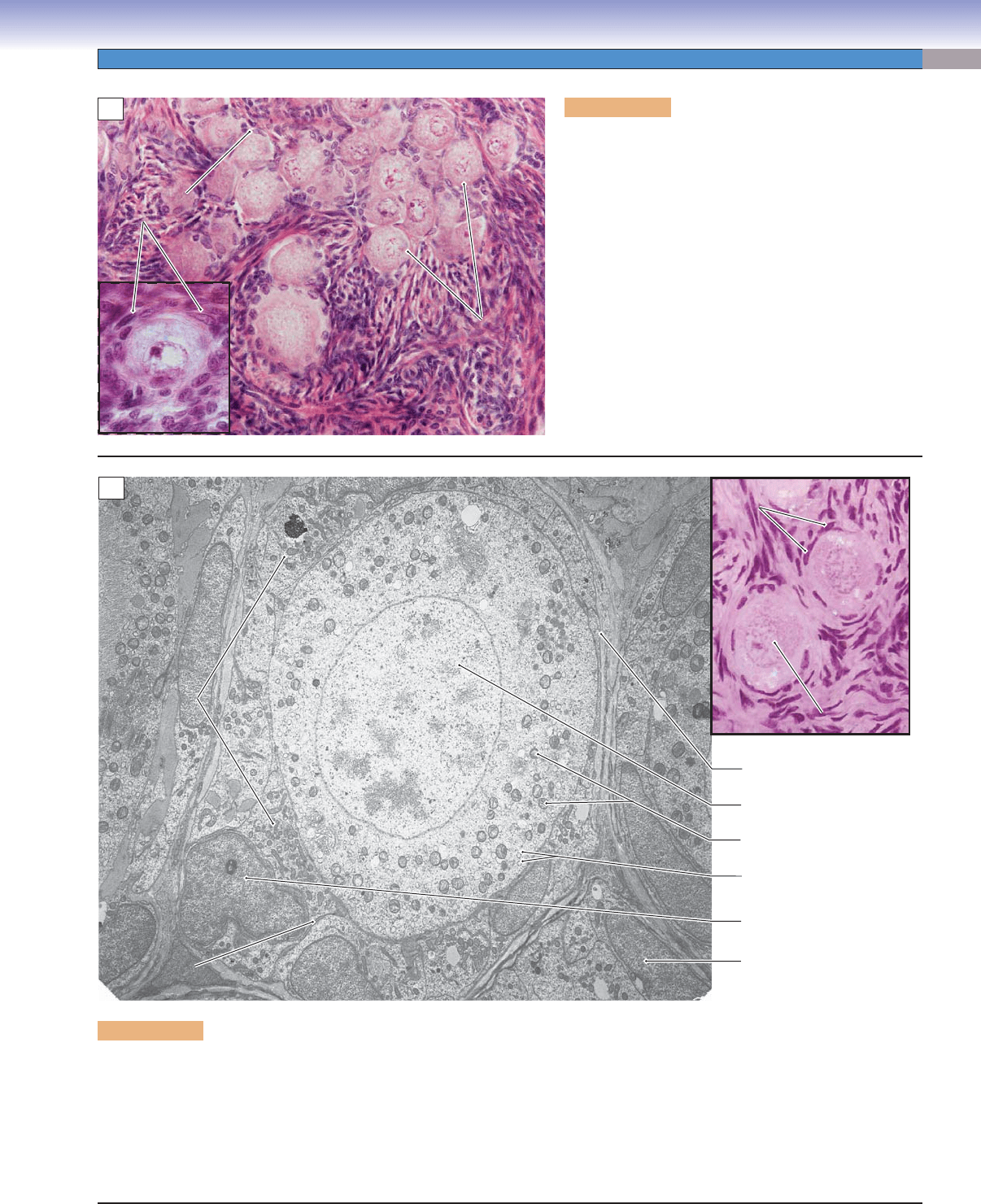
Figure 19-4A. Primordial follicles, ovary. H&E, 290;
inset 110
Primordial follicles are the smallest and most numerous
type of follicles in the cortex of the ovary. Each primordial
follicle contains a germ cell (primary oocyte) in a resting
state that may persist for as long as 50 years. The primary
oocyte is surrounded by a layer of squamous cells called
follicular cells. These follicular cells are somatic cells that
support the oocyte. The oocyte has a pale appearance
and a large nucleus with a prominent nucleolus. About
1 million follicles are present in the ovaries at the time
of birth; however, only a few hundred of these follicles
become mature. The follicles begin to grow at puberty,
and there is a constant loss of follicles throughout the
reproductive years. At menopause, only a few follicles
remain.
Squamous
Squamous
follicular cells
follicular cells
Squamous
follicular cells
Primordial
Primordial
follicles
follicles
Primordial
Primordial
follicle
follicle
Primordial
follicles
Primordial
follicle
A
Follicular
Follicular
cells
cells
Follicular
cells
Basal lamina of follicle
Nucleus of primary oocyteNucleus of primary oocyte
Nucleus of
Nucleus of
primary oocyte
primary oocyte
Nucleus of
primary oocyte
Mitochondria of primary oocyte
Mitochondria of
Mitochondria of
follicle cells
follicle cells
Mitochondria of
follicle cells
Granules in oocyte
Nucleus of follicular cell
Nucleus of stromal cell
Junction between
Junction between
follicular cells
follicular cells
Junction between
follicular cells
B
Figure 19-4B. Primordial follicle. EM, 3,900; inset (color) H&E, 500
The primary oocyte at the center of this primordial follicle may appear to be in interphase of the cell cycle, but it is arrested in dictyo-
tene of prophase I of meiosis. What appear to be patches of heterochromatin in the nucleus are partially decondensed tetrads com-
posed of paired homologous chromosomes. The oocyte has been in prophase of meiosis I before birth of the individual. Follicular
cells form a simple squamous epithelium that surrounds the oocyte. Note that these cells adhere tightly to the surface of the oocyte.
Indeed, there are junctions between the oocyte and the follicle cells, although they are not readily identifi able here. Neighboring fol-
licular cells are also connected by junctional complexes, and there is a basal lamina between the follicular cells and the surrounding
interstitial tissue of the ovarian cortex.
CUI_Chap19.indd 375 6/19/2010 12:20:17 PM
376
UNIT 3
■
Organ Systems
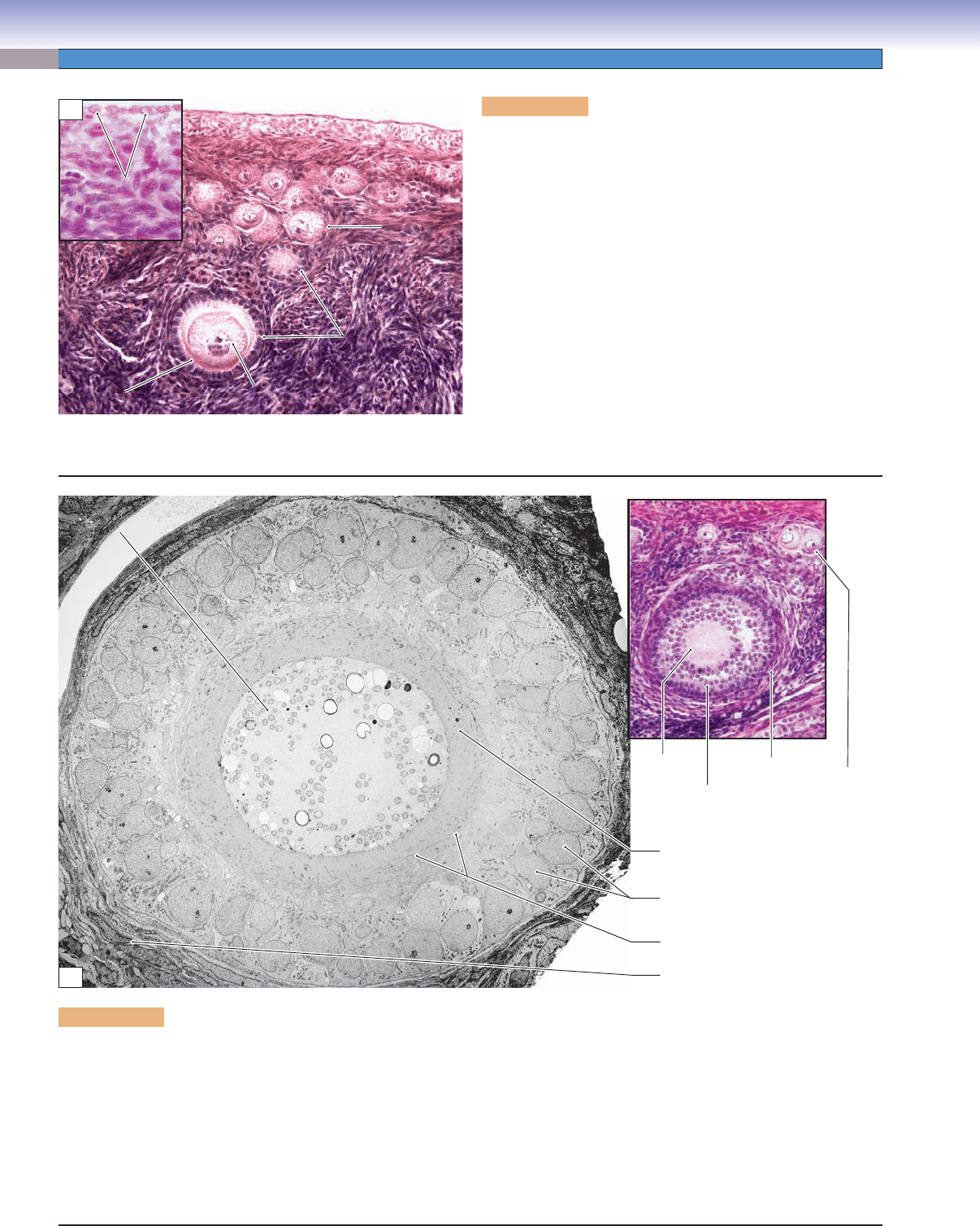
Figure 19-5A. Primary follicles, ovary. H&E, 202; inset
438
Primary follicles develop from primordial follicles. Each primary
follicle consists of a primary oocyte and cuboidal follicle cells.
These follicle cells increase in height (from squamous cells to
cuboidal cells), and their cellular layers gradually increase as the
follicle continues to grow. At this stage, follicle cells are called
granulosa cells, because their cytoplasm begins to have a granu-
lar appearance. The primary follicles can be classifi ed into unil-
aminar primary follicles and multilaminar primary follicles. The
unilaminar primary follicle has a single layer of cuboidal granu-
losa cells with a smaller oocyte. The multilaminar primary fol-
licle has several layers of cuboidal granulosa cells surrounding a
relatively large oocyte. As the oocyte increases its size, the zona
pellucida emerges as an amorphous layer between the surface
of the oocytes and the surrounding granulosa cells (Fig. 19-5B).
Situated outside of the basement membrane of the granulosa
cells are stromal cells that fl atten and develop into a sheath that
surrounds the follicle; this layer is called the theca folliculi.
Cuboidal follicle cells
Cuboidal follicle cells
of primary
of primary
(unilaminar) follicle
(unilaminar) follicle
Cuboidal follicle cells
of primary
(unilaminar) follicle
Primordial
Primordial
follicle
follicle
Primordial
follicle
Germinal
Germinal
epithelium
epithelium
Germinal
epithelium
Zona
Zona
pellucida
pellucida
Zona
pellucida
Oocyte
Oocyte
Oocyte
A
Primary
oocyte
Granulosa
cells
Theca
folliculi
Primordial
follicle
Zona pellucida
Granulosa cells
Microvilli
Theca folliculi
Cytoplasm of oocyte
Cytoplasm of oocyte
Cytoplasm of oocyte
B
Figure 19-5B. Growing (primary) follicle. EM, 3,200; inset (color) H&E, 152
The oocyte in the center of this growing follicle has been sectioned off center so that the nucleus is not shown. Although the oocyte has
begun to grow, it is still arrested in prophase of meiosis I. Note the membrane-bound vesicles in the cytoplasm of the oocyte; these will
participate in the cortical granule reaction if the oocyte becomes fertilized. The follicle cells that surrounded the oocyte have prolifer-
ated and transformed into granulosa cells. At this stage, the granulosa comprises about two layers of cuboidal cells. The inner granu-
losa cells no longer have smooth close contact with the surface of the oocyte because a layer of amorphous extracellular material, the
zona pellucida, has developed. As the granulosa cells continue to proliferate, several layers of cells will accumulate, and ultimately,
a fl uid-fi lled space, the antrum, will develop. Changes are also underway in the stroma adjacent to the growing follicle. The stromal
cells (fi broblasts) have become concentrated and fl attened against the basal lamina of the granulosa. These theca folliculi cells will
develop properties of steroid hormone–synthesizing cells if development of the follicle continues.
CUI_Chap19.indd 376 6/19/2010 12:20:22 PM
CHAPTER 19
■
Female Reproductive System
377
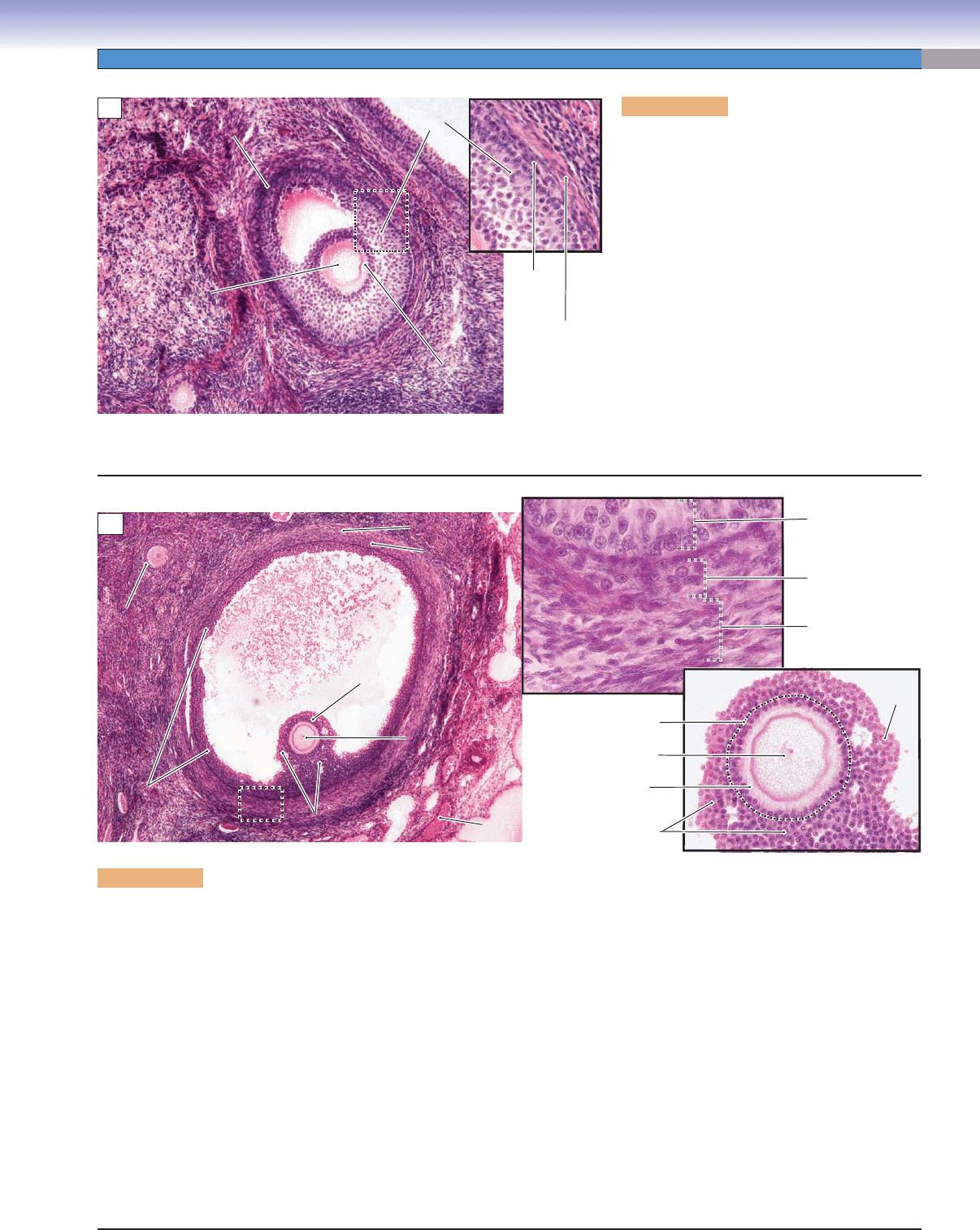
Figure 19-6A. Secondary follicles, ovary. H&E,
108; inset 211
The secondary follicle develops from the continued
growth of the multilaminar primary follicle.
Spaces fi lled with follicular fl uid (liquor folliculi)
appear among the granulosa cells within the sec-
ondary follicle. These spaces gradually merge to
form a single large space called the antrum. The
zona pellucida is distinct, and the theca folliculi
(surrounding the follicle) develops into the theca
interna and theca externa. The theca interna
is the inner vascular layer containing cuboidal
(steroid-producing) secretory cells. These cells
secrete androgens, which diffuse into the granu-
losa cells where they are converted into estrogens
in response to FSH. The theca externa is an outer
connective tissue layer containing mainly colla-
gen and some small squamous cells mixed with a
few smooth muscle cells.
Primary
Primary
oocyte
oocyte
Primary
oocyte
Secondary
Secondary
follicle
follicle
Secondary
follicle
Antrum
Antrum
Antrum
Granulosa
Granulosa
cells
cells
Granulosa
cells
Zona
Zona
pellucida
pellucida
Zona
pellucida
Theca
Theca
interna
interna
Theca
interna
Theca
Theca
externa
externa
Theca
externa
A
Granulosa cells
Theca interna
Theca externa
Cumulus
oophorus
Corona radiata
Nucleus of oocyte
Zona pellucida
Blood
Blood
vessel
vessel
Blood
vessel
Cumulus oophorus
Antrum
Antrum
Antrum
Primary
Primary
follicle
follicle
Primary
follicle
Membrana granulosa
Membrana granulosa
(g
(g
ranulosa cells)
ranulosa cells)
Membrana granulosa
(granulosa cells)
Corona
Corona
radiata
radiata
Corona
radiata
Oocyte
Oocyte
Oocyte
Cumulus
Cumulus
oophorus
oophorus
Cumulus
oophorus
Theca interna
Theca interna
Theca interna
Theca externa
Theca externa
Theca externa
B
Figure 19-6B. Graafi an follicles, ovary. H&E, 54; inset (upper) 429; inset (lower) 178
The Graafi an follicle is a mature follicle; it is also called a preovulatory follicle. At this stage, the follicle has grown to a large size
(about 25 mm) and bulges from the surface of the ovary. The decreased number of granulosa cells and increased volume of fl uid in
the antrum result in the oocyte being located at the periphery of the follicle. The membrana granulosa is formed by multiple cellular
layers of granulosa cells lining the inner wall of the antrum. Some granulosa cells form a hillock called the cumulus oophorus, which
supports and houses the oocyte. The inner granulosa cells of the cumulus oophorus form a single layer called the corona radiata,
which immediately surrounds the oocyte. As the follicle grows, most of the granulosa cells gradually loosen from the cumulus
oophorus, but the corona radiata remains in contact with the oocyte. Eventually, the oocyte, with the corona radiata, fl oats freely in
the antrum before ovulation. The oocyte remains as a primary oocyte in the graafi an follicle until pituitary secretion of LH increases
sharply (LH surge); this stimulates the primary oocyte to complete the fi rst meiotic division and become a secondary oocyte. The
secondary oocyte with the corona radiata and polar body (from the fi rst oocyte division) are released from the graafi an follicle of the
ovary. After the secondary oocyte reaches the ampulla of the oviduct, the second meiotic division occurs, if fertilization takes place.
A spermatozoan must penetrate the corona radiata and zona pellucida to complete the fertilization process. The upper inset shows
the theca folliculi (theca interna and theca externa). The lower inset shows the oocyte surrounded by granulosa cells.
The ovarian cycle is under the control of the hormones FSH and LH produced by the gonadotrophs of the anterior pituitary
gland. FSH stimulates estrogen production and follicular growth; LH stimulates meiotic division of the primary oocyte, ovulation,
and development of the corpus luteum. The estrogens play an important role in the stimulation of follicle growth by promoting
proliferation of the granulosa cells, and they also stimulate the mammary glands to prepare for lactation.
CUI_Chap19.indd 377 6/19/2010 12:20:25 PM
378
UNIT 3
■
Organ Systems
Ovulated
secondary oocyte
Corpus
albicans
Corpus luteum
Theca
Theca
lutein cells
lutein cells
Theca
lutein cells
Theca
Theca
lutein cells
lutein cells
Theca
lutein cells
Granulosa
Granulosa
lutein cells
lutein cells
Granulosa
lutein cells
Nuclei of granulosa
Nuclei of granulosa
lutein cells
lutein cells
Nuclei of granulosa
lutein cells
Cytoplasm of
Cytoplasm of
granulosa lutein cells
granulosa lutein cells
Cytoplasm of
granulosa lutein cells
Blood
Blood
vessels
vessels
Blood
vessels
Connective
Connective
tissue
tissue
Connective
tissue
A
Blood
Blood
vessels
vessels
Blood
vessels
Corpus albicans
Corpus albicans
Corpus albicans
Corpus albicans
Corpus albicans
Corpus albicans
B
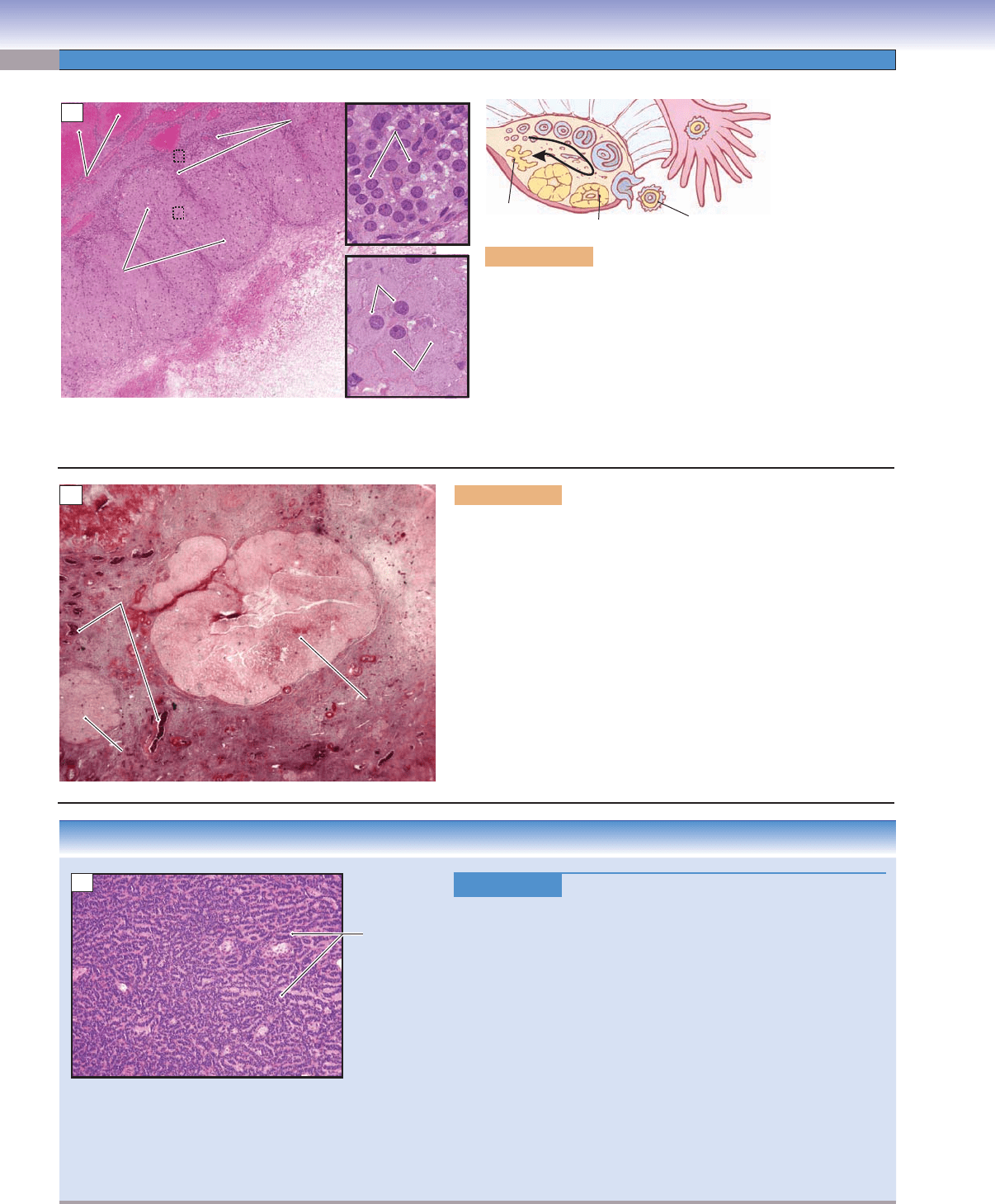
Figure 19-7A. Corpus luteum, ovary. H&E, 36; insets 363
After ovulation, the remaining portion (wall) of the graafi an
follicle transforms into the corpus luteum (yellow body). The wall
of the corpus luteum is folded and contains granulosa lutein cells
(derived from granulosa cells) and theca lutein cells (from the theca
interna). The granulosa lutein cells are large and have pale cyto-
plasm; these cells have features of steroid hormone–producing cells,
and they produce primarily progesterone. The theca lutein cells are
smaller but also have features of steroid hormone–secreting cells;
these cells secrete primarily progesterone and androgens.
Figure 19-7B. Corpus albicans, ovary. H&E, 34
In the absence of fertilization, the corpus luteum is active only for a
short period of time (10–14 days). The corpus luteum degenerates,
decreases in size, and forms a structure called the corpus albicans.
The corpus albicans consists of dense connective tissue that appears
as a white scar; it gradually decreases in size and remains in the ovary
for months to years. However, if fertilization and implantation occur,
the corpus luteum is rescued from degeneration by human chorionic
gonadotropin (hCG) hormone from the placenta. During pregnancy,
the corpus luteum will remain active for the fi rst 6 months of gesta-
tion, after which it degenerates, and the corpus albicans is formed.
Formation of the corpus luteum is stimulated by the LH surge.
CLINICAL CORRELATION
Figure 19-7C.
Granulosa Cell Tumor. H&E, 52
Granulosa cell tumor of the ovary is a neoplasm composed of ovar
-
ian granulosa and, occasionally, theca cells. Granulosa cell tumors
may arise at any age and are divided into juvenile and adult types.
These tumors may produce excess estrogen, the result of which
may cause precocious puberty, endometrial hyperplasia, and endo-
metrial cancer. Symptoms may include abdominal pain, hemoperi-
toneum with hypotension, and mimicking an ectopic pregnancy in
younger patients because of rupture of the tumor. Histologically,
the tumor cells are small and cuboidal, and may be arranged in a
variety of patterns including solid, trabecular, and cordlike. The
tumor cells often contain a groove resembling a coffee bean. Small
follicle-like structures named Call-Exner bodies may be visible in
well-differentiated tumors. The behavior of granulosa cell tumors
is variable and may take an aggressive course in some patients.
A total abdominal hysterectomy and bilateral salpingo-oophorec-
tomy are the treatments of choice in the early stage.
Granulosa cell
tumor with
neoplastic
cells arranged
in cords
C
CUI_Chap19.indd 378 6/19/2010 12:20:30 PM
CHAPTER 19
■
Female Reproductive System
379
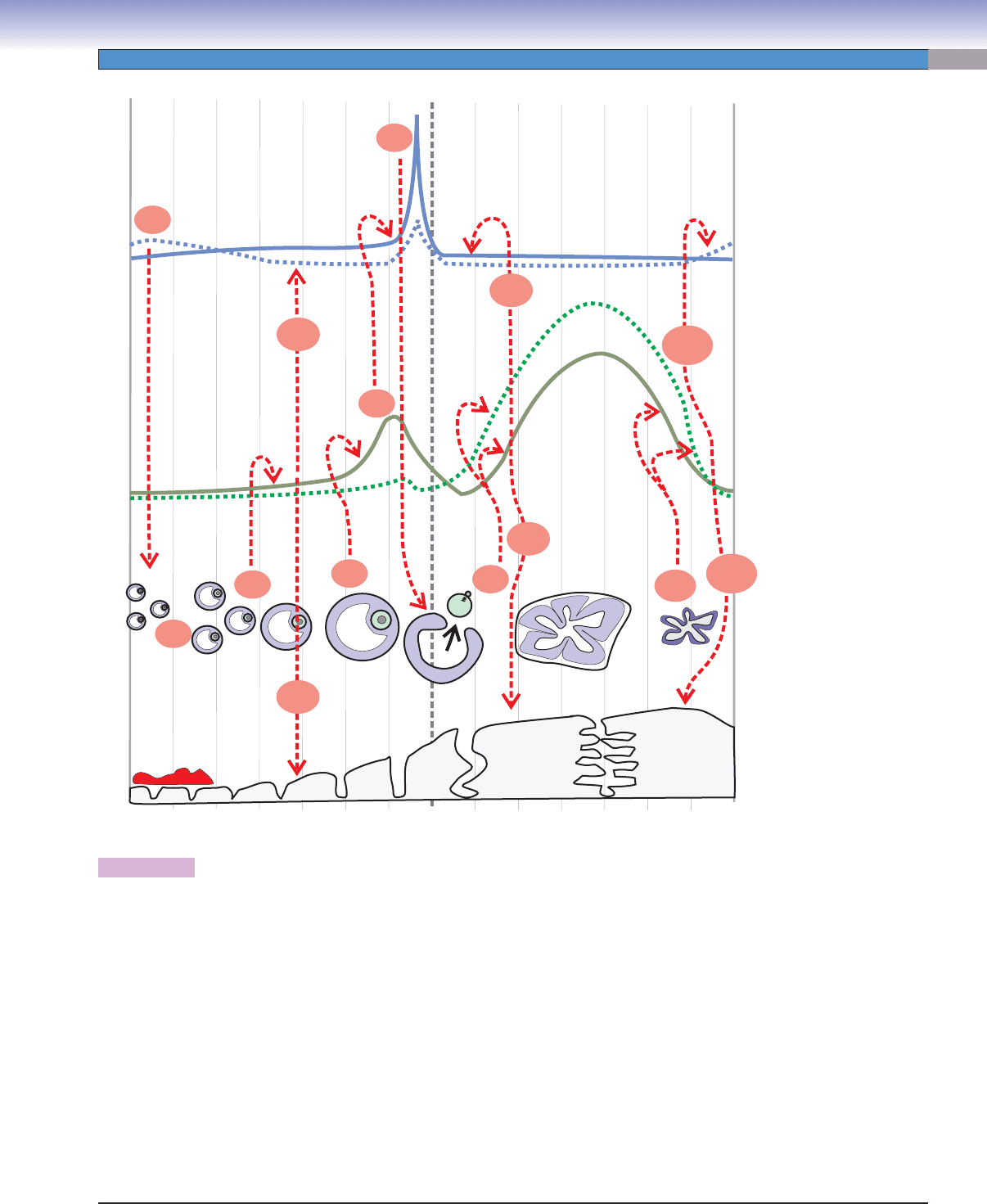
Figure 19-8. Events of the female reproductive cycle.
The following sequence of events refer to the numbered events labeled in red in the diagram above. (1) At the beginning of the female
reproductive cycle, there are rising levels of gonadotropic hormones from the anterior pituitary, most importantly FSH. (2) This rise
promotes ovarian recruitment of a cohort of antral follicles to proceed into advanced development and then selection of typically a
single dominant follicle at about day 6. (3) These follicles secrete steroid hormones, most prominently estrogens, that (4a) promote
rebuilding of the endometrium (proliferative phase) and (4b) exert a negative feedback on FSH secretion by pituitary gonadotropes.
(5) In the latter part of the follicular phase, the dominant follicle secretes increasing amounts of estrogens (and, to a lesser extent,
progesterone). (6) When circulating estrogen reaches a threshold level (about 200 pg/mL) for a duration of about 36 hours, pituitary
gonadotropes are stimulated to sharply increase secretion of gonadotropic hormones––most importantly, LH. (7) This LH surge
from the pituitary brings about fi nal maturation of the dominant follicle culminating in ovulation (about 40 hours after initiation
of the LH surge) and formation of the corpus luteum from the remaining components of the follicle. (8) The corpus luteum secretes
progesterone as well as estrogens. (9a) This induces a change in the endometrium from the proliferative phase to the secretory phase.
(9b) Meanwhile, gonadotropin secretion is greatly reduced, probably because of negative feedback effects of the high progesterone
and estrogen levels coming from the corpus luteum. (10) Without LH support, the corpus luteum fails after about 10 days, and ste-
roid hormone levels fall. (11a) This loss of steroid hormone support results in degenerative changes in the endometrium culminating
in menstruation. (11b) The fall in progesterone also releases the pituitary gonadotropes from negative feedback with the result that
FSH secretion starts to rise toward the end of the cycle, and this starts another round of follicle recruitment.
J. Naftel
Day of nominal female reproductive cycle
0
71421
28
Progesterone
Progesterone
Progesterone
Estradiol
Estradiol
Estradiol
LH
LH
LH
FSH
FSH
FSH
Pituitary
gonadotroph
hormones
Ovarian
steroid
hormones
Ovary
Endometrium
Endometrium
Hormone concentration in plasma
(1)
(2)
(3)
(4a)
(4b)
(9b)
(9a)
(5)
(6)
(7)
(8)
(10)
(11a)
(11b)
CUI_Chap19.indd 379 6/19/2010 12:20:34 PM
380
UNIT 3
■
Organ Systems
Oviducts (Fallopian Tubes)
Lumen
Lumen
Lumen
Mucosa
Mucosa
Mucosa
Muscularis
Muscularis
Muscularis
Serosa
Serosa
Serosa
Peg cells
Peg cells
Peg cells
Lamina propria
Lamina propria
Lamina propria
Cilia
Cilia
Cilia
Ciliated cells
Ciliated cells
Ciliated cells
A
Cilia
Microvilli
Basal bodies
Nucleus of
ciliated cell
Basal lamina
B
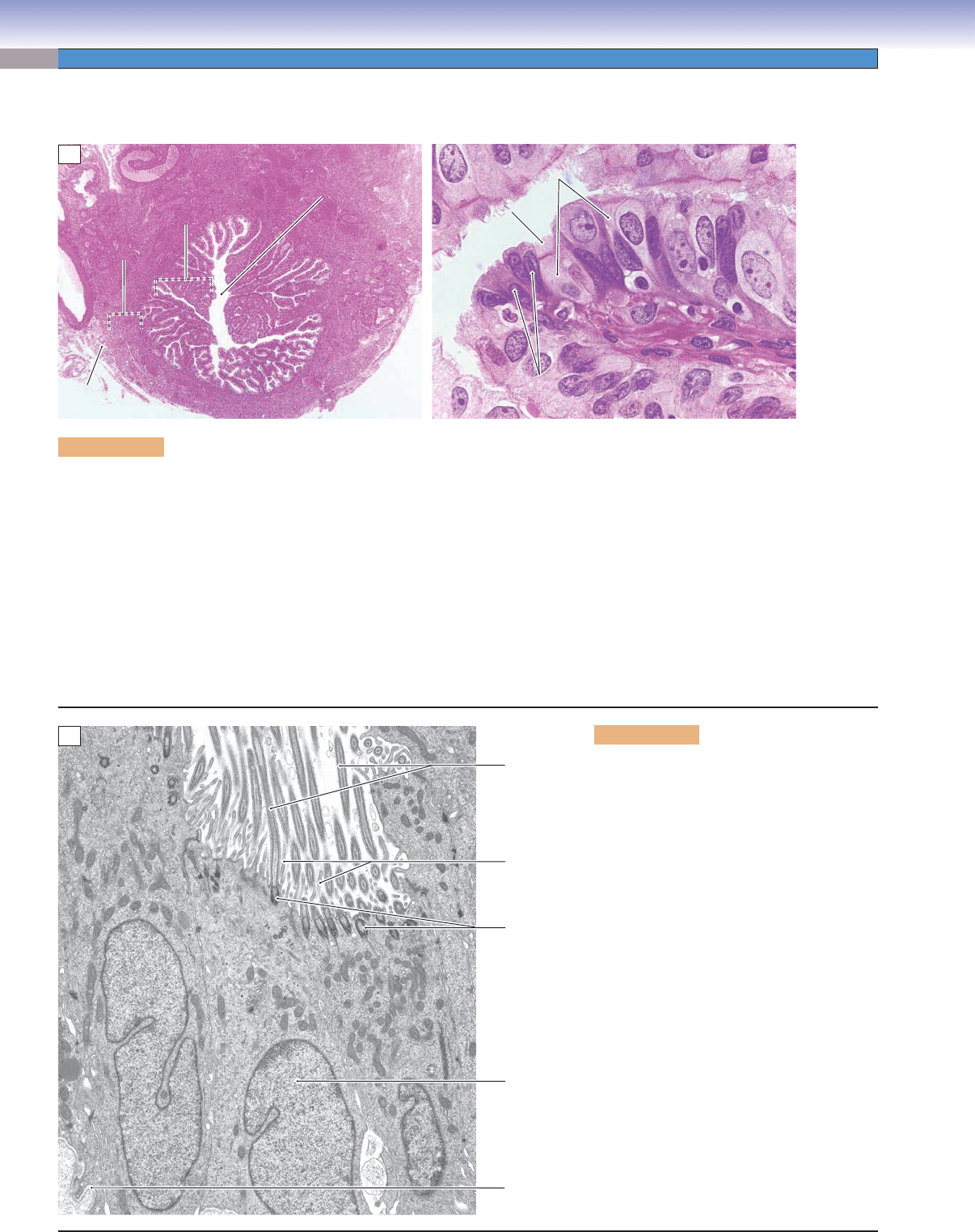
Figure 19-9A. Oviduct (fallopian tube). H&E, left 17; right 680
The oviduct (fallopian tube) can be divided into four regions: the infundibulum, ampulla, isthmus, and intramural portion (Fig. 19-1).
The infundibulum is a funnel-shaped opening that has a fringe of tentacle-like extensions called fi mbriae. The ampulla has a rela-
tively large, labyrinthine lumen where fertilization usually takes place. The isthmus is a narrow portion of the oviduct, close to the
uterus. The intramural portion is the terminal segment and is located within the uterine wall. The wall of the oviduct consists of a
mucosa (simple columnar epithelium and lamina propria), muscularis (inner circular and outer longitudinal smooth muscle), and
serosa. The epithelium of the oviduct contains ciliated cells and peg cells. The cells vary in height according to hormonal stimula-
tion. The oviduct provides an ideal environment for the fertilization of the oocyte and initial development of the embryo as well
as transportation of the zygote (fertilized oocyte) to the uterus. On the left is a low-magnifi cation view of the ampulla; on the right
is a higher magnifi cation view of the mucosa. Ciliated cells help sweep the oocyte toward the uterus. Each ciliated cell has a pale
appearance with many cilia on its apical surface. These cells have a large nucleus and a fair amount of cytoplasm. Peg cells are
secretory cells that produce nutrient-rich secretions to nourish and protect the oocyte and promote fertilization. They are small
in size and interspersed among the ciliated cells.
Figure 19-9B. Epithelial cells lining the
oviduct. EM, 8,900
The simple columnar epithelium that lines
the oviduct is composed of two cell types
(ciliated cells and peg cells); only ciliated cells
are shown here. These ciliated cells func-
tion, along with smooth muscle of the mus-
cularis, in mixing the contents (gametes) of
the lumen and in transporting the oocyte and
zygote at a precisely controlled rate along the
length of the lumen of the oviduct. The num-
ber and activity of cilia change in response
to changes in the levels of steroid hormones
throughout the reproductive cycle, reaching
a peak at the time of ovulation when estro-
gens dominate. Note that these cells also bear
numerous microvilli, suggesting an additional
absorptive function.
CUI_Chap19.indd 380 6/19/2010 12:20:35 PM
CHAPTER 19
■
Female Reproductive System
381
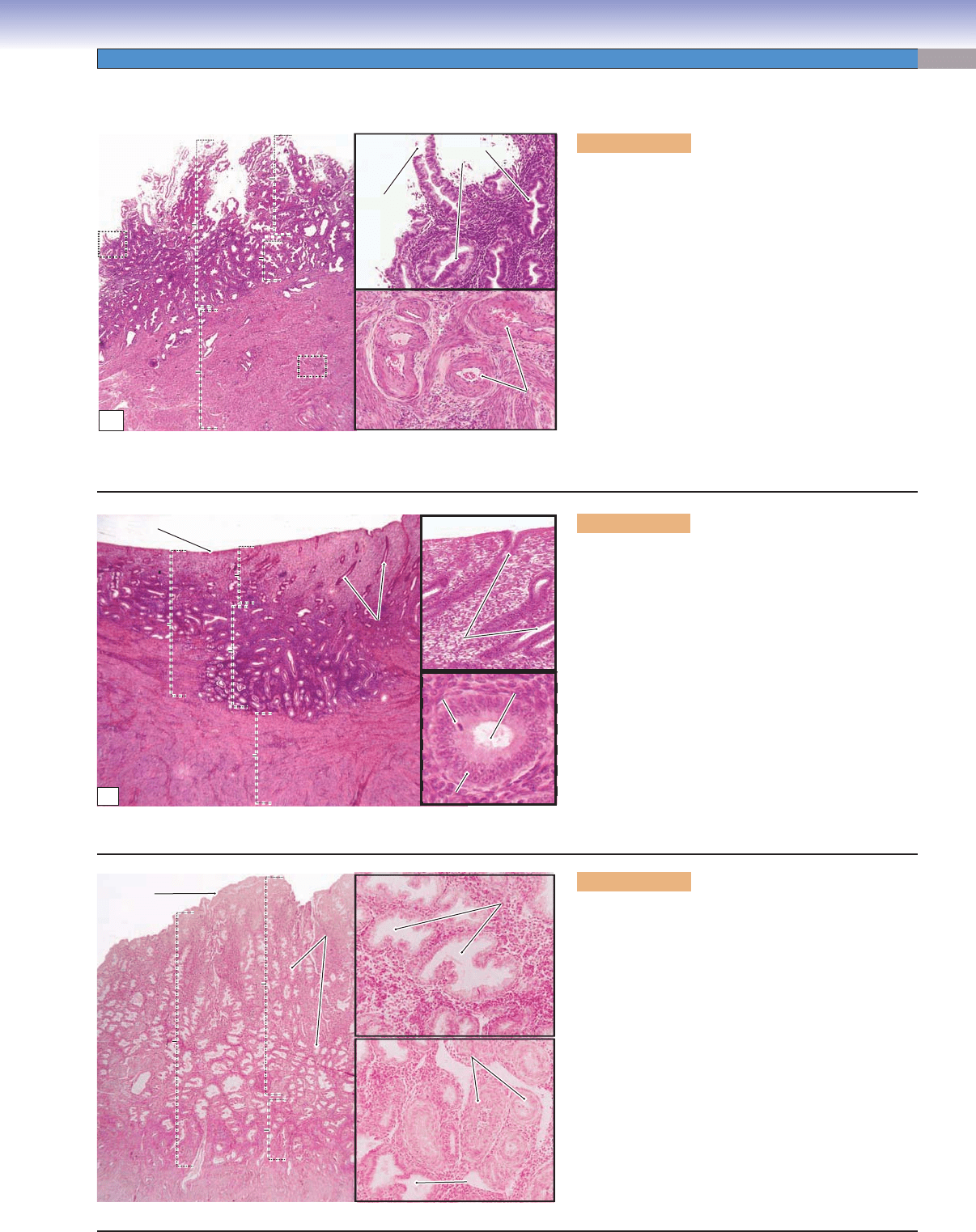
Figure 19-10A. Menstrual phase of the endome-
trium, uterus (days 1–4 of the cycle). H&E, 13;
insets 93
The wall of the uterus includes the endometrium, the
myometrium, and serosa. The endometrium, the mucosa
of the uterus, is composed of a surface epithelium and
simple tubular uterine glands within a stroma of con-
nective tissue. The endometrium consists of the basalis
(basal layer) and the functionalis (functional layer). The
functionalis is near the lumen and undergoes changes
during the menstrual cycle. During the menstrual phase,
the functionalis sloughs off as a result of ischemia and
necrosis caused by contraction of the coiled arteries.
This occurs when fertilization does not take place and
the corpus luteum atrophies, causing the levels of estro-
gen and progesterone to fall. The menstrual phase is the
initial stage of the menstrual cycle; the endometrium
will begin to recover at the end of the menstrual phase.
Endometrium
Endometrium
Endometrium
Myometrium
Myometrium
Myometrium
Functionalis
Functionalis
Functionalis
Basalis
Basalis
Basalis
Sloughed
Sloughed
gland
gland
Sloughed
gland
Uterine
Uterine
glands
glands
Uterine
glands
Myometrium
Myometrium
Myometrium
Arteries in the
Arteries in the
myometrium
myometrium
Arteries in the
myometrium
A
Endometrium
Endometrium
Endometrium
Luminal surface
Basalis
Basalis
Basalis
Straight
Straight
uterine glands
uterine glands
Straight
uterine glands
Straight
Straight
uterine glands
uterine glands
Straight
uterine glands
Mitotic
Mitotic
figures
figures
Mitotic
figures
Lumen of
Lumen of
gland
gland
Lumen of
gland
Glandular epithelium
Glandular epithelium
Glandular epithelium
Myometrium
Myometrium
Myometrium
B
Luminal
Luminal
surface
surface
Luminal
surface
Endometrium
Endometrium
Endometrium
Myometrium
Myometrium
Myometrium
Basalis
Basalis
Basalis
Functionalis
Functionalis
Functionalis
Uterine
Uterine
glands
glands
Uterine
glands
Lumen of
Lumen of
uterine glands
uterine glands
Lumen of
uterine glands
Coiled arteries
Coiled arteries
Coiled arteries
Stroma
Stroma
Stroma
Lumen of
Lumen of
uterine gland
uterine gland
Lumen of
uterine gland
C
Uterus
Figure 19-10B. Proliferative phase of the endome-
trium, uterus (days 5–14 of the cycle). H&E, 18;
inset (upper) 68; inset (lower) 293
The proliferative phase follows the menstrual phase.
The epithelium, uterine glands, and connective tissue
of the functionalis are rebuilt by proliferation and dif-
ferentiation of cells that remained in the basalis. At this
stage, the uterine glands are straight and have narrow
lumens as shown here; the surface of the endometrium
is smooth. The epithelial lining of the uterine glands
commonly appears as pseudostratifi ed columnar
epithelium because of proliferation of the lining cells.
Mitotic fi gures are occasionally seen (inset). The glands
open onto the luminal surface of the uterus. During the
proliferative phase, the changes in the endometrium are
driven by estrogens that are produced by the granulosa
cells of the developing follicles.
Figure 19-10C. Secretory phase of the endome-
trium, uterus (days 15–28 of the cycle). H&E, 14;
insets 89
The secretory phase begins shortly after ovulation occurs.
It is infl uenced by progesterone produced by the corpus
luteum. At this stage, the endometrium becomes thick-
est (6–7 mm), and the uterine glands are coiled and have
large sacculated lumens. The upper inset shows tortuous
glands with large, irregular, sawtooth-shaped lumens.
The lower inset shows coiled arteries found in the endo-
metrial stroma. These coiled arteries are also called spiral
arteries and extend transiently from the basalis into the
functionalis of the endometrium. The coiled arteries arise
from arcuate arteries of the myometrium. During the
secretory phase, these spiral arteries become elongated
and highly coiled and extend into the functionalis of
the endometrium. The arcuate arteries also give rise to
straight arteries that permanently supply the basalis.
CUI_Chap19.indd 381 6/19/2010 12:20:37 PM
382
UNIT 3
■
Organ Systems
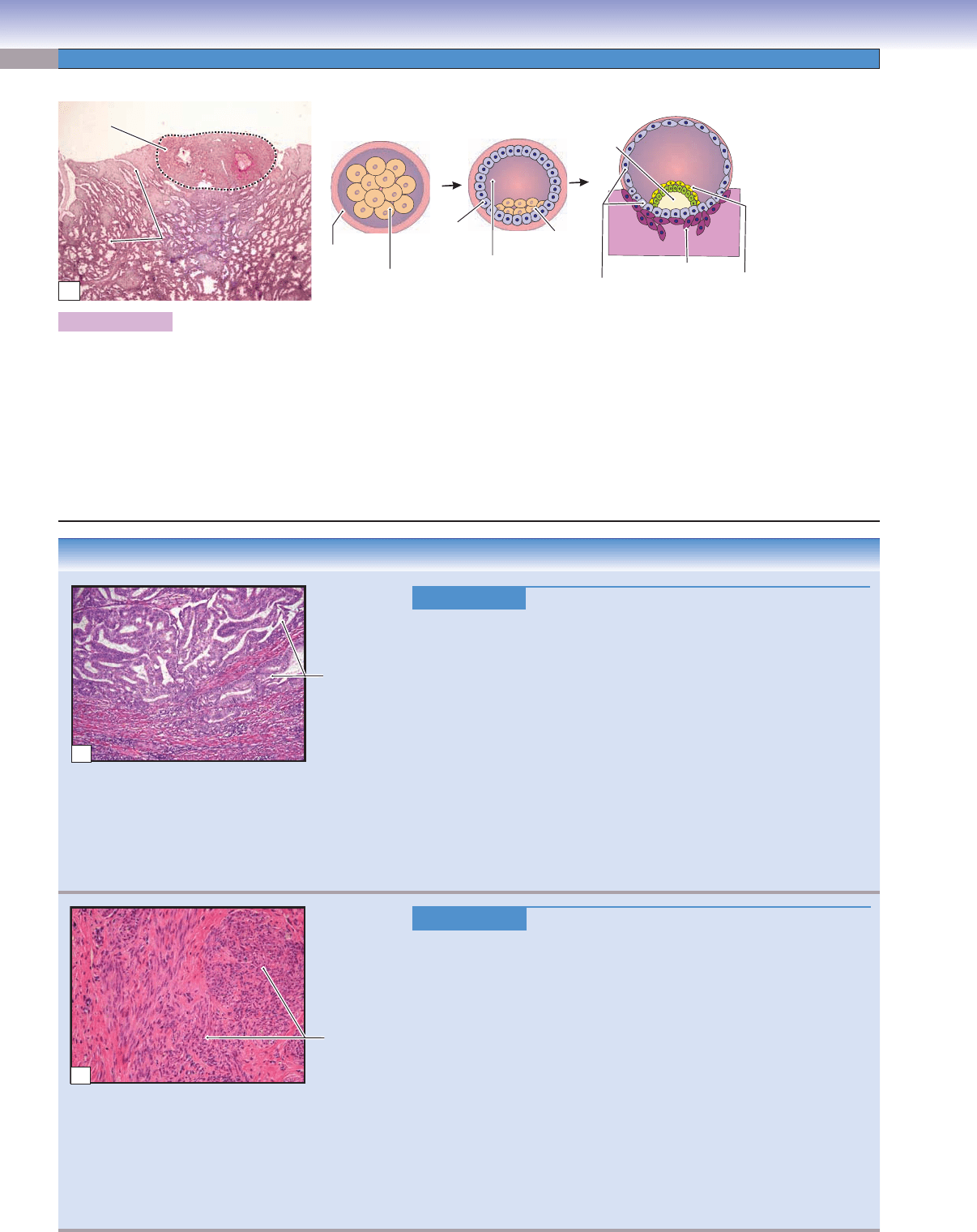
D.Cui
Morula
Zona
pellucida
Blastomeres
(subdivided zygote)
Trophoblast
Cytotrophoblast
Blastocyst
cavity
(blastocoel)
Inner cell
mass
(embryoblast)
Syncytiotrophoblast
Bilaminal
embryonic disc
Blastocyst
Implantation
Blastocyst
cavity
Amniotic
cavity
Implantation
site
Uterine
Uterine
glands
glands
Uterine
glands
Endometrium
A
Figure 19-11A. Implantation, endometrium of the uterus. H&E, 8
After an ovum has been successfully fertilized by a spermatozoan in the ampulla of the oviduct, the zygote (fertilized oocyte)
undergoes mitotic cell division (cleavage) and becomes a multicellular structure called the morula. The morula develops into the
blastocyst, which is transported into the uterus. The process of the blastocyst attaching to the endometrium of the uterus is called
implantation. Implantation occurs at the end of the secretory phase; the endometrium during this period of time is also called the
premenstrual endometrium (days 25–28). Implantation usually occurs on the posterior wall of the body of the uterus. If implanta-
tion succeeds, the trophoblast differentiates into two cell layers: an inner cytotrophoblast layer and an outer syncytiotrophoblast
layer. The syncytiotrophoblast attaches to and invades the endometrium of the uterus, and the process of placentation begins. hCG
secreted by the placenta stimulates the corpus luteum to remain active and continue to secrete estrogen and progesterone during the
pregnancy. The photomicrograph on the left shows an implantation site enclosed within the connective tissue of the endometrium.
CLINICAL CORRELATIONS
Figure 19-11B.
Endometrial Adenocarcinoma. H&E, 48
Endometrial adenocarcinoma is the most common form of endometrial
cancer, accounting for approximately 80% of cases. The majority of cases
of endometrial adenocarcinoma arise in the setting of elevated levels of
estrogen unopposed by the action of progesterone, causing endometrial
hyperplasia. Some cases, however, arise in postmenopausal women with
atrophy of the endometrium. Excess or unopposed estrogen may be due to
chronic anovulation, obesity, ovarian granulosa cell tumors, or exogenous
hormone intake. In the early stage, the cancer is usually asymptomatic.
Common symptoms include vaginal bleeding, menorrhagia, metrorrhagia,
and lower abdominal pain. Histologically, the cancer is characterized by
the presence of cells resembling the glandular cells of the endometrium,
and range from well differentiated with gland formation to poorly differ-
entiated with solid sheets of neoplastic cells. Endometrial biopsy is widely
used in the diagnosis of the cancer. Treatment options include surgical
removal of the uterus, radiation therapy, and chemotherapy.
Figure 19-11C.
Uterine Leiomyoma. H&E, 95
Uterine leiomyoma, or fi broid, is a benign neoplasm, derived from smooth
muscle cells of the uterine myometrium. Leiomyomas represent the most
common benign neoplasm in women, and occur more frequently in African
Americans. Leiomyomas occur in the reproductive years when estrogen levels
are high, and tend to regress during menopause. Most patients with fi broids
are asymptomatic, but, as the tumor enlarges, symptoms may include abnor-
mal bleeding, menorrhagia, lower abdominal pain, and increased urinary
frequency. Grossly, leiomyomas are well circumscribed and may be in sub-
serosal, intramural, or submucosal locations. Leiomyomas can be single but
are often multiple and may become quite large. The cut surface is typically
white to tan, with a whorled, bulging appearance. Histologically, the tumor
cells appear as well- differentiated, spindle-shaped smooth muscle cells, often
with increased extracellular matrix, such as collagen, proteoglycan, and
fi bronectin. Leiomyomas rarely become their malignant counterpart, leio-
myosarcomas, which usually develop de novo. Treatment options include
hysterectomy, myomectomy (removal of the fi broid), and hormone therapy.
Adenocarcinoma
invading the
myometrium
B
Fascicles o
f
smooth
muscle
C
CUI_Chap19.indd 382 6/19/2010 12:20:44 PM
CHAPTER 19
■
Female Reproductive System
383
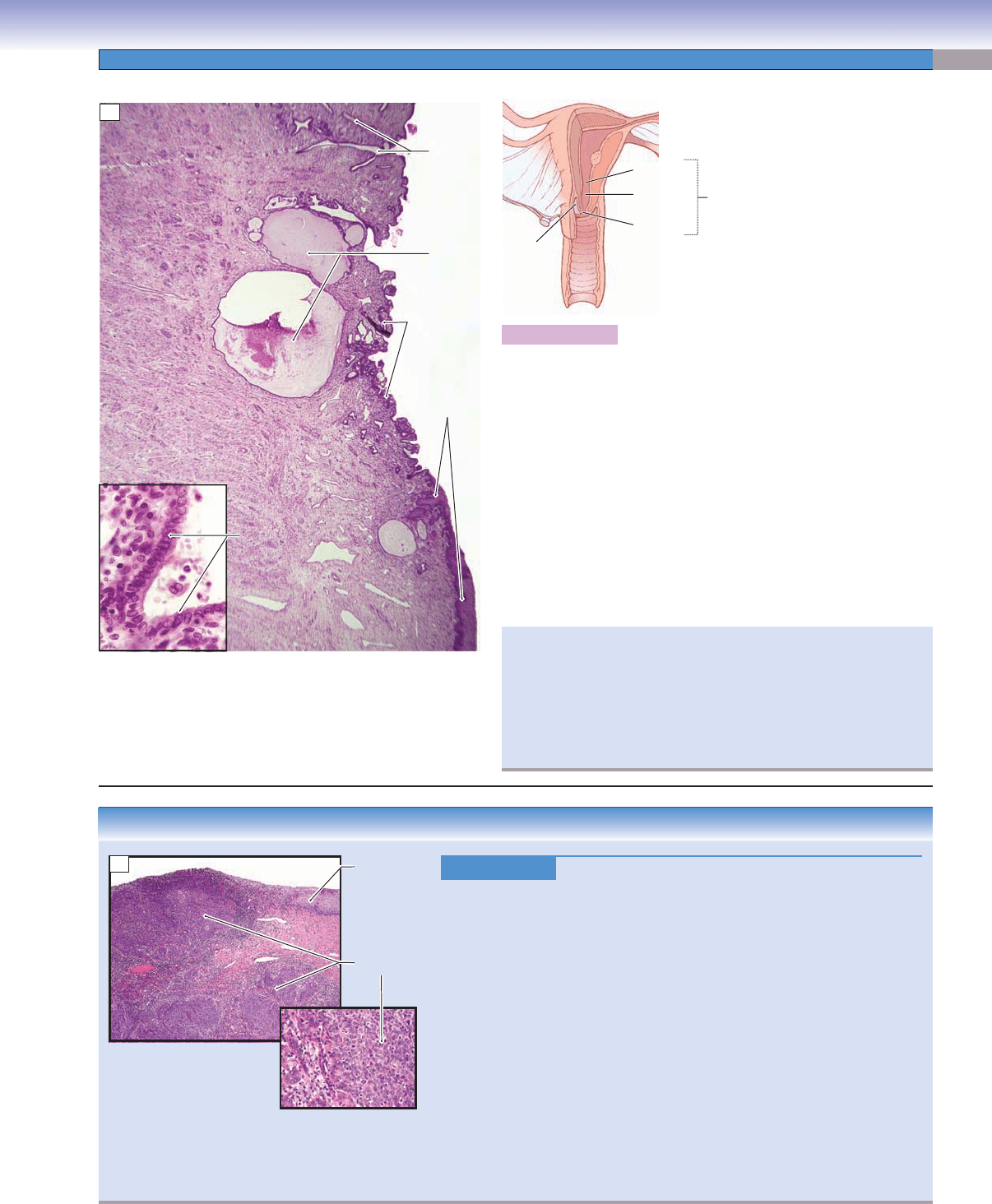
Figure 19-12A. Cervix. H&E, 17; inset 350
The inferior part of the uterus forms the cervical canal, which bulges
into the vagina. The internal os is the opening from the endocervical
canal to the uterus; the external os is the opening to the vaginal canal.
The surface of the endocervix is lined by simple columnar epithelium,
which consists of mucus-secreting cells (inset); the ectocervix is lined
by stratifi ed squamous epithelium. The cervix contains long branched
mucous glands known as cervical glands; when these glands become
obstructed they form cervical cysts (nabothian cysts). The secretion
of the cervix changes depending on the stage of the menstrual cycle;
however, the mucosa of the cervix does not slough off as does the
endometrium of the uterus. The cervical stroma is composed of dense
connective tissue mixed with a small amount (about 15%) of smooth
muscle. Usually, the cervix has a narrow canal; however, during deliv-
ery, dilation of the cervix allows the baby to pass through the canal.
Branched
cervical
glands
Cervical
cysts
Internal os
Endocervical
canal
Ectocervix
Stratified
squamous
epithelium
(ectocervix)
External os
Cervix
Cervical stroma
Cervical stroma
Cervical stroma
Simple columnar
Simple columnar
epithelium
epithelium
(endocervix)
(endocervix)
Simple columnar
epithelium
(endocervix)
Endocervix
Endocervix
Endocervix
A
The cervical transformation (transition) zone is the area of the
cervical mucosa between the original squamocolumnar junction
and the restored or new squamocolumnar junction that is formed
through the processes of squamous metaplasia and squamous
epithelialization. The majority of cervical carcinomas arise in this
zone, and it is important that this area be sampled during screening
with a Papanicolaou smear.
CLINICAL CORRELATION
Figure 19-12B.
Cervical Cancer. H&E (upper left), 20; (lower right), 115
Cervical cancer is a malignant neoplasm of the uterine cervix, the major
-
ity of which are squamous cell carcinomas. Risk factors include the early
onset of sexual activity, multiple sexual partners, and exposure to human
papillomavirus (HPV). Invasive squamous cell carcinoma is preceded by
precursor lesions called cervical intraepithelial neoplasia, in which dysplas-
tic epithelial changes are present. The majority of intraepithelial lesions
are related to infection by HPV. The introduction of screening using the
Papanicolaou smear, or “Pap” smear, has dramatically reduced the inci-
dence of invasive cervical lesions. Symptoms of cervical cancer include
abnormal vaginal bleeding, postcoital bleeding, and vaginal discharge. His-
tologically, the cancer typically arises in the cervical transformation zone
and may show superfi cial ulceration with endophytic or exophytic growth
patterns. The cancer can spread by direct invasion to nearby tissues and
organs or metastasize through hematogenous or lymphatic routes. Garda-
sil, a vaccine against certain HPV types, is used in young women to prevent
infection by the virus. Treatment options include surgical removal of the
uterus (hysterectomy), radiation therapy, and chemotherapy.
Squamous
epithelium
Squamous cell
carcinoma
B
CUI_Chap19.indd 383 6/19/2010 12:20:46 PM
384
UNIT 3
■
Organ Systems
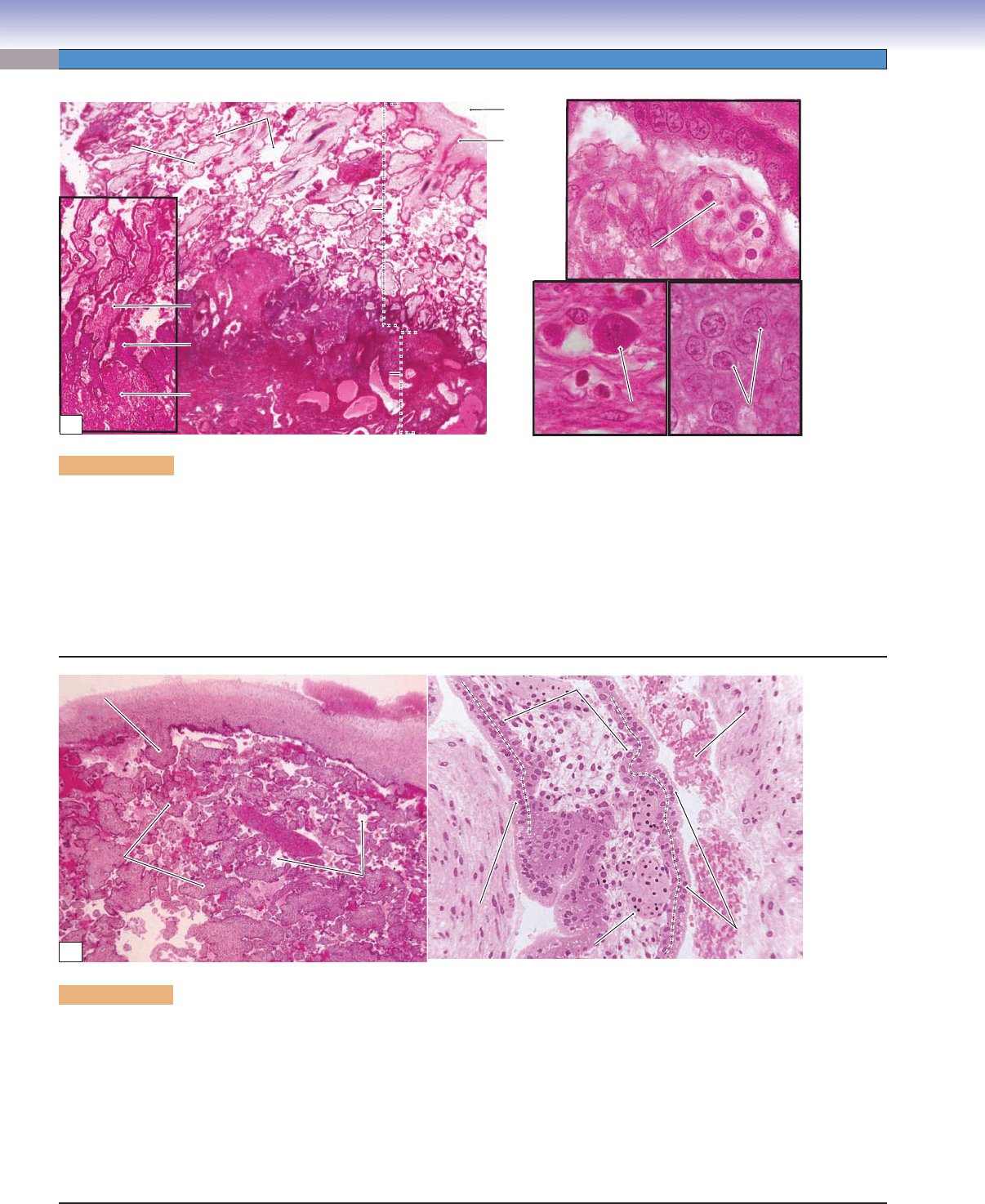
Figure 19-13A. Overview of the placenta. H&E, left 13; left inset 55; right (upper) 704; right (lower) 748
The placenta consists of the maternal portion and the fetal portion. It is a temporary organ that provides a bridge for exchanging
gases, nutrients, hormones, and other materials between the maternal and fetal blood circulations. The maternal portion is the
decidua basalis. The fetal portion consists of the chorionic plate (Fig. 19-11A), chorionic villi, and cytotrophoblastic shell. Fetal
blood fl ows within the blood vessels of the chorionic villi; maternal blood is contained within the intervillous space. The placental
barrier prevents the fetal blood from mixing with the maternal blood. The decidua basalis forms when stromal fi broblasts of the
endometrium are transformed into decidual cells at the site of implantation. The syncytiotrophoblast invades the maternal blood
vessels replacing smooth muscle in the vessel walls. Syncytiotrophoblasts also line the surface of the intervillous space. The cytotro-
phoblast forms an interface (cytotrophoblastic shell) between the maternal and fetal tissues.
Decidual cell
Decidual cell
Decidual cell
Cells in
Cells in
cytotrophoblastic shell
cytotrophoblastic shell
Cells in
cytotrophoblastic shell
Fetal blood cells
Fetal blood cells
within the chorionic villus
within the chorionic villus
Fetal blood cells
within the chorionic villus
Chorionic
plate
Amniotic
cavity
Floating
Floating
chorionic
chorionic
villus
villus
Floating
chorionic
villus
Intervilluus space
Intervilluus space
Intervillous space
Fetal
Fetal
portion
portion
Fetal
portion
Maternal portion
Maternal portion
(decidua basalis)
(decidua basalis)
Maternal portion
(decidua basalis)
Anchoring
Anchoring
villus
villus
Anchoring
villus
Decidua
Decidua
basalis
basalis
Decidua
basalis
Cytotrophoblastic
Cytotrophoblastic
shell
shell
Cytotrophoblastic
shell
A
Chorionic
Chorionic
villus
villus
Chorionic
villus
Stem
Stem
villus
villus
Stem
villus
Chorionic plate
Chorionic plate
Chorionic plate
Fetal blood vessel
Fetal blood vessel
Fetal blood vessel
Syncytiotrophoblast
Syncytiotrophoblast
Syncytiotrophoblast
Syncytiotrophoblast
Syncytiotrophoblast
Syncytiotrophoblast
Intervillous
Intervillous
space
space
Intervillous
space
Amniotic cavity
Amniotic cavity
Amniotic cavity
Cytotrophoblast
Cytotrophoblast
Cytotrophoblast
Maternal blood in the
Maternal blood in the
intervillous space
intervillous space
Maternal blood in the
intervillous space
Chorionic villus
Chorionic villus
Chorionic villus
B
Figure 19-13B. Fetal portion of the placenta. H&E, left 18; right 136
The chorionic plate consists of connective tissue and forms the wall of the amniotic cavity; it contains chorionic arteries and veins. The
chorionic villi can be classifi ed on the basis of their developmental stages: (1) Primary chorionic villi are newly formed villi at an early
stage (about the second week of implantation), and consist of only a trophoblast layer. (2) Secondary chorionic villi develop at the end of
the second week when mesenchymal tissue grows into the villi and forms a mesenchymal core within the trophoblastic shell. (3) Tertiary
chorionic villi develop at the third week, at which time the fetal blood and blood vessels are formed within the chorionic villi. By the end of
the third week, the fetal blood begins to fl ow, and gas and nutrient exchange takes place between the fetal and maternal blood by diffusion
through the placental barrier. The placental barrier is composed of the syncytiotrophoblast, cytotrophoblast, connective tissue of the villus,
endothelium of the fetal capillary, and the basement membranes of the trophoblast and endothelium. The syncytiotrophoblast produces
hCG hormone, which plays an important role in maintaining pregnancy via stimulation of the corpus luteum to secrete progesterone.
CUI_Chap19.indd 384 6/19/2010 12:20:50 PM