Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


Jacobs-Reitsma W (2000) Campylobacter in the food
supply. In: Nachamkin I and Blaser MJ (eds) Campylo-
bacter, 2nd edn. pp. 467–481. Washington, DC: Ameri-
can Society for Microbiology.
Nachamkin I and Skirrow MB (1998) Campylobacter,
Arcobacter, and Helicobacter. In: Collier L, Balows A
and Sussman M (eds) Topley and Wilson’s Microbiology
and Microbial Infections, 9th edn. vol. 2, pp.
1237–1256. London: Edward Arnold.
Skirrow MB (1998) Infection with Campylobacter and
Arcobacter. In: Collier L, Balows A and Sussman M
(eds) Topley and Wilson’s Microbiology and Microbial
Infections, 9th edn. vol. 3, pp. 567–580. London:
Edward Arnold.
Solomon EB and Hoover DG (1999) Campylobacter
jejuni: a bacterial paradox. Journal of Food Safety 19:
121–136.
Todd ECD (1997) Epidemiology of foodborne diseases: a
worldwide review. World Health Statistics Quarterly 50:
30–50.
Wesley IV (1996) Helicobacter and Arcobacter species:
risks for foods and beverages. Journal of Food Protec-
tion 59: 1127–1132.
Detection
M B Skirrow, Gloucestershire Royal Hospital,
Gloucester, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 The conventional means of detecting campylobacters
is by isolation in culture. In this article their micro-
aerobic growth requirements and special needs for
isolation from foods are described, including selective
enrichment and plating on selective agar. Direct
detection of campylobacters by immunological and
DNA probe techniques are becoming more sensitive
and specific by the application of polymerase chain
reaction (PCR) methods, but they are as yet too com-
plex to be adopted routinely. Campylobacters can
be provisionally identified by phenotypic methods
in most laboratories, but definitive identification
requires molecular methods that are available only
in reference laboratories. Strain typing of campylo-
bacters (serotyping, phage typing, molecular typing)
is also best performed in reference laboratories. Ad-
vances in molecular typing in particular are paving
the way for better source tracing and understanding
of the epidemiology of campylobacter infection.
Principles of Campylobacter Cultivation
0002The failure of traditional cultural methods to provide
the conditions necessary for the growth of campylo-
bacters was the main reason why their role in human
disease remained hidden for so long. The main pecu-
liarity of campylobacters is that they are strictly
microaerophilic and require specially prepared at-
mospheres for satisfactory growth. Specific selection,
either by means of selective media or filtration, is
essential for their isolation from feces or other
specimens containing mixed organisms. Moreover,
they only grow well on supplemented media, and
Campylobacter jejuni, C. coli,andC. lari – the so-
called thermophilic group that causes campylobacter
enteritis – have an optimum growth temperature of
42–43
C.
Oxygen Sensitivity
0003Oxygen sensitivity is the most critical factor in the
cultivation of campylobacters. Campylobacters have
a respiratory type of metabolism based on the krebs
cycle, so oxygen is necessary for growth; yet oxygen
at atmospheric pressures is toxic. This toxicity is due
to superoxides and free radicals that form in unsup-
plemented media exposed to air, particularly in the
light. Campylobacters are especially vulnerable to
these compounds despite being able to produce super-
oxide dismutase and catalase. They are most vulner-
able in the resting phase; once they have started to
grow they become more oxygen-tolerant, probably
owing to the production of nicotinamide adenine
dinucleotide (NAD) or nicotinamide adenine di-
nucleotide phosphate (NADP), which forms a
physiological barrier that protects oxygen-sensitive
enzymes. The practical points that arise from this
are twofold:
1.
0004Heavy inocula are required to initiate growth on
unsupplemented media. Large populations usually
have a few bacteria that are able to start growing
and thereby create conditions suitable for other
cells to grow. The result of seeding campylobacters
on unsupplemented media tends to be either
confluent growth or none at all.
2.
0005The key supplements for growing campylo-
bacters are agents that neutralize superoxides
and free radicals; any nutrient value they have
is incidental. Blood, hemin, hematin, activated
charcoal, dihydroxyphenyl, and iron compounds
are examples of such agents. A simple and
widely used supplement is the triple combination
of ferrous sulfate, sodium metabisulfite, and
sodium pyruvate, each at a final concentration of
0.025% (FBP).
786
CAMPYLOBACTER
/Detection

Detection in Food by Culture
0006 The isolation of campylobacters from food is more
difficult than from the feces of a patient with cam-
pylobacter enteritis, as there are usually far fewer
organisms present. For fecal specimens direct plate
culture is normally adequate – indeed, organisms
may be so plentiful that a presumptive diagnosis can
be made by direct microscopy – but for food, selective
enrichment cultures are essential. Possible exceptions
are raw poultry products, which may be so heavily
contaminated that enrichment is not critical; indeed,
for some chicken samples enrichment has proved to
be less sensitive than direct plating.
0007 The principle of the enrichment method is to incu-
bate the food (after stomaching or other treatment to
break it down) in a selective broth for 24 – 48 h and
then subculture on a selective agar for the isolation
and identification of individual colonies. However,
for campylobacters that have been subjected to hot
or cold stress, which causes sublethal injury, other
techniques may be necessary. As the treatment the
foods have received is not always known, there is
much to be said for including the more sensitive
techniques routinely.
0008 When properly carried out, cultural methods are
able to detect 1 campylobacter colony-forming unit
(CFU) in 2 g food that contains at least 10
6
g
1
of
other bacteria.
Specimen Handling and Transport
0009 The correct handling and preservation of specimens
are crucial for food specimens; incorrect handling
negates the value of sensitive isolation procedures.
The three most important factors are refrigeration
(as near to 4
C as possible), exclusion of oxygen,
and prevention of drying. Oxygen may be excluded
by gassing with 100% N
2
, but this is not always
practicable. Provided specimens are not unduly large,
they can be placed in a semisolid transport medium,
such as Cary-Blair medium (0.16% agar), or directly
into a campylobacter-selective broth, each containing
either FBP or sodium bisulfite 0.01%. The choice of
medium may be critical, and it is often better to use a
highly selective formulation, as campylobacters do
not compete well with other microorganisms. The
choice will be influenced by the nature of the sample,
the physical state of the target organisms, and the
time likely to elapse before cultures are set up.
0010 Milk and liquid foods should be held refrigerated
after adding sodium bisulfite 0.01% and either
sodium thioglycollate 0.15% or 100% N
2
. Under
these conditions there is little loss of viability over
several days, but the sooner specimens are cultured
the better.
Enrichment Techniques
0011Campylobacters that have been frozen, chilled (4
C),
or subjected to mild heating become sublethally in-
jured. This is manifested by increased susceptibility
to antibiotics (notably rifampicin and polymyxin),
deoxycholate, oxygen radicals such as peroxides,
and high incubation temperatures. This susceptibility
is thought to be due to damage to the outer membrane
of the bacterial cell and it can significantly reduce the
efficacy of detection by culture.
0012Thus the first stage of an isolation procedure is
designed to allow the organisms time to recover.
Ideally this is done in a nonselective broth incubated
at 37
C. This is feasible with samples such as water
containing few competing flora, and in which cam-
pylobacters are often severely injured. However, for
samples such as chicken, preincubation in nonselec-
tive media often results in a reduced isolation rate
because the high numbers of competing flora over-
whelm Campylobacter. Given the unpredictability of
bacterial contamination levels, it is better to use se-
lective media for the routine examination of food,
water, and environmental samples. The broth should
be at about room temperature when inoculated, and
if the volume is large, incubation is best done in a
water bath.
0013In choosing a liquid-selective medium it is import-
ant to take one that is able to suppress the growth of
competing flora adequately, particularly Pseudomo-
nas and Proteus spp. The choice will depend partly on
the type of sample being examined, as some of the
many available formulae perform better with some
materials than others. A good all-round highly select-
ive medium is Exeter broth (Table 1).
0014Various protocols have been laid down for incuba-
tion procedures. In general, maximum sensitivity can
tbl0001Table 1 Formula for Exeter campylobacter-selective
enrichU
`
ment broth (and agar)
Nutrient broth
a
1l
Sodium metabisulfite 0.25 g
Sodium pyruvate 0.25 g
b
Ferrous sulfate (7.H
2
O) 0.25 g
Polymyxin 2500 IU
Rifampicin 5 mg
Trimethoprim 10 mg
c
Cefoperazone 15 mg
Amphotericin 2 mg
Lysed horse blood 50 ml
(New Zealand agar
d
15 g)
a
Nutrient broth no. 2 (CM67, Oxoid Ltd, Basingstoke, UK) in original
formula.
b
Commercially available as MAST SV61 Campylobacter growth
supplement.
c
Commercially available as MAST SV59 Campylobacter-selective
supplement.
d
Only for solid plating medium.
CAMPYLOBACTER
/Detection 787

be attained by initial incubation at 37
C for 18 h
followed by incubation at 42–43
C for 30 h. This
latter period can be extended for a further 24 h, and
with some lightly contaminated samples the use of
this extension has been shown to improve isolation
rates. With highly selective media like Exeter broth it
is possible to incubate samples at 37
C throughout.
In general, as large a volume of broth as is practicable
should be used in order to accommodate as much of
the sample as possible; a minimum of 25 g in 225 ml
broth is recommended.
0015 For liquid samples such as milk, it may be con-
venient to add the sample to an equal volume of
double-strength medium. For maximum sensitivity,
however, it is necessary to examine large volumes
(around 200 ml) and this can present problems.
Alternative methods of testing large volumes are to
culture gauze or cotton wool pads through which
the milk has been filtered, or to culture centrifuged
deposits.
0016 It is generally acceptable to incubate fluid cultures
in closed vessels containing air. Slight increases in
sensitivity can be attained by the use of Erlenmeyer
flasks with stoppered side-arms, so that air can be
partially extracted and replaced with a mixture of
10% carbon dioxide, 10% hydrogen, and 80% nitro-
gen. Best results are obtained if there is a constant
flow of gas mixture with agitation of the broth.
Subculture to Agar Plates
0017 Mature enrichment cultures are subcultured on a
campylobacter-selective agar. There are numerous
formulae, but either charcoal, cefoperazone, deoxy-
cholate (CCDA) or Exeter agars are recommended.
Hydrogen peroxide and other potentially toxic
oxygen metabolites can accumulate in agar even if
the plates are stored in the dark under refrigeration.
It has been shown that these compounds act synergi-
cally with antibiotics, such as rifampicin, to inhibit
campylobacter growth severely. Thus for maximum
sensitivity it is important to use fresh plates and
include FBP supplement in the agar, even if blood is
also included.
0018 Plates are incubated at 42–43
C in a microaerobic
atmosphere containing 5–10% oxygen and prefer-
ably some hydrogen. If cylinder gases are available,
the easiest method is to extract two-thirds of the air
from a closed container, such as an anaerobic jar
(without catalyst), and replace it with a mixture of
10% carbon dioxide, 10% hydrogen, and 80% nitro-
gen. If there is no cylinder gas, an anaerobic-type gas-
generating envelope can be used, and the jar partially
evacuated after closure. Alternatively, special gas-
generating envelopes for campylobacters are com-
mercially available for use in jars with a catalyst.
0019Growth is usually visible after 24 h, but occasional
strains do not appear until incubation has been main-
tained for 48 h.
0020The foregoing protocols are designed to detect the
main causes of campylobacter enteritis, namely
C. jejuni and C. coli (they will also detect C. lari).
Other species of campylobacter and related bacteria,
such as C. uppsaliensis, C. hyointestinalis, and Arco-
bacter butzleri, which have been implicated to a lesser
degree, are unlikely to be detected. Those wishing
to isolate these bacteria, for research or whatever
reason, must use special selective media incubated at
37
C rather than 42
C. Alteratively, nonselective
media may be used in conjunction with membrane
filters placed on the agar.
Fecal Indicator Bacteria and Campylobacters
0021It will be evident from the foregoing account that
the culture of campylobacters from food is time-
consuming and costly, especially if regular monitor-
ing is undertaken. Campylobacters are rarely found in
the absence of fecal bacteria, so for processed foods it
is reasonable to screen for the latter rather than look
for campylobacters. Most raw meats have fecal coli-
forms on them, and it must be assumed they also have
campylobacters. In short, it pays to think carefully
about the value of screening for campylobacters
before undertaking a monitoring program; it could
be unproductive and uneconomic.
Identification
0022In general, most Campylobacter colonies are typically
flat, effuse, and wet-looking, although other morpho-
types can occur. Identity is confirmed by a positive
oxidase reaction and the presence of characteristic
motile, spiral, or S-shaped Gram-negative organisms
in wet preparations and Gram-stained smears. Add-
itional basic identification tests are shown in Table 2.
Sets of these tests are available from commercial
sources and one includes simple resistogram typing.
Latex agglutination tests for identification are also
available commercially, but they need careful assess-
ment. Molecular methods that depend on the analysis
of DNA fragments can perform well in identification
tests, but they tend to be too complex for general use.
In choosing a test appropriate to one’s needs it is
important to know whether it discriminates between
groups of species, single species, or strains within a
species.
0023Meat samples, especially chicken meats, are likely
to carry Arcobacter spp. These bacteria closely resem-
ble Campylobacter spp. on agar plates. Arcobacter
spp. can be distinguished by their ability to grow in
air at 25
C(Table 2). Not all Arcobacter spp. grow at
42
C.
788
CAMPYLOBACTER
/Detection
Typing
0024 Serotyping on the basis of heat-stable lipopolysac-
charide antigens (Penner system) and heat-labile
flagellar and outer-membrane protein antigens (Lior
system) is the main typing method in current use.
There are several hundred designated serotypes, but
only a limited number are found frequently. The dis-
criminatory power of serotyping can be enhanced by
the parallel use of biotyping and/or phage typing.
Typing facilities are only available at reference
laboratories.
0025 In recent years a plethora of molecular-typing
methods have appeared based on the analysis of frag-
ments of DNA split by specific enzymes. Their
discriminatory powers and complexity vary widely.
Some are simple enough for wide application, but all
suffer from a lack of standardization. Until this prob-
lem is resolved, serotyping, supplemented with phage
typing, remains the basic typing method.
Detection in Food by Noncultural Methods
0026 Immunological methods that make use of high-
affinity monoclonal antibodies were the first noncul-
tural methods to be used for the direct detection of
campylobacters. The antibody/bacterial antigen reac-
tion was detected by latex agglutination or enzyme-
linked immunosorbent assay (ELISA). Work on these
techniques was largely foresaken in favor of molecu-
lar methods, in which fragments of DNA specific to
the bacterium are recognized by specific probes and
then amplified by PCR. A sensitivity of 3–15 C. jejuni
cells in 100 ml water and 3 g
1
has been claimed.
These methods work better with samples that do
not contain an excess of other bacteria or biological
material, but they have recently been made to work
with feces. The main problem is that they need spe-
cialized skills and reagents. False-positive results are
likely unless scrupulous care is taken to avoid con-
tamination with DNA. These methods are likely to
come into their own as they become refined and easier
to use.
Detection in Suspected Food Poisoning
0027Outbreaks of campylobacter enteritis usually come to
light through the recognition of a sudden excess of
campylobacter isolations in a clinical laboratory, or,
less often, by the recognition of an excess of diarrhea
in a community. Either way the laboratory plays a key
role, as the infection cannot be diagnosed clinically.
Unfortunately, outbreak investigations are hampered
by the long time that elapses between food consump-
tion and awareness of an outbreak: the average
incubation period is 3 days; people tend not to
seek medical attention until they have been ill for
several days; sampling, testing, and reporting may
take 2–3 days; and several more days may pass before
someone realizes that cases are epidemiologically
connected. Thus, the investigation may only start
2 weeks or more after ingestion of the food, long
after suspect items have been discarded. Even if
foods are available, the vulnerability of campylo-
bacters mitigates against their survival in detectable
numbers. (See Food Poisoning: Tracing Origins and
Testing.)
0028For the above reasons reliance must often be placed
on statistical associations of infection with foods
eaten. Such evidence can be powerful and prove
beyond all reasonable doubt that a particular food
was the vehicle of infection. Protocols for investigat-
ing such outbreaks can be complex and require close
cooperation between community doctors, public
health workers, microbiologists, veterinarians, and
food producers. The prime essential is to have all
efforts directed and coordinated by one person.
See also: Campylobacter: Properties and Occurrence;
Campylobacteriosis; Food Poisoning: Tracing Origins
and Testing
Further Reading
Advisory Committee on the Microbiological Safety of Food
(1999) Report on Microbial Antibiotic Resistance in
Relation to Food Safety. London: Stationery Office.
tbl0002 Table 2 Basic differential characters of campylobacters likely to be found in food
Species Growth at 25
C Hippurate hydrolysis Indoxylacetate hydrolysis Sensitivities
Nalidixic acid Cephalothin
C. jejuni þ þ SR
C. coli þ SR
C. lari RR
C. fetus þ RS
Arcobacter spp. þ
a
þ SR
, negative; þ, positive; R, resistant (no zone of inhibition to 30 mg disk); S, sensitive (any zone of inhibition to 30 mg disk).
a
Growth in air.
CAMPYLOBACTER
/Detection 789

Corry JEL, Post DE, Colin P and Laisney MJ (1995) Culture
media for the isolation of campylobacters. International
Journal of Food Microbiology 26: 43–76.
Hurtado A and Owen RJ (1997) A molecular scheme based
on 23S rRNA gene polymorphisms for rapid identifica-
tion of Campylobacter and Arcobacter species. Journal
of Clinical Microbiology 35: 2401–2404.
Johnson LG and Murano EA (1999) Comparison of three
protocols for the isolation of Arcobacter from poultry.
Journal of Food Protection 62: 610–614.
Mason MJ, Humphrey TJ and Martin KW (1999) Isolation
of sublethally injured campylobacters from poultry and
water sources. British Journal of Biomedical Science 56:
2–5.
Nachamkin I and Skirrow MB (1998) Campylobacter,
Arcobacter, and Helicobacter. In: Collier L, Balows A
and Sussman M (eds) Topley and Wilson’s Microbiology
and Microbial Infections, 9th edn, vol. 2, pp. 1237–
1256. London: Edward Arnold.
Nachamkin I, Engberg J and Aerestrup FM (2000) Diagno-
sis and antimicrobial susceptibility of Campylobacter
species. In: Nachamkin I and Blaser MJ (eds) Campylo-
bacter, 2nd edn, pp. 45–66. Washington DC, ASM Press.
Owen RJ (1995) Update on epidemiological typing of Cam-
pylobacter. PHLS Microbiology Digest 12: 2–6.
Owen RJ, Lorenz E and Gibson J (1997) Application of the
Mast resistotyping scheme to Campylobacter jejuni and
C. coli. Journal of Medical Microbiology 46: 34–38.
Roberts D, Hooper W and Greenwood M (eds) (1995)
Practical Food Microbiology, 2nd edn. London: Public
Health Laboratory Service.
Waage AS, Vardund T, Lund V and Kapperud G (1999)
Detection of small numbers of Campylobacter jejuni and
Campylobacter coli cells in environmental water, sewage,
and food samples by a seminested PCR assay. Applied and
Environmental Microbiology 65: 1636–1643.
Campylobacteriosis
M B Skirrow, Gloucestershire Royal Hospital,
Gloucester, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Campylobacteriosis, or Campylobacter enteritis, is
an infection of the intestines manifest by acute
diarrhea and abdominal pain. It is the most frequently
reported form of infective diarrhea in the human
population in most industrialized nations. Although
the illness seldom lasts more than a few days,
occasional patients develop complications, such as
reactive arthritis or Guillain–Barre
´
syndrome (GBS),
a serious neurological disorder that can result in
permanent disability or even death. The burden of
campylobacteriosis on society in terms of health
care, economic costs, and suffering is immense. This
article describes the clinical manifestations, path-
ology, and treatment of the disease, and ends by
considering options for its prevention and control.
There are many approaches to control, but ultimately
the only one that will have lasting impact is the con-
trol of infection in food-producing animals, especially
broiler chickens.
Clinical Features
0002Campylobacter enteritis is caused mainly by Cam-
pylobacter jejuni and C. coli (See Campylobacter:
Properties and Occurrence), but before describing
the disease due to these organisms, brief mention is
made of an uncommon low-grade septicemic form of
infection known as systemic campylobacteriosis,
usually caused by C. fetus. Although blood stream
invasion by C. fetus may arise from intestinal colon-
ization, diarrhea is not a common feature. This form
of infection is limited to patients with disease of the
immune system, cancer, or some other chronic disease
compromising their immunity. It is of minor import-
ance relative to Campylobacter enteritis, but it earns
a place here because C. fetus infection has been ac-
quired by eating raw calves’ liver. C. fetus is a
common inhabitant of the intestinal tract of sheep
and cattle, in which it may cause septic abortion.
0003Campylobacter enteritis is an acute self-limiting
diarrheal disease clinically indistinguishable from Sal-
monella enteritis, although minor differences become
apparent when groups of patients are compared.
0004Infection can be established with as few as 500
organisms. The average incubation period is 3 days
(range 1–7 days). In most patients the illness starts
with abdominal pain and diarrhea, but in about one-
third of patients there is an influenza-like prodrome
of malaise, headache, and fever, sometimes with
rigors, for a period ranging from a few hours to a
day or so before the onset of gastrointestinal symp-
toms. Profuse diarrhea lasts for 2–3 days and is
almost invariably accompanied by abdominal pain,
which is sometimes severe enough to simulate acute
appendicitis and cause some patients to undergo
emergency surgery. Occasionally there is genuine ap-
pendicitis. Children sometimes have abdominal pain
without diarrhea. Surveys of patients affected in com-
munity outbreaks show that, on average, about 50%
have fever, 40% myalgia, 8% rigors, 14% frank
blood in their stools, but only 15% vomit, even
though nausea is common.
0005Some patients present with acute colitis that is dif-
ficult to distinguish from an acute attack of idiopathic
ulcerative colitis (inflammatory bowel disease). Acute
790
CAMPYLOBACTER
/Campylobacteriosis

complications are rare but include intestinal haemor-
rhage, toxic megacolon, hemolytic–uremic syndrome,
pancreatitis, and septic abortion.
0006 After a few days the diarrhea eases and about 80%
of patients recover within a week, irrespective of any
treatment they may receive. Minor relapses have been
reported in about 20% of patients after a day or two
without diarrhea.
0007 Young and middle-aged adults seem to be most
severely affected by the infection. Unlike salmonel-
losis, Campylobacter enteritis in infants is often mild,
and although infection in old people tends to be more
invasive, it is seldom dangerous. Death is rare and
virtually limited to frail patients debilitated from
other causes.
Late Complications
0008 There are two late complications that typically arise
1–2 weeks after the onset of illness: reactive arthritis
and GBS.
Reactive Arthritis
0009 Reactive (aseptic) arthritis affects about 1% of pa-
tients, particularly those possessing the human leuko-
cyte antigen (HLA) B27. The ankles, knees, wrists,
and the small joints of the hands are most frequently
affected, often in migratory fashion. It can cause
painful debility lasting for several months, but it is
ultimately benign. Clinically it is the same as the
reactive arthritis that sometimes follows other forms
of acute bacterial enteritis.
Guillain–Barre
´
Syndrome
0010 Another name for GBS is postinfective polyneuropathy.
It is a serious, though fortunately rare complication
causing paralysis that does not always resolve com-
pletely. Severely affected patients develop respiratory
paralysis and have to be nursed on a ventilator. Surveys
indicate that Campylobacter infection is the antecedent
event in 14–41% of patients with GBS – it is the most
commonly identified trigger for the disease.
0011 The mechanism of this distressing condition, in
which the myelin in peripheral nerves becomes lost
or damaged, is thought to be immunological. Certain
C. jejuni strains are particularly associated with GBS,
and some have been found to possess cell wall epi-
topes that cross-react with proteins in peripheral
nerve myelin. It is believed that this triggers immuno-
logical attack and destruction of the myelin.
Convalescent Excretion
0012 Excretion of Campylobacter in feces falls off expo-
nentially after illness. About 50% of patients are
culture-negative after 3 weeks, and virtually all are
negative after 3 months. Long-term carriage is un-
known except in patients with severe immune defi-
ciency, such as hypogammaglobulinemia or acquired
immune deficiency syndrome (AIDS). Spread of infec-
tion from a healthy excreter is a remote risk. In the
case of food handlers, provided they have formed
stools there is no need to exclude them from work.
0013The basic features of Campylobacter enteritis are
summarized in Table 1.
Pathology
0014The essential lesion in Campylobacter enteritis is
an acute inflammation of the jejunum and small
intestine, which progresses to the cecum, colon, and
rectum. The histopathology of the intestinal mucosa
is one of acute inflammatory cellular infiltration in-
distinguishable from that seen in Salmonella, Shi-
gella, or other acute bacterial infections of the gut.
The terminal ileum and cecum are often particularly
affected, and it is this feature that causes the
symptoms that mimic acute appendicitis.
0015Campylobacter are invasive and may be present in
the blood stream at the onset of illness, as indicated
by the high fever and rigors experienced by some
patients. Unlike C. fetus, C. jejuni and C. coli are
sensitive to the natural killing power of normal
serum, so any bacteremia is likely to be transient
and hence seldom detected in blood cultures (bacter-
emia reported in only 0.15% of infections). Regional
lymph nodes are often enlarged and inflamed. A chol-
era-like enterotoxin and at least one cytotoxin are
produced in modest quantities by many strains of C.
jejuni and C. coli, but the role played by these in
pathogenesis is unclear.
Immunity
0016Circulating (humoral) antibodies are produced within
a few days of illness and for at least several months
patients are refractory to reinfection with the same
strain. People regularly exposed to infection develop
tbl0001Table 1 Basic features of Campylobacter enteritis
Feature Duration and details
Incubation period 3 days (range 1–7 days)
Main symptoms Diarrhea, abdominal pain, fever
Mean duration of illness
a
Incapacity 3.8 days
Symptoms 14.6 days
Mean duration of fecal
Campylobacter excretion
a
38 days (maximum 69 days)
Exclusion from food handling Until stools formed
a
Figures taken from a Norwegian study of 135 sporadic cases.
CAMPYLOBACTER
/Campylobacteriosis 791

solid immunity. Children in developing countries,
where transmission rates are high, become immune
within the first 2 years or so of life, and occupation-
ally exposed groups in industrialized countries also
become immune. For example, in a milkborne out-
break of Campylobacter enteritis in the USA, 76% of
people exposed for the first time were ill, whereas no
person who habitually drank raw milk became ill.
In the UK significant amounts of Campylobacter-
specific antibody were found in 18% of veterinary as-
sistants, 36% of cattle abattoir workers, and 27–68%
of workers in poultry-processing plants, compared
with 2–5% in nonexposed adults. Infection with one
or two strains may be sufficient to give broad immun-
ity, although there are patients who have had two
attacks of Campylobacter enteritis several months
apart; in each case the second infection has been
with a different strain. It is not known how long
immunity lasts, but regular exposure is probably
necessary for its maintenance.
Treatment
0017 As Campylobacter enteritis almost always resolves
spontaneously, treatment is primarily symptomatic
and supportive. The most important element, as
with all forms of acute diarrhea, is the correction of
dehydration and electrolyte loss, particularly in
infants and old people, who are least able to do this
of their own accord. In many cases simply getting
patients to increase their fluid intake with assorted
drinks is sufficient, but giving a balanced electrolyte
preparation such as Dioralyte is ideal.
0018 Antimicrobial therapy is effective if given within a
day or two of the onset of illness, but a bacteriological
diagnosis has seldom been made at this stage. If a
patient is still suffering from acute symptoms when
a positive report is received, antimicrobial therapy is
justified. Erythromycin is the antibiotic of choice for
both children and adults. In patients with severe diar-
rheal illness, who might be put at risk if treatment
were delayed until a bacteriological report was avail-
able, there is a case for treating empirically with an
antimicrobial agent effective against the common
enteropathogenic bacteria. Ciprofloxacin, or an
equivalent quinolone drug, was once the ideal agent
here, and it still may be in some places. Unfortunately,
in recent years resistance rates in Campylobacter (as
well as Salmonella) have soared to around 50% in
some European countries, so that its use has been
drastically compromised. This is almost certainly a
result of the widespread use of quinolones in poultry.
0019 Fortunately erythromycin resistance is less of a
problem. In industrialized countries resistance has
remained at about 1–5% of strains, but higher rates
have been found in some developing countries,
notably 65% in Thailand. Erythromycin resistance
is much more common in C. coli than C. jejuni,
probably due to the use of tylosin, a similar macrolide
antibiotic, in pig rearing.
Prevention
0020Basic measures for the prevention of any communic-
able intestinal infection apply equally to Campylo-
bacter enteritis. These include the treatment and safe
disposal of sewage, the provision of potable water, the
pasteurization or equivalent heat treatment of milk,
and the general hygienic processing and handling
of food. An important aspect of the prevention of
Campylobacter infection is the interruption of trans-
mission from food-producing animals, particularly
poultry, to the final food product. Each of these is
now considered.
Sewage Disposal
0021Campylobacter are plentiful in raw sewage. The dis-
charge of untreated sewage is undesirable as it helps
to maintain the Campylobacter population in the
environment. Conventional sewage treatment is ef-
fective in eliminating Campylobacter. In one study
over 78% were removed after primary sedimentation,
and less than 0.1% remained in the final effluent.
Water Purification
0022Campylobacter are ubiquitous in natural surface
waters, including sea water. They are capable of sur-
viving for several weeks in cold water (below 15
C).
Survival is increased in waters that have an autoch-
thonous microflora. Campylobacter also appear to be
capable of forming viable but nonculturable forms,
which are alleged to survive for several months or
longer. However, the potential role of such dormant
cells in the epidemiology of Campylobacter has
yet to be established. Conventional treatments are
fully adequate for removing Campylobacter, which
are generally more sensitive to chlorine and other
disinfecting agents than Escherichia coli. Contact
with monochloramine 1.0 mg l
1
for 15 min or
free chlorine 0.1 mg l
1
for 5 min causes more than
99% inactivation. Campylobacter are also sensitive
to ultraviolet light and are destroyed by protocols
designed to kill E. coli.
0023Major community outbreaks of Campylobacter
enteritis have been caused by the distribution of
unchlorinated or inadequately chlorinated water (See
Campylobacter: Properties and Occurrence), which
serves to emphasize the importance of proper treatment.
This applies equally to remote oligotrophic lakes and
surface waters, which become contaminated from wild
792
CAMPYLOBACTER
/Campylobacteriosis

birds and other animals. A number of outbreaks have
arisen as a result of the failure of outdated, overloaded,
or inadequately maintained water works or distribution
systems. (See Water Supplies: Water Treatment.)
Heat Treatment of Milk
0024 Pasteurization and other orthodox treatment pro-
cesses are fully effective in destroying Campylobacter.
Despite this, milkborne outbreaks of infection regu-
larly occur, even where it is illegal to sell raw milk
to the public. Some of the largest outbreaks of Cam-
pylobacter enteritis on record have been milkborne,
mostly from the distribution of raw milk, but a few
of them from ostensibly pasteurized milk. Thus,
although compulsory pasteurization is a highly
desirable goal, it is unlikely to eliminate all risks of
milkborne infection. Bad design, malfunctioning of
machinery, or those running the machinery, the diffi-
culty of designing satisfactory small pasteurizing
units at reasonable cost are all factors that need at-
tention in order to minimize risks. Electricity supply
failures putting pasteurizing machinery out of action
and bad weather preventing the delivery of milk to
central pasteurizing plants have also been precipitat-
ing factors in outbreaks of milkborne infection.
Food Hygiene
0025 Measures taken to maintain good hygiene and food-
handling practice in restaurants and other catering
establishments are fundamental to the prevention of
Campylobacter enteritis. Much infection is believed
to be transmitted through the cross-contamination
of cooked or ready-to-eat foods, such as bread and
salads, from raw poultry or other raw meats. The
separation of raw from cooked foods and the use of
dedicated equipment for each, such as chopping
boards, mixers, knives, and other utensils, is the
single most important principle to be observed. If
raw meats cannot be stored separately they should
always be placed on a bottom shelf so they cannot
drip juices on to other foods.
0026 Raw poultry should be handled as little as possible;
handling and even washing carcasses only spreads
organisms around work areas. The discipline of
washing hands after touching raw meats of any sort
should be rigorously observed.
0027 It has been shown that Campylobacter can be isol-
ated from the flesh of chicken carcasses even when the
surface has been disinfected by immersion in boiling
water. Chicken muscle affords the organism some
protection from the effects of heat and this is the
probable explanation for the implication of barbe-
cued chicken in outbreaks of Campylobacter enter-
itis. It is therefore particularly important that chicken
and other poultry meat is properly cooked.
0028These rules must be taught to all professional food
handlers and it is the responsibility of health author-
ities to see that correct instruction is carried out and
maintained to satisfactory standards. Analysis of out-
breaks shows that many arose through ignorance of
these basic rules. (See Poultry: Chicken.)
Control of
Campylobacter
in Poultry
0029Elimination of Campylobacter from food-producing
animals is clearly impracticable owing to the wide
natural distribution of the organisms. Yet there
are ways of reducing colonization in farm animals,
especially in poultry.
0030Campylobacter colonization in broiler chicken
flocks does not usually appear until 2 weeks or more
after hatching. This is taken to indicate horizontal
transmission of Campylobacter from the environ-
ment either within or outside the broiler house.
Thus there is the possibility of preventing coloniza-
tion, or at least extending the Campylobacter-free
period, by improving hygienic practice among
broiler-house attendants and proofing houses against
intrusion by birds and rodents. Such interventions
have met with partial success, notably in Scandinavia
and The Netherlands.
0031In some cases water has been shown to be a crucial
factor in promoting colonization. Many broiler
houses are served by unchlorinated private borehole
supplies that are suspect. Even in mains-supplied
houses Campylobacter can become established in dis-
tribution systems beyond header tanks. Experimental
interventions, in which header tanks and distribution
pipework have been thoroughly cleaned and disin-
fected, have been followed by dramatic falls in colon-
ization rates in the broilers. Unfortunately such
measures are difficult to sustain under agricultural
conditions and further research is needed.
0032It is generally believed that, unlike Salmonella in-
fection, vertical transmission of Campylobacter from
parent flocks does not occur. This view has been
challenged by the results of a 5-year study in the
UK, in which the distribution of C. jejuni serotypes
in broiler flocks supplied with day-old chicks from
two hatcheries pointed to vertical rather than
horizontal transmission. C. jejuni readily survives in
embryonated eggs. If vertical transmission is con-
firmed, there is the possibility of preventing Cam-
pylobacter colonization of broilers by ensuring that
breeder flocks are kept free from infection.
0033The principle of competitive exclusion, in which
normal intestinal flora is artificially established in
newly hatched chicks in order to exclude pathogens
such as Salmonella, is not applicable to Campylo-
bacter control, as the intestinal flora has already
become established by the time Campylobacter
CAMPYLOBACTER
/Campylobacteriosis 793

make their appearance. An experimental oral vaccine
has been used with some success in broiler chicken
flocks. This is a sound approach that could have
major benefit.
0034 The total elimination of Campylobacter from
broiler flocks is probably not practicable, but redu-
cing the extent of colonization may be sufficient to
curtail transmission to the human population. The
logistics, precise methods, and costs of such measures
have yet to be worked out, but they are urgently
needed if there is to be any hope of reducing the
present unacceptable burden of the disease. These
measures need to be studied in relation to the prob-
lems of cross-contamination during the mechanical
processing of poultry, which are discussed elsewhere
(See Campylobacter: Properties and Occurrence.)
0035 Terminal irradiation of dressed poultry is an option
that removes all pathogens, including Campylo-
bacter, but there are problems with this, not least
public acceptability. (See Irradiation of Foods: Basic
Principles.)
0036 Waste disposal from poultry farms An added ad-
vantage of controlling Campylobacter colonization
of poultry is that fewer bacteria would be returned
to the environment and to surface waters. Heavily
colonized flocks have a prodigious output of Cam-
pylobacter that are likely to be recycled in farm
stock via surface water and wild or feral animals
that are closely associated with farms, such as
magpies, jackdaws, starlings, pigeons, sparrows,
rats, and mice. Cattle with access to surface water
are commonly colonized, whereas those with access
only to mains water have been found to be free of
Campylobacter.
Public Education
0037 It has been said that if everyone handled their foods
properly, foodborne Campylobacter enteritis would
virtually disappear. This is probably true, but it is an
unrealistic expectation. Yet much could be done to
improve matters. Surveys to assess public knowledge
of the rudiments of food hygiene have revealed abys-
mal ignorance. It should not be difficult to remedy
this. Even to impart the simplest facts about handling
poultry could have an impact that far outweighs the
effort – and it would help control salmonellosis as
well as Campylobacter enteritis. Television is the
most influential medium and a substantial impact
could be made by broadcasting high-quality enter-
taining yet informative spot ‘advertisements.’
The understandable fears of the poultry and retail
industries could be allayed by inviting their participa-
tion and ensuring that the content of such spots
was sensibly balanced. With appropriate professional
skills, it could even be turned to their advantage.
Public moneys used to fund such a venture should
be amply offset by the savings from infections
prevented.
See also: Campylobacter: Properties and Occurrence;
Irradiation of Foods: Basic Principles; Poultry: Chicken;
Water Supplies: Water Treatment
Further Reading
Advisory Committee on the Microbiological Safety of Food
(1999) Report on Microbial Antibiotic Resistance in
Relation to Food Safety. London: Stationery Office.
Humphrey TJ (1989) Salmonella, campylobacter and
poultry: possible control measures. Abstracts on
Hygiene and communicable diseases 64: R1–R8.
Lastovica AL and Skirrow MB (2000) Clinical significance
of Campylobacter and related species other than Cam-
pylobacter jejuni. In: Nachamkin I and Blaser MJ (eds)
Campylobacter, 2nd edn, pp. 89–120. Washington,
DC:American Society for Microbiology.
Nachamkin I, Mishu Allos B and Ho TW (2000) Campylo-
bacter jejuni infection and the association with Guillain–
Barre
´
syndrome. In: Nachamkin I and Blaser MJ (eds)
Campylobacter, 2nd edn, pp. 155–175. Washington,
DC: American Society for Microbiology.
Newell DG and Wagenaar JA (2000) Poultry infections and
their control at farm level. In: Nachamkin I and Blaser
MJ (eds) Campylobacter, 2nd edn, pp. 497–509. Wash-
ington, DC: American Society for Microbiology.
Piddock LJV (1995) Quinolone resistance and Campylo-
bacter spp. Journal of Antimicrobial Chemotherapy 36:
891–898.
Ransom GM, Kaplan B, McNamara AM and Wachsmuth
IK Campylobacter prevention and control: the USDA-
Food Safety and Inspection Service role and new food
safety approaches. In: Nachamkin I and Blaser MJ (eds)
Campylobacter, 2nd edn, pp. 511–528. Washington,
DC: American Society for Microbiology.
Rice BE, Rollins DM, Mallinson ET, Carr L and Joseph FW
(2000) Campylobacter jejuni in broiler chickens: colon-
ization and humoral immunity following oral vaccin-
ation and experimental infection. Vaccine 15: 1922–
1932.
Skirrow MB and Blaser MJ (2000) Clinical aspects of Cam-
pylobacter infection. In: Nachamkin I and Blaser MJ
(eds) Campylobacter, 2nd edn, pp. 69–88. Washington,
DC: American Society for Microbiology.
Smith KE, Bender JB and Osterholm MT (2000) Antimi-
crobial resistance in animals and relevance to human
infections. In: Nachamkin I and Blaser MJ (eds) Cam-
pylobacter, 2nd edn, pp. 483–495. Washington, DC:A-
merican Society for Microbiology.
Van de Giessen AW, Tilburg JJHC, Ritmeester WS and van
der Plas J (1998) Reduction of campylobacter infections
in broiler flocks by application of hygiene measures.
Epidemiology and Infection 121: 57–66.
794
CAMPYLOBACTER
/Campylobacteriosis
Wassenaar TM and Blaser MJ (1999) Pathophysiology of
Campylobacter jejuni infections in humans. Microbes
and Infection 1: 1023–1033.
Yang S, Leff MG, McTague D et al. (1998) Multistate
surveillance for food-handling, preparation, and
consumption behaviors associated with foodborne
diseases: 1995 and 1996 BRFSS food-safety questions.
Morbidity and Mortality Weekly Report 47: 33–56.
CANCER
Contents
Epidemiology
Carcinogens in the Food Chain
Diet in Cancer Prevention
Diet in Cancer Treatment
Epidemiology
A Trichopoulou and P Lagiou, University of Athens
Medical School, Goudi, Athens, Greece
D Trichopoulos, Harvard School of Public Health,
Boston, MA, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Nutritional Epidemiology of Cancer
Methodological Complexities
0001 Epidemiological studies exploring the role of diet in
the etiology of cancer have several methodological
complexities, which may be classified into partially
overlapping categories as follows:
.
0002 Instruments for ascertainment of past diet are
inherently weak; therefore, random misclassifi-
cation of dietary factors of causal importance
may be extensive, leading to substantial underesti-
mation of genuine effects and to false-negative
results.
.
0003 Random misclassification may be so extensive as to
substantially reduce the power of a study, to the
extent that an apparently positive result may be as
likely to reflect a statistical artefact (alpha error) as
a biologically genuine association.
.
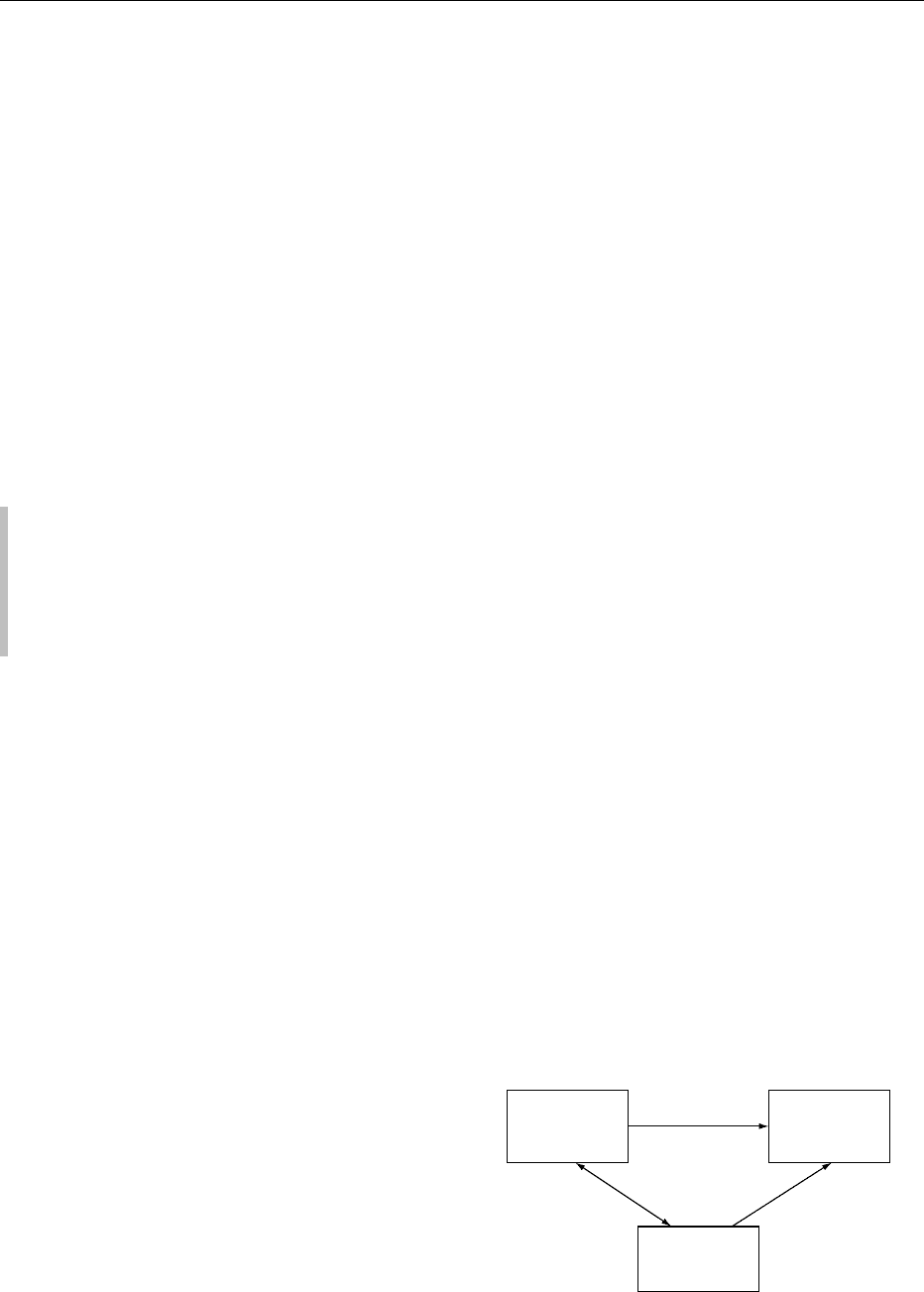
0004 Mutual confounding among nutritional factors is
extensive and complex, because there are many
nutritional factors, and many of them have a
common dietary origin (Figure 1).
.
0005 Random misclassification of nutritional factors
may substantially reduce the ability to control
their confounding influences.
.
0006Most nutritional factors implicated in human
carcinogenesis are considered to be late-stage
agents (promoters or growth enhancers) rather
than early stage agents (initiators). All of them,
however, have their own specific latent periods.
This poses theoretical and practical difficulties
in the definition of a common latency when the
effect of more than one nutritional factors are
considered in relation to a specific cancer in any
particular study.
.
0007The exposure–response curve describing cancer
risk in relation to a particular nutritional variable
may be sigmoid, implying the existence of thresh-
olds below or above which no association could be
documented between the two variables.
.
0008When a particular cancer has several independently
operating nutritional causes, the relative risk
associated with any particular nutritional cause
decreases with the prevalence or the abundance of
the other nutritional causes.
.
0009On the contrary, when two factors are jointly ne-
cessary for the causation of a particular cancer, for
example, an unknown initiator and a particular
Exposure
e.g. high intake
of red meat
Outcome
e.g. colorectal
cancer
Confounder
e.g. low intake
of vegetables
increases risk
increases
risk
fig0001Figure 1 Confounding.
CANCER/Epidemiology 795