Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


illness with symptoms similar to those of staphylo-
coccal food poisoning are reported to the CDC, but
are not classified because of inadequate information
about the presence of staphylococci or enterotoxin in
the foods involved. (See Food Poisoning: Tracing
Origins and Testing.)
0002 Staphylococcal foodborne outbreaks vary in size,
and can involve one or two persons to as many as
over 1000 people. One outbreak in the USA involved
1300 people attending a picnic in Indiana. Baked ham
was the implicated food. An even larger outbreak
occurred in Japan, involving 1500 people who
became ill from eating contaminated rice balls con-
tained in lunch boxes prepared at one location. (See
Food Poisoning: Statistics.)
Symptoms of the Disease
0003 The major symptoms of staphylococcal food
poisoning, i.e., vomiting and diarrhea, occur within
1–6 h after ingestion of food containing enterotoxin.
A representative set of symptoms observed in 122
cases of illness that occurred among high-school
students after they had eaten cream puffs is given
in Table 1.
0004 Ninety-five (57%) of the 165 students who ate the
cream puffs became ill, whereas none of those who
did not eat them became ill. This is typical of out-
breaks involving a large number of people. The aver-
age onset time in the outbreak was also normal for
large outbreaks, with a few having earlier onset times,
usually because of consumption of large amounts of
toxin or increased sensitivity of some individuals, and
a few that have delayed onset times of 7–8 h. Al-
though vomiting is the symptom most frequently ob-
served, some individuals may have other symptoms,
such as diarrhea without vomiting. Diarrhea may
not be observed in milder cases, whereas vomiting
usually is. Changes in temperature and blood pressure
are not common, particularly with milder cases,
although it is known that in experimental cases a
change in temperature can occur, either up or
down; a drastic lowering of blood pressure may also
occur.
0005Death is uncommon with this type of food
poisoning, but deaths have occurred in children or
older individuals, often with other complications.
Two children, 3 and 4 years of age, died within 24 h
after each drank 125 ml of milk from a goat with
staphylococcal mastitis. The deaths of the children
and the results of the autopsy indicated that the chil-
dren received a relatively large amount of enterotoxin
in the milk they drank.
0006Several deaths of older people who consumed food
containing enterotoxin have been reported; the deaths
usually occurred after severe vomiting and diarrhea.
One elderly woman died of acute vascular collapse
secondary to fulminating gastroenteritis in an out-
break of staphylococcal food poisoning after eating
baked ham. Of 28 other people who were known
to have become ill with symptoms characterized
by vomiting, diarrhea, and severe prostration, six
individuals required hospitalization.
0007A 57-year-old woman reportedly in excellent
health died of shock within a few hours of the onset
of illness after eating a cold plate lunch at a restaur-
ant. Three other individuals developed severe gastro-
enteritis after eating plate lunches at the same
restaurant.
Requirements Necessary for Food
Poisoning
0008Certain conditions are necessary for staphylococcal
food poisoning to occur: (1) the food must be a good
medium for the growth of staphylococci and the pro-
duction of enterotoxin; (2) enterotoxigenic staphylo-
cocci must be present in the food; (3) the food must be
held at a warm temperature for several hours for
the staphylococci to grow to sufficient numbers to
produce enterotoxin.
Foods Involved in Outbreaks
0009A variety of foods can support growth of enterotoxi-
genic staphylococci. Foods involved in outbreaks are
usually rich in protein, and include meat and meat
products, poultry, milk and dairy products, salads
(tuna, chicken, ham, and potato), custards, pudding,
and cream-filled bakery products. (See Cream: Types
of Cream; Milk: Processing of Liquid Milk; Poultry:
Chicken; Ducks and Geese; Turkey.)
tbl0001 Table 1 Symptoms of staphylococcal food poisoning from 122
cases
a
Symptom Reaction
Cases
b
None Mild Severe
Vomiting 122 15 12 95
Pains in abdomen 122 6 40 76
Diarrhea 103 13 75 15
Headache 101 29 59 13
Muscular cramping 113 41 58 14
a
Includes 94 students, eight lunchroom supervisors who took cream puffs
home, and 20 cases resulting from the consumption of cream puffs sold at
three cafe
´
s and from a bakery truck.
b
Cases from which this information was available.
Data from Dennison GA (1936) Epidemiology and symptomatology of a
Staphylococcus food poisoning. American Journal of Public Health 26:
1168–1175.
STAPHYLOCOCCUS
/Food Poisoning 5557

Source of Contamination
0010 Staphylococci can be found in most raw foods. How-
ever, the most frequent source of contamination of
foods implicated in staphylococcal food-poisoning
outbreaks is the food handler. Most foods involved
in such incidents are cooked, and are recontaminated
in the final preparation for serving. A food handler
with any type of staphylococcal infection or one who
is carrying the organism in his or her nose is a likely
source of contamination.
0011 An outbreak occurred in California in 1983 involv-
ing several hundred children in an Easter-egg hunt.
The source of the contamination was an infected
lesion on the hands of the person who prepared the
eggs. Another outbreak involved packaged sliced ham
that was contaminated with staphylococci from the
nose of the person who packaged it. The ham was
packaged on a Saturday morning and sold through-
out the day without any of the consumers getting sick.
The unsold ham was stored in a relatively deep pan
and refrigerated overnight. Cooling might have been
quite slow because of the size of the pan. On Sunday
morning, the ham was warmed before being sold
around 11:00 a.m. People who bought the ham
on Sunday became ill with staphylococcal food
poisoning. Enterotoxin A (SEA) was isolated from
the leftover ham.
0012 Animals carry staphylococci in their noses and cer-
tain animal diseases, such as mastitis, are caused by
staphylococci. However, animals are less important
sources of contamination because, even though raw
meats and milk are usually contaminated with
staphylococci, cooking and pasteurization tempera-
tures will destroy the organisms. In addition, the
presence of other competing microorganisms in the
raw foods inhibits staphylococcal growth. An excep-
tion is when staphylococci are present in much higher
numbers than other organisms, as in the case of milk
from a mastitic animal, e.g., the two children who
died after drinking milk from a goat with mastitis.
0013 Equipment can sometimes be a source of contamin-
ation. An outbreak associated with baked ham
resulted from contamination of the ham with the
meat slicer. The same strain of enterotoxigenic
S. aureus was isolated from both the ham and the slicer.
Conditions Necessary for Growth and
Toxin Production
0014 In order for food poisoning to occur, the food con-
taining an enterotoxigenic staphylococcal strain must
be held at a warm temperature, usually room tem-
perature or above, for several hours (at least 4 h) for
the staphylococci to grow to sufficient numbers to
produce enterotoxin. Growth of staphylococci to a
population of 1 million or more organisms per gram
of food is assumed necessary to produce enough
enterotoxin to cause illness.
0015Care needs to be taken in interpreting the signifi-
cance of staphylococcal numbers in food when inves-
tigating an outbreak. Not all staphylococcal strains
produce enterotoxin. A large number of staphylo-
cocci in a food may indicate poor hygienic practices
but, to incriminate a food definitely as the cause of
food poisoning, it is necessary to demonstrate that the
staphylococcal isolate produces enterotoxin. Alterna-
tively, the lack of staphylococci or the presence of low
numbers does not indicate the absence of enterotoxin
in the suspect food. This is especially important in the
case of heat-processed foods. Absence of viable
staphylococci does not necessarily indicate a safe
product because preformed enterotoxin may not be
inactivated.
0016Data from outbreaks indicate that less than 1 mgof
SEA can result in illness. In a chocolate milk outbreak
in 1985, it was found that 100–200 ng of SEA was
sufficient to cause staphylococcal food poisoning in
children. SEA is the most toxic enterotoxin and the
one most commonly involved in staphylococcal food-
poisoning outbreaks.
Site of Action
Emetic Action
0017The site of the emetic action of enterotoxin in the
monkey is in the abdominal viscera, with the sensory
stimulus for emesis reaching the vomiting center of
the brain via the vagus and sympathetic nerves. This
is supported by experiments in which transthoracic
vagotomy partially protected the monkey from the
emetic action of enterotoxin given intragastrically
and, when coupled with abdominal sympathectomy,
the monkey was completely resistant to the emetic
action of enterotoxin. The monkeys with deafferen-
tated abdominal viscera still vomited as normal
animals when the emetic compound, Veriloid, was
administered. Bilateral destruction of the area post-
rema on the floor of the fourth ventricle (chemorecep-
tor trigger zone) made the monkeys completely
refractory to the emetic action of enterotoxin given
intravenously or intragastrically.
0018Attempts to determine the site of action of entero-
toxin in the intestinal tract have been unsuccessful.
Specific binding of enterotoxin to cells closely related
to intestinal epithelial cells that have been cited as
potential target cells for direct cytopathic effects of
the staphylococcal enterotoxins was not detectable.
Binding of SEA in the rat intestinal tract was not
5558
STAPHYLOCOCCUS
/Food Poisoning

detectable, but rather the enterotoxin passed through
the gastrointestinal mucous membrane within 15 min
after administration and was detected in the kidney.
Neuronal binding of SEA in the intestinal tract was
not demonstrated; this binding might have been
expected based on the finding that the sensory stimu-
lus for vomiting reaches the vomiting center by way
of the vagus and sympathetic nerves.
Diarrheal Action
0019 Diarrhea is the second most common symptom seen
in staphylococcal food poisoning. In outbreaks in-
volving a large number of people, as many individuals
develop diarrhea as have an emetic reaction. Stimula-
tion of this reaction is not understood because the
mechanism of action is apparently quite different
from that of the so-called diarrheal diseases such as
cholera and Clostridium perfringens and Bacillus
cereus food poisoning. The toxins responsible for
the diarrheal diseases elicit an ileal loop reaction in
rabbits, whereas the staphylococcal enterotoxins do
not. Enterotoxin B (SEB) had no effect on the absorp-
tive mechanism of the rat small intestine, but the
enterotoxin somehow triggered a secretory mechan-
ism that resulted in a net secretion of fluids. The
actual mechanism responsible for stimulating excre-
tion has not been elucidated. (See Bacillus: Food
Poisoning; Clostridium: Food Poisoning by Clostri-
dium perfringens.)
Enteritis
0020 Enteritis is another effect of enterotoxins taken orally,
but it is not easily observed except by special examin-
ation. Pseudomembranous enterocolitis was observed
to be associated with staphylococcal infections in
patients who had been administered antibiotics to
control infection during surgery. Many of these pa-
tients died before the cause of their illness was diag-
nosed. The staphylococci had become resistant to the
antibiotics used and grew prolifically in the intestinal
tracts of these patients because the normal flora had
been eliminated by the antibiotics. These staphylo-
cocci were potent producers of enterotoxin, later
identified as SEA and SEB. Experiments in animals
with SEB revealed that enteritis can be produced in
monkeys, dogs, and chinchillas, with the severity of
enteritis depending on the amount of enterotoxin
given intragastrically. Autopsy of dogs 24 h after
ingesting SEB revealed acute enteritis with edema,
hyperemia, and ulcerations of the mucosa, and
destruction of the surface of the epithelium. Severe
round cell infiltration of the mucosa and destruction
of the surface of the epithelium were observed
by microscopic examination. These observations in
animals were similar to changes characteristic of
acute exogenous gastritis in humans resulting from
staphylococcal food poisoning. These findings, deter-
mined by gastroscopic examination, include patchy
mucosal hyperemia, regional edema, muscular irrita-
tion, erosions, petechiae and purulent exudate.
Examination 48 h later revealed the stomachs had
returned to normal. Acute gastroenteritis was ob-
served in monkeys 2 h after intragastric administra-
tion of SEB, with the most severe changes occurring at
4–8 h postinoculation. The mucosa was again normal
after 72 h postinoculation.
Death
0021Death is uncommon in staphylococcal food poisoning,
hence there is little opportunity to observe the patho-
logical effects of enterotoxin. However, autopsy of
the two children who died after drinking milk from
a mastitic goat revealed a moderate amount of pul-
monary edema marked with congestion of the alveo-
lar vessels and, in a few areas, there appeared to be
hemorrhages into the alveolae. There was a small
amount of leukocytic infiltration in the periportal
areas of the liver. These findings are similar to those
observed in monkeys that received a lethal dose of
enterotoxins by intravenous injection; in these animals
there was a decrease in intravascular fluid volume
with an increase in lung weight. The fluid was con-
fined to the perivascular and peribronchial interstitial
space; the lymphatics in these areas were gorged. The
primary pathological change was degeneration and
necrosis of capillary endothelial cells, with some but
less frequent damage to the endothelium of venules.
Also noted were interstitial hemorrhage and edema, a
histolytic infiltrate, and a striking herniation of capil-
lary endothelium into the vascular lumen. Apparently
these changes were brought about by the enterotoxin
binding to leukocytes with subsequent sequestering of
toxin-bound leukocytes in the lungs.
Treatment and Course of Illness
0022The rapid development of the illness makes it impos-
sible to prevent the symptoms from developing after
the enterotoxin has been ingested; once the symptoms
have occurred there is no treatment that will counter-
act them. In most cases recovery is within a few hours
and no treatment is necessary; however, in severe
cases where vomiting and diarrhea are excessive,
treatment intravenously with fluids is beneficial,
particularly to restore the salt balance.
0023A misunderstanding of the disease by the medical
attendant can lead to unfortunate results. Such was
the case when a young man afflicted with the illness
was given antibiotics, with death as a result. If the
disease was due to the ingestion of the organisms,
STAPHYLOCOCCUS
/Food Poisoning 5559

treatment with the proper antibiotic may be desirable
but, because it is due to a toxin, antibiotic treatment
is of no benefit. However, it could have an adverse
effect, particularly if the staphylococci were resistant
to the antibiotic. In this case the natural flora of the
intestinal tract would be eliminated and this would
allow the staphylococci to grow uninhibited and pro-
duce enterotoxin. Staphylococci are not good com-
petitors and usually do not grow in the intestinal tract
in the presence of the natural flora.
Prevention
Temperature Control
0024 Most staphylococcal food-poisoning outbreaks could
be prevented if proper temperature controls were
observed during holding of the food after its prepar-
ation and before being served. One method is proper
refrigeration of susceptible foods after they are pre-
pared. The lower the temperature, the slower the
growth of the staphylococci, with little or no growth
at refrigeration temperatures. An excellent example
of the effect of refrigeration is an outbreak from
cream-filled coffee cake that occurred in Wisconsin
in 1970. Approximately 50 people became ill after
eating the cake, with differing severity of symptoms,
depending on the length of time the cakes stood
unrefrigerated before being eaten. The cakes were
made by a bakery and delivered to several stores at
5:30 a.m. on a warm Saturday morning; the cakes
were not refrigerated at the stores. Purchases were
made all day Saturday and on Sunday morning.
Many who bought the cakes on Saturday did not eat
them until Sunday morning, but in most cases the
cakes were refrigerated by the purchasers. Most of
those who bought the cakes early Saturday morning
and refrigerated them did not become ill. No one who
ate cakes purchased at the bakery became ill because
the cakes were refrigerated at the bakery. The source
of the staphylococci was from the throat of the food
handler who had placed the cream filling into the
cakes with his hand. The organisms isolated from
his throat and the cakes produced enterotoxin E; not
many staphylococci produce this enterotoxin and its
involvement in food poisoning is rare.
0025 Some of the largest outbreaks of staphylococcal
food poisoning have occurred at picnics, a number
of these from baked ham sandwiches. Baked ham is
an excellent medium for the growth of staphylococci,
which is not always appreciated because it is a cooked
food. However, if the ham is recontaminated after
the baking, the results can be tragic. Providing
refrigeration for such a large quantity of food is diffi-
cult at a large picnic and normally the food will be at
the picnic for a number of hours before being con-
sumed. In cases such as this, every effort should be
made to provide refrigeration for the food at the
picnic grounds or not to transport it to the grounds
until shortly before it is to be served. (See Pork.)
0026One error that is frequently made is to place the
food in large containers to conserve space before it is
placed in the refrigerator. Under these conditions,
cooling is very slow and allows sufficient time for
the staphylococci to grow and produce enterotoxin.
A staphylococcal food-poisoning outbreak, in which
104 of 231 inmates in a country jail in New York
became ill, resulted from inadequate refrigeration of
macaroni salad. It had been prepared the day before it
was served and had been stored overnight in two
large, deep containers in a walk-in cooler. Isolation
of over 10
7
staphylococci per gram from the maca-
roni salad indicated inadequate cooling.
Food-Handling Practices
0027In the New York jail outbreak described in the previ-
ous section, it was ascertained that the food was
prepared by inmates who were inadequately trained
and not well supervised. Many food-poisoning out-
breaks are a result of inadequate training and super-
vision of the individuals preparing the food. The
major conclusion from both the First and Second
National Conferences for Food Protection held in
Denver, Colorado, in 1971 and in Washington, DC,
in 1984 was the need to educate the food handler as
well as the consumer on food safety. Unfortunately,
very little has been done in this area.
Food-Handler’s Infections
0028One method of preventing staphylococcal food-
poisoning outbreaks is to prohibit food handlers
with infections from handling foods. In some coun-
tries food handlers who are staphylococcal carriers
are not allowed to handle foods as long as they are
carriers. In the UK an assistant cook, who carried the
same staphylococcal organism in her nose as the one
isolated from lemon snow pudding involved in the
illness of six adults and 101 children in a primary
school, was excluded from work until the organisms
were eradicated by treatment with gentamicin cream.
The pudding contained large numbers of staphylo-
cocci (1.5 10
8
g
1
) that produced SEA and entero-
toxin D, as did the staphylococci isolated from the
nose of the assistant cook. Although it was feasible to
exclude the cook in this case, usually it is difficult and
impractical to bar workers who are carriers of
staphylococci in their noses or throats from handling
foods because approximately 50% of the population
are carriers. On the other hand, food handlers with
5560
STAPHYLOCOCCUS
/Food Poisoning

any type of infection should not be permitted to
handle foods, particularly if the food is for mass
feeding. The only viable solutions to this problem
are proper refrigeration of vulnerable foods between
preparation and consumption, or maintaining the
temperature above 45
C.
See also: Bacillus: Food Poisoning; Cadmium:
Toxicology; Clostridium: Food Poisoning by Clostridium
perfringens; Cream: Types of Cream; Food Poisoning:
Tracing Origins and Testing; Statistics; Milk: Processing
of Liquid Milk; Poultry: Chicken; Ducks and Geese;
Turkey
Further Reading
Bergdoll MS (1979) Staphylococcal intoxications. In: Rie-
mann H and Bryan FL (eds) Food-Borne Infections and
Intoxications, pp. 443–494. New York: Academic Press.
Bergdoll MS (1983) Enterotoxins. In: Adlam C and Easmon
CSF (eds) Staphylococci and Staphylococcal Infections,
vol. 2, pp. 559–597. London: Academic Press.
Bergdoll MS (1989) Staphylococcus aureus. In: Doyle MP
(ed.) Foodborne Bacterial Pathogens, pp. 463–523. New
York: Marcel Decker.
Dack GM (1956) Staphylococcus food poisoning. In: Dack
GM (ed.) Food Poisoning, 3rd edn. Chicago: University
of Chicago Press.
STARCH
Contents
Structure, Properties, and Determination
Sources and Processing
Functional Properties
Modified Starches
Resistant Starch
Structure, Properties, and
Determination
D S Jackson, University of Nebraska, Lincoln, NE, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Starch Structure
Amylose and Amylopectin Polymers
0001 Starch is a mixture of two glucose polymers. These
polymers are initially enclosed within a semicrystal-
line granule formed inside starch-synthesizing plant
organelles. Amylopectin, the larger of the polymers,
is an alpha-1, 4-linked, alpha-1,6-branched (4–6%
branching) polymer with an average molecular
weight near 10
8
. Amylose, a smaller, mostly linear
polymer, is also composed of alpha-1,4-linked glu-
cose units; long chains are sometimes connected
with alpha-1,6 branches, although branching
probably accounts for < 1 % of the glucose unit con-
nections. The molecular weight of amylose is ap-
proximately 10
5
. The molecular weight of starch
polymers varies depending upon its plant source.
Amylopectins have been reported to vary from
50 10
6
to 500 10
6
, and amyloses from 1600 to
1 10
6
. The degree of branching also varies.
Common starches typically have 25–35% amylose
and 65–75% amylopectin.
Genetic Differences
0002Several genetically modified starches are available.
The most common forms are the waxy starches
and the high-amylose starches. Waxy starch, which
contains 100% amylopectin, is found in grains
(i.e.,maize, sorghum, and wheat) that have three
recessive waxy genes. Combinations of recessive
(wx) and dominant (Wx) waxy genes result in
starches with varying percentages of amylopectin
from 75 (WxWxWx) to nearly 100% (wxwxwx).
High-amylose (ae) starches are available with ap-
proximately 53 or 70% amylose.
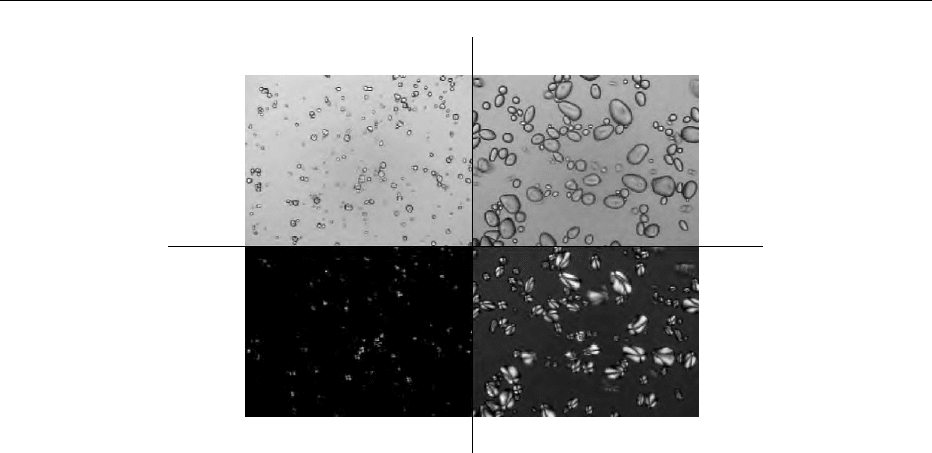
Microscopy of Granules
0003Starch granules have unique microscopic structures
(Figures 1 and 2), and the source of starch can
frequently be determined by a trained observer. The
shape and size of starch granules differ according to
the botanical source and the environmental condition
under which a crop was grown. Typically, rice and
maize starch have angular (polyhedral) granules;
potato starch has oval-shaped granules. Wheat starch
STARCH/Structure, Properties, and Determination 5561
consists of spherical and flat circular (lens)-shaped
granules. Sizes also vary widely. Rice starch granules
are very small (6 mm diameter), while potato starch
granules can exceed 100 mm. The mean diameter of
maize starch granules is 35 mm; wheat starch has a
bimodal distribution of granular sizes – small (B)
granules average 4 mm, while the large (A) granules
average 14 mm. Granules can also have compound
structures (i.e., oats, rice) which appear as separate
starch grains in a single amyloplast enclosure.
0004 Several microscopic techniques have found wide-
spread use. When observed under polarized light,
undamaged starch granules (as defined by the reten-
tion of crystalline structure) exhibit a phenomenon
called birefringence (Figure 1). This birefringence is
the result of polarized light being bent as it traverses a
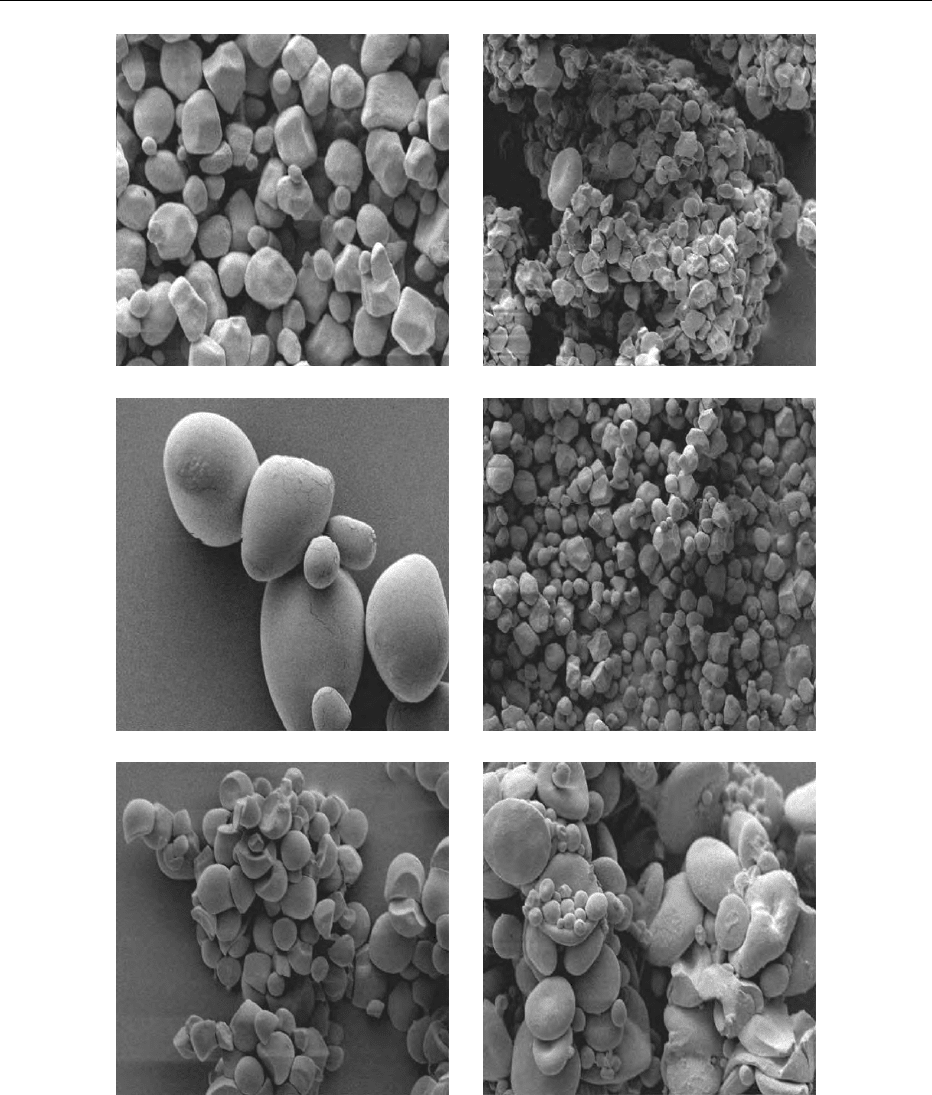
region of high molecular order. Scanning electron
microscopy (Figure 2), as well as other higher-
magnification techniques, have proven extremely
useful in identifying the three-dimensional structure
of starch granules, as well as showing the interrela-
tionships of starch granules and other chemical com-
ponents in cereal grains, tubers, and other food
systems.
Changes during Hydration and Heating
0005 Starch granules, when exposed to water, undergo
swelling and upon heating undergo a process of irre-
versible swelling and crystalline melting called gelat-
inization. If the crystalline region is destroyed,
granular birefringent properties disappear. The tem-
perature at which birefringence is lost has been de-
fined by some as the gelatinization point. Since loss of
crystallinity causes loss of birefringence, additional
thermal disruptions of the granule still occur after
the gelatinization point as defined using microscopy
techniques. When starch granules are exposed to
liquid water below 40–50
C, the amorphous gel-
like portions of the starch granule absorb water, caus-
ing the granule to swell. When the temperature is
>40–50
C, and water is in excess, granules begin to
undergo reversible swelling and around 60–80
C lose
birefringence and undergo irreversible swelling.
During the transition from reversible swelling to loss
of birefringence, the amorphous regions have a
rubber-like structure and the specific volume of the
amorphous areas increases, as does the mobility of
molecular segments which are thermally softened and
plasticized by water. At the gelatinization tempera-
ture, the mobility of molecules increases rapidly.
Granule components are in a more flowable state.
The mobility of molecules in the amorphous regions
and the mobility of molecular regions which traverse
both crystalline and amorphous regions cooperatively
contribute to intergranular stresses. The continued
hydration of amorphous areas places additional stress
on those molecular regions (including regions within
the same molecule) which have remained crystalline.
These molecular movements have a cooperative effect
on granule swelling and the overall melting of starch
crystallites.
Starch Sources: Grain and Tuber/Root Structure
0006The majority of starch in cereal grains is located in the
endosperm. Many grains can be referred to as having
‘soft or floury starch’ or ‘hard or vitreous starch.’
Corn
Normal
light
Polarized
light
Potato
fig0001 Figure 1 Light micrographs (100) of corn (left) and potato starch (right) shown using normal (top) and polarized (bottom) light
microscopy.
5562 STARCH/Structure, Properties, and Determination
There is little evidence that the molecular components
of their starches are any different. The packing of the
starch granules within a kernel, however, is different.
Floury maize kernels have less protein binding the
starch granules together, and starch granules within
more flinty maize kernels are encased more tightly
within a protein matrix. Cereal starch is obtained
via wet milling; after the endosperm is disrupted, the
starch is collected by washing and centrifugation.
0007Cassava root, from which tapioca starch is pro-
duced, typically contains 25% starch. The roots
have a hard or cork-like outer layer which is usually
(a) (b)
(c) (d)
(e) (f)
fig0002 Figure 2 Scanning electron micrographs (1000) of (a) corn, (b) oat, (c) potato, (d) rice, (e) tapioca, and (f) wheat starches.
STARCH/Structure, Properties, and Determination 5563
removed before starch processing. Starch is collected
by disrupting the cells, screening, and subsequent
collection by washing and centrifugation.
0008 Potatoes are also another important starch source;
they typically contain about 22% starch. Raw pota-
toes are ground to disrupt cell walls; the pulp is
washed, and screened. Starch is later collected via
centrifugation. Starch can also be obtained, as a by-
product, from commercial production of value-added
potato products such as french fries, instant potatoes
and potato chips (crisps).
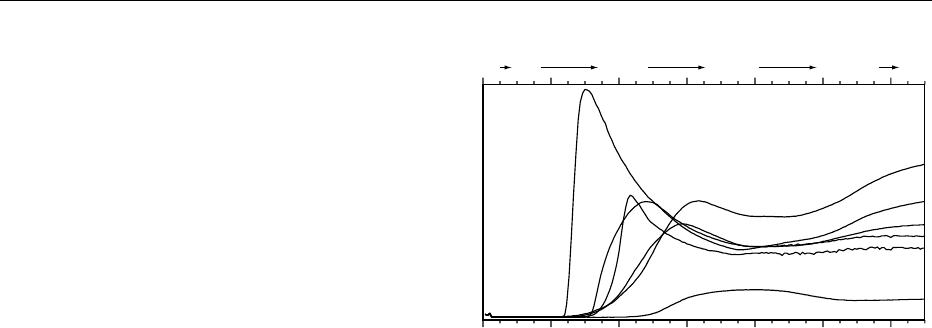
Viscosity Measures
Amylograph/Rapid Viscoanalyzer
0009 The viscosity of cooked starches is important to the
food industry. One of the most important industrial
measures of starch properties uses amylograph or
Rapid Viscoanalyzer (RVA) instruments to measure
a starch’s thermal behavior. In the standard amylo-
graph, a 3–5% starch dispersion is mixed in a cylin-
drical bowl. Paddles mix the starch dispersion, and
the force these paddles encounter is recorded with a
computer. The test begins with the gradual heating
(1.5
C min
1
) of the starch dispersion. The starch
granules swell and the viscosity of the mixture in-
creases as the temperature increases because the
swollen granules occupy more area within the mixing
vessel. When the temperature reaches 95
C, the
starch mixture continues to be stirred while the tem-
perature is maintained for 60 min. When swollen un-
modified granules are exposed to shear, the viscosity
of the mixture decreases because the granules break
apart into smaller pieces. After the holding cycle, the
starch is subsequently cooled to 50
C (also at 1–5
C
min
1
) and a highly viscous gel structure can form by
hydrogen binding and water entrapment between
starch polymers. The RVA is a similar device that
uses smaller sample sizes and has programmable
heating, cooling, and stir speeds (the manufacturers
of the amylograph also make a instrument suitable
for analyzing small amounts of starch). Typical RVA
curves are shown in Figure 3.
Chemical Methods
Determination of Total Starch
0010 There are several chemical methods available to
measure the total amount of starch in a sample. For
samples high in starch content (cereal grains, tubers,
and their products), starch’s optical rotation in solu-
tion can be determined using a polarimeter. Samples
are initially extracted with ethanol to remove
optically active soluble materials and the remaining
starch is suspended in a calcium chloride solution and
placed in a boiling water bath. Proteins are removed
in the procedure with stannic chloride-phosphotungs-
tic acid. The resulting filtered solution’s optical rota-
tion is measured in the polarimeter and used to
calculate percent starch; a similar optical procedure
uses hydrochloric acid and a saturated lead solution.
More recently developed methods of starch analysis,
however, usually rely on the ability of the enzymes
alpha-amylase and amyloglucosidase to degrade
cooked (or chemically treated) starch to glucose.
These methods often have the advantage of being
applicable to a wider range of starch-containing
products. For these procedures, it is usually essential
to gelatinize fully (cook/disperse) the starch. For
common materials without extensive resistant starch
(fiber-like starch), the sample can be gelatinized in an
autoclave. For more difficult-to-gelatinize samples,
starch can be dispersed in methyl sulfoxide (also
known as dimethyl sulfoxide or DMSO) prior to
enzymatic digestion.
0011After the starch is digested with enzymes to glu-
cose, most methods subsequently convert the glucose
solution into a colored product that can be measured
colorimetrically in a spectrophotometer. In fact, how-
ever, many of the glucose measurement techniques
can be used at this stage. The percentage of starch is
calculated by multiplying the measured amount of
glucose evolved from the enzymatic treatment. Total
glucose is multiplied by 0.9 to determine total starch;
this calculation accounts for the difference in molecu-
lar weight between individual glucose units and
glucose polymers. In addition to these chemical total
starch methods, indirect procedures using near
024681012
Time (min)
Temperature (⬚C)
5050 50 95 95 50
Potato
Wheat
Waxy corn
Corn
Rice
53% Amylose corn
fig0003Figure 3 Representative Rapid Viscoanalyzer curves for
potato, wheat, corn rice, waxy corn, and 53% amylose corn
starches.
5564 STARCH/Structure, Properties, and Determination
infrared spectroscopy (NIR) technology (especially
for grain/cereal crops) have proven to be very useful.
While NIR methods must rely on these chemical pro-
cedures for method development and subsequent ma-
chine calibration, when used appropriately they are
extremely rapid and can be performed by personnel
not necessarily trained in complex chemical analyses.
Determination of Percentage Amylose
0012 Since amylose and amylopectin have unique physical
and chemical properties, and their relative propor-
tions influence the overall properties of starches, the
determination of the ratio of these polymers becomes
important. Potentiometric titration is considered one
of the better techniques for determining the percent-
age of linear components (i.e., amylose) in starch. It
relies on the affinity between amylose and iodine.
Potato and wheat starches have typical iodine affin-
ities of approximately 19.9%, whereas maize starch
has an iodine affinity of 19.0%.
0013 Colorimetric tests for the percentage of amylose
are also widely used. Solutions of amylose and iodine
result in a deep blue-purple color. Amylopectin and
iodine show only a slight affinity towards each other;
their solutions have a reddish color. The blue value
test relies on these properties; starch samples are dis-
persed in a sodium hydroxide solution and, after
neutralization, the samples are allowed to react with
an iodine solution. The absorbance (usually at 620–
680 nm) of the solutions is measured to calculate blue
value, and the apparent percentage amylose content
can be determined by developing a blue value stand-
ard curve with ‘purified’ amylose. Unfortunately,
commercially available amyloses are usually not
exactingly pure, nor is such a pure amylose available
for every kind of starch. Accurate chemical determin-
ations of amylose content from different starch
sources is made more difficult because not only do
amyloses from different botanical sources have differ-
ent iodine affinities, but different amylopectins will
also bind a small amount of iodine and thus cannot be
discounted in amylose determinations. A newer pro-
cedure for amylose determination relies upon the
complexing action of concanavalin A (A) with amy-
lopectin. The procedures precipitate amylopectin
from starch solutions, leaving only amylose. The
amylose is thus subsequently analyzed in much the
same way as for total starch determinations.
Instrumental Methods
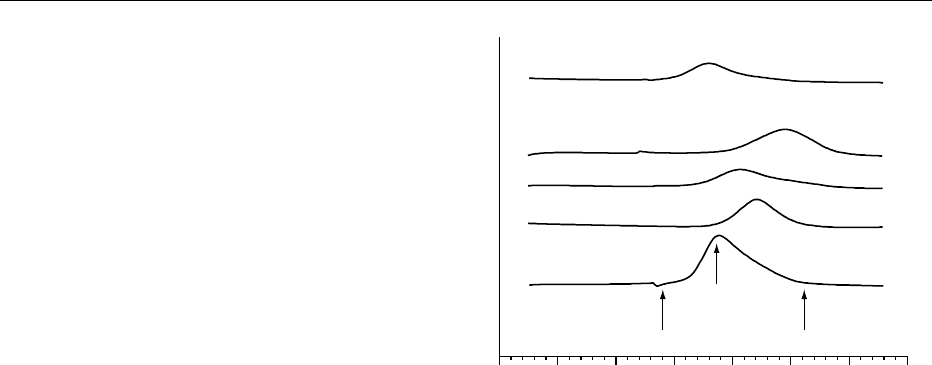
Differential Scanning Calorimetry
0014 The differential scanning calorimeter (DSC) is widely
used to determine the crystalline melting temperature
of various starches (Figure 4). Small samples of
starches are heated at a constant rate and the endo-
thermic heat flow is recorded. Melting of crystalline
sites (or some starch chemists postulate melting of
crystalline sites and unfolding of double helices)
results in a thermal event typically recorded as
an endotherm. Usually, a broad crystalline melting
range is recorded; sites of crystallinity melt at differ-
ent temperatures depending upon their individual
structure, the action of solvent (usually water), and
the interaction of individual polymers which are con-
tained and traverse crystalline sites. DSC can also be
used to examine the recrystallization of gelatinized
starches. Most notably, DSC is used to study the
retrogradation process under various environmental
conditions of time and temperature, and the inter-
actions of starch with complexing agents and crystal-
lization promoting or inhibiting ingredients.
X-Ray Analysis
0015X-ray analysis of starch is useful in determining the
extent of crystallinity and crystallite structure, the
botanical origin of starches, the formation of starch
complexes, and can be used in structural studies to
determine spacing within starch helices. Unlike DSC,
X-ray diffraction is less subject to scientific debate
regarding the ‘true’ measurement of starch crystallin-
ity. The diffraction patterns (groupings of spectral
lines) of native starches have been broadly classified
as A, B, C and V (Figure 5). Researchers have also
proposed variants on these patterns. Cereal grain
30 40 50 60 70 80 90 100
Temperature (⬚C)
Wheat
Waxy corn
Rice
Regular corn
Potato
End
Start
Gelatinization
temperature
fig0004Figure 4 Differential scanning calorimetry (DSC) endotherms
of wheat, waxy corn, rice, corn, and potato starches (scanned at
10
C min
1
, > 60% water). The figure shows the start of crystal-
line melting, point of maximum endothermic energy (gelatiniza-
tion temperature), and temperature at which all crystals have
melted.
STARCH/Structure, Properties, and Determination 5565
starches generally have the A pattern, although defat-
ted high-amylose starches have a B pattern. Bean and
cassava starches have a C pattern and potato starch
has a B pattern. Complexes between fatty acids and
amyloses, seen especially strongly in some high-
amylose maize starches, exhibit a characteristic V
pattern.
Chromatography
0016 Size exclusion chromatography has been important in
determining the fine structure of amylose and amylo-
pectin molecules, as well as the relative proportion of
those molecules in food materials. In addition, chro-
matographic techniques have proven useful in deter-
mining the relative solubility of starch polymers in
solution and the percentage of amylose in starches.
Chromatography can be conducted using conven-
tional gel filtration techniques (soft gels), or more
rapid high-performance liquid chromatography me-
thods with rigid stationary-phase material (Figure 6).
Starch samples are first dispersed (usually in methyl
sulfoxide, also known as DMSO, NaOH, or water)
and injected into a chromatographic system. The
amylopectin usually elutes at or extremely close to
the void volume of most modern column systems, and
the smaller amylose elutes later. The molecular
weight of these materials can be determined by
coupling the chromatographic system to a laser
light-scattering detector, or can be estimated by
employing known-molecular-weight standards of
pure carbohydrate polymers. The relative molecular
weights or sizes of starch polymers can be compared,
as well as the relative effect of various food-
processing unit operations on starch structure. The
extent of starch depolymerization caused by food or
industrial processing is also easily measured using
size exclusion liquid chromatography. Amylases
can be used, coupled with chromatography and
postchromatographic chemical analysis, to determine
the extent and length of polymer branches, and other
details about the fine structure of particular starches.
Nuclear Magnetic Resonance Spectroscopy
0017Nuclear magnetic resonance (NMR) is a powerful
tool that has been used to understand starch–water
interactions and the molecular relationship between
chemical groups in starch molecules. For example,
wide-line
1
H NMR has been used to characterize
the mobility of water associated with starch pre-,
post-, and during gelatinization; these results have
confirmed the notion that gelatinization is a melting
phenomenon. In addition, both
1
H and
13
C NMR
have been used to study the degree of branching
3 13182328
A (Corn)
B (Potato)
C (Bean)
V (Lipid complex)
2Θ
8
fig0005 Figure 5 X-ray diffraction patterns (40 kV, 30 mA, Cu K-alpha
radiation, 2-theta diffraction angle) of a lipid complexed corn
(V-pattern), bean (C-pattern), potato (B-pattern), and corn (A-
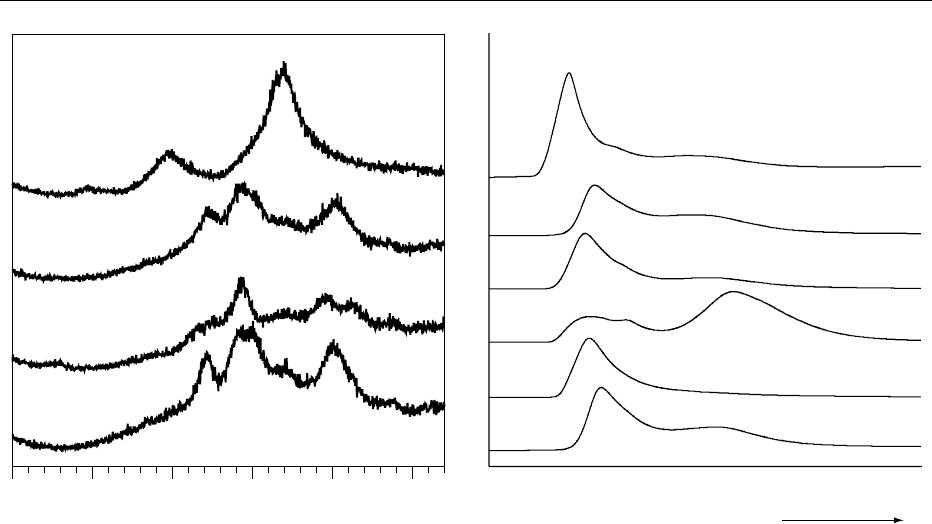
pattern) starches.
Potato
Wheat
Rice
70% Amylose
Waxy corn
Regular corn
Amylopectin
Amylose
Decreasing (log) molecular size
fig0006Figure 6 Typical high-performance size exclusion chromato-
grams (HPSEC) of potato, wheat, rice, 70% amylose, corn, waxy
corn, and corn starches. The figure shows amylopectin and
amylose peaks. Starch was dispersed in methyl sulfoxide
(DMSO) before injection into the HPSEC system consisting
of four columns linked in series. Carbohydrate was detected
using a refractive index detector.
5566 STARCH/Structure, Properties, and Determination