Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


Vanhoe H (1993) A review of the capabilities of ICP-MS for
trace element analysis in body fluids and tissues. Journal
of Trace Elements and Electrolytes in Health and
Disease 7: 131.
Wolfe WR, Holden JM and Schubert A (1992) Selenium
content of selected foods important for improved assess-
ment of dietary intake. Journal of Food Composition
and Analysis 5: 2.
Physiology
C D Thomson, University of Otago, Dunedin,
New Zealand
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Selenium first attracted attention in the 1930s as a
toxic trace element that caused ‘alkali disease’ in
livestock consuming high-selenium plants. In 1957,
selenium was shown to be essential for animals when
traces of this element prevented liver necrosis in vita-
min E-deficient rats, and later to prevent a variety of
economically important diseases such as white muscle
disease in cattle and sheep, hepatosis dietetica in
swine, and exudative diathesis in poultry. The dem-
onstration in 1973 of a biochemical function for
selenium as a constituent of the enzyme glutathione
peroxidase helped to explain the interrelationship
between selenium and vitamin E. The importance of
selenium in human nutrition was highlighted in
reports in 1979 of the selenium responsive condition,
Keshan disease in China, and selenium deficiency in a
patient on total parenteral nutrition in New Zealand.
Considerable research during the last two decades
has provided information on the molecular biology,
metabolism, and importance of selenium in human
nutrition, leading to a much greater understanding
of the functions of selenium and the establishment
of recommended dietary intakes.
Metabolism of Selenium
0002 Comparatively little is known about the forms of
selenium in foods. The major form in cereals and
other plants is selenomethionine, while the most
likely form in animal foods is selenocysteine, as this
is the active form in functional selenoproteins in the
mammalian body. Inorganic forms are often used
in experimental diets and as supplements, but the
extent of occurrence of inorganic or other forms
of selenium in foods is not clear. The metabolism of
selenium, including absorption, transport, distribu-
tion, excretion, retention, and transformation to
the active form, is very much dependent on the
chemical form and amount of selenium ingested,
and on interacting dietary factors. There is consider-
able species variation in many aspects of selenium
metabolism.
Absorption
0003Selenium is absorbed mainly from the duodenum.
Selenomethionine and methionine share the same
active transport mechanism, but little is known
about the transport of selenocysteine. Absorption of
inorganic forms of selenium such as selenite and
selenate is via a passive mechanism.
0004While the absorption of selenium is generally high
in humans, probably about 80% from food selenium,
selenomethionine appears to be better absorbed than
selenite. Absorption of selenium is unaffected by sel-
enium status, and there appears to be no homeostatic
regulation of absorption. Selenium is better absorbed
from a high-protein diet, and the absorption of sele-
nomethionine may be influenced by the methionine
content of the diet.
Bioavailability
0005As well as absorption, utilization of a nutrient may
also include transformation to a biochemically active
form, which, for selenium, is assessed from changes in
tissue glutathione peroxidase. Few studies have been
made in humans of the bioavailability of selenium,
but animal studies show a wide variation in the avail-
ability from different foods. In rats, the bioavailabil-
ity from mushrooms, tuna, wheat, beef kidney, and
Brazil nuts is 5, 57, 83, 97, and 124%, respectively, in
comparison with sodium selenite. In humans, the
bioavailability of selenium from fish is low in com-
parison with wheat. Human studies also show differ-
ences among various forms of selenium such as
selenate, wheat, and yeast, but this also depends
upon the criterion of measurement used for availabil-
ity, indicating the need to consider several variables,
including short-term changes in glutathione peroxid-
ase activity, long-term retention of tissue selenium,
and metabolic conversion to biologically active
forms.
Transport
0006Little is known about the transport of selenium in the
body, although it appears to be transported bound to
plasma proteins. A selenium-containing protein called
selenoprotein P, isolated from rat and human plasma,
SELENIUM/Physiology 5117
has been suggested as a transport protein, and plasma
also contains extracellular glutathione peroxidase,
but lower-molecular-weight forms of selenium are
more likely to act as transport proteins.
Metabolism and Distribution
0007 An outline of selenium metabolism is shown in
Figure 1. In animal tissues, selenium occurs in associ-
ation with protein, and is present in two main com-
partments or forms. The first is selenocysteine, which
is present as the active form of selenium in selenopro-
teins, including the selenoenzyme glutathione per-
oxidase. The second is selenomethionine, which is
incorporated in place of methionine in a variety of
proteins, unregulated by the selenium status of the
animal.
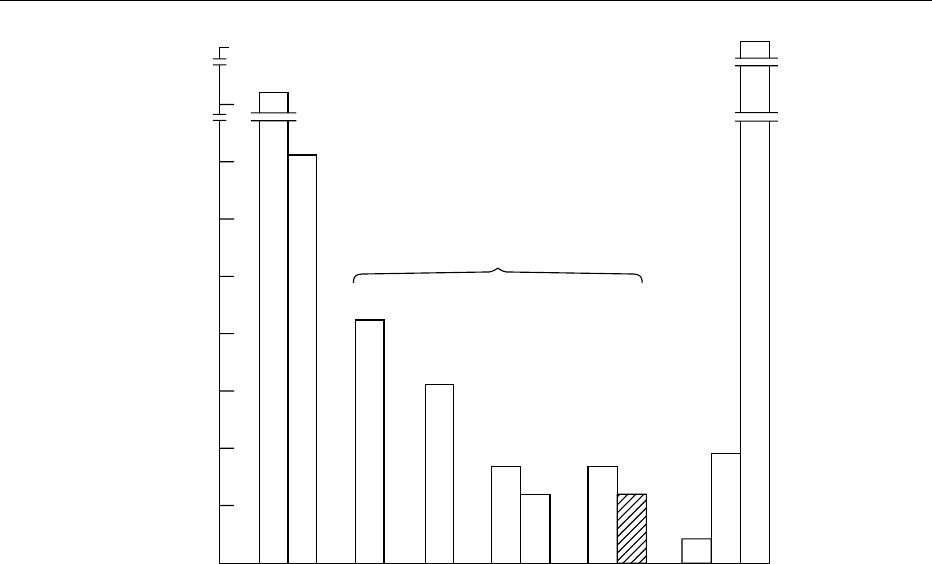
0008 Selenium levels in tissue are influenced by dietary
selenium intake; this is reflected in the wide variation
in blood selenium levels of residents of countries with
differing soil selenium levels (Figure 2). The total
amount of selenium in the body ranges from 3 to
20 mg, depending on intake of selenium. Retention
of selenium is also profoundly influenced by the form
administered, with selenomethionine being much
more effective in raising blood selenium levels than
sodium selenite or selenate. Selenomethonine appears
to follow the same metabolic pathway as methionine
and is incorporated nonspecifically into protein in its
place. This contributes to tissue selenium, where it
may in fact accumulate, but has no physiological
function and is not available for synthesis of func-
tional forms of selenium until it is catabolized. Selen-
ate is reduced to selenite, then selenide, and in this
oxidation state (2) is introduced into selenocysteine,
the active form of selenoproteins. The selenium from
inorganic selenium, or from catabolism of seleno-
methionine or selenocysteine, is incorporated into
selenocysteine, which enters regulated selenium
metabolism and is then incorporated into seleno-
proteins. Selenium intake from selenate, selenite, or
selenocysteine, unlike that from selenomethionine,
will be excreted in urine if in excess.
Incorporation of Selenium into Selenoproteins
0009All functional mammalian selenoproteins contain
selenocysteine at the active site. Selenium is incorpor-
ated by replacement of oxygen into serine to form
selenocysteine, while serine is attached to a unique
tRNA (transfer ribonucleic acid). Selenocysteine is
encoded by a unique stop codon UGA on the mRNA
specific for the selenoprotein. Regulation of seleno-
protein synthesis appears to be via individual mRNAs
(messenger RNAs) at the transcriptional or posttran-
scriptional levels in response to selenium availability,
as well factors such as the chemical form of selenium
and oxygen exposure. However, there is differential
depression of selenoprotein synthesis in response to
an inadequate selenium supply with preservation of
the metabolically most important proteins. This has
been termed the ‘hierarchy’ of importance of func-
tional selenoproteins.
Excretion
0010Urine is the principal route of excretion of selenium,
followed by feces, which mainly contain unabsorbed
selenium. Homeostasis of selenium is achieved by
regulation of its excretion. Daily urinary excretion
of selenium is closely associated with plasma selen-
ium and dietary selenium intake and has been used as
an indicator of selenium status. Balance studies show
Selenomethionine
in methionine pool
Selenium
metabolism
Excretory
metabolites in
urine, breath
Transport
form
Selenocysteine,
inorganic, other forms
Selenomethionine
Dietary selenium Tissue selenium
Selenomethionine in
tissue proteins
Selenocysteine in
glutahione peroxidase,
other selenoproteins
fig0001 Figure 1 Outline of selenium metabolism.
5118 SELENIUM/Physiology
that over a wide range of intakes, urinary excretion
accounts for 50–60% of the total amount excreted.
Measurement of the plasma renal clearance of selen-
ium, which expresses its rate of excretion in the urine
in terms of the amount contained in a unit volume of
plasma, shows that the kidneys of residents of the
low-selenium country, New Zealand, excrete selen-
ium more sparingly than those of North Americans,
and Chinese from low-selenium areas have an even
lower renal clearance. This indicates a possible
adaptation to low selenium status.
0011 Trimethylselenonium ion, one of several urinary
metabolites, was once thought to be a detoxification
product of selenium and appears to be a minor me-
tabolite in humans. Another methylated metabolite,
methylselenol, may constitute a larger proportion of
urinary selenium. Small losses of selenium occur
through the skin or hair or, at high intakes, in expired
air as volatile dimethylselenide.
Excretion of Selenium in Milk
0012 Most of the selenium in human milk is protein-
bound; at least nine selenium-containing proteins
have been detected in milk with glutathione peroxid-
ase accounting for 15–30% of total selenium.
Role of Selenium in the Body
Selenoproteins
0013Selenium exerts its biological effect through several
selenoproteins, of which there may be upwards of 30
in mammalian systems. Identification and character-
ization of many of these proteins in recent years have
resulted in major advances in our understanding
of the function of selenium. The following seleno-
proteins have been purified and studied.
.
0014glutathione peroxidases;
.
0015cytosolic, cellular
.
0016gastrointestinal
.
0017plasma
.
0018phospholipid hydroperoxide
.
0019selenoprotein P;
.
0020iodothyronine 5
0
-deiodinases;
.
0021sperm capsule selenoprotein;
.
0022selenoprotein-W;
.
0023thioredoxin reductase;
.
0024selenophosphate synthetase;
.
002558-, 56-, and 14-kDa Se-binding protein.
0026Glutathione peroxidases The first of these sele-
noproteins to be characterized was glutathione
3000
800
350
300
250
200
150
100
50
0
Venezuela
USA
Australia
Finland
New Zealand
China
Auckland
122 Otago
104
8
25
116
210
Number of subjects
Whole blood selenium (ng ml
−1
)
fig0002 Figure 2 Blood selenium concentrations of healthy adults in Venezuela, the USA, Australia, Finland, New Zealand, and China (low-
and high-selenium areas). (To convert nanograms of Se per milliliter to micromoles per liter, multiply by 0.0127.)
SELENIUM/Physiology 5119

peroxidase, which consists of four identical subunits,
each containing one selenocysteine at the active site.
Activity of this enzyme can be reduced to less than
1% in tissues of selenium-deficient animals. Glu-
tathione peroxidase present in cells (including eryth-
rocytes), plasma, and the gastrointestinal tract may
function in vivo to remove hydrogen peroxide,
thereby preventing the initiation of peroxidation of
membranes and oxidative damage. However, the sig-
nificance of this function in the body is uncertain, and
it seems likely that the oxidant defense role for selen-
ium is exerted more through other selenoproteins.
Glutathione peroxidase may have more specific
functions in arachidonic acid metabolism in plate-
lets, microbiocidal activity in leukocytes, and the
immune response mechanism or perhaps as a storage
protein.
0027 Another selenium-containing enzyme, phospho-
lipid hydroperoxide glutathione peroxidase, is differ-
ent from the classic glutathione peroxidase in that it
can metabolize fatty acid hydroperoxides that are
esterified in phospholipids in cell membranes. This
enzyme can inhibit microsomal lipid peroxidation
and is most likely the basis of the selenium/vitamin
E interaction in the pathogenesis of several deficiency
diseases in animals.
0028 Selenoprotein P A plasma protein designated sele-
noprotein-P has been purified and characterized from
rat and human plasma and is also associated with
endothelial cells. Selenoprotein-P is a glycoprotein
containing selenium as selenocysteine, and its concen-
tration in rat plasma falls to less than 10% of the
control in selenium deficiency. Its function is un-
known, but it may have an extracellular oxidant de-
fense role because its presence correlates with
selenium protection of selenium-deficient rats against
diquat-induced lipid peroxidation and liver necrosis.
A transport role has also been suggested for this
protein.
0029 Iodothyronine deiodinases The discovery that type I
iodothyronine 5
0
-deiodinase and, more recently, type
II and type III deiodinases are selenoproteins indicates
a role for selenium in the metabolism of thyroid hor-
mones that are essential for growth and development.
This enzyme catalyzes the conversion of thyroxine
(T
4
) to its active metabolite triiodothyronine (T
3
)in
the liver and kidney, and selenium deficiency results
in an increase in levels of plasma T
4
and a corres-
ponding decrease in levels of more active T
3
. Selen-
ium is preferentially supplied to this enzyme rather
than glutathione peroxidase when the selenium supply
is inadequate. The interactions of selenium and iodine
deficiencies have implications for both human and
animal health and livestock production. In humans,
selenium deficiency can either exacerbate or amelior-
ate the effects of concurrent iodine deficiency as has
been observed in the development of iodine deficiency
disorders in Zaire.
0030Thioredoxin reductase A recent addition to the
list of selenoproteins is thioredoxin reductase, an
NADPH-dependent flavoenzyme that reduces the
disulfide of thioredoxin. This enzyme regenerates
ascorbic acid from dehydroascorbic acid. The activity
of thioredoxin reductase declines in selenium defi-
ciency, and there is evidence that selenium is present
in the active site as selenocysteine.
0031Selenoprotein W Selenoprotein W is a selenoprotein
found in muscle and other tissues. Its concentration
decreases during selenium deficiency, and it may be
involved in the development of muscular degener-
ation in selenium-deficient sheep.
0032Other selenoproteins Several other selenium-
containing enzymes have been identified in
microorganisms, and other selenoproteins have
been found in animal tissues, suggesting further
functions for selenium. These include a specific sele-
noprotein in prostate tissue, a mitochondrial seleno-
protein in sperm, and a 14-kDa and 56/58-kDa
selenium-binding protein. One of two selenopho-
sphate synthetases recently identified contains seleno-
cysteine, and it is possible that this enzyme may be
involved in the regulation of selenium homeostasis.
Selenium and Host Defense Towards Viruses
0033The seasonal nature of Keshan disease suggested
the likely involvement of an infectious agent, which
led to recent work on host response to myocarditic
and amyocarditic strains of Coxsackie virus B
3
in
mice. Selenium deficiency potentiated cardiotoxi-
city of myocarditic strains, but in addition, the amyo-
carditic strain caused heart lesions in selenium
deficient mice. This indicated that this specific nutri-
ent deficiency allowed a benign virus to become viru-
lent, apparently as a result of a change in the viral
genome. The observation that selenium deficiency
may accelerate viral evolution may help to clarify
the etiology of Keshan disease and may also be
applicable to other RNA viruses. Vitamin E defi-
ciency had effects similar to those observed with
selenium deficiency, which suggests the involvement
of antioxidant properties of the two nutrients. This is
the first reported instance of an influence of host
nutritional status on the genetic composition of the
pathogen.
5120 SELENIUM/Physiology

Selenium and Immune Function
0034 Adequate selenium is essential for a variety of aspects
of the immune function. Selenium is necessary for the
development of the acquired immune system, and has
a role to play in the defense system of animals against
bacteria and other infections. The recent finding of a
role for selenium in cell-mediated immunity to Cox-
sackie virus in mice indicates a protective effect of
selenium against viral infection. The mechanisms for
the involvement of selenium in the immune system
are likely to be related to its antioxidant function
through one of the antioxidant selenoproteins
glutathione peroxidase, phospholipid glutathione
peroxidase, or selenoprotein-P.
Deficiency
0035 Interaction between selenium and vitamin E is ob-
served in the etiology of many deficiency diseases in
animals and pure selenium deficiency is in fact rare.
Thus, selenium deficiency may only occur when low
selenium status is linked with an additional stress
such as chemical exposure, increased oxidant stress
due to vitamin E deficiency, exercise, or increased
dietary intake of polyunsaturated fatty acids. Al-
though residents in some low-selenium areas have
low blood selenium, glutathione peroxidase activity,
and Selenoprotein P levels, there is little evidence that
these are suboptimal or have resulted in any notice-
able oxidative damage or changes in other oxidative
defense mechanisms. Moreover, people have not
shown noticeably improved health when glutathione
peroxidase activity is saturated by selenium supple-
mentation. However, an exception to this general rule
may be found in the problem of Keshan disease in
China. Whether any of the newer functions of selen-
ium are suboptimal in persons with low selenium
status is being investigated.
Selenium-responsive Diseases in Humans
0036 Keshan disease, an endemic cardiomyopathy occur-
ring in low-selenium areas of China, was reported in
1979 to be responsive to supplementation with
sodium selenite. The principal pathological finding is
multifocal necrosis of the myocardium that causes
cardiac enlargement, congestive heart failure, cardio-
genic shock, and death. The disease is associated with
low selenium intake and low blood and hair levels,
and affects mainly children and women of child-
bearing age. It is probably the only case of naturally
occurring selenium deficiency. Because some features
of Keshan disease (e.g., seasonal variation) cannot be
explained solely on the basis of a very low selenium
status, Chinese researchers have suggested that other
factors may be involved, such as a virus, mineral im-
balance, or environmental toxins. Recent research on
Coxsackie virus B-induced myocarditis in selenium-
deficient mice supports a possible viral involvement in
Keshan disease. Another disease that has been associ-
ated with poor selenium status in China and Russia is
Kashin–Beck disease, an endemic osteoarthritis that
occurs during preadolescent or adolescent years.
Again, other etiologic factors such as contamination
of grain by fungi and high concentrations of organic
matter (e.g., fulvic acid) may be contributing factors.
The main features of the disease are shortened stature
and joint deformation, resulting from multiple focal
necroses in the growth plate of tubular bones.
0037Selenium deficiency has been associated with long-
term intravenous nutrition, because of the low levels
of selenium in the fluids. Clinical symptoms of
cardiomyopathy, muscle pain, and muscular weak-
ness are responsive to selenium supplementation,
but are not seen in all patients with extremely low
selenium status, indicating that there may be other
interacting factors. Furthermore, children on very
low selenium synthetic diets for inborn errors of me-
tabolism such as phenylketonuria do not develop
selenium-deficiency syndromes.
0038It is not clear whether syndromes in animals such as
the selenium-responsive muscular dystrophy observed
in sheep are related to human diseases. Although per-
sistent anecdotal reports from New Zealand farmers
in low-selenium areas indicate their conviction that
selenium relieves the farmers’ muscular aches and
pains, double-blind trials have failed to give a clear-
cut answer.
Selenium and Cancer
0039Several lines of scientific enquiry suggest that an in-
creased risk of cancer occurs as a result of low levels
of selenium in the diet. An association between selen-
ium and cancer was first proposed 30 years ago when
it was observed that regional cancer mortality rates
in the USA correlated with selenium exposure, as
reflected by concentrations in plants. Evidence for
the role of selenium as an anticarcinogenic agent
comes from in vitro and animal studies that suggest
that selenium is protective against tumorigenesis at
high levels of intake and from case-controlled pro-
spective studies in human subjects. However, epi-
demiological evidence linking a low selenium status
with an increased incidence of cancer is conflicting.
Few intervention studies in humans have been carried
out. In Linxian China, a significant effect of a com-
bination of vitamin E, b-carotene and selenium was
observed on mortality, particularly from esophageal
cancer. Recently a 10-year controlled clinical trial to
test the efficacy of selenium in preventing skin cancer
SELENIUM/Physiology 5121

was completed in the USA. There was no effect of
daily supplementation with 200 mg of selenium on the
primary endpoint skin cancer, but there was a statis-
tically significant reduction in several additional end-
points such as total cancer mortality (50%), and
incidence of cancer of the prostate (63%), lung
(46%), colorectal (58%), and total cancer. Further
studies are needed to confirm these observations.
Selenium and Cardiovascular Disease
0040 Similarly, dietary deficiency of selenium has been
implicated in the etiology of cardiovascular diseases,
but the evidence at present is less convincing than for
cancer. Although a large case-control study in Finland
suggested that selenium was an independent risk
factor for myocardial infarction in a low-selenium
population, evaluation of prospective epidemio-
logical studies has failed to provide sufficient evi-
dence to implicate selenium deficiency in most
aspects of cardiovascular disease. While some investi-
gations have observed a relationship between low
serum-selenium levels and risk of coronary disease,
others have not. However, selenium may have some
role in protection against thrombosis and low-density
lipoprotein oxidation, in particular in individuals
such as smokers at risk from increased oxidant stress.
Further evidence must come from controlled inter-
vention trials to clarify any possible role for selenium
in atherosclerotic disease.
Toxicity
0041 The margin between an adequate and toxic intake of
selenium is quite narrow. Overexposure or selenosis
may occur from consuming high-selenium foods
grown in seleniferous areas in Venezuela and some
areas of China. People following long-term liberal
megadosing can also attain an undesirably high sel-
enium status. The most common sign of poisoning is
loss of hair and nails, but lesions of the skin, nervous
system, and teeth may also be involved. Garlic odor
on the breath is an indication of excessive selenium
exposure resulting from expiration of dimethylsele-
nide. Sensitive biochemical techniques are lacking for
selenium toxicity, which is at present diagnosed from
hair loss and nail changes. Some effects of selenium
toxicity are seen in individuals with dietary intakes as
low as 900 mg, and the maximum safe dietary intake
has been suggested as 400 mg per day.
Assessment of Selenium Status
0042 Blood selenium concentration is generally considered
a useful measure of both selenium status and intake,
but other tissues are often assessed as well. Plasma
selenium reflects short-term status and erythrocyte
selenium long-term status, but blood selenium con-
centrations are influenced by the chemical form of
selenium ingested as a result of the different patterns
of absorption and retention outlined previously. Toe-
nails are often used, but selenium-containing sham-
poos restrict the use of hair. Urinary excretion can
also be used to assess selenium status, and total
dietary intake is estimated as twice the daily urinary
excretion.
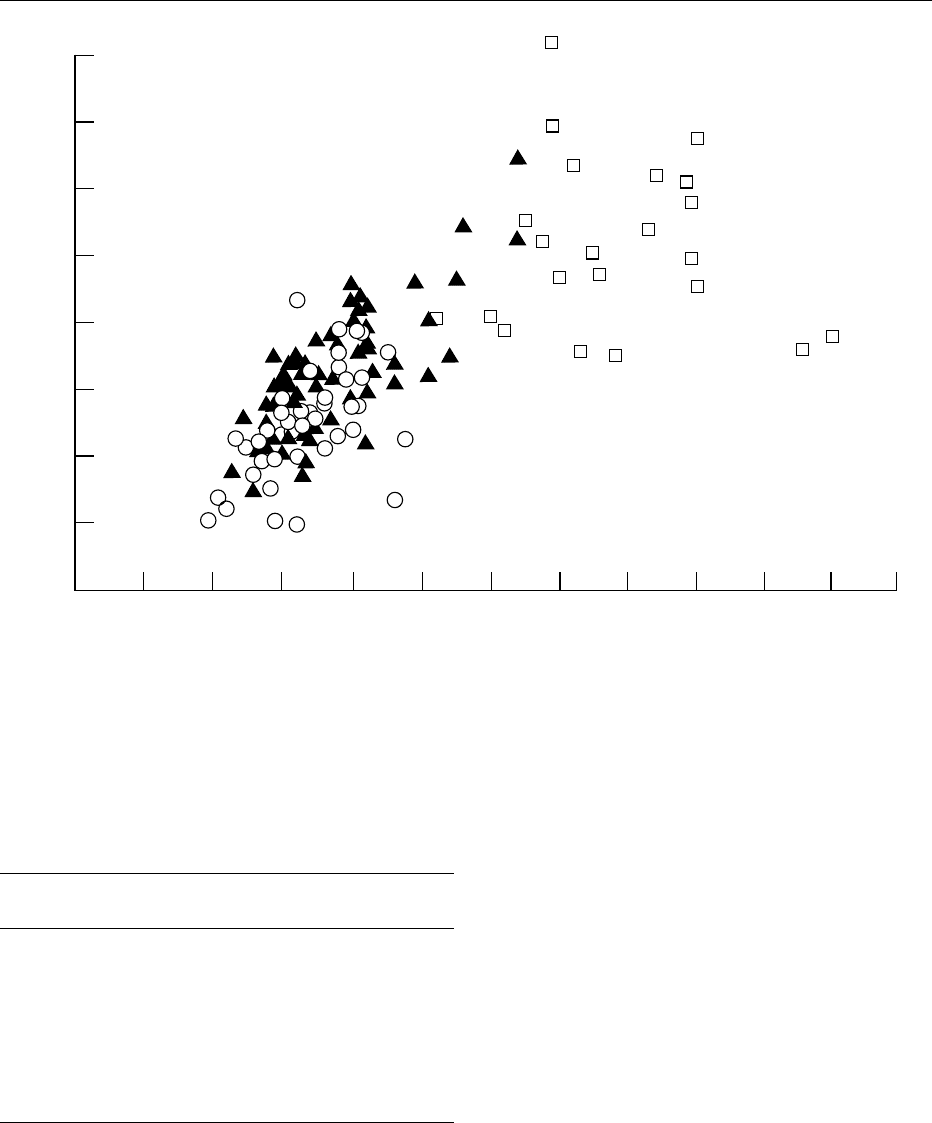
0043The close relationship between blood or red-cell
glutathione peroxidase activity and selenium con-
centrations (Figure 3) is useful for assessment in
people with a relatively low status, but not once
the saturating activity of the enzyme is reached at
blood selenium concentrations above 100 mgl
1
(1.27 mmol l
1
). More recently, mesurement of sele-
noprotein P has been used to assess selenium status,
and there is the potential for measurement of other
enzymes as functional markers. However, their use is
limited at present by the lack of simple assay tech-
niques. Furthermore, the conclusions drawn from
measurement of one selenoprotein may not apply to
all biological functions of selenium because of the
differences in responses of tissues and these proteins
to deficient, adequate, or high levels of selenium in
terms of their ‘hierarchy’ of importance. Therefore,
there may be no single indicator of functional selen-
ium status, but rather a series of markers that apply to
specific problems associated with suboptimal selen-
ium status. The situation is further complicated by the
large number of interacting factors, including, pro-
tein, methionine, polyunsaturated fatty acids and
other oxidant stressors, vitamin E, other trace elem-
ents, and heavy metals such as mercury, cadmium,
and lead.
Dietary Intake
0044Food is the major source of selenium; drinking water
contributes little. Dietary intake varies with the
geographic source of foods and eating habits of the
people. Plant food concentrations reflect selenium
content of soils and its availability for uptake, as
plants do not require selenium for growth; cereals
and grains grown in soils poor or rich in selenium
may vary over 100-fold in selenium content. Animal
foods vary less. Fish and organ meats are the richest
sources followed by muscle meats, cereals, grains,
and dairy products, with fruits and vegetables mostly
poor sources. Average daily dietary intakes vary con-
siderably, depending on the levels of selenium in soils
(Table 1), ranging from 10–20 mg of selenium in low
soil-selenium areas of China where Keshan disease is
endemic, 30–60 mg in New Zealand, and up to 200 mg
5122 SELENIUM/Physiology
in seleniferous areas in Venezuela. In 1985, selenium
was added to fertilizers in Finland to increase selen-
ium intake throughout the population, and the daily
intake rose from 40 mg to close to 100 mg per day,
resulting in an increase in serum selenium in healthy
individuals from 65–70 mgl
1
in 1985 to 120 mgl
1
in
1989–1991. In New Zealand, intakes are increasing
due to increasing importation of Australian wheat,
and selenium status is rising accordingly. However,
this increase is greater than expected from the
increase in wheat selenium, indicating that other
dietary factors are involved. These differing intakes
in various countries are reflected in the wide range of
blood selenium concentrations found in residents of
these countries (Figure 2).
Requirements and Recommended Dietary
Allowances (RDAs)
0045Many countries have proposed recommended dietary
intakes based upon estimates of requirements from
Chinese intakes for endemic and nonendemic Keshan
disease areas, as well as intakes at which maximal
levels of plasma glutathione peroxidase activity oc-
curred. The recommended dietary intake for Austra-
lia was the first set in the world in 1986 and may have
been cautiously on the high side at 85 and 70 mg
0
0.02 0.04 0.06 0.08 0.10 0.12 0.14 0.16 0.18 0.20 0.22 0.24
4
8
12
16
20
24
28
32
Selenium concentration (µg Se per milliliter of erythrocytes)
Glutathione peroxidase activity (units per gram of Hb)
fig0003 Figure 3 Relationship between selenium concentration of erythrocytes and glutathione peroxidase activities for New Zealand
residents: Otago patients (s): Otago blood donors (m) and overseas subjects (h). (To convert nanograms of Se per milliliter to
micromoles per liter, multiply by 0.0127.) From Rea HM, Thomson CD, Campbell DR and Robinson MF (1979) Relation between
erythrocyte selenium concentrations and glutathione peroxidase (EC 1.11.1.9) activities in New Zealand residents and visitors to New
Zealand. British Journal of Nutrition 42: 201–208, with permission.
tbl0001 Table 1 Daily dietary intakes of selenium and whole blood
selenium concentrations
Country Seleniumintake
(mgperday)
Blood selenium
(mgl
1
)
China (Keshan area) 9–11 10–20
New Zealand (before 1990) 28–32 50–100
(post 1990) 30–60 60–120
Finland (1985) 30 50–100
Finland (1989–1990) 100 120
UK 60 80–320
USA 62–216 150–400
Venezuela (Caracas) 218 350
China (seleniferous area) 5000 3200
From Thomson CD (2002) Selenium. In: Mann JI and Truswell AS (eds)
Essentials in Human Nutrition, 2nd edn, pp. 172–181. Oxford: Oxford
University Press, with permission.
SELENIUM/Physiology 5123
selenium for Australian men and women. Others,
including the recommended intakes of the USA, the
UK, and other European countries, are summarized in
Table 2. Each set of recommended intakes can be met
from habitual diets in each country. Whether optimal
health depends upon saturation of glutathione perox-
idase activity has yet to be resolved, leading to dis-
agreement regarding the use of this approach for
assessing selenium requirements. The US RDAs are
based on the desirability of the full activity of glu-
tathione peroxidase, whereas a WHO group con-
cluded that only two-thirds of the maximal activity
was needed, based on the observation that abnormal-
ities in metabolism of hydrogen peroxide in blood
cells is apparent only when enzyme activity falls to
one-quarter or less of normal. This has led to a wide
range of dietary recommendations, with the WHO
recommendations approaching intakes in countries
with a naturally low selenium status such as New
Zealand. In the future, several of the newly dis-
covered selenoproteins might be used as endpoints
for determining selenium requirements. However,
the maximal activity of some of these proteins occurs
at dietary intakes of selenium less than those needed
for maximal glutathione peroxidase activity. This
would no doubt lead to dietary recommendations
lower than current values.
See also: Bioavailability of Nutrients; Cadmium:
Toxicology; Cancer: Diet in Cancer Prevention; Coronary
Heart Disease: Prevention; Dietary Requirements of
Adults; Mercury: Toxicology; Tocopherols: Physiology
Further Reading
Arthur JR, Beckett GJ and Mitchell JH (1999) The inter-
actions between selenium and iodine deficiencies in man
and animals. Nutrition Research Reviews 12: 55–73.
Barceloux DG (1999) Selenium. Clinical Toxicology 37:
145–172.
Beck MA (1998) The influence of antioxidants on viral
infection. Nutrition Reviews 56: S140–S145.
Burk RF and Levander OA (1999) Selenium. In: Shils ME,
Olson JA, Shike M and Ross CA (eds) Modern Nutrition
in Health and Disease, 9th edn, pp. 265–276. Baltimore,
MD: Williams & Wilkins.
Dreosti I (1990) Selenium. In: Truswell A, Dreosti I, English
R, Ritihauser I and Palmer N (eds) Recommended Nu-
trient Intakes Australian Papers. Sydney: Australian Pro-
fessional Publications.
Levander OA and Burk RF (1996) Selenium. In: Ziegler EE
and Filer LJ (eds) Present Knowledge in Nutrition, 7th
edn, pp. 320–328. Washington, DC: ILSI Press.
Reilly C (1996) Selenium in Food and Health. London:
Blackie Academic & Professional.
Robinson MF (1989) Selenium in human nutrition in New
Zealand. Nutrition Reviews 47: 99–107.
Thomson CD (1998) Selenium speciation in human body
fluids. Analyst 123: 827–831.
World Health Organization (1996) Trace Elements in
Human Nutrition and Health, pp. 105–122. Geneva:
WHO.
tbl0002 Table 2 Recommended intakes of selenium for adults (mg/day)
Australia
(1990)
RDI
USA &
Canada
(2000)
RDA
UK (1991) Germany, Austria,
Switzerland (2000)
RNI
WHO
a
(1996)
NR
LNRI RNI
Men 85 55 40 75 30–70 40
Women 70 55 40 60 30–70 30
a
World Health Organization (1996) Trace Elements in Human Nutrition and
Health, pp. 105–122. Geneva: WHO.
RDI, recommended dietary intake; RDA, recommended dietary allowance;
RNI, reference nutrient intake; LNRI, lower reference nutrient intake; NR,
normative requirement estimate.
5124 SELENIUM/Physiology

SENSORY EVALUATION
Contents
Sensory Characteristics of Human Foods
Food Acceptability and Sensory Evaluation
Practical Considerations
Sensory Difference Testing
Sensory Rating and Scoring Methods
Descriptive Analysis
Appearance
Texture
Aroma
Taste
Sensory Characteristics of
Human Foods
R York, Canadian Food Inspection Agency, Winnipeg,
Manitoba, Canada
M Vaisey-Genser, The University of Manitoba,
Winnipeg, Manitoba, Canada
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Satisfaction with the sensory features of foods and
beverages is a major determinant of the consumer’s
nutritional status. If something does not taste ‘good,’
it is not likely to become part of the food habit.
However, the colloquial term ‘good’ is a reflection
of an integrated response to the several food features
that are considered in detail in following sections.
The present discussion is an introduction to sensory
evaluation that focuses on its ongoing evolution as a
discipline.
Definitions
0002 Early work in sensory evaluation was referred to as
organoleptic testing, a term that was discarded in the
1960s because it failed to recognize the complexity of
the sensory impression. In 1975, the US Institute of
Food Technologists defined the subject as a scientific
discipline used to evoke, measure, analyze, and inter-
pret reactions to those characteristics of foods and
materials as they are perceived by the senses of
sight, smell, taste, touch, and hearing. This definition
has since been extended to include the purpose of
providing information for decision-making with eco-
nomic consequences. As the field increases in sophis-
tication, the term ‘sensory science’ is becoming the
descriptor of choice rather than sensory evaluation.
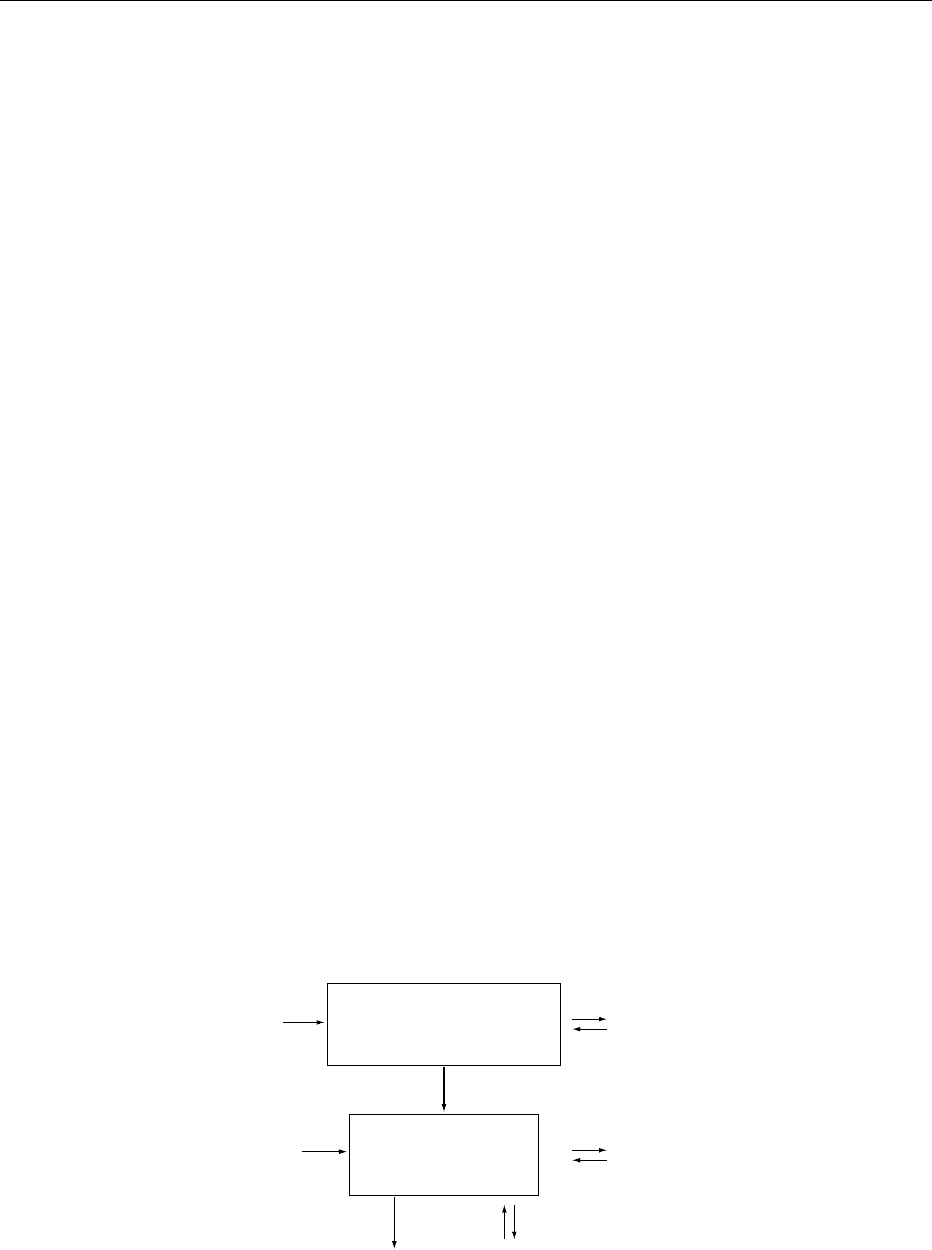
The sequence and the strategy for sensory science
measurements is illustrated in Figure 1.
Justification
0003Sensory measurements provide a unique resource
of information for the evaluation of foods. Humans
are sensitive and complex instruments capable of
measuring and integrating simple and complex
stimuli, repeating measurements after a brief resting
stage, and differentiating relevant from irrelevant
information. Accordingly, most physical tests for
‘ideal’ product characteristics are based on human
definition. The results are reliable and repeatable as
long as the test conditions are controlled.
History
0004Among sensory features, aroma seems to have cap-
tured major interest in early times, perhaps reflecting
the importance of spices for foods and of other aro-
matics used in perfumes and oils. In 320 bce (Before
the Common Era), a treatise on odor was put forth
by Theophrastus in Greece. That was followed by the
occasional classic on the nature of smell capped by
Linnaeus, odor classification, which appeared in
1756. Over time, the ‘expert taster’ became relied
upon within specific commodities, most notably
teas, wines, and other alcoholic beverages.
0005Sensory evaluation as we know it today stems from
the attention to methodology that began in the latter
part of the nineteenth century. This included methods
as simple as the score card to monitor commodity
quality and as sophisticated as the Weber–Fechner
Law, which related the sensory response quantita-
tively with incremental changes in a physical stimu-
lus. This spawned the discipline of psychophysics, a
SENSORY EVALUATION/Sensory Characteristics of Human Foods 5125
hybrid of psychology and physiology. The late nine-
teenth century saw the introduction of statistical
methods for handling sensory data.
0006 There were two sensory landmarks in the twentieth
century: the development of statistically sturdy meas-
urement methods and attention to the selection,
training, and performance monitoring of sensory
panelists. In the early 1930s, rating scales were de-
veloped to measure the intensity of specific food qual-
ities such as the tenderness of meat, and concurrently,
paired comparison and rank order methods were
introduced. The early 1950s was marked by the intro-
duction of the flavor profile system for the qualitative
analysis of foods by the Arthur D. Little Company
(ADL) in Massachusetts. ADL introduced training of
selected members from an industry in the systematic
‘descriptive analysis’ of their products.
0007 The mid-1950s saw further advances in statistical
methods for both design and analysis as well as the
launch in the USA of forced-choice methods such as
duo–trio and the triangle test, which originated in the
USA and Sweden, respectively. These tools are still
widely used by industry for sensory testing in their
quality control laboratories. A singular contribution
from this era was the nine-point hedonic scale for
measuring how much a food was liked or disliked.
Developed by the food acceptance branch of the US
Quartermaster Food and Container Institute in Chi-
cago, this tool has been used far beyond its original
purpose, which was to assist the development of
more acceptable rations for the military. It remains
a worldwide standard tool for food-preference
measurement.
0008 The momentum in sensory evaluation continued
throughout the 1960s marked by three major events:
(1) the 1961 formation of Committee E-18 within the
American Society for Testing of Materials (ASTM),
(2) the publication in 1963 of the Texture Profile
Method by scientists at General Foods Corporation
led by Alina Szczesniak, and (3) the 1965 Academic
Press publication of Principles of Sensory Evaluation
of Food, written by Amerine, Pangborn, and Roessler
at the University of California in Davis, a book that
promptly became a standard text. Further steps for-
ward were the 1968 opening of the Monell Chemical
Senses Center in Philadelphia to concentrate on basic
research of the senses under the leadership of physi-
ologist Morley Kare, and the 1969 introduction of the
Journal of Texture Studies.
0009In the early 1970s, the International Organization
for Standardization/Organization Internationale de
Normalisation (ISO) formed a subcommittee, TC34/
SC12, for Sensory Evaluation with the aim of having
internationally agreed upon standards for sensory
methodologies. This group currently includes repre-
sentatives from 17 countries as members and 30
countries as observers.
0010During the 1970s and 1980s, newer methods
of data handling erupted with the maturing of the
computer age. Multivariate analyses became the
norm, facilitating methods such as response surface
and principal-component analyses. Communication
worldwide was sparked by international symposia
such as the Mediterranean Odor Conference in
Cannes in 1970 followed by the later conferences
in Switzerland, Sweden, and the UK. New journals
such as 1974s Chemical Senses and Flavor (now
Chemical Senses), and later, in 1986, the Journal of
Sensory Studies emerged followed by Food Quality
and Preference in 1988. The 1990s saw the formation
of the Sensometrics Society for the development of the
special methodologies and statistical methods, which
were needed by the fields of sensory and consumer
science.
Take action
Analyze and
interpret
data from
these numbers
Measure
perceptions
with
sensory
analysis test
methods
Numbers guide
product decisions
Perceptions become
meaningful numbers
Decisions have
economic
consequences
Human perceptions
about products
fig0001 Figure 1 Sequence and strategy of sensory science measurements.
5126 SENSORY EVALUATION/Sensory Characteristics of Human Foods