Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

Nutraceuticals See Functional Foods
NUTRITION EDUCATION
S S Deshpande, Central Institute of Agricultural
Engineering, Nabibagh, Bhopal, India
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Advances in nutrition research have provided means
of prevention and control of some of the major crip-
pling nutritional disorder with sever socioeconomic
and health repercussions. The next logical step after
the discovery of such solutions will be their propaga-
tion among the concerned community members. It is
here that health and nutrition education has a role
to play. The emphasis in these nutrition education
programs ought to be on the proper use of natural
dietary sources of nutrients and the need for full use
of available health services and health and nutrition
intervention program launched by government and
other agencies.
0002 Nutrition education programs, when properly im-
plemented, have the potential to bring out desired
behavior modifications among the communities. But
for them to be successful, there are several obvious
prerequisites such as the right approach suited to the
community appropriately, motivated change agents,
suitable educational strategies in terms of media,
messages, etc. The ultimate impact of any nutritional
education effort hinges on the extent to which the
above criteria are satisfied.
0003 Nutrition education has been defined as the process
by which beliefs, attitudes, environmental influences,
and understanding about food lead to practices
that are scientifically sound, practical, and consistent
with individual needs and available food resources;
nutrition education should be available to all individ-
uals and families. The fundamental philosophy of
nutrition education is that efforts should focus on
the establishment and protection of nutritional health
rather than on crisis intervention. It is needed, regard-
less of income, location or cultural, social or economic
practices, or level of education. Nutrition education
must be a continuing process throughout the life cycle
as new research brings additional knowledge.
Scope
0004 Education means a change in behavior. It moves the
individual from lack of interest and ignorance to
increasing appreciation and knowledge and finally
to action. Nutrition education offers a great oppor-
tunity to individuals to learn about the essentials of
nutrition for health and to take steps to improve the
quality of their diets and thus their well-being.
0005Nutrition education must continue throughout the
individual’s life in order to accommodate for devel-
opments in nutrition science and for changing eco-
nomic circumstances, health requirements, and the
new food products appearing in the nation’s market.
This requires a greatly expanded use of the mass
media, and the involvement of governmental and
private agencies and universities, as well as the food
industries.
Concept
0006A concept is an idea around which the content of
nutrition education curricula can be built.
What is Nutrition Education?
0007Nutrition education is the process of teaching the
science of nutrition to an individual or group. Health
professionals have a different role in educating an
individual in the clinic, community, or long-term
health-care facility. In these settings, the dietician,
nutritionist, or nurse serves to assist or enable indi-
viduals to incorporate changes in eating patterns and
behavior into their lives. The major focus of this type
of nutrition is not knowledge and facts, but rather the
development of permanent behavioral changes. This
is the art of nutrition education – breaking down a
large body of knowledge into small, individual com-
ponents that are represented to a patient or client at a
rate and level, at which they are able to absorb and
use the information. Effective education is making
nutrition information digestible and usable in an
everyday setting.
Steps Involved in Nutrition Education
0008The development of an organized, coordinated nutri-
tion education program requires a series of steps:
.
0009Consumer research is needed to determine con-
sumer use of existing information attitudes, know-
ledge, levels of awareness and concern, current
4164 NUTRITION EDUCATION

nutrition practices, and type of education to which
they should be most receptive.
.
0010 Nutritional surveillance data are needed to deter-
mine the most important public information prob-
lems for determining reasonable objectives to be
used in formulating the nutrition education.
.
0011 Most appropriate target populations for nutrition
education are determined on the basis of aware-
ness, nutritional status, current knowledge, and
receptivity to nutritional information.
.
0012 A nutrition education message should be designed
that is appropriate for the needs of the selected
population groups.
.
0013 The curricula for the nutrition education program
must be well thought out and planned. At every
step, the learner and the educator should work
together to develop goals, objectives, and appro-
priate activities and resources to meet the goal.
.
0014 Evaluation is crucial to any successful educational
effort.
Why Nutrition Education?
0015 A number of forces have emerged to stimulate in-
creased recognition of the need for a stronger, more
comprehensive and creative effort at nutrition educa-
tion. These factors include:
.
0016 Many serious as well as less serious health problems
are the result of lifestyles and personal habits, includ-
ing habits of food consumption. Individual modifi-
cations in lifestyles may improve health status.
.
0017 Food Patterns. Differing forms of food vary in
nutritive value as well as in taste appeal. The aver-
age consumer is often mystified and unaware of
how to make the wisest food choices from such a
variety. Thus, there is a great need for education to
enable consumers to select wisely an appropriate
diet from the vast supply of food available.
.
0018 Lifestyles are drastically different from those of the
turn of the century. The public must be knowledge-
able about how to meet nutritional needs without
overindulgence in foods.
.
0019 Nutrition education is also necessary to aid the con-
sumer to make economical food choices, that is, to
save money while getting optimal nutrition. This is
especially important for the low-income consumer.
.
0020 On a global basis, there is a real possibility of food
shortages. Therefore, the consumer should know
how to provide nutritional substitutes for unavail-
able food items.
What to Emphasize in Nutrition Education
0021 It is very difficult to define the basic knowledge that
should be conveyed to the public about nutrition.
Much will depend upon what the learners already
know, how they evaluate their present dietary habits
and nutritional status, what their present eating habits
actually are, how much they desire to know, and what
changes they are willing or can afford to make.
Nutrition Education Strategies
0022In view of the multifactorial influences on food
habits, there is no one way to persuade people to
change their food choices. Thus, nutrition education
must use a variety of techniques that must be a part of
total family and community environments.
0023In other words, nutrition education involves infor-
mation exchange as well as techniques to motivate
and reinforce improved food habits. Successful nutri-
tion education must include endeavors to make
beliefs, attitudes, values, environmental factors, and
individual ideas about food conducive to nutrition-
ally sound, practical, and acceptable dietary habits.
Nutritional education can be approached in various
ways. What might be termed the rational–empirical
curriculum design is the approach that is typically
used by educators; it is logical and planned, and
it involves behavioral objectives, activities that
are designed to achieve objectives, and evaluation
to determine the discrepancy between planned and
achieved outcomes. The idea of self-responsibility
for health suggests the basic notion that the individual
possesses a dignity, worth, and responsibility to maxi-
mize these characteristics. Self-responsibility assumes
that the individual has the potential and motivation
to make wise judgments about factors that affect their
health status. Another strategy has been termed the
travel metaphor method. The idea is that there is
a body of knowledge, facts, concepts, values and
believes that are known and understood by the edu-
cator. It is the educator’s responsibility to lead the
learner through this body of knowledge and beliefs,
and point out to the learner what is thought to be of
importance. The educator is thus a travel guide whose
job is to provide the student with a set of stimuli and
the opportunity to take advantage and react posi-
tively. It then becomes the responsibility of the stu-
dent to determine how they will make use of the
contacts provided by the educator.
0024Another approach called the garden metaphor ex-
plains how humans grow, develop and flower natur-
ally. The educator has the opportunity to nurture this
environment so that the ‘child’ has the most oppor-
tunity to mature and to learn.
0025Another approach to health and nutrition educa-
tion takes a strategy of social manipulation. The basic
premise is that the matters affecting health are too
urgent, too important, and beyond the individual’s
NUTRITION EDUCATION 4165

power to control on their own. Thus, the role of the
health educator is seen as one of attempting to control
behavior and to shape the desired responses. This
approach is often employed by the mass media.
0026 The manipulative approach is more concerned
with the behavior response patterns rather than the
manner in which the individual reaches these pat-
terns. The approach is an attempt to reach the desired
behavior through a short-cut method and does not
take time to prepare the individual to make fully
informed, wise choices.
0027 The most appropriate and effective strategy for
stimulating improved food habits will depend upon
the knowledge, background, personal characteristics,
and motivation of the audience. It may also depend
upon the size of the target group. Ideally, the
approach should be individualized to the target audi-
ence’s needs, goals, objectives, and other characteris-
tics. A mix of various approaches may be necessary.
Systems Approach to Nutrition Education
0028 The ‘systems’ approach to nutrition education pro-
vides a useful and practical tool to aid the nutrition
educator in deciding what should be taught and how
it should be taught. Simply defined, the systems ap-
proach is a flow of steps needed to achieve the desired
objectives. The approach consists of input, process,
and output.
0029 A successful nutrition education effort must incorp-
orate managerial elements that are crucial to the
success of all program planning. These elements,
which could be termed the input, are essential to an
effective nutrition education process. They include
needs assessment and identification of problems;
study of available resources and alternative strategies
of intervention; determination of objectives and goals;
assignment of resources to implement program; staff
development to implement program, and program
monitoring and evaluation. Crucial to the entire pro-
cess is a firm organization base and administrative and
budgetary support for nutrition education efforts.
Follow-up and Evaluation
0030 Nutritional counseling follow-up, in order to evalu-
ate learning, is an essential factor, which needs to be
included in the plan. After an initial interview, follow-
up is usually planned for some time during the next 1–
2 weeks or perhaps at a later time in the same week.
As clients progress toward a goal, follow-up visits are
generally spaced further and further apart. In a
follow-up session, the client’s progress needs to be
measured against the objectives, and the client needs
to receive positive feedback about their progress. In
the event that no progress has been made or the client
has slipped back into old habits, the counsellor needs
to pursue the problem assertively. The problem needs
to be identified and new goals or methods of achiev-
ing the goals established.
Summary
0031Nutrition education is a broad area; however, the
nutritionists or nurses facilitating it are usually con-
centrated in the acute or long-term care facilities and
community clinics. In all aspects of teaching and
counseling, instructional objectives need to be estab-
lished, the learner’s knowledge assessed, behavioral
objectives written, evaluation tools devised, informa-
tion needs screened and organized, education mater-
ials selected, and instruction critiqued and revised. It
is also essential to keep the learner’s needs in the
forefront and work to maintain a rapport with the
client.
0032Education is not complete until the learning has
been evaluated. Formal and informal tools may be
used to measure learning against established object-
ives. Evaluation helps identify if further teaching
or clarification of information is needed. To some
degree, demonstrating successful learning at evalu-
ation reinforces continuance of new behaviors,
which is the goal of nutrition education.
See also: Community Nutrition; Dietary Requirements
of Adults; Famine, Starvation, and Fasting; Food
Safety
Further Reading
American Dietetic Association (1973) Position paper on
nutrition education for the public. Journal of the
American Dietetic Association 62: 429.
Caliendo MA (1986) Nutrition Education. Definitions and
Concepts in Nutrition and Preventive Health Care,
pp. 410–437. New York: Macmillan.
Deshpande SS (1999) Study of nutritional pattern of some
selected villages around Bhopal with special reference to
soybean consumption. Ph.D. Thesis, Barkatullah Uni-
versity, Bhopal.
Griffin GA (1974) Strategies in Curriculum Development
In: Conference on Education in Nutrition, Looking
Forward from the Post. New York: Columbia Univer-
sity, Teachers College.
Rau P (1982) Experiences in nutrition education. Nutrition
22(2): 3.
Robinson CH, Lawler MR, Chenowth WL and Garwick
AE (1986) Nutrition Problems and Programs in the
Community. Normal & Therapeutic Nutrition, 17th
edn., pp. 355–357. New York: Macmillan.
SNE Concepts for Food & Nutrition Education (1982)
Journal of Nutrition Education 14: 1.
4166 NUTRITION EDUCATION
NUTRITION POLICIES IN WHO EUROPEAN
MEMBER STATES
A Robertson, WHO Regional Office for Europe,
Copenhagen, Denmark
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 In December 1992, after more than 2 years of pre-
paratory work by the member states and the joint
efforts of the World Health Organization (WHO)
and the Food and Agriculture Organization (FAO),
the International Conference on Nutrition (ICN) was
convened in Rome to:
.
0002 increase public awareness of the extent and serious-
ness of nutrition- and diet-related problems world-
wide
.
0003 promote effective strategies and actions to address
these problems
.
0004 encourage the political commitment necessary to
do so
Each of the 159 participating countries and the Euro-
pean Community reaffirmed their determination to
insure sustained nutritional well-being for all people
and committed themselves to achieve this goal by
unanimously adopting the World Declaration and
Plan of Action for Nutrition. The nine action-oriented
strategies of the World Declaration and Plan of Action
for Nutrition are summarized in Table 1. These
provide a framework for national plans of action.
0005 In 1996 a follow-up to ICN (Table 2) was held in
the European region through a FAO/WHO consult-
ation in Warsaw, Poland. Its aim was to assess imple-
mentation of the World Declaration. Representatives
from European member states and Canada, the USA,
the European Commission and the Holy See attended
the meeting along with representatives from the
United Nations Development Program (UNDP), the
United Nations Children’s Fund (UNICEF), nongo-
vernmental organizations (NGOs) and the private
sector.
Methods
0006Member states were requested to prepare a summary
report of their progress for the 1996 follow-up meet-
ing in Poland. Based on the 35 reports received
(response rate of 70%) the WHO Nutrition Unit
compiled an overview of the situation.
0007Member States were grouped into eight geographic
regions: Balkan, Baltic, Central Asian Republics
(CAR), countries of central and eastern European
(CCEE), western Europe, southern Europe, Com-
monwealth of Independent States (CIS), excluding
CAR, and Nordic countries (Table 3). The aim of
this is to facilitate comparative analysis and interpret-
ation and assist in drawing conclusions and recom-
mendations.
Results
0008The country data are presented in tables under the
headings of the strategies of the Plan of Action for
Nutrition adopted at the ICN.
Discussion
Developing Food and Nutrition Policy
0009Around the time of ICN (1992), some member states
in Central Asia, the former Soviet Union and the
Balkan region were not fully independent and so
were unlikely to have information about the ICN.
Thus food and nutrition specialists in some parts of
the WHO European region were probably unaware
of the ICN and so it is hardly surprising that many
countries had not developed national plans of action
according to the ICN objectives.
0010Moreover a few WHO member states are not
members of FAO (1998) and others have only
recently joined. This probably explains why there
were more health than agriculture representatives
present – 66% compared with 27% – at the consult-
ation in Poland in 1996.
0011One of the difficulties when attempting to develop
intersectoral policies is the level of commitment that
tbl0001 Table 1 The nine action-oriented strategies of the plan of
action for nutrition
Incorporating nutritional objectives, considerations, and
components into development policies and programs
Improving household food security
Protecting consumers through improved food quality and safety
Promoting breast-feeding
Caring for the socioeconomically deprived and nutritionally
vulnerable
Preventing and controlling specific micronutrient deficiencies
Promoting appropriate diets and healthy lifestyles
Assessing, analyzing, and monitoring nutrition situations
Preventing and managing infectious diseases (N.B. not included
in this analysis, since not mentioned in any country reports)
NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES 4167
each stakeholder has to public health versus their own
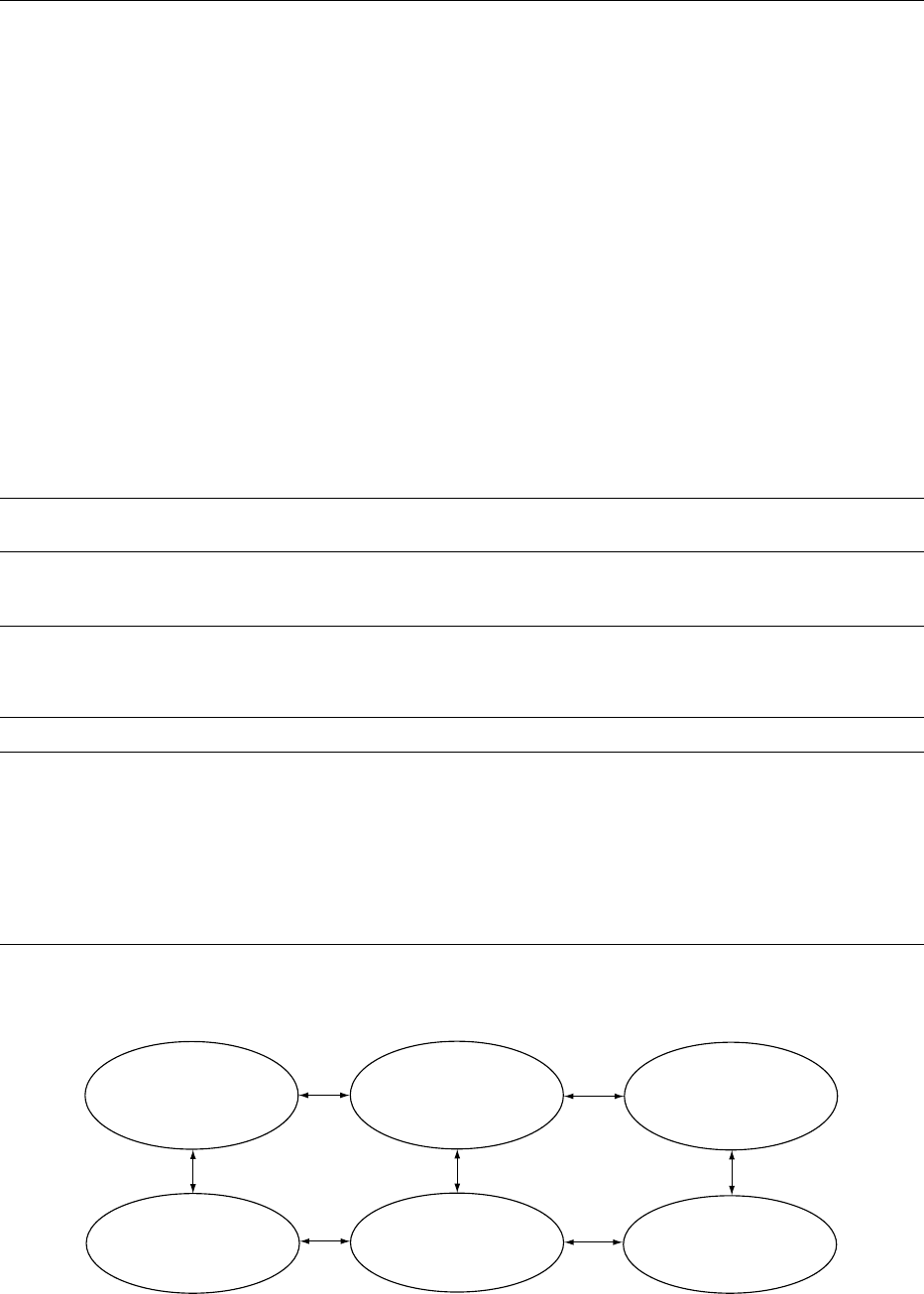
possibly diverging interests (Figure 1). It is improb-
able that intersectoral policies will be implemented,
unless all stakeholders are committed to the process.
However, the long-term interests of the agriculture
sector, the food industry, wholesale and retail repre-
sentatives are dependent on policies which have been
developed in collaboration with the voluntary sector
and consumers. Consumers, the customers of the
food industry, should be more involved in the process
whereby food policy is developed.
Intrasectoral Collaboration within the Health
Sector
0012 Good collaboration between nutrition and food
safety is essential because the public and consumers
perceive food in a holistic way. Consumers do not
compartmentalize food or distinguish between food
safety and nutrition – consumers want good whole-
some food they can enjoy without fear. There appears
to be far more collaboration between the nutritionists
and food safety specialists working in central and
eastern Europe compared with those in western
Europe.
0013There may be several reasons for the stronger col-
laboration in central and eastern Europe. Nutrition is
a relatively new science and in eastern parts of Europe
its evolution seems to be closely linked to ‘hygiene’
and the sanitary–epidemiology system. In eastern
Europe nutrition and food hygiene have evolved
from the same postgraduate specialization, usually
as a specialization of medicine. In former socialist
countries food safety is traditionally under ministries
of health, whereas in some western European
tbl0003 Table 3 Member states of the World Health Organization European region, 1996
Balkan Baltic CARandTurkey CCEE WesternEurope Southern Europe CIS Nordic
Albania Estonia Kazakhstan Bulgaria
a
Austria Greece Armenia Denmark
Bosnia and Herzegovina Latvia Kyrgyzstan
a
Czech Republic Belgium
a
Israel Azerbaijan Finland
a
Croatia Lithuania Tadjikistan
a
Hungary France Italy Belarus Iceland
Federal Republic of
Yugoslavia (Serbia
and Montenegro)
Turkey
Turkmenistan
a
Uzbekistan
Poland
Romania
Slovakia
Germany
Ireland
Luxembourg
Netherlands
a
Switzerland
UK
Malta
Monaco
a
Portugal
a
San Marino
a
Spain
a
Georgia
a
Republic of
Moldova
Russian
Federation
a
Ukraine
Norway
Sweden
Former Yugoslav Republic
of Macedonia
a
Slovenia
a
a
No report submitted (Finland was added later).
CAR, Central Asian Republics; CCEE, countries of central and eastern Europe; CIS, Commonwealth of Independent States.
Public health specialists
in food control and
nutrition
Public health specialists
collaborate with public
interest groups
Agriculture, food industry,
and health specialists
collaborate with public
interest groups
The health sector
develops
its food policy
The health sector
seeks alliance with
consumers
Create a sustainable
market for the food
industry
fig0001 Figure 1 From intra- to intersectoral policy development food priorities for health.
tbl0002 Table 2 Member states at the International Conference on Nutrition follow-up consultation, Poland, September 1996
Total no. of FAO/WHO
memberstatesinvited
Total no. of
countries present
Total no. of
representatives
Percent of health and agriculture
representatives from European region
Total no. of reports
submitted (Europeanregion)
57 40 62 66% health 35
27% agriculture
7% others
FAO, Food and Agriculture Organization; WHO, World Health Organization.
4168 NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES

countries only nutrition is under ministries of health
and the responsibility for food legislation and en-
forcement may be with ministries of agriculture or
trade in the west. However this is changing, especially
in some European Union (EU) member states, where
ministries of health are taking a much more proactive
role in protecting consumers and their health.
0014 Coordination between public health specialists
working in food safety and nutrition is important
for many other reasons. One is that from time to
time food control authorities may issue warnings
about food, e.g., chicken that contains Salmonella,
or fish and vegetables which are contaminated.
Meanwhile, as part of national campaigns, nutrition-
ists promote the consumption of vegetables, fish, and
poultry. Public health specialists must deliver consist-
ent and reliable information to avoid public confu-
sion. Closer cooperation between nutritionists and
food safety specialists can prevent the promotion of
conflicting messages.
Intersectoral Collaboration
0015 Public health specialists dealing with food safety and
nutrition should strengthen their collaboration with
other sectors dealing with food, e.g., agriculture, food
industry, wholesalers and retailers, voluntary sector
and public interest groups representing consumer
interests. Consumers have a vested interest in
supporting the supply of safe food of good quality
that is nutritionally healthy and the food industry has
a vested interest in supplying healthy consumers.
There is an opportunity for the health sector to
strengthen health alliances with public interest groups
working in the voluntary sector.
0016 Surprisingly, in the country reports, there was very
little mention about the importance of collaboration
with consumer agencies except by Hungary, Norway,
Poland, and Sweden. In these countries there is an
understanding that the food industry can profitably
increase the availability of vegetables and fruit, low-
fat milk, and lean meat, on condition that it is assured
a market.
Assessing the Nutrition Situation
0017 Almost all countries reported a need to improve
nutrition information systems. According to DAFNE
(Network of the Pan-European Food Data Bank
Based on Household Budget Surveys: countries par-
ticipating are Belgium, Denmark, Greece, Germany,
Hungary, Ireland, Poland, Portugal, Spain, and the
UK), some had no information, while some use sec-
ondary data or access nutrition information from
household budget surveys. Some had information
from one-off surveys that were sponsored through
international cooperation. The Nordic countries and
the UK seem to have established the most comprehen-
sive surveillance systems that provide information on
food consumption and nutritional status on a routine
basis. Clearly it will take time for some countries to
achieve this level of sophistication but ultimately
these data are essential to facilitate food and nutrition
policy development.
0018It seems unlikely that, at least in the near future,
nationally representative nutrition surveys will be
carried out on a regular basis; therefore other strat-
egies have to be found: members of DAFNE extract
nutrition-related data from household budget surveys;
in Italy secondary data sources were used to develop a
national policy. Mortality data are available from the
WHO Health For All database which is accessible
through the internet from the WHO website. These
data allow comparison of mortality statistics between
different countries. FAO food balance sheets provide
data such as the percentage energy coming from
carbohydrate, fat, protein, and alcohol and the quan-
tity of vegetables and fruits available nationally. These
data are directly accessible from the FAO website.
0019In the future the EU may encourage its member
states, and those wishing to join, to develop standard
information systems. This will allow comparison of
data on food intake, nutritional status, and diet-
related behavior in different EU member states and
so facilitate the development of cost-effective strat-
egies that enable countries to save money on treating
preventable diseases.
Improving Food Security
0020After the Second World War the main aim in Europe
was to increase the supply of food, especially animal
products, e.g., meat and milk. However the postwar
policy was too successful (Table 4) and in the 1980s
until the present time Europe has surplus stocks of
butter, meat, and milk.
0021Since the Second World War, new scientific
evidence has led to the level of recommended daily
protein intake being reduced. For example the level
of protein intake recommended by the FAO, WHO,
and the United Nations University (UNU) in 1986
was 0.75 g kg
1
day
1
. This new level resulted in
many countries reducing the level of their national
recommended protein intakes for adults from 120 g
to around 50 g per person per day. There is now some
evidence suggesting that excess intake of some sources
of protein, especially from red meat, could be associ-
ated with ill health.
0022Various hypotheses exist to explain how meat con-
sumption may contribute to chronic diseases such as
heart disease and certain cancers. Meat intake is as-
sociated with an increased intake of saturated fats
NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES 4169
which are linked to an increased risk of cardiovascu-
lar diseases and breast and colorectal cancer. Exces-
sive protein intake may be associated with increased
excretion of calcium and so possibly exacerbate the
prevalence of osteoporosis. Excess intake of protein is
associated with increased risk of renal disease, espe-
cially in infants, since the kidneys have to excrete
excessive solute loads and so excess protein intake is
perhaps linked to the risk of developing high blood
pressure later in life. It is advisable that ministries of
health review their national recommended intakes to
insure that these are in line with current international
recommendations.
0023 Lessons learned over the past 50 years suggest
future food policies should insure that:
.
0024 cereal and potato production should be geared to
supply > 50% energy
.
0025 vegetables (excluding potatoes) and fruit produc-
tion should be geared to supply a consumption of at
least 400 g per day per person
Given the recommendations, contained in most diet-
ary guidelines, ‘to protect, promote and support the
consumption of cereals, potatoes, vegetables and
fruit,’ it is surprising that there was no mention of
the need to increase the production of these foods in
the country reports. Without a food policy which
guarantees food security in the form of cereals, pota-
toes, vegetables, and fruit, it is difficult to see how
national targets for a healthy diet can be achieved.
0026 One of the reasons why families living in countries
undergoing economic transition (CEE and CIS) are
not suffering from protein/energy deficiency is
because many produce a large percentage of their
own potatoes, vegetables, and fruit. In Russia, town
dwellers produce 88% of their potatoes, 43% of their
meat, 39% of their milk, and 28% of their eggs on
urban household plots. This important share of pro-
duction is generated on plots of 0.2–0.5 ha which
together constitute only 4% of the total amount of
agricultural land in Russia. In addition, imports from
abroad have supplemented national food production
and currently 50% of chickens and 30% of meat
consumed in the Russian Federation is imported. In
the short term, imports are essential during times of
hardship and economic transition, but in the long
term agricultural polices should promote sustainable
production and protect local food production to
insure national food and nutrition security.
0027In eastern Europe the agriculture sector forms a
much higher percentage of national gross domestic
product compared with western Europe. Almost 30%
of the population in some CEE countries are employed
in agriculture compared with only 1 or 2% in western
Europe. Many economists are concerned about the
impact when more countries join the EU because the
Common Agriculture Policy (CAP) is not sustainable.
The CAP receives almost half the EU budget and in
1995 it cost EU taxpayers 39 billion ECU. During the
CAP reform process, health recommendations and
dietary guidelines should influence the reformed
policy in addition to concerns about national employ-
ment and the national food security of the EU acces-
sion countries.
Protecting Health Through Food Safety and Quality
0028In some reports there was no mention of the import-
ance of food safety, especially in the countries of
southern Europe. As mentioned in the introduction,
it is vital to strengthen the collaboration between
food control and nutrition agencies. Some western
governments are already attempting to bring these
two disciplines under one food authority and three-
quarters (27 out of 35 countries) did include food
safety in their ICN reports. Close collaboration be-
comes even more essential as the line between food
safety and nutrition becomes more and more blurred
with the introduction of precooked foods; functional,
novel, and special dietary foods; and supplements.
Moreover, with the introduction of food into global
trade, the public’s need for information will be
immense. To provide reliable information, both food
safety specialists and nutritionists need data on food
intake patterns. More effective use could be made of
resources if joint surveillance and risk management of
food intake are carried out together.
0029Foodborne diseases are among the most wide-
spread health problems in the contemporary world.
tbl0004 Table 4 Food policy in the twentieth century
1950s 1960s 1970s 1980s 21st century
Food insecurity and perceived
nutrient deficiency, especially
protein
Increased food
production and
consumption,
especially of animal
protein and fat
Surplus stocks of
food, especially
animal products
Links identified between
mortality from NCDs and
diets high in animal fats
and low in vegetables
and fruit
The opportunity to
change food
policy to meet
health and
environmental
recommendations
NCDs, noncommunicable diseases.
4170 NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES

In rich and poor countries alike they impose substan-
tial health burdens, ranging in severity from mild
indispositions to fatal illnesses. The emergence of
new foodborne diseases is an ominous trend. Epi-
demics due to newly identified pathogens such
as Campylobacter jejuni, Listeria monocytogenes,
Escherichia coli 157:H7 and bovine spongiform en-
cephalopathy (BSE) have hit industrialized countries.
Salmonella outbreaks are one of the main causes of
epidemics in Europe. Global trade will make it
more difficult to contain foodborne diseases within
national borders and enforce national food laws. In
addition, chemical contamination, toxic materials,
pesticides, veterinary drugs, and other agrochemicals
require constant surveillance to insure their safe use.
Similarly, the use of food additives can improve the
quality of the food supply but appropriate controls
are necessary to insure their proper use.
0030 Most regions included in their country reports the
need to harmonize their national food legislation with
the EU and World Trade Organization (WTO). Many
countries stated they are lining up to join either the
EU or WTO (12 countries) and so intend to harmon-
ize their national legislation with international direct-
ives set by the EU or Codex Alimentarius. It is
essential that health professionals, especially those
working in public health, become more informed
about international agreements on global food trade
and take a full part in the WTO Committee on Sani-
tary and Phytosanitary Measures (SPS Committee).
Only if public health specialists, from both food
safety and nutrition, participate can they hope to
influence future food policies.
Promoting Breast-Feeding
0031 Clearly there is a lot to be done in the European region
to promote breast-feeding. More than one-third (13)
of the 35 member states made no reference to breast-
feeding in their country report. This does not neces-
sarily mean that there are no active breast-feeding
programs in the country (e.g., Romania) but it does
mean that there is probably little coordination be-
tween those responsible for nutrition policy and
those responsible for promoting breast-feeding.
Perhaps this is because breast-feeding is regarded as a
clinical issue dealt with by midwives and primary
health care workers. However, public health nutri-
tionists and hygienists in CCEE and the CIS do have
an important role and should be active in the develop-
ment of national policies to promote breast-feeding.
0032 National breast-feeding initiatives will only be
successful if policies are developed and enforced
according to guidelines from the Baby-Friendly
Hospital Initiative (BFHI) and the International
Code for the marketing of breast milk substitutes.
It is necessary to national and regional trends
(marketing strategies and breast-feeding levels) to
interpret the national situation and make recommen-
dations to policy-makers.
0033The BFHI jointly launched in 1991 by WHO and
UNICEF, aims to enable women to choose and prac-
tice breast-feeding as the primary source of nutrition
up to about 6 months by minimizing obstacles which
make it difficult or prevent women from exercising
their right to breast-feed and to insure the cessation of
free and low-cost infant formula supply to hospitals.
The BFHI targets maternity services and hospitals,
particularly health workers and those responsible
for policies to help mothers succeed in breast-feeding.
To become a baby-friendly hospital every facility
providing maternity services and care for newborn
infants should implement the Ten Steps to Successful
Breastfeeding outlined in the joint WHO/UNICEF
statement entitled Protecting, Promoting and Sup-
porting Breastfeeding: The Special Role of Maternity
Services and should end free and/or low cost supplies
of breast milk substitutes.
0034There is clearly a vital need to increase the number
of Baby-Friendly Hospitals in Europe and develop
and enforce national legislation which is based on
the International Code of Marketing of Breast Milk
Substitutes.
0035In some countries there may be conflict between
nutritionists, hygienists, and new breast-feeding
policies. Some hygiene standards and decrees in the
former Soviet countries, such as the recommendation
that mothers should be separated from their babies
after birth, contradict the current UNICEF and WHO
recommendations to promote the ‘rooming-in’ of
babies with their mothers. In addition, National Nu-
trition Institutes involved with research and develop-
ment of breast milk substitutes and weaning foods
may unintentionally interfere with breast-feeding
promotion.
0036Complementary feeding (weaning) was not dis-
cussed in detail in any report and only mentioned
very briefly in two country reports, those of Albania
and Italy. Perhaps this is because the categories listed
in the World Declaration of ICN do not specifically
include complementary feeding, only breast-feeding.
This was perhaps an oversight by the ICN committees
since it is clearly important that all member states
address their policies on infant and young child feed-
ing. It is around the age of 6–24 months when mor-
tality and morbidity levels are at their highest. It is
likely that the high prevalence of anemia seen in some
parts of the European region is due to poor feeding
practices, such as the early introduction of foods and
drinks, especially cows’ milk and tea, before the age
of 6 months.
NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES 4171

Caring for the Deprived and Vulnerable
0037 In the region around 70% of the population is
suffering from physical and mental exhaustion as
people cope with increasingly uncertain conditions
related to very rapid economic and social change.
This is especially true for the countries of the former
Soviet Union where policy-makers are not used to
developing safety nets for vulnerable groups. The
transition to a market economy has resulted in
soaring consumer prices due to a reduction in subsid-
ies while salaries have remained low. In addition there
is rising unemployment as a result of industrial
restructuring and the new monetary polices have hit
vulnerable groups in particular. Mechanisms must be
developed to identify and protect the vulnerable
groups in society.
0038 Caring for vulnerable groups was mentioned in
almost three-quarters (22) of the country reports.
Many initiatives were related to the physiologically
vulnerable, such as children, pregnant women, or
the elderly. In addition, welfare safety nets, aimed
at insuring a minimum family income by setting
minimum wages, pensions, and unemployment bene-
fits, were considered necessary for economically
vulnerable groups such as the poor, low-income, un-
employed, and refugees or immigrants and those with
large or one-parent families.
0039 The gap between the rich and poor is increasing in
many countries in Europe, and as a phenomenon of
the economic transition in central and eastern
Europe, unemployment has appeared in many. If
this trend continues, the food intake and nutritional
status of vulnerable groups should be monitored
closely in order to develop safety nets and prevent
food insecurity. Among European industrialized
nations the UK was exceptional in the pace and extent
of the increase in inequality in the 1980s and by 1990
the level of inequality was almost back to 1930 levels.
0040 Poverty is a growing concern in Europe, especially
for those with incomes below societies’ poverty lines.
In 1994 it was estimated that 13.5% of the Polish
population (about 5 million) had average monthly
expenditures lower than the relative poverty line. In
1995, 4 million children in the UK lived in families
with incomes below 50% of average earnings. Lack
of food is associated with poverty, which can be
measured by estimating the percentage of disposable
income spent on food: in Romania the average figure
is around 60%; and in Poland around 40%, com-
pared with 22% in the EU.
0041 Coping within a limited budget often means that
healthier, safer foods are not affordable. In Lithuania
increased food prices have caused socially deprived
people to consume cheaper, less nutrient-dense foods
which are more likely to be contaminated. In Poland
the prevalence of nutrient deficiencies is highest
amongst the unemployed and low-income families
with many children. Poor people in the UK consume
much lower quantities of vegetables and fruit.
0042There is growing evidence for the protective effect
of vegetables and fruit against chronic diseases such
as cancer and coronary heart disease. This suggests
that the low intakes of vegetables by poor people
may directly increase their risk of these diseases.
Inadequate diets also have adverse consequences on
a child’s health, education, and future employability
and there are demonstrable costs to society in each
instance.
Micronutrient Deficiencies
0043There is no doubt that, in the European region of
WHO, the most prevalent health problems related
to diet are noncommunicable diseases such as cardio-
vascular diseases and cancers and not deficiency
diseases. Nevertheless, micronutrient deficiency does
exist in certain European countries under certain
circumstances.
0044Iodine One of the most prevalent nutrient deficien-
cies is iodine. Iodine deficiency disorders (IDD) are
prevalent throughout Europe and only six countries
have no IDD (Finland, Iceland, Norway, Sweden,
Switzerland, and the UK). Although this problem
has been largely eliminated in some countries in west-
ern Europe, it is reemerging in some countries in CEE
and the CIS. For example, in Albania and Tadjikistan
iodine deficiency is severe and in some other countries
the prevalence of IDD is increasing.
0045The main public health strategy recommended to
solve this problem is universal salt iodization. This
means insuring that all the salt used by the food-
processing industry, the mass catering sector, and
households is iodized. In some countries there is no
universal iodization and only table salt is iodized
(Italy, Poland). This could be a problem, especially
in western Europe where most of the population get
their salt from processed food products and not from
home-cooked food to which salt is added during
cooking or eating. Therefore nutritional epidemiolo-
gists should monitor the source of a population’s salt,
and so iodine.
0046In addition to insuring that iodized salt is used in
food processing and mass catering, policy-makers
should consider the need to include a recommenda-
tion to feed iodized salt to animals (cows). In the
Nordic countries and the UK iodine is given to cows
in the form of ‘salt-lick’ and so milk and milk prod-
ucts supply around 40–70% of the iodine intake in
humans. In addition to insuring elimination of iodine
4172 NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES

deficiency, this has the added benefit of limiting the
amount of salt consumed by the population.
0047 In CCEE and the CIS, cardiovascular diseases are
responsible for 68% of all premature deaths, while in
the rest of Europe this figure is only 43%. Moreover,
proportionally, cerebrovascular diseases are mark-
edly higher in CCEE and CIS. Because of the strong
link between high salt intake and cerebrovascular
disease, the WHO recommends a salt intake of no
more than 6 g per capita per day. In Italy a campaign
on the role of salt in the diet was launched. This
campaign aims to eliminate IDD through the promo-
tion of iodized salt, but at the same time preventing
hypertension and vascular diseases through limitation
of salt intake.
0048 Iron The other main nutrient likely to be deficient in
European countries is iron. Iron deficiency was men-
tioned as a problem by one fourth (9) of 35 member
states. Prevalence studies show that anemia is wide-
spread in central Asia and the Caucasus. For example,
in Kazakhstan and Azerbaijan up to 70% of children
younger than 2 years of age have low hemoglobin
levels. In addition, 20–30% of women of child-
bearing age also have low hemoglobin levels. These
problems may not be related solely to iron deficiency
in the diet. For example, it has already been men-
tioned that early introduction of cows’ milk is a
major cause of iron deficiency in the young. Anemia
in adults is associated with the presence of iron-
absorption inhibitors in the diet, such as tea and
coffee, which is frequently consumed in eastern Euro-
pean countries; or lack of absorption enhancers, such
as vitamin C from vegetables and fruit.
0049 Folate Folate deficiency is associated with neural
tube defects. Denmark, Poland, and the UK men-
tioned national strategies related to solving this prob-
lem. Folate may also play an important role in the
prevention of coronary heart disease by helping to
reduce levels of homocysteine. The main food sources
of folate are Brussels sprouts, asparagus, spinach,
broccoli, cabbage, cauliflower, parsnip, iceberg let-
tuce, beans, peas, and beef and yeast extracts – yet
another reason why national food and nutrition po-
lices and dietary guidelines should promote vegetable
production and consumption.
0050 Other micronutrients There may be situations when
the only solution to solve micronutrient deficiency is by
food fortification of bread or salt, for example (such as
for iodine deficiency), or, more rarely, by supplements
(during emergencies). However, generally, where pos-
sible, WHO promotes primary prevention strategies
such as increasing vegetable consumption rather than
advocating consumption of nutraceuticals, food sup-
plements, or multivitamin tablets. Population strat-
egies advocating the use of vitamin supplements are
not the solution to micronutrient deficiencies in
Europe. Vitamin supplements may have many disad-
vantages: side-effects; nutrient imbalances; toxicity;
malabsorption; long-term dependence and lack of
confidence in locally produced foods, and, finally,
supplements are an unnecessary expense.
Appropriate Diets and Lifestyles
0051Countries of the CARs and the CIS must pay more
attention to the link between diet and noncommunic-
able diseases (NCD), such as cardiovascular diseases,
certain cancers, diabetes, hypertension, and obesity.
Some of the country reports focused too much on
deficiency of protein and micronutrients. In focusing
on deficiency the link between premature mortality
from NCD and a diet high in fat, salt, fatty red meat,
and fatty/sugary foods and simultaneously low in
vegetables and fruit is neglected.
0052Some countries in the CIS and central Asia men-
tioned the need to increase the teaching of dietology/
dietetics. There is still a tendency in some countries to
prescribe many different types of diets for different
disorders. Many of these dietary prescriptions have
not been scientifically proven. In addition, many of
the individuals referred for dietary treatment are
suffering from obesity, diabetes, heart disease, high
blood pressure, and other conditions related to un-
healthy lifestyles. These cases should be treated using
the healthy nutrition principles developed for the
population. Dental caries is also widespread in many
European countries and there can be little doubt that
this is related to frequent high intakes of sugar as well
as poor oral hygiene.
0053Some countries, such as Albania, Israel, Kazakh-
stan, Latvia, Romania, Slovakia, the Republic of
Moldova, Ukraine, and Uzbekistan made no mention
of the link between diet and NCDs. Moreover, only
one-third (12) of 35 member states mentioned obesity
(Austria, Azerbaijan, Czech Republic, Denmark,
Estonia, Hungary, Lithuania, Luxembourg, Malta,
Poland, Turkey, and the UK), despite the fact that
the prevalence of obesity is high and appears to be
increasing in every country in Europe. For example,
the Russian Federation has one of the highest preva-
lences, where 55% of the female population is over-
weight. Little mention of obesity probably reflects the
lack of data on body weight and height and illustrates
the need for countries to collect anthropometric data
as part of their health information system.
0054Physical activity and obesity Obesity is a chronic
medical problem caused by a combination of an
NUTRITION POLICIES IN WHO EUROPEAN MEMBER STATES 4173