Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


0012 Specification of the correct resins requires as much
understanding as that required by a diner choosing a
menu for a successful meal: no one would order Blue
Stilton to quench a thirst. Examples of the variations
in the nature of some synthetic resins are as follows:
1.
0013 PUs give all-round properties resulting from their
hardness, coupled with flexibility; the surface
preparation required to avoid their delamination
has to be more scrupulous than with, for example,
acrylics; PUs possess excellent acid resistance.
2.
0014 In general, acrylics are used for hardness and,
principally, color retention.
3.
0015 Polyesters carried in styrene offer quick cure and
good chemical resistance to some chemicals, but
produce a strong smell during application and
need a temperature of at least 10
C to cure satis-
factorily.
4.
0016 Epoxy types (i.e., epoxy–hardener two-pack
systems) are versatile in that the resultant proper-
ties can be varied by selection of the appropriate
hardener; they undoubtedly have excellent resist-
ance to alkalis and can be used in a solvent-free
form, but their resistance to marring and certain
chemicals is poor. (Marring is the phenomenon of
marks being left on a surface through the moving
contact of another over it. Epoxy-derived surfaces
are prone to this marring effect.)
5.
0017 Methacrylates cure quickly and at low tempera-
tures, and exhibit rapid hardening, but during
application they give off a pungent smell which
dissipates quickly. (They are used, with special
care, extensively in Europe in food factories and
breweries.) Again, chemical resistance properties
vary with relation to specific chemicals.
The methods of curing of the above resins differ
widely, from using the moisture in the atmosphere
to requiring a peroxide catalyst (when it is known as
a free radical mechanism).
Floors
0018 There has long been a search for a floor finish that is
as near perfection as possible, and the arguments
concerning seamless surfaces and tiles have continued
for some years.
0019 In the years since 1945, seamless resin-based floor
finishes have developed considerably from small begin-
nings. Initially they were mainly to be found in the form
of clear varnishes or paints based on synthetic resins
such as alkyds and phenolics, which gave harder coat-
ings than the traditional types then available.
0020 Using resins as binders for fillers and/or aggregates
to produce polymer concretes or screeds (self-leveling
or troweled) began to be feasible with the exploitation
of the emerging technology associated with epoxy
resin chemistry. Since then, other polymers have
come to the fore in this applicational area; PUs, un-
saturated polyesters, and methacrylates are perhaps
the most prominent. The substitution of part of the
water component of a cementitious formulation with
a thermoplastic emulsion resin, in order to offer a
moderately upgraded performance over the unmodi-
fied original, yielded an economical product (so-
called polymer concrete but, more correctly,
polymer-modified concrete).
0021When there is a new development in any area, there
are usually two positive reactions amongst those who
are to specify their use. One is to resist the trend, to
adhere to the traditional methods or products and
look for examples of failures that argue for this atti-
tude. Caution is to be applauded and encouraged, but
not if it means totally resisting cost-effective improve-
ments. The opposite situation is perhaps more
frightening in that a specifier welcomes a new devel-
opment with open arms and wishes to use it at the
slightest provocation. The disastrous consequences
can be heightened by the fact that the first few instal-
lations may be successful and the next, failures.
0022It must be firmly established that no single syn-
thetic resin will offer all of the properties that will
cope with the varying in-service requirements pre-
sented to the specifier, whether it be in connection
with a new floor area or a refurbished one. For
example, the solvent resistances are quite different,
as are the resistances to specific chemicals. Physical
properties associated with impact, abrasion, elonga-
tion, and hardness also differ widely. Consideration
during application of health and safety, and particu-
larly odor, are also of considerable relevance.
0023The retardation of the rate of acceptance of all
seamless resin-based floors has been caused by high-
lighting the failures rather than the greater majority
of successes. These failures have, in the main, been
attributable to the following, and stating them will
not only be of historical interest but act as a caution-
ary and educational exercise:
1.
0024Lack of basic understanding by specifiers of the
substance, nature, and properties of synthetic
resins and the formulated derivatives.
2.
0025Lack of experience of many self-styled ‘specialist’
contractors in installing the systems on the one
hand, and a lack of basic understanding of this
particular medium to cope with the unexpected
on site, on the other.
3.
0026Lack of site knowledge by certain of the formula-
tors of the systems, resulting in the systems not
being ‘workman-proof,’ but only ‘technologist-
friendly’!
2238 FACTORY CONSTRUCTION/Materials for Internal Surfaces
Indeed, in many cases the decision as to whether a
coating (measured in mm) or a screed (measured in
mm) should be laid is made without real understand-
ing and often decided purely on cost – a sure recipe
for disaster! A specific procedure for preparing the
surface to take the finish is essential.
Coatings
0027 In order simply to keep the level of dusting of
concrete down, impregnation or coating with a clear
resin is satisfactory. Acrylics, methacrylates, PUs or
epoxy types, in unmodified or clear form, give good
results. As far as impregnation or priming is con-
cerned, the variable porosity of a concrete surface
must first be taken into consideration; in this respect
just one application of the resin may not seal the
surface as, in areas of high porosity, there will be no
resin present on or at the surface. In such cases add-
itional applications have to be made until a satisfac-
tory state is arrived at; if much extra solvent-carried
medium has had to be added, the surface must be
allowed to vent before proceeding further.
0028 Clear or pigmented (paint) multicoat systems are
suitable where the substrate is smooth or of very low
profile. Antislip characteristics can be built in by
casting fine sand in an intermediate film.
0029 Perusal of trade and academic literature will pro-
vide information concerning the respective chemical
resistance of the various resin species. Various key
facts must be elicited and thence a specification
drawn up in an informed way.
Screeds
0030 If a substrate is pitted, potholed, or simply uneven,
or has special requirements, a screed is needed. By
substituting part of the water in a cementitious for-
mulation with a thermoplastic emulsion, the so-called
polymer screeds are constituted. These provide
nondusting flat surfaces of varying hardness and cer-
tainly upgrade the ‘straight’ cementitious finish.
However, they do not have the degree of chemical
and abrasion resistance often required in industry.
This is where other synthetic resins come in – epoxies,
PUs, acrylics, and methacrylates. These are now well-
known, and success is achieved by combining the
most advantageous combinations of resin and aggre-
gate (the selection of the latter plays a major part as
far as wear and antislip properties are concerned).
The main two methods of application are by trowel
or, where a formulation where self-level is used, by
pouring.
0031 One of the requirements of the food industry, as
mentioned before, is a sterile floor; in order to achieve
this, the topping must give an excellent BS 4247
rating. One method, of course, is to steam-clean or
to use virtually boiling water. Many systems, such as
epoxies, do not possess a high enough heat distortion
temperature to resist such daily treatment and, as a
result, develop hairline cracks (thermal degradation).
To some extent this can be overcome by introducing
some elasticity, but the solution is to use a medium
that does possess a high distortion point.
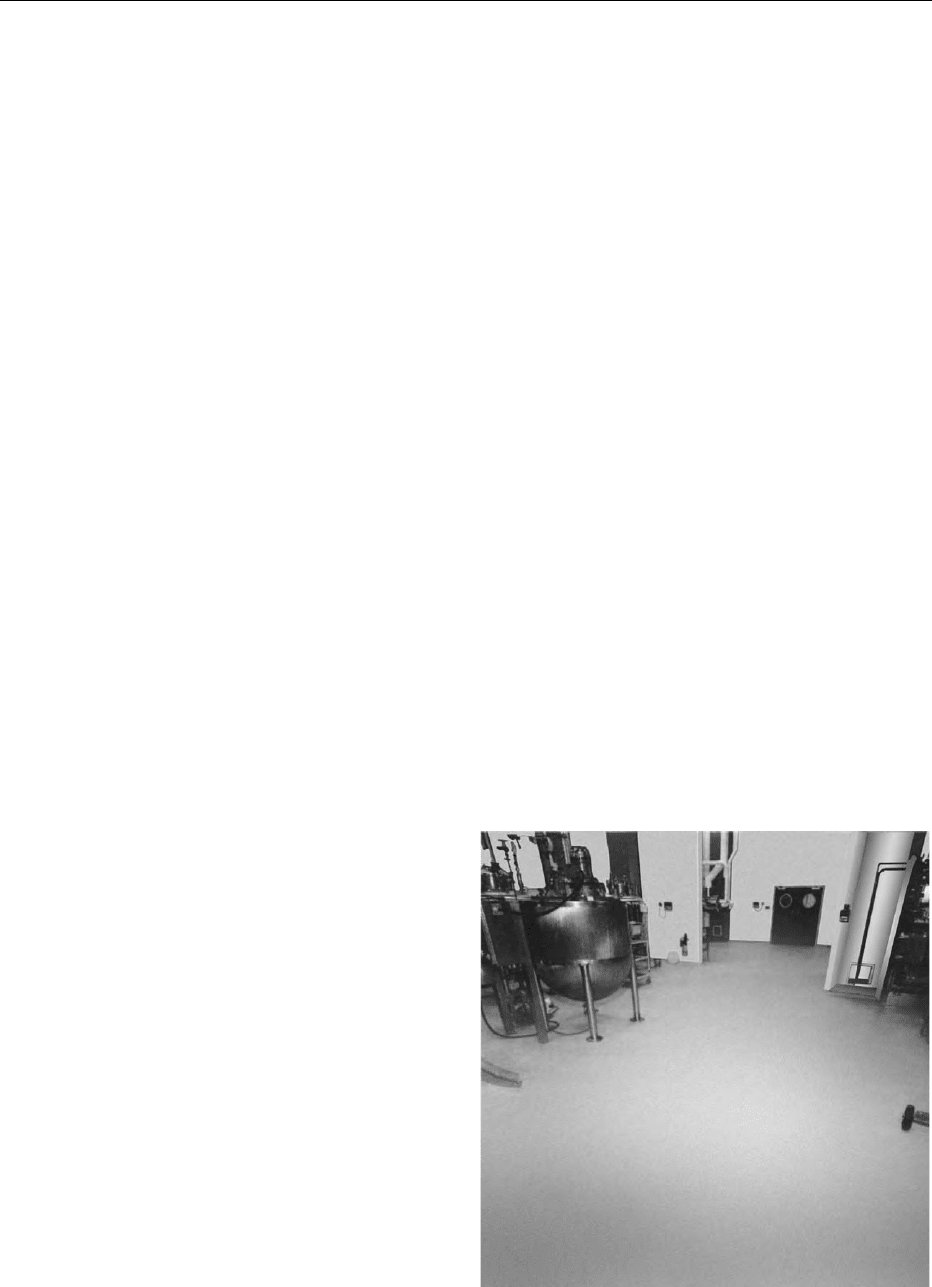
0032Another approach is to utilize a PU-modified con-
crete; this has been done and improvements are still
being made (Figure 1).
0033Table 1 details the characteristics of a typical
epoxy-based screed. Choosing from a wide variety
of hardeners which, with the epoxy resin itself, form
the two-pack system, a wide variation of properties
can be achieved.
0034Table 2 details the characteristics of a typical PU-
modified concrete used where high heat distortion
temperatures are required, together with excellent
physicals.
0035Table 3 proposes a scheme for the project manager
to follow when installing a resin floor.
0036Finally, one very important matter, often over-
looked, is cleaning or aftercare. The chemicals used
previously may well not be at all appropriate for the
resin-based surface, and it is the duty of the formula-
tor, through the contractor, to identify the best means
and detail it in the relevant technical data sheets. (See
Cleaning Procedures in the Factory: Types of Deter-
gent; Types of Disinfectant; Overall Approach;
Modern Systems.)
fig0001Figure 1 Polyurethane-modified concrete laid by Swansback.
Photographic Unit of the Boots Company plc.
FACTORY CONSTRUCTION/Materials for Internal Surfaces 2239
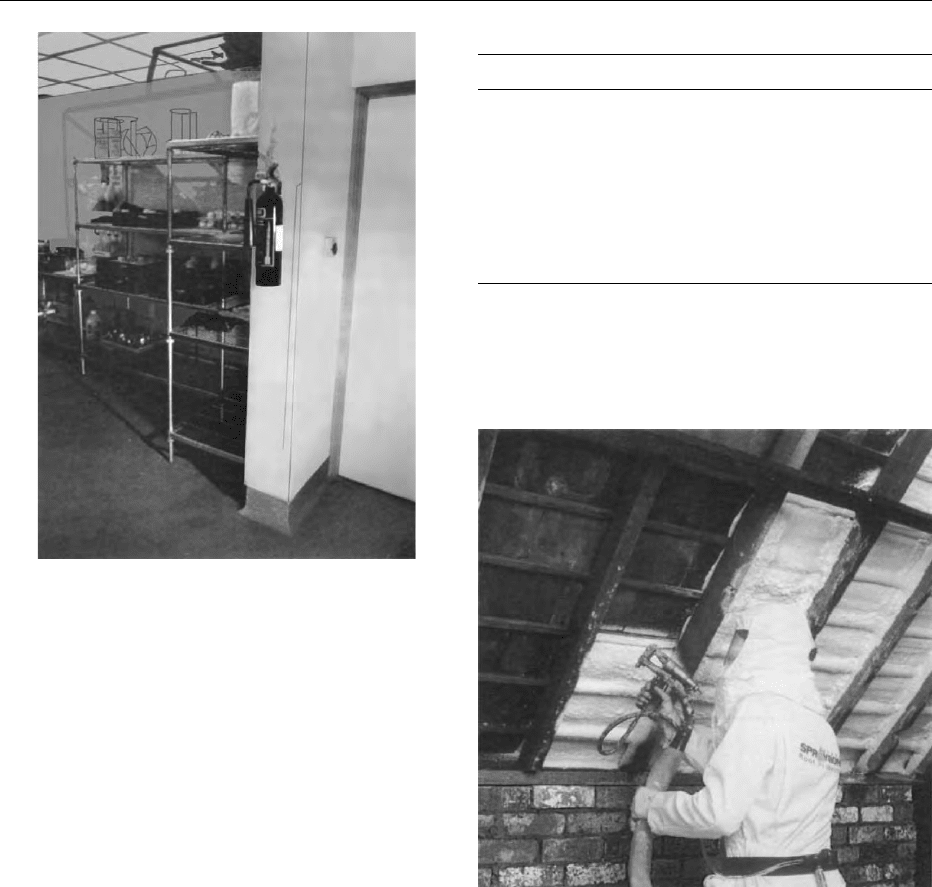
Walls
0037 Much of the reasoning and statements contained in
the Floors section of this article apply to walls. For
example, a seamless surface is usually easier to keep
sterile than a grout-containing tiled surface, although
in many situations tiles are preferable. A good
example of the latter is in the corridors of the London
Underground system where gouging and graffiti are
made very difficult by using specific and glossy tiles;
but here sterility is not a significant factor.
0038 In the food industry, as in industry as a whole, the
wall finish must resist the chemical and physical
attack of the inherent service conditions. For example,
it is quite common to steam-clean and, in such cases,
the basic resin in the finish is required to (but does not
always!) possess a sufficiently high heat distortion
temperature to resist the frequent expansions and
contractions.
0039 It has been firmly established by psychologists that
the color and texture of surroundings have a great
effect on the mental attitude of those in the vicinity.
This is not surprising when one considers the effect
the sun has on all of us when it comes out. Until 20
years ago, there was no pressure to arrange for the
decor in the fitting shop to be the same as that in the
chairman’s office. Although this attitude has changed
in essence, the desire could not be sensibly realized
owing to the technical shortcomings of available pres-
tigious wall finishes. In other words, the formulation
of multicolored and textured systems of classical or
upmarket appearance has never been a problem, but
the technical inadequacies of the systems did not
make them suitable for the more demanding service
conditions found in food industry situations.
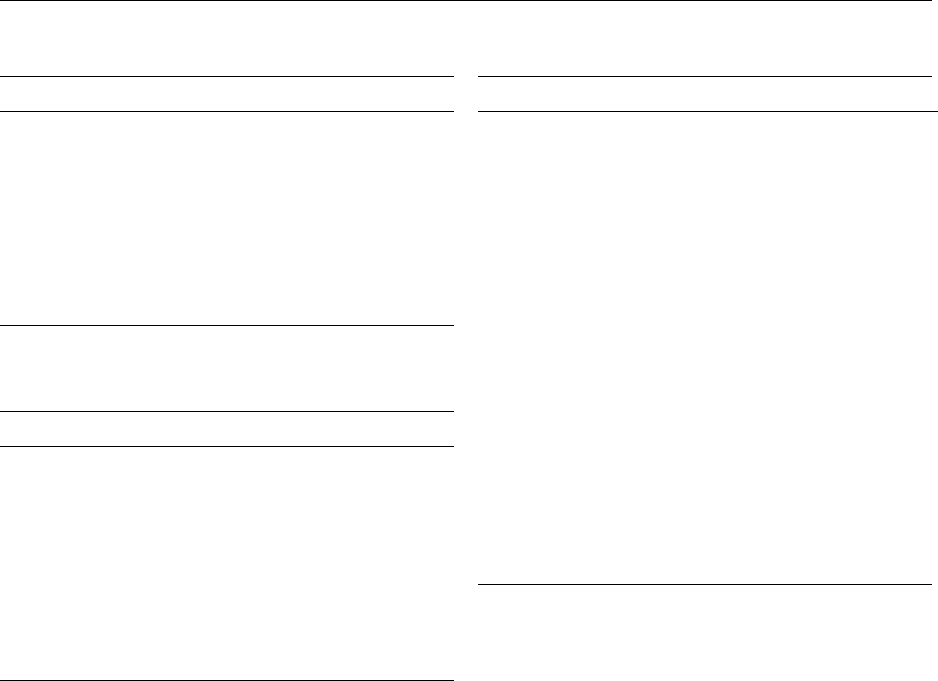
0040Multicolored, durable, and resistant coatings have
been around for some time, but they have been paint-
like and thus of flat profile (Figure 2); in addition, the
application of more than one coat was required, thus
involving considerable labor costs. They have also
been associated during application with the unpleas-
ant smell and fire risk characteristic of solvents. This
has meant either causing aggravation amongst those
working in the vicinity, or carrying out the particular
project only when the building was totally vacated;
the suitable time for application was therefore some-
what restricted. Textured systems have often had an
upmarket appearance suitable for the chairman’s
office, but lacked the physical and chemical resistance
properties needed for more aggressive service condi-
tions, or they have had the necessary degree of resist-
ance but not the necessary classical and upmarket
appearance needed for the more prestigious sites.
tbl0001 Table 1 Typical characteristics of an epoxy concrete (filler and/
or aggregate and resin)
Characteristic Value Units
Compressive strength 55–110 N mm
2
Compressive modulus 0.5–20 kN mm
2
Flexural strength 25–50 N mm
2
Tensile strength 9–20 N mm
2
Elongation at break 0–15 %
Linear coefficient 25–30 10
6
per
C
Water absorption (7 days at 25
C) 0.1 %
Maximum service (temperature
under load)
40–80
C
Rate of development of strength 6–48 h at 20
C
tbl0002 Table 2 Typical characteristics of a polyurethane-modified
concrete
Characteristic Ucrete HF Concrete (124)
c
Density 2090 kg m
3
2250 kg m
3
Compressive strength 50 N m
2
27 N m
3
Elastic modules
(compression)
1200 N m
3
21 000 N m
2
Tensile strength 6 N m
2a
2.1 N m
2b
Flexural strength 14 N m
2
3.5 N m
2
Coefficient of thermal
expansion
1.5 10
5
per
C1.1 10
5
per
C
Thermal conductivity 1.1 W m
1
per
C 1.3 W per m per
C
VICAT softening point 130
C
Surface resistivity 3 10
8
O 4 10
4
O
a
1800 lbs in
2
.
b
300 lb m
2
.
c
(124) means 1 part cement, 2 parts sand and 4 parts aggregate.
tbl0003Table 3 Suggested scheme for managing a resin-based floor
installation
Stage effort Item
60% Evaluation
a
History of substrate
Past usage
Service requirements
Identification of appropriate system
and preparation
Installation constraints
Specification settled
Selection of proficient contractor
20% Installation I
(preparation of the
surface)
Contractor efficiency
Achievement of suitable surface state
Grinding, scrabbling, or shotblasting
Rectifying deficiencies
Lack of damp-proof membrane
(DPM)
Contamination
Unevenness
Slope
20% Installation II
(application of system)
Contractor efficiency
Scrupulous following of
instructions
Adequate barriers and notices
Client cooperation
Employee discipline
a
Using, in part, a formulated questionnaire.
2240 FACTORY CONSTRUCTION/Materials for Internal Surfaces
0041 Thus the way has been open for some time for
systems of virtually universal suitability, with
minimum hazards on application, and the ability to
provide textured or smooth finishes. These are now
gradually becoming available, especially utilizing the
properties of PU-based systems which are no longer
handicapped by yellowing on exposure to light.
0042 Within reason, what applies to floors applies to
ceilings. Thus, by using resin-based systems, a com-
plete hygienic envelope can be achieved for floor,
walls, and ceiling.
Roof Stabilization
0043 Many factories in the food industry were built before
World War II and consequently have tile roofs. These
can become unstable with the passing years. Puresin-
sprayed systems have been developed to secure and
stabilize these structures internally without complete
rebuilding.
0044 Stability and insulation are achieved through tech-
nically advanced closed-cell, rigid polyisocyanurate
(or related) foams which are tailor-made for the pur-
pose with British Board of Agre
´
ment (BBA) approval.
Application is by spray at right angles to the prepared
underside of tiles or slates of a roof requiring refur-
bishment. The latter procedure, coupled with a very
fast-curing or setting time, insures that foam does not
run out from between the tiles or slates and down the
outer surface of the pitched structure. Such foam has
fire-retardant qualities, passing class 1 (BS 476 part 7,
1971). Typical characteristics of the system are shown
in Table 4.
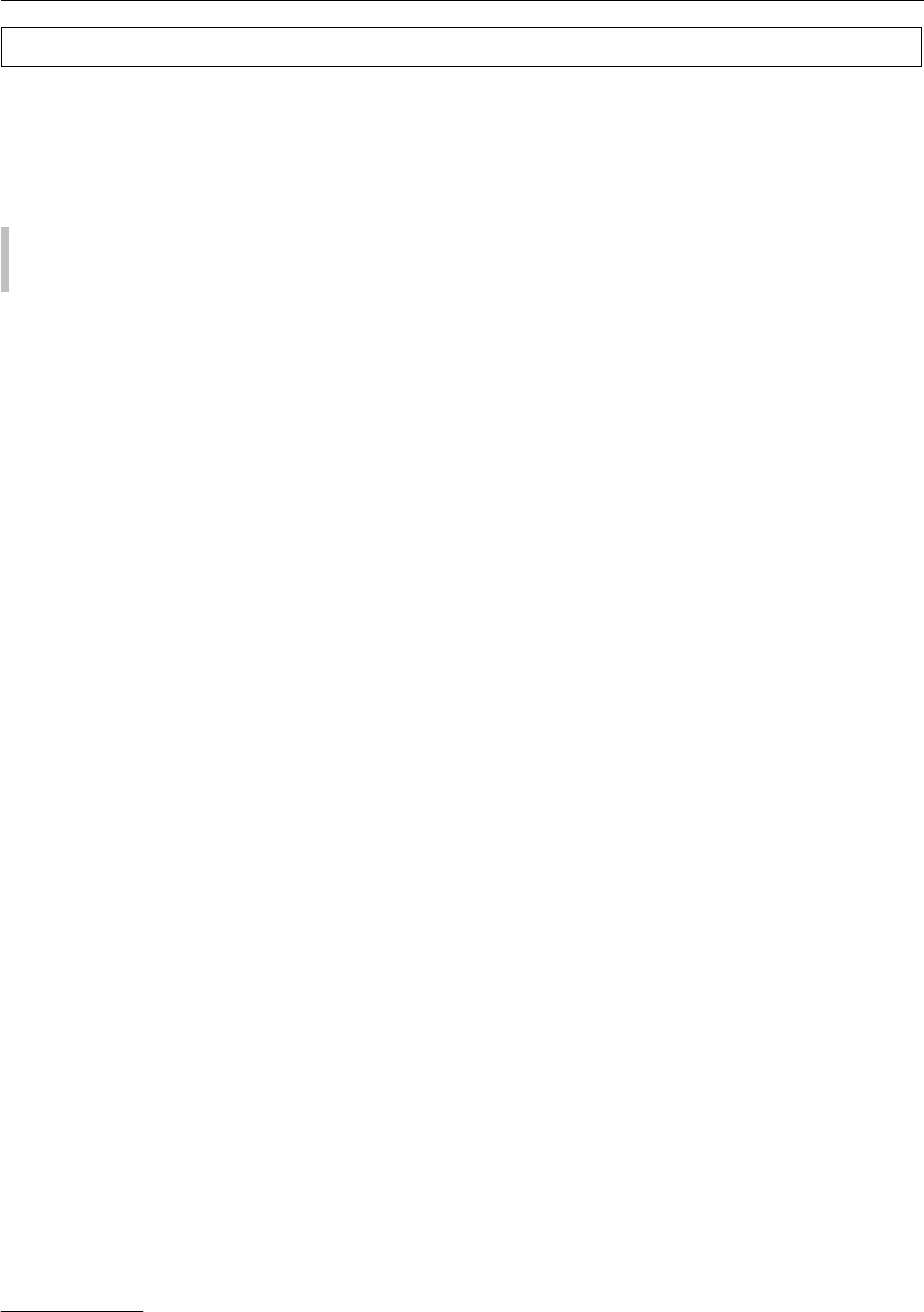
0045As with all resin-based systems, the installation
must be carried out by trained and experienced con-
tractors who can appraise the site as being suitable,
recognize and carry out the vital preparation work,
and spray the system correctly. In addition, they
should insure that the roof space is adequately venti-
lated to avoid structural deterioration through
condensation (Figure 3).
0046The foam is sprayed between (not over) the rafters
and the purlins and over the battens (i.e., on their
fig0003Figure 3 Stabilizing polyurethane Spraybond foam being
applied. Courtesy of Liquid Polymers plc.
fig0002 Figure 2 A polyurethane-based wall finish by Sempol Surfaces
Ltd in association with an epoxy seamless floor in a food factory.
tbl0004Table 4 Typical stabilizing foam properties
Property Value
Closed-cell content 90% minimum
Thermal conductivity
a
Initial 0.017 WMC
Aged 0.020 WMC
Water vapor transmission
b
10.6 mg per Nh
c
Service temperatures 50
Cto70
C
Density (overall) 42 kg cm
3
(approximate)
Tensile strength 117 kPa
Shear strength 77 kPa
Burning characteristics See text
a
See comments in text on roof ventilation and insulation.
b
25 mm thick at 30
C, 88% relative humidity.
c
Nh are Newton hours.
All tests results according to BS 4370.
WMC, watts per square metre per Kelvin.
FACTORY CONSTRUCTION/Materials for Internal Surfaces 2241

inside face), leaving the outer face uncoated and thus
allowing moisture evaporation. A foamed thickness
of 25 mm is preferred. Before expanding (foaming),
the liquid penetrates cracks and joints and, on curing
as a foam, bonds the slates or tiles, thus increasing the
stability of the structure chiefly against the force of
winds.
0047 In the industrial context, the duration of applica-
tion will depend on the surface area of the structure
which may, of course, be of considerable size. A single
day is all a house-sized roof will take.
0048 As already mentioned, a roof thus treated will be
sealed against wind, driven rain, and snow, i.e., storm
conditions. However, it must be noted that this will
not prevent leaks owing to cracked or displaced tiles,
slates or faulty flashings, valleys, and gutters. These
are avoided by correct, appropriate preparation of the
roof before refurbishing with the system.
0049 Being one of the best insulants commercially avail-
able, the foam, when of the order of 25 mm thick,
achieves a degree of improved insulation that should
be approximately 0.8 W m
2
per
C. Because of this,
coupled with good ventilation, the chances of conden-
sation are reduced.
0050 There are other attractions associated with this
method of refurbishment. It is carried out at a lower
cost than reroofing. The application is easy, being
from inside the roof, so that no scaffolding is re-
quired. Furthermore, there is minimum disturbance
of below-roof activity during the initial installation.
Final Comments
0051 Most problems stem from lack of knowledge of the
nature of the synthetic resin involved. Such knowl-
edge must be acquired through the medium of either
an informed contractor, fair-minded suppliers who
are prepared to say ‘you need a system based upon a
type x resin which we do not make’, or an independ-
ent resin consultant. The academic institutions can
help considerably by including far greater input on
the basic subject of synthetic resins in their syllabuses
for graduate courses in architecture, civil engineering,
and surveying.
0052 An informed, experienced, specialist contractor is
essential and can often be identified by the fact that
the company has existed for a considerable number of
years and can offer visits to past installations or, at
least, produce a substantial list of case histories and
offer good postinstallation technical service. The
basic technical knowledge referred to above is likely
to be present if the contractor formulates his or her
own systems, and is not purely a ‘menu-reader’ of
material suppliers’ literature which cannot hope to
cover all of the potentially threatening situations
arising on site.
0053For success, not only should a system based upon
the correct resin be selected, but also a good major
percentage of the effort put into the project should be
in preinstallation activity by way of full appraisal
of the site, coupled with the resultant, specifically
appropriate substrate preparation. Sadly, all too fre-
quently this is carried out after, for example, a floor
finish has failed, and only then do protimeters and the
like appear on the scene! A protimeter is an instru-
ment which measures the degree of moisture in a
surface (concrete) by means of a probe and the read-
ing on a dial of a small current of electricity which
indicates the percentage moisture. Increasing the
depth of the hole into which the probe is placed
allows moisture levels at different depths to be deter-
mined – so quantifying ‘rising damp.’
See also: Cleaning Procedures in the Factory: Types of
Detergent; Types of Disinfectant; Overall Approach;
Modern Systems
Further Reading
Jolly AC (1965) Polyurethane floor coatings. Flooring and
Finishing News 10(5): 33, 34, 37, 38.
Jolly AC (1968) Seamless flooring in the can. Cleaning and
Maintenance (4): 22, 23, 25, 26, 53.
Jolly AC (1979) A hundred years of resins. Polymer Paint
and Colour Journal 169(4001): 514, 515.
Jolly AC (1982) Seamless floors versus tiles. Polymer Paint
and Colour Journal 172(4062): 10.
Jolly AC (1985) Resin floor finishes. Architects’ Journal
181(6): 63–66.
Jolly AC (1987) Educating for change. Construction Sur-
veyor 21(64): 9, 10.
Jolly AC (1989a) Elastic, seamless roof finishing. Architects
and Surveyors Institute Journal 1(1): 29, 30.
Jolly AC (1989b) Seamless resin floors in perspective.
Building, Trade and Industry 5(4): 28, 29.
Jolly AC (1989c) Stabilising roofs using foam technology.
Dairy Industries International 54(10): 36, 37.
Jolly AC (1990a) Getting the seamless floor right. Building
and Maintenance May/June, pp. 11, 12.
Jolly AC (1990b) Are the technological advances available
being fully utilised? Building and Maintenance Sept/Oct,
pp. 7, 8.
Jolly AC (1990c) The dangers of surface knowledge. Dairy
Industries International 56(11): 25, 27.
2242 FACTORY CONSTRUCTION/Materials for Internal Surfaces
Factory Inspection See Hazard Analysis Critical Control Point
FAMINE, STARVATION, AND FASTING
E M Widdowson
y
and A Ashworth,LondonSchoolof
Hygiene and Tropical Medicine, London, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 Despite man’s ingenuity and technological advances,
it is a sad reflection that at the start of the twenty-first
century, famine and starvation still abound, often
with such catastrophic loss of life that it can be meas-
ured in millions. Indeed, ‘food security’ has become
an industry, and ‘humanitarian assistance’ the voca-
tion of a burgeoning number of organizations who do
nothing else. It is a damning indictment of our times
that when the medical relief organization Me
´
decins
Sans Frontie
`
res was awarded the Nobel Peace Prize,
they were working in over 80 countries.
0002 We shall examine the causes of famine and starva-
tion, both past and present, and some of the physio-
logical changes that have important consequences for
those looking after the afflicted. We shall also look
at fasting and starvation in the midst of plenty, in
particular anorexia nervosa and bulimia.
Causes and Effects of Famine
0003 Famine can be defined as a prolonged scarcity of food
causing many in a district or country to die from
starvation and/or disease. In communities dependent
on subsistence farming, ‘hungry seasons’ are not
uncommon, but coping strategies exist to mitigate
the adverse effects and insure survival. For example,
nonessential items may be sold and debts called in,
and there may be greater use of wild foods. What
distinguishes ‘famine’ from ‘hunger’ is that in famine,
the usual coping strategies are insufficient. Thus
famines are characteristically accompanied by ex-
treme measures that may disrupt future livelihoods,
for example, the selling of animals, land, and other
essential items. In a famine, families are often driven
to eat unconventional items, such as rodents, beetles,
worms, roots, leaves, bark, grass, candles, and leather.
0004 Famines have occurred from time to time through-
out history, and there are many records of them in
early writings, such as the Bible. In general, they were
caused by crop failure due to droughts, floods or
pestilence (e.g., locusts, blight). In Europe in the
Middle Ages, they were often accompanied by out-
breaks of typhus, cholera, typhoid, dysentery, small-
pox, measles, and scarlet fever, and famine led to their
spread and severity. In more recent times, misguided
political gambits have caused disastrous food short-
ages, as witnessed by the famines in the former Soviet
Union and China, where privately owned small farms
were merged into collectives and crops procured by
the State to provide the wealth to support industrial-
ization. Some 30 million people are estimated to have
starved to death in China during Chairman Mao’s
Great Leap Forward.
0005Starvation may be used as a political tactic and
knowingly engineered (as in the internment camps
of Belsen). Incongruously, countries gripped by
famine often continue to export staple food crops,
as was the case in the Irish famine of the 1840s and
more recently in the famines in Ethiopia and Sudan.
Mass movements of populations in search of food or
fleeing from conflict situations have become com-
monplace on our television screens. Tented camps
and humanitarian aid may be a refuge from starva-
tion, but thousands of people with weakened immune
systems living in close proximity are vulnerable to
epidemic diseases, and many die as a result. Table 1
shows some of the twentieth century famines and the
estimated number of deaths.
0006Increasingly, famines are linked with ineffective
political structures, armed conflicts, environmental
degradation, and ethnic or religious unrest emanating
from disregard of civil and human rights. The effects
are wide-ranging. The use of land mines, for example,
limits access to local markets and hampers food relief
efforts in the short term, but also continues to kill,
maim, and disrupt agricultural production in the
long term, as seen in Mozambique, Angola, and
Somalia. Forced conscription of young men for
combat adversely affects food production and food
security in rural areas, and arms purchases divert
foreign exchange from already under-resourced
health and development budgets and deter inward
economic investment. Evidence of the effects of
climate change can be seen in unusually prolonged
periods of low rainfall at one extreme and increased
y
Deceased.
FAMINE, STARVATION, AND FASTING 2243
frequency of hurricanes and floods at the other. These
wreak havoc to crops and livelihoods, decrease soil
fertility, increase erosion, desertification and salina-
tion, and disrupt transport routes. These factors,
however, are associated with famine only where
populations are chronically poor. Hence, combating
poverty is a major concern in famine prevention and
mitigation.
Structural and Physiological
Consequences of Undernutrition and
Starvation
0007 Starvation implies that little or no food is eaten.
Undernutrition arises when some food is eaten, but
the amount is insufficient to meet physiological and
metabolic requirements. In many ways, the effects
of starvation and undernutrition are the same, and
the differences are those of degree. It goes without
saying that a starving or undernourished person loses
weight, but the organs and tissues lose weight at
different rates. The least essential tissues suffer first;
hence, adipose tissue is mobilized and the fat oxidized
to provide the energy necessary for the metabolic
processes that must go on if life is to be preserved.
0008 Some loss of nitrogen is inevitable despite the in-
creased production of free fatty acids, and this comes,
to a large extent, from the proteins of skeletal muscle,
leading to shrinkage of the muscle fibers. The break-
down of muscle proteins provides the amino acids
alanine and glutamine, whose carbon skeleton can
be used to make glucose. The skin also loses protein,
both structural and cellular, and becomes thin and
easily infected. The loss of its protein, together with
the loss of subcutaneous fat, makes the skin hang
loosely on the bones.
0009The internal organs lose weight, the liver some-
times a great deal. In edematous malnutrition, how-
ever, the liver may increase in weight by as much as
50% owing to the accumulation of fat, which is
caused, at least in part, by a reduced synthesis of
lipoproteins that transport triglycerides out of the
liver and into plasma. The alimentary tract loses
weight and becomes thin, and there are marked
changes in the gut mucosa, especially the villi, which
become flattened and broader, and have reduced
levels of digestive enzymes. The heart and kidneys
tend to lose weight in parallel with the body, and
their function is impaired. The brain is preferentially
protected, although there is a reduced density of
neuronal synapses and dendrites.
0010Healthy, well-nourished individuals operate with
considerable ‘spare capacity.’ Thus, our bodies are
able to respond when we run very fast or eat a very
large meal. This excess capacity, however, is ex-
pensive to maintain, and when food intakes are
insufficient, it is reduced to conserve energy. This
‘down-sizing’ of the body’s functional capacity affects
every system, organ, and cell, and is termed ‘reductive
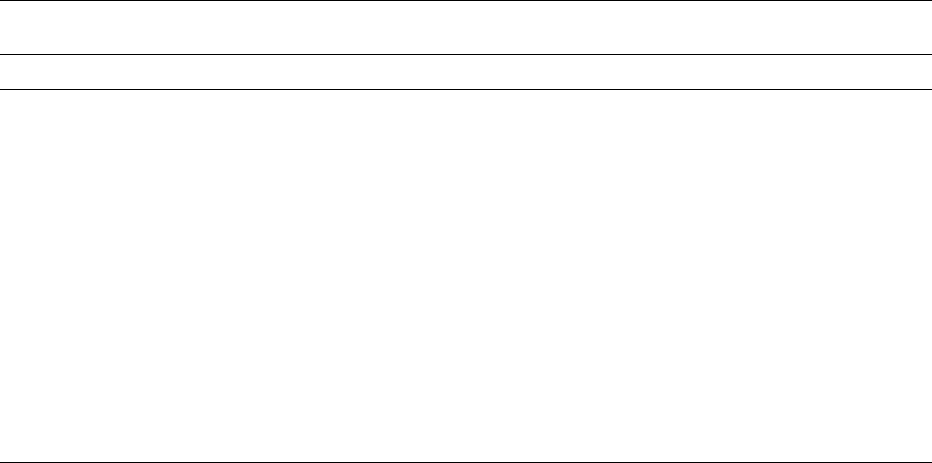
adaptation’ (see Figure 1). One example of reductive
adaptation is the slowing down of the sodium pump
in cell membranes. The purpose of this pumping
activity is to maintain the correct concentration gra-
dient, and it normally accounts for about one-third
tbl0001 Table 1 Selected twentieth century famines.
Year Location Number of deaths Notes
1899–1900 India 1 million Drought
1915–1918 Germany 200 000 War
1918–19 Uganda 4 400
1920–21 North China 500 000 Drought
1921–22 Russia, Ukraine and Volga region 1.3–5 million Drought
1928–29 China, Shensi, Honan, and Kansu 3 million
1932–33 Russia 3–10 million Collectivization
1941–43 Greece 450 000 War
1941–44 Leningrad 1 million War
1941–42 Poland, Warsaw 43 000 War
1943 Ruanda-Urundi 35 000–50 000
1943–47 India, Bengal 3 million Drought and war
1958–62 China 30 million Collectivization and natural disasters
1967 India, Bihar Relief operations mitigated the effects of
the disaster
Drought
1971–73 Ethiopia 1.5 million Drought
1988 Sudan 250 000 in Bahr El Ghazal War
1998 Sudan 60 000 War
a
Adapted from Alamgir M (1981) An approach towards a theory of famine. In: Robson JRK (ed) Famine: Its Causes, Effects and Management. London:
Gordon and Breach Science and Watson F (1999) One hundred years of famine – a pause for reflection. Field Exchange Issue 8: 20–23.
2244 FAMINE, STARVATION, AND FASTING
of the basal energy expenditure. Although energy-
sparing, this slower pump rate is not entirely benefi-
cial, as it allows sodium to accumulate inside cells and
potassium to be lost, thus contributing to potassium
deficiency. There are several serious consequences of
potassium deficiency, including fluid retention and
edema, and impaired cardiac function. Other func-
tional changes in starvation include a slower heart
rate, reduced ability of the kidneys to excrete excess
sodium and excess fluid, which increases the risk of
heart failure, and reduced ability to make glucose,
increasing the risk of hypoglycemia and hypothermia.
Thus, there are both positive and negative conse-
quences of ‘reductive adaptation’.
0011 The resting metabolic rate per kilogram body-
weight is not greatly reduced in moderate undernutri-
tion, but in a starving person, it ultimately falls, as
does body temperature. In moderate undernutrition,
the digestive tract functions normally, provided there
is no infection, but in a starving person, diarrhea may
become severe. This has been attributed, at least in
part, to the colonization of the normally sterile upper
intestine with bacteria, which then produce toxins,
damaging the gut mucosa and increasing fluid
secretion into the gut. The dehydration resulting
from this may prove fatal. In addition, some of these
bacteria deconjugate bile salts, reducing the body’s
ability to absorb fat.
0012The survival time of an adult who takes no food
depends upon the availability of clean water. If plenty
of water is available, a previously well-nourished
adult can survive without any food for about 60
days – the exact time depending partly on the amount
of fat in the body. Starving or near-starving infants
and young children are in a far worse plight, particu-
larly if they are also short of water, because their
requirements for energy and water per kilogram
bodyweight are greater than those of adults.
0013Extreme wasting occurs among hospitalized
patients, the causes varying with the nature of the
disease or type of trauma. Some conditions, including
cancer, markedly depress the appetite leading to semi-
starvation as a result of low food intake. Some condi-
tions lead to actual loss of nutrients, for example
gastrointestinal diseases and postoperative drainage.
Injury and infections trigger an increased demand
for nutrients to fuel the immune response, including
amino acids for the synthesis of acute phase proteins.
These are derived from muscle protein breakdown,
causing wasting. Malnutrition in hospital, however, is
also often the result of prolonged underfeeding due to
inadequate or inappropriate nutritional support.
Even in affluent countries, as many as 50% of hospi-
talized patients are malnourished.
Refeeding after Undernutrition and
Starvation
0014When World War II ended in Europe in May 1945,
several groups of doctors and nutritionists went to the
liberated camps to supervise the feeding of the starv-
ing inmates. It was generally believed that the digest-
ive tract would not be able to tolerate food for some
time, and that intravenous feeding would be neces-
sary in the early stages. This proved not to be true.
The previously starving men had good appetites and
took very large amounts of food (25–42 MJ, 6000–
10 000 kcal per day). They gained about 10 kg in 6
weeks, and the response was similar in young and old
men. The same is true for severely malnourished chil-
dren. After a few days of treatment, they become very
hungry and will double their food intake and gain
weight very rapidly. After a few weeks, when their
weight deficit has been corrected and they approach a
normal weight for their height, their appetites and
food intakes revert back to levels appropriate for
well-nourished children of a similar size.
0015The physiological and metabolic changes that occur
in starvation have to be taken into consideration
Anorexia
Loss Deficiency
Infection
Reduced intake
Starvation Malabsorption Neoplasm
Reduced mass
Infection
Small bowel
overgrowth
Losses
Specific
deficiency
Reduced work
Loss of reserve
tissue and
functional capacity
LOSS OF HOMEOSTASIS
Body composition
changed
Physiological and metabolic
responses changed
Efficient use
Reduced requirement
fig0001 Figure 1 Schema showing the changes that occur in severe
malnutrition. When malnutrition is prolonged, the adaptive
changes are insufficient to maintain homeostasis. Reproduced
with permission of Oxford University Press from Golden MNH
(1996) Severe Malnutrition. In: Weatherall DJ, Ledingham JGG
and Warrell DA (eds) Oxford Textbook of Medicine, Vol. 1.
FAMINE, STARVATION, AND FASTING 2245

during refeeding, otherwise death from cardiac fail-
ure, infection, hypoglycemia, and hypothermia are
likely. Treatment is considered in two main phases:
a short stabilization period to treat infections and
correct the main metabolic disturbances (e.g., fluid
and electrolyte imbalance, and micronutrient defi-
ciencies) and a longer rehabilitation period to replace
lost tissues. Many humanitarian aid agencies looking
after starving populations have a very organized
system of identifying those who are severely malnour-
ished so they can prioritize them for supervised refeed-
ing. Aid agencies often use food preparations that have
been specifically formulated for severe malnutrition to
provide the correct amounts of energy, protein, potas-
sium, magnesium, and micronutrients. In hospitals
and nutrition rehabilitation centers, suitable prepar-
ations can be made from milk, sugar, oil, and an
electrolyte/mineral mix, and/or modified local foods.
0016 The essential characteristics of successful dietary
treatment in the stabilization phase are small, fre-
quent feeds day and night that provide just enough
energy and protein to meet maintenance needs. This
will halt any further loss of tissue and, together with
provision of potassium, magnesium, and micro-
nutrients, will restore normal functioning of the
deranged metabolic machinery. In the rehabilitation
phase, the aim is to restore the lost tissues. This
involves providing large amounts of the nutrients
that provide the building blocks for tissue synthesis,
and high energy intakes to cover the energy cost.
Thus, the aim in this phase of rapid catch-up growth
is to encourage children to eat as much as possible
and to provide them with diets that are high in energy
and protein, whilst continuing to give extra potas-
sium, magnesium, and micronutrients.
Fetal Undernutrition
0017 The question sometimes arises as to whether an infant
born small for its gestational age because of under-
nutrition before birth will remain small. This is diffi-
cult to answer because the genetic make-up of human
individuals is so diverse, and genes, as well as nutri-
tion, influence the rate of growth. Animal studies
with pure-bred strains provide some information.
The ‘runt’ pig, born much smaller than its littermates,
is unlikely to catch up to its larger siblings, and rats
that are born very immature, when undernourished
during the suckling period, take less food after
weaning and remain small for the rest of their lives.
There is some evidence that this is also true for small
newborns in developing countries, especially if their
smallness is because they are short in length, rather
than thin. It is difficult, however, to separate the effect
of fetal undernutrition from the growth-limiting
effects of being raised in the same environment that
detrimentally affected fetal growth. Interestingly, no
long-term effects on adult size were found in those
individuals whose mothers suffered 6 months of star-
vation in the Dutch famine of 1944–45 but then were
raised with a good standard of living. There seems
little doubt, however, that the earlier undernutrition
is imposed, the more likely it is that the effect will be
permanent. Barker and colleagues have suggested
that retarded growth of the developing fetus is asso-
ciated with a number of chronic conditions in adult-
hood, including diabetes, hypertension, and ischemic
heart disease.
Role of Fasting in Health and Disease
0018Some people fast even when they are healthy and
there is plenty of food available. The reason may be
political: thus, ‘hunger strikes’ are used by political
prisoners and others from time to time to draw atten-
tion to their cause. Some fast for religious reasons.
Religious fasting is usually of a short duration. Ram-
adan, for example, held in the ninth month of the
Muslim year, involves going without food or drink
between sunrise and sunset for the month. This short
period of abstinence is likely to do little harm, and in
any case, those who might be injured by it (e.g.,
pregnant women) are exempt from the fast.
0019A more serious problem is anorexia nervosa. This
is a psychiatric eating disorder that tends to run in
families and appears to be increasing in prevalence.
The sufferers, usually adolescent girls and young
women, are obsessed with the idea that they are too
fat, and that they must lose weight and remain very
thin. They may have been overweight in the past, but
not necessarily so. They often come from better-off
homes, where there is no shortage of food. Long-
standing cases may repress the sensation of hunger,
but for others, the sensation persists, and so the term
‘anorexia’ is misleading. Sometimes, the desire for
food overcomes them; they eat a great deal and then
deliberately induce vomiting; this condition is called
bulimia. Or they may resort to laxatives and diuretics.
The effects of insufficient food are the same as those
already described, and death from starvation is not
unknown. One of the symptoms is often amenorrhea.
This is also characteristic of ballet dancers and gym-
nasts who deliberately eat too little food in order to
maintain an acceptable size and shape. (See Anorexia
Nervosa; Bulimia Nervosa.)
0020If the patient with anorexia nervosa can be per-
suaded to take more food, which is not easy, then
physical recovery and restoration of weight take
place just as in others who have starved and then
been refed.
2246 FAMINE, STARVATION, AND FASTING
See also: Anorexia Nervosa; Bulimia Nervosa
Further Reading
Action Against Hunger (2001) The Geopolitics of Hunger,
2000–2001: Hunger and Power. London: Lynne Rien-
ner.
Alamgir M (1981) An approach towards a theory of
famine. In: Robson JRK (ed) Famine: Its Causes, Effects
and Management. London: Gordon and Breach Science.
Barker DJP (1994) Mothers, Babies and Disease in Later
Life. London: BMJ.
DeRose L, Messer E and Millman S (1998) Who’s Hungry?
And How Do We Know?: Food Shortage, Poverty, and
Deprivation. Tokyo: United Nations University Press.
Dreze J, Sen A and Hussain A (eds) (1995) The Political
Economy of Hunger. Oxford: Clarendon Press.
Garrow JS, James WPT and Ralph A (eds) (2000) Human
Nutrition and Dietetics, 10th edn. London: Churchill
Livingstone.
Golden MHN (1996) Severe malnutrition. In: Weatherall
DJ, Ledingham JGG and Warrell DA (eds) Oxford Text-
book of Medicine, 3rd edn., vol. 1, pp. 1278–1296.
Oxford: Oxford University Press.
Keys A, Brozek J, Henschel A, Mickelesen O and Taylor HL
(1950) The Biology of Human Starvation. Minneapolis,
MN: University of Minnesota Press.
Von Braun J, Teklu T and Webb P (1999) Famine in Africa:
Causes, Responses and Prevention. Baltimore, MD: The
Johns Hopkins University Press.
Waterlow JC (1992) Protein Energy Malnutrition. London:
Edward Arnold.
Watson F (1999) One hundred years of famine – a pause for
reflection. Field Exchange Issue 8: 20–23.
Widdowson EM (1951) The response to unlimited food. In:
Studies of Undernutrition, Wuppertal 1946–9. MRC
Special Report Series No. 275. London: Her Majesty’s
Stationery Office.
World Health Organization (1999) Management of Severe
Malnutrition: A Manual for Physicians and other Senior
Health Workers. Geneva: World Health Organization.
FAO See Food and Agriculture Organization of the United Nations
FAT SUBSTITUTES
Use of Fat-replaced Foods in
Reducing Fat and Energy Intake
D L Miller, Central Soya Company Inc., Fort Wayne, IN,
USA
L J Cheskin, Johns Hopkins University, Baltimore, MD,
USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 The availability of ‘fat-free,’‘low-fat,’ and ‘reduced-
fat’ foods has skyrocketed in recent years. This rise in
the number of fat-modified products is due in large
part to the development of ‘fat replacers’ which are
substances that replace one or more of the functional
qualities of fat in a food without supplying all of
calories associated with fat.
0002 The safety of using fat replacers has received much
attention, but comparatively few studies have investi-
gated how these products will influence food intake
and energy regulation in humans. Until recently, few
studies examined the effects of varying the level of fat
in foods on energy intake and body composition.
Indeed, until the mid-1980s, there was relatively little
emphasis on the role of dietary fat in obesity, and the
technology for formulating palatable reduced-fat
foods was limited. Thus, only recently have studies
assessing the effectiveness of such substances in
reducing both dietary fat and energy intake been
undertaken.
0003Despite this paucity of published data, some nutri-
tion professionals and the general public alike assume
that using fat-replaced products will bring about
automatic reductions in fat intake. We know very
little, though, about how consumers will use fat-
replaced foods. For example, fat-replaced foods may
be substituted for higher-fat versions of foods (using
low-fat mayonnaise instead of regular mayonnaise),
and/or substituted for ‘forbidden foods’ (eating fat-
free potato chips when regular potato chips had been
omitted from the diet), or, finally, used as a license to
increase intake of other types of foods (‘If I use the
fat-free salad dressing I can have a piece of cheesecake
for dessert’). If fat-replaced foods are used ineffect-
ively, this could potentially result in increases in
FAT SUBSTITUTES/Use of Fat-replaced Foods in Reducing Fat and Energy Intake 2247