Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


The Concept of Frailty
0006 Frailty has been defined as the loss of a person’s
capacity to withstand minor environmental stresses.
Although ‘frailty’ is sometimes used to avoid a precise
definition of disability, in a more scientific way, it
may be useful to help health workers understand
what appears to be ‘a syndrome of multi-system re-
duction in physiological capacity compromising an
old person’s function . . . and leading to unstable
disability.’ In frail elderly people, just treating the
acute illness is often insufficient: in the clinical
context, reduced musculoskeletal function, aerobic
capacity, cognitive and neurological function, and
nutritional reserve are the features measured to define
frailty, because these deficits reduce the capacity for
interaction with the environment. In an old patient
presenting with an acute illness, all these different
aspects of reserve and function need to be optimized
if the patient is to have a chance of recovery. The
frailty syndrome is sometimes seen as a downward
spiral (or the ‘dwindles’ in the USA), and research
confirms the frequently very major role of nutrition
in the clinical context.
0007 It is clinically useful to diagnose frailty by measur-
ing the four key capacities, thereby identifying elderly
people at risk of unstable disability with a view to
reversing these problems if realistic. The suggested
methods for measuring the components of frailty for
muscle function include grip strength, ability to stand
from sitting, aerobic capacity by measuring a 6-min
walk in outpatients or a treadmill test, various cogni-
tive tests, and practical functioning tests to assess the
mind; and for nutritional state, body mass index (in
people unable to stand or markedly kyphosed, demi-
span or other measures can be used to estimate skel-
etal size). (See Nutritional Assessment: Functional
Tests.)
Nutrition, Diabetes, and Vascular Risk in
Migrant Populations
0008 It has been documented repeatedly that populations
of apparently all genetic descents other than from
temperate climates appeared to change from virtually
zero rates of vascular disease associated with obesity,
diabetes, hypertension, and hyperlipidemia (and a
combination of these – syndrome X) to very high
rates and severity of these if they moved from a
rural, underdeveloped life to a ‘western’-type urban
lifestyle. All these conditions are age-associated ill-
nesses and occur at younger ages, even sometimes
at reproductive ages in women, and more severely
than in European-descent populations. The changes
can occur within one generation and are generally
believed to be due at least in part to dietary changes
in combination with reduced energy expenditure
sometimes. This susceptibility to the Western lifestyle
is found in genetically extremely diverse populations
from Melanesia, the Indian Subcontinent, and Africa,
and indigenous Indian people in the Americas, etc.
Hunter–gatherers, who were the evolutionary ances-
tors of Europeans in a temperate climate, may have
evolved in response to increased meat-eating and
reduced vegetable intake in such a way that does
not affect fertility. Increased fat intake has been sug-
gested in the etiology of diabetes, e.g., in the Pima
Indians. Several intervention studies support this hy-
pothesis, e.g., if Australian Aboriginal people eat
their traditional diet for 5 weeks, it very quickly
reverses the diabetes and obesity that they present
with. Baschetti has emphasized the role of high-
density energy foods in causing these pathologies in
susceptible populations and stated that the concen-
tration of sucrose should not exceed 4.18 MJ l
1
.
Dietary potassium (in vegetables and fruit) is reduced
by Westernization, and, since it is protective in this
context, it has been suggested that potassium be
added to drinks. Tropical and subtropical diets have
a much larger ratio of vegetables to animal intake
compared with those from temperature climates and
it is interesting that the traditional Caribbean diet
is closest to the present UK government recom-
mended diet.
0009The high rate of vascular diseases in populations
of tropical or subtropical descent is not purely due
to these factors. Social factors are very significant,
too, poverty being responsible for about 38% of the
excess stroke morbidity in Afro-Americans compared
with Euro-Americans. The potential health gains
from lifestyle modification, however, clearly merit
investment in appropriate education and facilities.
Usual Weight Changes During Aging
0010Both undernutrition and obesity jeopardize the health
of old populations all over the world, particularly in
urbanized societies. Most data derive from developed
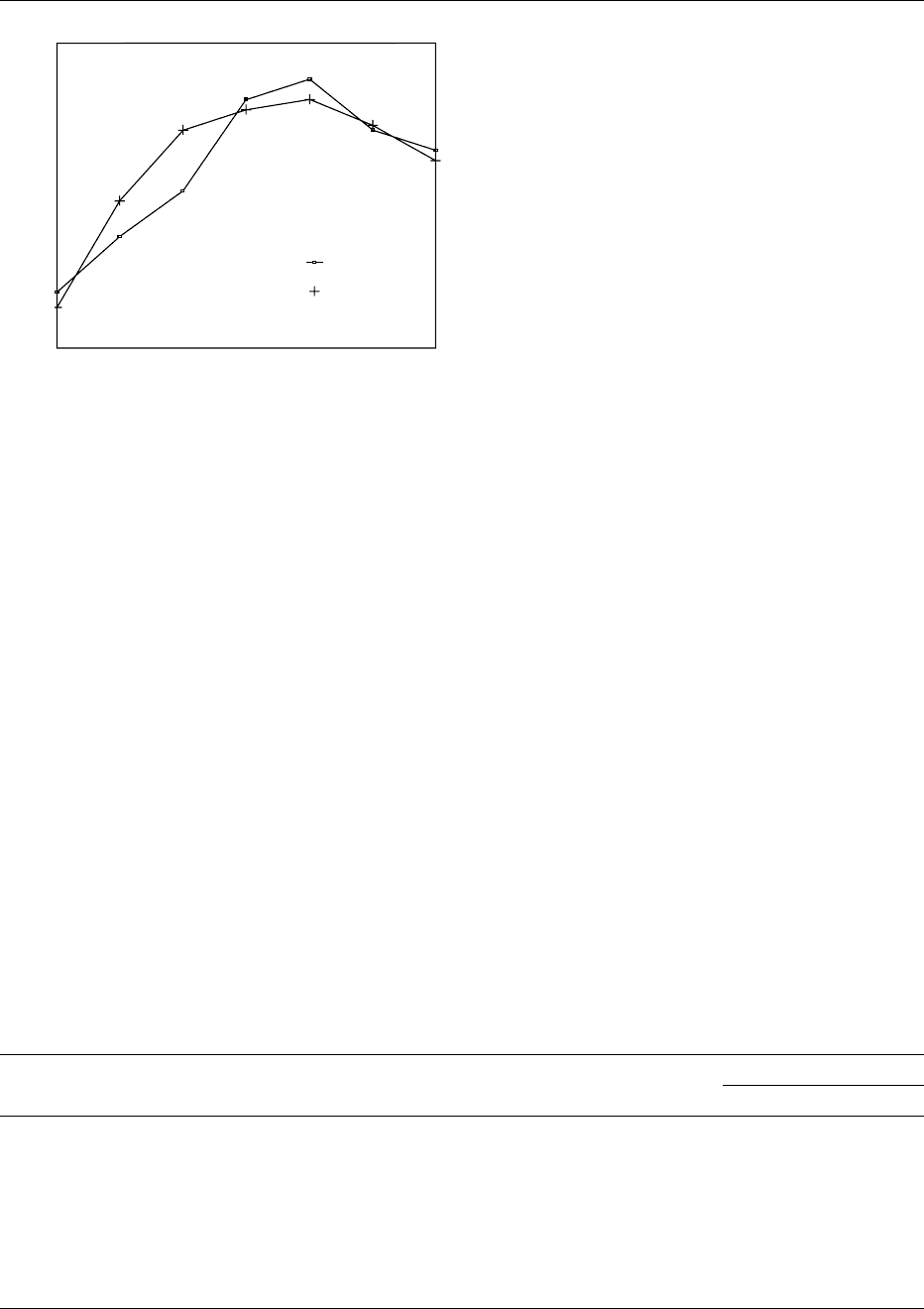
countries. Figure 1 shows the usual changes observed
cross-sectionally in a representative UK sample.
0011The average trend of a slight slow weight loss after
the age of 60 has been found in numerous surveys (see
Table 1): one exception to this was a study in New
Mexico on volunteers with no health problems and
whom the authors described as socially privileged and
unusually health-conscious. (Exclusion of any health
problems in a UK community survey in Nottingham,
which excluded old people living in institutions,
would have meant that 95% of the elderly volun-
teers would have been excluded.)
ELDERLY/Nutritional Status 2017
0012 Explanations for the slight but distinct tendency for
weight loss in old age are awaited. Metabolic changes
so far studied during aging would be compatible with
a tendency to gain weight. It has been suggested that
appetite is reduced during aging by neuroendocrine
changes. This ‘anorexia of aging’ should not be con-
fused with the distinct epidemiology of old patients
who notice anorexia and mention it to the health
team, and in whom a search for a specific cause has
a high yield. Low income, poor dentition, and solitary
eating may be important, as may be rising taste or
smell thresholds for which there is ample evidence.
Since about 95% of the elderly population living in
the community in the UK have some illness or limita-
tion, these conditions, the drugs prescribed for them,
or the social consequences of them also play a role.
Resting metabolic rate is lower in older subjects, even
after correcting for the changes in body composition,
so this alone would cause weight gain if the diet were
to remain constant or adjusting to energy expend-
iture. One hypothesis that might explain the observed
changes and for which there is some limited support
in research might be that, as we age, the energy costs
of daily activities increase. Several authors have dem-
onstrated that weight stability is associated with the
best health in old age. The converse has also been
shown: that weight loss is the most ominous predictor
rather than thinness itself. People who are observed to
be thin in old age include three groups: those who are
lean and fit throughout life, smokers who are lean
and not so fit, and those most at risk who have lost
weight recently. This last group may be perceived as
frail.
Body Composition Changes
0013During aging, there is a tendency for centripetal re-
distribution of fat, which is variable and includes
internal fat deposition. The consequent practical
problems for practitioners is the reduced use of limb
subcutaneous fat measurements to reflect total body
fat. Likewise, in old women especially, this trend plus
height loss associated with osteoporosis may produce
apparent abdominal protrusion and a very common
false label of obesity by doctors assessing on the basis
of abdominal examination. Muscle mass decreases
during aging, although physical training can to some
extent modify this trend. In illness or trauma, dehy-
dration is very common in old people as kidney water
conservation ability falls with age, and the threshold
to thirst commonly rises with old age.
Gut Changes During Aging
0014For most purposes, these are negligible in terms of the
old person’s nutritional status. Probably, the most
significant change is oral health, in particular the
dental health, which, time and again every year,
tbl0001 Table 1 Longitudinal studies reporting weight change in old age arranged in descending order of magnitude of weight change found
(combined group of men and women)
Reference Age (years) of subjects Duration of study (years) Number of subjects Weight change (kgper year)
Men Women
Steen (1988) 70–81 11 23 0.64 0.55
Stevens et al. (1991) >65 at entry 25 370 0.56*
Rissanen et al. (1988) 60–69 4–7 294 0.06 0.4
>70 4–7 0.36 0.7
Lehmann et al. (1996) 65–100 4 629 0.21 0.34
Williamson et al. (1990) 65–74 10 1856 0.11 0.17
Garry et al. (1992) 60–84 9 157 ns 0.14
Friedlander et al. (1977) 65–69 5 1813 ns
>70 5 ns
ns, not significant.
16−24
22
23
24
25
26
27
28
25−34 35−44 45−54
Age (years)
Body mass index (kg/m
2
)
55−64
Women
Men
65−74
75+
fig0001 Figure 1 Mean body mass index by age and sex: health survey
for England.
2018 ELDERLY/Nutritional Status
is shown in many studies to be a relevant factor in
explaining undernutrition in the elderly. Esophageal
motility may become disordered occasionally during
aging, but a much more common finding is in the
stomach, where gastric acid production may be re-
duced. The importance of this in terms of health is
particularly the increased risk of gastroenteritis be-
cause the acid barrier is reduced. The small bowel and
large bowel have a considerable reserve function,
and aging per se is unlikely to affect this unless of
course diseases develop.
What is Optimal BMI in Old Age?
0015 With this question comes that of ‘who defines the
norm’? Tables most widely available for adults are
based on young white volunteers. There are only a
few longitudinal data available at present upon which
to base BMI advice for elders in any population, and
tables are mostly norms using percentiles based on
cross-sectional studies, point surveys, and ‘healthy’
elderly volunteers rather than on health outcomes,
unfortunately. As with all BMI descriptive data, the
BMI norms have increased, particularly in Western-
ized societies, first in the USA and now in Europe.
The norms established in the 80s were apparently no
longer valid in the 1990s. The definition of ‘norms’ is
particularly problematic in old age: in a typical UK
community free-living volunteer elder population,
only 5% of the over-65s have no medical problem.
If all illnesses were excluded in establishing norms,
these tables would be based on 5% of the elderly
population – who could thus be described as super-
fit elders. Compared with our knowledge about
younger people, this state of ignorance regarding old
people and BMI needs explaining, and may reflect the
lack of research investment by public bodies and
private companies.
Population Studies
0016 A 1996 review on BMI in old age relied on data from
a 1979 survey (Build Study) and had no people aged
over 69 (see Table 2). What can be seen from this
table, however, is that the optimum BMI in terms of
mortality apparently rises very significantly with age.
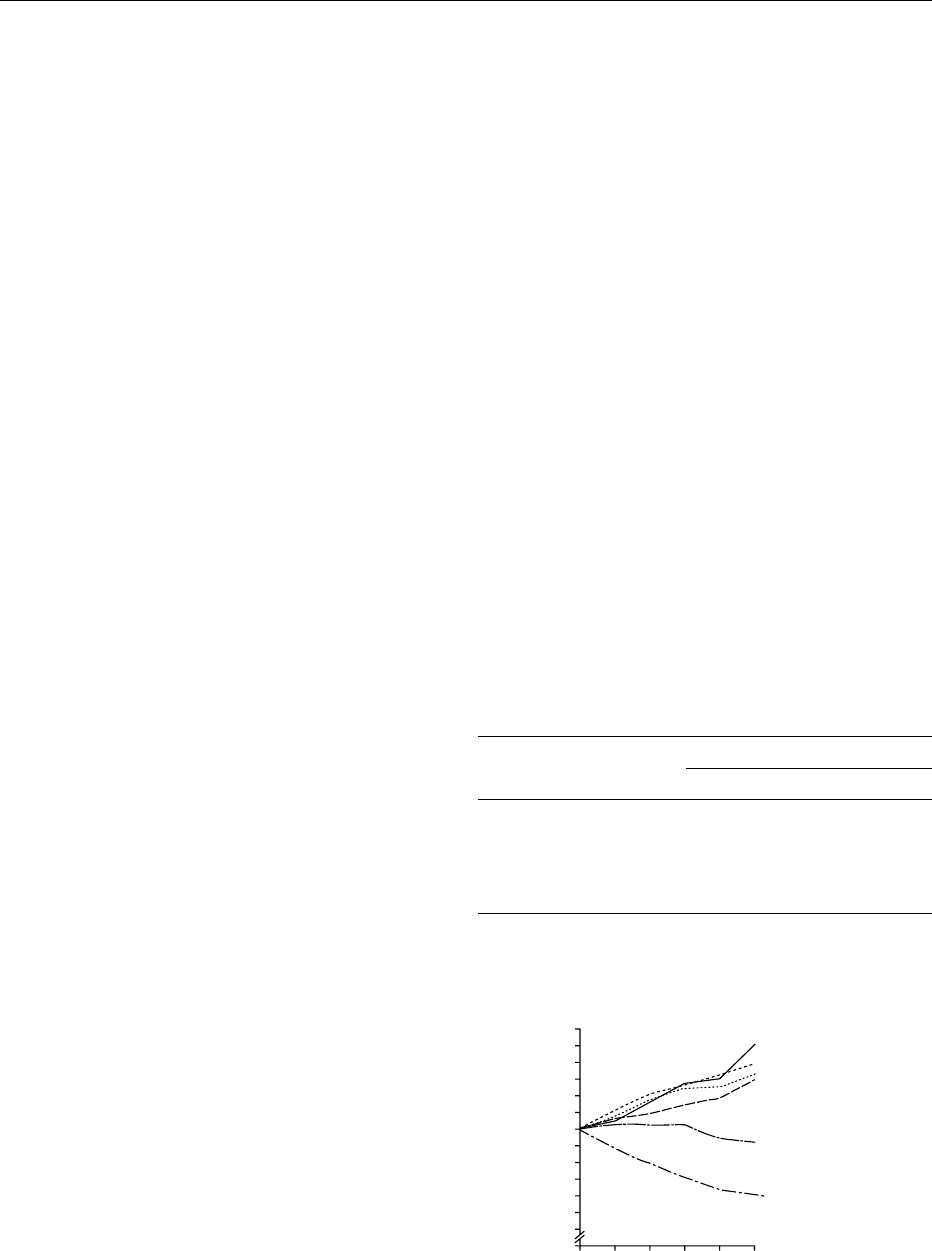
In Finland, a whole population local survey in Tam-
pere of people aged 85 years and older showed a
correlation between longer survival and higher BMI
(see Figure 2).
0017 A very large US survey of 22 000 subjects also
showed a flattening of the U-shaped curve relating
BMI to mortality with increasing age cohorts. The
obesity risks of vascular disease and cancer do not
disappear in old age, but it has been argued that
selective survival of those less vulnerable to these
risks occurs. The Nottingham Longitudinal Study of
Activity and Aging, which measured BMI and health
in 629 relatively well but not super-fit elders living in
the community at the time of the initial survey, inter-
estingly showed neither an increase in morbidity nor
an increase in mortality in the low BMI volunteers
initially and at 4-year follow-up. One possible ex-
planation for this apparent anomaly is that whereas
most population surveys include significantly dis-
abled or ill elderly subjects, if these people are
excluded, thinness has no apparent ominous signifi-
cance, at least not over 4 years. This fits with the
emphasis many authors and clinicians have put on
nutrition reserve in elders and the importance of
regaining this reserve after intercurrent illness or
trauma. Nevertheless, the subject cannot be said to
be fully understood as yet, and confounders are very
likely to be significant and to vary from sample to
sample. What the data do suggest, however, is that if
old people are fit, well, and mobile, thinness has little
ominous significance, but in any studies that include
hospital attenders, it appears that thinness is a very
powerful predictor of poor outcome.
0018In terms of disability prevention, the data from the
US National Health and Nutrition Examination
tbl0002Table 2 Effect of age on body mass index associated with the
lowest mortality
a
Age group (years) Bodymassindex (kgm
2
)
Men Women
20–29 21.4 19.5
30–39 21.6 23.4
40–49 22.9 23.2
50–59 25.8 25.2
60–69 26.6 27.3
a
Data from Build Study 1979.
0
0
0.4
0.6
0.8
1.0
Relative survival rate
1.2
1.4
1.6
<20.0 103
102
28.0 81
Body mass index No
65
26.0−27.9
8124.0−25.9
94
22.0−23.9
20.0−21.9
1
Years of follow up
2345
fig0002Figure 2 Five-year relative survival curves according to body
mass index in subjects aged 85 and over.
ELDERLY/Nutritional Status 2019
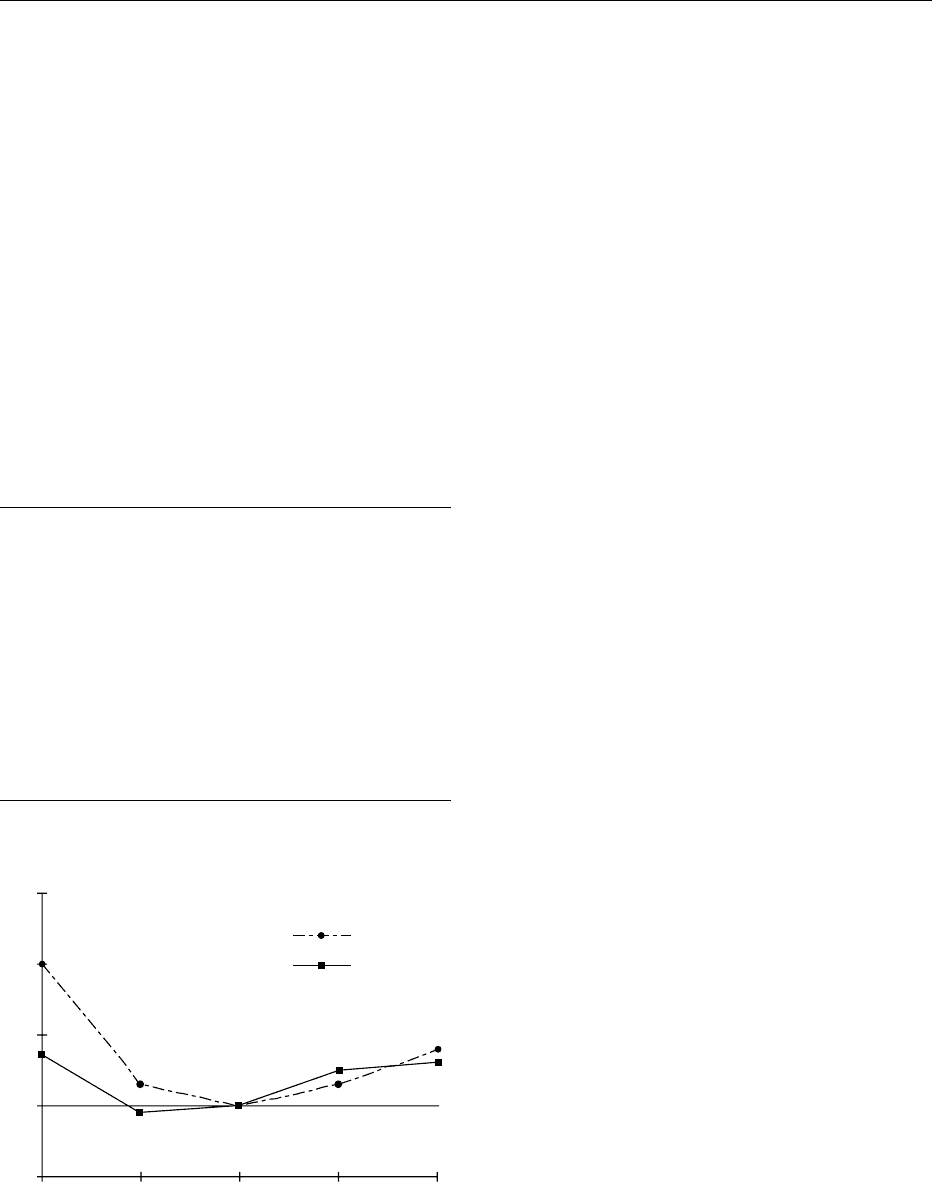
Survey (NHANES) in 1994 supported the U-shaped
curve hypothesis: both extremes of BMI in elderly
volunteers apparently independently predicted worse
functional status (independence in activities of daily
living) (Figure 3). In the old group of women who had
lost more than 5% of their weight over 8–16 years,
there was an associated doubling in the rate of mobil-
ity disability, even after adjustments were made for
age, smoking, and education. Weight loss rather than
thinness was again the main predictor of poor
outcome. In a detailed description of the NHANES
follow-up, it was found that the initial BMI at both
15% extremes was an independent predictor of
disability in old men and old women, even 11–13
years later, even after correcting for 22 potential
confounders, and even after excluding those who
died within 2 years of the first survey (in whom, it
might have been argued, weight loss was a result of
illness).
0019BMI ranges are therefore a changing phenomenon
over time both within and between elderly popula-
tions. At present, outcome data are lacking on which
to base advice to an elderly person regarding opti-
mum weight, except that overweight is clearly related
to joint pains. Survival is reduced in thinner elders
overall, but a high waist–hip ratio is probably not
advisable in the presence of hypertension, vascular
disease, or diabetes.
Hospital Patients
0020Surveys of nutritional status and health in old age
that include disabled, ill, or traumatized elderly pa-
tients consistently highlight thinness and recent
weight loss as powerful ominous independent pre-
dictors of health outcome. Although, with different
methods, hospital inpatient surveys yield a wide
range of prevalences for undernutrition in old hos-
pital inpatients, in the UK, 40% is accepted by Gov-
ernment Department documents. The commonness
of thinness in old inpatients may explain why staff
(unlike relatives) usually miss the diagnosis and has
prompted the growth of screening tools of varying
efficacy. Research suggests that, so far, no question-
naire screening tools to be administered by nurses on
general wards are safe, unlike their use by dieticians,
and safer alternatives are either anthropometry or
simply an eyeball estimation of whether the patient
is thin, average, or fat: the nurse is asked to tick the
relevant box. (See Nutritional Assessment: Functional
Tests.)
0021The association and ominous significance of
malnutrition with illness and disability are likely to
be complex. In some cases, the illness or disability, or
their attendant pharmacological and social conse-
quences, may precede and cause negative energy
balance. In others, the causal relationship may be
reversed. In the clinical context, therefore, it is crucial
to tackle both the illness and the malnutrition, if
appropriate, and, to avoid recurrence, an attempt
should be made to determine the sequence of events
in each individual: sometimes, a third factor will have
caused both the illness and the malnutrition simultan-
eously. In a study on very acute illnesses leading to old
people’s admission, using retrospective dietary histor-
ies, it was found that, compared with control groups,
these patients had had lower dietary intakes over the
preceding month – even though the criterion for in-
clusion was that the patients were absolutely fine the
day before the day of admission. This suggests that
Male
Female
< 5
0
1
2
3
4
5−15 15−85
BMI rank
Relative risk
85−95
> 95
fig0003 Figure 3 Relationship between body mass index percentile
rank and relative risk for functional impairment for men and
women. Final logistic regression model after removing from the
sample those 307 persons who died within 2 years of the comple-
tion of the NHANES-I Epidemiologic Follow-up Study (n ¼2746).
tbl0003 Table 3 Factors associated with high-risk undernutrition in old
age
Environmental causes
Poverty
Social isolation
Depression
Social construction of disability (being housebound)
Individual factors
Poor dentition
Chronic lung disease
History of gastric surgery
Cognitive impairment
Dysphagia
Bereavement and depression
Alcohol excess
Recent unintended weight loss of 3 kg
2020 ELDERLY/Nutritional Status

undernutrition may cause or precede very acute ill-
ness. Of course, in the clinical context, the reverse is
also often found.
0022 Frequently, depression and physical illnesses pre-
sent simultaneously in the elderly, and in many, a
vicious circle is present by the time treatment starts:
malnutrition can perpetuate anorexia by increasing
small bowel microbial overgrowth, which is even
more likely to follow undernutrition in the elderly
than in children because of the high prevalence of
age-associated achlorhydria (in atrophic gastritis,
now known to be due to Helicobacter pylori infec-
tion) in elderly patients. When depression and anor-
exia are both very marked and coexist in old age,
endoscopy is indicated. In stroke patients, weakness
in swallowing is commonly compounded by starva-
tion from the time of stroke, and tube feeding is
required to correct this starvation weakness of the
bulbar muscles.
0023 Negative energy and nitrogen balance very quickly
and severely impair immune function, even in fit
elderly volunteers, and even within 9 weeks of
starting on an equal-calorie but low-protein diet. In
the clinical context, it has been demonstrated that a
low lymphocyte count, which can have numerous
causes (e.g., inflammation, undernutrition), correl-
ates closely with the risk of readmission of the
patient.
0024 What is less well known in elderly care is the im-
portance of careful management of the refeeding syn-
drome, and work is awaited to see whether this and
consequent hypophosphatemia are being missed, as is
our clinical impression, in a number of cases of eld-
erly patients in hospital. (See Elderly: Nutritionally
Related Problems; Nutritional Management of Geri-
atric Patients; Phosphorus: Properties and Determin-
ation; Physiology.)
0025 In rehabilitation wards for the elderly, research has
confirmed very elegantly that poor nutritional status
on admission and, in particular, weight loss during
the preceding year are the most powerful independent
predictors of poor outcome, even after correcting for
numerous potential confounders, including 22 that
did correlate with outcome. Equally important ran-
domized controlled trials of nutritional supplemen-
tation have demonstrated lasting positive outcomes in
elderly hip fracture patients and pneumonia patients:
functional ability in the long term benefitted from
the intervention, and average hospital stay was
shortened.
0026 When viewed together, these data explain the
primary concern regarding undernutrition in elderly
patients and consequent rejection of blanket obesity-
avoidance advice intended for other adults, which is
sometimes inappropriately followed by old patients.
0027-Specific nutritional deficiencies in hospital patients
Certain micronutrient deficiencies in old inpatients
denote specific pathological conditions. Iron defi-
ciency in old age (in particular postmenopause) in
developed countries is due to gut pathology (e.g.,
ulcer or cancer) in over 90% of cases, according to
two London studies. Vitamin D deficiency may be
due to anticonvulsant medication, folate deficiency
may reflect anticonvulsant medication but, more
commonly, inadequate diet due to poor self-care,
and this is common in early dementia. It was so
common that it was thought to cause dementia,
although, at present, the consensus appears to be
that early dementia leads to difficulty organizing
food if people are living on their own, and the
first lab routine test to show this is folate. Folate
deficiency is also very commonly associated with
alcoholism. (See Elderly: Nutritionally Related
Problems.)
0028Immobility itself in old age has been shown to be
associated with more rapid protein turnover than is
seen in fit peers: it was demonstrated long ago that, in
the UK, housebound elderly people are in negative
nitrogen balance. If protein turnover is more rapid in
the elderly during immobility (and endocrine mecha-
nisms are possible), a slight imbalance of intake or
expenditure will lead more rapidly to more muscle
loss while the body prioritizes visceral protein syn-
thesis. This may explain the downward spiral of
frailty sometimes seen in ill, traumatized or disabled
patients.
Nutritional Status in Elderly Nursing Home
Residents
0029Undernutrition is very common in this group. Many
residents barely eat enough to maintain basal metab-
olism. The reason for poor nutritional status in ad-
vanced dementia may vary, and research has produced
a range of answers, including insufficient time spent
helping at meal times, inappropriate food consistency,
and possibly a change in energy balance control. Drug
effects on appetite or bowels and nutrient utilization
also need to be considered in each case. Energy ex-
penditure generally drives energy intake in humans – if
an old person is less mobile, their appetite will there-
fore be reduced and micronutrient deficiencies will,
and often do, result if the nutrient density of the food
is not appropriately increased. Vitamin D deficiency is
common in housebound elders without access to
sunlight, and sufficient vitamin D consumption
would require an unacceptably high intake of fatty
fish. Quite why there are such high rates of general
undernutrition in this group, however, is unclear,
even if the individual micronutrient deficiencies are
easier to explain. (See Elderly: Nutritionally Related
ELDERLY/Nutritional Status 2021

Problems; Nutritional Management of Geriatric
Patients.)
0030 In 1995, the Caroline Walker Trust produced mul-
tidisciplinary guidelines for optimal nutrition for in-
stitutionalized elderly. It is written to be understood
by service users and service providers, and covers
food provision, dental checks, weight monitoring,
etc. plus triggers for referral for medical review (any
unexplained 3-kg weight loss). The importance of
formulating an individualized plan suitable for each
elderly resident is emphasized.
0031 Ethical questions regarding the degree of interven-
tion considered appropriate in terminal illness and in
dementia frequently occur in this setting. In several
observational studies in nursing homes investigating
the management of advanced dementia patients who
appear not to be eating enough, tube feeding pro-
duced no benefit in terms of comfort and none in
terms of survival.
See also: Elderly: Nutritionally Related Problems;
Nutritional Management of Geriatric Patients; Nutritional
Assessment: Functional Tests; Phosphorus: Properties
and Determination; Physiology
Further Reading
Campbell AJ and Buchner DM (1997) Unstable disability
and the fluctuations of frailty. Age and Ageing 26:
315–318.
Caroline Walker Trust (1995) Eating Well for Older People.
Report of an Expert Working Group. Practical and Nu-
tritional Guidelines for Food in Residential and Nursing
Homes and for Communal Meals. London: Caroline
Walker Trust.
Ebrahim S and Kalache A (eds) (1996) Epidemiology in Old
Age. London: BMJ Publishing Group.
Galanos AN et al. (1994) Nutrition and function: is there
a relationship between body mass index and the
functional capabilities of community dwelling elderly.
Journal of the American Geriatrics Society 42:
147–168.
Gillick MR (2000) Rethinking the role of tube feeding in
patients with advanced dementia. New England Journal
of Medicine 342: 206–210.
Lehmann A (1996) Nutrition and health – what is new?
Reviews in Clinical Gerontology 6: 147–168.
Rabeneck L, McCullough LB et al. (1997) Ethically justi-
fied, clinically comprehensive guidelines for percutan-
eous endoscopic gastrostomy tube placement. Lancet
349: 496–498.
Roth SG et al. (1999) Calorie restriction in primates: will it
work and how will we know? Journal of the American
Geriatrics Society 7: 896–903.
Tallis R (ed.) (1998) Increasing Longevity: Medical, Social
and Political Implications. London: The Royal College
of Physicians.
Nutritionally Related Problems
J B Blumberg, Tufts University, Boston, MA, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001Nutrition influences the progressive loss of tissue
function with aging and plays an important role in
the genesis of several major chronic degenerative dis-
eases. Aging influences nutritional requirements and
nutritional status through changes in appetite and in
pathways of nutrient absorption, utilization, and ex-
cretion (Table 1). Further, a variety of socioeconomic
and psychological factors as well as the presence and
treatment of current disease(s) common to older
adults affect dietary patterns and nutritional status.
Thus, some of the nutritional problems of the elderly
are the consequence of long-term (chronic) inter-
actions between diet and aging, beginning in adoles-
cence and young adulthood, while others are
associated with the more immediate (acute) result of
old age itself.
Acute nutritionally related problems
Anemia
0002The most consistently reported hematopoietic change
with aging is a higher prevalence of anemia which
increases with each successive decade of life. Al-
though anemia is prevalent among healthy elderly,
its cause does not generally appear to be due to hem-
olysis or deficiencies of iron, folate, or vitamin B
12
.
Elderly people with this unexplained anemia have
lower leukocyte and neutrophil counts than do non-
anemic subjects. Experimental and clinical studies
tbl0001Table 1
Change inphysiologic function Change in nutrient requirement
#Muscle mass (sarcopenia) #Calories
#Bone density (osteopenia) "Vitamins D and K, calcium
#Immune function (anergy) "Vitamins B
6
, C, and E, zinc
#Skin cholecalciferol synthesis "Vitamin D
"Winter parathyroid hormone
production
"Vitamin D
#Calcium bioavailability "Vitamin D
#Hepatic uptake of retinol #Vitamin A
"Oxidative stress status "b-carotene, vitamins C and E
"Levels of homocysteine "Folate, vitamins B
6
and B
12
#Efficiency in pyridoxal
utilization
"Vitamin B
6
"Gastric pH (gastric atrophy) "Vitamin B
12
and folic acid,
calcium, iron, zinc
2022 ELDERLY/Nutritionally Related Problems

suggest this anemia of aging is due to a reduction
in bone marrow reserve capacity (erythropoietin-
dependent progenitor cell proliferation) with de-
creased hormonal responsiveness to hematologic
stress. Chronic inflammation is also a possible
mechanism. However, any elderly individual with
anemia must be fully evaluated for the possibility of
drug-induced or occult gastrointestinal blood loss,
bone marrow failure, chronic hemolysis, and nutri-
tional deficiency before attributing an anemia to age
alone.
Anorexia and Weight Loss
0003 A decline in calorie intake is a well-recognized con-
comitant of increasing age. Surveys reveal that almost
20% of older adults consume less than 1000 calories
(4.2 MJ) per day; among institutionalized elderly and
those whose income is at poverty levels, the preva-
lence may increase twofold. Protein-calorie malnutri-
tion is a common finding among geriatric patients.
Marasmus may occur in older patients because the
combination of a small but balanced caloric intake
with a contribution from muscle-protein catabolism
is sufficient to maintain serum albumin. Thus, weight
loss is an ominous sign in the elderly which needs to
be taken seriously.
0004 The etiology of anorexia and weight loss in the
elderly is multifactorial and includes both physio-
logical and pathological causes. Age-related declines
in metabolic rate due to loss of lean body mass
(sarcopenia) and decreased expenditure of energy on
physical activity contribute to lower calorie intakes
in the elderly. Social factors such as poverty, isolation,
and requirements for assistance with food shopping
and preparation can be a source of impairment to
adequate nutrition. Physical factors such as disabil-
ities or immobility and poor oral health can also
interfere with conducting activities of daily living
associated with nutrition.
0005 Psychiatric disorders, e.g., dementias and depres-
sion, as well as states associated with bereavement
and isolation affect nutritional status. These condi-
tions are not uncommon among the elderly and are
usually associated with anorexia and weight loss.
Among institutionalized elderly with low body
weight and at risk of malnutrition or B vitamin defi-
ciency, a higher prevalence of dementia and depres-
sion is noted. Indifference, memory loss, impaired
cognition, and disturbed or erratic behavior associ-
ated with these conditions all contribute to reduced
food intake. Inadequate nutrition may further exacer-
bate psychiatric symptoms. Experimental studies
suggest an increased activity of the hypothalamic–
pituitary–adrenal axis production of corticotropin-
releasing factor and/or neuropeptide Y may be
involved in the anorexia of some of these psychiatric
conditions.
0006Several diseases common among the elderly affect
food intake. Chronic obstructive pulmonary disease
increases the effort required to eat. Congestive heart
failure is associated with anorexia which is aggravated
by the cachexic effect of cardiac glycosides used to
treat the condition. Some cancers and all antineoplas-
tic drugs can precipitate anorexia. Esophageal reflux
can lead to pain on swallowing and decreased food
intake.
0007Anorexia may also occur as a concomitant of
normal aging. Gustatory papillae begin to atrophy
in middle age and taste and olfactory thresholds
increase with age. Studies in old animals indicate a
reduced drive in the endogenous opioid feeding
system, particularly the k-receptor ligand dynorphin,
and the increased satiety action of the gastrointestinal
hormone cholecystokinin may provide a biochemical
basis for the anorexia of aging.
Constipation
0008Constipation is a common complaint among the
elderly, with women reporting this difficulty more
frequently than men. The discomfort associated
with constipation may affect an older person’s food
intake. The tone of intestinal smooth muscles and
gastrointestinal tract activity diminish with age.
However, the lack of dietary fiber, dehydration, and/
or immobility appear to be the primary causes of
most cases of uncomplicated constipation. A variety
of drug treatments common among elderly patients,
particularly those with anticholinergic actions, may
also cause severe constipation. The requirement for
assistance in using the toilet may cause an older adult
not to respond to the urge to defecate which can result
in a later inability to defecate at will due to desensi-
tization of rectal stretch receptors. Important compli-
cations of constipation in the elderly include fecal
impaction, abnormally large colon, and intestinal ob-
struction. Also, straining at stool may create sudden
severe circulatory changes in the aged. In most in-
stances, the treatment of simple constipation in the
elderly includes advice to increase fiber consumption
(and fluid intake) in the diet and/or as supplements
(e.g., vegetable mucilloids and modified cellulose
products). The pathogenesis of another age-related
condition of the colon associated with the absence
of fiber in western diets is diverticular disease.
Dehydration
0009Thirst and water intake are critical to the main-
tenance of fluid and electrolyte balance since it is
only through such intakes that water deficits can be
ELDERLY/Nutritionally Related Problems 2023

replenished. Fluid and electrolyte disorders are
common in the elderly and abnormalities in salt and
water homeostasis are a significant cause of morbid-
ity and mortality in geriatric patients. Older adults
respond to dehydration with greater increases in
plasma sodium concentration and osmolality than
young subjects, yet do not become markedly thirsty
and drink enough to dilute their body fluids to pre-
deprivation levels. Thirst in response to heat stress
and thermal dehydration is also reduced in the elderly
despite a reduced capacity for thermoregulation (heat
loss).
0010 The mechanism of the thirst deficit in the elderly is
not fully defined. Age-related changes in receptors
that detect dehydration of the cell (osmoreceptors)
and decreases in plasma volume (baroreceptors) and
in the endogenous opioid system have been suggested
to play a role in this condition. Changes in renal
function with age, such as diminished glomerular
filtration rate, urinary concentrating ability, and
sodium-conserving capacity, can act to reduce the
ability to conserve salt and water and predispose an
older person to hypovolemia and dehydration. The
decreasing activity of the renin–angiotensin–aldoster-
one system with age may also contribute to dimin-
ished sodium and water homeostasis in the elderly.
0011 Older adults may become dehydrated when ex-
posed to even mild stresses such as water restriction,
fever, infection, or diarrhea. When the diminished
thirst response in an elderly individual is accompan-
ied by illness or physical incapacity that increases
water loss or prevents access to water, dangerous
dehydration may follow. In the elderly, dehydration
is a common cause of renal impairment and failure
and electrolyte disturbances. Dehydration and hypo-
natremia can also lead to confusional states that fur-
ther interfere with fluid intake. While the extent of
dehydration in free-living elderly has not been estab-
lished, age-related impairments of thirst sensation
place them at risk of dehydration.
Gastric Atrophy
0012 Selective functions of the digestive tract experience
some diminution of function with age, although
many of these changes do not appear significantly to
influence nutrient requirements in the elderly. An
increased incidence of gastric acid hyposecretion
(hypochlorhydria) resulting from atrophy of the gas-
tric glands of the fundic mucosa of the stomach is
noted among about 30% of people over 60 years.
This gastric atrophy (type A) is asymptomatic but,
when the condition is severe, is associated with perni-
cious anemia due to a decreased secretion of intrinsic
factor. Gastric atrophy is also associated with faster
gastric emptying rates and a higher pH with bacterial
overgrowth in the proximal small intestine. These
latter effects of gastric atrophy may interfere with
the bioavailability of several nutrients, including cal-
cium, iron, folic acid, and vitamin B
12
. In addition to
absorbing or utilizing these nutrients, the overgrowth
of some aerobic organisms may contribute to the
nutritional status of the host via the synthesis and
secretion of some nutrients, e.g., vitamin K. The
high intraluminal pH of the stomach and proximal
small intestine found in gastric atrophy may also
prevent the release of some nutrients from dietary
fiber or protein and other food complexes. Dietary
recommendations for several micronutrients should
be adjusted for older adults with gastric atrophy and
include the use of appropriate nutrient supplements.
Chronic Nutritionally Related Problems
Cancer
0013Cancer develops as a result of interactions between
genetic and environmental factors. An estimated 90%
of all cancer cases are attributed to environmental
factors, including tobacco smoking, radiation,
industrial pollutants, viruses, and diet. Analyses of
epidemiological studies suggest that 35% of cancer
deaths may be related to diet. Evidence linking diet
and cancer has been derived from experimental
in vitro and animal studies, metabolic and biochem-
ical studies in humans, and epidemiological investi-
gations. In general, the epidemiological studies have
demonstrated that populations migrating from an
area with its own pattern of cancer incidence rates
acquire rates characteristic of their new location. Fur-
ther, large changes in incidence rates for many types
of cancer within genetically stable populations have
been associated with changes in dietary patterns. Al-
though the cumulative data for the relationship be-
tween both the causal and protective effects of diet
and cancer are compelling, the evidence, particularly
with regard to quantitative levels of specific nutrients,
remains far from conclusive.
0014Various studies indicate that a high intake of total
fat increases the risk of some types of cancer, notably
cancer of the breast and colon but also of the prostate,
rectum, and ovaries. Cancer mortality correlates
better with total dietary fat intake than with the
type of fat. However, several epidemiological studies
have demonstrated a strong relationship between sat-
urated fatty acids or animal fat and increased cancer
risk. In contrast, animal studies indicate monounsatu-
rated and n-6 polyunsaturated fats promote carcino-
genesis more effectively, while n-3 fatty acids can
reduce tumor growth rates. Several mechanisms
have been proposed to explain the effects of fat on
2024 ELDERLY/Nutritionally Related Problems

cancer, including its alteration of steroid hormones
and endocrine changes, immune function, cell mem-
brane fluidity, and (for colon cancer) fecal floral and
bile acids. Excess body weight and obesity are also
associated with an increased risk of several cancers,
including those of the breast, endometrium, ovaries,
colon, rectum, prostate, and gallbladder. Other diet-
ary factors, including alcohol and naturally occurring
contaminants, e.g., aflatoxins and N-nitroso com-
pounds, also pose a potential cancer risk.
0015 Dietary patterns emphasizing foods high in fiber
are associated with low rates of certain cancers, espe-
cially breast and colon cancer. The protective effect of
fiber may be due to a concomitant reduction of total
calories and fat and/or by altering gastrointestinal
factors such as intraluminal pH, gut flora, and transit
time. Fiber-containing foods such as fruits and vege-
tables are also important sources of b-carotene, vita-
mins A, C, and E, phenols, and indoles as well as a
large number of other phytochemicals with potential
cancer-preventive activity. Generous dietary intakes
of b-carotene are associated with a reduced incidence
of lung, breast, oral mucosa, bladder, and esophageal
cancers; however, clinical trials with large supplemen-
tal doses of b-carotene resulted in an increased risk of
cancer among smokers. Vitamin C has a potentially
protective effect against esophageal, stomach, cer-
vical, breast, and lung cancers. Low intakes of vita-
min E are strongly correlated with risk of cancer in
many, but not all, organs. b-carotene and vitamins C
and E may share a related antioxidant, free radical
scavenging mechanism against carcinogenesis. Evi-
dence also suggests that calcium and selenium have
protective effects against some forms of cancer.
0016 While the evidence associating specific nutrients
with cancer risk remains equivocal, dietary guidelines
have been promulgated by a number of health organ-
izations which recommend avoiding obesity, reducing
total fat to 30% or less of calories, consuming high-
fiber foods and a variety of fruits and green and
yellow vegetables in the daily diet, and minimizing
the intake of alcohol and smoked, salt-cured, and
nitrate-cured foods. Evidence suggesting the ability
of these dietary patterns or supplementation with
putative protective nutrients to reverse existing
cancers or lower rates of cancer recurrence is limited
and equivocal.
0017 Established cancers as well as antitumor treatments
may have a variety of effects on the nutritional status
of the affected geriatric patient. Anorexia and weight
loss are common and may result in progressive
wasting and undernutrition (cancer cachexia). Alter-
ations in protein, carbohydrate, and fat metabolism
are associated with many cancers. Malabsorption and
protein-losing enteropathy are also a concomitant
of various malignancies. Hormonal abnormalities
induced by tumors may affect the status of different
nutrients. Radiation, surgery, and drug therapies each
have consequences which predispose the patient to
potentially serious nutrition problems.
Vision Disorders
0018Aging is associated with extensive postsynthetic
modifications to eye lens proteins resulting in aggre-
gation with eventual polymerization and precipita-
tion to form opacities or age-related cataracts. The
prevalence of cataract increases with age, reaching
about 50% in people 75–85 years old; prevalence
rates are higher if early lens changes are included in
the calculation. Oxidation of lens proteins is highly
correlated with cataract and research studies provide
evidence for a close relationship between cataracto-
genesis and nutrition. An elevated status of dietary
antioxidants is strongly correlated with a lower inci-
dence of cataract. Ascorbic acid concentration in the
lens can be as much as 30 times that in plasma but
decreases in aged and cataractous lens. Vitamin E is
associated with protection against oxidative insults
and glutathione-dependent antioxidant reactions are
compromised in the lens with age and cataracts. The
effect of other nutrients, e.g., folic acid, riboflavin,
vitamin B
6
, taurine, and tryptophan, has been exam-
ined but evidence supporting their protective role
against cataractogenesis remains limited. Intake of
the xanthophyll carotenoids, lutein and zeaxanthin,
is inversely correlated with the incidence of cataract
and cataract extractions.
0019Age-related macular degeneration (AMD) is the
leading cause of irreversible blindness among older
adults. The retina is rich in highly polyunsaturated
fatty acids, particularly docosahexaenoic acid, and
thus vulnerable to lipid peroxidation. This situation
is compounded by exposure to light, high oxygen
tension, and high concentrations of retinol. The
macula contains a full complement of antioxidant
defenses but is unusually rich in lutein and zeax-
anthin, which provides its yellow pigment and optical
density, and absent in b-carotene and lycopene. Ob-
servational studies indicate that generous intakes of
lutein and zeaxanthin are associated with a signifi-
cant reduction in risk of AMD. Zinc plays a role in the
metabolic function of several antioxidant enzymes in
the chorioretinal complex and limited evidence sug-
gests increased zinc intake may benefit visual acuity
in AMD patients.
Coronary Heart Disease
0020The progressive focal narrowing of coronary arteries
by atherosclerosis, beginning as early as age 10, leads
ELDERLY/Nutritionally Related Problems 2025

to an inadequate circulation of blood in local areas of
heart muscle. These changes can result in angina
pectoris, myocardial infarction (heart attack), and
sudden death in older adults. These and related dis-
orders are termed coronary heart disease (CHD) and,
in western countries, account for more deaths annu-
ally than any other group of diseases. The prevalence
of CHD is greater among men than women and in-
creases markedly in those over 65 years of age. Med-
ical interventions and changes in lifestyle during the
past two decades have reduced the age-corrected
death rate from CHD by about 40%; however,
without a further reduction in risk factors and/or an
improvement in treatments, CHD prevalence and
incidence will increase in the future because of the
aging of the population. The causes of CHD are
multifactorial and include cigarette smoking, high
blood pressure, obesity, and high blood cholesterol
(hypercholesterolemia).
0021 The relationship between diet, lipoprotein metab-
olism, atherogenesis, and CHD has been defined by
extensive scientific investigations conducted during
the last 75 years. This work indicates a strong, con-
tinuous, and graded relationship between total blood
cholesterol levels, the severity of atherosclerosis, and
risk for CHD. Dietary saturated fat and cholesterol
raise total blood cholesterol and low-density lipo-
protein (LDL) cholesterol levels; LDL is the major
atherogenic lipoprotein and accounts for most of the
CHD risk associated with elevated plasma total chol-
esterol. Polyunsaturated and monounsaturated fat
lowers total blood cholesterol and LDL cholesterol
levels when substituted for saturated fat in the diet.
High-density lipoprotein (HDL) is considered to pro-
tect against CHD and is associated with female sex,
estrogen use, exercise, moderate alcohol consump-
tion, and weight loss.
0022 Diet is considered the cornerstone of therapy to
reduce borderline (200–239 mg dl
1
) and high-risk
(240 mg dl
1
) blood cholesterol levels whether or
not drug therapy is eventually added to the regimen.
Dietary guidelines to reduce risk of CHD include
recommendations of nutrient intake as a percent of
total calories of less than 30% from fat (less than
10% from saturated fat, up to 10% from polyunsat-
urated fat, and 10–15% from monounsaturated fat),
50–60% from carbohydrates, and 10–20% from
protein. Total calorie intake should be designed to
achieve and maintain desirable weight. In addition,
daily cholesterol intake should be less than 300 mg.
Individuals at very high risk of CHD should further
reduce saturated fat and cholesterol intake. Adher-
ence to these dietary guidelines has been proven to
lower blood cholesterol by 10–25%. Elevated plasma
homocysteine is an independent risk factor for CHD.
Homocysteine concentrations can be reduced by
increasing the intake of folic acid, vitamin B
6
,and/
or vitamin B
12
; however, prospective studies demon-
strating a decreased incidence of CHD with B vitamin
interventions have not been completed. Supplemen-
tation with vitamin E and/or fish oil may play a role in
the primary and secondary prevention of CHD but
the results of clinical trials are equivocal.
Diabetes
0023Type 2 diabetes, formerly called noninsulin-depend-
ent diabetes mellitus, accounts for about 90% of
all cases of the disease. The onset of type 2 diabetes
is gradual (with no or mild symptoms), usually
appearing in midlife among people who are over-
weight or obese. Although type 2 diabetics display
normal pancreatic histology, secrete insulin in re-
sponse to glucose ingestion, and have normal to
high levels of circulating insulin, they are less able to
use this insulin (insulin resistance). Type 1 diabetes,
formerly called insulin-dependent diabetes mellitus, is
characterized by an absolute deficiency of insulin
caused by b-cell destruction of the islets of Langer-
hans in the pancreas. Type 1 diabetes usually begins
abruptly in adolescents and young adults of normal
body weight. No method has been identified which
prevents type 1 diabetes and these patients require
insulin administration for survival. Genetic predis-
position appears to play an important role in both
type 1 and type 2 diabetes. The specific cellular basis
of hyperglycemia and related metabolic abnormal-
ities in type 2 diabetes is not yet clear, although
three defects appear to be involved: a diminished
pancreatic b-cell response to glucose; a reduced syn-
thesis or function of cellular receptors for insulin; and
an impaired ability to utilize glucose following bind-
ing to cellular receptors. Clinical complications of
diabetes include heart disease and stroke, kidney dis-
ease, blindness, nontraumatic leg and foot amputa-
tions, and death.
0024Dietary therapy is considered the key to the man-
agement of type 2 diabetes. Obesity is strongly asso-
ciated with the onset and severity of type 2 diabetes
with more than 80% of patients being more than
15% in excess of their desirable body weight at the
time of diagnosis. Weight loss reduces insulin resist-
ance as well as fasting and postprandial blood glucose
levels in overweight diabetics. Dietary recommenda-
tions for the management of diabetes include: 50–
60% of total calories as carbohydrate (emphasizing
complex carbohydrates and water-soluble fiber); de-
creased protein in those with renal insufficiency; 30%
or less of total calories as fat (with reduced intake of
saturated fat); and limited alcohol intake (restricted
entirely in poorly controlled diabetes). Limited and
2026 ELDERLY/Nutritionally Related Problems