Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

IMPLANTS IN THE LOAD CARRYING PART OF THE DENTITION • 957
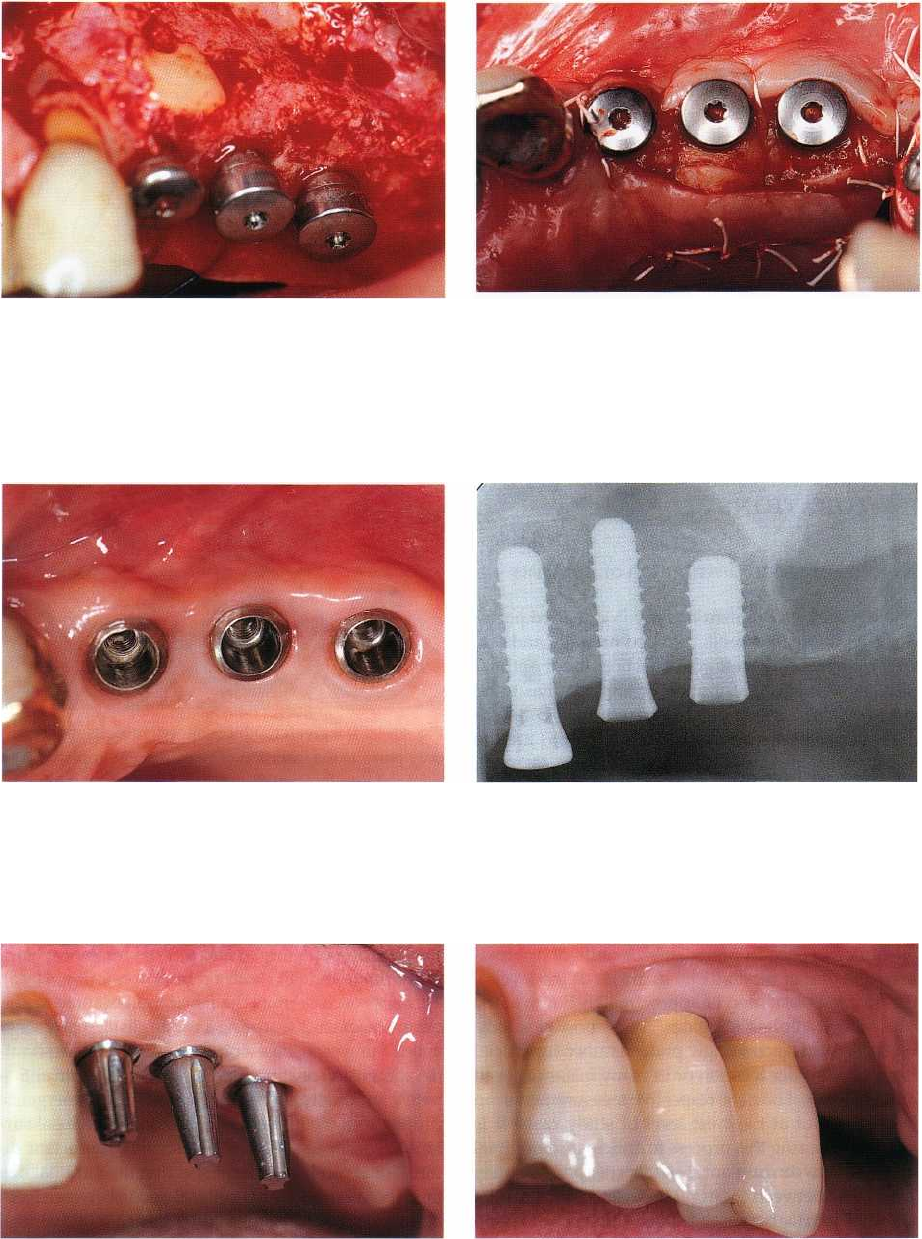
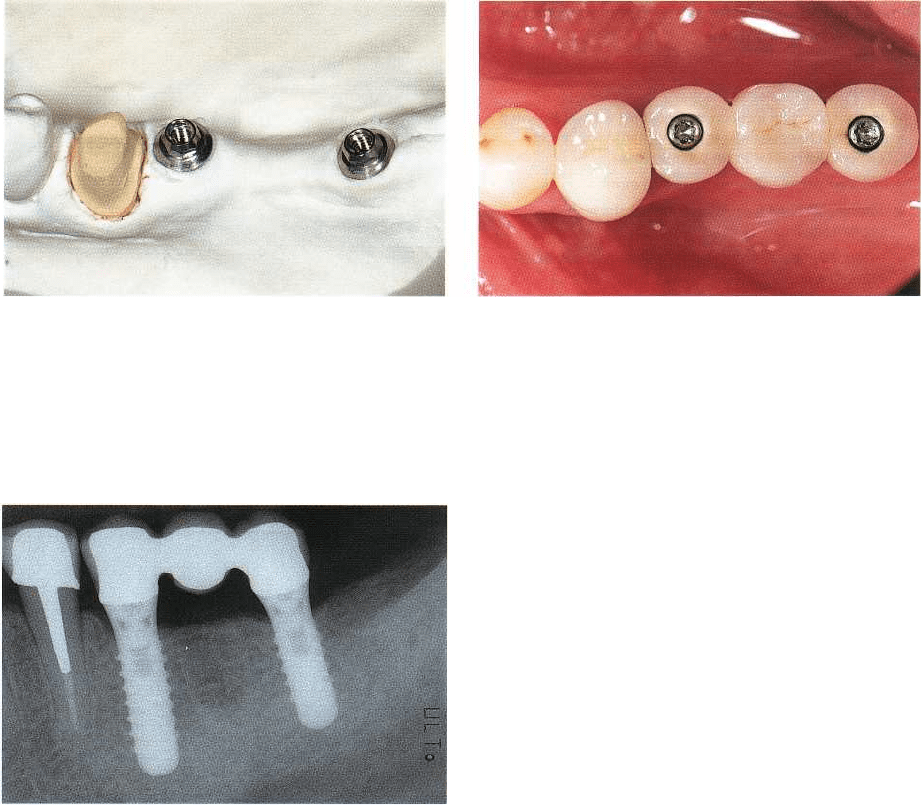
Fig. 41-38. Eight months following the combined ante-
rior sinus floor elevation and lateral bone augmenta-
tion procedure, the site is reopened and three implants
are inserted.
Fig. 41-39. In order to increase the amount of kerati-
nized mucosa on the vestibular aspect of the implants,
the flap is repositioned accordingly. The resulting defi-
ciency on the palatal aspect is compensated for by
means of a connective tissue being part of the partial
thickness flap.
Fig. 41-40. Three months after implant placement, fa-Fig. 41-41. The corresponding radiograph confirms suc-
vorable peri-implant soft tissue conditions have been
cessful osseointegration of the three implants that are
re-established.
mostly located in augmented bone.
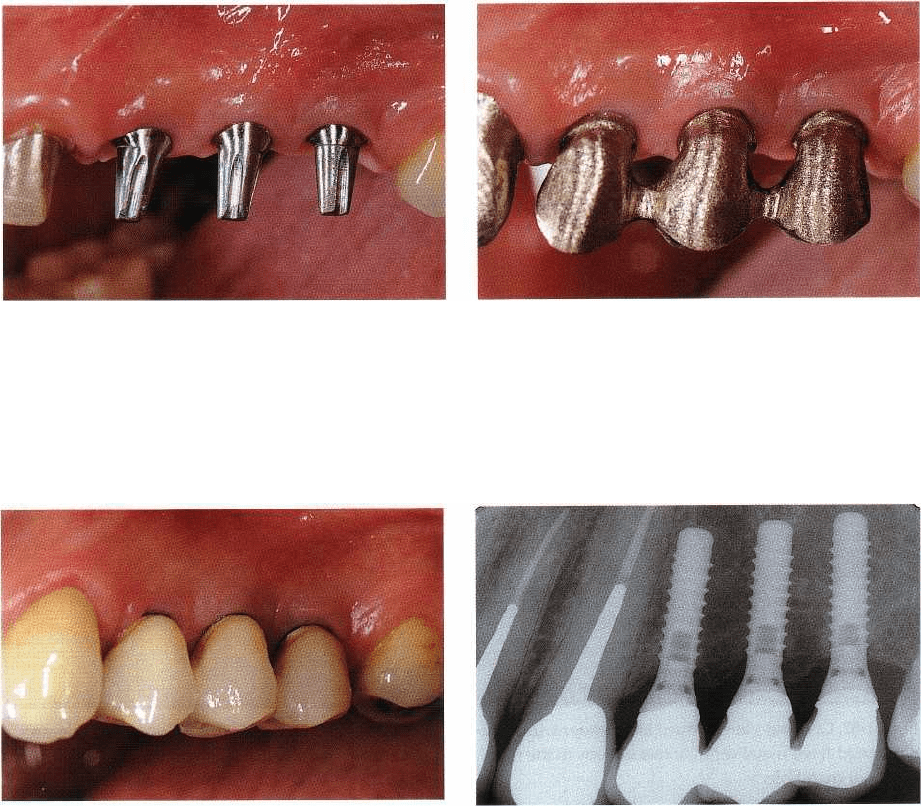
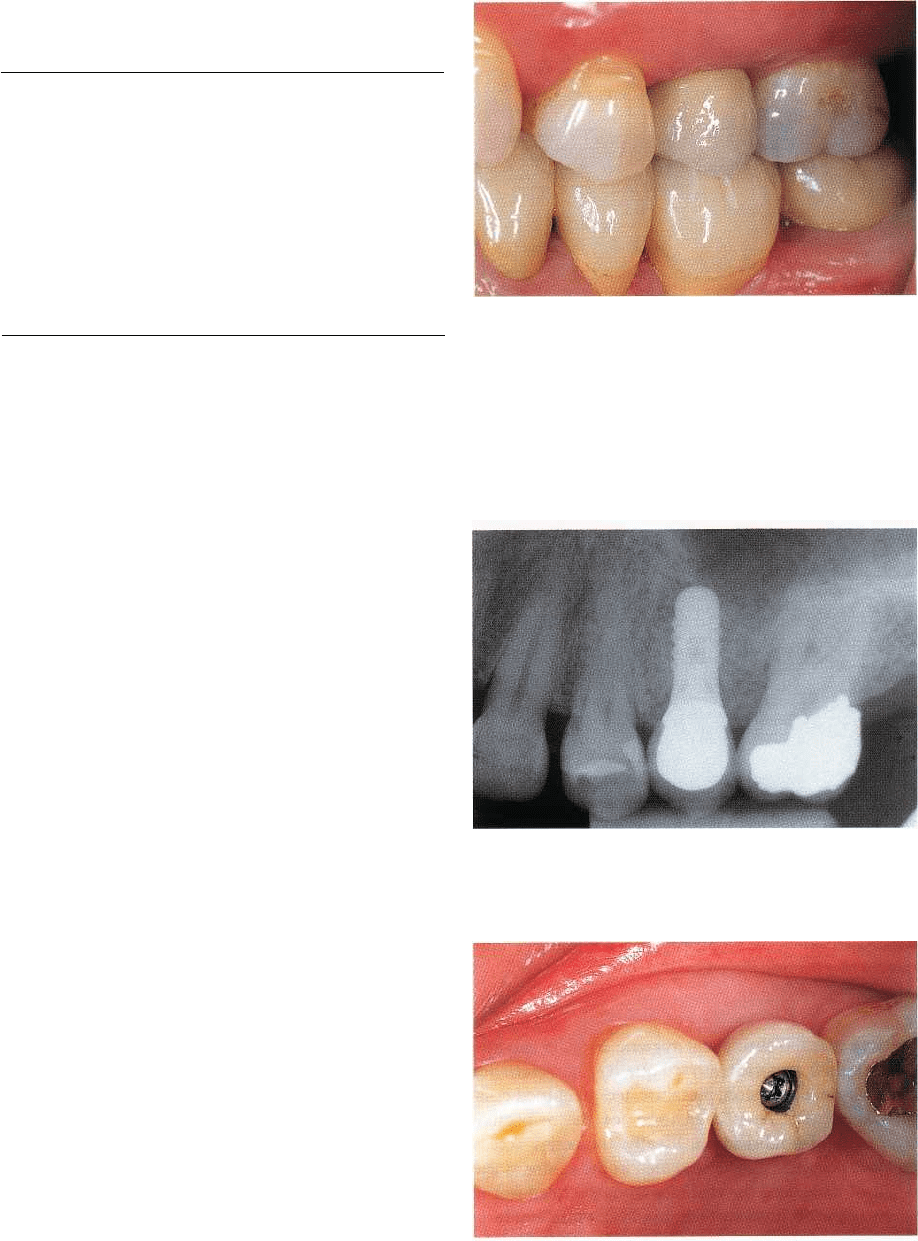
Fig. 41-42. In a case of implant shoulder location corn-
Fig. 41-43. Clinical view of the final three-unit metal-ce-
patible with cementation, respective solid abutments
ramic implant suprastructure, featuring a flat and con-
are selected and tightened to 35 Ncm with a calibratedtinuous emergence profile and adequate access for in-
torque wrench.
terimplant oral hygiene.
95
8
' CHAPTER 41
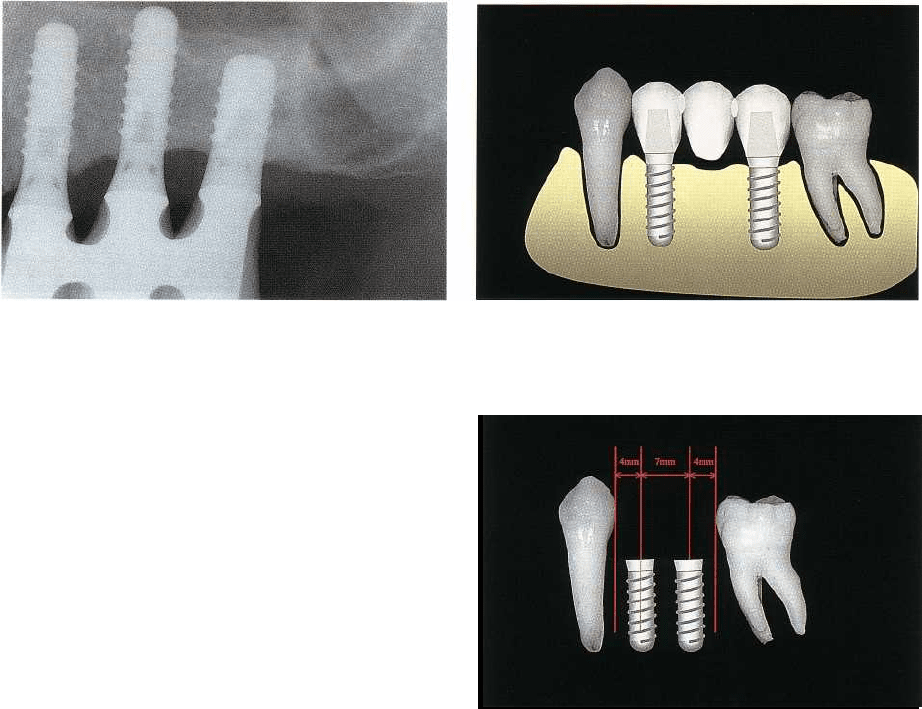
Fig. 41-44. The 4-year follow-up radiograph confirms
stable conditions at the osseointegrated interface.
MULTIPLE-UNIT TOOTH-BOUND
POSTERIOR IMPLANT
RESTORATIONS
Number, size and distribution of implants
When it comes to implant therapy in extended poste-
rior edentulous segments confined mesially and dis-
tally by remaining teeth, the question about optimal
number, size and distribution of implants has to be
raised again. Among the key parameters to be ad-
dressed during the decision-making process are the
mesio-distal dimension of the edentulous segment,
the
precise alveolar bone crest volume (including bone
height and crest width in an oro-facial direction), the
opposing dentition (premolars or molars), interarch
distance and specific occlusal parameters, as well as
the periodontal, endodontic and structural conditions
of the neighboring teeth.
One feasible approach consists of segmenting the
edentulous space in premolar-size units of approxi-
mately 7 mm of mesio-distal diameter at the level of
the
occlusal plane, and of approximately 5 mm at the
prospective implant shoulder. As on posterior loca-
tions clinicians increasingly prefer a rather superficial
implant shoulder location or in many instances even
a
supramucosal one, the respective measurements can
be
carried out at the crest level of study casts. It is
important during this process to anticipate a minimal
distance between implant shoulders of approximately
2 mm, and between a natural tooth and an implant of
about 1.5 mm (to be measured at the interproximal soft
tissue level). Again, the treatment objective, i.e. a long-
lasting implant-supported FPD, should be predict-
ably
reached on the one hand with optimal efficacy
and on
the other hand with a minimum of invasive
ness and
cost. The still existing controversy of whether
each
missing occlusal unit should be replaced by one
implant or whether a minimal number of implants
should be used, has already been addressed earlier in
this chapter.
Fig. 41-45. Schematic representation of a tooth-bound
posterior edentulous segment, restored by two im-
plants and a three-unit FPD with a central pontic.
Fig. 41-46. If a given tooth-bound edentulous space
only permits the insertion of two adjacent implants, a
minimal interimplant distance of 2 mm and a minimal
implant-to-tooth distance of 1.5 mm (at the interproxi
-
mal soft tissue level) should be respected.
In the case of three missing occlusal units and in the
absence of other particular restrictive conditions such
as limited local bone volume, the authors recommend
the insertion of a mesial and a distal implant to sup-
port a three-unit FPD with a central pontic (Fig. 41-45).
This approach permits the fabrication of three metal-
ceramic elements featuring a mesio-distal diameter of
about 7 mm each. Based on an average implant shoul
-
der dimension of approximately 5 mm, one can antici-
pate a gradually increasing, harmonious emergence
profile from the implant shoulder to the occlusal sur-
face. In order to satisfy the remaining important di-
mensional conditions, i.e. respecting the minimal dis-
tance between adjacent implants and in between teeth
and implants, one needs to dispose of a minimal total
mesio-distal gap distance of 21-22 mm (Fig. 41-47).
In the case of two missing occlusal units, one should
try as a general rule to select the largest possible
implant diameters with respect to the total mesio-dis-
tal distance of the given tooth-bound edentulous seg-
ment. Decisive parameters are again interimplant dis-
tance and space between implants and adjacent teeth,
as well as oro-facial crest width at the two prospective
implant sites. For a total gap diameter of about 14-15
IMPLANTS IN THE LOAD CARRYING PART OF THE DENTITION • 959
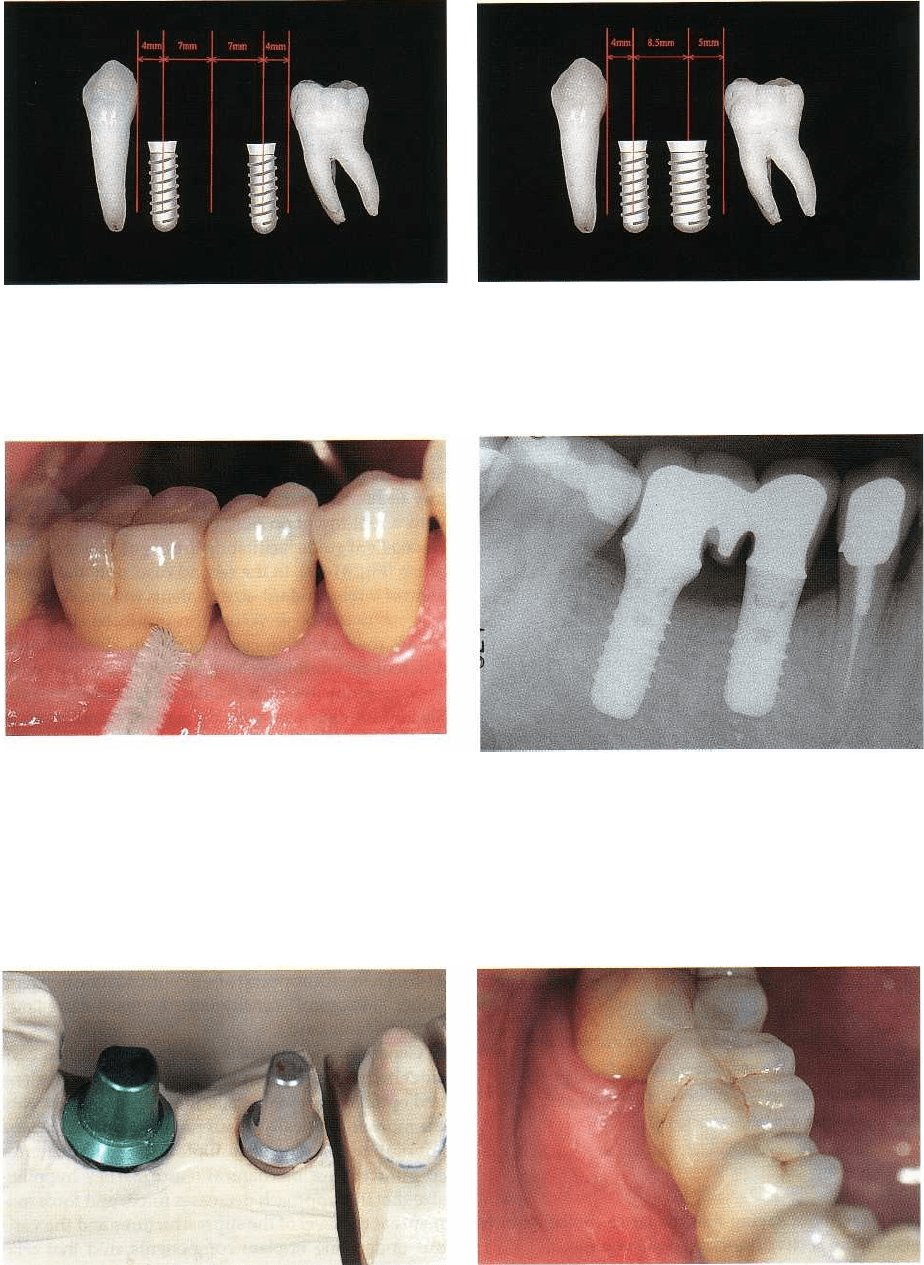
Fig. 41-47. In the case of three missing occlusal units,
an implant-supported FPD with a central pontic (ap-
proximately 7 mm in width) may be considered as a vi-
able solution.
Fig. 41-49. Vestibular aspect of a metal-ceramic restora
-
tion supported by two screw-type implants. Due to an
excess of mesio-distal space, the implants have been
separated by approximately 4 mm. Instead of a tradi-
tional pontic, a root imitation has been performed close
to the distal implant, providing an adequate guide for
an
interdental brush in view of an efficient plaque con
trol
at the marginal area of the implant restoration.
Fig. 41-48. In the presence of a mesio-distal gap width
of approximately 17 mm, one may consider the combi-
nation of a standard and an increased-diameter ("wide
neck
"
) implant. The same minimal interimplant and
implant-to-tooth distances have to be respected.
Fig. 41-50. With respect to cleansibility, the respective
prosthesis design is clearly visible on the postoperative
radiograph.
Fig. 41-51. The corresponding master model visualizes
the different dimensions and distances involved in this
individual case.
Fig. 41-52. On an oblique view the vestibular axial pro-
file of the implant restoration becomes visible. Soft tis-
sue (cheek and tongue) support and harmony with ad-
jacent teeth are of paramount importance.
mm, two standard-size implants are most suitable nation of one standard and one wide-diameter/wide-
(Fig. 41-46),
while for one of 17 to 18 mm the combi- platform implant is considered adequate (Fig. 41-48).
960 • CHAPTER
41
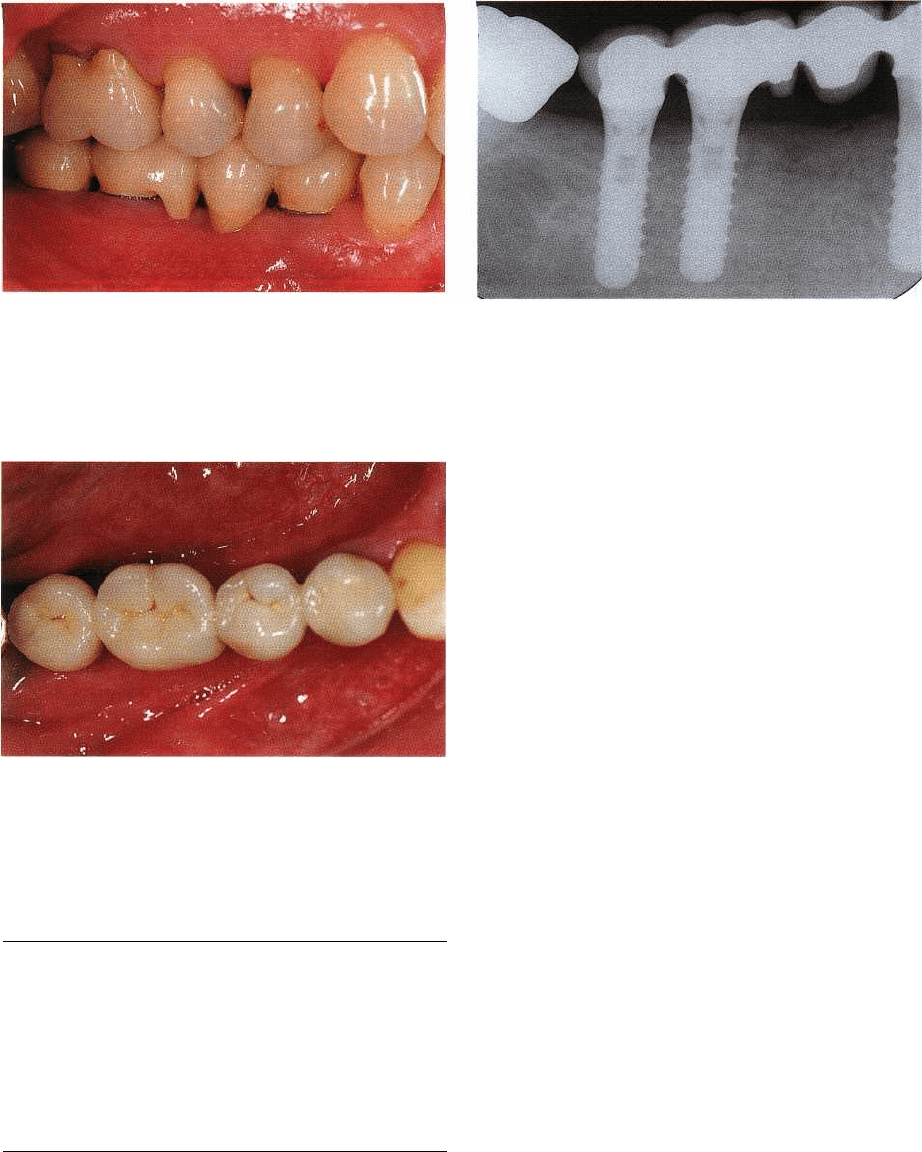
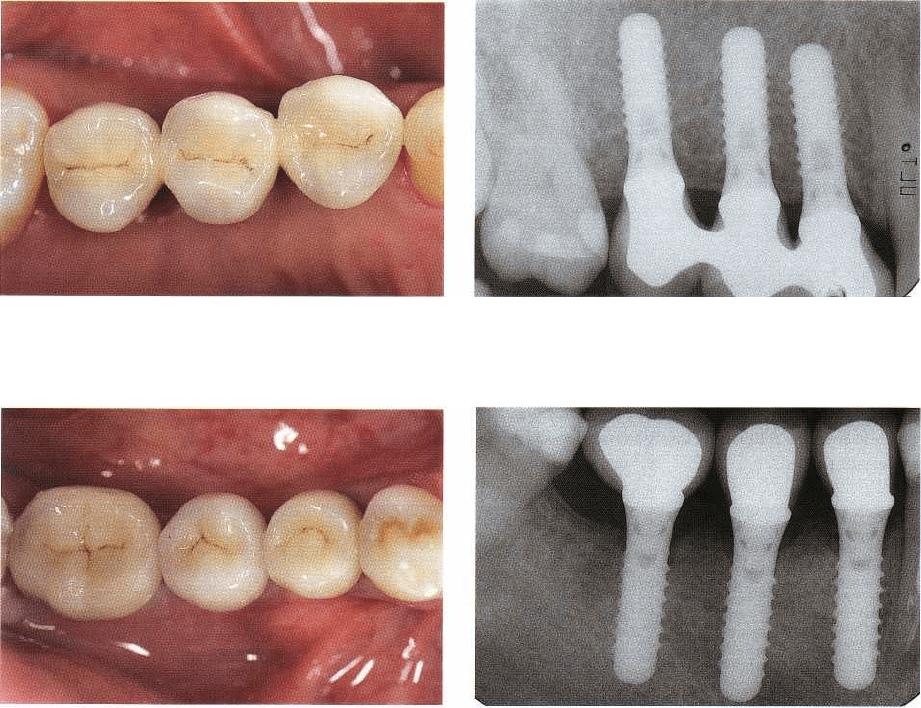
Fig. 41-53. Buccal view of an extended edentulous right
mandibular tooth-bound gap treated with an implant
restoration. In the pontic area a design favoring the effi-
cacy of an interdental brush close to the implant mar-
gins has been applied.
Fig. 41-55. Occlusal view of the completed 4-unit im-
plant-borne fixed porcelain-fused-to-metal prosthesis.
Table 41.5. Splinting of multiple adjacent posterior
implants
Parameters to consider:
• access for oral hygiene
• marginal adaptation/"passive fit"
• technical simplicity/ease of eventual
reinterventions
• "overload" of the osseointegrated interface
• "rotational forces" on implant components
• screw-loosening/fatigue fractures
It goes without saying that the latter choice requires
also the respective oro-facial bone volume.
These are just frequently encountered clinical ex-
amples, but in the function of other morphology and
dimensions of edentulous tooth-bound segments, ad-
ditional approaches and implant combinations may be
envisioned. Two such particular clinical situations are
presented in Figs. 41-49 to 41-52 and Figs. 41-53 to 41-
55. In the first case, the gap diameter required the two
adjacent implants to be spaced wider than the
Fig. 41-54. The related radiograph illustrates the chosen
design in the pontic area in terms of access to and effi-
cacy of interproximal plaque control.
normally advocated interproximal 2 mm. The labora-
tory technician compensated for this excess of space
with a root-imitation pontic which in turn provided an
excellent guide facilitating the use of an interdental
brush (Fig. 41-49). In the second case, only the place-
ment of three standard-size implants was possible due
to a restricted bone volume in oro-facial direction.
Again, the technician could optimally distribute the
different restoration volumes but still comply with
basic prerequisites such as a flat axial emergence pro-
file and optimal access for the patient's oral hygiene (
Figs. 41-53, 41-54).
Splinted versus single-unit restorations of
multiple adjacent posterior implants
Another persisting controversial issue relates to the
question whether multiple adjacent implants in the
load carrying part of the dentition should support
splinted or segmented single-unit restorations (Table
41-5). There still appears to be a confrontation between
rather "biological" considerations versus more "me-
chanical" thinking.
Generally speaking, the biologically oriented con-
siderations, insisting on easy access for oral hygiene
and optimal marginal adaptation, represent probably
the more scientifically-based point of view. Clinicians
advocating splinting of multiple adjacent implants do
so primarily for mechanical reasons. They hypothe-
size that this approach decreases forces and force mo-
ments at the level of the suprastructures and the vari-
ous underlying implant components, and that rela-
tively frequent mechanical complications such as
screw-loosening and fractures may be significantly
reduced or prevented by this measure. The related
literature does not at present provide a clear answer, as
randomized long-term clinical trials addressing this
particular parameter are still scarce. Some more
general reports do exist, however, addressing mainly
IMPLANTS IN THE LOAD CARRYING PART OF THE DENTITION •
961
Fig. 41-56. The implant shoulder-abutment complex of
the three left maxillary posterior implants has been pre
-
pared with fine-grain diamond burrs under abundant
water cooling in order to facilitate the configuration of
the related suprastructure. Particular emphasis was
given to margins following closely the scalloped course
of the soft tissue.
Fig. 41-57. In a case of reduced-diameter implants,
splinting of adjacent units may reduce the risk for tech
nical complications. A metal framework try-in prior to
the application of the ceramic veneering may help to
detect and eliminate an eventual non-passive fit at an
early stage.
Fig. 41-58. The vestibular view of the final metal-ce-
ramic restoration illustrates the impact on esthetics of a
metal margin. This aspect should be discussed with the
patient before treatment. In case of a high smile line,
one may consider an increased sink depth during im-
plant surgery
type and frequency of mechanical complications
(
Goodacre et al. 1999).
Among the frequently forwarded arguments to
plead
the case of splinting are reduced-diameter (Figs.
41-56
to 41-59) or short (i.e. less than 8 mm) implants,
implants inserted in low-density bone, implants
placed
in augmented or grafted (e.g. after anterior sinus floor
elevation) bone, or implant restorations in the posterior
segments of patients with verified nota
ble occlusal
parafunctions or bruxism. One should be
aware,
however, that the majority of these arguments
are
primarily based on clinical opinions and eventually
common sense, and that to date they are lacking
formal scientific evidence. In fact, there is increased
indication, derived from prospective multicenter
studies (although not addressing this parameter in
particular), that splinting does not appear to be a
prerequisite for preventing excessive crestal bone re-
sorption or even loss of osseointegration. Nowadays,
Fig. 41-59. On the 1-year follow-up radiograph an ac
ceptable marginal fidelity can be assessed.
the authors would seriously reconsider their respec-
tive choice related to the suprastructure design pre-
sented in Figs. 41-60 and 41-61. Definitely, in the pres
-
ence of standard-size (i.e. addressing both diameter
and length) implants, which are placed in normal
density original (non-augmented or grafted) bone,
single-unit restorations are recommended as they
comply better with the various parameters that are
important from a more biological point of view, as
demonstrated by the clinical example presented in
Figs. 41-62 and 41-63.
POSTERIOR SINGLE-TOOTH
REPLACEMENT
At the time when most implant systems had basically
only one "standard" dimension at disposition, this
962 • CHAPTER
41
Fig. 41-60. Occlusal view of a right maxillary posterior
three-unit implant restoration featuring premolar-sized
segments.
Fig. 41-61. The corresponding follow-up radiograph
confirms acceptable peri-implant conditions.
Fig. 41-62. Occlusal view of three independent, implant
-
supported fixed metal-ceramic restorations in the
right
posterior mandible.
corresponded to approximately 4–5 mm at the im-
plant shoulder and thus was optimally suited for
premolar-size restorations, featuring a continuously
increasing (towards coronally) flat axial emergence
profile and a mesio-distal diameter of about 7–8 mm
at the occlusal surface. Clinicians were not infre-
quently faced with posterior single-tooth sites, how-
ever, that did not comply with these dimensions, for
example in the case of missing first molars or after the
loss of persisting deciduous (primary) second molars.
As a consequence, the resulting implant restorations
featured either unfavorable excessive interproximal
overcontour or wide open embrasures. The first situ-
ation was difficult to clean, while the second led to
undesired food retention (impaction). Nowadays
most
of the leading implant manufacturers offer wide
-
body/wide-platform implants designed for the re-
placement of multirooted teeth (Fig. 41-3).
Premolar-size single-tooth restorations
When it comes to posterior single-tooth gaps that
dimensionally correspond to an average premolar,
Fig. 41-63. As confirmed by the follow-up radiograph,
an increased (more molar-like) dimension has been
given to the most distal restoration, despite the fact
that a standard-sized implant had to be used for re-
stricted bone volume reasons.
standard-size screw-form implants are well suited.
The respective implant dimensions which include
both the intrabony part and the implant shoulder,
offer the additional advantage of being mostly com-
patible with a limited bone volume in oro-facial direc-
tion. Whenever feasible, a straightforward low-main-
tenance restorative design is advocated, which nor-
mally consists of a cementable porcelain-fused-to-
metal crown with vestibular and oral axial contours
that are in harmony with the adjacent teeth and thus
provide adequate guidance for cheek and tongue
(
Figs. 41-64 to 41-66).
Molar-size single-tooth restorations
If a given posterior single-tooth gap corresponds
rather to the mesio-distal dimension of a molar, it is
recommended, for the reasons quoted in the previous
paragraph, that the insertion of a wide-neck implant
is planned (Bahat & Handelsman 1996). This ap-
proach, however, also requires the respective bone
volume in an oro-facial direction. If this is not the case,
the presurgical site analysis, eventually in the form of
IMPLANTS IN THE LOAD CARRYING PART OF THE DENTITION • 963
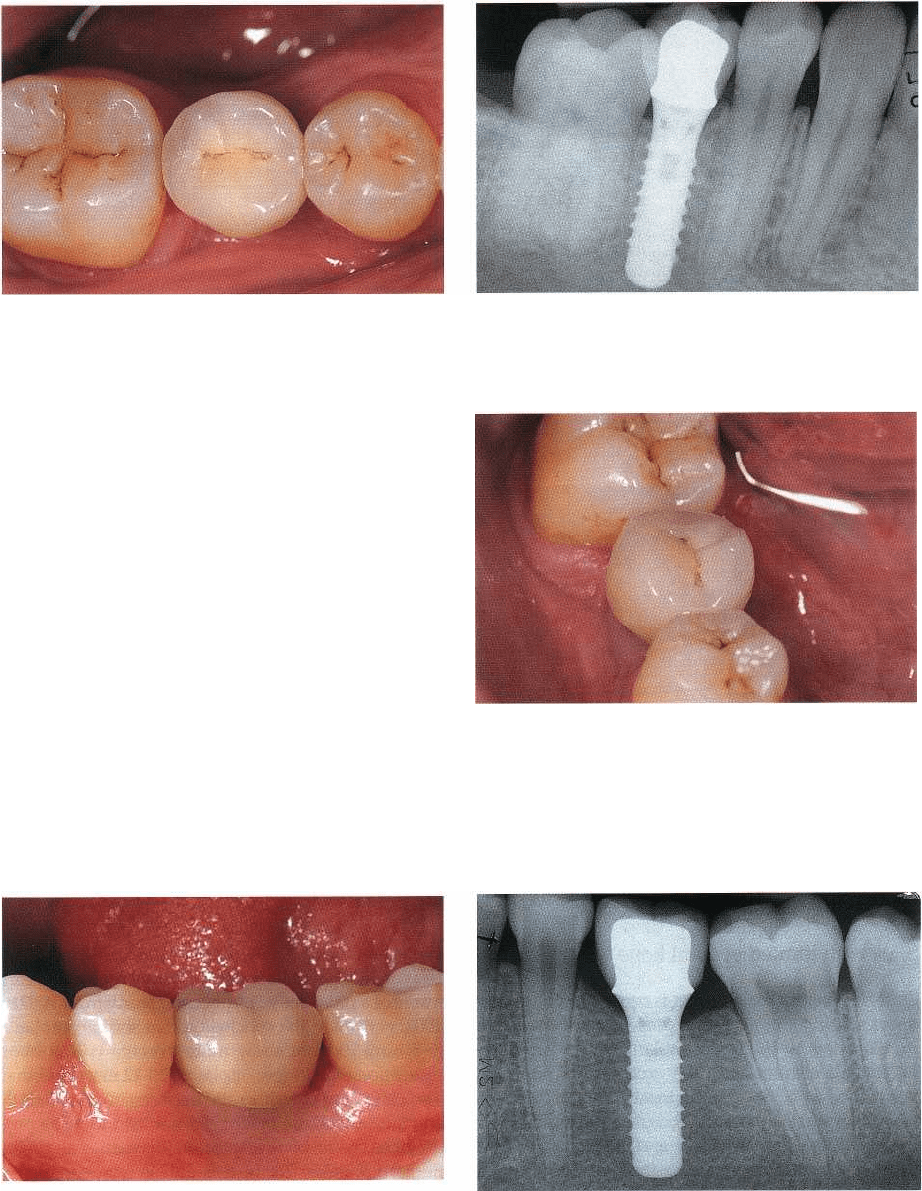
Fig. 41-64. Occlusal view of a single-tooth implant res
-
toration replacing a missing mandibular right second
premolar.
a bone-mapping, should identify whether it is possible
to have an implant placement in combination with a
lateral bone augmentation procedure according to a
simultaneous approach. If the local bone anatomy
requires a bone augmentation according to a staged
protocol, one has to carefully ponder and discuss with
the patient if this additional effort, risk and ultimately
also cost can be justified by an anticipated implant
restoration featuring close-to-ideal axial contours and
embrasures.
A clinical example demonstrating the potential of
increased-diameter implants for the optimal replace-
ment of a single missing mandibular molar is given in
Figs. 41-67 and 41-68.
Fig. 41-65. The 5-year radiographic follow-up displays
favorable bony conditions around this 12 mm solid
screw implant.
Fig. 41-66. On the oblique view one can notice that an
axial contour similar to that present on the adjacent
natural teeth has been applied to facilitate oral hygiene
and to assure adequate soft tissue (cheek and tongue)
guidance and support.
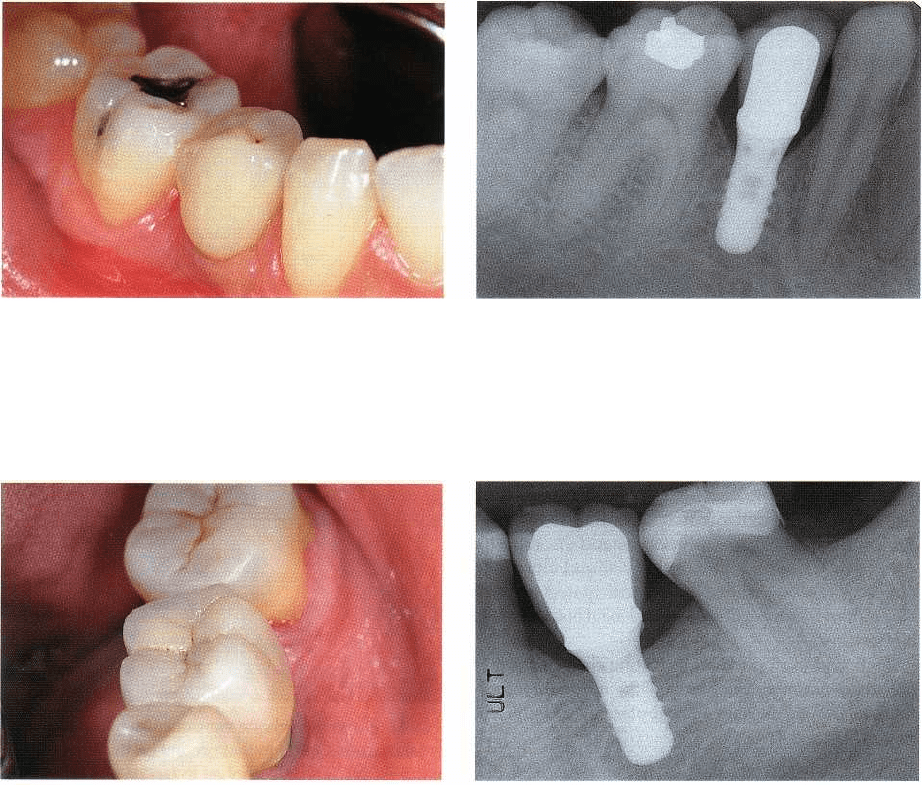
Fig. 41-67. In a case of the replacement of a single miss
-
ing molar, ideally the use of an implant with corre-
sponding dimensions is recommended to permit a res-
toration featuring optimal subjective comfort and clean-
sibility.
Fig. 41-68. On the 1-year radiographic follow-up a di-
ameter-increased ("wide neck") implant can be noted
which is essential for a suprastructure design without
extremely open interdental embrasures, which would
be prone to food retention and oral parafunctions.
964 • CHAPTER 41
Fig. 41-69. Clinical aspect of a single-tooth implant res
-
toration in the mandibular right premolar area.
Fig. 41-70. The related 2-year follow-up radiograph
shows a so-called unfavorable relationship between the
height of the suprastructure and the length of the sup
-
porting implant. The placement of a longer implant
was not possible due to the limited local bone condi-
tions.
Fig. 41-71. Oblique view of a molar single-tooth im
-
plant restoration in the left mandible.
Sites with limited vertical bone volume
Quite frequently the clinician is confronted with pos-
terior single-tooth gaps that present all of the major
prerequisites for successful implant therapy listed ear
lier in this chapter, with the exception of sufficient
vertical bone height for the insertion of an implant
featuring what is broadly accepted as an adequate
length of the implant itself and in relation to the
prospective length of the suprastructure. The question
that arises is whether there is a minimal implant
length required in the context of posterior single-tooth
restorations and whether the ratio between implant
length and suprastructure length has an influence on
crestal bone resorption and ultimately on the longev-
ity of the entire implant-suprastructure complex. The
Fig. 41-72. A short diameter-increased screw implant
supporting a long molar-sized suprastructure is dis-
played on the 1-year follow-up radiograph. Note that a
normal level of the first bone-to-implant contact has
been maintained.
analysis of the respective implant data collected at the
University of Geneva School of Dental Medicine in the
frame of a prospective multicenter study from 1989 to
2002, permitted the conclusion that shorter implants
(
6-8 mm) did not show more average crestal bone
resorption than longer implants (10-12 mm), and that
a so-called unfavorable ratio between implant length
and suprastructure height did not lead to more pro-
nounced crestal bone resorption (Bernard et al. 1995a,
Bernard & Belser 2002). This data is corroborated by
other recently published reports (ten Bruggenkate et
al. 1998, Bischof et al. 2001, Deporter et al. 2001).
Two examples of respective clinical anecdotal-type
evidence, one premolar-size and one molar-size sin-
gle-tooth restoration, are presented in Figs. 41-69 and
41-70 and Figs. 41-71 and 41-72.
IMPLANTS IN THE LOAD CARRYING PART OF THE DENTITION • 965
Table 41.6. Indications for screw-retained posterior
fixed implant restorations
Parameters to consider:
•
implant shoulder location incompatible with a cemented
suprastructure, i.e. inaccessible for meticulous excess
cement removal (> 2 mm submucosally)
•
reduced intermaxillary distance (< 5 mm)
•
foreseeable need for reintervention at the respective
implant site
•
extended implant-supported rehabilitations, involving
numerous implants
•
high overall level of complexity (e.g. non-parallel implants)
CLINICAL APPLICATIONS
Screw-retained implant restorations
For many years there was a strong tendency to design
most of the fixed implant restorations as screw-re-
tained suprastructures. Retrievability, and by this
maintaining the possibility for modification, exten-
sion or eventually repair of the prosthesis, was the
main rationale for this strategy. One should be aware,
however, that this approach also encompasses notable
specific inconveniences: colonization of the inner
compartments of the implant-abutment-suprastruc-
ture complex with mostly anaerobic microorganisms,
risk for loosening or fracture of screws, increased
technical complexity and related costs, possible inter
-
ference with structural parameters (weakening of the
metal-ceramic design) and esthetics, as well as a
"
higher maintenance profile" (Sutter et al. 1993, Wie
1995, Hebei & Gajjar 1997, Keller et al. 1998). As far as
the microbial colonization is concerned, it remains
unknown to date whether and under which condi-
tions this may have an adverse effect on the longevity
of osseointegrated implants.
For these reasons there exists currently a distinct
trend towards cementable fixed implant restorations
in the load carrying part of the dentition.
The main indications for screw-retention are listed
in Table 41-6.
Transocclusal screw-retention
If for one of the aforementioned reasons a transoc-
clusally screw-retained suprastructure is adopted,
several parameters should be taken into considera-
tion. First, the screw-access channel should be centred
on the occlusal surface in order not to interfere too
much with the area to be occupied by the cuspids.
A typical clinical example documenting an indica-
tion for a screw-retained posterior single-tooth resto-
ration is given in Figs. 41-73 to 41-75. A reduced inter
-
arch distance has led to a deeper than usual implant
shoulder location which in turn is neither accessible
for well-controlled excess cement removal nor in
reach
Fig. 41-73. Left lateral view showing the intermaxillary
relationship of a young patient in centric occlusion.
The missing maxillary second premolar has been re-
placed by a single-tooth, screw-retained implant resto
-
ration. Screw-retention was chosen for two reasons:
limited interocclusal distance and implant shoulder lo
-
cation incompatible with cementation.
Fig. 41-74. 1-year follow-up radiograph of the de
-
scribed 8 mm solid screw implant.
Fig. 41-75. Ideally, the screw-access channel should be
located in the center of the occlusal surface. This re-
duces both the risk for interference with an appropriate
metal-ceramic design in general, and the risk for porce
-
lain fractures in particular.
966 • CHAPTER 41
Fig. 41-76. Occlusal view of a mandibular master
model comprising two posterior implant analogues
and a prepared natural second premolar abutment.
Note the proximity of the mesial implant and the sec
-
ond premolar on the one hand, and the distinct lingual
position of the two implants on the other.
Fig. 41-78. The related 3-year follow-up radiograph
documents an only minimal distance between implant
shoulder and occlusal surface. Under such conditions,
a slight reduction of the alveolar ridge prior to implant
placement would have provided more vertical leeway
for compensating the lingual implant position and ulti
mately for covering the occlusal screw.
for the patient's routine oral hygiene. In order to bene
-
fit from their superior surface quality characteristics
and marginal precision, prefabricated machined cast-
on components have been used for the respective
suprastructure fabrication. Ideally, the screw-access
channel occupies a restricted area in the centre of the
occlusal table, and the distance from the head of the
screw to the occlusal surface should be sufficient for a
subsequent composite cover-restoration (Fig. 41-75).
Furthermore, the principles of the metal-ceramic
technology require a well-defined space for develop-
ing an adequate metal support for a uniform thickness
of the overlaying stratification of porcelain. Even in a
case of a well-centred occlusal perforation, the latter
occupies close to half of the mesio-distal and oro-facial
diameter of the occlusal table, and thereby signifi-
cantly weakens the overall mechanical resistance of
Fig. 41-77. The clinical view of the completed transoc
-
clusally screw-retained three-unit implant-supported
FPD demonstrates that the lingual implant position did
not allow for a suprastructure that is in line with the
adjacent teeth. Furthermore, the screws are reaching
the occlusal surface, leaving no space for an esthetic
coverage with composite resin.
the structure. If the screw-access channel is not cen-
tered, however, additional problems are created in the
sense of both weakening the restoration and interfer-
ing with esthetical criteria. Under such circumstances
one should consider, for example, the use of angled
abutments as currently offered by most of the leading
implant systems.
Another key parameter represents the interarch
distance, or more specifically, the distance between the
implant shoulder and the plane of occlusion. Accord-
ing to our experience this distance should be at least
equal to 5 mm. This is minimal and does not permit —
for esthetic reasons — the occlusal screw to be sub-
sequently covered with a composite resin restoration.
In this context 6-7 mm are clearly more adequate.
A combination of several well-known problems,
which are frequently encountered after implant place
-
ment in the posterior mandible, are shown in Figs.
41-76 to 41-78. Two implants have been inserted to
restore a distally shortened arch with a three-unit FPD.
Owing to the local bone anatomy, the implants were
placed in a more lingual position than the original
teeth (Fig. 41-76). The — for these particular circum-
stances — too superficial implant shoulder location did
not provide sufficient distance to gradually correct the
discrepancy between the actual implant shoulder po-
sition and the ideal occlusal location. Furthermore, the
necessity to keep the screw-access in the center of the
occlusal table, and the insufficient room for composite
screw-head coverage, ultimately led to a considerable
compromise (Fig. 41-77). The final radiograph (Fig.
41-78) clearly shows that the presurgical bone volume
would have permitted a vertical reduction of the eden
-
tulous bone crest to be performed prior to implant
insertion. By this token the suboptimal implant posi-
tion could have been partially corrected by the im-
plant restoration, and the occlusal screw covered by
composite resin, or a screw-retained restoration even-