Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

ORTHODONTICS AND PERIODONTICS • 765
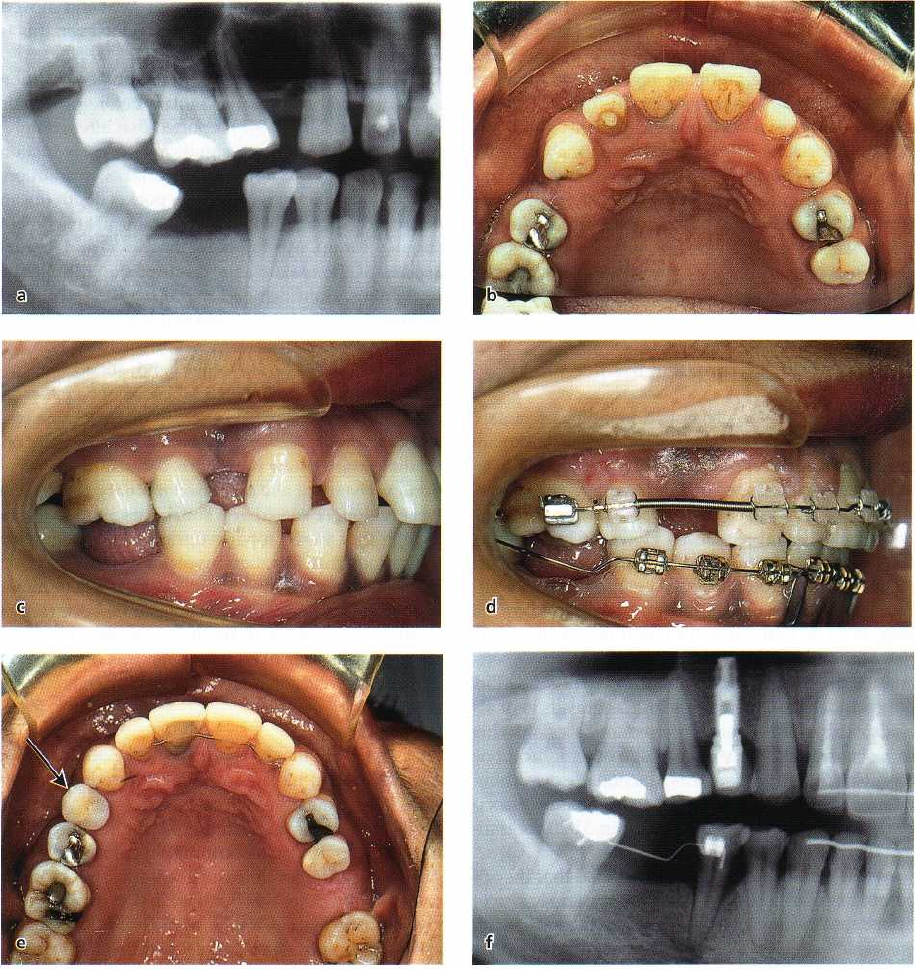
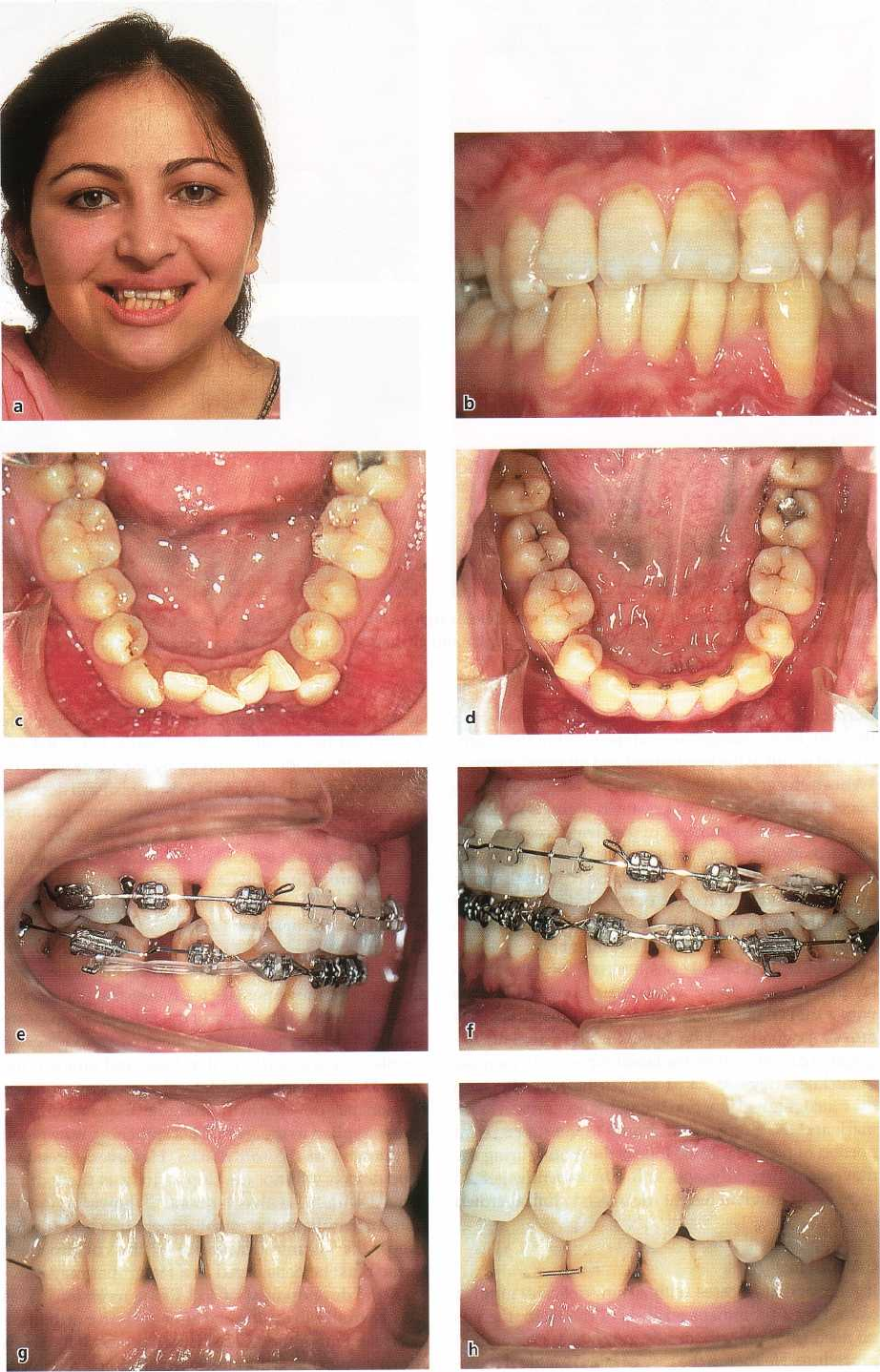
Fig. 31-20. Uprighting and leveling of maxillary and mandibular molars (compare a and f) plus consolidation of
multiple small spaces into one area before placing single-tooth implant for missing maxillary right first premolar
(arrow) in adult female patient.
would still appear sensible to avoid gross interfer-
ences, like raising the bite when a maxillary incisor in
lingual inversion is moved over the mandibular teeth,
and to mitigate evident occlusal interferences on sin-
gle teeth with markedly increased mobility. However,
it may be a futile exercise to try and eliminate all
occlusal trauma during active tooth movement and a
more practical solution is to concentrate on controlling
the inflammation. After appliance removal, however,
occlusal adjustment by selective grinding may be re-
quired. Even though good occlusal function is part of
the orthodontic treatment goal, correct cusp-fossa re-
lationships cannot always be achieved in adults with
orthodontic therapy alone. In general terms, the ad-
justment should be directed toward obtaining even
and stable tooth contacts in centric relation, a straight
forward slide from centric relation to centric occlusion
without any side shifts or lateral deviation, freedom
in centric, smooth gliding contacts in centric and ec-
centric mandibular motion, and elimination of balanc-
ing side interferences (Burgett et al. 1992).
The importance of reducing jiggling of teeth after
orthodontic treatment of patients with moderate to
advanced periodontitis may be significant: (1) tooth
mobility generally increases with loss of support for
the teeth, (2) animal experiments have shown that
bone dehiscences produced by jiggling forces will
regenerate after elimination of the jiggling trauma,
and (3) occlusal adjustment may be a factor in the
healing of periodontal defects, especially bony de-
766 • CHAPTER
31
fects, after periodontal treatment. Therefore, the
bonded orthodontic retainers, which stabilize the
teeth, may secure optimal conditions for improved
periodontal healing and bone regeneration after the
orthodontic treatment period (Fig. 31-5). In fact, long-
term follow-ups of orthodontic patients with ad-
vanced periodontal tissue breakdown may demon-
strate better periodontal conditions, with marked cre-
stal lamina dura contours, many years after appliance
removal than at the end of the orthodontic treatment
(Figs. 31-7, 31-8). If bonded retainers had not been
used in many such cases, the most affected teeth
would probably have been lost with time.
Molar uprighting, furcation involvement
The problem of mesially tipped mandibular molars
because of non-replacement of missing first molars
has been the subject of many anecdotal reports over
the past 30 years. Tipped molars have been considered
a causative or at least an aggravating factor for future
periodontal tissue breakdown. However, Lundgren et
al. (1992) recently observed that 73 molars that had
remained in a markedly tipped position for at least 10
years, with most molars having been tipped for as
long as 20-30 years, did not constitute an increased
risk for initiation or aggravation of moderate peri-
odontal disease at their mesial surface. The study did
not consider the potential risk for aggravation of al-
ready established advanced periodontitis lesions.This
lack of correlation may not exclude other indications
for molar uprighting, such as functionally disturbing
interferences, paralleling or space problems associ-
ated with prosthetic rehabilitation (Fig. 31-20), or trau
matic occlusion.
In this context it must be emphasized that the ap-
parent angular bone loss along the mesial surface of
tipped molars may be illusive and solely represent an
anatomic variation, since lines drawn from the adja-
cent cemento-enamel junctions appear to parallel the
alveolar crest (Ritchey & Orban 1954). While upright-
ing such a tooth appears to cause a shallowing-out of
the angular defect, with new bone forming at the
mesial alveolar crest, it may merely reflect the inclina
-
tion of the molar relative to the alveolar bone, and the
attachment level remains unchanged. When there is a
definite osseous defect caused by periodontitis on the
mesial surface of the inclined molar, uprighting the
tooth and tipping it distally will widen the osseous
defect. Any coronal position of bone may be due to the
extrusion component of the mechanotherapy.
Furcation defects generally remain the same or get
worse during orthodontic treatment. For example, if
tipped molars have furcation involvement before or-
thodontic uprighting, simultaneous extrusion may in
-
crease the severity of the furcation defects, especially
in the presence of inflammation (Burch et al. 1992).
Hence, initial periodontal therapy and maintenance is
essential. The mandibular molar can be split into two
roots, one or both of which may be kept and moved
orthodontically into new positions. However, this is
difficult treatment (Muller et al. 1995).
In a thorough study of periodontal condition
around tipped mandibular molars before prosthetic
replacement, Lang (1977) reported that after comple-
tion of the hygiene phase, significant pocket reduction
(mean 1.0 mm) was noted on all surfaces. In addition,
a further significant reduction in pocket depth (mean
0.6 mm), associated with a gain of clinical attachment
(
mean 0.4 mm), was found on the mesial and lingual
aspects of the molars as a result of the orthodontic
uprighting. He concluded that uprighting of tipped
molars is a simple and predictable procedure, pro-
vided excellent plaque control is maintained.
Kessler (1976), on the other hand, stated that up-
righting of mesially inclined molars is not a panacea,
and showed some cases in which evident bone loss
and furcation involvement developed during the or-
thodontic uprighting procedure. Because of the furca
-
tion involvement and increased mobility, these teeth
were no longer considered suitable as abutments, al-
though they were properly uprighted. Radiographic
indications that furcation involvement may develop
between the roots at the end of orthodontic molar
uprighting is evident also in other studies, even when
extrusive movement of the tipped molars has been
avoided (Diedrich 1989). However, it is not unlikely
that this radiolucent area reflects immature bone.
Conclusion
As risks may be involved in orthodontic uprighting of
mesially tipped molars in cases with periodontal le-
sions along their mesial surface, or with furcation
involvement, the indications for molar uprighting
must be apparent. Excellent oral hygiene is required
during the orthodontic treatment, with careful consid
-
eration of the force distribution, and avoiding extru-
sion as much as possible. The developments of regen
-
erative techniques may make it possible in the future
to obtain better outcomes in orthodontic therapy of
periodontally compromised patients.
Tooth movement and implant esthetics
Osseointegrated implants may be used (1) to provide
anchorage for orthodontic tooth movement and later
serve as abutments for restorative treatment, and (2)
to replace single missing teeth. The use of implants as
anchors for orthodontic treatment is discussed in
Chapter 43, and will not be dealt with here.
It is difficult to achieve esthetically satisfactory re-
sults with artificial crowns on single-tooth implants,
and the orthodontist may play a role in the interdisci-
plinary treatment planning team of specialists. There
are at least three areas where orthodontics may be
considered:
• redistribution of the available space in the dental
ORTHODONTICS AND PERIODONTICS • 7
6
7
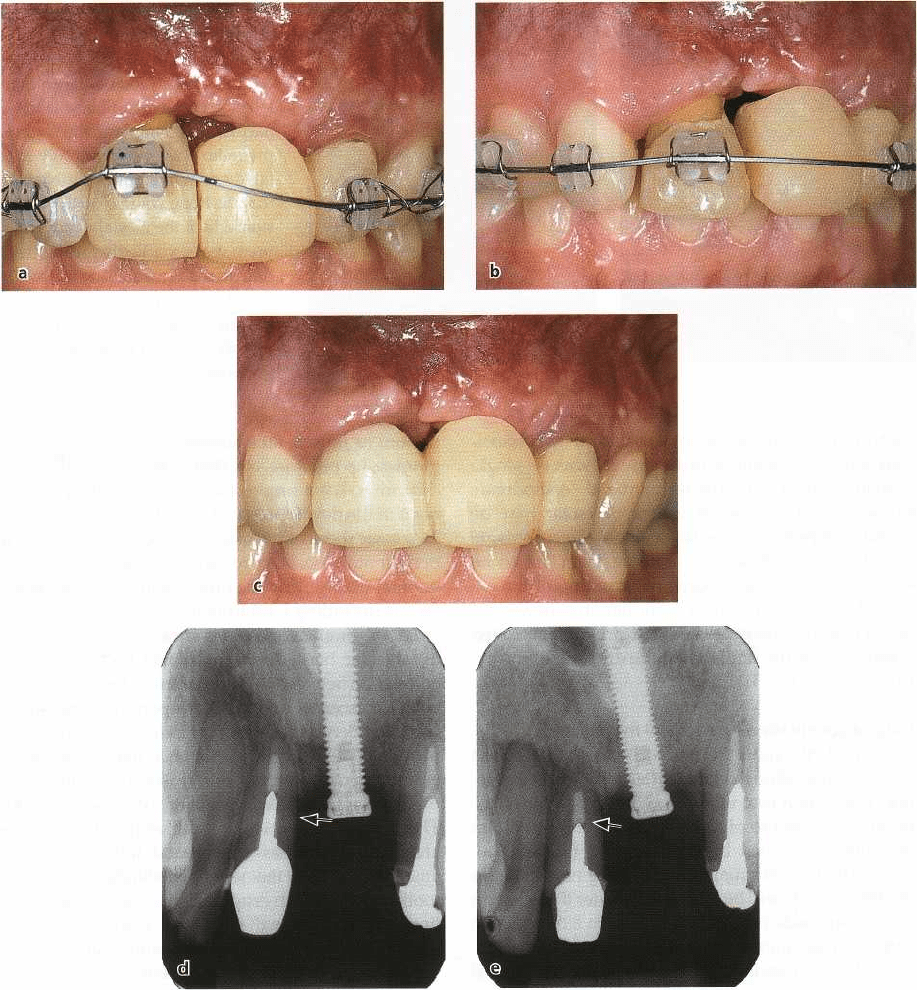
Fig. 31-21. Orthodontic improvement of periodontal soft and hard tissues associated with implant placement and a
large anterior defect in young adult female patient. As in Fig. 31-15 the periodontal tissues will follow the selec-
tively extruded incisor incisally (a-c), and thus improve the possibilities for a successful connective tissue graft
from the palate when the gingival papillae is reconstructed. Note the more incisal relationship of bone level relative
to
the implant in the radiographs before and after treatment (arrows in d,e).
arch when tooth positions for implant placement are
not optimal
•
orthodontic ridge augmentation by vertical tooth
movement
•
orthodontic ridge augmentation by horizontal
tooth
movement.
Redistribution of space
Orthodontic movement of neighboring teeth to opti
mal
positions is often required in association with
placement
of implants substituting missing maxillary
central or
lateral incisors (Spear et al. 1997). Another
common indication is a lack of adequate space for the
implant. Fig. 31-20 illustrates a typical case with mul-
tiple small spaces between the teeth and not enough
room to place an implant in the maxillary first premo
lar
region.
Ridge
augmentation - vertical movement
During selective orthodontic extrusion of one single
tooth, both the alveolar bone and the soft periodontal
tissues will follow the extruded tooth in an incisal
direction, as discussed under forced eruption earlier in
this chapter. By this means, it is possible to signifi-
768 • CHAPTER
31
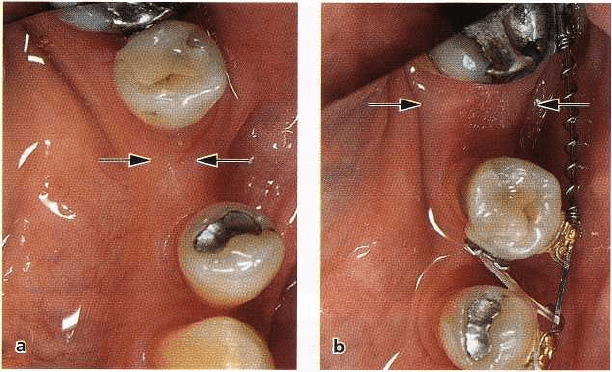
Fig. 31-22. Orthodontic ridge aug
-
mentation before implant place-
ment. Since the buccolingual
width of the alveolar bone on the
left side of the mandible was too
narrow for an implant, the second
premolar was orthodontically ro-
tated and moved mesially. Note
that the bone volume on the ten-
sion side of the mesially moved
premolar is markedly greater than
that on the pressure side (arrows).
It will now be possible to place
the implant in the position pre-
viously occupied by the second
premolar.
cantly improve the periodontal tissue esthetics associ
-
ated with fabrication of prosthetic crowns on single
implants (Fig. 31-21). The technique of "orthodontic
extraction" of a hopeless incisor or molar may be
useful to improve the results for single-tooth implants
in patients in whom one or more teeth are to be
extracted. Following progressive grinding of the ex-
truded tooth to prevent it from jiggling, new peri-
odontal tissues are generated that provide improved
conditions for the implant, after extraction of the ex-
truded tooth (Fig. 31-15).
Ridge
augmentation — horizontal movement
If an implant cannot be placed because of reduced
buccolingual ridge thickness after a previous extrac-
tion, one option is to move a premolar into the eden-
tulous space and to place the implant in the position
previously occupied by the premolar (Spear et al.
1997). The buccolingual volume of the new bone on
the tension side will be markedly greater than that on
the pressure side (Fig. 31-22). This is an alternative to
surgical ridge augmentation (GBR or bone graft). Fig.
31-22 shows a case in which the mesial movement and
uprighting of a mandibular first premolar provided
new bone of adequate width for implant placement in
a
previously atrophied alveolar bone area. Similar
generation of bone can be obtained in patients who
have no molars by moving a terminal premolar dis-
tally in the dental arch.
GINGIVAL RECESSION
Labial recession
"Normal" age changes
Gingival recession, with exposure of cementum on
facial surfaces of teeth, may occur on single or multi-
ple teeth. Many factors have been implicated in the
etiology, including plaque, position of the tooth in the
arch, faulty toothbrushing, traumatic occlusion, high
frenum or muscle attachments, lack in dimension of
gingiva, lip pressure, etc. (Baker & Seymor 1976). It is
difficult to see a single cause of, or a solitary mecha-
nism in the development of, labial gingival recession.
Two basic types of recession may occur, one related to
periodontal disease, or to factors associated with peri
-
odontal disease, and the other relating to mechanical
factors, including toothbrushing.
Labial gingival recessions are always accompanied
by alveolar bone dehiscences, and there is a direct
correlation between the millimetric extension of labial
bone dehiscences and the corresponding gingival re-
cessions (Bernimoulin & Curilovic 1977). It has been
postulated that a root dehiscence may establish an
environment which, for one reason or another, may
predispose to gingival recession (Wennstrom 1990).
The position in which a tooth erupts through the
alveolar process has a profound influence on the
amount of gingiva that will be established around the
tooth. When a tooth erupts close to the mucogingival
line, only a minimal width, or complete lack, of
gingiva may be observed labially, and localized gingi-
val recessions may occur in patients at a young age.
Thus the "normal" age changes that will then take
place are important. Longitudinal monitoring of labial
gingival dimensions during the development of the
dentition has shown that provided adequate plaque
control is established and maintained, a significant
increase of the gingival height will generally occur.
Spontaneous improvement of localized mandibular
labial recessions is the rule rather than the exception,
and in some teeth the recessions were totally elimi-
nated during a 3-year observation period (Andlin-
Sobocki et al. 1991). Also, spontaneous changes of
tooth positions in a buccolingual direction will affect
the gingival dimension.These alterations in gingival
dimensions are similar to, albeit less pronounced than,
those observed during orthodontic treatment (see be
-
low).
Favorable tooth movements, and tissue factors
Alterations of mucogingival dimensions may occur
ORTHODONTICS AND PERIODONTICS • 769
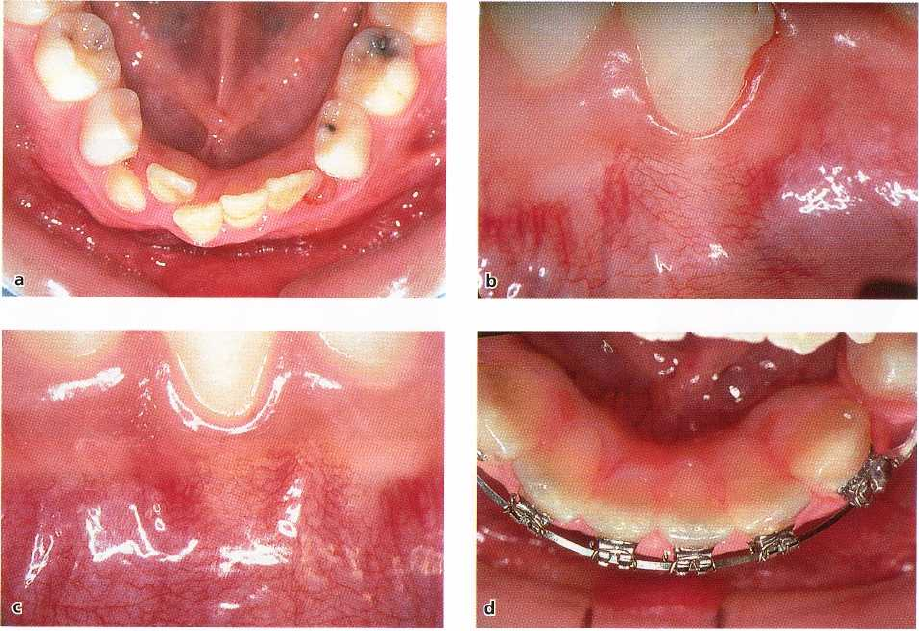
Fig. 31-23. Thin labial gingiva on prominent mandibular right central incisor (a,b) spontaneously became thicker
when the incisor was orthodontically moved lingually and aligned (c) after premolar extractions. (d) shows condi
-
tion after appliance removal.
during orthodontic treatment. Contrary to beliefs in
the past, these changes are independent of the apico-
coronal width of the keratinized and attached gingiva.
Wennstrom et al. (1987) found no relationship be-
tween the initial width of keratinized gingiva and the
tendency for development of gingival recession dur-
ing orthodontic tooth movements in monkeys. In-
stead, it is the buccolingual thickness (volume), which
may be the determining factor for the development of
gingival recession and attachment loss at sites with
gingivitis during orthodontic treatment.
A tooth that is facially positioned within the alveo-
lar process may show an alveolar bone dehiscence
with a thin covering soft tissue. When such a tooth is
moved lingually during orthodontic treatment, the
gingival dimensions on the labial aspects will increase
in thickness (Figs. 31-23, 31-24). Furthermore, because
the mucogingival junction is a stable anatomical land
-
mark and the gingiva is anchored to the supracrestal
portion of the root, it will follow the tooth during the
movement lingually and will consequently get an
increase in gingival height (decreased clinical crown
height).
Conclusion
It follows that in cases with a thin (delicate) gingiva
caused by a prominent position of the teeth, there is
no need for a preorthodontic gingival augmentation
procedure. Neither in the case of labial gingival reces-
sions should a mucogingival surgical procedure be
performed before orthodontic therapy, when the po-
sition of the tooth is improved by the treatment. The
recession, as well as the bone dehiscence, will decrease
as a consequence of the lingual movement of the tooth
into a more proper position within the alveolar bone.
If still indicated at the end of orthodontic therapy, the
surgical procedure will have a higher predictability of
success than if it had been performed before the tooth
movement (Wennstrom 1996).
Unfavorable tooth movements,
and tissue factors
Orthodontic movements of teeth
away
from the geneti
-
cally determined envelope of the alveolar process are
risk movements for development of mucogingival
problems, particularly in thin bone and gingival tis-
sues. During frontal and lateral expansion of teeth,
tension may develop in the marginal tissues due to the
forces applied to the teeth. This stretching may result
in thinning of the soft tissues. However, recession-
type defects will not develop as long as the tooth is
moved within the alveolar bone. If, however, the ex-
pansion results in the establishment of a bone dehis
-
cence, the volume (thickness) of the covering soft
tissue must be considered as a factor that may influ-
ence the development of soft tissue recessions. This
may be true both during and after the active orthodon
tic treatment period. The labial orthodontic tooth
movement
per se
will not cause soft tissue recession.
770 • CHAPTER 31

ORTHODONTICS AND PERIODONTICS • 771
However, the thin gingiva that will be the conse-
quence of such movement may serve as a locus mino
-
ris resistentia to developing soft tissue defects in the
presence of bacterial plaque and/or mechanical trau-
ma caused by improper toothbrushing techniques, or
orthodontic correction of marked rotations of the in-
cisors.
For stability reasons as well, expansion in the
mandibular arch should normally be avoided, if pos-
sible. If frontal expansion is still performed in associa
-
tion with orthodontic therapy, the buccolingual thick-
ness of the hard and soft tissues should be evaluated.
If surgical intervention is considered necessary in or-
der to reduce the risk for development of soft tissue
recessions, this should aim at increasing the thickness
of the covering tissue (e.g. grafts), and not the apico-
coronal width of the gingiva.
Conclusion
Before any kind of orthodontic therapy is started, it is
important to check the buccolingual thickness of the
bone and soft tissues on the pressure side of all teeth,
which are to be moved. When tissues are delicate and
thin, careful instructions in adequate plaque control
measures should be provided, and controlled before
and during treatment as well as after removal of the
fixed appliances, in order to reduce the risk for devel-
opment of labial gingival recession.
Interdental recession
Esthetic considerations with regard to defect papillae
Until recently, most clinical emphasis with regard to
gingival recession was given to the labial defects. If
left untreated, most labial gingival recessions will not
progress significantly with time, at least if oral hy-
giene is good, and the main indication for treatment
is
the esthetic implications for the patient. From an
esthetic point of view, however, it would appear that
interdental recession, manifest as more or less pro-
nounced empty spaces ("dark triangles") between the
teeth, would be equally or more important. Compared
with a labial recession, in most patients the loss of
interdental papillae would be more visible, both in
normal conversation and upon smiling.
Since quality of life (esthetics and lack of pain) has
become increasingly more important in recent years
in selection of periodontal therapies, disfigurement of
the gingival papillae during orthodontic treatment of
periodontal patients must be avoided, if possible. The
development of interdental recession during ortho-
dontic treatment in adults may be caused by one of
three factors: (1) advanced periodontal disease, by the
tissue destruction or due to pocket elimination by
surgery, (2) triangular tooth shape due to abnormal
interproximal wear of teeth in crowded positions be-
fore the orthodontic treatment, and (3) diverging roots
of teeth due to improper bracket placement. To begin
with, there is an obvious difference in dental esthetics
between patients with advanced periodontitis who
have been treated according to "old" and "new" con-
cepts for periodontal therapy. In the past, pocket elimi
-
nation by gingivectomies frequently resulted in ad-
vanced root exposure and complete loss of interdental
papillae (Fig. 31-7). However, even with careful non-
surgical periodontal therapy in the preparation of
patients with advanced periodontal disease for ortho-
dontic treatment, the clinical outcome of the interdis-
ciplinary treatment will normally result in marked
interdental recessions, if special precautions are not
taken (see below)
Clinical options
for treatment
There are only a few options available for the treat-
ment of interdental gingival recession associated with
orthodontic treatment in the periodontal patient:
1.
mucogingival surgery, using coronally positioned
flaps and GTR techniques (Pini Prato et al. 1992)
2.
the provision of a gingival prosthesis
3.
orthodontic paralleling of the roots of neighboring
teeth
4.
mesio-distal enamel reduction ("stripping").
Of these techniques, the mucogingival surgery as-
pects are discussed in Chapter 27, and will not be
commented on here. The gingival prosthesis may be
useful in cases of markedly compromised dentitions,
where the psychological implications of having pro-
nounced retractions are serious. It may be regarded as
a last resort. In contrast, the mesio-distal contouring
of teeth is a very useful technique to routinely improve
the esthetic results achieved by orthodontic treatment
in most adult and adolescent patients (Figs. 31-3, 31-4,
31-6, 31-25).
Benefits of mesiodistal enamel reduction
("stripping")
Introduced by Tuverson in 1980, mesio-distal recon-
touring of teeth has now become a routine procedure
in orthodontics. It is generally performed on three
indications: (1) treatment of slight-to-moderate
crowding without arch expansion, (2) correction of
width discrepancies (so-called TSD = tooth size dis-
crepancies) between maxillary and mandibular teeth,
and (3) to prevent interdental recession from develop-
ing during orthodontic treatment. The principle in-
Fig. 31-24. Marked labial gingival recession on prominent left mandibular canine in female young adult patient (a
-
c). After extraction of two premolars and the left central incisor (sic!), the mandibular arch was leveled orthodonti
cally (d). (e) and (f) show the clinical condition towards end of orthodontic therapy, and (g-h) at follow-up 1 year
af
ter appliance removal. Note spontaneous improvement of gingival recession (f-h).
772 • CHAPTER 31
volved in stripping is to recontour those teeth which
for one reason or another have abnormal morphology,
towards an ideal anatomical shape (Figs.
31-6, 31-25).
In doing so, a good occlusion with optimal tooth
contact point relationships and normal interdental
gingival papillary contours will be achievable (Figs.
31-
5, 31-6, 31-25).
In many adult patients with malocclusion, particu-
larly in cases with crowded and overlapping incisors,
the crowns of the incisors are much wider at their
incisal edges than at the cervical region. As the crowd
-
ing is unraveled by orthodontic levelling in these
instances, the contact point between the incisors will
become located in the incisal 1 mm, and a more or less
evident space develops above the interproximal con-
tacts of the incisors. Similar, or even more pronounced,
loss of the interdental papillae between the maxillary
and mandibular incisors, is commonly seen after or-
thodontic treatment in patients with advanced peri-
odontal destruction.
Short-term (Zachrisson & Mjor
1975)
and long-term
(
> 10 years)(Thordarson et al.
1991)
follow-up studies
after extensive grinding of teeth have demonstrated
that no harmful side-effects are observed subsequent
to the procedure, provided adequate cooling is used
during the grinding and the prepared surfaces are
made smooth and self-cleansing. After the diastema is
created, the space between the teeth is closed ortho-
dontically. As this occurs, the roots of neighboring
teeth come closer together, the contact area is length-
ened, and the reduced papilla can fill out the small
space between the teeth (Tarnow et al.
1992).
In pa-
tients with advanced periodontal disease, it is not
always possible to restitute all papillae in the denti-
tion. Even if it is not possible to eliminate the interden
-
tal recession completely after the orthodontic treat-
ment, the esthetic appearance is in most patients sub
-
stantially improved by stripping (Figs.
31-3, 31-4).
MINOR SURGERY ASSOCIATED
WITH ORTHODONTIC THERAPY
Several forms of minor periodontal surgery may be
used to improve or stabilize the results achieved by
orthodontic treatment of malocclusion. More than
30
years ago, Edwards
(1970)
described clinical tech-
niques to help prevent rotational relapse, re-opening
of closed extraction spaces (Edwards
1971),
and a
simple yet effective technique for frenotomy (Ed-
wards
1977).
At about the same time, a gingivectomy
technique to increase clinical crown length for esthetic
improvement of orthodontic results in specific situ-
ations was reported (Monefeldt & Zachrisson
1977).
Removal of gingival invaginations in extraction sites
following orthodontic space closure has also been a
subject of considerable interest to orthodontists.
Fiberotomy
The problem of relapse of orthodontically treated
teeth
in general, and rotated teeth in particular, has
been
well recognized for years. Methods to reduce the
occurrence of rotational relapse may include (1) com-
plete correction, or overcorrection, of rotated teeth,
(2)
long-term retention with bonded lingual retainers,
and
(3)
the use of fiberotomy.
Two soft-tissue periodontal entities may influence
the stability: the principal fibers of the periodontal
ligament, and the supra-alveolar fibers. Whereas the
fibers of the periodontal ligament and transseptal
groups remodel efficiently and histologically com-
pletely in only
2
to
3
months after orthodontic rotation
of teeth, the supra-alveolar fibers are apparently more
stable, with a slow turnover. Since the gingival soft
tissues are composed primarily of non-elastic col-
lagenous fibers, the exact mechanism by which the
gingival soft tissues may apply a force capable of
moving the teeth is as yet unknown. From a practical
and clinical point of view, however, the supracrestal
gingival tissues seemingly do contribute to rotational
relapse, as evidenced by the effect of the circumferen-
tial supracrestal fiberotomy (CSF) technique.
Basically this technique consists of inserting a scal
-
pel into the gingival sulcus and severing the epithelial
attachment surrounding the involved teeth. The blade
also transects the transseptal fibers by interdentally
entering the periodontal ligament space. Various
modifications of the original CSF technique have been
described, in which the scalpel is inserted below the
gingival margin, or the cut is reduced to interdental
vertical incisions buccally and lingually (Fig.
31-26).
In
neither case are surgical dressings indicated, and
clinical healing is usually complete in
7-10
days.The
fiberotomy procedure is not recommended during
active tooth movement, or in the presence of gingival
inflammation. When performed in healthy tissues af-
ter orthodontic therapy, there is negligible loss of at-
tachment (Edwards
1988).
The long-term effectiveness of fiberotomy was
evaluated in a prospective follow-up study over a
period of
15
years by Edwards
(1988).
The degree of
crowding was examined for CSF and control cases at
4-6
years and at
12-14
years after treatment. A signifi-
cant effect of the fiberotomy was observed at both time
intervals. The surgical procedure was more successful
in the maxillary than in the mandibular anterior re-
gion; more effective in alleviating rotational than
labiolingual relapse; and more useful in reducing re-
lapse in cases with severe rather than mild irregularity
of teeth. There was no clinically significant increase in
sulcus depth, nor signs of gingival labial recession.
Frenotomy
The contribution of the maxillary labial frenum to the
etiology of a persisting midline diastema, and to re-
ORTHODONTICS AND PERIODONTICS • 773
Fig. 31-25. Adult female patient with maxillary crowding and large overjet (a,b). After premolar extractions, ortho
-
dontic distalization of canines resulted in the development of marked interdental recessions in the anterior region
(c). Marked triangular incisor morphology and uneven incisal edges necessitated extensive recontouring (c,d) to al
-
low gingival fill-in after treatment (e,f).
opening of diastemas after orthodontic closure, is con-
troversial. The probability for diastema closure in the
long run is the same whether or not frenectomy is
performed. However, very hyperplastic types of fre-
num, with a fan-like attachment, may obstruct di-
astema closure and should be relocated.
In the past, the most common surgical procedure
was
frenectomy,
an excision-type operation, which was
often carried over to the palatal aspects. However, a
frequently observed complication may be an undesir-
able loss of the interdental papilla between the maxil-
lary central incisors. For this reason, the
frenotomy
(Fig.
31-27), which represents a more gentle operation, will
produce esthetically preferable results. With freno-
tomy, the attachment of the frenum to gingiva and
periosteum is severed, and the insertion of the frenum
774 • CHAPTER 31
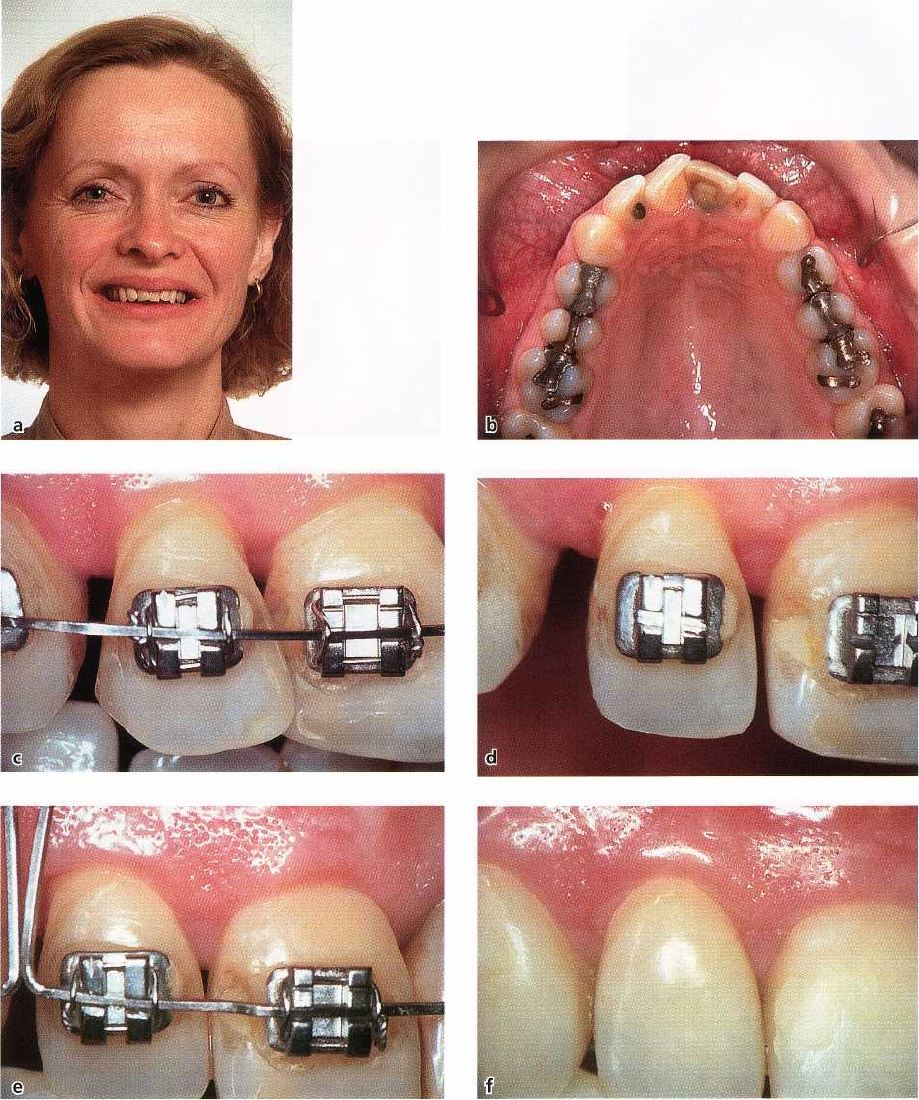
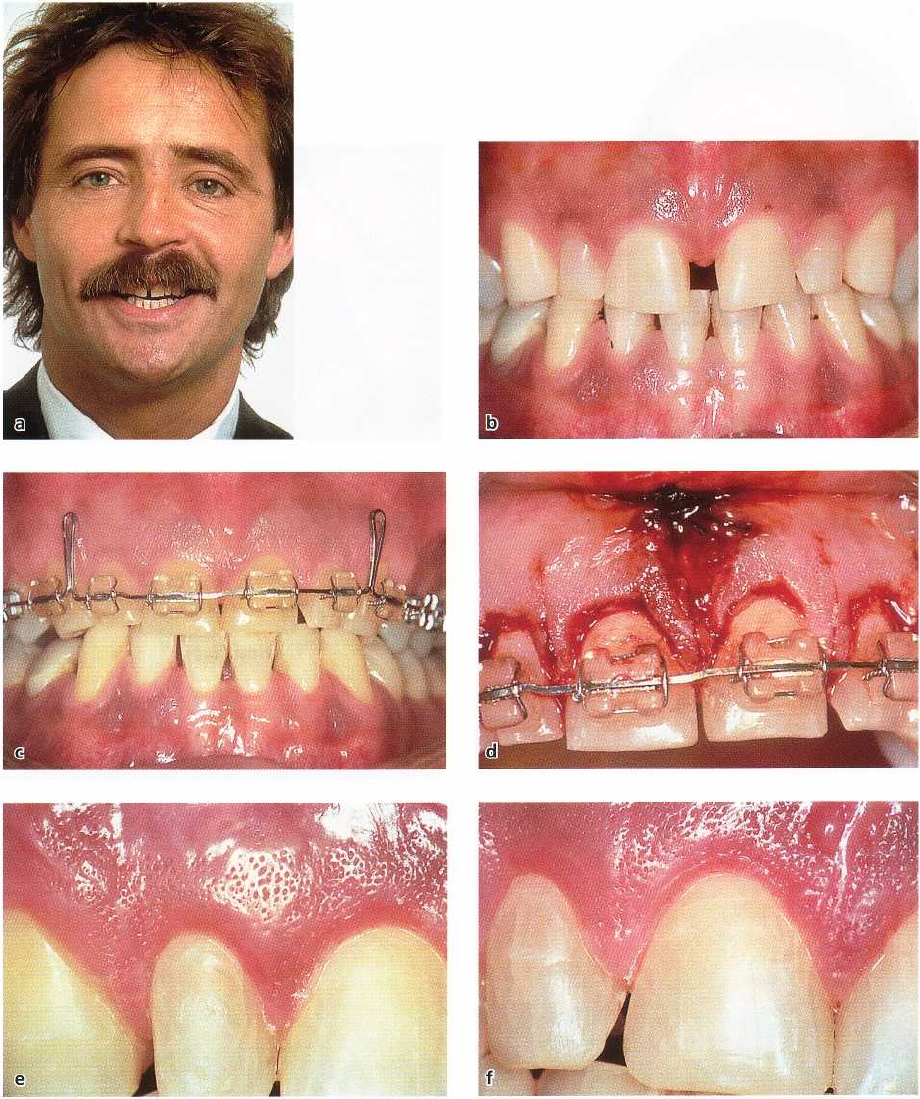
Fig. 31-26. Adult male patient with median diastema, small teeth, and low attaching frenum (a,b), in whom several
different types of minor surgeries were performed (d) in order to improve and stabilize the orthodontic treatment
result (c). Gingivectomy over four incisors increased crown length. Note healing with intact stippling 2 months
later (e,f). The surgical procedure also comprised frenotomy and fiberotomies with interdental vertical cuts (d).
is relocated several millimeters up onto the alveolar may be combined with fiberotomy and gingivectomy
mucosa.
If a marked sutural bone cleft is observed in
(Fig. 31-26).
the pretreatment radiographs, the cut is extended to
sever the fibers within the coronal part of the mid-
palatal suture.Tissue healing after a frenotomy proce-
Removal of gingival invaginations (clefts)
dure is usually uneventful (Fig. 31-27). To further
reduce the relapse tendency and/or increase clinical Incomplete adaptation of supporting structures dur
crown
height of single or several teeth, the frenotomy ing orthodontic closure of extraction spaces in adults