Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

EXAMINATION OF PATIENTS WITH PERIODONTAL DISEASE • 4
0
5
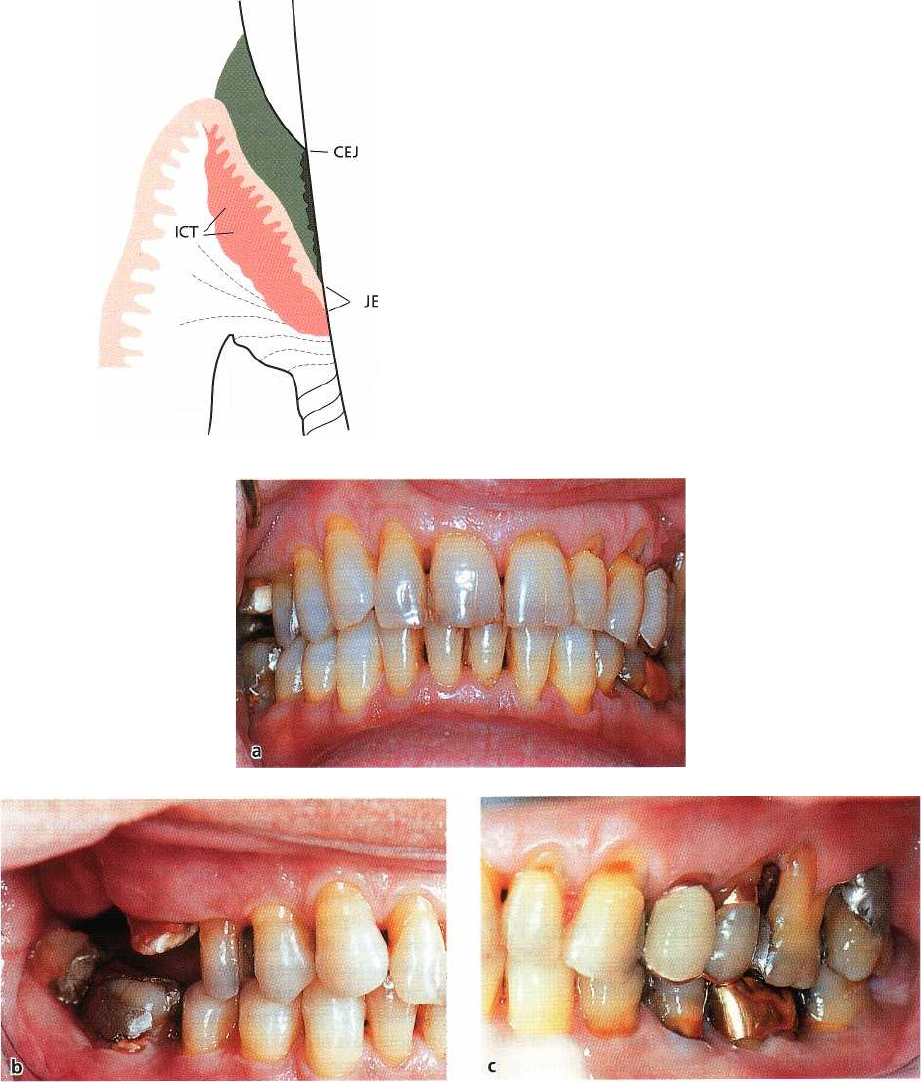
Fig. 18-3. Schematic drawing illustrating the histologic
features of periodontal disease. Note the infiltrated con
-
nective tissue area (ICT).
Fig. 18-4. (a-c) Clinical status of a 55-year-old male with periodontal disease.
are present, inflammatory lesions residing in the overt
portion of the gingiva are distinguished by probing in
the superficial marginal tissue. When the infiltrate
resides in sites with deepened pockets and attachment
loss, the inflammatory lesion in the apical part of the
pocket must be identified by probing to the bottom of
the deepened pocket.
Bleeding on probing:
a blunt periodontal probe is in-
serted to the "bottom" of the gingival pocket and is
moved gently along the tooth (root) surface (Fig. 18-5).
If bleeding is provoked by this instrumentation, the
site examined is considered inflamed.
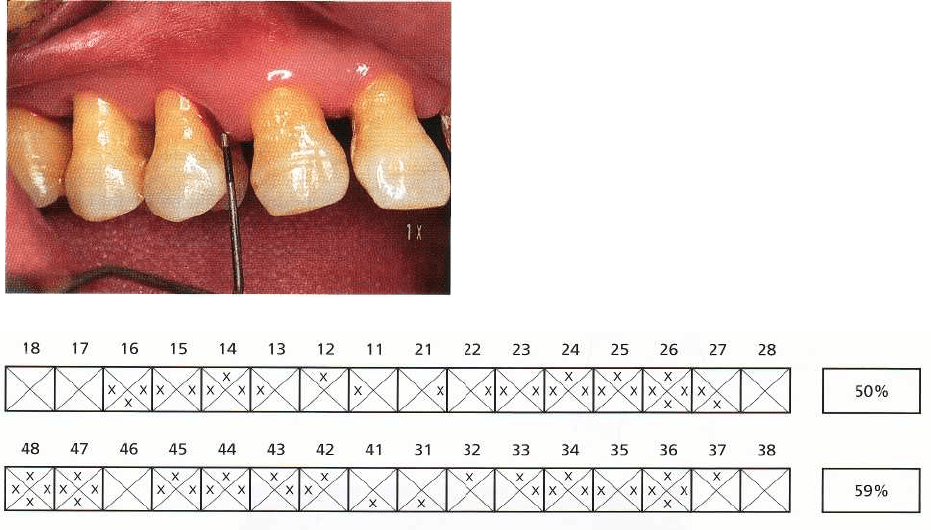
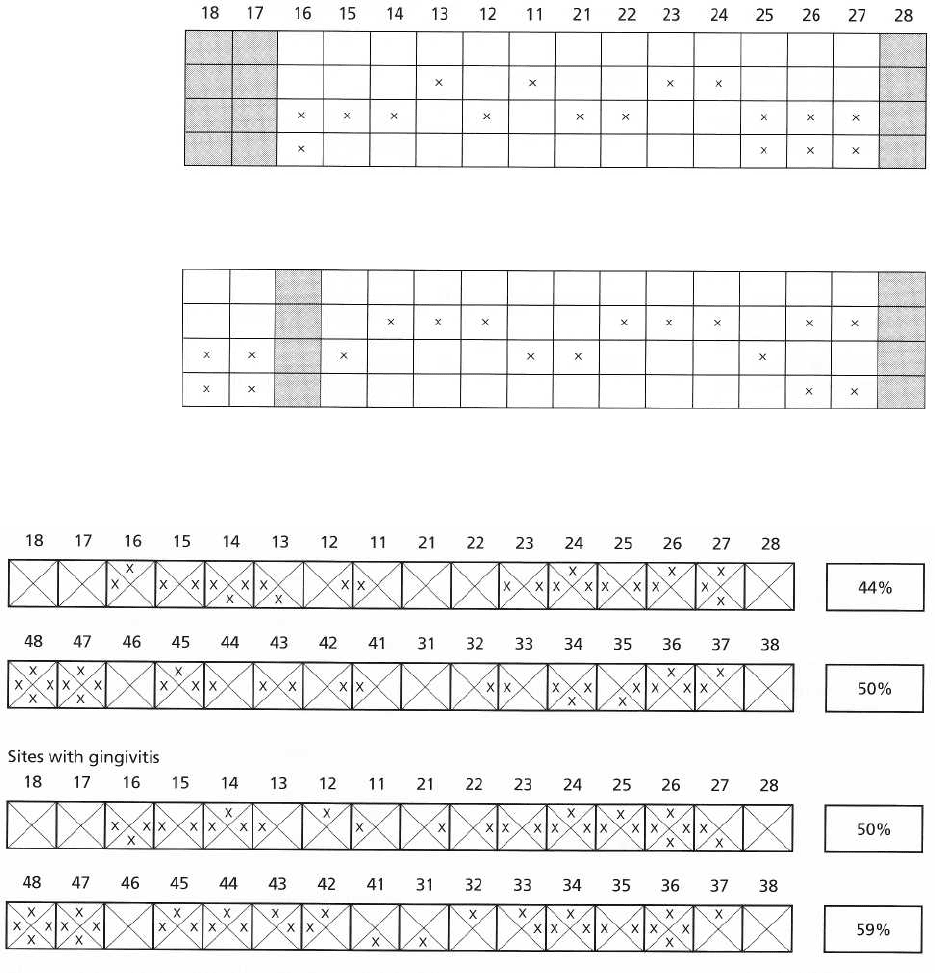
Fig. 18-6 illustrates the chart used to identify gingi-
val sites which at the initial examination of the 55-
year-old patient referred to above were found to bleed
on probing. Each tooth in the chart is represented by a
square and each tooth surface by a triangle. The upper
triangle represents the palatal/lingual gingival
unit,
the bottom triangle the buccal unit and the re
maining
fields the two approximal gingival units. A
cross is
inserted in the fields of the chart which corre-
406 • CHAPTER
18
Fig. 18-5. Pocket probing used to identify gingival in-
flammation. A site is considered inflamed if bleeding is
provoked by gentle probing to the bottom of the
pocket.
Sites with gingivitis
Fig. 18-6. The gingivitis chart of the patient seen in Fig. 18-4.
spond to the inflamed gingival units. The mean gin-
givitis score is given as a percentage figure. In the
present patient (Fig. 18-4a-c), 27 out of a total number
of 52 gingival units in the maxilla bled on probing. The
gingivitis score for the maxillary dentition is thus 50%.
The corresponding score for the mandibular dentition
is
59%. This method of charting not only serves as a
means of documenting areas of health and disease in
the dentition but similar charting during the course of
therapy will disclose sites which turn healthy or re-
main inflamed.
THE PERIODONTAL LIGAMENT —
THE ROOT CEMENTUM
In order to evaluate the amount of tissue lost in peri-
odontal disease and also to identify the apical exten-
sion of the inflammatory lesion, the following pa-
rameters should be recorded:
1.
pocket depth (probing depth)
2.
attachment level (probing attachment level)
3.
furcation involvement
4.
tooth mobility
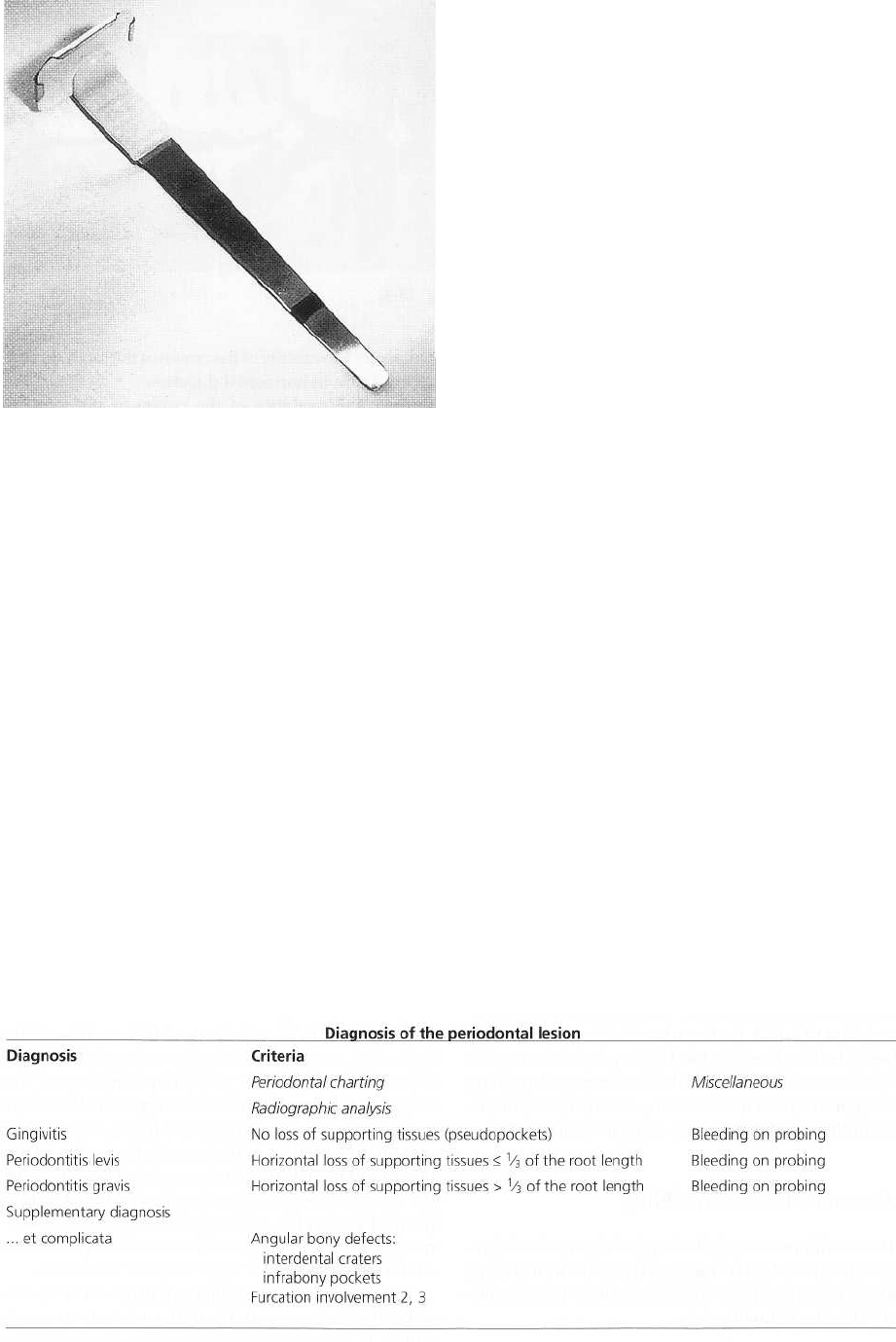
Assessment of pocket depth
The pocket (-probing-) depth, i.e. the distance from the
gingival margin to the bottom of the gingival pocket,
is
measured by means of a graduated probe (Fig. 18-7).
The pocket depth should be assessed at each surface
of all teeth in the dentition. In the periodontal chart
(
Fig. 18-10) it may be sufficient to identify only the
deepest value recorded at each tooth surface. Pocket
depth values of < 4 mm may be excluded from the
chart since such pockets can be regarded as falling
within normal variations.
Results from pocket depth measurements will only
in rare situations (when the gingival margin coincides
with the cemento-enamel junction) give proper infor-
mation regarding the extent of loss of probing attach-
ment. For example, an inflammatory edema may
cause a swelling of the free gingiva resulting in a
coronal displacement of the gingival margin without a
concomitant migration of the dentogingival epithe-
lium to a level apical to the cemento-enamel junction.
In such a situation a pocket depth exceeding 3-4 mm
represents a "pseudopocket". In other situations, an
obvious loss of attachment may have occurred with-
out a concomitant increase of the pocket depth. A
situation of this kind is shown in Fig. 18-7 at the buccal
aspect of teeth 21 and 22 (two-digit systems; FDI 1970)
where recessions of the gingiva can be seen.
Assessment of attachment level
Attachment levels may be assessed by means of a
graduated probe and expressed as the distance in mm
from the cemento-enamel junction to the bottom of the
probeable gingival pocket. The longest distance for
each tooth surface is recorded and may be included in
the periodontal chart.
EXAMINATION OF PATIENTS WITH PERIODONTAL DISEASE •
407
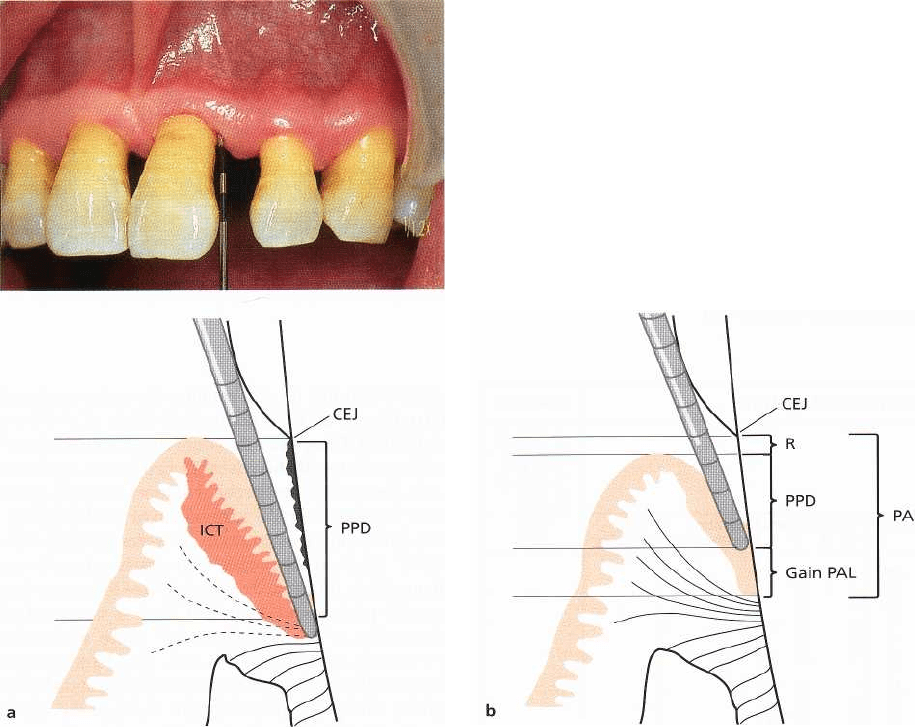
Fig. 18-7. Measurement of probing depth. Note the gin
-
gival recession at the buccal aspect of teeth 21 and 22.
Fig. 18-8. (a) In the presence of an inflammatory cell infiltrate (ICT) in the gingiva, the probe penetrates apically to
the bottom of the histologic pocket. (b) Following successful therapy the swelling is reduced (R = recession) and the
cell infiltrate is replaced by collagen. The probe fails to reach the apical part of the dentogingival epithelium. CEJ =
cemento-enamel junction. PPD = probing pocket depth. PAL = probing attachment level, R = recession. Gain PAL =
recorded-false-gain of attachment ("clinical attachment
"
).
Errors inherent in periodontal probing
The distances recorded in a periodontal examination
using a periodontal probe have generally been as-
sumed to represent a fairly accurate estimate of the
pocket depth or attachment level at a given site. In
other words, the tip of the probe has been assumed to
identify the level of the most apical cells of the dento-
gingival epithelium. Results from research published
in the 1970s have demonstrated, however, that this is
seldom the case (Saglie et al. 1975, Listgarten et al.
1976, Armitage et al. 1977, Ezis & Burgett 1978, Spray
et al. 1978, Robinson & Vitek 1979, van der Velden
1979, Magnusson & Listgarten 1980, Polson et al.
1980). Listgarten (1980) listed a variety of factors
which influence the result of a measurement made
with a periodontal probe. These factors include (1) the
thickness of the probe used, (2) malposition of the
probe due to anatomic features such as the contour of
the tooth surface, (3) the pressure applied on the in-
strument during probing, and (4) the degree of inflam-
matory cell infiltration in the soft tissue and accompa-
nying loss of collagen. Listgarten suggested that "a
distinction should be made between the histological
and the clinical pocket depth to differentiate between
the depth of the actual anatomic defect and the meas-
urement recorded by the probe".
Measurement errors depending on factors such as
the thickness of the probe, the contour of the tooth
surface and improper angulation of the probe can be
reduced or avoided by the selection of a proper instru-
ment and careful management of the examination
procedure. More difficult to avoid, however, are errors
resulting from variations in probing force and the
extent of inflammatory alterations of the periodontal
tissues. As a rule, the greater the probing force, the
deeper the penetration of the probe into the tissue. In
this context it should be realized that in investigations
designed to disclose the force used by different clini-
cians, the probing force was found to range from 3 to
130 g (Gabathuler & Hassell 1971, Hassell et al. 1973),
and also to differ by as much as 2:1 for the same dentist
408 • CHAPTER 18
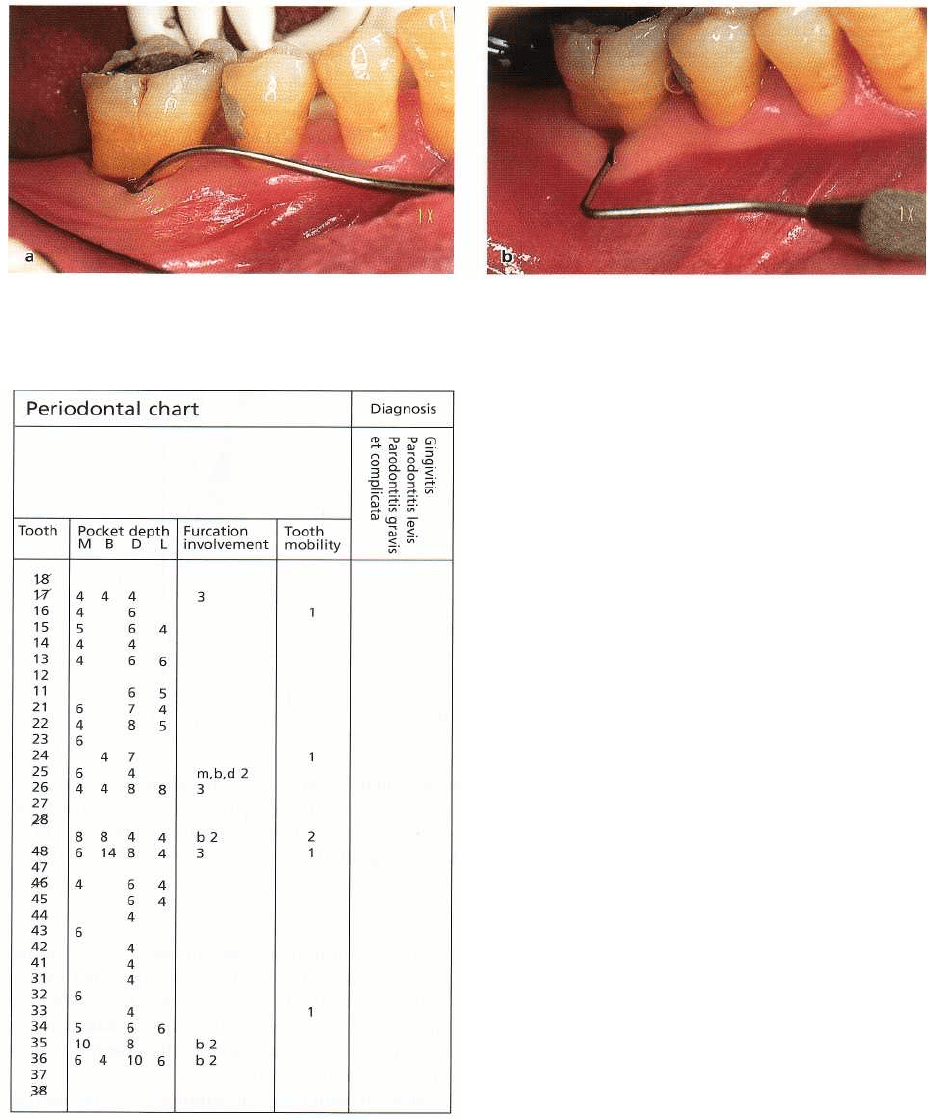
Fig. 18-9. A periodontal probe inserted into the buccal furcation area of a mandibular molar. A furcation involve
-
ment of degree 2 was found.
Fig. 18-10. Periodontal chart including the data ob-
tained from the examination of the patient presented in
Fig. 18-4.
from one examination to another. In order to exclude
measurement errors related to the effect of variations
in probing force, so-called pressure sensitive probes
have been developed. Such probes will enable the
examiner to probe with a predetermined force (van der
Velden & de Vries 1978, Vitek et al. 1979, Poison et
al.
1980). However, over and underestimation of the
"
true" pocket depth or attachment level may also
occur when this type of probing device is employed (
Armitage et al. 1977, Robinson & Vitek 1979, Poison
et
a1.1980). Thus, when the connective tissue subjacent
to
the pocket epithelium is infiltrated by inflammatory
cells, the periodontal probe will most certainly pene-
trate beyond the apical termination of the dentogingi-
val epithelium. This results in an overestimation of the
"true" depth of the pocket. Conversely, when the in-
flammatory infiltrate decreases in size following suc-
cessful periodontal treatment, and a concomitant
deposition of new collagen takes place within the
previously inflamed tissue area, the dentogingival
tissue will become more resistant to penetration by the
probe. The probe may now fail to reach the apical
termination of the epithelium. This results in an un-
derestimation of the "true" pocket depth or attach-
ment level. The magnitude of the difference between
the probing measurement and the histologic "true"
pocket depth (Gain PAL; Fig. 18-8b) may range from
fractions of a millimeter to several millimeters (List-
garten 1980).
From this discussion it should be understood that
reduction of pocket depth following periodontal treat-
ment and/or gain of attachment, assessed by peri-
odontal probing, are not necessarily signs of forma-
tion of a new connective tissue attachment in the
bottom of the previous pocket. Rather, such a change
may merely represent a resolution of the inflamma-
tory process and may thus occur without an accom-
panying attachment gain (Fig. 18-8). In this context it
should be realized that the terms "pocket depth" and
"gain and loss of attachment" in modern literature
have often been changed to the more exact terms
"
probing depth" and "gain and loss of clinical attach-
ment" or "probing pocket depth" and "probing at-
tachment level".
Current knowledge of the histopathology of peri-
odontal lesions and healing of such lesions has thus
resulted in an altered concept regarding the validity
of periodontal probing. However, despite difficulties
in
interpreting the proper significance of pocket depth
and attachment level measurements, such determina
-
tions still give the clinician a useful estimate of the
degree of disease involvement, and particularly so
EXAMINATION OF PATIENTS WITH PERIODONTAL DISEASE • 409
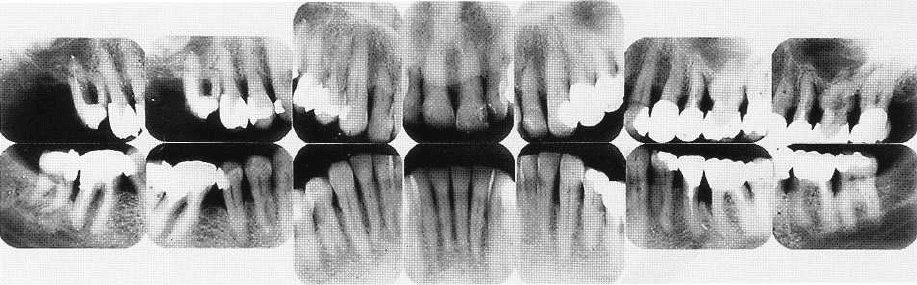
Fig. 18-11. Radiographic status of the patient presented in Fig. 18-4.
when the information obtained is related to other
findings of the examination procedure such as "bleed
-
ing on probing", and alveolar bone height alterations.
Assessment of furcation involvement
In the progression of periodontal disease around
multi-rooted teeth, the destructive process may in-
volve the supporting structures of the furcation area
(
Fig. 18-9). Elaborate therapeutic techniques must
often be used to treat such
furcation involvements
prop
-
erly. Therefore, the precise identification of the pres-
ence and extension of periodontal tissue breakdown
within the furcation area is of importance for proper
diagnosis and treatment planning.
Furcation involvements may be classified into:
Degree 1: Horizontal loss of supporting tissues not
exceeding
1
/3
of the width of the tooth.
Degree 2: Horizontal loss of supporting tissues ex-
ceeding
1
/3
of the width of the tooth, but not encom
-
passing the total width of the furcation area.
Degree 3: Horizontal "through-and-through" de-
struction of the supporting tissues in the
furcation.
The degree of furcation involvement is presented in
the periodontal chart (Fig. 18-10) together with a de-
scription of which tooth surface the involvement has
been identified on (e.g. tooth 26: m, b, d 2; tooth 48: b
2; tooth 36: b 2). A detailed discussion regarding diag
-
nosis of furcation involvements and treatment of fur-
cation-involved teeth is presented in Chapter 28.
Assessment of tooth mobility
The continuous loss of the supporting tissues in pro-
gressive periodontal disease may result in increased
tooth mobility. Increased tooth mobility may be clas-
sified in the following way:
Degree 1: Movability of the crown of the tooth 0.2-1
mm in horizontal direction
Degree 2: Movability of the crown of the tooth exceed-
ing 1 mm in horizontal direction
Degree 3: Movability of the crown of the tooth in
vertical direction as well.
It must be understood that plaque-associated peri-
odontal disease is not the only cause of increased tooth
mobility. For instance, overloading of teeth and
trauma may result in tooth hypermobility. Increased
tooth mobility can frequently also be observed in
conjunction with periapical lesions, immediately fol-
lowing periodontal surgery, etc. From a therapeutic
point of view it is important, therefore, to assess not
only the degree of increased tooth mobility but also
the cause of the observed hypermobility (see Chapters
15 and 27).
All data collected in conjunction with measure-
ments of pocket (-probing-) depth as well as from the
assessments of furcation involvement and tooth mo-
bility are included in the periodontal chart (Fig. 18-10).
The various teeth in this chart are denoted according
to the two-digit system adopted by FDI in 1970.
THE ALVEOLAR BONE
Radiographic analysis
The height of the alveolar bone and the outline of the
bone crest are examined in the radiographs in Fig.
18-
11. The radiographs provide information of the
height
and configuration of the interproximal alveolar
bone.
Covering structures (bone tissue, teeth) often
make it
difficult to identify properly the outline of the
buccal
and lingual alveolar bone crest. The analysis of
the
radiographs must therefore be combined with a
detailed evaluation of the pocket depth and attach-
ment level data in order to arrive at a correct estimate
concerning "horizontal" and "vertical" bone loss.
Following active treatment, patients must be en-
rolled in a follow-up and maintenance care program
aimed at preventing recurrence of periodontal dis-
ease. This program includes regular reexaminations
to study the periodontal conditions. Such reexamina-
410 • CHAPTER. 18
Fig. 18-12. The Eggen device for obtaining "stand
-
ardized" radiographs.
tions often require repeated radiographic analysis of
teeth and jaws at given time intervals. To enable mean
-
ingful comparative analysis, a radiographic technique
should be used which produces periodic reproducible
roentgenograms. A technique of this kind has been
described by, for example, Eggen (1969) (Fig.
18-12).
Sounding
In order to arrive at a correct diagnosis with respect to
the alveolar bone level, the presence of angular bony
defects and interdental osseous craters etc., an addi-
tional method, called "sounding", may be used. Fol-
lowing local anesthesia the periodontal probe is in-
serted into the pocket. The tip of the probe is forced
through the supraalveolar connective tissue to make
contact with the bone and the distance from the ce-
mento-enamel junction to the bone level is assessed in
mm.
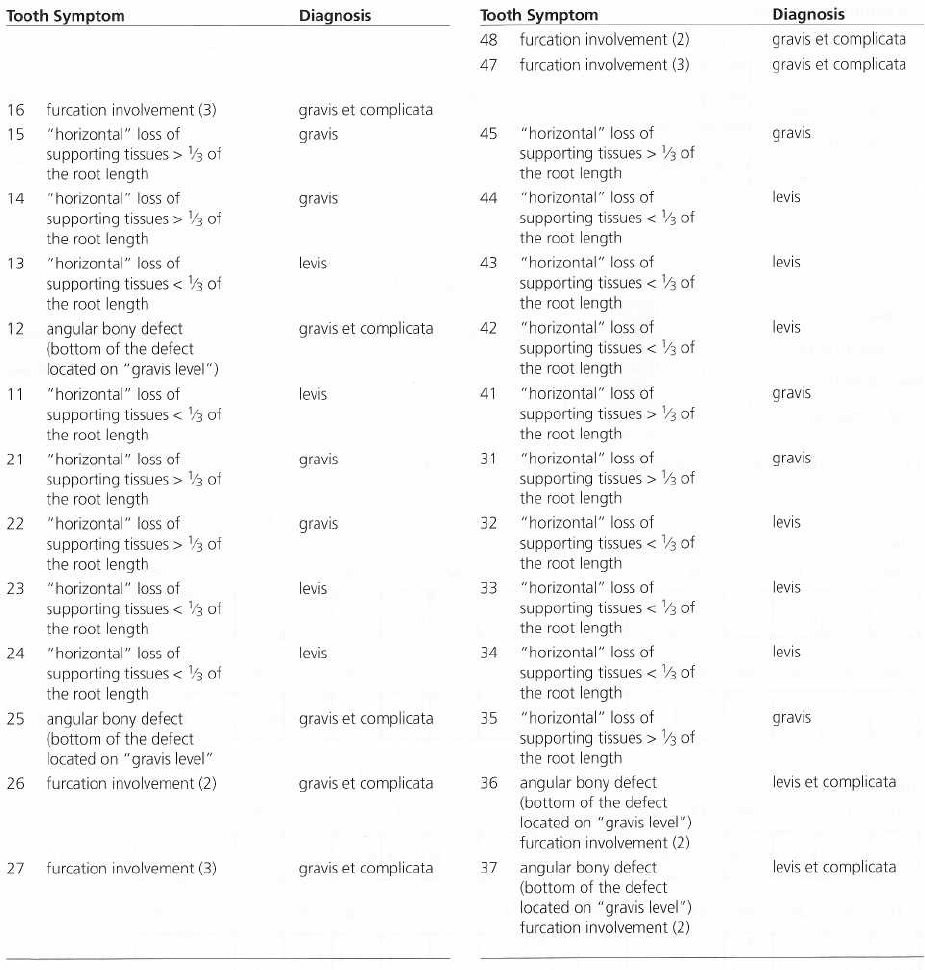
DIAGNOSIS OF PERIODONTAL
LESIONS
The information regarding the condition of the vari
ous
periodontal structures (the gingiva, the periodontal
ligament, the root cementum and the alveolar bone)
which has been obtained through the compre
hensive
examination presented above should form the
basis for
a proper assessment of the periodontal con
dition (Fig.
18-13). It is advantageous to give each
tooth in the
dentition an individual "diagnosis". Four
different "
diagnoses" may be used:
Gingivitis
This diagnosis is used when one or several gingival
units around a particular tooth are found to bleed on
probing. Probing pocket depth and probing attach-
ment level measurements and the radiographic analy-
sis
must
fail
to indicate loss of supporting tissues.
"
Pseudopockets" may be present.
Fig. 18-13. The conditions of the periodontal tissues around each individual tooth in the dentition are described us
ing different criteria (periodontal charting, radiographic analysis) and diagnosis.
EXAMINATION OF PATIENTS WITH PERIODONTAL DISEASE • 411
Periodontitis levis
(
overt periodontitis)
The pocket depth and attachment level measurements
and radiographic analysis indicate an even ("horizon-
tal") loss of supporting tissues not exceeding one third
of the length of the root. Inflammation must be pre-
sent, i.e. "bleeding on probing" will occur when the
site is probed to the "bottom of the pocket".
Periodontitis gravis (
advanced periodontitis)
Pocket depth and attachment level measurements and
the radiographic analysis indicate an even ("horizon-
tal") loss of supporting tissues exceeding one third of
the length of the root. "Bleeding on probing" to the
"
bottom of the pocket" must be present.
A supplementary diagnosis
periodontitis complicate
is used
1.
when an angular bony defect (infrabony pocket,
interdental osseous crater) is present adjacent to a
tooth, and
2.
for a multi-rooted tooth in which furcation involve-
ments of degree 2 or 3 have been identified.
A chart of diagnosis is shown in Fig. 18-14. This par-
ticular chart refers to the patient whose clinical status
is shown in Fig. 18-4a-c, periodontal chart in Fig. 18-10
and radiographic status in Fig. 18-11. The various
teeth have received the diagnoses described in Fig.
18-14.
412 • CHAPTER 18
Periodontal diagnosis
Gingivitis
Periodontitis levis
Periodontitis gravis
... et complicata
48 47 46 45 44 43 42 41 31 32 33 34 35 36 37 38
Gingivitis
Periodontitis levis
Periodontitis gravis
... et complicata
Fig.
18-14.
Chart of diagnosis describing the patient in Fig. 18-4.
Sites with plaque
Fig.
18-15.
The plaque and gingivitis chart of the patient presented in Fig. 18-4.
ORAL HYGIENE STATUS
In conjunction with examination of the periodontal
tissues, the patient's oral hygiene must also be evalu-
ated. Absence or presence of plaque on each tooth
surface in the dentition is recorded. The bacterial de-
posits may be stained with a disclosing solution to
facilitate their detection. The presence of plaque is
marked in appropriate fields in the plaque chart
shown
in Fig. 18-15. The mean plaque score for the dentition
is given as a percentage value in correspon
dence with
the system used for gingivitis.
Alterations with respect to the presence of plaque
and gingival inflammation are illustrated in a simple
way by the repeated use of the combined plaque and
gingivitis chart (Fig. 18-15) during the course of treat-
ment.
In addition to the assessment of plaque, retention
factors for plaque, such as supra and subgingival
calculus and defective margins of dental restorations,
should also be identified and included in the peri-
odontal chart.
CONCLUSION
The methods described above for the examination of
patients with respect to periodontal disease provide a
EXAMINATION OF PATIENTS WITH PERIODONTAL DISEASE • 413
thorough analysis of the presence, extent and severity
of the disease in the dentition. The correct diagnosis
for each individual tooth should form the basis for the
treatment planning of the individual case.
REFERENCES
Armitage, G.C., Svanberg, G.K. & Loe, H. (1977). Microscopic
evaluation of clinical measurements of connective tissue at-
tachment level.
Journal of Clinical Periodontology
4, 173-190.
Eggen, S. (1969). Standardisered intraoral rontgenteknik.
Sveriges Tandldkareforbunds Tidning
17, 867-872.
Ezis, I. & Burgett, F. (1978). Probing related to attachment levels
on recently erupted teeth.
Journal of Dental Research
57, Spec
Issue A 307, Abstract No. 932.
Gabathuler, H. & Hassell, T. (1971). A pressure sensitive peri-
odontal probe.
Helvetica Odontologica Acta 15,
114-117.
Hassell,
T.M., Germann, M.A. & Saxer, V.P. (1973). Periodontal
probing: investigator discrepancies and correlations between
probing force and recorded depth.
Helvetica Odontologica Acta
17, 38-42.
Listgarten, M.A. (1980). Periodontal probing: What does it
mean?
Journal of Clinical Periodontology
7,
165-176.
Listgarten, M.A., Mao, R. & Robinson, P.J. (1976). Periodontal
probing and the relationship of the probe tip to periodontal
tissues.
Journal of Periodontology
47, 511-513.
Magnusson, I. & Listgarten, M.A. (1980). Histological evaluation
of probing depth following periodontal treatment.
Journal of
Clinical Periodontology
7, 26-31.
Page, R.C. & Schroeder, H.E. (1976). Pathogenesis of chronic
inflammatory periodontal disease. A summary of current
work.
Laboratory Investigations 33,
235-249.
Poison, A.M., Caton, J.G., Yeaple, R.N. & Zander, H.A. (1980).
Histological determination of probe tip penetration into gin-
gival sulcus of humans using an electronic pressure-sensitive
probe.
Journal of Clinical Periodontology
7, 479-488.
Robinson, P.J. & Vitek, R.M. (1979). The relationship between
gingival inflammation and resistance to probe penetration.
Journal of Periodontal Research
14, 239-243.
Saglie, R., Johansen, J.R. & Flotra, L. (1975). The zone of com-
pletely and partially destructed periodontal fibers in patho-
logical pockets.
Journal of Clinical Periodontology 2,
198-202.
Spray, J.R., Garnick, J.J., Doles, L.R. & Klawitter, J.J. (1978).
Microscopic demonstration of the position of periodontal
probes.
Journal of Periodontology
49, 148-152.
van der Velden, U. (1979). Probing force and the relationship of
the probe tip to the periodontal tissues.
Journal of Clinical
Periodontology 6,
106-114.
van der Velden, U. & de Vries, J.H. (1978). Introduction of a new
periodontal probe: The pressure probe.
Journal of Clinical
Periodontal< <g y 5,
188-197.
Vitek, R.M., Robinson, P.J. & Lautenschlager, E.P. (1979). Devel-
opment of a force-controlled periodontal instrument.
Journal of
Periodontal Research
14, 93-94.
CHAPTER 19
Treatment Planning
JAN LINDHE, STURE NYMAN AND NIKLAUS P. LANG
Screening for periodontal disease
Diagnosis
Treatment planning
Initial treatment plan
Case presentation
Initial (cause-related) therapy
Re-evaluation
Planning of additional therapy
Additional (corrective) therapy
Supportive periodontal therapy
Case reports
Caries and periodontal diseases are opportunistic in-
fections associated with biofilm formation on the sur-
faces of teeth. Factors such as bacterial specificity and
pathogenicity as well as the disposition of the individ-
ual for disease, e.g. local and general resistance, may
influence the onset, the rate of progression and clinical
character of the plaque-associated dental disorders.
Findings from animal experiments and longitudinal
studies in humans, however, have demonstrated that
treatment, including the elimination or the control of
the plaque infection and the introduction of careful
plaque control measures, in most, if not all, cases
results in dental and periodontal health. Even if health
cannot always be achieved and maintained, the arrest
of disease progression following treatment must be
the
goal of modern dental care.
The treatment of patients affected by caries and
periodontal disease, including symptoms of associ-
ated pathologic conditions such as pulpitis, periapical
periodontitis, marginal abscess, tooth migration, etc.,
may from a didactic point of view be divided into
three
different stages: initial, cause-related therapy,
additional therapeutic measures (corrective phase)
and supportive periodontal therapy (or maintenance
therapy).
Treatment goals
In every patient with periodontitis, a treatment strat-
egy which includes the elimination of the opportun-
istic infection must be defined and followed. This
treatment strategy must also define the clinical out-
come parameters to be reached. Such clinical parame
-
ters include:
1.
Reduction or resolution of gingivitis (bleeding on
probing; BoP)
2.
Reduction in probing pocket depth (PPD)
3.
Elimination of open furcations in multirooted teeth
4.
Individually satisfactory esthetics and function.
Based on data obtained from longitudinal clinical
studies, which included surgical as well as non-surgi
-
cal approaches of therapy, the treatment goals may be
further specified:
1.
< 10 %, of sites BoP+
2.
No sites with PPD > 5 mm, but preferably <_ 4 mm
3.
No furcation involvement of degree II or III.
In this context it must also be emphasized that risk
factors for periodontitis that can be controlled must be
addressed as well. The two main risk factors for
chronic periodontitis are
improper plaque control
and
smoking.
Hence the treatment plan must include meas
ures to improve the patient's plaque control
perform
ance. In addition, efforts must be made to
stimulate a
smoker to enroll in smoking cessation
programs.
Initial, cause-related therapy
The objective of this treatment is the removal or con-
trol of the various biofilms.
Additional therapeutic
measures
This includes traditional therapeutic measures such as
periodontal surgery, endodontic therapy, restorative
and prosthetic treatment. The volume of corrective
therapy required and the selection of means for the
restorative and prosthetic therapy can be determined
only when the level of success of the causative therapy