Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

TREATMENT PLANNING • 415
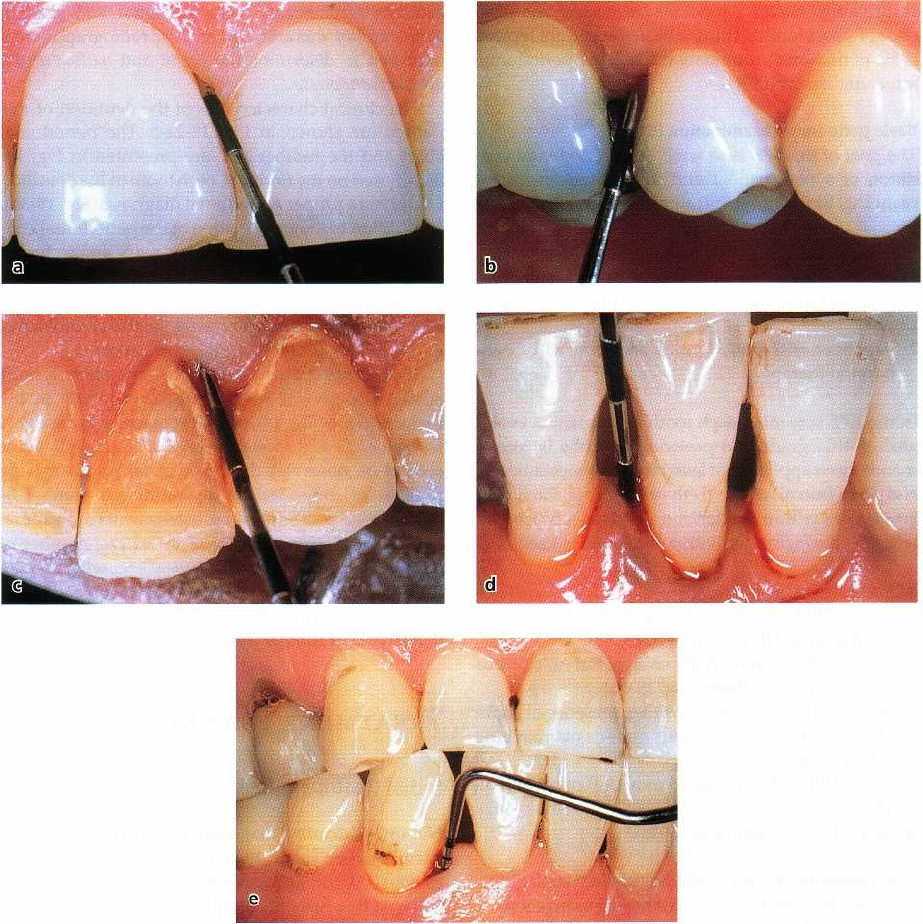
Fig. 19-1a-e. Clinical illustration of the basic periodontal examination scores. (a)
BPE
score O. (b)
BPE
score 1. (c)
BPE
score 2. (d)
BPE
score 3. (e)
BPE
score 4.
can be properly evaluated. The patient's ability to
cooperate in the overall therapy must determine the
content of the corrective treatment. If this ability is
failing or lacking, it may at times not be worth initiat-
ing treatment procedures which only in the fully co-
operative patient will permanently improve oral es-
thetics and function. The validity of this statement can
be exemplified by the results of studies aimed at as-
sessing the relative value of different types of surgical
methods in the treatment of periodontal disease. Thus,
a number of clinical trials (Lindhe & Nyman 1975,
Nyman et al. 1975, 1977, Rosling et al. 1976a,b, Nyman
& Lindhe 1979) have demonstrated that gingivectomy
and flap procedures performed in patients with
proper plaque control levels often result in gain of
alveolar bone and clinical attachment, while surgery
in plaque-contaminated dentitions may cause addi-
tional destruction of the periodontium.
Supportive periodontal therapy (SPT)
The aim of this treatment is the prevention of disease
recurrence. For each individual patient a recall system
must be designed which includes (1) self-performed
but professionally monitored plaque control pro-
grams, (2) scaling and root planing measures, (3) fluo
-
ride application, etc. In addition, this treatment in-
volves the regular control of fillings and other resto-
rations made during the corrective phase of therapy.
SCREENING FOR PERIODONTAL
DISEASE
A patient seeking dental care is usually screened for
the presence of carious lesions by means of clinical
probing and bitewing radiographs. Likewise it is im-
416 • CHAPTER
19
perative that such a patient is screened for the pres-
ence of periodontitis using a basic procedure termed
basic periodontal examination (BPE) (or periodontal
screening record (PSR)).
Basic periodontal examination (BPE)
The goal of the BPE is to screen the periodontal con-
dition of a new patient and to facilitate treatment
planning. BPE scoring will allow the therapist to iden
-
tify:
1.
A patient with reasonably healthy periodontal con-
ditions, but in need of long term preventive meas-
ures
2.
A patient with periodontitis and in need of peri-
odontal therapy.
In the BPE screening each tooth or implant is evalu-
ated. A thin graduated periodontal probe is recom-
mended and applied to at least two sites (mesio-buccal
and disto-buccal) of the teeth or implants. Each den-
tate sextant within the dentition is given a BPE score,
whereby the
highest
individual site score is used.
BPE scoring system
Score 0 = PPD 3 mm, BoP negative, no calculus or
overhanging fillings (Fig. 19-la)
Score 1 = PPD 5 3 mm, BoP positive, but no calculus
or overhanging fillings (Fig. 19-lb)
Score 2 = PPD 3 mm, BoP positive, presence of supra
and/or subgingival calculus and/or overhanging
fillings (Fig. 19-1c)
Score 3 = PPD > 3 mm but 5 mm, BoP positive (Fig.
19-1d)
Score 4 = PPD > 5 mm (Fig. 19-le).
If an examiner identifies one single site with a PPD >
5 mm within a sextant, the sextant will receive a score
of 4, and no further assessment needs to be made in
this particular sextant. Patients with sextants scored 0,
1 or 2 belong to the relatively healthy category. A
patient that exhibits a sextant scoring 3 or 4 must
undergo a more comprehensive periodontal examina-
tion (for details see Chapter 18).
The aim of the present text is to explain the overall
objectives of the treatment planning for patients with
BPE scores of 3 and 4 and who therefore have under-
gone a comprehensive diagnostic process.
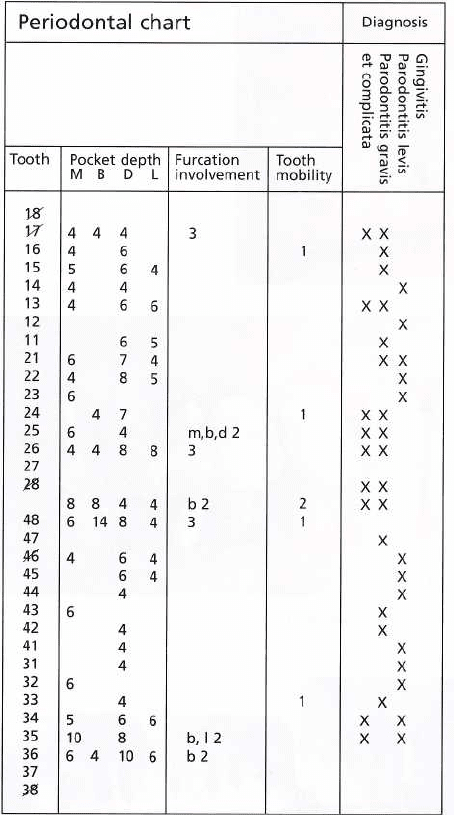
DIAGNOSIS
The basis for the treatment planning described in this
chapter is established by the clinical data collected
from the examination of the patient presented in
Chapter 18. This particular patient (U.N., male, 55
years of age) was examined with respect to his peri-
odontal conditions, i.e. gingival sites displaying signs
of bleeding on probing
were identified,
pocket depths
and
furcation involvements
were measured and graded,
tooth mobility
was assessed and the radiographs were
analyzed to determine the
height
and
outline
of the
alveolar bone crest.
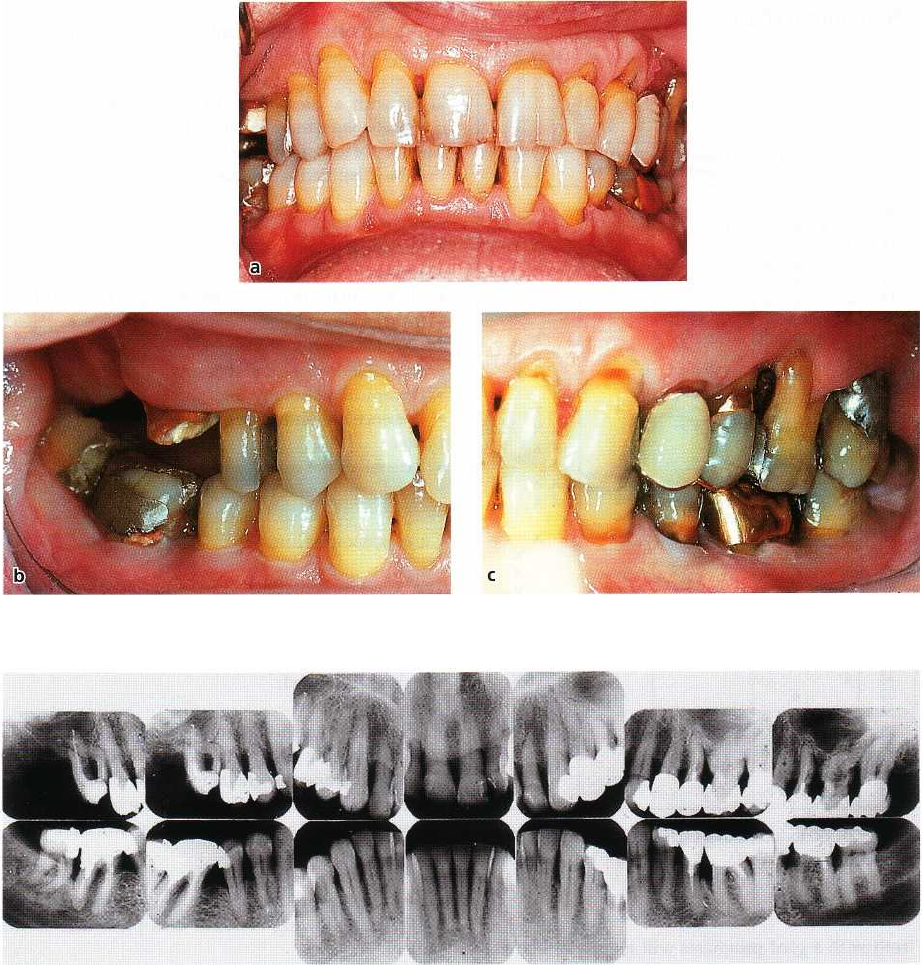
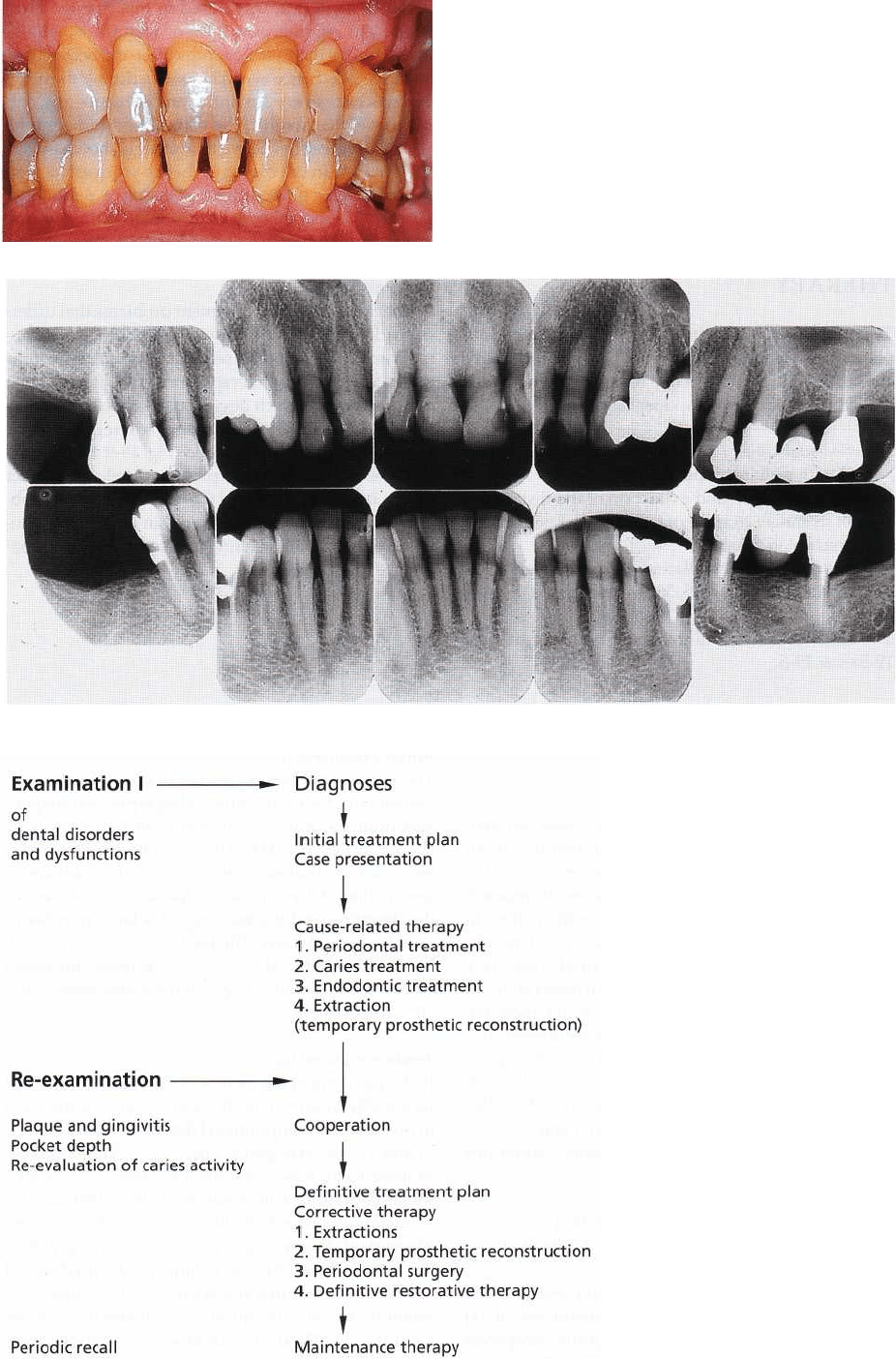
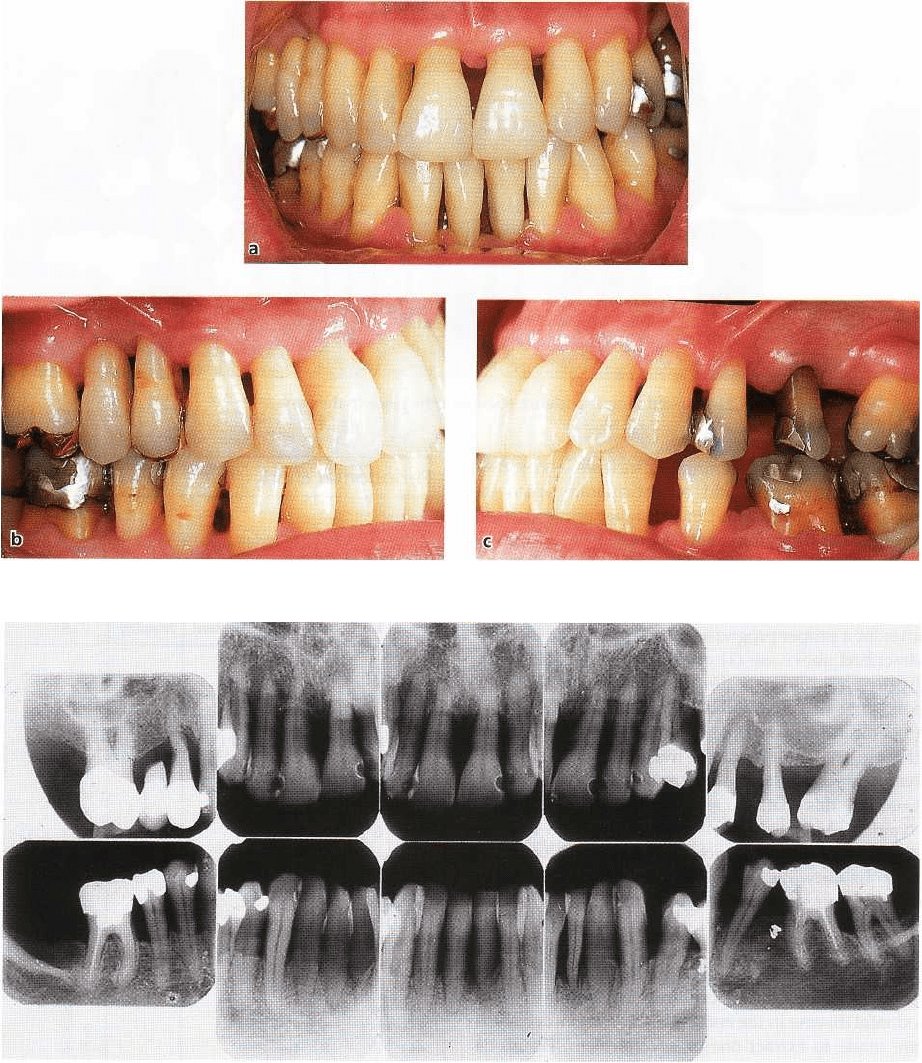
The clinical characteristics of the dentition of this
patient are shown in Fig. 19-2a-c. The periodontal
chart and the radiographs are presented in Fig. 19-
3a,b. Based on the findings, each tooth in the dentition
was given a proper periodontal diagnosis (Fig. 19-3b).
In addition to the examination of the periodontal con-
dition, detailed assessments of primary and recurrent
caries were made for all tooth surfaces in the dentition.
Furthermore, the patient was also examined with re-
spect to endodontic problems, occlusal problems,
temporomandibular joint dysfunction etc.
The present patient had secondary caries lesions
adjacent to several restorations, particularly in the
molar regions (Fig. 19-2b), and root caries in the distal
surface of 25 and mesial surface of 26 (Fig. 19-3a). It
should be observed that in a patient with a large
number of caries lesions an additional number of
examination procedures, e.g. assessments of secretion
rate and buffering capacity of the saliva, number of
lactobacilli and
Streptococcus mu tans
etc., will facilitate
the selection of proper therapeutic measures. In addi-
tion, a periapical lesion was observed in 47 and several
defective root fillings were identified (Fig. 19-3a).
TREATMENT PLANNING
Initial treatment plan
Not until a detailed diagnosis of all pathologic condi-
tions has been made, have proper prerequisites been
established for an appropriate tentative treatment
plan. At this early stage in the management of a pa-
tient, it is in most instances impossible to make defi-
nite decisions regarding all aspects of the corrective
therapy, because:
1. The degree of success of the initial treatment remains
unknown:
the result of the initial cause-related treat
-
ment of an individual case forms the basis for the
selection of means for additional therapy. The de-
gree of disease elimination that can be reached
depends on the outcome of subgingival scaling and
root planing, but also on the patient's ability to
adopt adequate dietary habits and to exercise
proper plaque control techniques.
2. The patient's "subjective" need for treatment is not
known:
when the dentist has completed the exami-
nation of the patient and an inventory has been
made regarding, for example, periodontal disease,
caries, pulpal disease and temporomandibular
joint disease, the observations are presented — "the
case presentation" — for the patient. During the case
presentation session it is important to find out if the
patient's subjective need for dental therapy coin-
TREATMENT PLANNING • 4
1
7
Fig. 19-2a-c. Clinical status of a 55-year-old male patient (U.N.) with periodontitis.
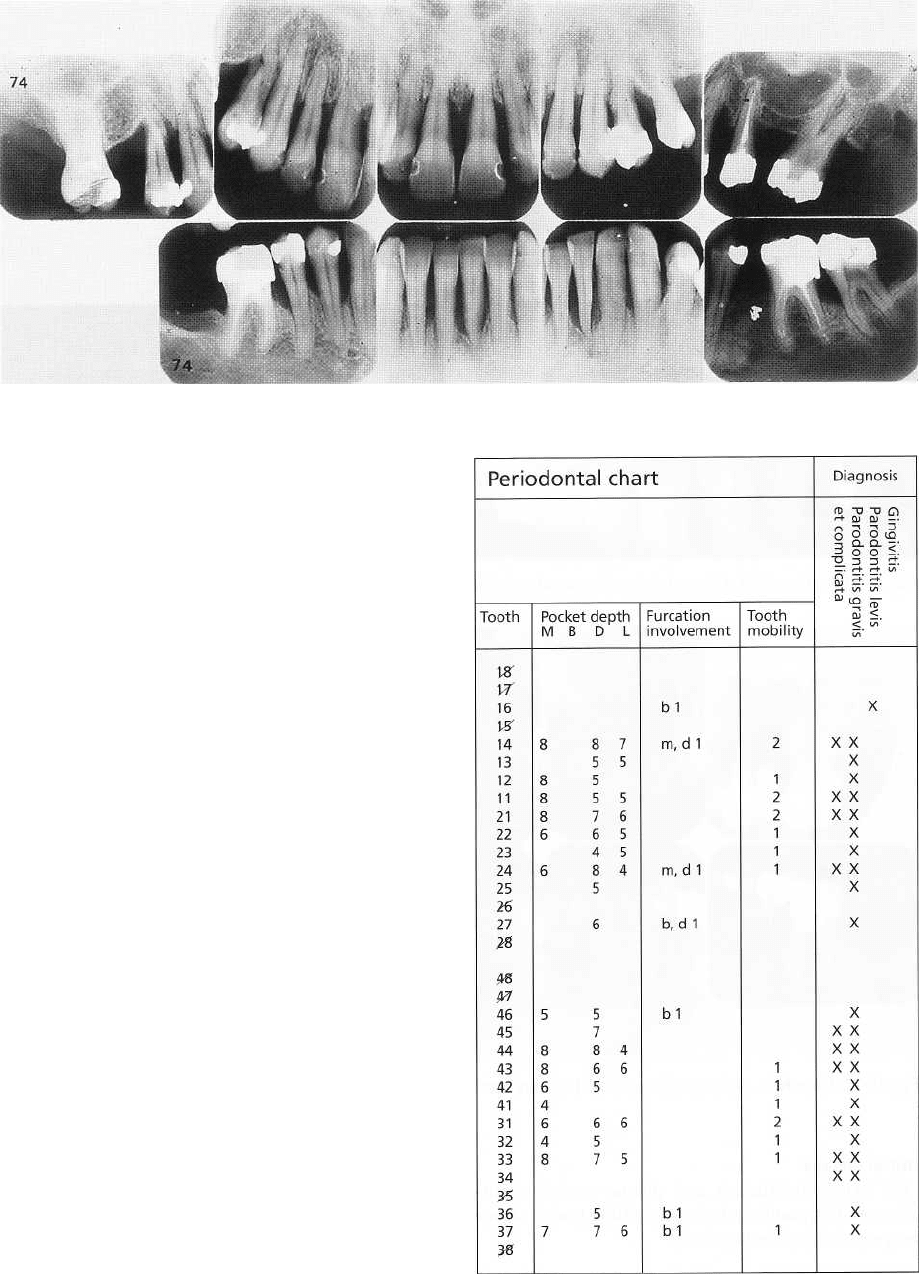
Fig. 19-3a. Radiographs relating to patient U.N. described in Fig. 19-2.
cides with the dentist's professional appreciation of
the kind and volume of therapy that is required.
It is
important that the dentist understands that the
main
objective of dental therapy, besides
elimination of
pain, is to satisfy the patient's demands regarding
esthetics and chewing function (comfort),
demands
which certainly vary considerably from one indi-
vidual to another.
3. The result of certain parts of the treatment cannot be
predicted:
in patients exhibiting advanced forms of
caries and periodontal disease it is often impossible
to anticipate if all teeth which are present at the
initial examination can be successfully treated, or
to
predict the result of certain parts of the intended
therapy. In other words, critical and difficult parts
of the treatment must be performed first, and the
outcome of this treatment must be evaluated before
all aspects of the definitive corrective treatment can
be properly anticipated and described.
Single tooth risk assessment
Based on the result of the comprehensive examination
(
including assessments of periodontitis, caries and the
endodontal status) and the resulting diagnosis, as well
as considering the patient's needs regarding esthetics
and function, a pre-therapeutic risk assessment is
made for all teeth (roots) present.
Three major questions are addressed:
1.
Which tooth/root has
a good
prognosis?
2.
Which tooth/root is
"irrational-to-treat"?
3.
Which tooth/root has
a questionable
prognosis?
418 • CHAPTER 19
Fig. 19-3b. Periodontal chart relating to patient U.N.
(Fig. 19-2).
Teeth with
a good
prognosis will require a relatively
simple therapy and may be regarded as secure abut-
ments for function.
Teeth which are considered "irrational-to-treat"
should be extracted during initial, cause-related ther-
apy. Such teeth may be identified on the basis of the
following criteria:
Periodontal
•
Recurrent periodontal abscesses
•
Periodontic-endodontic lesions
•
Attachment loss to the apex
Endodontal
•
Root perforation in the apical half of the root
•
Periapical pathology in the presence of obturating
post and core
Dental
•
Long fracture of the root
•
Oblique fracture in the middle third of the root
•
Caries lesions that extend into the root canal
Functional
•
Third molars without antagonists and with perio-
dontitis/caries
Teeth with a
questionable
prognosis are in need of
comprehensive therapy and must be brought into the
category of teeth that have a
good
prognosis. Such teeth
may be identified on the basis of the following critera:
Periodontal
•
Furcation involvement
•
Angular bone defects
•
"Horizontal" bone loss involving > two-thirds of
the root
Endodontal
•
Incomplete root canal therapy
•
Periapical pathology
•
Presence of voluminous posts/screws
Dental
•
Extensive root caries
Case presentation
The "Case presentation" is an essential component of
the initial treatment and must include a description
for the patient of different therapeutic goals. At the
case presentation for Mr. U.N. the following treatment
plan was described:
•
The teeth in the dentition from 15 to 24 and from 45
to 35 probably will not present the dentist with any
major therapeutic challenges. For the remaining
teeth in the dentition, however, the treatment may
involve several complicated or unpredictable meas-
ures.
Based on the pre-therapeutic risk assessment (Fig.
19-4), the following scenario was presented to the
patient:
•
48
and
47 extraction: cannot be treated due to the
advanced loss of supporting tissue at the buccal
aspect of the teeth in combination with deep furca-
tion involvements and periapical periodontitis as
far as 47 is concerned (Fig. 19-3).
•
16 extraction: even if it is possible, from a
therapeu
tic point of view, to preserve the palatal
root, the
maintenance of this root does not improve
esthetics
or chewing comfort; the tooth has no
antagonist
after extraction of 47 (Fig. 19-3).
• 25 and
27 extraction: 25 cannot be treated due to
advanced root caries in combination with advanced
loss of periodontal tissue support at the distal aspect
of the tooth; 27 has a periodontal pocket communi
-
cating with periapical lesions in combination with
furcation involvement of degree 3 (Fig. 19-3).
•
26, 36
and
37 present a number of therapeutic
prob
lems:
26 shows signs of deep and extended root caries
TREATMENT PLANNING • 419
16 15 14 13 12
11
21 22 23 24 25 26 27
Good prognosis
+ + + + + + + + +
Questionable prognosis
+
Irrational-to-treat
+ + +
48 47 45 44 43 42
41
31 32 33 34 35 36 37
Good prognosis
+ + + + + + + + + +
Questionable prognosis
+ +
Irrational-to-treat
+ +
Fig. 19-4. Outcome of the pre-therapeutic risk assessment made for patient U.N. described in Fig. 19-2.
in the mesiobuccal root in combination with furca-
tion involvement of degree 2 m,b,d (Figs. 19-2c &
19-3). Note the unfavorable root- and root canal
anatomy of the buccal roots; predictable endodontic
treatment? The palatal root of 26 can, however, be
maintained.
In 36 there is a deep angular bony defect at the
mesial aspect and furcation involvements of degree
2 at both the buccal and lingual surface; 37 has a
deep infrabony pocket at the distal surface (10 mm,
see the periodontal chart) and furcation involve-
ment of degree 2 b. The distal root of 36 or the mesial
root of 37 (or both) are available for treatment.
Two different
alternatives for treatment
were presented
to the patient:
• Alternative 1.
Extraction of 25 and all molars and
the
maintenance of a dentition comprising 15-24
and 45-35. This alternative may be adequate with
re
spect to "chewing comfort" but may be question-
able from an esthetic point of view.
• Alternative 2.
Extraction of the molars in the right
side of the maxilla and mandible (16, 48, 47) and also
of 25 and 27; root separation of 26 with the mainte
-
nance of the palatal root to be used as abutment for
a 3-unit bridge to replace the extracted 25; root
separation of one of the molars 36 or 37 with the
maintenance of one root to be used as abutment for
a 3-unit bridge to obtain occlusal contact with the
maxillary bridge.
It should be observed that
alternative 2
involves a
considerably larger volume of therapy than
alternative
1.
In a situation like this, expected benefits inherent in
a
certain treatment versus obvious disadvantages
should always be explained to and discussed with the
patient. His/her attitude to the alternatives presented
must guide the dentist in the design of a proper plan
for the overall treatment. In the present case the pa-
tient preferred the treatment described as
alternative 2.
INITIAL (CAUSE-RELATED)
THERAPY
The treatment was initiated and included the follow-
ing measures to eliminate or control the plaque infec-
tion:
1. Instruction
in oral hygiene measures with sub-
sequent check-ups and reinstruction.
2. Scaling and root planing
in combination with re-
moval of retention factors for plaque.
3. Excavation and restoration
of carious lesions.
4. Endodontic treatment 26
(palatal root) and 37 (mesial
root). Endodontic treatment was carried out at an
early stage to allow a proper evaluation of healing
before the restorative treatment was initiated.
5. Extraction
of 16, 48, 47. Temporary prosthetic re-
placement (for esthetic and functional reasons) of
teeth which, during this initial phase of the treat-
ment, have to be extracted should preferably be
made in the form of removable partial dentures.
The use of a removable prosthesis allows the den-
tist to eventually choose between a removable par-
tial denture and a fixed bridge as permanent pros-
thetic therapy. If, on the other hand, the temporary
prosthetic reconstruction is made in the form of a
fixed bridge, the permanent prosthetic therapy
must inevitably include fixed bridgework. Such an
alternative may, however, during the course of
treatment appear to be contraindicated. In the pre-
sent case a temporary prosthesis was not made.
RE-EVALUATION
The initial phase of therapy is terminated with a thor-
ough analysis of the results obtained with respect to
the elimination or degree of control of the dental
infections. This implies that a re-evaluation of the
patient's caries activity must be performed as well as
new assessments of gingival conditions, pocket
depths, tooth mobility, etc. The result of this re-evalu
-
ation forms the basis for the selection, if necessary, of
additional or corrective measures which are to be
performed in the phase of definitive treatment.
420 • CHAPTER
19
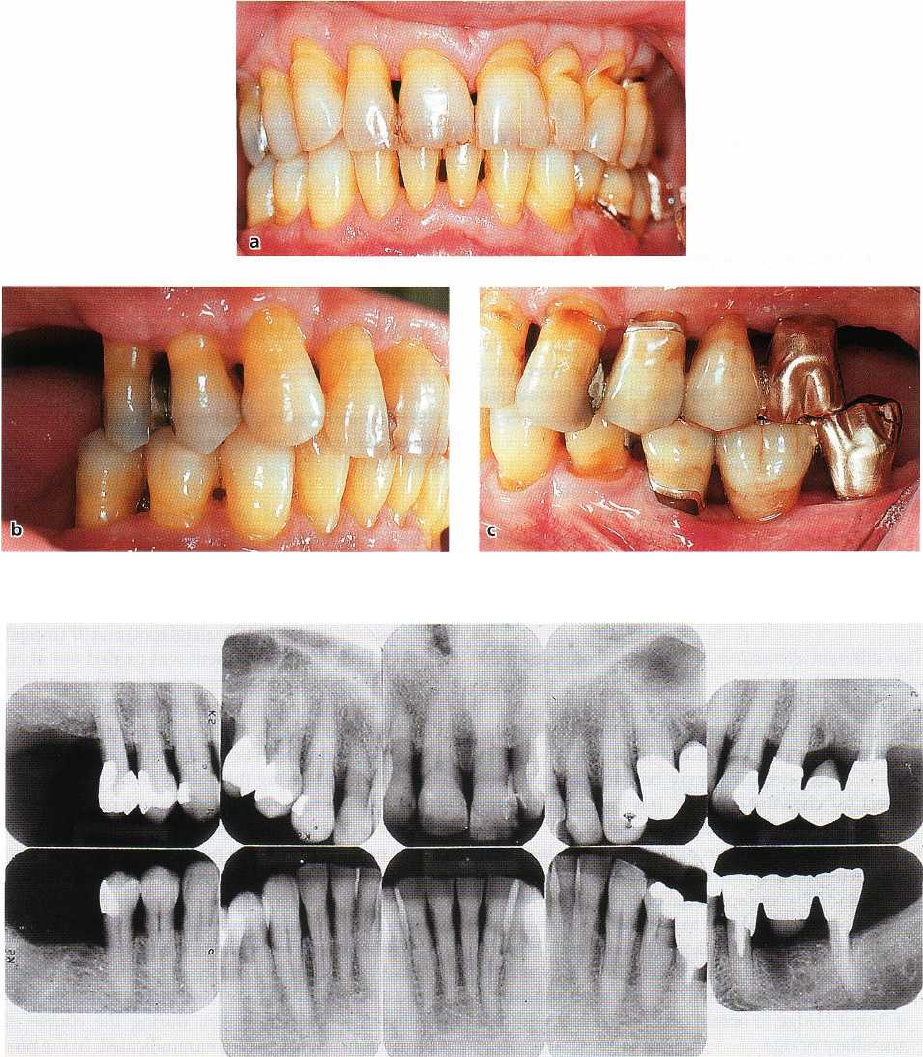
Fig. 19-5a-c. Clinical status of patient U.N. after periodontal and restorative treatment. Compare with Fig. 19-2.
Fig. 19-6. Radiographs of patient U.N. after periodontal and restorative treatment. Compare with Fig. 19-3a.
Planning of additional therapy (definitive
treatment plan)
If the results from the re-evaluation, made 1-2 months
after the termination of the initial treatment phase,
show that caries and periodontal disease have been
brought under control, the additional treatment may
be carried out in the following sequence:
1.
Extraction
of teeth that cannot be maintained. If
such extractions include teeth which must be re-
placed for esthetic or functional reasons, a tempo-
rary removable partial denture or a temporary
fixed bridge must be inserted.
2. Additional endodontic treatment
3. Periodontal surgery:
The type and extent of surgical
treatment should be based on probing depth, and
"
bleeding on probing" measurements should be
made at re-evaluation. Periodontal surgery is often
limited to those areas of the dentition where the
inflammatory lesions were not resolved by scaling
and root planing and in areas where furcation in-
volvements persist.
4. Installation of dental implants:
In regions of the den-
tition where tooth abutments are missing, implant
TREATMENT PLANNING • 421
Fig. 19-8. Radiographs of patient U.N. obtained 11 years after treatment.
Fig. 19-9. Flow chart describing
the sequence of delivery of vari-
ous treatment procedures in the
overall therapy.
422 • CHAPTER
19
therapy for esthetic and functional reasons may be
considered. It is essential to realize that implant
therapy must be initiated first when dental infec-
tions are under control, i.e. after successful peri-
odontal therapy.
5.
Definitive restorative and prosthetic treatment
including
permanent restorative therapy (crown and
bridge,
removable partial dentures, etc.).
ADDITIONAL (CORRECTIVE)
THERAPY
The present patient exhibited, after initial therapy, low
plaque and gingivitis scores (5-10%) and no active
carious lesions. The corrective treatment therefore in-
cluded the following components:
1.
Periodontal surgery
at sites which bled on probing
and with probing depths > 4 mm.
2.
Root separation
37 and extraction of the distal root.
Root separation
26 and extraction of the buccal roots.
3.
Extraction
36, 25 and 27.
4. Preparation and installation of
fixed bridges
24, 25,
26 (palatal root) and 35, 36, 37 (mesial root).
The result of the overall treatment is shown in Figs.
19-5a-c & 19-6.
SUPPORTIVE PERIODONTAL
THERAPY
Following completion of initial,
cause-related and addi-
tional therapy
the patient must be enrolled in a recall
system which aims to prevent the recurrence of dis-
ease. The time interval between the recall appoint-
ments must be related to the ability of the patient to
maintain a proper oral hygiene standard. Findings
reported from several long-term clinical trials have
suggested that a maintenance program based on recall
appointments once every 3 months is, for most pa-
tients, effective in preventing disease recurrence.
It is
important to emphasize, however, that the recall program
must be designed to meet the individual patient's need. Some
patients must be recalled every month, while other patients
may have to be checked only once a year.
At the various recall visits the following procedures
should be carried out:
1.
Evaluation of the oral hygiene standard
2.
Scaling and polishing of the teeth (if indicated).
At least once a year a comprehensive examination
should be performed including assessments of (1)
caries, (2) gingivitis, (3) pathologically deepened
pockets, (4) furcation involvements, (5) tooth mobility
and (6) alterations of the alveolar bone level.
The patient (Mr. U.N.) used in this chapter to de-
scribe the guiding principles of treatment planning
was, during the first 6 months after the active treat-
ment, recalled once every 2 months, during the next 6
months once every 3 months, and subsequently only
once every 6 months. The clinical and radiographic
status 11 years after active treatment is shown in Figs.
19-7 & 19-8. In the course of this 11-year period there
were no signs of recurrence of caries or periodontal
disease. The buccal cusp of the crown of 15 was frac-
tured approximately 5 years after active therapy and
the tooth was restored with a gold crown with a
porcelain facing.
The large variety of treatment problems that differ-
ent patients present may obviously require that devia
-
tions are made from the sequence of treatment steps
(initial cause-related therapy, corrective therapy, etc.)
discussed above. Such deviations may be accepted as
long as the fundamental principles regarding the
overall therapy are understood (Fig. 19-9: flow chart).
Three patients will be presented below together
with a brief description of their specific dental prob-
lems and the treatment delivered in order to demon-
strate the rationale behind such variations in the se-
quence of therapy.
CASE REPORTS
Patient K.A. (female, 29 years old)
Initial examination
The periodontal status (pocket depths, furcation in-
volvements, tooth mobility, radiographs and diagno-
ses) from the initial examination of patient K.A. is
shown in Fig. 19-10a,b. The data obtained from this
examination disclosed the presence of an advanced
destruction of the supporting tissues in most parts of
the dentition and the presence of a large number of
angular bony defects. The teeth 14, 12, 11, 21, 22, 23,
24, 25, 43, 42, 41, 31, 32, 33, 37 exhibited increased
mobility. The plaque and gingivitis scores were 75 and
70%, respectively.
Treatment planning
In the planning of the treatment of this case, it seemed
reasonable to anticipate the extraction of some teeth
in this severely compromised dentition, namely 14,11,
21 and 31 (see radiograph: Fig. 19-10a). The extraction
of these teeth, however, calls for extensive prosthetic
therapy. Should additional teeth be scheduled for
extraction in order to facilitate or make the outcome
of prosthetic therapy more predictable? The neighbor-
ing teeth of 11, 21, 31, also exhibited advanced loss of
supporting structures and showed signs of increased
mobility. It could be questioned, therefore, if these
teeth (i.e. 12, 22, 41, 32) could serve as proper abut-
ments for a fixed bridge. The extraction of tooth 31
would most likely enforce the additional extraction of
TREATMENT PLANNING • 4
2
3
Fig. 19-10a. Case K.A. (29-year-old female patient). Radiographs prior to therapy
the remaining three mandibular incisors, and conse-
quently a therapy could be anticipated which in-
cluded the preparation and installation of a fixed
bridge extending from tooth 44 to tooth 34. Extraction
of 11 and 21 would motivate the extraction of 12, 22,
14 and 24 as well, and call for a bridge construction
that extended from tooth 16 to 25 or 26. The prerequi
-
sites for a proper prognosis for the prosthetic therapy
described above are (1) optimal self-performed oral
hygiene, (2) proper healing of the periodontal tissues
following cause-related and corrective therapy, and (
3) a carefully monitored maintenance care program.
If
these prerequisites can be met, it may, on the other
hand, be possible to avoid all anticipated tooth extrac
-
tions in this patient and the prosthetic therapy
avoided. As stated above most of the teeth had in-
creased mobility. This mobility, however, did not dis-
turb the chewing comfort of this patient. The tooth
mobility
per se,
therefore, was not regarded as an
indication for splinting.
Conclusions:
In a case of this character extensive efforts
should be made to properly treat inflammatory peri-
odontal disease in the entire dentition
before
decisions
are made to extract one or several teeth. Decisions
regarding tooth extraction should, if possible, not be
made until after healing following periodontal sur-
gery.
Treatment
Subsequent to initial examination, the patient was
given a detailed "case presentation" and information
regarding alternative goals of and prerequisites for the
overall treatment. This information included a de-
scription of the role of dental plaque in the etiology of
periodontal disease and the significance of optimal
plaque control for a successful outcome of therapy. A
treatment program was subsequently planned which
aimed at maintaining all teeth, thereby avoiding ex-
tensive prosthetic therapy. The overall treatment was
performed in the following sequence:
Fig. 19-10b. Periodontal chart relating to case K.A. (Fig.
19-10a).
424 • CHAPTER 19
Fig. 19-11a-c. Case K.A. Clinical status 5 years after initial treatment.
Fig. 19-12. Case K.A. Radiographs obtained 8 years after treatment.
Initial
therapy
Oral hyiene instruction and plaque control evalu
ation.
Scaling and root planing. Adjustment of im
proper
amalgam restorations.
Additional therapy (following evaluation at
re-examination)
Periodontal surgery involving careful removal of sub-
gingival soft and hard deposits and root planing. All
teeth in the dentition could be maintained and the
furcation involvements in the premolar and molar
areas could be treated successfully with furcation
plasty (see Chapter 29). After healing, a fixed bridge
(
16, 15, 14) was fabricated and inserted on esthetic
indications.
Supportive therapy
During the first 6 months after completion of the initial
and corrective therapy, the patient was recalled for
maintenance care every 3 weeks. This interval be-
tween the recall appointments was then gradually
extended to 3 months.