Jan Lindhe. Clinical Periodontology
Подождите немного. Документ загружается.

TREATMENT PLANNING • 425
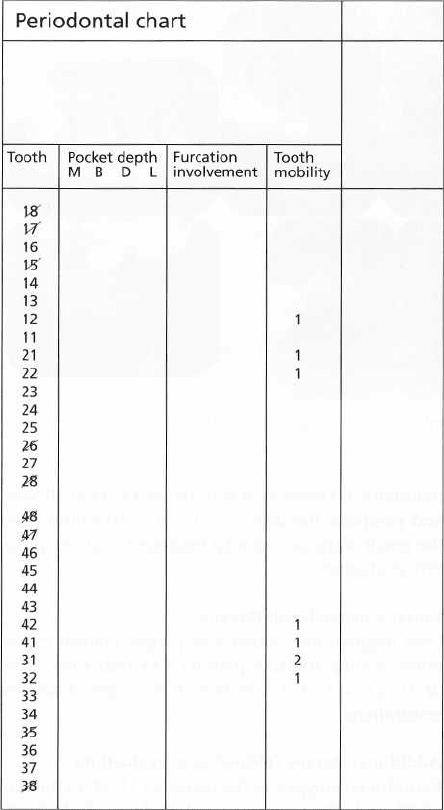
Fig. 19-13. Case K.A. Periodontal chart from recordings
made 8 years after treatment. (Fig. 19-12).
Concluding remarks
The result of the treatment is shown in Fig. 19-11a-c
(clinical status 5 years after initial treatment), Fig.
19-12 (radiographs 8 years after treatment) and Fig.
19-13 (periodontal chart 8 years after treatment).
There was no recurrence of destructive periodontal
disease during the period of maintenance.
The planning of the overall treatment and the se-
quence of the different treatment procedures used in
this case were selected for presentation in order to
illustrate the following principle:
In patients exhibiting
a
generalized advanced breakdown of the periodontal tissues,
but with an intact number of teeth, considerable efforts should
be made to maintain all teeth.
Extraction of one
single
tooth in such a dentition will frequently also call
for the
extraction of several others for "prosthetic
reasons".
The end result of such an approach thus
includes an
extensive, prosthetic rehabilitation which,
if the
treatment planning had been properly done,
would
have been entirely unneccessary.
Patient B.H. (female, 40 years old)
Initial examination
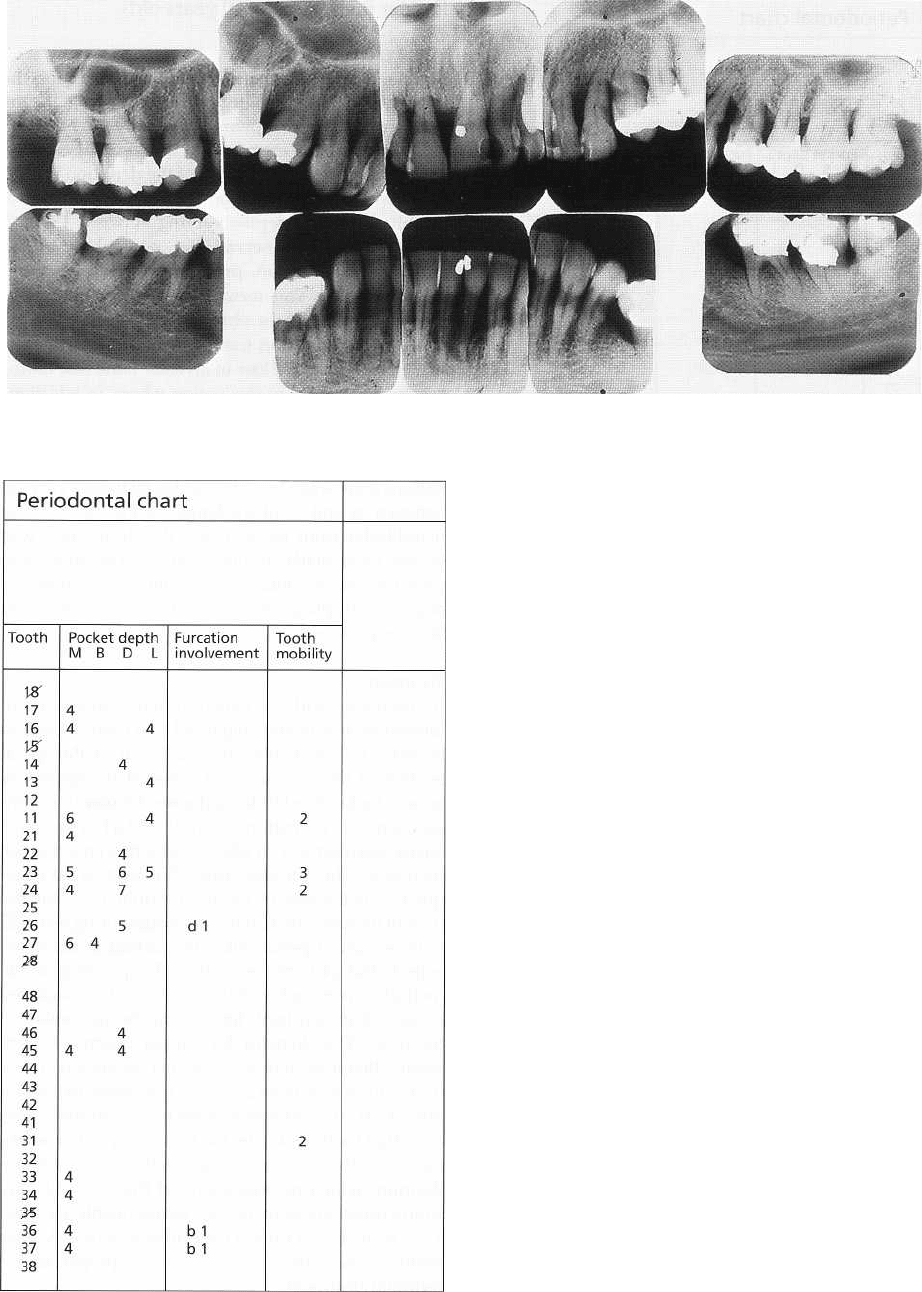
The periodontal status (pocket depths, furcation in-
volvements, tooth mobility, radiographs) from the in-
itial examination is shown in Fig. 19-14a,b. The data
obtained from this examination disclosed essentially
shallow pockets in most parts of the dentition except
for isolated areas (the region 11-24) where some sites
exhibited probing depths varying between 4 and 7
mm. It should be observed that, particularly in the
maxillary front region, pronounced gingival reces-
sions prevailed. This means that even the moderate
probing depth values obtained reflected advanced
loss of the supporting tissues. This was further con-
firmed by the severe loss of alveolar bone (see radio-
graphs: Fig. 19-14) in this region where, in addition,
some of the teeth exhibited increased mobility (tooth
11: degree 2 in combination with elongation; tooth 23:
degree 3 and tooth 24: degree 2). In the posterior tooth
regions there was a loss of periodontal tissues varying
between
1
/3
and
1
/2
of the length of the roots. In the
mandibular front tooth region the destruction was
severe, particularly around tooth 31. This tooth was
found to be non-vital and exhibited a mobility of
degree 2. The plaque and gingivitis scores were 25 and
30%, respectively.
Treatment
In discussing with the patient different treatment al-
ternatives, it was first suggested that tooth 23 was to
be extracted. Not more than 2-3 mm of the apical
portion of the root was still invested in supporting
bone. The tooth exhibited a degree 3 mobility in con-
junction with premature occlusal contact in the inter-
cuspal position and on laterotrusive movement of the
mandible. The question arose, however, what cons-
quences extraction of tooth 23 would have for the
overall therapy. For instance: the neighboring teeth (22
with advanced periodontal destruction at the distal
aspect, and 24 with severe loss of supporting tissue
including increased mobility) could not be considered
proper abutment teeth for a 3-unit bridge replacing
tooth 23. The demand for proper abutment teeth
would therefore require a further extension of the
bridge to include teeth 21 and 25 (following extraction
also of 24). This extension of the bridge implies, how-
ever, that tooth 11 will be the first nonsplinted neigh-
boring tooth. Considering the small amount of perio-
dontium which persisted around this tooth, it may
from a prosthetic point of view be reasonable to extract
11 as well, and to extend the bridge to tooth 13, since
tooth 12 may also be considered improper as the
terminal abutment.
From this discussion, it is apparent that extraction
of one single tooth (23) in this dentition will lead to
extraction of a number of additional teeth to exclude
their incorporation in the permanent reconstruction.
The result is, thus, an extensive bridge therapy which
can be avoided if only the critical tooth (23) can be
426 • CHAPTER 19
Fig. 19-14a. Case B.H. (40-year-old female patient). Radiographs from the initial examination.
Fig. 19-14b. Periodontal chart relating to case B.H. (Fig.
19-14a).
maintained. Therefore it was decided to treat all teeth
and postpone the decision of tooth extractions until
the result of the periodontal treatment could be prop-
erly evaluated.
Initial (cause-related) therapy
Oral hygiene instruction and plaque control evalu-
ation. Scaling and root planing. Occlusal adjustment
of 11, 23 and 24. Correction of improper amalgam
restorations.
Additional therapy (following re-evaluation)
Periodontal surgery in the region of 11-24. Extraction
of 28 and 48 (semi-impacted molars). Endodontic
treatment of 31.
Six months following this part of the corrective
treatment, a new evaluation disclosed that no pathol-
ogically deepened pockets were present and that the
mobility had decreased in all initially hypermobile
teeth (11: from degree 2 to 1; 23: from degree 3 to 2; 24:
from degree 2 to 0; 31 from degree 2 to 1). All teeth
could, thus, be maintained and there were no indica-
tions for additional tooth extractions. The treatment
was completed with a crown restoration in tooth 25.
Supportive therapy
During the first year after completion of the corrective
therapy, the patient was enrolled in a maintenance
care program with recall appointments once every 3
months and thereafter once every 6 months.
The result of the treatment (12 years after) is shown
in Fig. 19-15a-c (clinical status) and Fig. 19-16 (radio-
graphs). No further loss of supporting tissues had
occurred during this observation period.
TREATMENT PLANNING • 4
2
7
Fig. 19-15a-c. Case B.H. Clinical status 12 years after treatment.
Fig. 19-16. Case B.H. Radiographs obtained 12 years after active therapy. Note that no loss of alveolar bone has
occurred during the 12 years of maintenance. Compare with Fig. 19-14.
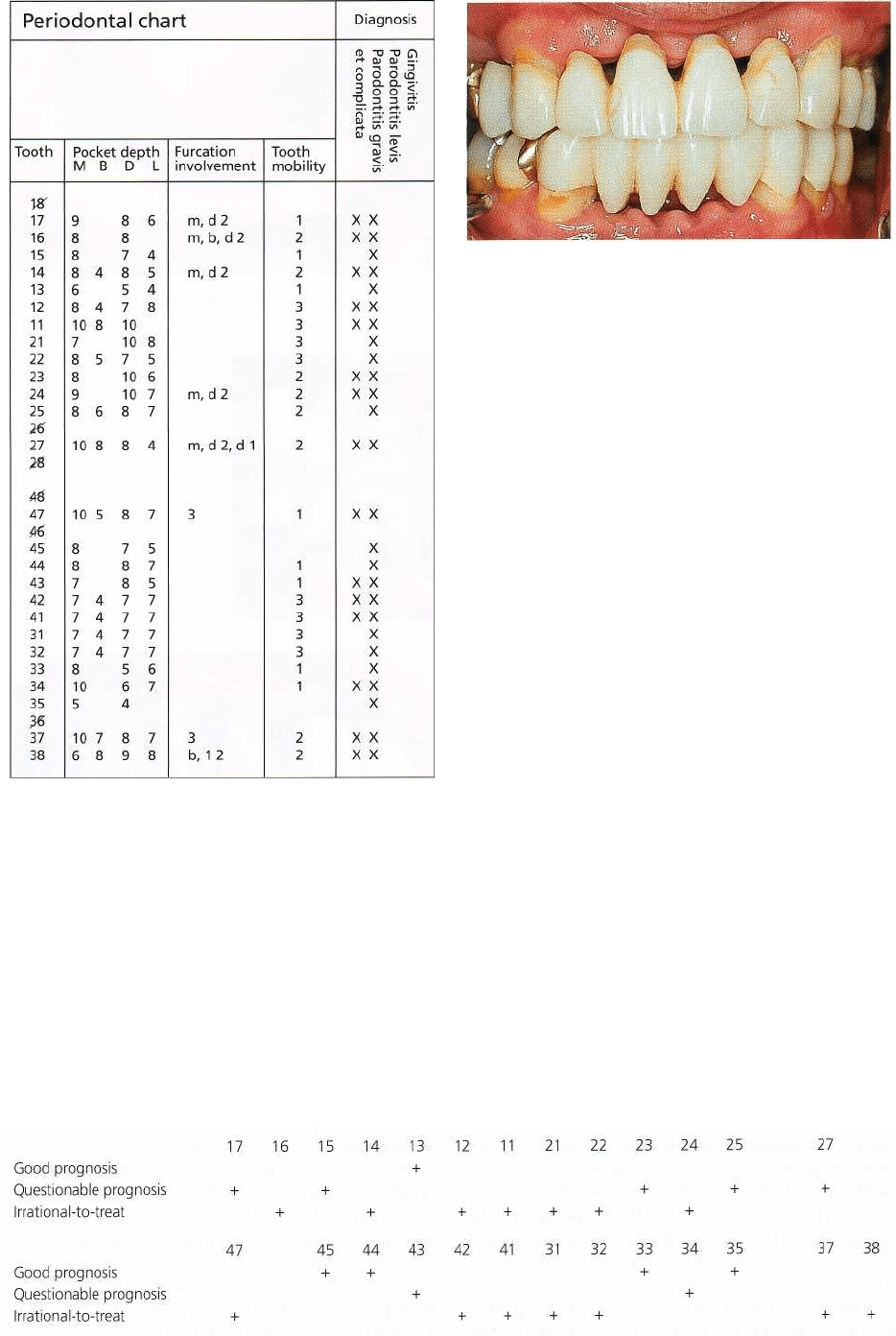
Patient P.O.S. (male, 30 years old)
Initial examination
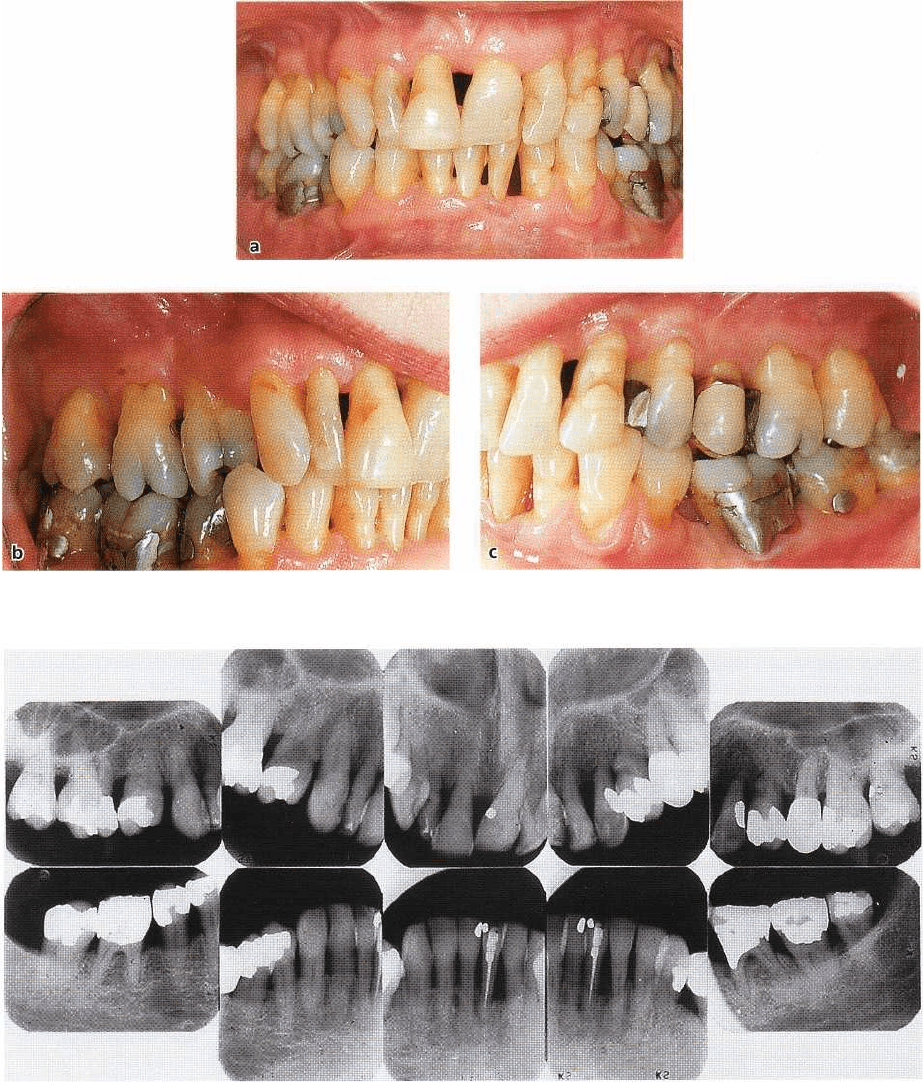
The clinical status of this patient is illustrated in Fig.
19-17a-c and the periodontal status (pocket depths,
furcation involvements, tooth mobility, radiographs
and diagnoses) from the initial examination in Fig.
19-
18. The dentition was characterized by severe de-
struction of the supporting apparatus, including ad-
vanced loss of the interradicular periodontal tissues
in
all molars and the two first maxillary premolars.
Most teeth were markedly mobile, particularly the
incisors in both jaws. The plaque and gingivitis scores
were close to 100%.
Treatment planning
A thorough analysis of the periodontal conditions in
this patient revealed that certain teeth could no longer
be treated and maintained but had to be extracted.
Hence, it was decided to extract teeth 14 and 24 (fur-
cation involvement of degree 2 from both mesial and
distal aspects) and 12, 11, 21, 22 (loss of the supporting
428 • CHAPTER 19
Fig. 19-17a-c. Case P.O.S. (30-year-old male patient). Clinical status prior to surgery.
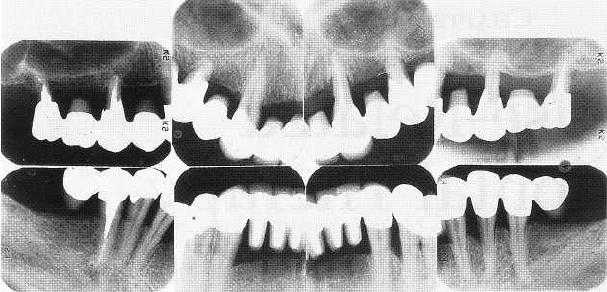
Fig. 19-18a. Case P.O.S. Radiographs from the initial examination.
tissues to a level close to or beyond the apices in
combination with a mobility of degree 3). In the man-
dible, 42, 41, 31, 32 and 37 could not be maintained.
The overall treatment of this patient, therefore, had to
include prosthetic replacement of a number of teeth.
Alternative 1
Mandible:
In the planning phase, it was anticipated
that the prosthetic rehabilitation of the mandibular
dentition should not involve any technical difficulties
since 33 and 43 as well as 34, 35 and 44, 45 were
available for periodontal therapy and, hence, could be
used as abutment teeth for a cross-arch fixed bridge. It
did not seem reasonable to maintain the furcation-
involved 47 and 38. Hence these teeth were scheduled
for extraction. In this context it should be understood
that if 47 and 38 were to be maintained, the treatment
would have included not only endodontic measures
but also root separation and periodontal surgery, pro-
duction of posts and cores, and the incorporation of
the preserved roots as abutments in the cross-arch
bridge construction.
TREATMENT PLANNING • 429
Fig. 19-18b. Periodontal chart relating to case P.O.S.
(Fig. 19-18a).
Maxilla:
The maxillary dentition presented more diffi-
cult therapeutic problems. If the patient was to be
restored with a fixed bridge, it was considered perti-
nent to maintain the two maxillary canines (teeth 13
and 23) and at least one tooth in the premolar (molar)
regions on both sides of the jaw (15 and 25) and one
or more roots of 17,16 and 27.
Definitive
prosthetic
treatment of the maxillary dentition by means of a
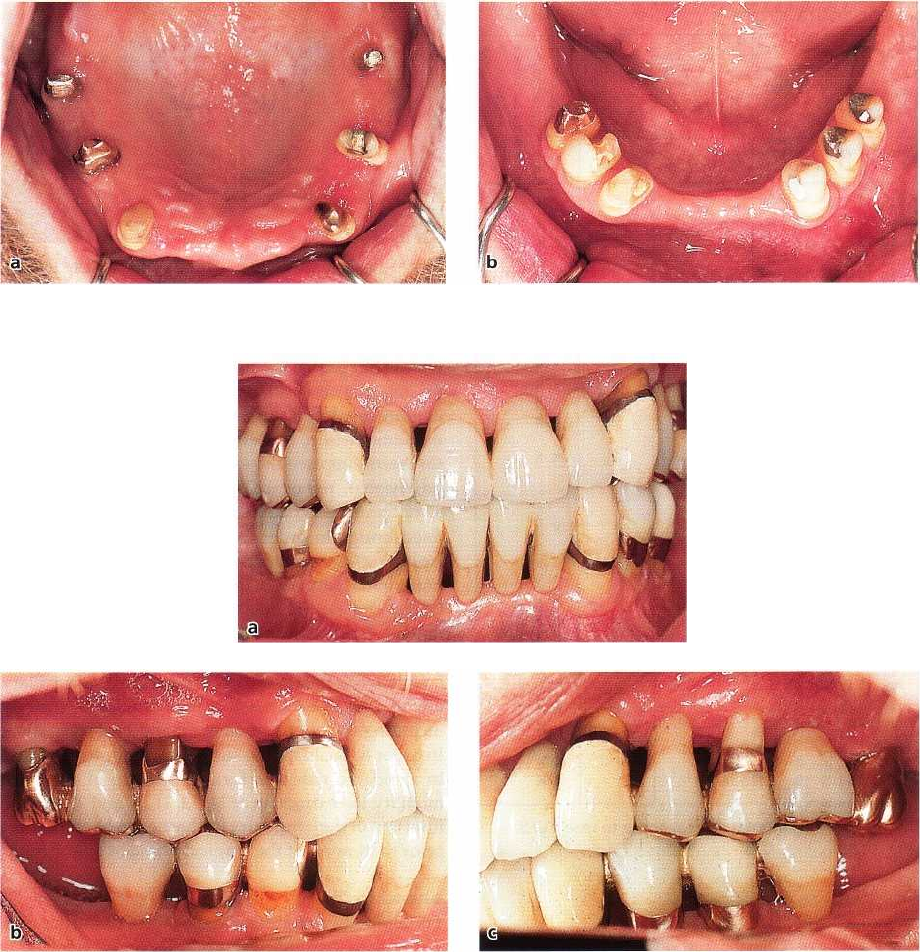
Fig. 19-19. Case P.O.S. Clinical status of the front tooth
region at completion of the initial, cause-related treat
ment.
removable, partial denture was not considered appro
-
priate since the various abutment teeth for such a
denture displayed a markedly increased mobility. For
the same reason, it was considered inappropriate to
temporarily
replace the extracted teeth by means of a
provisional, removable partial denture. The provi-
sional prosthesis had to be fabricated in the form of a
fixed bridge in order to enable proper stabilization
(
splinting) of the hypermobile 13, 23 and 25 prior to
periodontal surgery. In the present case the temporary
bridge did not include tooth 15 and the maxillary
molars. Tooth 15 was to be left uncovered in order to
facilitate endodontic therapy and the preparation and
insertion of a post and core. In addition, the maxillary
molars had to be accessible for periodontal therapy
including endodontic treatment and root separation.
In order to facilitate the surgical procedures and also
to avoid the risk of a further increase of the tooth
mobility, the extraction of 14, 21 and 22 and the
insertion of the temporary bridge had to be carried out
prior to the start of the surgical phase of treatment.
Alternative 2
The alternative treatment to the
one
outlined above is
a
complete denture in the maxilla and a removable
partial denture in the mandible with the use of 45, 44,
43 and 33, 34, 35 as abutment teeth.
Treatment
The clinical and radiographical symptoms of the ad-
vanced disease as well as the therapeutic alternatives
were thoroughly discussed with the patient. This dis-
Fig. 19-18c. Pre-therapeutic risk assessment made for patient P.O.S. described in Figs. 19-17 and 19-19a,b.
430 • CHAPTER
19
Fig. 19-20a-b. Case P.O.S. The abutment teeth used for a maxillary (a) and a mandibular (b) bridge.
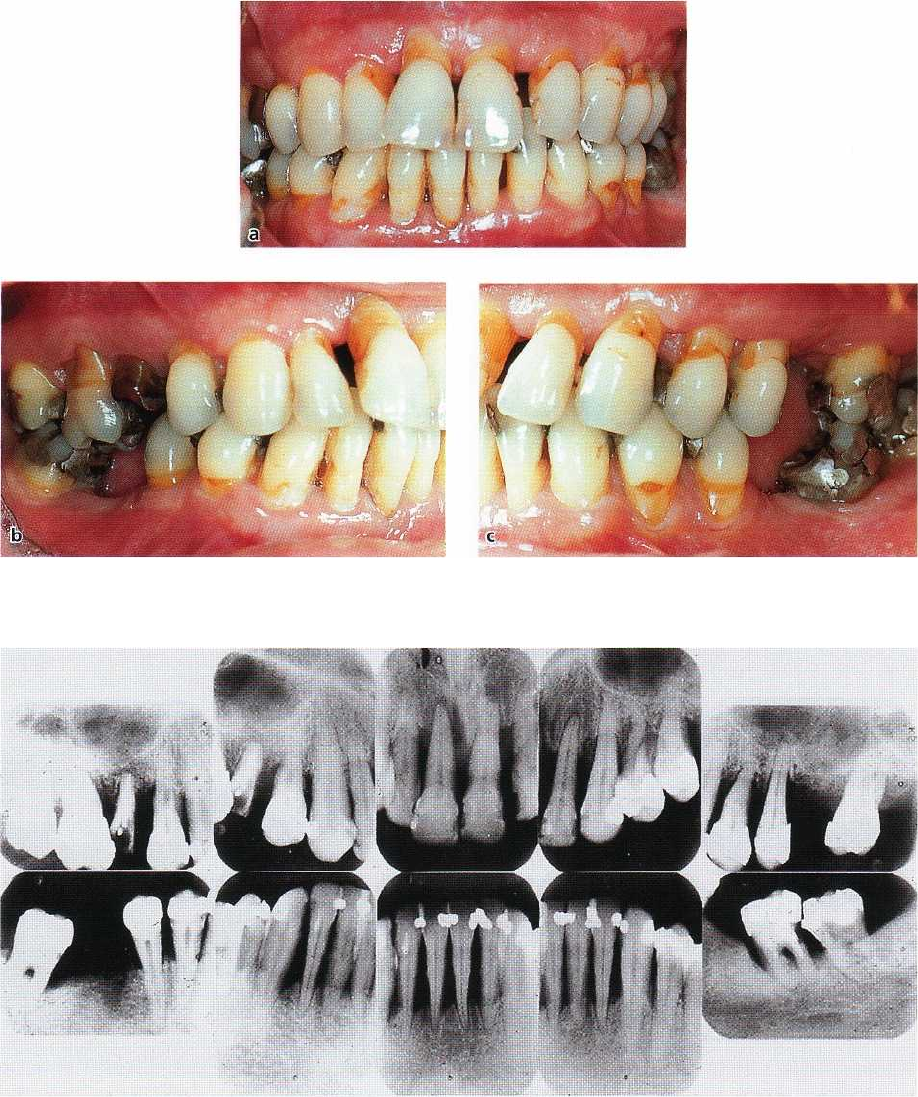
Fig. 19-21a-c. Case P.O.S. Clinical photographs illustrating the result of treatment after 8 years of maintenance.
cussion included a detailed explanation of the role of
optimal plaque control for the long-term good prog-
nosis. The treatment was performed according to
al-
ternative 1
and in the following sequence:
Initial (cause-related) therapy
Instruction regarding oral hygiene measures. Scaling
and root planing. Evaluation of the ability of the pa-
tient to maintain a high standard of oral hygiene.
Extraction of 14, 12, 11, 21, 22. Temporary acrylic
bridge 14, 13, 12, 11, 21, 22, 23, 24, 25; (24 was tempo
-
rarily maintained in order to ensure proper stability
of
the temporary bridge).
Extraction of 47, 42, 41, 31, 32, 37, 38. Temporary
acrylic bridge 44, 43, 42, 41, 31, 32, 33, 34, 35; (45:
because the tooth was non-vital it was not incorpo
rated in the temporary bridge to facilitate endodontic
treatment). Endodontic treatment 15, 45. The clinical
status at the completion of the initial treatment is seen
in Fig. 14-19.
Additional therapy
Periodontal surgery around the teeth which at the
re-
evaluation after initial therapy still exhibited pathol-
ogically deepened pockets which bled on probing. The
palatal roots of 17 and 27 were maintained and the
buccal roots were extracted following separation.
Extraction of 16 and 24. Following healing after
surgery, posts and cores were inserted in 17, 15, 27 and
45 (Fig. 19-20a,b) and permanent fixed bridges were
designed and fabricated with the following outline:
TREATMENT PLANNING • 431
Fig. 19-22. Case P.O.S. Radio-
graphs obtained 8 years after com-
pletion of active therapy. Note
that
no further loss of alveolar
bone has
occurred during the 8
years of
maintenance.
Maxilla:
17 (palatal root), 16, 15, 14, 13, 12, 11, 21, 22,
23, 24, 25, 26, 27 (palatal root).
Mandible:
46, 45, 44, 43, 42, 41, 31, 32, 33, 34, 35, 36.
Supportive therapy
After completion of active treatment this patient was
enrolled in a maintenance care program including
recall
appointments once every 3 months. Clinical
photographs (Fig. 19-21a-c) and radiographs (Fig. 19-
22) illustrate the result of the treatment at the 8-year
control. No further loss of supporting tissues occurred
during the maintenance period.
REFERENCES
Lindhe, J. & Nyman, S. (1975). The effect of plaque control and
surgical pocket elimination on the establishment and mainte-
nance of periodontal health. A longitudinal study of peri-
odontal therapy in cases of advanced disease.
Journal of Clini-
cal Periodontology 2,
67-79.
Nyman, S. & Lindhe, J. (1979). A longitudinal study of combined
periodontal and prosthetic treatment of patients with ad-
vanced periodontal disease.
Journal of Periodontology
50, 163-
169.
Nyman, S., Lindhe, J. It Rosling, B. (1977). Periodontal surgery
in
plaque-infected dentitions.
Journal of Clinical Periodontology
4,
240-249.
Nyman, S., Rosling, B. & Lindhe, J. (1975). Effect of professional
tooth cleaning on healing after periodontal surgery.
Journal of
Clinical Periodontology 2,
80-86.
Rosling, B., Nyman, S. & Lindhe, J. (1976a). The effect of system-
atic plaque control on bone regeneration in infrabony pock
ets.
Journal of Clinical Periodontology 3,
38-53.
Rosling, B., Nyman, S., Lindhe, J. & Jern, B. (1976b). The healing
potential of the periodontal tissues following different tech-
niques of periodontal surgery in plaque-free dentitions. A
2-
year clinical study.
Journal of Clinical Periodontology 3,
233-
250.
CHAPTER 20
Cause-Related
Periodontal Therapy
HARALD RYLANDER AND JAN LINDHE
Objectives of initial, cause-related
periodontal therapy
Means of initial, cause-related periodontal
therapy
Scaling and root planing
Removal of plaque-retention factors
Healing after initial, cause-related therapy
Clinical measurements
Structural measurements
Evaluation of the effect of the initial,
cause-related therapy
The overall treatment of patients with caries and peri
-
odontal disease, including associated pathologic con-
ditions (e.g. pulpal and periapical lesions, tooth mi-
gration, tooth loss) can he divided into three different
but frequently overlapping phases (see Chapter 19):
The phase of initial, cause-related therapy is
aimed at
bringing caries and gingivitis under control and at
arresting the further progression of periodontal tissue
destruction.
The phase of additional therapy is
aimed at restoring
function and esthetics.
The phase
u
f supportive therapy is
aimed at preventing
recurrence of caries and periodontal disease.
OBJECTIVES OF INITIAL, CAUSE-
RELATED PERIODONTAL THERAPY
The measures used in initial, cause-related periodon-
tal therapy aim at the elimination — and the prevention
of their recurrence — of supra and subgingivally lo-
cated bacterial deposits from the tooth surfaces. This
is accomplished by:
•
motivating the patient to understand and combat
dental disease
(patient information)
•
giving the patient
instruction
on how to properly
clean his/her teeth
(self-performed plaque control
methods),
see Chapter 21
•
scaling and root planing
•
removal of additional
retention factors
for plaque such
as overhanging margins of restorations, ill-fitting
crowns, etc.
MEANS OF INITIAL, CAUSE-
RELATED PERIODONTAL
THERAPY
Scaling and root planing
Definitions
Scaling is
a procedure which aims at the removal of
plaque and calculus from the tooth surface. Depend-
ing on the location of the deposits, scaling is per-
formed by supragingival and/or subgingival instru-
mentation.
Root planing
denotes a technique of instru
-
mentation by which the "softened" cementum is re-
moved and the root surface is made "hard" and
"
smooth". Subgingival scaling and root planing can
be
performed as either
closed
or
open
procedures and
often under local anesthesia. The
closed
procedure
implies subgingival instrumentation without inten-
tional displacement of the gingiva. The root surface is,
thus, not accessible for direct visual inspection. The
open
procedure calls for exposure of the affected root
surface by measures which displace the gingival tis-
sue. The gingiva is thus incised and reflected or re-
sected to facilitate access and visibility in the field of
operation.

CAUSE-RELATED PERIODONTAL THERAPY • 433
Fig. 20-1. A double-ended hand
instrument with col-grip. The
cutting edges of the blades are
centered over the long axis of the
handle.
Instruments and instrumentation
Instruments used for scaling and root planing are
classified as:
1.
Hand instruments
2.
Ultrasonic and sonic instruments
3.
Rotating instruments
4.
Reciprocating instruments
5. Laser instruments
Hand instruments
A hand instrument is composed of three parts: The
working part
(the blade), the
shank
and the
handle.
The
cutting edges of the blade are centered over the long
axis of the handle in order to give the instrument
proper balance (Fig. 20-1). The blade is often made of
carbon steel, stainless steel
or
tungsten carbide.
Curettes
(Fig. 20-2): Curettes are instruments used for
both scaling and root planing. The working part of the
curette is the spoon-shaped blade which has two
curved cutting edges. The two edges are united by the
rounded toe. The curettes are usually made "double-
ended" with mirror-turned blades. The length and
angulation of the shank as well as the dimensions of
the blade differ between different brands of the instru
-
ment (Fig. 20-3).
Sickles
(Fig. 20-4): The sickle is manufactured with
either a curved or a straight blade which has a trian-
gular cross section and two cutting edges. The "facial"
surface between the two cutting edges is flat in lateral
direction but may be curved in the direction of its long
axis. The "facial" surface converges with the two lat-
eral surfaces of the blade. The sickles are mainly used
for supragingival debridement or scaling in shallow
pockets.
Hoes
(Fig. 20-5): The hoe has only one cutting edge.
The blade is turned at a 100° angle to the shank with
the cutting edge beveled at a 45° angle. The blade can
he positioned at four different inclinations in relation
to the shank: facial, lingual, distal and mesial. The hoe
is mainly used for supragingival scaling but is an
excellent instrument to use for root planing during
periodontal surgery.
Instrumentation
Supragingival scaling:
The debridement of the denti-
tion of a patient with periodontal disease often starts
with supragingival scaling. Supragingival calculus
and gross overhangs of restorations are removed (Fig.
20-6). This initial phase of the debridement can be
performed with the use of hand instruments or ultra-
sonic instruments (see below). When hand instrumen
-
tation is preferred for the initial debridement, a curette
or a sickle is often used to simply split off calculus
from its attachment to the enamel and/or the exposed
part of the root. Following hand instrumentation the
clinical crowns should be polished using rubber cups
and first pumice and subsequently more fine-grained
(
grainsize of 2-4tm) polishing pastes. In many cases
the
supragingival scaling effort can be completed in one
session. This will allow the patient, without further
delay, to implement the new and "improved" self-per-
formed plaque control program.
Fig. 20-2. Schematic illustration of the design of the
blade of a curette.
434 • CHAPTER 20
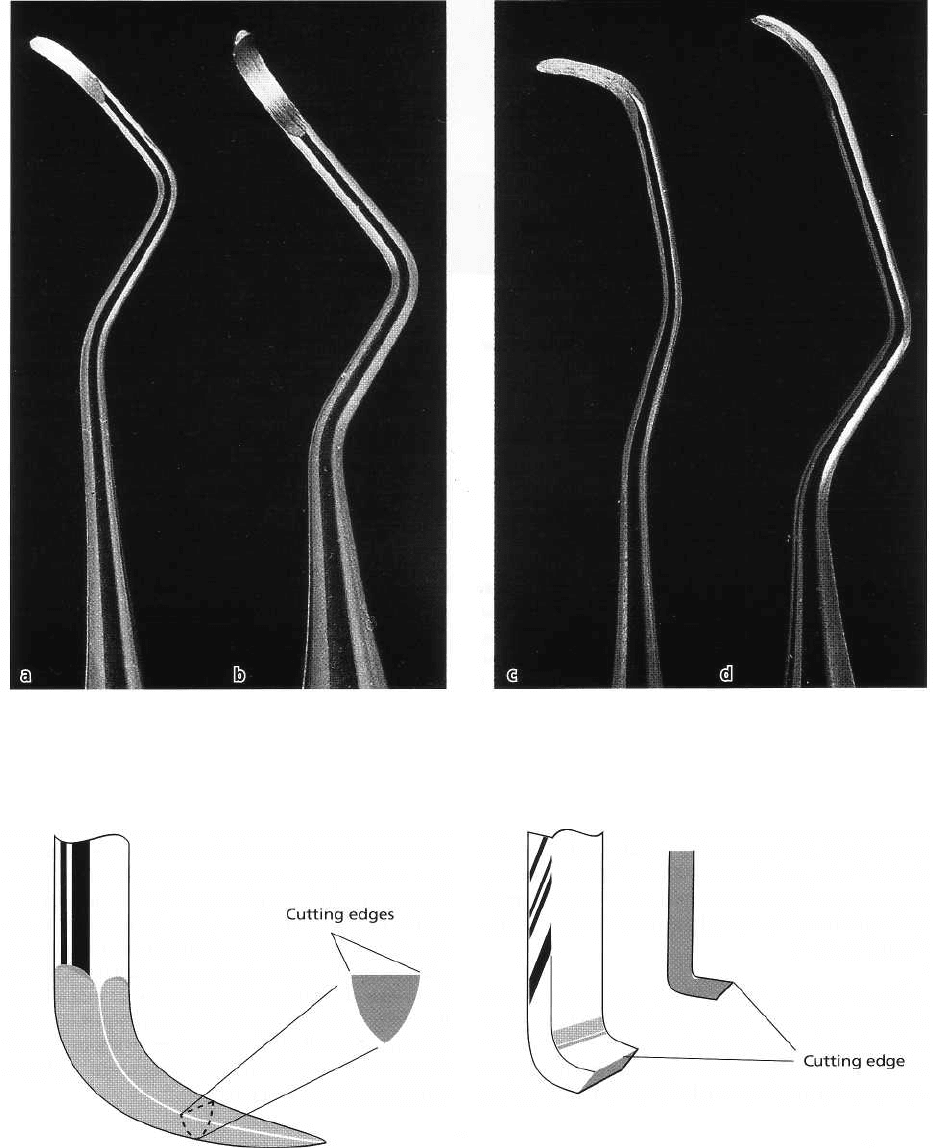
Fig. 20-3. Curettes with different lengths and angulations of the shank. (a) and (b) are curettes used for supragingi
-
val and (c) and (d) curettes for subgingival instrumentation. Increased angulation of the shank (b and d) of the cu
-
rettes permits proper instrumentation in posterior tooth regions.
Fig. 20-4. Schematic illustration of the cross section of
the blade of a sickle. Note the positions of the cutting
edges.
Subgingival scaling and root planning:
Performed with
hand instruments, these treatment procedures aim at
removing not only soft and hard deposits from the
root
surface but also small amounts of tooth sub-
stance.
Root cementum and also root dentine are re-
moved in
the shape of small chips which carry the
Fig. 20-5. The cross section of a hoe. Note the position
of the cutting edge.
deposits and which during the cutting operation are
curled up at the front side (in the cutting direction) of
the blade of the instrument. This method of instru-
mentation is denoted "orthogonal cutting", which im-
plies the removal of tooth substance by means of an
edge which to a varying extent penetrates the hard
substance of the root. The result of the cutting opera-