Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

a-amylase or amyloglucosidase to some samples and
incubating them at 28–30
C for 48 h, it can be seen
whether any treatment clears the sample. If it works,
the problem is identified and an easy solution has
been found.
Use of Transglutaminase in Functional
Properties of Food
0075Transglutaminase (EC 2.3.2.13) catalyzes in vitro
cross-linking in whey proteins, soya proteins, wheat
proteins, beef myosin, casein and crude actomyosin
refined from mechanically deboned poultry meat. In
recent years, on the basis of the enzyme’s reaction to
gelatinize various food proteins through the forma-
tion of cross-links, this enzyme has been used in at-
tempts to improve the functional properties of food.
The modification of food proteins by transglutami-
nase may lead to textured products, help to protect
lysine in food proteins from various chemical reac-
tions, encapsulate lipids and/or lipid-soluble mater-
ials, form heat- and water-resistant films, avoid heat
treatment for gelation, improve elasticity and water-
holding capacity, modify solubility and functional
properties, and produce food proteins of higher
nutritional value through cross-linking of different
proteins containing complementary limiting essential
amino acids.
0076An overview of the application possibilities for
microbial transglutaminase in food processing is
given in Table 9. In meat and fish processing it is of
great interest to maximize the yield of marketable
products, particularly by restructuring low-value
cuts and trimmings to improve their appearance,
flavor, and texture. In vegetables and fruit transglu-
taminase is used to maintain freshness, by coating
them with a membrane containing transglutaminase
and proteins. Literature reports also cite a method
developed for reducing the allergenicity of some
food proteins and/or peptides: a
s1
-casein was treated
tbl0009 Table 9 Overview of application of microbial transglutaminase in food processing
Source Product Effect
Meat Hamburger, meatballs, stuffed dumplings Improved elasticity, texture, taste, and flavor
Canned meat Good texture and appearance
Frozen meat Improved texture and reduced cost
Molded meat Restructuring of meat
Fish Fish paste Improved texture and appearance
Krill Krill paste Improved texture
Collagens Shark-fin imitation Imitation of delicious food
Wheat Baked foods Improved texture and high volume
Soya bean Mapuo doufu Improved shelf-life
Fried tofu (aburaage) Improved texture
Tofu Improved shelf-life
Vegetables and fruits Celery Food preservation
Casein Mineral absorption promoters Improved mineral absorption in intestine
Gelatin Sweet foods Low-calorie foods with good texture, firmness, and elasticity
Fat, oil, and proteins Solid fats Pork-fat substitute with good taste, texture, and flavor
Plant proteins Protein powders Gel formation with good texture and taste
Seasonings Seasonings Improve taste and flavor
Partially reproduced from Zhu Y, Rinzern A, Tramper J and Bol J (1995) Microbial transglutaminase – a review of its production and application in food
processing. Applied Microbiology and Biotechnology 44: 277–282 with permission.
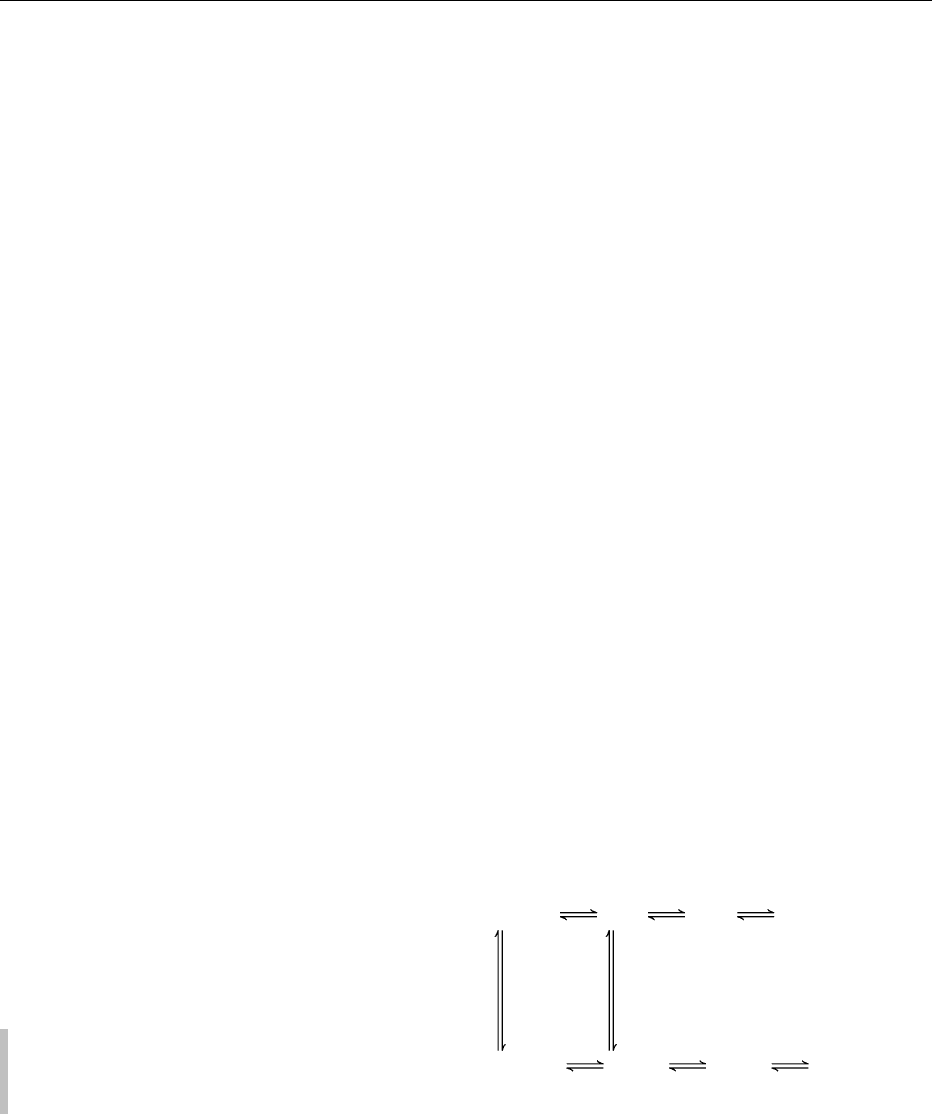
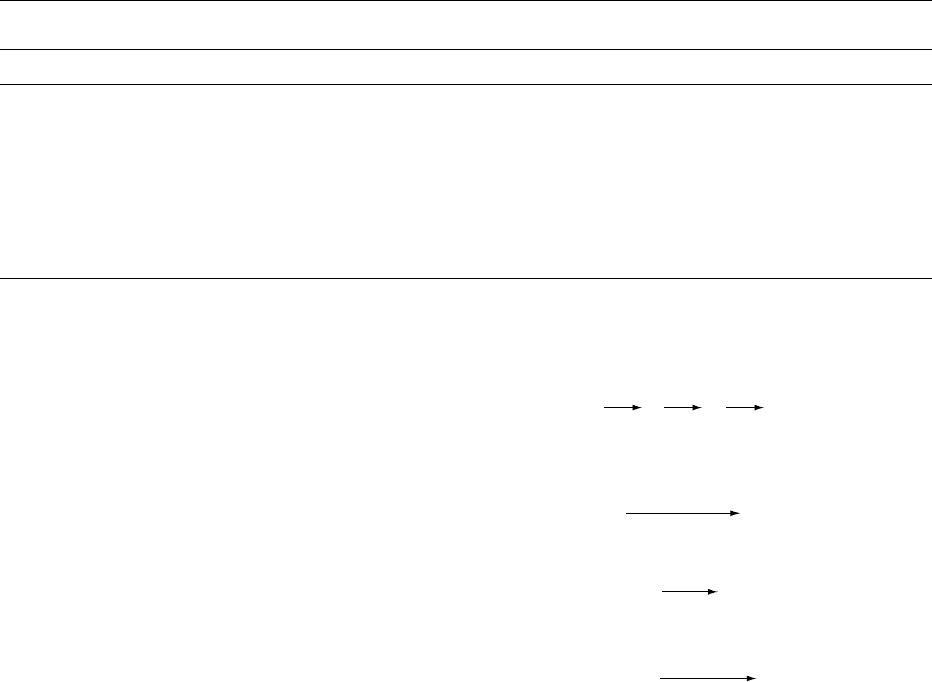
Brewing
Malt
Barley
Maize
Rice
β-Glucanase
Cellulase
Fermentation
α-Amylase
Glucoamylase
Peptidase
Aging
Filtration
Bottling
fig0006 Figure 6 Enzymes used in brewing. Data from Bigelis R (1993)
Carbohydrases. In: Nagodawithana T and Redd G (eds) Enzymes
in Food Processing, pp. 121–147. California: Academic Press.
ENZYMES/Uses in Food Processing 2137

with transglutaminase to manufacture cross-linked
casein, which was less allergenic.
0077 In developing countries, many people are still
suffering from starvation and efforts are being
focused on producing acceptable protein foods from
nonanimal protein, to solve the problem of protein
deficiency. On the other hand, in addition to their
awareness of health problems caused by obesity,
people in developed countries are increasingly aware
of the environmental burden caused by surplus live-
stock. When presented with a novel food product,
consumers are very sensitive to properties such as
flavor, nutritional value, appearance, shelf-life, and
palatability. In this respect, protein modification by
enzymes, especially by microbial transglutaminase,
the mass production of which can be achieved by
fermentation from cheap substrates, is one of the
most promising alternatives in developing novel
protein foods.
0078 Up to now, commercial transglutaminase has been
merely obtained from animal tissues. The compli-
cated separation and purification procedure results
in an extremely high price for the enzyme. The pro-
duction of transglutaminase derived from micro-
organisms was not reported until the late 1980s, and
recently a modified downstream process for purify-
ing microbial transglutaminase was described. The
microbial process no doubt has an advantage in its
independence from regional and climatic condition,
in addition to its reasonable cost. But it is still of great
interest to improve fermentation and downstream
processing to reduce production cost. Modification
of strains by genetic engineering is one of the alterna-
tives.
Cleaning
0079 A major use of enzymes as proteases has been in the
production of detergents. These are used widely in the
food industry, especially for cleaning-in-place appli-
cations, where the equipment is sensitive to heat. (See
Cleaning Procedures in the Factory: Types of Deter-
gent.)
0080 Pancreatin (extracted from the pancreatic glands
of animals), which contains the protein-degrading
enzyme trypsin, was used as early as 1913 in laundry
detergents. The detergent, being mainly composed of
ordinary washing soda (sodium carbonate), had an
excellent softening effect on water and helped to dis-
solve dirt. The trypsin, however, had only a limited
effect.
0081 During the 1960s, there was a significant new de-
velopment in the detergent industry when a mixture of
serine and microbial proteases, which appeared to be
less degradable by soaps, alkalis and temperature,
replaced trypsin. These enzymes have a serine-histi-
dine active site and produce their effect in the pH
range 6.5–10.0 and a temperature range of 30–60
C.
0082There was a temporary setback in the early 1970s
when it was realized that enzymes could cause allergic
reactions among the staff working in the enzyme
plant, in detergent factories, or the end users.
0083The introduction of encapsulated proteases in the
1980s and the withdrawal of the US Federal Trade
Commission’s restrictions were followed by a resur-
gence in the demand for proteases in detergents. Pro-
teases remove protein stains and deposits from a wide
range of food sources. These organic stains have a
tendency to adhere strongly to textile fibers and equip-
ment surfaces. The proteins act as glues, preventing
water-borne detergent systems from removing some
of the other components of the stain/deposit, such as
pigments and particulate material. Nonenzymatic de-
tergents are inefficient in removing proteins and can
result in permanent stains due to oxidation and de-
naturing caused by bleaching and drying.
0084Proteases hydrolyze proteins and break them down
into more soluble polypeptides. Through the com-
bined effect of surfactants and enzymes, stubborn
stains/deposits can be removed. Though protein
stains can be easily digested by enzymes, oil and
fatty stains have always been troublesome to remove.
The trend towards lower cleaning temperatures has
made the removal of grease spots an even greater
problem.
0085Amylases are also used to remove residues of
starchy foods, such as mashed potato, spaghetti, oat-
meal porridge, custard, gravy, and chocolate.
See also: Beers: Biochemistry of Fermentation; Biscuits,
Cookies, and Crackers: Methods of Manufacture; Bread:
Breadmaking Processes; Chemistry of Baking; Cakes:
Methods of Manufacture; Chemistry of Baking; Cheeses:
Starter Cultures Employed in Cheese-making; Mold-
ripened Cheeses: Stilton and Related Varieties; Surface
Mold-ripened Cheese Varieties; Enzymes: Functions and
Characteristics; Uses in Analysis; Fermented Milks:
Types of Fermented Milks; Other Relevant Products;
Wines: Production of Table Wines; Production of
Sparkling Wines
Further Reading
Alkorta I, Garbisu C, Liama MJ and Serra JL (1998) Indus-
trial applications of pectic enzymes: a review. Process
Biochemistry 33: 21–28.
Bigelis R (1993) Carbohydrases. In: Nagodawithana T and
Redd G (eds) Enzymes in Food Processing, pp. 121–147.
California: Academic Press.
Chitpinityol S and Crabbe MJ (1998) Chymosin and aspar-
tic proteinases. Food Chemistry 61: 395–418.
2138 ENZYMES/Uses in Food Processing
Cowan DA (1994) Industrial enzymes. In: Moses V and
Cape RE (eds) Biotechnology, pp. 311–340. UK: Har-
wood Academic Publisher.
Godfrey T and West SI (1996) Introduction to industrial
enzymology. In: Godfrey T and West SI (eds) Enzym-
ology, pp. 1–8. London: MacMillan Press.
Godtfredesen SE (1993) Lipases. In: Nagodawithana T and
Redd G (eds) Enzymes in Food Processing, pp. 205–214.
California: Academic Press.
Goll DE, Robson RM and Stromer MH (1977) Muscle
proteins. In: Whitaker JR and Tannenbaum SR (eds)
Food Proteins, pp. 121–174. Westport: AVI.
Guzman-Maldonado H and Paredes-Lopez O (1995) Amy-
lolytic enzymes and products derived from starch: a
review. Critical Reviews in Food Science and Nutrition
35: 373–403.
Lanzarini G and Pifferi PG (1990) Enzymes in fruit juice
industry. In: Cantarelli C and Lanzarini G (eds)
Biotechnology Applications in Beverage Production,
pp. 189–221. London: Elsevier.
Linko P (1987) Enzymes in the industrial utilization of
cereals. In: Kruger JE, Lineback D and Stauffer CE
(eds) Enzymes and their Role in Cereal Technology,
pp. 357–374. St Paul: AACC.
Mathewson PR (2000) Enzymatic activity during bread
baking. Cereal Foods World 45: 98–101.
O’Rourke T (1996) Brewing. In: Godfrey T and West SI
(eds) Enzymology, pp. 103–131. London: MacMillan
Press.
Schmid RD and Verger R (1998) Lipases: interfacial
enzymes with attractive applications. Angewandthe
Chemie International Edition (in English) 37: 1608–
1633.
Whitaker JR (1982) Enzymes of importance in high protein
foods. In: Dupuy P (ed.) Proceedings on the Use of
Enzymes in Food Technology, pp. 329–358. Paris:
Lavoisier.
Zhu Y, Rinzem A, Tramper J and Bol J (1995) Microbial
transglutaminase – a review of its production and appli-
cation in food processing. Applied Microbiology and
Biotechnology 44: 277–282.
Uses in Analysis
J R Whitaker, University of California, Davis, CA, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
0001 Enzymes are ideal for analyses because of their high
specificity and sensitivity. Any compound that affects
the activity of an enzyme, i.e., substrate, inhibitor, or
activator, can be determined rapidly and quantita-
tively by adding such compounds to a controlled
enzyme reaction and comparing the results without
the compound (control). Also, measurements of ac-
tivities of selected enzymes in a biological specimen
under standard conditions are useful in medicine for
the diagnosis and prognosis of almost all diseases.
More recently they have been used for determining
specific genetically related diseases. They are also used
for assessing nutritional deficiencies, physical damage
to organs, suitability for and adequacy of processing
and quality of foods, identifying subcellular organ-
elles and membrane structures, and structural config-
urations of molecules. Enzymes are ideal reporters for
measuring antigens to specific antibodies (enzyme
immunoassays).
0002Enzyme usage in analyses is not new. Peroxidase
was used for hydrogen peroxide analysis as early as
1845. Enzymatic carbohydrate determination in bio-
logical materials was an accepted method by the end
of the nineteenth century. But most progress in using
enzymes analytically has occurred in the last 20 years
as a result of readily available pure enzymes, better
understanding of the factors which affect enzyme
activity, enzyme kits for specific determinations,
easily usable sensitive techniques, and instrumenta-
tion matching the specificity and sensitivity of the
enzymes. The rapid progress in sequencing genes,
including the human genome, is due to two specific
types of enzymes: the restriction endonucleases and
the polymerases.
Principles and Applications
0003Compounds to be measured must bind stereospecific-
ally at the active site of an enzyme or another specific
location on the enzyme such that the activity of the
enzyme is affected (eqn 1).
E + S E
.
S E
.
P E + P
E
.
X + S E
.
S
.
X E
.
P
.
X E
.
X + P
X
K
d
X
K
d
k'
1
k'
−1
k
1
k
−1
k'
3
k'
2
k'
−3
k'
−2
k
2
k
−2
k
3
k
−3
(1)
E, enzyme; S, substrate; ES, enzyme-substrate com-
plex; EP, enzyme-product complex; P, product; X,
inhibitor or activator; EX, enzyme-inhibitor (or acti-
vator) complex; ESX, enzyme-substrate-inhibitor (or
activator) complex; EPX, enzyme-product-inhibitor
(or activator) complex; K
d
, dissociation constant; k
1
,
k
2
, k
3
, k
0
1
, k
0
2
and k
0
3
are forward rate constants.
0004There must be a predictable relationship between the
concentration of a compound and its effect on enzym-
atic activity. Standard curves for compounds and
ENZYMES/Uses in Analysis 2139
their products, including enzymes, to be determined
are required in order to obtain absolute concentra-
tions. In preparing the standard curve of initial vel-
ocity, v
o
, versus compound or product concentration,
purity of the analyte is essential and exact reproduc-
tion of experimental conditions is required. In the
total change method (below), strict adherence to ex-
perimental conditions (such as rate of reaction) is not
required, but it is essential to have pure standard
compounds and products and to insure the reaction
has gone to completion.
Determination of Substrate
Concentration
000 5 The concentration of any compound that serves as a
substrate, S, for an enzyme can be determined quan-
titatively by its effect on the initial velocity, v
o
, of the
reaction, provided K
m
and V
max
are known, as shown
in eqn 2, and provided [S]
o
<20K
m
:
v
o
¼ V
max
½S
o
=ðK
m
þ½S
o
Þð2Þ
Best results are obtained at [S]
o
<5K
m
. This is called
the rate (or kinetic) assay method.
0006 The concentration of a compound that is a sub-
strate can also be determined by a total change
method when all the substrate is converted to prod-
uct, which is then measured. It is essential to insure
that all substrate has been converted to product,
which may take several hours at the concentration
of enzyme used in rate assays. Therefore, higher
concentrations of enzymes are used in total change
method assays than in rate assays. The total
change method cannot be used for reactions that
reach an equilibrium between substrate and product
unless the product is trapped, forcing the reaction to
completion. An example is alcohol dehydrogenase
(alcohol:NAD
þ
oxidoreductase, EC 1.1.1.1) acting
on ethanol and NAD
þ
, as shown in eqn 3. Hydro-
xylamine is used to trap ethanal as the oxime, forcing
the reaction to completion (eqn 4). The NADH con-
centration is measured spectrophotometrically.
CH
3
CH
2
OH þ NAD
þ
Ð CH
3
CHO þ NADH þ H
þ
ð3Þ
CH
3
CHO þ NH
2
OH Ð CH
3
CHNOH þ H
2
O ð4Þ
0007Special care must be taken in determining concentra-
tions of substrates which exist in more than one
anomeric form, in equilibrium with each other. An
example is the mutarotation of reducing sugars. Glu-
cose at equilibrium exists in the a, b, and open-chain
forms in the ratio of 33:66:1, respectively. Glucose
oxidase, often used to determine glucose concentra-
tions, has strong preference for the b-d-glucose
anomer, versus the a-d-glucose anomer (156:1 rela-
tive rate of oxidation). Therefore, both the total
change method and the rate assay method may not
give the correct concentration, unless a standard
curve for glucose is established under the exact same
conditions.
0008Some examples of compounds that can be quanti-
tatively determined because they are enzyme sub-
strates are shown in Table 1. Only a very few
examples are given, since, with more than 1000
enzymes with individual specificities, at least that
number of compounds can be uniquely determined.
(See Fructose; Lactose; Starch: Structure, Properties,
and Determination.)
0009Advantages of enzyme analyses for substrates,
versus other types, include: (1) the very high specifi-
city, permitting isomers to be distinguished; (2) no
need for partial purification; and (3) the ability to
work at room temperature, or below, with thermo-
labile compounds. An example will illustrate this.
Reducing sugar methods, such as alkaline copper
solutions, ferricyanide or 3,5-dinitrosalicylic acid
for glucose, will determine all reducing sugars in
the solution, plus other reducing compounds. How-
ever, glucose oxidase, which catalyzes the reaction
tbl0001 Table 1 Analytical determination of compounds that are substrates
a
Compound Enzymeused Analysismethod
Ammonia Glutamate dehydrogenase S; NADH ! NAD
þ
Ethanol Alcohol dehydrogenase S; NAD
þ
! NADH
D-Fructose Hexokinase S; NADP
þ
! NADPH, in coupled assay
D-Glucose Glucose oxidase S; H
2
O
2
with peroxidase
L-Lactic acid L-Lactate dehydrogenase S; NAD
þ
! NADH
D-Lactic acid D-Lactate dehydrogenase S; NAD
þ
! NADH
Lactose b-Galactosidase S; H
2
O
2
with peroxidase and glucose oxidase
Starch Amyloglucosidase S; NADH ! NAD
þ
, in coupled assay through glucose and glucose oxidase
Urea Urease E; NH
3
electrode
a
S, spectrophotometric method; E, electrometric method.
Adapted from Guilbault GG (1984) Analytical Uses of Immobilized Enzymes. New York: Marcel Dekker.
2140 ENZYMES/Uses in Analysis
shown in eqn 5, will only determine glucose. Fur-
thermore, it is absolutely specific for d-glucose
versus l-glucose and oxidizes b-d-glucose 156
times more rapidly than a-d-glucose. The reaction
shown in eqn 6 is not catalyzed by glucose oxidase.
The rate is slower than that of eqn 5 and therefore
cannot be used to determine glucose concentration
by the rate method. Therefore, the H
2
O
2
concen-
tration is determined by use of peroxidase and a
chromagen that gives a colored compound that is
measured spectrophotometrically (coupled reac-
tions). The peroxidase and chromagen concentra-
tions must be high enough so that the rate of
reaction shown in eqn 5 is rate-determining, not
the reaction shown in eqn 7.
β-D-Glucose + O
2
β-D-Glucone-δ-lactone
Glucose
oxidase
(5)
+ H
2
O
2
β-D-Glucone-δ-lactone + H
2
O
β-
D-Gluconic acid
(6)
H
2
O
2
+ Chromagen
peroxidase
Colored compound
(7)
Determination of Inhibitor Concentration
0010 Any compound that decreases v
o
when added to an
enzyme–substrate system is an inhibitor. Compounds
that are reversible inhibitors can only be determined
by rate assay methods, while irreversible inhibitors
can be determined by either rate assays or total
change assays. When X in eqn 1 binds only to E,so
as to decrease enzyme activity (i.e., both ES and EX
are formed), it is a competitive inhibitor; k
0
1
is zero.
Therefore, the concentration of the compound can be
determined from the ratio of v
0
o
/v
o
, where v
0
o
is the
initial velocity determined in the presence of a fixed
concentration of inhibitor, [I], and v
o
is the initial
velocity determined in the absence of inhibitor pro-
vided K
m
,[S], and K
i
( ¼ [E][I]
o
/[EI]; K
d
in eqn 1)
for the inhibitor are known. This relationship is
shown as:
v
0
o
=v
o
¼ðK
m
þ½S
o
Þ=fð1 þ½I
o
=K
i
Þ=K
m
þ½S
o
gð8 Þ
0011 If X binds to E and E S equally well (eqn 1) and k
0
1
and k
0
2
are zero, the X is a linear noncompetitive
inhibitor. [I]
o
can be determined from:
v
0
o
=v
o
¼ 1 þ½I
o
=K
i
ð9 Þ
provided K
i
for the inhibitor is known.
0012If X binds only to ES (eqn 1) and k
0
2
is zero, then
X is a linear uncompetitive inhibitor. [I]
o
can be
determined from:
v
0
o
=v
o
¼ðK
m
þ½S
o
Þ=fK
m
þ½S
o
ð1 þ½I
o
=K
i
Þg ð10Þ
provided K
m
,[S]
o
, and K
i
are known.
0013If X reacts chemically with E to form an irrevers-
ible product, E-X, then the extent of inhibition is
linearly related to the concentration of X as long as
[X]<[E] and the reaction is allowed to go to comple-
tion (total change method). The concentration of X
can be calculated, provided [E]
o
is known by:
v
0
o
=v
o
¼ð½E
o
½E-XÞ=½E
o
ð11Þ
where [E-X] ¼ [X]and[E]
o
is concentration of total
active enzyme used. Table 2 gives a few examples of
compounds that can be determined enzymatically be-
cause they are enzyme inhibitors, thereby decreasing
v
o
when added to an enzyme–substrate system.
0014Theoretically, any compound that is a substrate can
be determined by inhibition kinetics since two sub-
strates (one at a fixed concentration, while the un-
known substrate concentration is variable) in the
system compete for binding at the active site of
the enzyme, based on their relative K
m
values. One
need only determine v
o
for one of the substrates (con-
trol), and treat the second substrate as a competitive
inhibitor to determine v
0
o
.(See Aluminum (Alumin-
ium): Properties and Determination; Ascorbic Acid:
Properties and Determination; Lead: Properties and
Determination; Mercury: Properties and Determin-
ation.)
Determination of Activator Concentration
0015Any compound that increases v
o
when added to an
enzyme-substrate system is an activator. Compounds
tbl0002Table 2 Analytical determination of compounds that are
inhibitors
a
Compound Enzymeused Analysismethod
Pesticides Cholinesterase E; H
þ
; thiocholine
DDT Carbonic anhydrase S; H
þ
with indicator
Heparin Ribonuclease S; degradation of RNA
Ascorbic acid Catalase S; uric acid
Ag
þ
Alcohol dehydrogenase
(yeast)
S; NAD
þ
! NADH
Al
3 þ
Alkaline phosphatase S; p-nitrophenol
Hg
2 þ
Alcohol dehydrogenase S; NAD
þ
! NADH
Pb
2 þ
Peroxidase F; fluorescent product
F
Liver esterase E; H
þ
S
2
Peroxidase F; fluorescent product
a
The methods listed for the anions may not be absolutely specific: similar
types of ions may interfere.
DDT, dichlorodiphenyltrichloroethane; E, electrometric method; F,
fluorescent method; S, spectrophotometric method.
Adapted from Guilbault GG (1984) Analytical Uses of Immobilized Enzymes.
New York: Marcel Dekker.
ENZYMES/Uses in Analysis 2141
that form a rapid equilibrium complex with an
enzyme (and/or ES) as shown in eqn 1 can only be
determined by rate assay methods. This is character-
ictic of coenzymes, such as NAD
þ
, NAD(P)
þ
, nucle-
otide triphosphate coenzymes adenosine triphosphate
(ATP), uridine 5
0
-triphosphate, cytidine 5
0
-triphos-
phate) and some metal ions. At a fixed concentration
of enzyme and substrate, the concentration of activa-
tor, A, can be determined from:
v
o
o
¼ v
2
o
v
o
¼ V
max
½A=ðK
d
þ½A Þð12Þ
providedK
d
(¼[E][A]/[E A])andV
max
areknown.v
2
o
is
initial velocity in the presence of the activator. In most
cases,v
o
intheabsenceofcoenzymeiszero,sothatv
0
o
¼
v
2
o
isobserved;thisistheincreaseinactivityinpresence
of a given concentration of A.(See Coenzymes.)
0016 Activators that form tight complexes (K
d
<10
9
mol l
1
) with enzyme, such as prosthetic groups and
some metal ions, increase activity of the enzyme in a
linear fashion (v
o
o
is directly proportional to [A]
o
).
Therefore, only a total change method is useful.
0017 It is essential to prepare a standard curve of v
o
versus [A]
o
in order to convert measured v
o
values
to absolute concentration. Purity of the standard
activator and reproduction of experimental condi-
tions are essential.
0018 Table 3 gives a few examples of compounds that
activate enzymes. Several inferences may be drawn
from the examples presented. With the exception of
O
2
, all the compounds listed are cofactors. They are
absolutely required for enzymatic activity.
0019 One enzyme may be used to analyze for several
compounds. For example, luciferase can determine
luciferin (substrate), ATP, Mg
þ
,andO
2
concentra-
tions, since all affect the activity of the enzyme
(eqn 13).
Luciferin+O
2
Luciferase
Oxidized luciferin
ATP, Mg
2+
(+ phosphorescence)
(13)
Determination of Enzyme Concentration
0020Determining enzyme concentration by measuring the
initial velocity, v
o
, at which a substrate is converted to
product seems straightforward. Yet it is fraught with
difficulties unless careful attention is given to the
design of the experiment, as time, substrate, pH,
temperature, activators, and inhibitors all affect v
o
for a fixed concentration of enzyme. Therefore, if the
enzyme concentration, [E]
o
, is to be measured accur-
ately and precisely, all these other parameters must
be controlled exactly among experiments. It is im-
portant to determine the initial velocity, v
o
, so that
changes in substrate concentration, stability of the
enzyme, approach to equilibrium, and/or inhibition
by the product are not factors. The substrate concen-
tration does not need to be much greater than K
m
when v
o
is measured. Any substrate concentration,
when precisely reproduced, will give a linear rela-
tionship between v
o
and [E]
o
, with a few exceptions.
The temperature should be below optimum tempera-
ture so the enzyme is stable and the pH must be close
to the optimum pH for maximum sensitivity.
0021Determination of absolute concentration of
enzyme based on v
o
requires a standard preparation
of the enzyme with known purity, based on activity.
For example, if it is known that a 5 ml aliquot con-
taining 1 mg of 100% active pure enzyme has a v
o
of
30 mmol of product formed per minute, while a 5 ml
aliquot of an unknown sample has a v
o
of 6 mmol of
product formed per minute under the same condi-
tions, then the unknown aliquot contains 0.2 mgof
the enzyme.
0022Table 4 gives a few selected examples of analytical
determinations of enzyme concentration. (See Spec-
troscopy: Fluorescence; Overview.)
Structural Analysis
0023Because of their high specificity, enzymes are ideal
probes of molecular structure. They can distinguish
between: d/l, cis/trans, a/b, and other stereospecific
configurations; nature, location, and sequence of
monomeric units in heteropolymers (proteins, carbo-
hydrates, nucleic acids); and secondary, tertiary, and
quaternary structures of polymers. They are useful in
determining location of enzymes and substrates in
organs (histochemistry) and in identifying subcellu-
lar organelles (based on enzyme composition), cell
walls and membranes. The restriction enzymes
and ligases are essential tools in recombinant DNA
tbl0003 Table 3 Analytical determination of compounds that are
activators
a
Compound Enzyme used Analysismethod
ATP Luciferase S; NADH ! NAD
þ
,in
coupled reaction
FAD
D-Amino acid oxidase E; O
2
electrode
K
þ
Phosphofructokinase S; activation of enzyme
Mg
2 þ
Luciferase F; chemiluminescence
Zn
2 þ
Aminopeptidase
apoenzyme
S; p-nitrophenol
O
2
Luciferase F; chemiluminescence
a
A few examples of many. There are alternative methods, depending on
instruments, substrates, and enzymes available.
ATP, adenosine triphosphate; FAD, flavin adenine dinucleotide; E,
electrometric method; F, fluorescent method; S, spectrophotometric
method.
Adapted from Guilbault GG (1984) Analytical Uses of Immobilized Enzymes.
New York: Marcel Dekker.
2142 ENZYMES/Uses in Analysis
technology and genetic engineering, being highly
specific for nucleotide primary and secondary struc-
tures. As probes of structure, unequivocal deter-
mination of activity, or lack of activity, is more
important than the absolute velocity of product for-
mation (v
o
).
Determination of
v
o
0024 Determination of v
o
for formation of product (dP/dt),
disappearance of substrate ( dS/dt), change in energy
(as heat), or change in pH is required for analytical
use of enzymes, as indicated by the preceding discus-
sion. This requires the ability to detect a change
during the reaction. Changes in absorbance, fluores-
cence, phosphorescence, electrical properties includ-
ing pH, or heat are appropriate monitors. Excellent
instrumentation is available for detection of all these
changes. The best methods are those where a continu-
ous recording of the change is possible, often with
software to convert the measured rate of change dir-
ectly to concentration of the compound being meas-
ured. Data accumulation and analysis are easy when
the change is continuously recorded. However, some-
times an aliquot of the reaction must be removed
periodically, another reagent added to give a colored
derivative (for example) of product or substrate and
then the concentration of the derivative determined.
Sometimes v
o
can be measured only after chromato-
graphic separation of the products. These are lengthy,
laborious assays that frequently lead to one-point
assays. v
o
, based on one-point assays, must be
accepted with great caution.
002 5 Often, solutions to difficult analyses are possible
via coupled enzyme assays. A coupled enzyme assay
involves two or more enzymes, in which the product
of the last enzyme is measured as shown in eqn 14.
The intent is to measure the concentration of A
(or E
1
). However, the product B is analytically very
difficult to determine, while D is very easy to
determine:
(14)
A
BCD
E
1
E
2
E
3
0026A specific example will illustrate this better (eqns
15–17).
(15)
Sucrose + H
2
O
Invertase
Glucose + Fructose
Glucose + O
2
+ H
2
O
Glucose
D-Gluconic acid + H
2
O
2
Oxidase
(16)
H
2
O
2
+ Chromagenic
substrate
Peroxidase
Fluorescent product
(or colored)
(17)
0027Coupled reactions often involve terminal enzymes
requiring NAD
þ
(NADH) or NADP
þ
(NADPH),
since the extinction coefficient at 340 nm is 6.22
10
3
mol l
1
cm
1
for NADH (or NADPH) versus
NAD
þ
(or NADP
þ
), a very large change.
0028Coupled reactions require enzymes with similar pH
optima and that v
o
( ¼ k
2
[E][S]
o
/(K
m
þ [S]
o
)) be at
least 100 times larger for reactions catalyzed by E
2
,
E
3
, etc., than for E
1
. This is usually met by using high
concentrations of E
2
, E
3
, etc. The rationale for this is
the concentrations of final product measured (D in
eqn 14; hydrogen peroxide in sucrose determination
eqns 15–17) must be a stoichiometric reflection of
concentration of substrate A (or E
1
) being deter-
mined. The examples in Tables 1–4 illustrate how
frequently coupled reactions are used.
0029Soluble enzyme systems are not required for deter-
mining v
o
(and analyte concentration). In fact,
present emphasis is on the use of immobilized enzyme
systems in columns, electrodes, biosensor chips
and antibody–enzyme conjugates (enzyme-linked
immunosorbent assay (ELISA), for example).
Immobilized enzymes are more stable than nonim-
mobilized enzymes and may be used repeatedly.
Dozens of enzyme electrodes are available (several
tbl0004 Table 4 Analytical determination of enzyme concentration
a
Enzyme Substrate used Analysismethod
Catalase H
2
O
2
E; O
2
b-Galactosidase o-Nitrophenyl-b-D-galactoside S; o-nitrophenol
Invertase Sucrose S; use of glucose oxidase/peroxidase coupled assay
Lipase Tributyrin E; H
þ
Pectin methylesterase Pectin E; titrate H
þ
formed
Peroxidase H
2
O
2
, 4-aminoantipyrine, p-hydroxybenzoate S; oxidized, conjugated 4-aminoantipyrine
Phosphatase, alkaline p-Nitrophenyl phosphate S; p-nitrophenol
Polyphenol oxidase Pyrocatechol S; benzoquinone
Xanthine oxidase Hypoxanthine S; uric acid
a
There are several methods available for each enzyme. Availability of instruments and substrates often determine choice of method.
E, electrometric method; F, fluorescent method; S, spectrophotometric method.
Adapted from Guilbault GG (1984) Analytical Uses of Immobilized Enzymes. New York: Marcel Dekker.
ENZYMES/Uses in Analysis 2143

commercially) that have response times equivalent to
a hydrogen (pH) electrode and can be used repeatedly
for several months. Biosensors involving multiple
microchips are being developed, which may deter-
mine up to eight or more enzymes, substrates, or
other compounds simultaneously when a drop of
blood, urine, or other biological fluid is added. (See
Immunoassays: Radioimmunoassay and Enzyme Im-
munoassay.)
See also: Aluminum (Aluminium): Properties and
Determination; Ascorbic Acid: Properties and
Determination; Coenzymes; Fructose; Immunoassays:
Radioimmunoassay and Enzyme Immunoassay; Lactose;
Lead: Properties and Determination; Mercury: Properties
and Determination; Spectroscopy: Overview; Starch:
Structure, Properties, and Determination
Further Reading
Bergmeyer HU, Bergmeyer J and Grassl M (eds) (1983)
Methods of Enzymatic Analysis, 3rd edn. Weinheim:
Verlag Chemie.
Colowick SP and Kaplan NO (eds) (1955–1999) Methods
in Enzymology, vols 1–300. Orlando: Academic Press.
Guilbault GG (1984) Analytical Uses of Immobilized
Enzymes. New York: Marcel Dekker.
Whitaker JR (1974) Analytical applications of enzymes. In:
Whitaker JR (ed.) Food Related Enzymes. Advances in
Chemistry Series 136: 31–78.
Whitaker JR (1984) Biological and biochemical assays in
food analysis. In: Stewart KK and Whitaker JR (eds)
Modern Methods of Food Analysis, pp. 187–225. West-
port: AVI.
Whitaker JR (1985) Analytical uses of enzymes. In: Gruen-
wedel DW and Whitaker JR (eds) Biological Techniques.
Food Analysis: Principles and Techniques, vol. 3, pp.
297–377. New York: Marcel Dekker.
Whitaker JR (1994) Principles of Enzymology for the Food
Sciences, 2nd edn. New York: Marcel Dekker.
Whitaker JR (1996) Enzymes. In: Fennema OR (ed.) Food
Chemistry, 3rd edn, pp. 514–518. New York: Marcel
Dekker.
EPIDEMIOLOGY
P C Elwood, Llandough Hospital, Penarth, South
Glamorgan, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Aims of Epidemiology
0001 Epidemiology is the study of health and disease in the
community. There are two groups of aims: first, to
describe the distribution, the pattern, and the natural
history of disease in the general population, and
second, to identify factors that may be causal in a
disease process, and to evaluate strategies for the
control, management, and prevention of a disease.
0002 In nutritional research, epidemiology aims to iden-
tify associations between nutrients or food items and
the risk of a disease, and then test these associations
to verify whether they are likely to be causal. In
practice, epidemiology is multifaceted and a number
of preliminary considerations will help to put it
into context within general medical and biological
research.
0003 Epidemiologists rarely generate hypotheses. Most
ideas about the causation of disease arise from clinical
observations, metabolic studies, or other intensive
investigations. The role of the epidemiologist is to
take these ideas and test them in representative
samples of the general community or, if appropriate,
in representative series of patients. In doing this the
epidemiologist not only tests the relevance of a factor
to the disease, but also seeks to obtain an estimate of
the relative importance of the mechanism or factor.
Furthermore, in a well-designed comprehensive
study, the extent to which the effect of any particular
factor of interest is independent of the effects of other
factors is established. This generally requires large
complex and long-term studies, based on samples of
subjects that truly represent the population.
0004The interest of the epidemiologist is therefore on
communities and his or her attention focuses ultim-
ately on lifestyles, on nutrition, and on environmental
factors. Thus the recent finding that certain throm-
bosis-related factors, such as plasma fibrinogen, are
very strongly predictive of future ischemic heart
disease events leads the epidemiologist on to search
for the dietary and lifestyle determinants of fibrino-
gen. The likely relevance of antioxidants to cancer
and other conditions leads the laboratory worker to
study free radicals and their cellular and other effects,
while the epidemiologist studies the relative protec-
tion given by diets rich in natural antioxidants, and
the effects of dietary antioxidant supplements. The
2144 EPIDEMIOLOGY

hypothesis that the regular consumption of fish is
associated with a low incidence of vascular disease
leads the biochemist to study the metabolism of fish
oils and mechanisms linking fish oils to blood pres-
sure and other cardiovascular risk factors, while the
epidemiologist sets up a randomized controlled trial
of fish eating and the incidence of vascular disease.
The different research approaches – clinical, labora-
tory, and epidemiological – are complementary and
all are needed.
0005 Only the epidemiologist, however, can estimate,
from studies based upon representative population
samples of individuals, the relative importance of
one particular factor to a disease, in comparison
with a host of other relevant factors. Thus, magne-
sium is a key element in many enzymes and is known
to be involved in a large number of metabolic and
other biological mechanisms. Only the epidemiolo-
gist can however estimate the importance of magne-
sium to health and disease in the population, and the
part played by magnesium deficiency, if any, in, say,
cardiovascular disease within a community.
The Concept of Risk Factors
0006 Epidemiologists were probably the first to use the
term ‘risk factor,’ applying it to any factor which
identifies an individual who is at increased risk of a
disease.
0007 The term is however vague and its limitations
should be understood. Thus the term is used to
cover factors which are inherent in a subject and
cannot be altered (such as sex and race, etc.), factors
which are likely to be causal and which can be
changed (such as dietary fat intake, blood pressure,
and plasma fibrinogen) and factors which confound
relationships of interest (such as age and social class).
Factors in this last group are perhaps the most diffi-
cult to identify and deal with. For example, in exam-
ining the relationship between a nutrient and a
disease, calorie intake can often be a confounding
variable, in that it is probably related to the intake
of the nutrient of interest (for most nutrients, the
more food that is eaten, the greater the intake of any
nutrient), and calorie intake, or total energy, is a good
surrogate measure for exercise level which, in turn, is
strongly related to the incidence of vascular and other
diseases.
0008 Another suggested modification of the concept of
‘risk factor’ is to refer to ‘predictors’ of a disease (such
as cholesterol level, blood pressure, plasma fibrino-
gen and other biochemical and hematological factors)
and ‘determinants’ of those predictors (such as diet-
ary fat intake, salt intake, smoking habit, and other
lifestyle and dietary factors). This last grouping has
the great advantage that it acknowledges the differ-
ence between factors involved at the level of meta-
bolic processes, and extrinsic factors, upon which
preventive strategies which are under the control of
subjects themselves, and population-based interven-
tion initiatives, can be focused.
Epidemiological Methods
0009A variety of strategies are used in epidemiology. Ba-
sically these can be divided into prospective and retro-
spective, and into observational and experimental.
Every combination of these is possible: changes over
time; comparisons between communities; individual
case-control comparisons; cross-sectional surveys;
prospective cohort studies; and the randomized con-
trolled trial (RCT) with intervention. Another way in
which the various strategies can be classified is by the
degree of certainty of the conclusions drawn from
them. This last is so important that the various
study designs which are described below are listed in
the order of the likely certainty of the conclusions that
can be drawn from the evidence they yield.
Trends with Time
0010There have been great changes in the mortality of
many diseases, including many cancers and coronary
heart disease (CHD), in most countries during the
past century and it is possible to look for dietary
changes which parallel these changes in disease inci-
dence. Great difficulties arise, however, because infor-
mation on past disease is uncertain and knowledge of
past dietary intakes is very poor. Diagnostic criteria
change, and the attributions of certain causes to
deaths have changed markedly over the years. In
addition, estimates of the nutrient content of food
change, as reflected in food composition tables. The
MONICA study, set up by the World Health Organ-
ization in about 40 countries to study changes over
time in CHD, and in relevant risk factors, is probably
the most ambitious study of this kind ever mounted.
0011Even if reliable data on both diets and disease were
available, the two cannot be linked with certainty
because many other relevant factors may have
changed concurrently. Diet is only one aspect of life-
style and it should never be considered in isolation.
Cross-community Comparisons
0012There are differences in disease rates in different com-
munities and some of these are large. Relating these to
differences in dietary intakes has generated a number
of interesting hypotheses. There are difficulties how-
ever in that the dietary data available for the different
EPIDEMIOLOGY 2145

communities may not be truly representative for
those communities, and the disease data may not be
truly comparable. The biggest stumbling block is the
virtual impossibility of linking differences in disease
incidence to dietary differences since many other
factors – genetic, behavioral, and environmental –
will almost certainly be different and may well be
far more important in determining disease risk than
dietary differences.
Case-control Studies
0013 The identification of patients with evidence of a dis-
ease and the comparison of possible risk factors in
these with the same factors in disease-free subjects is a
basic research strategy. Difficulties arise, however,
because the ‘cases’ are often patients with advanced
disease, who may not be representative of all such
patients. Furthermore, the observer cannot always be
‘blind’ with regard to whether a subject is a ‘case’ or a
‘control,’ and so that bias can easily be introduced
into the data on risk factors. Further difficulties arise
in the selection of suitable control subjects without
the disease, and though some of these difficulties can
be overcome by matching for factors such as sex, age,
and area of residence, uncertainties remain about
comparability between the cases and the controls
with respect to factors other than those believed to
be relevant to the disease.
0014 In nutritional research the case-control strategy has
only a very limited place because it necessitates in-
quiries about dietary intakes before the onset of the
disease, and it is very difficult for a patient to separate
out this information from dietary changes which have
been made since symptoms of the disease com-
menced. Furthermore, the case-control approach has
very little place in diseases with a high case fatality,
such as cancer and heart disease, because only a
selected subsample of all cases survive to be included
in any case-control study and these will certainly not
be representative of all patients with the disease. (See
Cancer: Epidemiology.)
Cross-sectional Survey
0015 One of the most common activities in epidemiology
and in social science is the conducting of surveys.
These can give estimates of the prevalence of a dis-
ease, the distribution of dietary intakes, and the levels
of risk factors, and associations between these can be
examined. For such purposes, it is essential that the
population sample selected for the study is truly rep-
resentative of the community being studied, and that
a high response rate is achieved because otherwise
representativeness will be compromised. Attention
has also to be given to the reproducibility of measure-
ments made. INTERSALT, an international collab-
orative study coordinated by WHO, was a good
example of a cross-sectional study. In this, about 40
research centers obtained data on blood pressure and
on salt excretion from 24-hr urine collections (a sur-
rogate for salt intake) in about 200 subjects per
center.
0016Cross-sectional studies have the great advantage
that all the data collected are contemporaneous, that
is, there is no dependence upon the memories of
subjects, nor is there any waiting for disease to
develop. On the other hand, surveys have the great
disadvantage that causal factors which predated the
onset of the disease cannot always be distinguished
from a factor which has been affected by the disease
itself. Thus, in a cross-sectional survey, differences in
dietary intakes between subjects with CHD and other
subjects, could equally well be the result of changes in
diet made by patients after their heart attack, or the
onset of angina, as the cause of the disease process.
0017One valuable role for cross-sectional surveys is the
identification of determinants of risk factors for dis-
ease. Thus the associations between dietary and other
lifestyle factors and, for example, serum cholesterol,
blood pressure, or serum fibrinogen can be examined.
Prospective Studies
0018The prospective, cohort, or longitudinal study is the
classic tool of the epidemiologist. In this, a representa-
tive population sample of subjects (a cohort) is exam-
ined and then followed forward in time. The
association between the levels of the various factors
measured at baseline, and the development of the
disease, is examined. In other words, the predictive
power for subsequent disease of dietary, lifestyle, bio-
chemical, hematological, and other factors is exam-
ined. The great advantage of this strategy is that the
suspected causal factors are measured before the dis-
ease becomes evident, and causal factors can therefore
be distinguished from factors which represent effects
of the disease.
0019The identification of factors showing greater than
chance associations with subsequent disease is how-
ever not the final answer. The degree to which the
predictive power of a factor for the disease is inde-
pendent of other factors must be examined. Thus, on
first analysis the dietary intakes of many dietary
factors is likely to be found to be predictive of a
range of diseases. It must be examined whether or
not such relationships are simply a consequence of
an age effect (older subjects having an increased risk
of most diseases and, probably, a reduced intake of
most nutrients) or due to confounding by smoking
2146 EPIDEMIOLOGY