Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

mostly on strong anion exchange (SAX) columns
using buffered mobile phases such as borate and
perchlorate mixtures and gradient elution. Azo dyes
and sulfonated intermediates can be separated using
weak anion exchange (WAX) columns with citric
acid mobile phase at pH 2.8. Because of poor repro-
ducibility (notably with the use of gradient elution),
the requirement for aggressive buffer systems and its
consequently relatively short column life, ion ex-
change has been largely superseded by reverse-phase
HPLC for the analysis of synthetic water-soluble
dyestuffs.
Reverse-Phase HPLC
0064 Synthetic dyes require buffered eluants to achieve
optimum pH conditions for desired separations on
reverse-phase HPLC, usually with organic mobile
phase modifiers methanol or acetonitrile. The column
materials used are short-chain (C
2
), octyl (C
8
), and
octadecyl (C
18
) alkyl-bonded silicas, though other
bonded phases such as amino (NH
2
) and cyano
(CN) have also been employed. Considerable inter-
est has been shown in the use of macroporous and
highly cross-linked polystyrene-divinylbenzene co-
polymer column packing materials. The mobile
phase may alter the affinity of ionic species for the
stationary phase by both ion suppression and ion-
pairing mechanisms.
0065Reverse-phase-HPLC with ion suppression has
been used to separate and identify various dyes,
eluting with phosphate buffers at various pH values
and methanol. Ammonium acetate has recently been
successfully used in this mode of reverse-phase
HPLC.
0066Ion-pair HPLC is perhaps the most widely used
chromatographic technique for the analysis of dyes,
subsidiary colors, and uncombined intermediates in
foodstuffs. Many published methods are available.
Most favored are ion-pair reagents derived from
quaternary ammonium compounds such as cetyltri-
methylammonium bromide (cetrimide) and tetra-
butylammonium phosphate. Again, buffered mobile
phases modified with organic solvents are generally
used.
0067Both isocratic and gradient systems can be
employed to separate dye mixtures; the latter is
often preferred for the separation of complex mix-
tures. Modern high-performance and computer-aided
instrumentation permits the use of many powerful
techniques which may be readily applied to aid in
the analysis of dyestuffs. These include:
.
0068automated sample handling and processing
.
0069automated chromatographic methods develop-
ment
.
0070high-sensitivity multiple-wavelength and diode-
array detectors
5
0
10
20
30
40
50
60
70
80
90
1
2
5
6
7
3
4
10
Time (min)
mAU
15 20 25
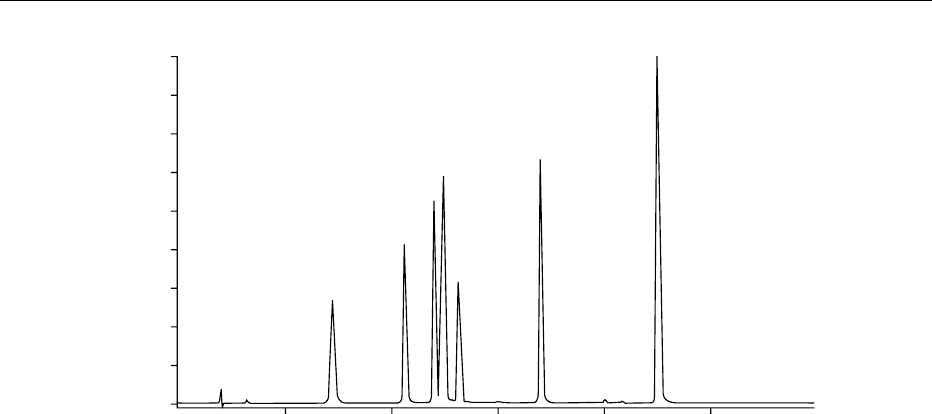
fig0002 Figure 2 High-performance liquid chromatographic (HPLC) chromatogram of red dye mixture separated by reverse-phase ion-pair
gradient elution. Conditions: solvent A ¼ 0.005 mol l
1
tetrabutylammonium bromide (TBAB) in methanol, solvent B ¼0.005 mol l
1
TBAB in 0.01 mol l
1
KH
2
PO
4
. Gradient elution profile: 50:50 to 100:0 (A:B) over 30 min linear, 10 min hold; solvent flow rate
¼0.4 ml min
1
; column: ODS 20 cm; detection wavelength: 520 nm. Peak identification: 1, amaranth; 2, allura red AC; 3,red
10B – nonpermitted analog of 4, Red 2 G; 5, ponceau 4R; 6, carmoisine; 7, erythrosine. Reproduced from Colours: Properties and
Determination of Synthetic Pigments, Encyclopaedia of Food Science, Food Technology and Nutrition, Macrae R, Robinson RK and Sadler
MJ (eds) 1993, Academic Press.
1566 COLORANTS (COLOURANTS)/Properties and Determinants of Synthetics Pigments
.0071 postrun qualitative and quantitative analysis
.
0072 liquid chromatography–mass spectrometry inter-
facing
Figure 2 shows a typical chromatogram of the separ-
ation of red food colors by gradient ion-pair HPLC. It
is possible to separate many of the UK-permitted and
several nonpermitted dyes on a single column system
by employing a combination of ion-pair gradient
elution and selective wavelength detection.
Diode Array Detection
0073 Diode array detectors have the ability to record the
entire spectral range of an eluting dye component
during an analysis. Absorbance data may be col-
lected simultaneously from 190 nm to as high as
800 nm and is achieved in real time. The diode
array detector allows the precise determination of
absorption maxima of adequately separated solutes
and facilitates positive peak identification and
peak purity analysis by rapid spectral scanning.
Chromatographic peaks may be identified by refer-
ence to spectral libraries of previously run reference
compounds. Multiple wavelength monitoring with
absorbance rationing may be used to characterize
and identify multicomponent dye mixtures in single
chromatographic runs. Chemometric techniques
similar to those used in direct spectrophotometry
have been used to characterize and quantify dye mix-
tures.
0074 These and other analogous methods and tech-
niques are also used for the detection and quantifica-
tion of nonpermitted dyes in foods.
See also: Adulteration of Foods: Detection; Amaranth;
Chromatography: Thin-layer Chromatography; High-
performance Liquid Chromatography; Gas
Chromatography; Supercritical Fluid Chromatography;
Colorants (Colourants): Properties and Determination of
Natural Pigments; Properties and Determinants of
Synthetic Pigments; Food Additives: Safety; Food
Labeling (Labelling): Applications; Food Safety; Mass
Spectrometry: Applications; Spectroscopy: Visible
Spectroscopy and Colorimetry
Further Reading
Damant A, Reynolds S and Macrae R (1989) The structural
identification of a secondary dye produced from the
reaction between sunset yellow and sodium meta-
bisulphite. Food Additives and Contaminants 6: 273–
282.
King RD (ed.) (1980) The determination of food colours.
In: Developments in Food Analysis Techniques 2, pp.
79–106. Barking: Applied Science Publishers.
Knowles ME, Gilbert J and McWeeny DJ (1974) Stability of
red food colours in the presence of nitrite in canned pork
luncheon meat. Journal of the Science of Food and Agri-
culture 25: 1239–1248.
Marmion DM (1984) Handbook of US Colorants for
Foods, Drugs, and Cosmetics, 2nd edn. New York:
John Wiley.
Marovatsanga L and Macrea R (1987) The determination
of added azo dye in soft drinks via its reduction prod-
ucts. Food Chemistry 24: 83–98.
Peters AT and Freeman HS (eds) (1995) Analytical Chemis-
try of Synthetic Colorants. Advances in Colour Chemistry
Series, vol. 2. London: Blackie Academic and Profes-
sional.
Reynolds SL, Scotter MJ and Wood R (1988) Determin-
ation of synthetic colouring matter in foodstuffs – col-
laborative trial. Journal of the Association of Public
Analysts 26: 7–25.
Trace Materials (Colours) Committee (1963) Analyst 88:
864.
Venkataraman K (ed.) (1977) The Analytical Chemistry of
Synthetic Dyes. New York: John Wiley.
Walford J (ed.) (1980) Developments in Food Colours 1.
Barking: Applied Science Publishers.
Walford J (ed.) (1984) Developments in Food Colours 2.
Barking: Elsevier Applied Science Publishers.
Colorimetry See Spectroscopy: Overview; Infrared and Raman; Near-infrared; Fluorescence; Atomic
Emission and Absorption; Nuclear Magnetic Resonance; Visible Spectroscopy and Colorimetry
Common Agricultural Policy See European Union: European Food Law Harmonization
COLORANTS (COLOURANTS)/Properties and Determinants of Synthetics Pigments 1567

COMMUNITY NUTRITION
J Cade, University of Leeds, Leeds, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Introduction
Community nutrition incorporates the study of nutri-
tion and the promotion of good health through food
and nutrient intake in populations. This article will
consider aspects of community nutrition relating to
dietary goals and recommendations for populations;
methods of assessing diet in population groups; and
promoting healthy eating at the community level.
0002 Community nutrition (public health nutrition) re-
quires a population approach. The community rather
than the individual is the focus of interest. This area
of nutrition focuses on the promotion of good health
and the primary prevention of diet-related illness. The
emphasis is on maintenance of health in the whole
population, although it will also include working
with high-risk groups and other subgroups within
the population. Community nutrition includes nutri-
tional surveillance; epidemiological studies of diet;
and also the development, implementation, and
evaluation of dietary recommendations and goals. A
community may be any group of individuals, for
example, the population of a town or country, or
the residents of an old people’s home.
Advice to the Community
0003 Dietary advice to the community has changed over
the years, depending on the nutrition-related diseases
of importance at the time and our understanding of
how they are caused. In the 1930s, for example, the
primary concern in Europe and North America was
the elimination of deficiency diseases. The concept of
a balanced diet was developed to try to provide the
minimum requirements of protein, vitamins, and
minerals. By the late 1950s, research suggested that
some chronic diseases could be related to overnutri-
tion and dieting to lose weight became popular. For
example, it was recommended that bread and potato
intake should be restricted to help avoid overweight.
However, by the 1980s, wholemeal bread and jacket
potatoes were being promoted as good sources of
dietary fiber.
0004 Recommended dietary allowances (RDAs) for
populations were first set in the 1930s and have been
revised at regular intervals. The current UK recom-
mendations were published in 1991, and are known as
dietary reference values (DRV). They include the ref-
erence nutrient intake (RNI) level which is the amount
of a nutrient (excluding energy) which is sufficient
for almost any individual. The RNI is 2 standard
deviations higher than the estimated average require-
ment and as such is higher than most people need. RNI
must be interpreted carefully when used in nutrition
education and is not intended to be used by individual
members of the public as a guide.
0005Dietary goals or guidelines, on the other hand, aim
to reduce the chances of developing chronic degenera-
tive diseases and are based on data from animal
experiments, metabolic studies, clinical trials, and epi-
demiological research. They give targets for the popu-
lation to aim at for some future time. The first set of
dietary goalswas published inSweden in 1968. The UK
has published its own goals. Nutrition goals were in-
cluded in the Health of the Nation White Paper (1992).
Further goals were included in the Department of
Health’s report in 1994 from the Committee on Med-
ical Aspects of Food Policy (COMA) on diet and car-
diovascular disease. The World Health Organization
(WHO) hasalso published population nutrient goals in
1990. These are recommended for use in all parts of the
world and have been expressed in absolute terms
rather than increases or decreases in existing nutrient
intake. The desirable change will then vary with the
population. For example, in some developing coun-
tries the goal for fat intake (lower limit) suggests the
need to increase average intakes slightly. Conversely,
for most industrialized countries a reduced fat intake is
desirable. Table 1 summarizes the COMA, Health of
the Nation, and WHO nutrient goals.
0006The recommendations are based on the best avail-
able evidence and may need to be changed in future.
For example, in the future they may need to address
optimal nutritional status.
Assessing Adequate Nutritional Status
0007In order to advise the community we need to know
what the community is already eating. The nutritional
status of the community can be defined as the presence
or absence of diet-related diseases and is related to the
health and well-being of the community. There is no
simple or single way to measure it so that information
has to be gathered from many sources.
Food and Nutrient Supply
0008National level Information on national food avail-
ability is collected annually by many governments in
the form of food balance sheets. The Food and Agri-
culture Organization (FAO) collects and publishes
1568 COMMUNITY NUTRITION
these statistics. It lists the total quantity of different
foods available for consumption in a country during a
specified time (usually one year). Data are limited
since there is no information available about sub-
groups of the population by region, ethnicity, age,
or socioeconomic level. Its accuracy is variable,
especially for areas with subsistence farming.
0009 Food balance sheets can be used to assess available
energy and nutrient intakes per capita. Comparing
changes over years can indicate trends towards or
away from national food security.
0010 Household level The National Food Survey carried
out by the UK Ministry of Agriculture, Fisheries and
Food (MAFF) assesses trends in food supplies and, by
inference, the food eaten. Nutrient intake can be calcu-
lated from these data. It records food purchased rather
than food eaten and does not distinguish between the
intakes of men, women, and children, nor does it in-
clude alcohol, candies (sweets), and soft drinks.
0011 As shown in Table 2, the National Food Survey is
particularly useful for assessing trends in food and
nutrient intake. In general, the food supply was con-
sistent with the amounts recommended to cover the
needs of most of the population.
0012 Itemized till receipts have also been shown to be
a good reflector of energy and fat intake in the
household in families which purchase the majority
of their food at supermarkets.
0013Individual level Assessing diet at the individual level
is usually done by survey. These use several different
methods such as a weighed intake, dietary recall or
record, or a food frequency questionnaire. Attempts
have been made to validate the resulting nutrient levels
by measuring biological markers. Surveys may look at
a representative sample of the population or a particu-
lar at-risk group. The UK government has commis-
sioned a series of regular surveys known as the
National Diet and Nutrition Surveys. The first one of
British adults was published in 1990. It aimed to re-
cruit a nationally representative sample of adults aged
16–64 living in private households in the UK to inform
food and health policy development and evaluation.
Subsequent surveys have studied preschool children,
the elderly, and young people. A second national
survey of adults is currently underway.
Anthropometric Measurements
0014Weight and height can be used to assess the level of
malnutrition or obesity by comparison with reference
data. Height can give evidence of past chronic malnu-
trition, whereas weight is more useful in assessing
recent nutritional experience. Overweight or obesity
tbl0001 Table 1 Comparison of dietary goals from the World Health Organization (WHO), Committee on Medical Aspects of Food Policy
(COMA), and Department of Health, Health of the Nation
WHO COMA Health of the Nation
goals by 2005
Dietary reference
value
a
Lower Upper
Total energy (MJ)
b
Maintain desirable body weight # Obesity –
Males to no more than 6% men 10.6
c
Females to no more than 8% women 8.1
Total fat 15 30 # to about 35% #by 12%, to no more than 35% 33 (35)
d
Saturated 0 10 #to no more than 10% # by 35%, to no more than 11% 10 (11)
d
Polyunsaturated 3 7 n-6 PUFA: no further
" n-3 PUFA: " from 0.1 to 0.2 g day
1
6 (6.5)
d
Cholesterol (mg day
1
) 0 300 No increase
Total carbohydrate (CHO) 55 75 50 47 (50)
d
Complex CHO 50 70 Increase 37 (39)
de
Free sugars 0 10 Increase from fruit and vegetables 10
f
(11)
d
Dietary fiber (g day
1
)27 40 18
g
Protein 10 15
Salt (g day
1
) 6 6 1.6
Alcohol
Units are percent total energy unless otherwise stated.
a
Values are population averages.
b
Energy intake to allow normal growth, pregnancy, lactation, work, activities and to maintain appropriate body reserves. Body mass index (kg m
2
)in
adults ¼ 20–22.
c
Estimated average requirement for men and women, aged 19–49 years, physical activity level 1.4.
d
Figures in brackets represent percentage of food energy.
e
Intrinsic and milk sugars and starch.
f
Nonstarch polysaccharides.
g
Nonmilk extrinsic sugars.
PUFA, polyunsaturated fatty acids.
COMMUNITY NUTRITION 1569
is most practically assessed using the body mass index
(weight in kg/height in m
2
).
Health Statistics
0015 Birth statistics such as neonatal, perinatal, or infant
mortality rates provide indirect information about
the nutritional status of a community, particularly
its disadvantaged groups. Death rates for diseases
which have a nutritional cause can also indicate
nutritional status in the community.
Qualitative Data
0016 Useful information about community food and nutri-
ent patterns can be obtained using qualitative meth-
odologies, such as informal interviews or focus group
discussions. If carefully carried out, these methods
can supplement data collected in the quantitative
methods described above and provide an indepth
understanding of issues such as motivations, food
choices, and particular food habits.
Success Level of General Advice
0017 In order to change a population’s diet, DRVs and
goals must have scientific credibility, political and
technical support, and be recognized as being neces-
sary and acceptable to the consumer. It may take
years to achieve the desirable change.
0018 Is the population meeting the DRVs for the UK popu-
lation? The results of three National Diet and Nutrition
Studies (NDNS) in the British population showing
the percentage who met the UK dietary goals are
presented in Table 3. Most subjects ate more total fat,
saturated fat, and refined sugars and less carbohydrate
and fiber than recommended. A comparison with a sub-
group of 15 000 women from the UK Women’s Cohort
Study shows that in this health-conscious group more
people were able to achieve the dietary goals than in the
earlier NDNS study of adult women.
0019People who consume diets which meet the nutrient
goals are more likely to eat cereals, wholemeal and
brown bread, skimmed or semiskimmed milk, poly-
unsaturated margarine, fruit, vegetables including
potatoes, low-fat meat, and nonfried fish. They also
eat less white bread, butter, margarine, whole milk,
high-fat cheese, eggs, fatty meat, and fried fish than
those who do not meet the goals. To achieve a par-
ticularly healthy diet independent predictive factors
have been found to be spending more money on food,
being a vegetarian, having a higher energy intake, and
a lower body mass index, and being older. Extra costs
of the food may make the cost of a diet which meets
the dietary goals too expensive for the elderly, un-
employed, and low-paid. It is worth noting, however,
that it is possible to consume a diet which meets the
dietary goals which is substantially cheaper than the
average cost of a diet which does not meet the goals.
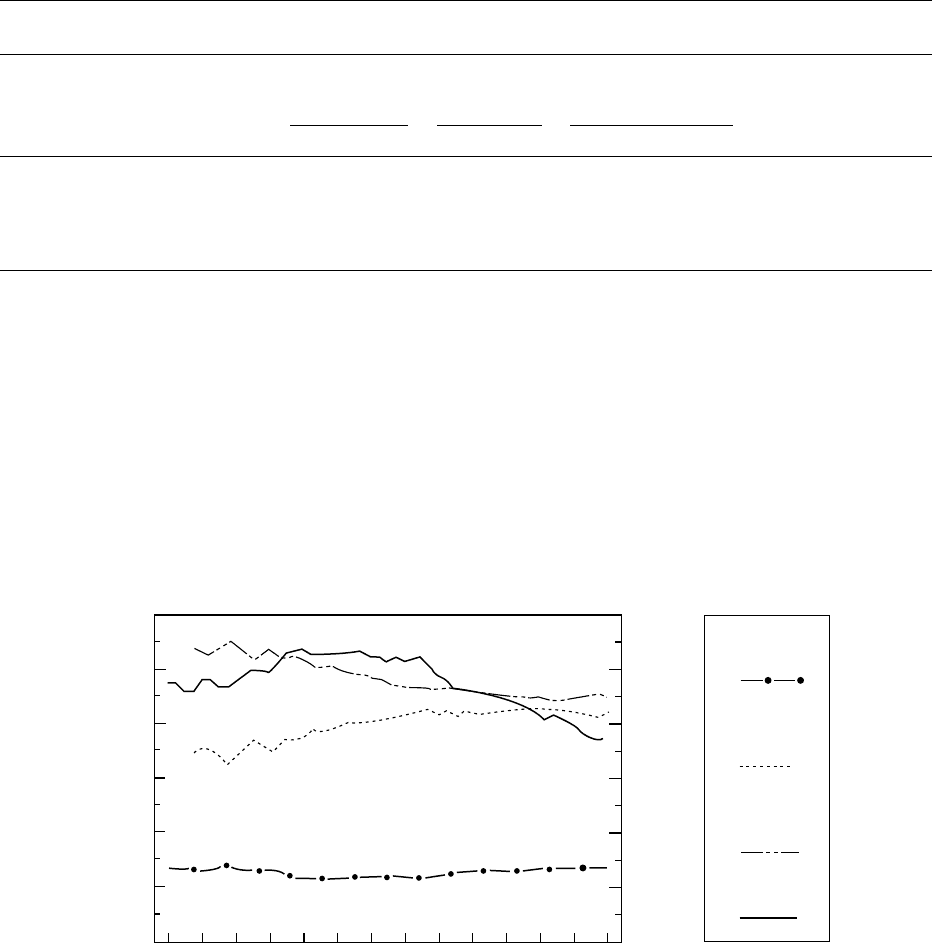
0020The National Food Survey can monitor progress
made by a population towards meeting the goals. It
has been analyzed for a 50-year period from 1940 to
1992. There has been a decline in the percentage of
food energy from carbohydrate and an increase in the
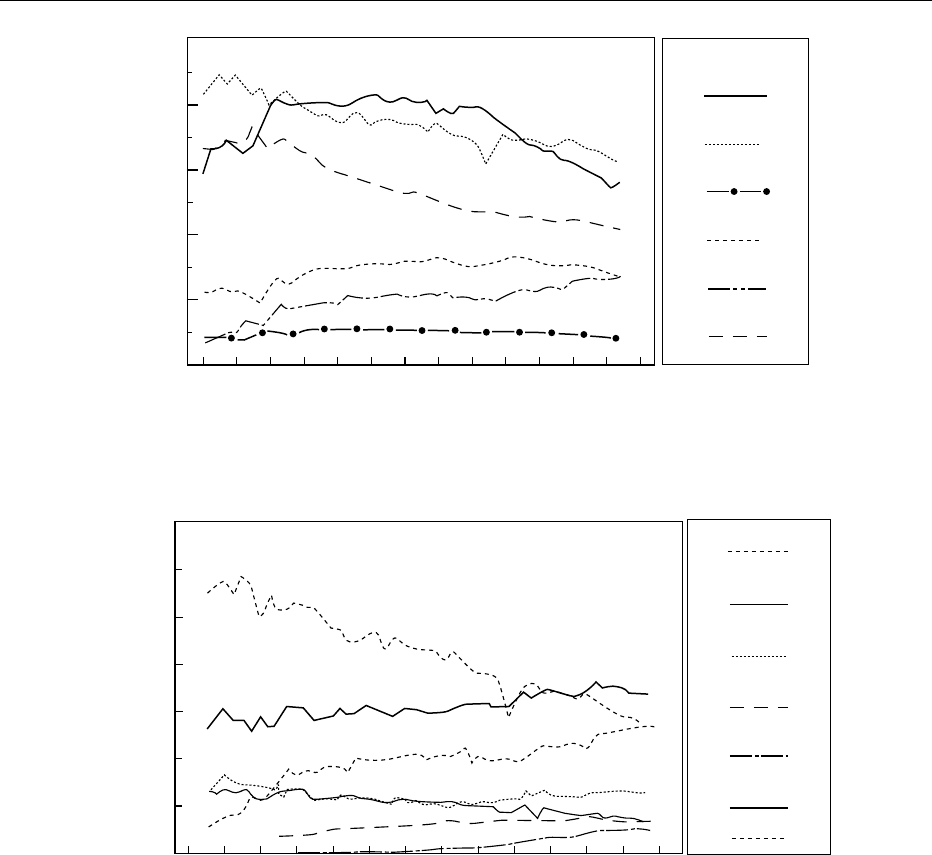
proportion from fat (Figure 1). There have been sub-
stantial changes in the types and quantities of foods
consumed over this period. Bread consumption has
fallen over this period from around 250 g day
1
in
1940 to 110 g day
1
in 1992 (Figure 2). Fresh potato
consumption has also declined, but fruit and other
vegetable consumption has increased from about
200 g day
1
to 300 g day
1
(Figure 3).
Community versus Individual Advice
0021Public health examines risk factors for disease in the
population as a whole and then designs prevention
strategies to reduce them. Meanwhile, the clinician
does the same for the individual patient.
0022Dietary goals for the population are based on iden-
tifying population intakes to maintain health. Health
is defined as a low rate of diet-related diseases. In
assessing whether a population is meeting the dietary
goal it is the entire range of nutrient intake which
matters. If the intake is normally distributed within
the population, then it can be summarized by the aver-
age intake of the population and its standard error.
0023Dietary goals require a population approach to
dietary change leading to a change in the average
intake. This will result in some individuals consuming
more and some less than the stated goal.
tbl0002 Table 2 Nutrient intake from the UK National Food Survey,
expressed as a percentage of recommended intakes current at
the time of the survey
195 8
a
1968
b
1978
b
1988
c
1998
d
Energy (kcal) 104 108 94 91 93
Protein (g) 100 127 121 123 147
Calcium (mg) 107 191 181 159 119
Iron (mg) 115 122 100 102 99
Thiamin (mg) 126 133 125 153 98
Riboflavin (mg) 108 129 138 123 149
Vitamin C (mg) 222 181 188 213 173
Recommended intakes:
a
British Medical Association (1950) Report of the Committee on Nutrition.
London: BMA.
b
Department of Health and Social Security (1969) Recommended Intakes of
Nutrients for the United Kingdom. London: HMSO.
c
Department of Health and Social Security (1979) Recommended Intakes of
Nutrients for the United Kingdom. London: HMSO.
d
Department of Health (1991) Dietary Reference Values for Food Energy and
Nutrients for the United Kingdom: Report of the Panel on Dietary Reference
Values, Committee on Medical Aspects of Food Policy. Report on Health and
Social Subjects 41. London: HMSO. Nutrient values from Ministry of
Agriculture, Fisheries and Food National Food Survey for years stated.
1570 COMMUNITY NUTRITION
Methods of Giving Advice to the
Community
0024 Much can be done to change a population’s diet.
Diets are chosen by individuals; government should
not enforce recommendations concerning diet
and health by restrictive legislation. Legislation
concerning the production and sale of food does
however affect a nation’s diet. An alternative
approach to change is to increase people’s knowledge
and awareness of food and its relationship to
health.
Health Promotion
0025Traditionally, nutrition education campaigns have
involved only one or two sections of the community
such as schools or the media. Success, if it was
measured at all, was limited. A more integrated ap-
proach is to involve as many groups of the community
% Food energy
Energy intake (kcal)
% Food energy
as fat
% Food energy
as protein
% Food energy
as carbohydrate
Energy intake
Year
60
50
40
30
20
10
0
1940 1944 1948 1952 1956 1960 1964 1968 1972 1976 1980 1984 1988 1992
500
1000
1500
2000
2500
3000
fig0001 Figure 1 Trends in proportion of daily energy intake in the British diet derived from carbohydrate, fat, and protein (National Food
Survey 1940–1992). From Department of Health (1994) Nutritional Aspects of Cardiovascular Disease. Report on Health and Social Subjects
46. London: HMSO with permission.
tbl0003 Table 3 Percentage of population meeting dietary goals
Dietary goal NDNS
UK adults
(1986^87)
a
NDNS
1
1
/
2
^4
1
/
2
years
(1992^93)
b
NDNS
65 years þfree-living
(1994^95)
UK Women’s Cohort
(1995)
d
Health-consciouswomen
Men Women Boys Girls Men Women
Total fat 35% food energy 12 15 42
e
42
e
46 41
Saturated fat 15% food energy 11 12 38
f
38
f
59 48 43
g
Total carbohydrate > 50% energy 9 12 60
h
57
h
31 30 54
i
Refined sugars
k
< 10% food energy 12 13 30 36
Fiber > 25 g day
1
45 16 3
l
1
l
32
j
Note that the goals are not meant to refer to children – the preschool age children survey has been included for comparison.
a
Gregory J, Foster K, Tyler H and Wiseman M. (1990) The Dietary and Nutritional Survey of British Adults. London: HMSO.
b
Gregory JR, Collins DL, Davies PSW, Hughes JM and Clarke PC (1995) National Diet and Nutrition Survey: Children aged 1
1
/2 to 4
1
/2 years. London: HMSO.
c
Finch S, Doyle W, Lowe C et al. (1998) National Diet and Nutrition Survey: People Aged 65 Years and Over,vol.1.Report of the Diet and Nutrition Survey.
London: Stationery Office.
d
Cade J, Upmeier H, Calvert C and Greenwood D (1999) Costs of a healthy diet: analysis from the UK Women’s Cohort Study. Public Health Nutrition 2:
505–512.
e
Less than 35% food energy from fat.
f
Less than 15% food energy from saturated fat.
g
0–10% total energy from saturated fatty acids.
h
Greater than or equal to 50% food energy from carbohydrate.
i
50–70% total carbohydrate.
j
27–40 g fiber.
k
Nonmilk extrinsic sugars.
l
20 g day
1
fiber.
NDNS, National Diet and Nutrition Studies.
COMMUNITY NUTRITION 1571
as possible and to use a variety of educational ap-
proaches. For example, Heart-Beat Wales is a health
promotion program which involves public education,
lay groups, schools, factories, retailers, and others.
Look After Your Heart is a multidisciplinary govern-
ment-backed campaign to reduce risk factors for cor-
onary heart disease. Evaluating the success of these
campaigns in terms of reduction of deaths from heart
disease is difficult. With regard to lowering fat intake,
general recommendations to the public without
individual dietary counseling are not very effective.
Despite educational campaigns to lower fat intake,
the level of saturated fat intake in Europe remains
considerably higher than desired.
0026Knowledge of the health risks of a food does not
inevitably lead to a change in its consumption. Why
people eat what they do is determined by a number of
factors; the health effects of a food may only have a
minor influence. Understanding these factors involves
the application of psychological models such as the
Theory of Planned Behavior or the Stages of Change
model. These models explore issues such as beliefs
about food and motivations for changing intakes.
Health education can change consumers’ purchasing
and eating habits. For example, the national pro-
motion of low-fat milk immediately increased its
consumption by 20%. Leaflets are often used, but
are ineffective with mass distribution.
Year
g day
−1
350
200
250
300
150
100
50
0
1940 1944 1948 1952 1956 1960 1964 1968 1972 1976 1980 1984 1988 1992
Fresh potatoes
Fresh green
vegetables
Other fresh
vegetables
Canned
vegetables
Frozen
Total vegetables
Total fruit
excluding potatoes
vegetables
fig0003 Figure 3 Trends in consumption of vegetables and fruit. From Department of Health (1994) Nutritional Aspects of Cardiovascular Dis-
ease. Report on Health and Social Subjects 46. London: HMSO with permission.
Year
g day
−1
500
400
300
200
100
0
1940 1944 1948 1952 1956 1960 1964 1968 1972 1976 1980 1984 1988 1992
Vegetables
Fats and oils
Total liquid milk
Meats
Fruit
Bread and cereals
fig0002 Figure 2 Consumption of selected foods. From Department of Health (1994) Nutritional Aspects of Cardiovascular Disease. Report on
Health and Social Subjects 46. London: HMSO with permission.
1572 COMMUNITY NUTRITION

0027 The media can have an important influence on
choice of foods consumed. This has been demon-
strated recently by the concerns over new-variant
Creutzfelt–Jakob syndrome from infected beef and
unknown risks associated with genetically modified
foods. Media reports have raised awareness of these
issues and people have altered their food intake pat-
terns, although there is no evidence to suggest that
these changes have been detrimental to overall nutri-
tional status.
Health Professionals
0028 General practitioners are encouraged to provide
health promotion, but have little training in nutrition.
Patients are rarely referred to a dietitian; the practice
nurse often provides most of the advice. Dietary
advice provided by untrained members of the primary
health care team can be misleading. Community diet-
itians can provide group-based training and educa-
tion. The UK Nutrition Society is now recognizing a
group of nutritionists with experience in community
nutrition and awarding an accreditation in public
health nutrition.
0029 Most district health authorities have their own
food and health policies which are often limited to
measures within their own services. Potential con-
tributors to these policies are groups within the com-
munity such as local shopkeepers, industry, and trade
unions. Health action zones have been set up to
address inequalities in health in the community.
Some have incorporated nutrition and access to food
as priorities.
Food Labeling
0030 Food should be appropriately and comprehensibly
labeled to aid consumer choice. As yet, there is no
standard format for labels. The format for nutrition
labeling of foods and food claims is regulated by
Codex Alimentarius, or the food code. This is a global
reference point and deals with creating food standards.
Nutrition labeling is often difficult to understand. Sup-
plying the consumer with nutrition information
through the internet or in-store computer terminals
as well as highlighting the most important information
may solve the problem of demands for both more and
understandable information.
Web-based Resources
0031 Knowledge of nutrition and health can be acquired
from the internet. Recent figures suggest that around
16 million people have access to the internet in the UK.
This figure is increasing. It is important for sites to
be rated in terms of content, credibility, and usability.
A number of sites are on the fringe of conventional
nutrition and may be promoting information which is
unhelpful or confusing. NHS Direct has been set up to
provide telephone or web-based health advice and
includes a nutrition component.
Reaching Vulnerable Groups
0032Nutrition advice should take account of the special
needs of particular subgroups, who may be vulner-
able to malnutrition due to their physiological
requirements, their cultural traditions, or their
economic problems.
Babies and Young Children
0033The health professions have a role in promoting
breast-feeding and the preparation of culturally ac-
ceptable and appropriate weaning foods. In the UK,
in order to meet the current dietary goals the diet is
likely to increase in bulk and so reduce energy density.
It is important to maintain adequate energy intakes
by not changing babies on to low-fat milks too early.
Children in lone-parent families tend to have lower
carotene and vitamin C intakes than other children.
Growth monitoring, particularly in developing coun-
tries, can be used to detect growth faltering. Remedial
action can then be taken.
Adolescents
0034On the whole this group is adequately nourished.
There is some concern, however, at the low levels of
iron intake in teenage girls. Adolescents on slimming
diets may be at risk of low intakes of some micro-
nutrients. Appropriate nutrition education at school,
backed up with the provision of healthy school meals,
may help to encourage suitable nutritional habits in
this group.
Pregnancy and Lactation
0035Most pregnant and lactating women in the UK con-
sume an adequate diet. This is, however, a time when
women come into contact with health care services
and may be open to nutrition education. Young girls
and other women at risk of having a low-birth-weight
baby should have particular attention paid to their
dietary intake. Periconceptual folate supplements are
recommended to prevent neural tube defects.
Elderly
0036The current dietary goals are appropriate for the
elderly. Energy intakes tend to decrease with increas-
ing age and there is a need for the elderly to consume
diets with an increased nutrient density. Health
professionals and other carers need to be aware of
the potential for the elderly to be consuming an
inadequate diet. The NDNS for people aged 65 and
over found that intakes of vitamin D, Mg, K, and Cu
COMMUNITY NUTRITION 1573

were low. A substantial proportion of people living in
institutions had low biochemical status indices for
vitamin C, Fe, and folate.
Low-income Groups
0037 Families on a low income and those living in tempor-
ary accommodation may find it difficult to eat a diet
which meets the recommendations. There is particu-
lar concern for people living in socially disadvantaged
areas since there is a greater risk of birth abnormal-
ities and a higher incidence of diseases such as coron-
ary heart disease and cancer in the adult population.
Ethnic Groups
0038 Many aspects of different ethnic dietary patterns will
promote health, such as high fruit or vegetable intakes.
Some ethnic groups, however, also consume diets
which are characterized by a high fat intake and
certain groups have a higher prevalence of obesity,
diabetes, and coronary heart disease. In some com-
munities women and children may be at risk of
vitamin D deficiency. Culturally acceptable nutrition
education needs to be in a form that can be under-
stood by the whole community. Personal intervention
by a trained member of the local community may give
the best results.
See also: Adolescents; Dietary Reference Values;
Elderly: Nutritional Status; Epidemiology; Ethnic
Foods; Food Labeling (Labelling): Applications;
Infants: Nutritional Requirements; Lactation: Human
Milk: Composition and Nutritional Value; Pregnancy:
Metabolic Adaptations and Nutritional Requirements
Further Reading
Committee on Medical Aspects of Food Policy (1994) Nu-
tritional Aspects of Cardiovascular Disease. Report on
Health and Social Subjects 46. London: HMSO.
Department of Health (1991) Dietary Reference Values for
Food Energy and Nutrients for the United Kingdom:
Report of the Panel on Dietary Reference Values, Com-
mittee on Medical Aspects of Food Policy. Report on
Health and Social Subjects 41. London: HMSO.
Department of Health (1992) The Health of the Nation: A
Strategy for Health in England. London: HMSO.
Finch S, Doyle W, Lowe C et al. (1998) National Diet and
Nutrition Survey: People aged 65 years and over, vol. 1.
Report of the Diet and Nutrition Survey. London:
Stationery Office.
Gregory J, Foster K, Tyler H and Wiseman M (1990) The
Dietary and Nutritional Survey of British Adults.
London: HMSO.
Gregory JR, Collins DL, Davies PSW, Hughes JM and
Clarke PC (1995) National Diet and Nutrition Survey:
Children aged 1½ to 4½ years. London: HMSO.
Ministry of Agriculture, Fisheries and Food (1999) National
Food Survey 1998. London: Stationery Office.
World Health Organization (1990) Diet, Nutrition and the
Prevention of Chronic Diseases. Technical Report Series
797. Geneva: World Health Organization.
CONDENSED MILK
H J Hess, Nestec Ltd, Vevey, Switzerland
This article is reproduced from Encyclopaedia of Food Science,
Food Technology and Nutrition, Copyright 1993, Academic Press.
Background
0001 Industrial production for both sweetened and
unsweetened condensed milk started around the
middle of the nineteenth century. However at the
beginning of the nineteenth century, food scientists
in Europe, mainly in France and England, and in the
USA had been working on the possibility of preserv-
ing milk as a concentrated liquid. Both products have
their industrial roots in the USA.
0002 The first sweetened condensed milk in hermetically
sealed cans was manufactured and sold in 1856 by
Gail Borden in the USA. The business grew rapidly
and spread to Europe by 1866 where a sweetened
condensed milk factory was set up in Cham, Switzer-
land, by Charles A. Page, a US consul assigned to the
country. The rapid success of this Swiss-based com-
pany within Europe led eventually to an expansion
of its manufacturing facilities in the USA. This organ-
ization, registered as the Anglo-Swiss Condensed
Milk Company, sold its US interest in 1902 to a
company established and registered at the end
of the nineteenth century as the Borden Condensed
Milk Company. In 1904, the remaining European
interests of the Anglo-Swiss Company merged with
Henry Nestle
´
, of Vevey, Switzerland, who also
manufactured this product. The new company was
called the Nestle
´
-Anglo-Swiss Condensed Milk
Company.
0003Until the early 1880s, unsweetened condensed milk
was also produced and was sold open in the market
1574 CONDENSED MILK

due to the lack of knowledge and success of long-life
preservation at that time.
0004 The basic process for preservation of unsweetened
condensed milk by heat sterilization was conceived by
John B. Meyenberg in 1882, a Swiss citizen, and an
employee of the Anglo-Swiss Condensed Milk Com-
pany. The idea of preserving milk without the add-
ition of sugar was made possible by his invention of a
revolving sterilizer working with steam under pres-
sure. Lacking sufficient support from his company
to continue his work, he migrated, in 1884, to the
USA and also obtained a patent for his invention in
that country. In 1885, Mr Meyenberg was cofounder
of the Helvetia Milk Condensing Company in the
State of Illinois, and during the same year, he achieved
the first successful manufacture of unsweetened
condensed milk. The name of this product was
changed to evaporated milk for a clearer distinction
from sweetened condensed milk, a situation that
prevails today.
0005 The initial phase of commercial production of
both products was hampered by various problems
and quality defects. Only at the beginning of the
twentieth century were constant quality standards
reached.
Definition of Products
Sweetened Condensed Milk
0006 Sweetened condensed milk is made by the addition
of sugar to whole milk and the removal of water
from the milk to about one-half of its original
volume. The product is canned or packaged in
other containers without sterilization, with the
sugar acting as a preservative. International standards
prescribe:
.
0007 a minimum milk fat content of 8%;
.
0008 a minimum milk solids content of 28%.
The minimum sugar content is often not specified
precisely but should be sufficient to avoid spoilage.
0009 Permitted stabilizers are usually specified as
sodium, potassium, and calcium salts of:
.
0010 hydrochloric acid;
.
0011 citric acid;
.
0012 carbonic acid;
.
0013 orthophosphoric acid;
.
0014 polyphosphoric acid.
0015 The name of the product may be:
.
0016 sweetened condensed milk;
.
0017 sweetened condensed whole milk; or
.
0018 sweetened full-cream condensed milk.
0019Legislation in some countries requires a somewhat
higher milk solids and fat content, usually 9% milk
fat and 31% total milk solids. However, there are also
provisions for skimmed sweetened condensed milk
with a milk solids content up to 24% and low-fat
compositions, in principle, of 4% fat and 24% total
milk solids.
0020Frequently, this product is fortified by the addition
of vitamins, mainly A, D
3
, and B
1
.(See Food Fortifi-
cation.)
Evaporated Milk
0021Evaporated milk is made by removal or evaporation
of water from milk but without the addition of sugar
or any other preservative material. The canned
product is heat-sterilized at 118–122
C for several
minutes. The product also may be packed in any
other sterilizable container.
0022International standards prescribe:
.
0023a minimum milk fat content of 7.5%;
.
0024a minimum milk solids content of 25.0%.
0025Permitted stabilizers are usually specified as
sodium, potassium, and calcium salts of:
.
0026hydrochloric acid;
.
0027citric acid;
.
0028carbonic acid;
.
0029orthophosphoric acid;
.
0030polyphosphoric acid.
In addition, some legislation permits the addition of
carrageenan up to 150 p.p.m.
0031The main name of the product is:
.
0032evaporated milk;
.
0033evaporated full-cream milk; or
.
0034unsweetened condensed full-cream milk.
0035Legislation in some countries requires a somewhat
higher fat and milk solids content, up to 9 and 31%,
respectively. However, there are also provisions for
either skimmed or low-fat evaporated milks:
.
0036skimmed evaporated milk with a minimum of 20%
milk solids;
.
0037low-fat evaporated milks, 4 or even 2% milk fat
and a milk solids content of 20–24%.
0038Fortification with vitamins of either or both A or
D
3
is common practice.
Recombined Milk Products
0039Sweetened condensed milk and evaporated milk are
often recombined in countries outside the traditional
dairy belt. (See Recombined and Filled Milks.)
0040For recombining, imported skim milk powder and
anhydrous milk fat are used to make up the milk
CONDENSED MILK 1575