Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


1104 Section XIV • Gynecology
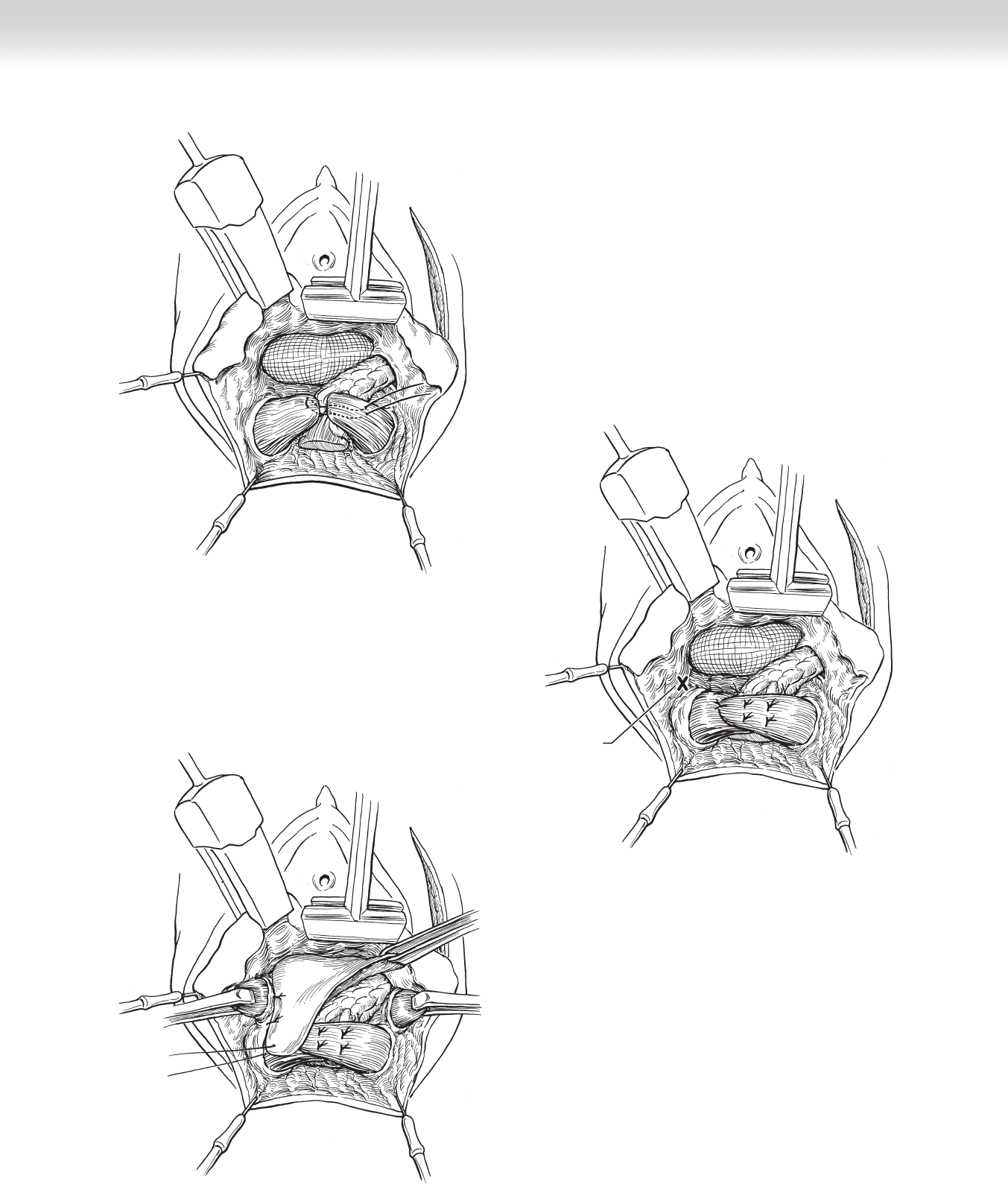
◆ The rectovaginal fascia is sutured to the center of the perineal body (Figures 99-19
and 99-20).
◆ The transverse perineal and bulbocavernosus (also called bulbospongiosus) muscles join the
anal sphincter and rectovaginal septum at the perineal body.
◆ If these muscles are not inextricably bound together, they may be joined end-to-end. If
there is excessive perineal laxity, the perineal muscles may also be overlapped, but such
overlap may require extensive lateral dissection of the transverse perineal muscles toward
the ischial tuberosities (Figure 99-21).
CHAPTER 99 • Repair of Rectovaginal Fistulae 1105
FIGURE 99 –19
Incise for transverse
perineal muscle
FIGURE 99 –20
FIGURE 99 –21

1106 Section XIV • Gynecology
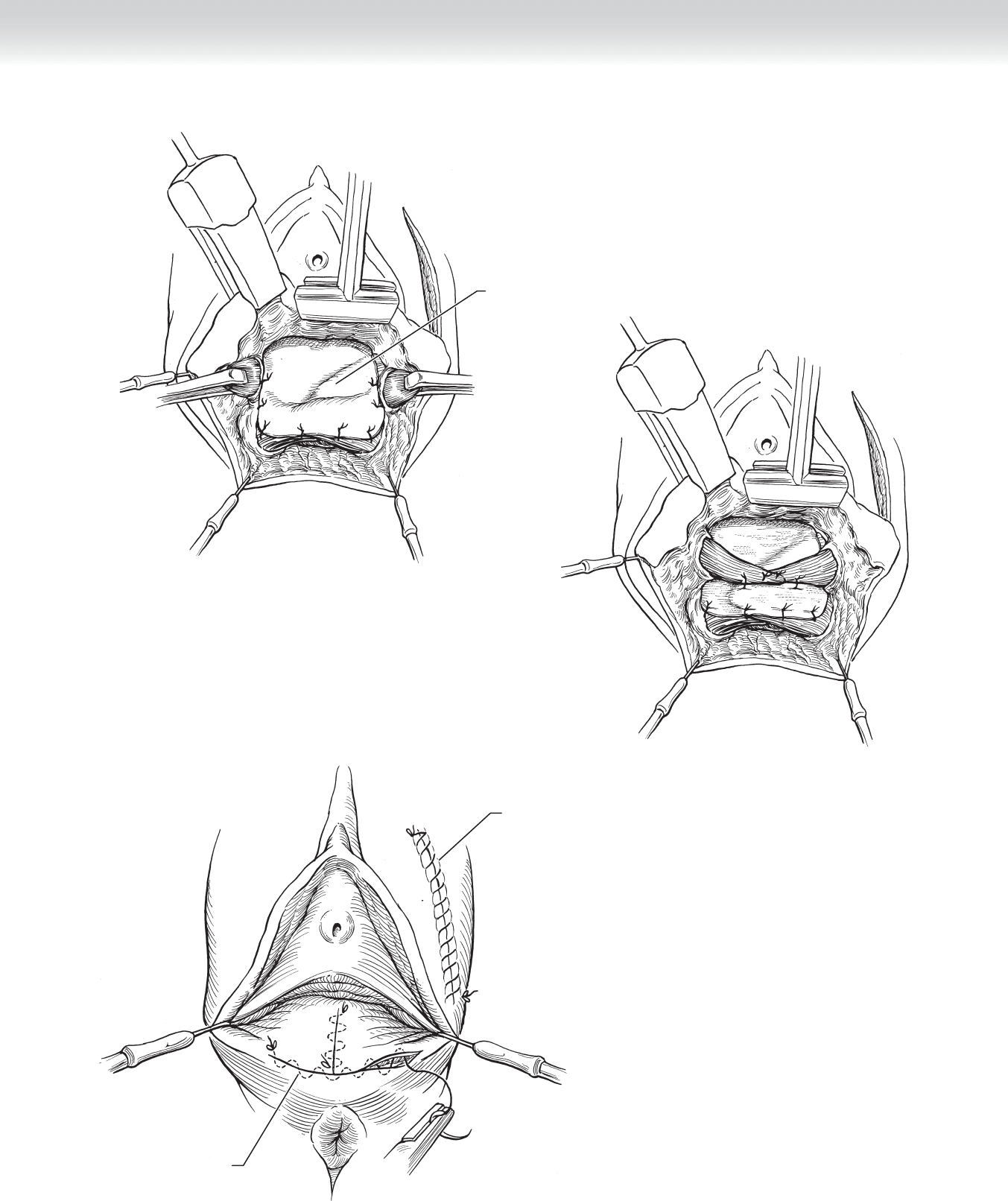
◆ A 00 or 000 rapid absorbable suture is used to close the vaginal mucosa and perineal skin
(Figures 99-22 through 99-24).
STEP 4: POSTOPERATIVE CARE
◆ The most common short-term complication is urinary retention, so a urinary catheter may
be necessary until the normal micturition refl ex recovers.
◆ Postoperative management consists of careful perineal hygiene and stool softeners.
◆ Excessive antibiotic use in the absence of infection may lead to diarrhea and impaired
wound healing of the rectal mucosal suture line, in addition to the increased risk of infec-
tion with resistant organisms.
◆ Although perineal skin breakdown is common, it does not seem to affect the ultimate
success of the repair.
STEP 5: PEARLS AND PITFALLS
◆ Long-term functional outcome of overlapping anal sphincteroplasty may be disappointing,
with anal continence rates as low as 50%.
◆ Patients should be counseled that restoration of anatomy does not guarantee restoration of
function.
CHAPTER 99 • Repair of Rectovaginal Fistulae 1107
Rectovaginal fascia
FIGURE 99 –22
FIGURE 99 –24
Subcuticular suture
Continuous suture
FIGURE 99 –23

1108 Section XIV • Gynecology
SELECTED REFERENCES
1. Martius H: Die Gynäkologischen Operationen. Leipzig, Georg Thieme, 1949.
2. Hankins GDV, Hauth JC, Gilstrap LC, et al: Early repair of episiotomy dehiscence. Obstet Gynecol
1990;75:48-51.
3. Mengert WF, Fish SA: Anterior rectal wall advancement. Technique for repair of complete perineal
laceration and rectovaginal fi stula. Obstet Gynecol 1955;3:262-267.
4. Noble GH: A new operation for complete laceration of the perineum designed for the purpose of
eliminating danger of infection from the rectum. Trans Am Gynecol Soc 1902;27:357-363.
5. Sultan AH, Kahn MA: Perineal and primary anal sphincter repairs. In Cardozo L, Staskin D (eds):
Textbook of Female Urology and Urogynecology. London, Isis Medical Media, 2001, pp 628-642.

1110
STEP 1: SURGICAL ANATOMY
◆ A comprehensive understanding of the location of the lymph nodes in relation to the chest
wall musculature, fascial boundaries, lymphatic drainage pathways, vascular supply
supporting structures, and innervation of surrounding tissues is essential for appropriate
surgical management.
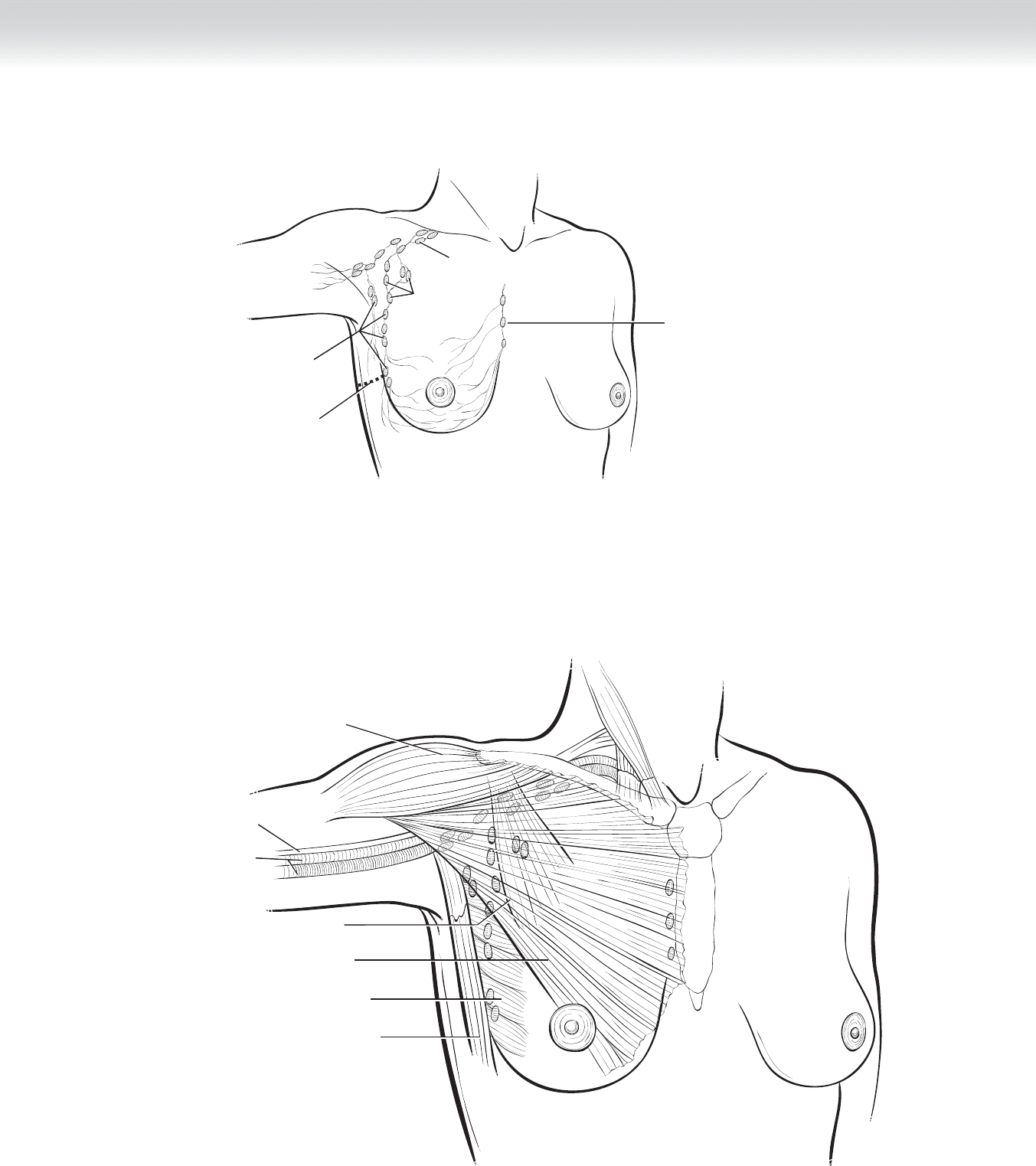
◆ Figure 100-1 demonstrates the breast gland and its rich intraparenchymal lymph channels
coursing toward the deeper major nodal reservoirs.
◆ Figure 100-2 illustrates the supporting structure of the chest wall musculature, the major
blood vessels, and the location of the lymph nodes.
◆ The lymph nodes lateral to the pectoralis minor muscle constitute level I nodes; those im-
mediately beneath the muscle, the level II nodes; and those medial to it, level III nodes. The
interpectoral nodes (Rotter’s nodes) are located between the pectoralis major and minor
muscles and are part of level III nodes. Internal mammary nodes are located medially along
internal mammary vessels beneath the sternum. Unnamed intramammary lymph nodes can
be present in all quadrants of the breast.
◆ The boundaries of the axilla are defi ned by the pectoral minor muscle medially, the latissi-
mus dorsi muscle laterally, the axillary vein superiorly, and the subscapularis and teres
major muscles posteriorly.
◆ Axillary lymph node dissection removes the lymph nodes lateral to the pectoralis minor
muscle (level I nodes) and posterior to the pectoralis minor muscle (level II nodes). In
some cases, the lymph nodes medial to the pectoralis (level III nodes) and the interpectoral
nodes (Rotter’s nodes) are also removed.
◆ Other types of lymph node procedures or treatments include the following:
◆ Sentinel node biopsy
◆ Lymph node sampling
◆ Excision of a palpable lymph node
◆ Axillary irradiation
CHAPTER
100
Axillary Node Dissection
Baiba J. Grube
CHAPTER 100 • Axillary Node Dissection 1111
Line of incision
Level II nodes
Level III nodes
Level I nodes
Internal mammary gland
FIGURE 100–1
Median nerve
Axillary artery and
vein
Latissimus dorsi muscle
Serratus anterior muscle
Pectoralis major muscle
Deltoid muscle
Pectoralis minor muscle
FIGURE 100–2

1112 Section XV • Miscellaneous Procedures
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Selection of a surgical option for local control of breast cancer is a complex decision based
on the tumor features, the body habitus, and individual choice. Interdisciplinary discussion
with radiation oncologists, medical oncologists, and plastic surgeons, in addition to the
oncologic surgeon, provides a comprehensive understanding of the options available to the
patient.
◆ Lumpectomy with axillary lymph node dissection may be an alternative procedure to a
modifi ed radical mastectomy for many women, especially in the current era of mammo-
graphic screening and identifi cation of early stage disease and with the use of induction
chemotherapy to reduce the size of the primary tumor.
◆ Discussion of the planned procedure with the anesthesiologist is critical.
◆ Long-acting paralytic agents should be avoided when an axillary dissection is planned to
detect intact motor nerve function.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The patient is placed in the supine position, close to the edge of the operating table for ease
of exposure of the axilla, with the arm extended on a padded arm board with or without a
wedge. The arm may be prepped out separately and covered in a sterile stockinette to allow
free rotation of the arm medially to relax the pectoralis major and minor muscles.
◆ Many incisions have been used for axillary dissection. The transverse incision approxi-
mately 1 cm below the hair-bearing area extending from the latissimus dorsi to the pectora-
lis major medially results in the most cosmetically attractive incision. Other incisions may
be perpendicular to the axilla or S-shaped incisions.
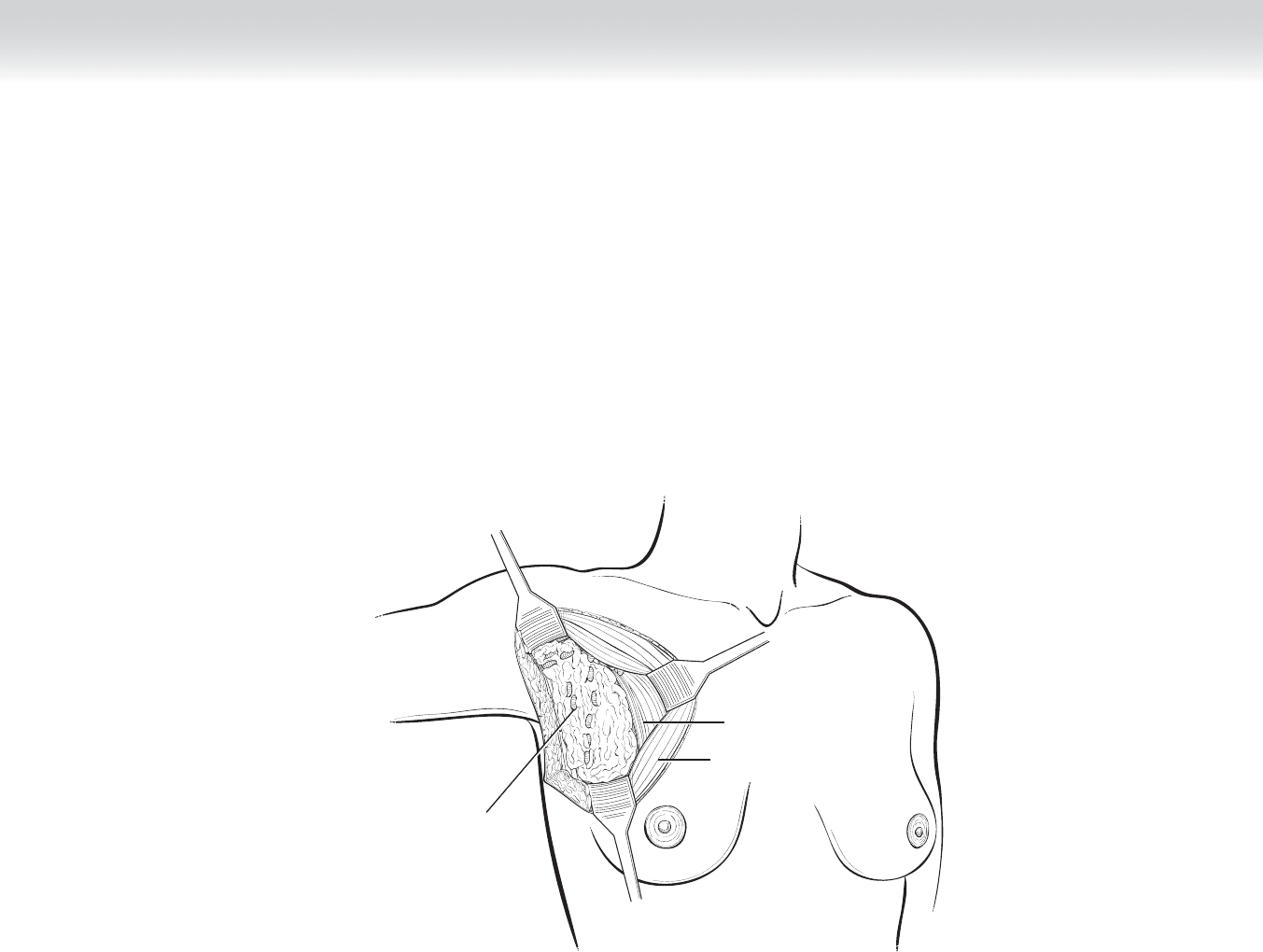
◆ A marking pen is used to draw the planned incision. The skin is incised and extended
through the dermis into the subcutaneous adipose tissue to expose the investing fascia of
the axilla (Figure 100-3). The thickness of the fl aps will vary according to body mass
index. In heavyset individuals, the fl aps will be thick and may cave into the axilla, making
dissection diffi cult. Adequate exposure is essential to avoid injury to important structures.
CHAPTER 100 • Axillary Node Dissection 1113
Pectoralis major muscle
retracted
Pectoralis minor muscle
Axillary fat and
lymph nodes
FIGURE 100–3

1114 Section XV • Miscellaneous Procedures
2. DISSECTION
◆ Dissection is initiated by elevating the skin fl aps with skin hooks or Freeman face lift
retractors with electrocautery.
◆ As the fl aps are elevated, the assistant holds upward tension on the skin fl aps while the
surgeon uses countertraction on the axillary fat pad.
◆ The skin fl aps are raised circumferentially and retracted with medium Richardson retractors
to expose the axillary fat and lymph nodes (see Figure 100-3).
◆ Dissection is initiated along the pectoralis major muscle medially from superior to inferior.
Care must be exercised to avoid injury to the medial anterior thoracic nerve (medial pecto-
ral nerve), which may penetrate both pectoral muscles and emerge medially or may course
along the lateral aspect of the pectoralis minor. Injury to this nerve may lead to atrophy of
part of the pectoralis major muscle.
◆ The fascia along the pectoralis major is incised and retracted medially with a small or
medium Richardson retractor, exposing the underlying pectoralis minor. The clavipectoral
fascia along the pectoralis minor is then incised and the retractor is replaced, exposing the
level II nodes posterior to the pectoralis minor. The arm may now be rotated medially to
take tension off the pectoral muscles and expose the axillary contents. Care must be taken
to avoid traction of the extremity and the brachial plexus in the anesthetized patient.
◆ The inferior refl ection of the axillary fascia is identifi ed, and dissection is continued from
medial to lateral on the serratus anterior muscle to the latissimus dorsi muscle laterally.
◆ Dissection is continued along the lateral aspect of the latissimus dorsi muscle to the level of
its tendinous insertion (Figure 100-4). This marks the location of the overlying axillary
vein. Dissection along the ventral aspect of the latissimus dorsi should be avoided until the
thoracodorsal nerve, artery, and vein are identifi ed, visualized, and maintained in view
during dissection.
◆ Dissection from the tendinous insertion of the latissimus dorsi proceeds medially, inferior to
the axillary vein.
◆ The superior extent of the axillary dissection should begin approximately 5 mm below the
axillary vein to preserve the lymphatics of the arm and reduce the likelihood of upper
extremity lymphedema (see Figure 100-4). This tissue is rich in lymphatics and blood
vessels, which should be ligated with fi ne silk ties or Weck Hemoclips.