Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.


1084 Section XIV • Gynecology
STEP 4: POSTOPERATIVE CARE
◆ Bladder drainage is maintained until the fi rst postoperative day.
◆ Diet is advanced as tolerated.
◆ Early ambulation is encouraged.
STEP 5: PEARLS AND PITFALLS
◆ Avoid suturing through the middle of the uterine pedicle, because a vessel may be easily
pierced, leading to a retroperitoneal hematoma.
◆ In a patient with previous pelvic surgery or history of endometriosis or pelvic infl ammatory
disease, a mechanical bowel preparation should be ordered to prepare for extensive bowel
lysis of adhesions.
◆ Use the appropriate-length instruments and sutures based on the depth of pelvis and weight
of the patient.
SELECTED REFERENCE
1. Rock JA, Jones HW (eds): TeLinde’s Operative Gynecology, 10th ed. Philadelphia, Lippincott Williams &
Wilkins, 2008.
1085
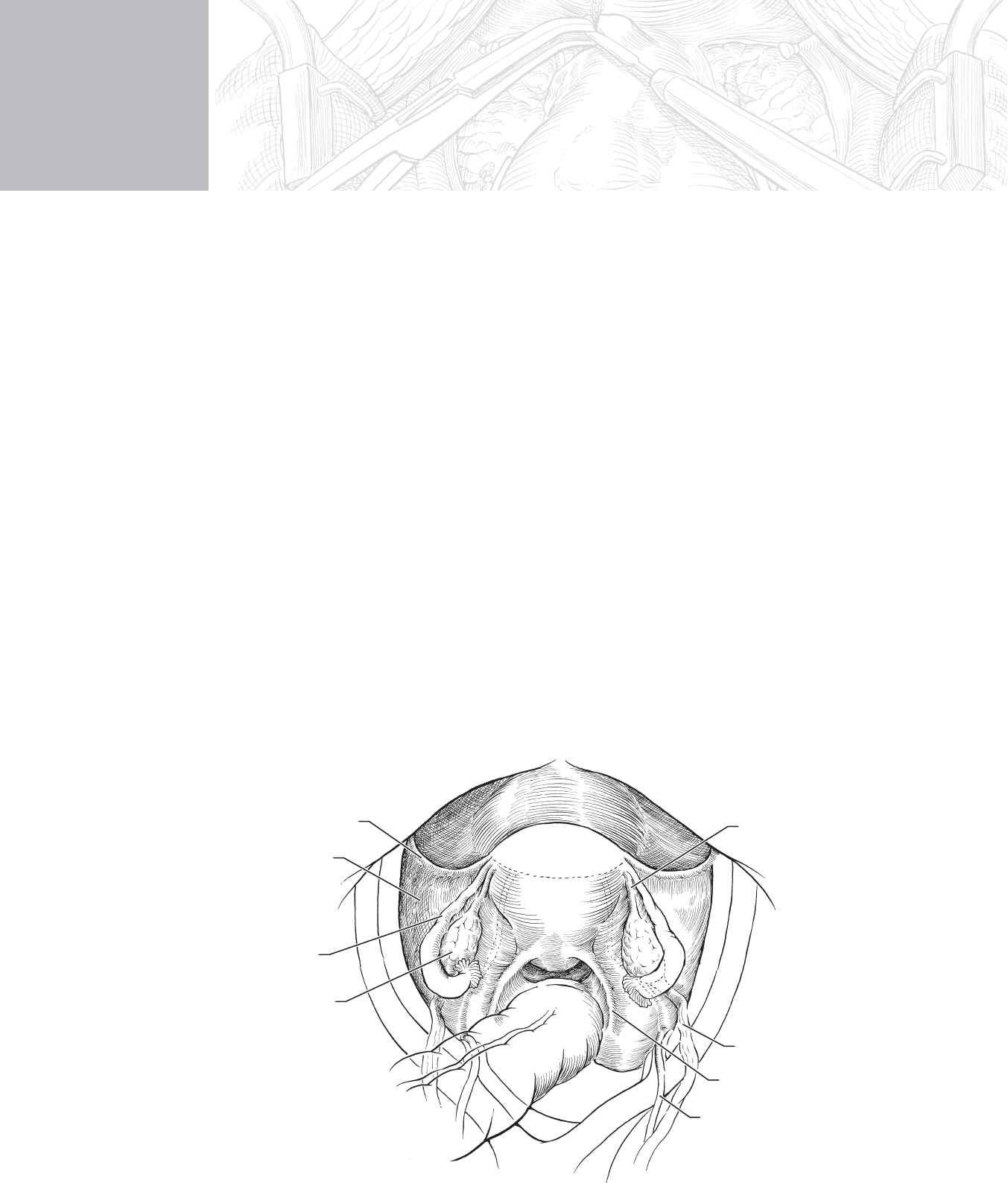
STEP 1: SURGICAL ANATOMY
◆ Figure 98-1 demonstrates the key anatomy of the uterus, fallopian tube, and ovary
(adnexa) as it pertains to the removal of the adnexa.
◆ The infundibulopelvic ligament carries the blood supply to the adnexa.
◆ Round ligaments are insubstantial anterior lateral attachments of the uterine fundus that
help maintain the normal uterine position. They are an important landmark in the open-
ing of the retroperitoneum for identifi cation of the ureters.
◆ Utero-ovarian ligaments connect the uterus to the adnexa.
◆ The ureters cross over the bifurcation of the common iliac arteries and are found inferior
to the infundibulopelvic ligament on the medial leaf of the broad ligament. The ureter
must be identifi ed before ligation of the infundibulopelvic ligament.
CHAPTER
98
Bilateral Salpingo-
Oophorectomy
Concepcion Diaz-Arrastia
Uterosacral
ligament
Infundibulopelvic
ligament
Ligament of
ovary
Uterus
Ovary
Fallopian tube
Round ligament
Broad ligament
Bladder
Bladder
Bladder
Ureter
FIGURE 98 –1

1086 Section XIV • Gynecology
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ The indications for salpingo-oophorectomy include excision of an ovarian mass or ovarian
cancer prophylaxis.
◆ Frozen section surgical consultation should be available for all cases of ovarian mass. If
intraoperative diagnosis of ovarian cancer is made, the surgeon and patient should be
prepared to proceed with ovarian cancer surgical staging or cytoreductive surgery as
indicated.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ In cases of a suspected ovarian mass, a vertical skin incision is recommended to allow for
excellent exposure, as well as the ability to extend the incision to the upper abdomen for
exploration, surgical staging, or cytoreductive surgery.
◆ A transverse Pfannenstiel incision or laparoscopic approach is acceptable for prophylactic
salpingo-oophorectomy. (See Chapter 97 for discussion of transverse incisions.)
2. DISSECTION
◆ The operative fi eld is prepared by placing the patient in Trendelenburg position, inserting
a self-retaining retractor to expose the pelvis, and packing the intestines away from the
operative fi eld with moist laparotomy pads.
◆ The uterus is grasped with atraumatic curved clamps placed on the uterine horns bilaterally
for upward traction.
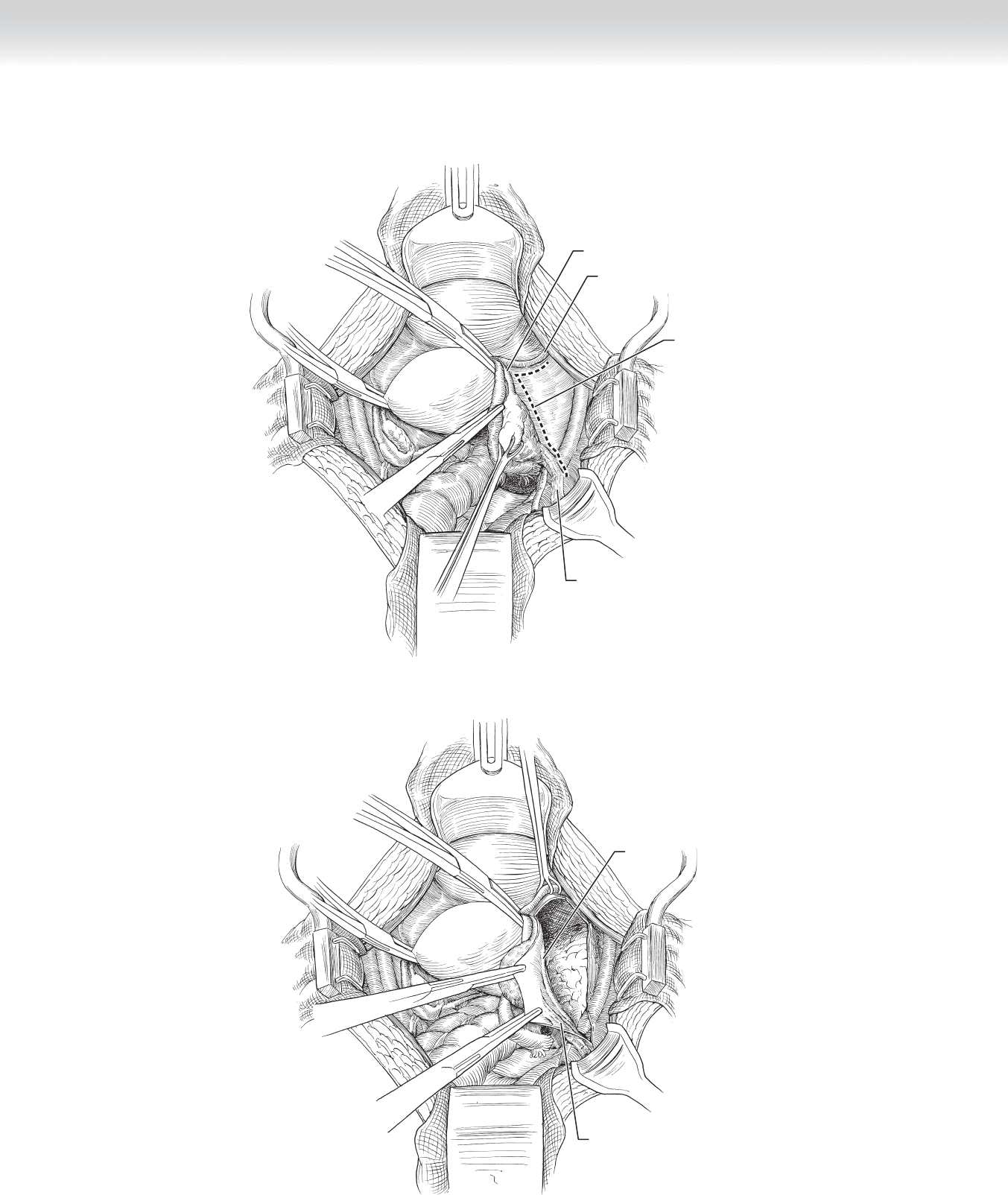
◆ An L-shaped incision is made on the peritoneum of the posterior leaf of the broad ligament,
parallel and posterior to the round ligament and lateral to the infundibulopelvic ligament
(Figure 98-2). This avascular retroperitoneal space is developed by blunt dissection. The
external iliac artery is identifi ed on the lateral leaf, and the ureter is identifi ed on the medial
leaf, inferior to the infundibulopelvic ligament (Figure 98-3).
CHAPTER 98 • Bilateral Salpingo-Oophorectomy 1087
Infundibulopelvic
ligament
Ligament of ovary
Round ligament
Incision through
posterior leaf of
broad ligament
FIGURE 98 –2
Ureter
Infundibulopelvic ligament
FIGURE 98 –3

1088 Section XIV • Gynecology
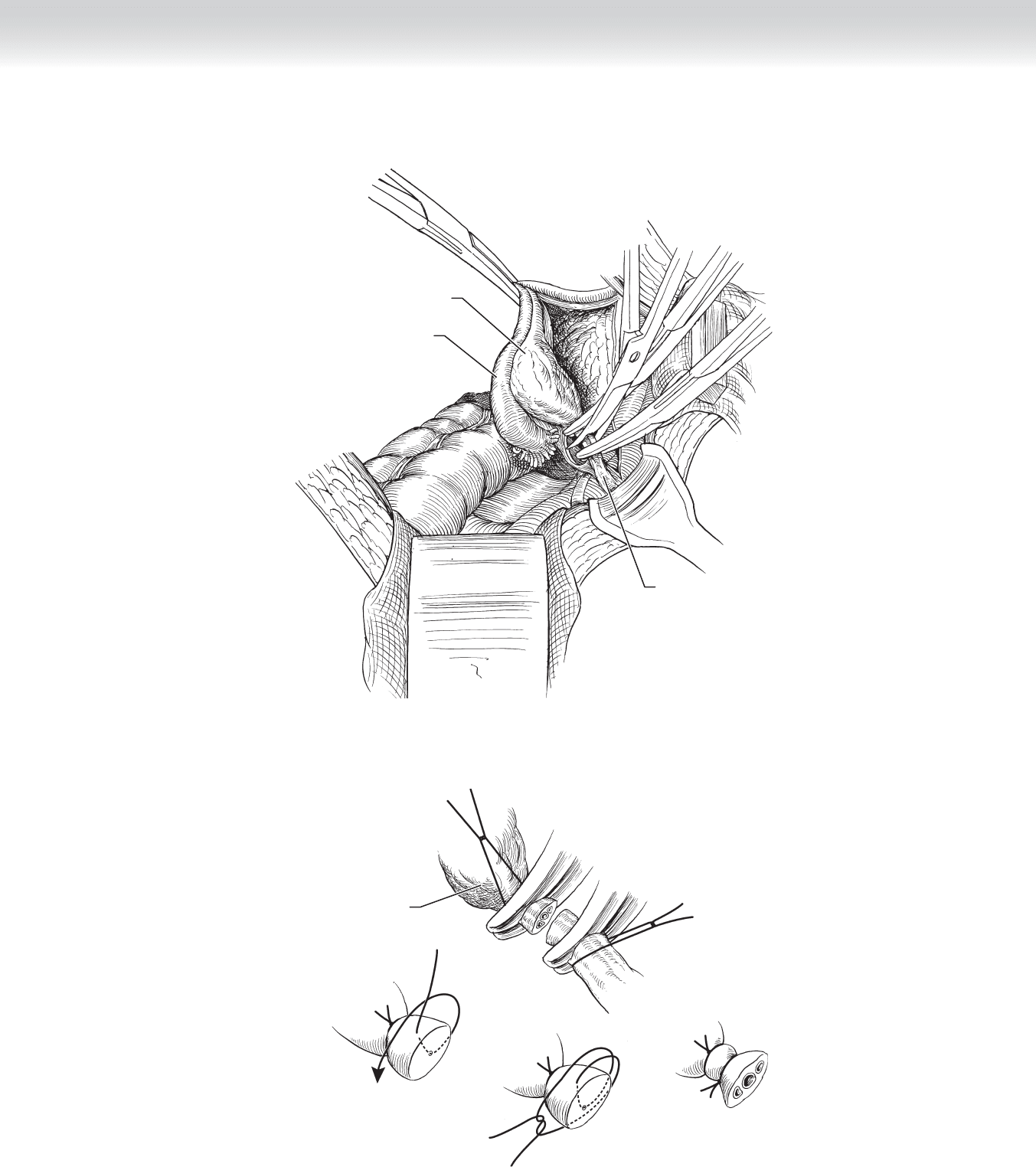
◆ Under visualization of the ureter, the surgeon makes a window in the medial leaf of the
broad ligament, between the vascular infundibulopelvic ligament and the ureter, then
clamps and incises the infundibulopelvic ligament (Figure 98-4).
◆ Because of the vascularity of the infundibulopelvic ligament and the risk of an ascending
retroperitoneal hematoma, the surgeon fi rst ligates the pedicle with a free tie then transfi xes
the pedicle with suture ligation (Figure 98-5).
CHAPTER 98 • Bilateral Salpingo-Oophorectomy 1089
Ovary
FIGURE 98 –5
Ovary
Fallopian tube
Infundibulopelvic ligament
FIGURE 98 –4
1090 Section XIV • Gynecology
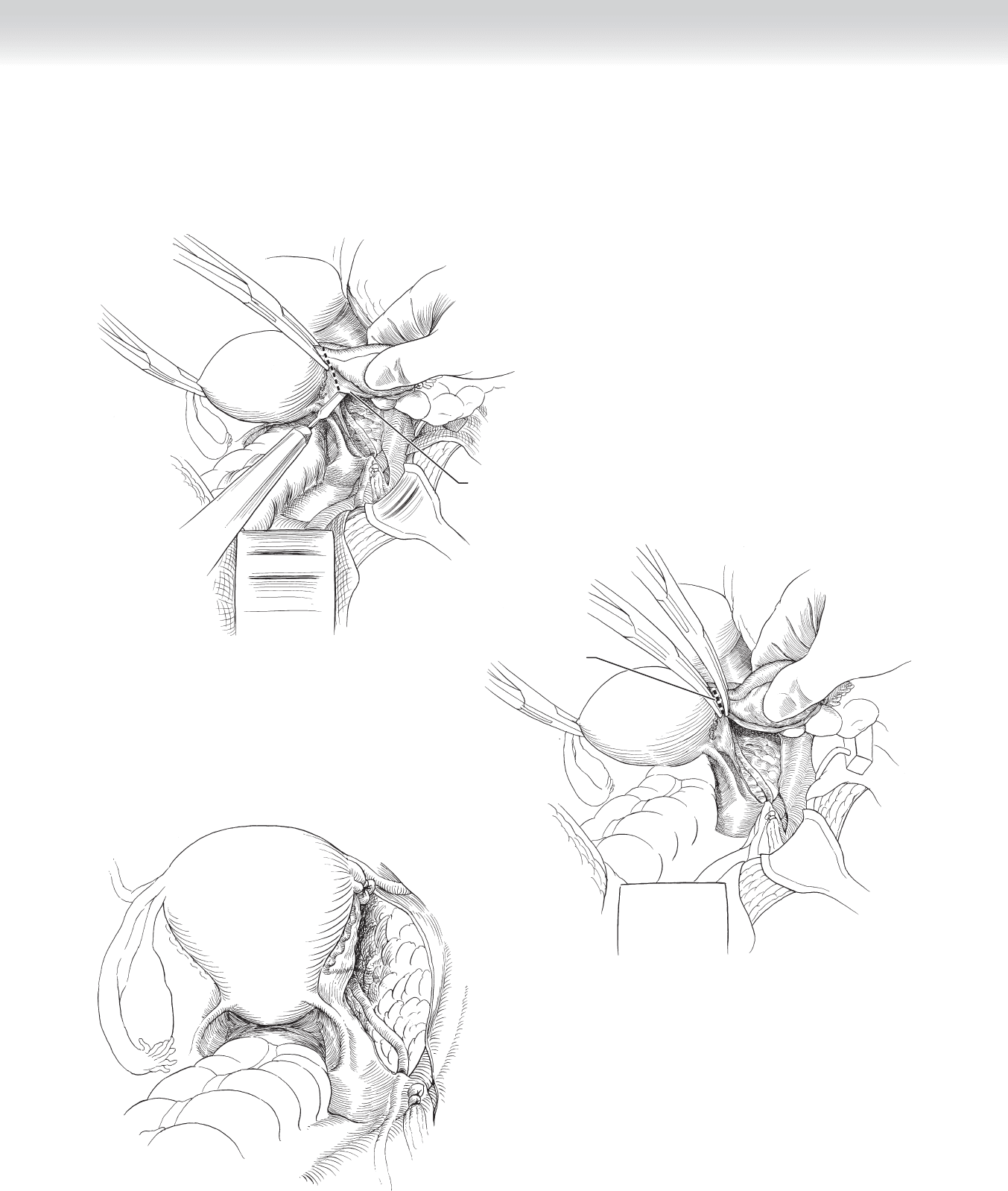
◆ Under full visualization of the ureter, incise the medial leaf of the peritoneum/broad ligament
from the infundibulopelvic pedicle to the uterus (Figure 98-6). Ligate the utero-ovarian liga-
ment, which is the remaining attachment of the adnexa (Figures 98-7 and 98-8).
Posterior leaf
of broad ligament
Dividing fallopian
tube and ligament of
ovary
FIGURE 98 –8
FIGURE 98 –7
FIGURE 98 –6

CHAPTER 98 • Bilateral Salpingo-Oophorectomy 1091
3. CLOSING
◆ The abdominal wall is closed in layers. The anterior rectus fascia is closed in a continuous
mass closure.
STEP 4: POSTOPERATIVE CARE
◆ Bladder drainage is maintained until the fi rst postoperative day.
◆ Diet is advanced as tolerated.
◆ Early ambulation is encouraged.
STEP 5: PEARLS AND PITFALLS
◆ Salpingo-oophorectomy in a menstruating woman will effect a surgical menopause, which
may cause severe hot fl ashes and other sequelae of premature menopause.
◆ Mechanical bowel preparation is advised in patients undergoing surgery for an ovarian
mass.
SELECTED REFERENCE
1. Rock JA, Jones HW (eds): TeLinde’s Operative Gynecology, 10th ed. Philadelphia, Lippincott Williams &
Wilkins, 2008.

1092
STEP 1: SURGICAL ANATOMY
◆ Although rectovaginal fi stulae may spontaneously arise from Crohn’s disease or malignancy,
most cases result from failed obstetric repairs and complications of posterior vaginal
prolapse repair operations.
◆ Successful repair requires a wide enough dissection to obtain a tension-free layered closure
of viable, well-vascularized tissue, using a pedicled Martius bulbocavernosus graft if
necessary.
◆ Although successful early secondary repair has been described, repair after postpartum
dehiscence is traditionally delayed for 3 months to allow maximal reinnervation and
vascularization of the wound.
◆ Numerous failed repairs may require a diverting colostomy before and 3 months following
reoperation to ensure adequate healing.
◆ Fistulae superior to the levator muscles may require an abdominal approach to achieve
adequate mobilization of tissue. In the pre-antibiotic era, the rectal advancement and
vaginal fl ap operations had the advantage of avoiding a suture line in the rectum. However,
the use of these operations may make overlapping the retracted muscle of the anal sphinc-
ter more diffi cult.
◆ Preoperatively, all patients receive a bowel preparation and prophylactic antibiotics.
◆ Infi ltration of the operative fi eld with 20 U of vasopressin in 100 mL of normal saline or a
local anesthetic with epinephrine reduces blood loss and helps hydrodissect scarred tissue
planes.
CHAPTER
99
Repair of Rectovaginal Fistulae
Margie A. Kahn
CHAPTER 99 • Repair of Rectovaginal Fistulae 1093
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Most postpartum fi stulae are accompanied by two quadrant anal sphincter defects identifi -
able by perineal dimples at the 3 o’clock and 9 o’clock positions.
◆ In the worst cases, the vaginal mucosa directly abuts the rectal mucosa. If gross inspection
and palpation are equivocal, endoanal ultrasonography and anorectal manometry may be
used to identify the anatomic and functional signifi cance of the defects. In the following
fi gure, the normal sphincter is on the right.
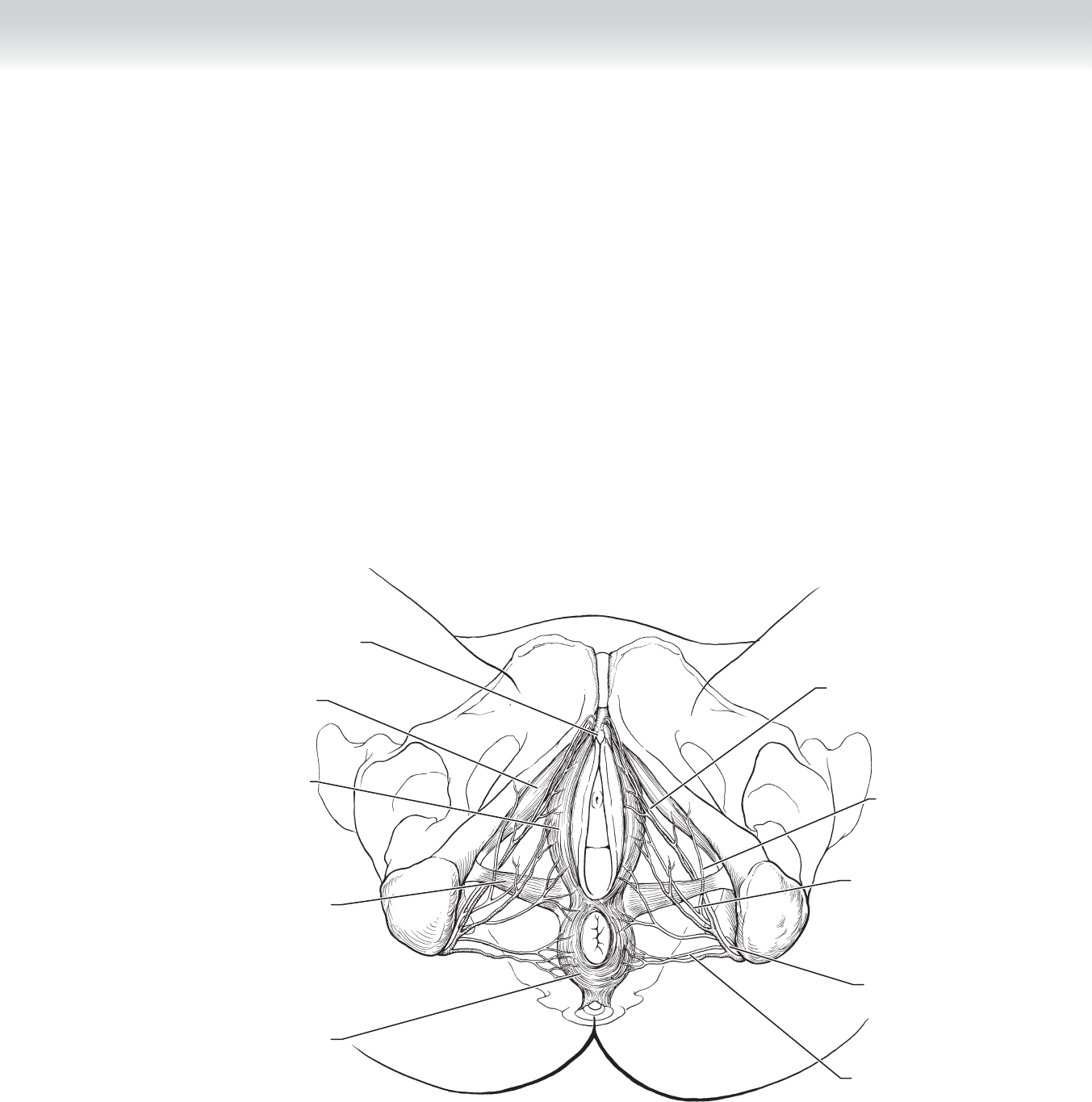
◆ Extensive dissection to achieve anal overlapping sphincteroplasty can interfere with the
neurovascular bundles at the 4 o’clock and 8 o’clock positions (Figure 99-1).
Inferior anal nerve
Superficial perineal
nerve
Pudendal nerve
Deep perineal
nerve
Dorsal nerve of clitoris
Anal sphincter muscle
Transverse perineal
muscle
Clitoris
Bulbocavernosus or
Bulbospongiosus
muscle
Ischiocavernosus
muscle
MC
FIGURE 99 –1