Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

1052 Section XIII • Amputations
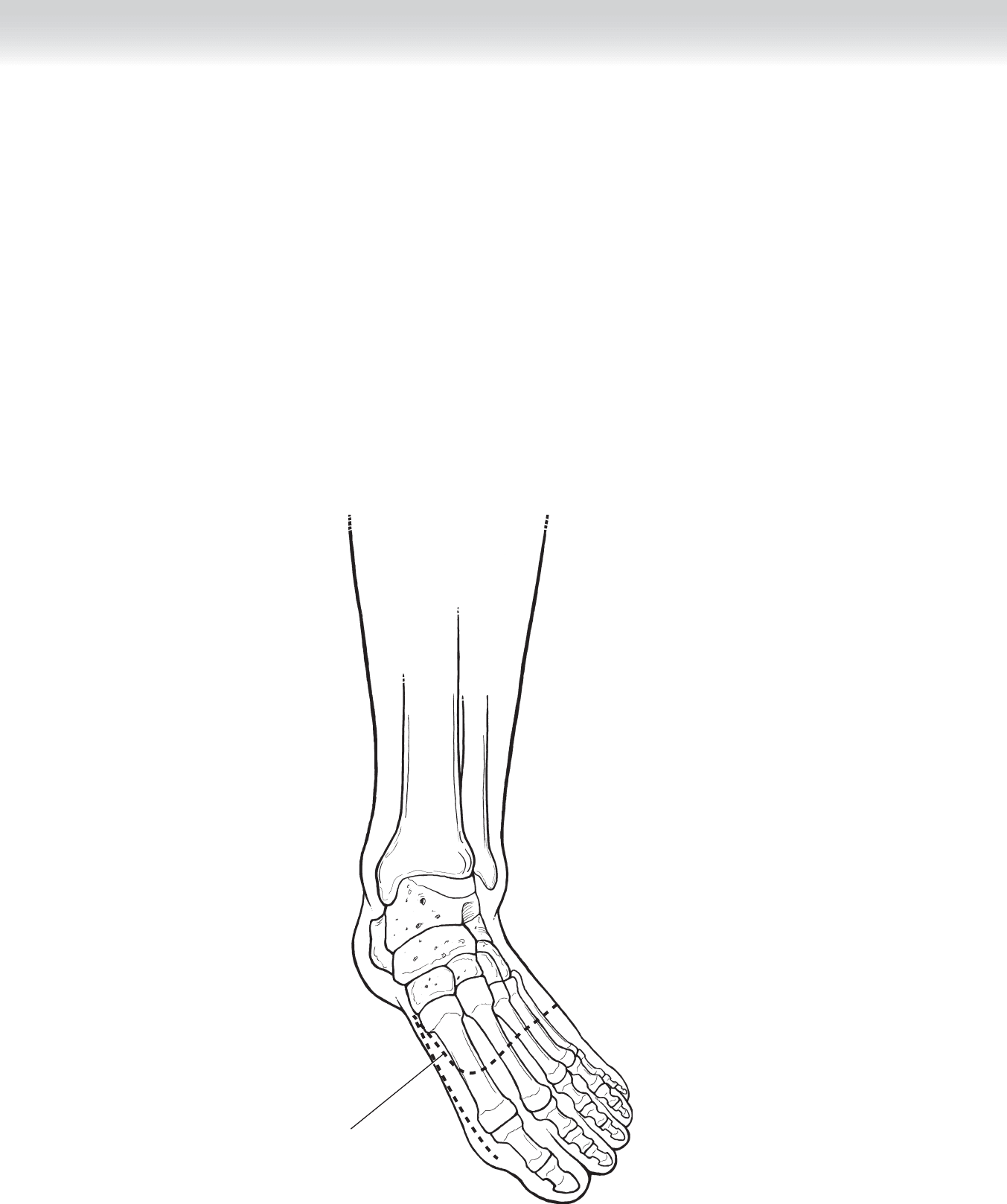
Line of incision
FIGURE 95 –2
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ General, spinal, or regional anesthesia may be selected when appropriate.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ The proposed incision is mapped on the foot. Dorsally, the incision is slightly curved just
distal to the midshaft of the metatarsal bones. The plantar fl ap extends to the metatarsopha-
langeal crease (Figure 95-2).
CHAPTER 95 • Transmetatarsal Amputation 1053
2. DISSECTION
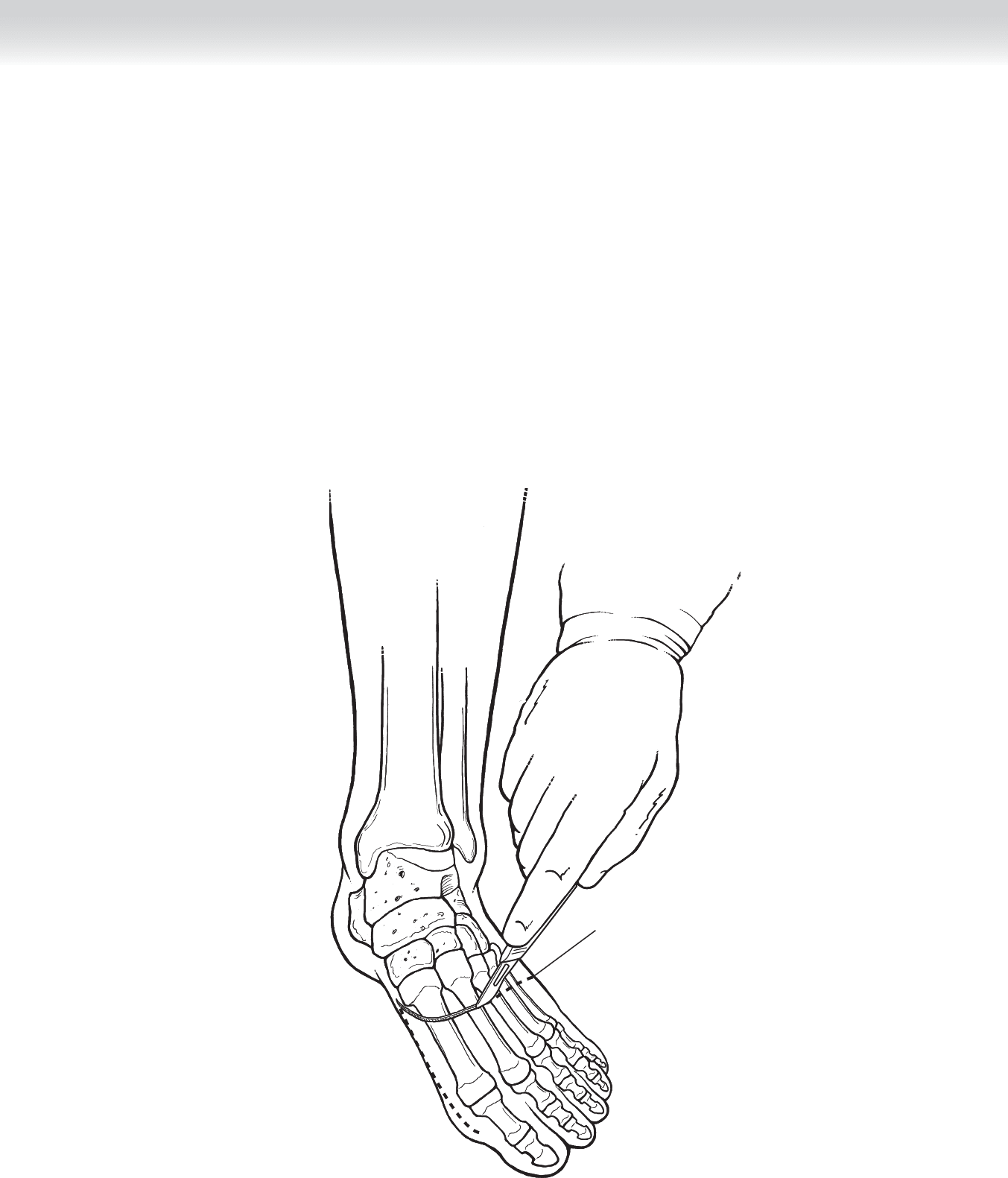
◆ The incision is begun on the dorsal surface of the foot directly down to the level of the
bone without undermining the fl aps. As the medial and lateral extents of the dorsal fl ap are
reached, the plantar incision is begun, leaving an acute angulation to avoid dog ears with
closure. Soft tissue coverage of the metatarsals will be provided by the long plantar fl ap.
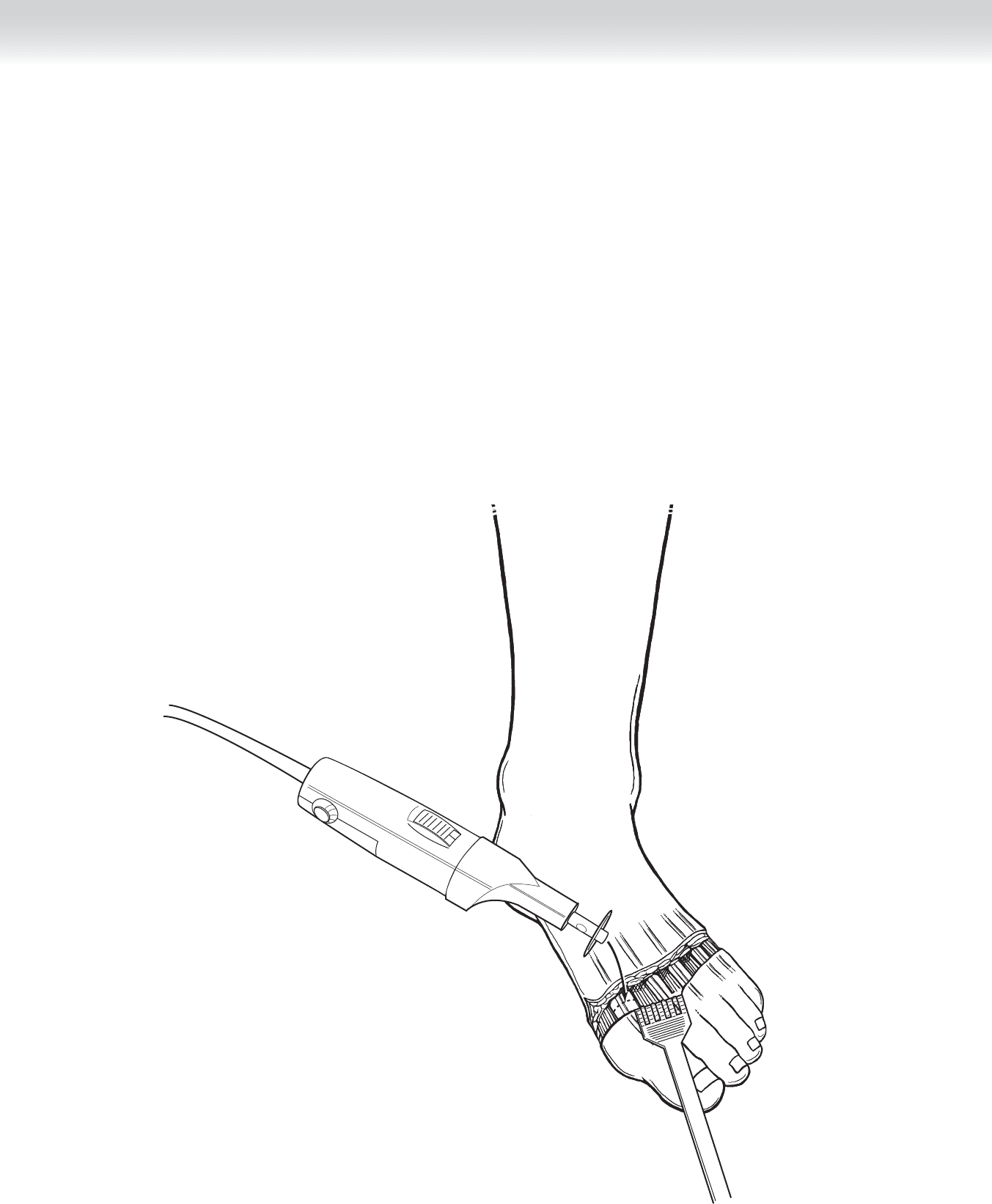
◆ Once hemostasis has been achieved, the small-bladed oscillating saw is used to divide the
metatarsal bones approximately 1 cm proximal to the dorsal skin fl ap, starting with the fi rst
metatarsal (Figure 95-3). The second metatarsal shaft is cut at the same level as the fi rst,
and the remaining metatarsals are cut 3 mm shorter than the fi rst two. The oscillating saw
is used to avoid splintering of the bones. The cut edges are smoothed with a rasp.
Incision through skin
and deep tissue
FIGURE 95 –3
1054 Section XIII • Amputations
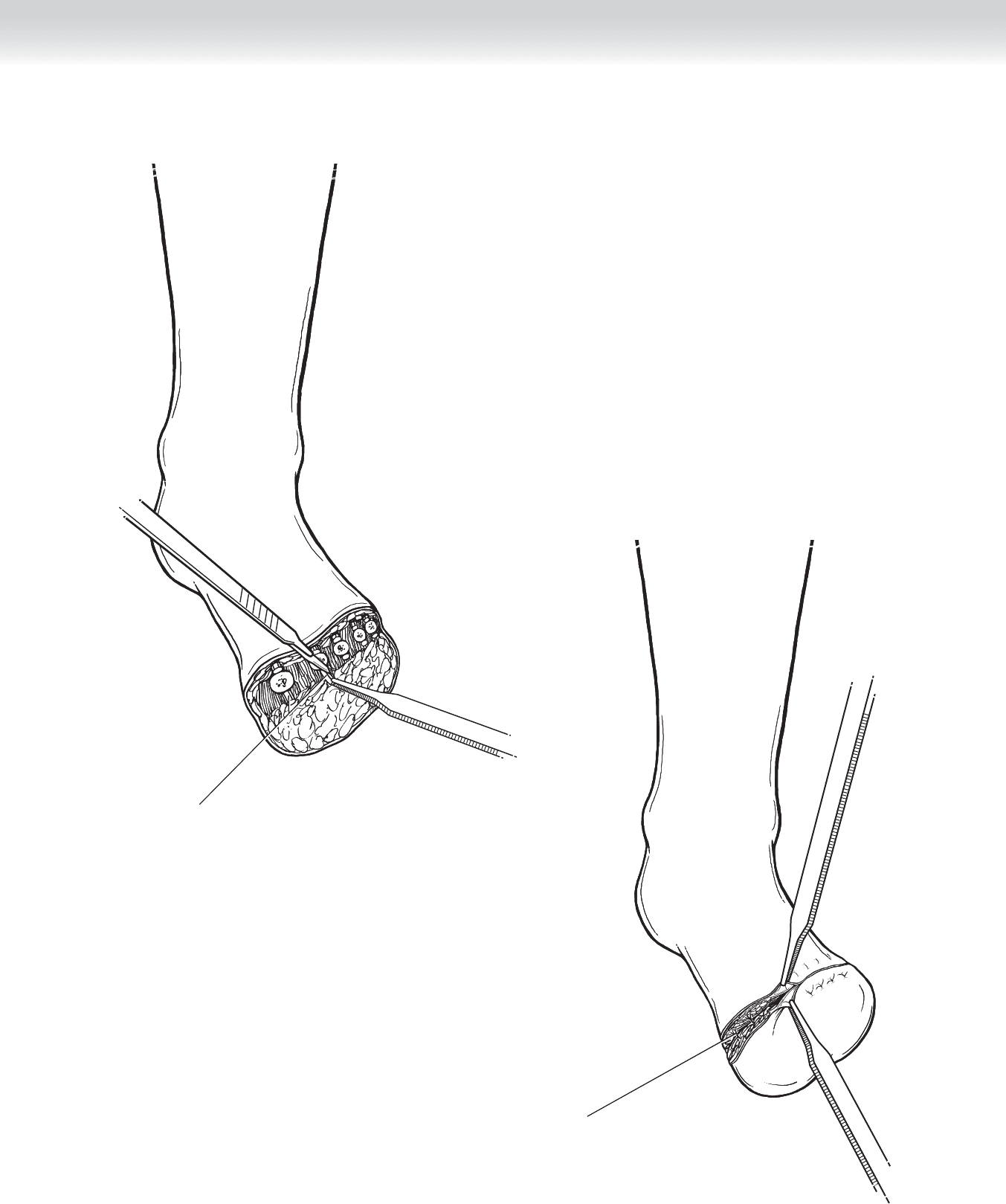
◆ The plantar soft tissues are divided to release the amputated segment. The tendons are
placed on stretch and cut short so that they retract into the stump (Figure 95-4).
◆ Redundant and devitalized soft tissues of the planter fl ap are trimmed and hemostasis is
ensured. An estimation of the tension on the closed fl ap is made, and if necessary, the
metatarsal bones are trimmed further (Figure 95-5).
3. CLOSING
◆ The superfi cial fascia may be approximated with 2-0 interrupted absorbable sutures.
◆ Skin staples or 2-0 vertical mattress permanent sutures are placed to close the wound and
are left in place until complete healing is certain (Figure 95-6).
FIGURE 95 –4
CHAPTER 95 • Transmetatarsal Amputation 1055
Superficial fascia approximated
with interrupted absorbable sutures
Flexor tendons
FIGURE 95 –5
FIGURE 95 –6

1056 Section XIII • Amputations
STEP 4: POSTOPERATIVE CARE
◆ A sturdy dressing such as a well-padded cast will help limit postoperative edema and
protect the stump. The stump should be inspected at least weekly to assess for viability and
infection.
◆ The patient should avoid weight bearing on the extremity until the wound is safely healed.
STEP 5: PEARLS AND PITFALLS
◆ Careful attention to hemostasis, debridement of devitalized tissue, and tension-free closure
will help ensure the optimal outcome.
◆ In the setting of a contaminated wound, the stump may be left open to heal by secondary
intention or subsequent grafting. Premature closure of a contaminated stump will likely
result in further soft tissue loss and necessitate a higher level of amputation.
SELECTED REFERENCES
1. Durham JR, McCoy DM, Sawchuk AP, et al: Open transmetatarsal amputation in the treatment of severe
foot infections. Am J Surg 1989;158:127-130.
2. Dwars BJ, van den Broek TA, Rauwerda JA, Bakker FC: Criteria for reliable selection of the lowest possible
level of amputation in peripheral vascular disease. J Vasc Surg 1992;15:536-542.
3. McKittrick LS, McKittrick JB, Risley TS: Transmetatarsal amputation for infection or gangrene in patients
with diabetes mellitus. Ann Surg 1949;130:826-842.
4. Effeney DJ, Lim RC, Schecter WP: Transmetatarsal amputation. Arch Surg 1977;112:1366-1370.

1057
INDICATION
◆ Hip disarticulation is performed for malignant soft tissue or bony tumors of the proximal
thigh region (below the lesser trochanter of the femur) in which negative margins cannot be
achieved without a less radical operation. Most sarcomas can be treated with limb-sparing
procedures and the use of adjuvant or neoadjuvant therapies. In general, bone and vessels
can be resected and replaced with grafts. Sacrifi ce of a single nerve, either the femoral nerve
or the sciatic nerve, would result in some neuromuscular dysfunction but is preferable to
amputation. This operation may be appropriate in locally recurrent cases of extensive
(unresectable) tumor involvement (usually when adjuvant radiotherapy options have
already been exhausted).
◆ This procedure can also be considered for massive trauma and crush injury to the lower
extremity or following multiple failed vascular procedures and distal amputations.
STEP 1: SURGICAL ANATOMY
◆ See Figure 96-2 for illustration of key anterior structures. See Figures 96-4 and 96-5 for the
posterior lateral anatomy, which must be considered with hip disarticulation.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Magnetic resonance imaging of soft tissue tumors of the proximal thigh can delineate the
extent of tumor involvement relative to muscular compartments, neurovascular bundles,
and bony structures. A bone scan is useful to ensure that the acetabulum and pelvis are
not involved with tumor. A Tru-Cut needle biopsy or an open biopsy should have already
been performed to confi rm the malignant nature of the tumor and the necessity of such a
radical operation.
◆ A complete neurologic examination of the involved extremity may reveal signifi cant loss of
function and intractable pain preoperatively.
◆ General anesthesia is used.
Hip Disarticulation
Celia Chao and Courtney M. Townsend, Jr.
CHAPTER
96
1058 Section XIII • Amputations
STEP 3: OPERATIVE STEPS
1. INCISION
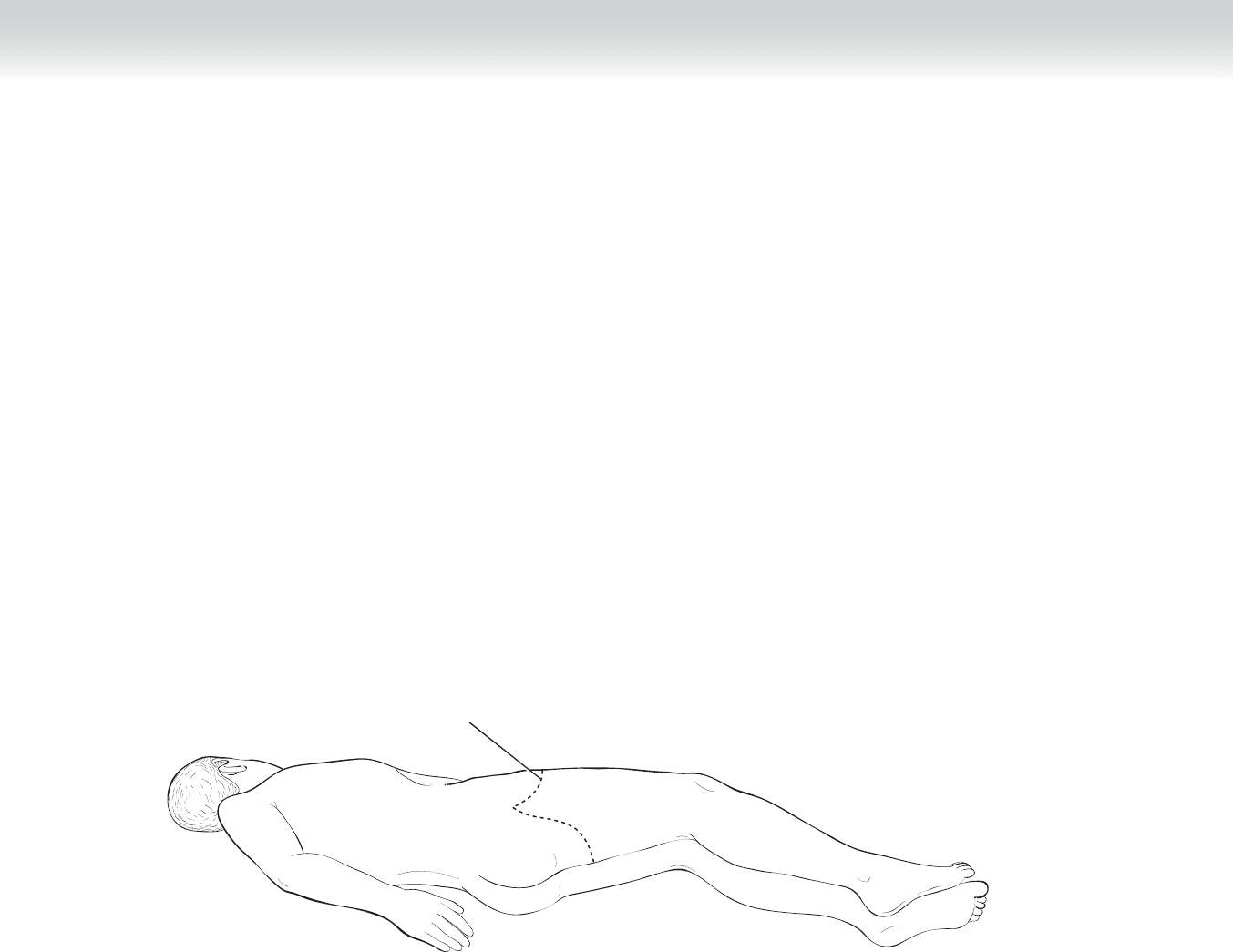
◆ A Foley catheter is placed in the bladder. The patient is positioned in the lateral decubitus
position to provide adequate exposure for both anterior and posterior aspects of the thigh
(Figure 96-1). A bean bag may be used to help maintain this position. The skin is prepped
from midchest down to the toes. The extremity below the thigh can be covered with a
stockinette, such that the entire leg can be manipulated and repositioned intraoperatively to
facilitate the resection.
Incision line
FIGURE 96 –1
CHAPTER 96 • Hip Disarticulation 1059
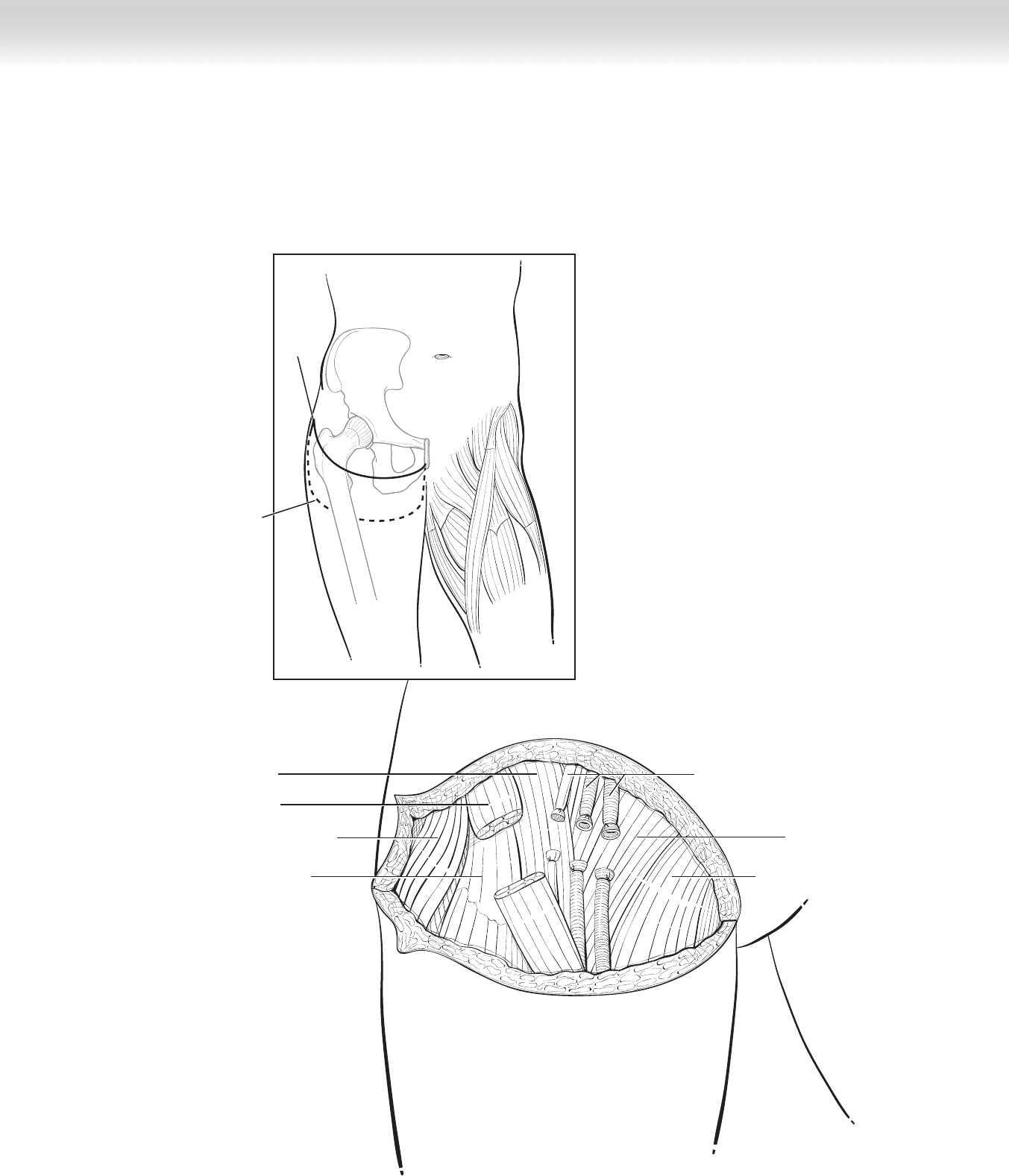
◆ Anteriorly, a skin incision is made approximately 3 cm below the inguinal ligament. The
posterior skin fl ap is much longer. It is approximately 6 to 8 cm below the anterior incision
to facilitate a fi sh-mouth closure at the lateral and medial corners (Figure 96-2; see also
Figure 96-1).
Iliopsoas muscle
Anterior
incision
Posterior
incision
Sartorius muscle
Tensor fasciae latae muscle
Rectus femoris muscle
Pectineus muscle
Femoral nerve, artery, and vein
Adductor longus muscle
FIGURE 96 –2
1060 Section XIII • Amputations
2. DISSECTION
◆ After dissecting past Scarpa’s fascia, the surgeon creates the anterior fl ap. The femoral ves-
sels are identifi ed below the inguinal ligament and are serially divided and suture ligated.
The femoral nerve and the sartorius muscles, lateral to the vessels, are also divided. The
femoral nerve should be on gentle traction and ligated just as it exits the inguinal ligament.
The residual nerve will retract beneath the external oblique aponeurosis. If a neuroma
forms, it should be well away from the weight-bearing portion of the stump. Muscles lateral
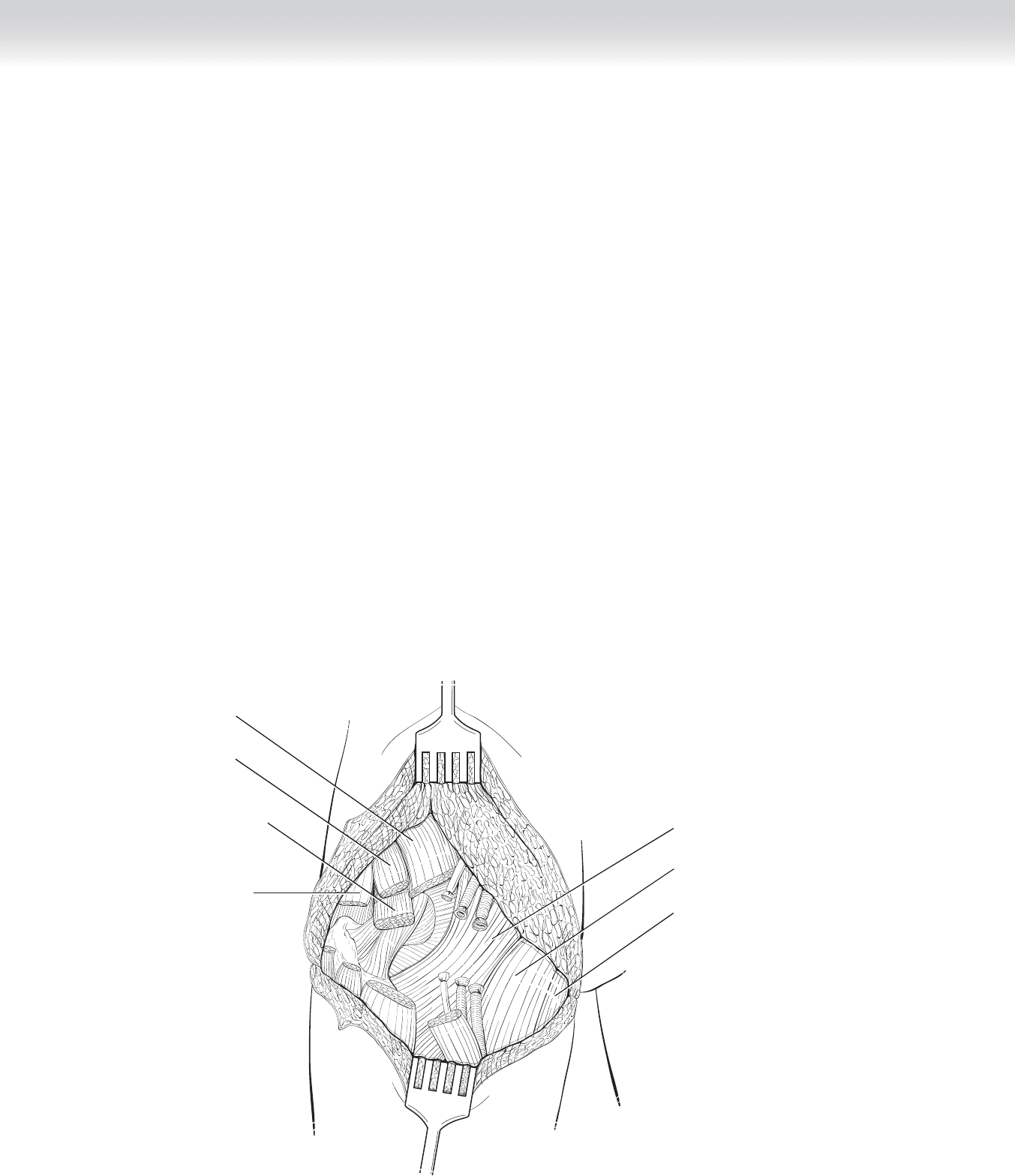
to the vessels are identifi ed and include the iliopsoas and the rectus femoris. The insertion
of the iliopsoas onto the less trochanter is divided with electrocautery, preserving most of
the proximal aspects of the muscle (Figure 96-3).
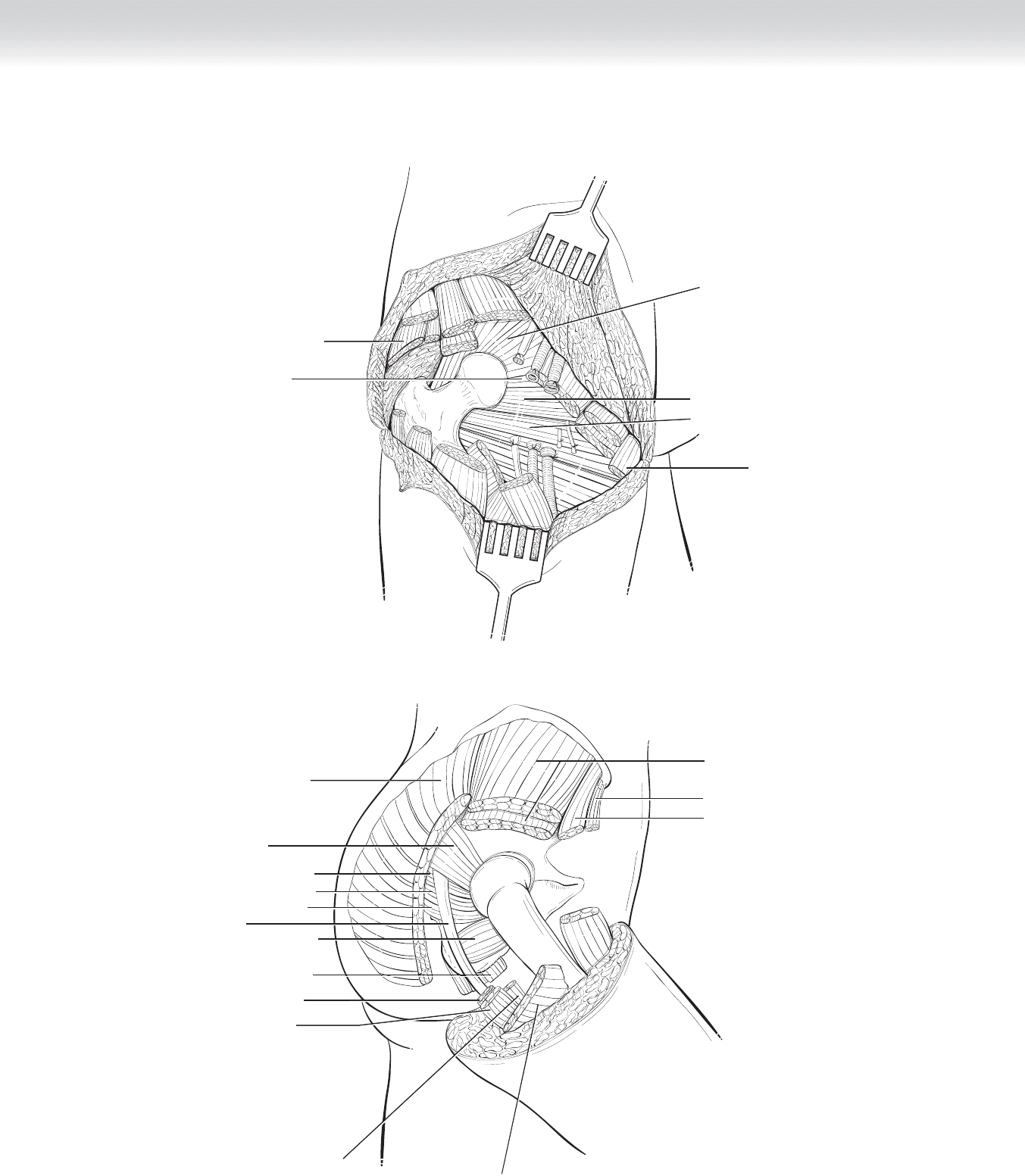
◆ Medially, a fi nger is passed beneath the pectineus muscle, and the muscle can be released
from its origin on the pubis using electrocautery. Continuing medially, the surgeon transects
the adductor magnus and brevis muscles and the gracilis muscles at their origin on the
symphysis pubis, exposing the obturator externus muscle (Figures 96-4 and 96-5).
Beneath the pectineus and adductor muscles, branches of the obturator nerve and vessels
are identifi ed and ligated. The tendinous insertion of the obturator externus muscle is cut
at its insertion into the lesser trochanter.
Sartorius muscle
Iliopsoas muscle
Tensor fasciae
latae muscle
Rectus femoris muscle
Adductor longus muscle
Pectineus muscle
Gracilis muscle
FIGURE 96 –3
CHAPTER 96 • Hip Disarticulation 1061
Gluteus maximus muscle
Gluteus maximus muscle
Gluteus medius muscle and
Gluteus minimus muscle
Sartorius muscle
Sciatic nerve
Inferior gemellus muscle
Quadratus femoris muscle
Biceps femoris muscle
Semimembranosus muscle
Semitendinosus muscle
Adductor magnus muscle
Superior gemellus muscle
Obturator internus muscle
Piriformis muscle
Tensor fasciae latae muscle
FIGURE 96 –5
Gracilis muscle
Piriformis muscle
Gluteus minimus muscle
Gluteus medius muscle
Obturator internus muscle
Superior gemellus muscle
FIGURE 96 –4