Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 92 • Insertion of Peritoneal Venous Shunts 1021
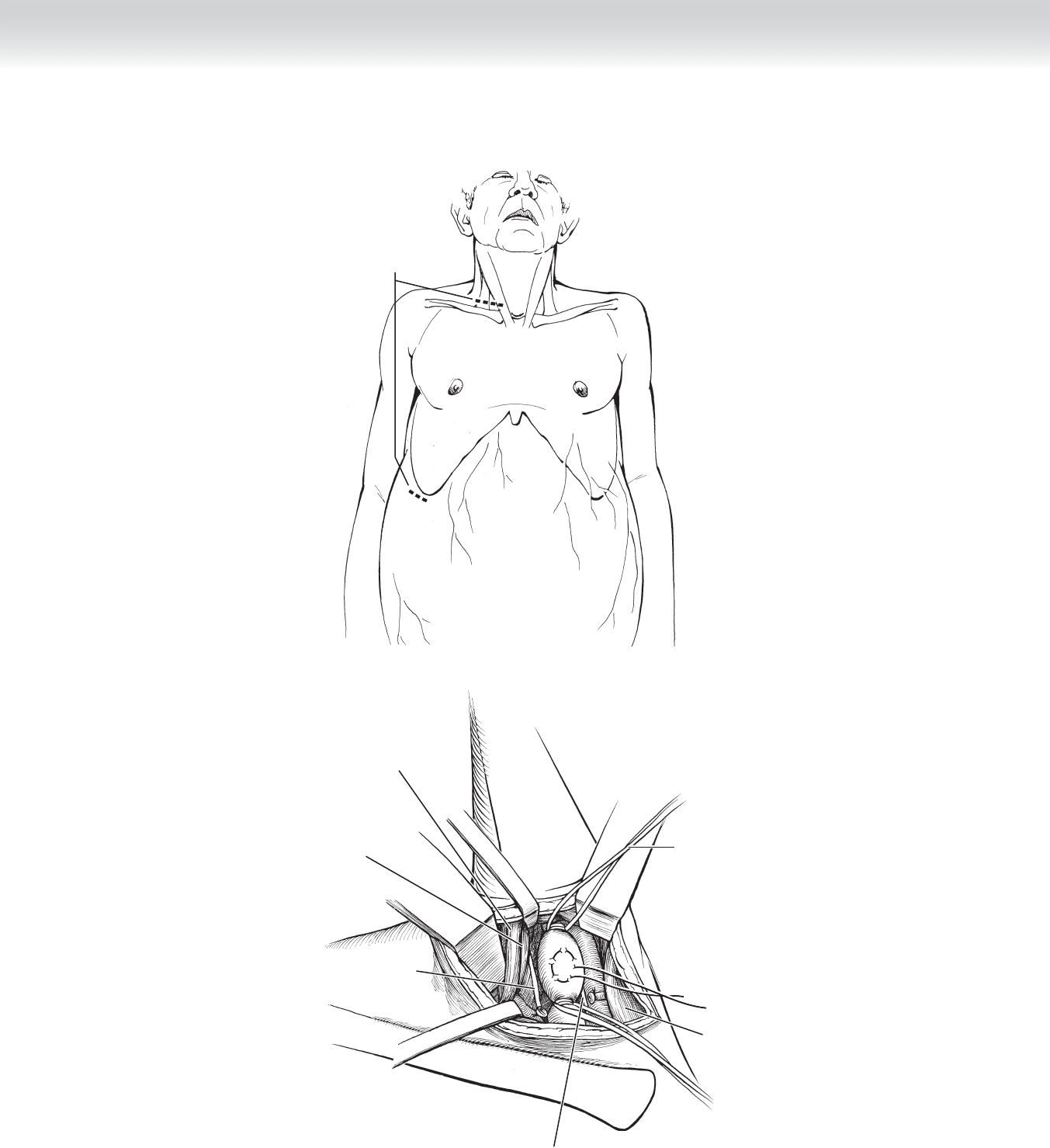
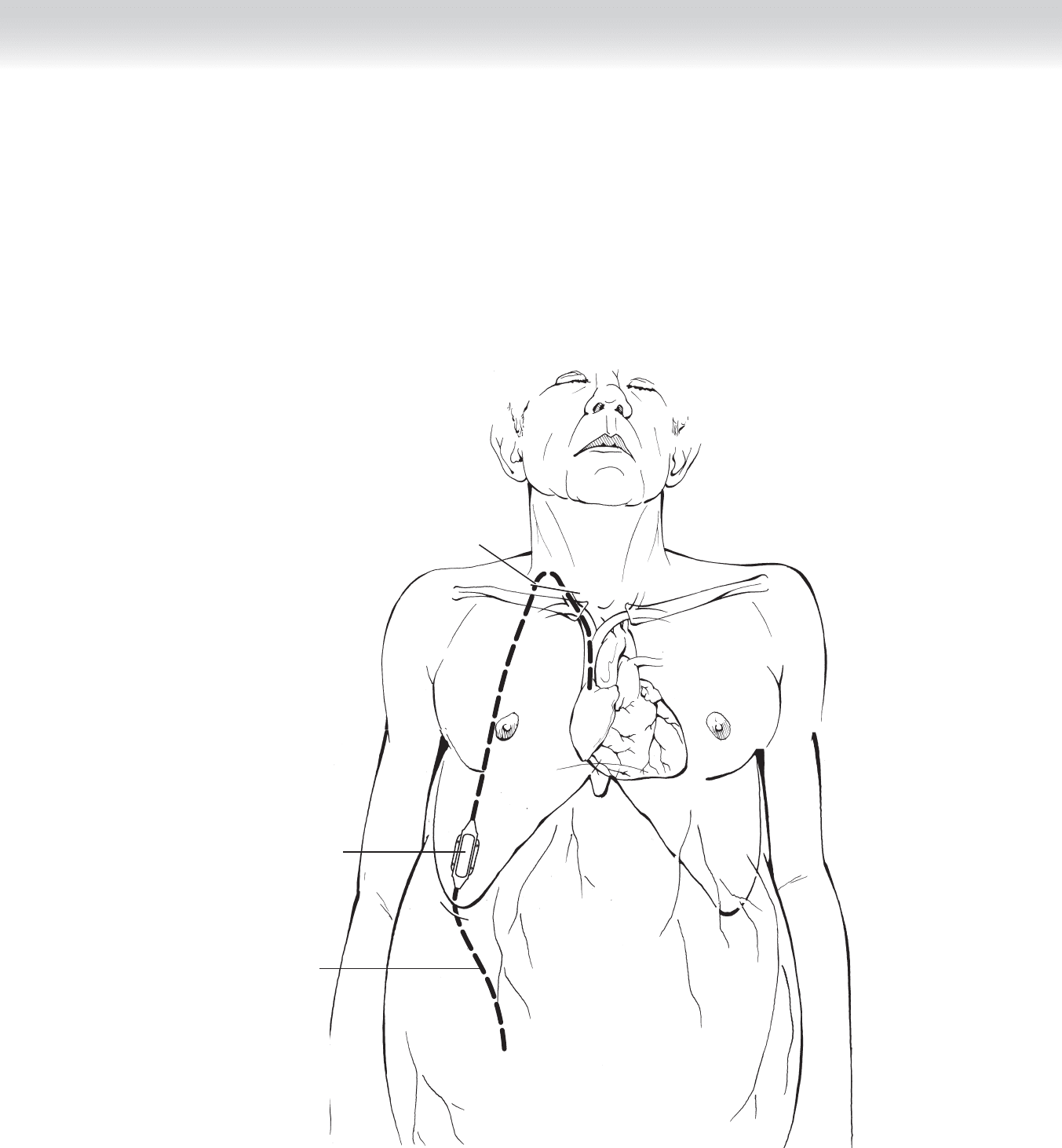
Proposed incisions
A
Elastic
vessel loop
Phrenic nerve
Vagus nerve
Prolene suture
Clavicular head of
sternocleidomastoid muscle
Omohyoid muscle
Sternal head of
sternocleidomastoid
muscle
Clavicle
B
FIGURE 92 –2

1022 Section XII • Vascular
2. DISSECTION
◆ The skin, subcutaneous fat, and platysma muscle are incised. The sternal and clavicular
heads of the sternocleidomastoid muscle are split. The jugular vein is located lateral to the
carotid artery and can be used as a landmark to facilitate the identifi cation of the vein. The
sheath that enwraps the vein keeps the vein from collapsing. This facilitates the circumfer-
ential dissection of the vein. If the dissection is close to the vein, damage to adjacent struc-
tures is minimal. The vein may have small tributaries coming into it, and disruption of
these may cause a moderate amount of bleeding. Identifi cation and ligation with division
of these small vessels is advised. Elastic vessel loops are used proximally and distally to
allow occlusion of the blood fl ow and control of the vessel in the operative fi eld (see
Figure 92-2, B).
◆ After the skin incision is made, the subcutaneous fat is incised to the muscle. A 0.5% to 1%
solution of lidocaine is injected into the subcutaneous tract from the abdominal incision to
the jugular incision. The tract should run laterally on the chest wall, outside the area of the
breast and over the clavicle. Marking the route of the tract on the skin will help you stay on
course when passing the catheter/shunt. Push a vascular tunneling device through the sub-
cutaneous tissues deep to the skin but above the muscle fascia, following the tract that was
injected with the anesthetic. Pull the shunt from the bottom up, taking care to orient the
shunt correctly. Denver shunts have a one-way pump that should fi t over the ribs. The
LeVeen shunts have a multiperforated abdominal end and a venous end that can be cut to
appropriate length (Figure 92-3).
CHAPTER 92 • Insertion of Peritoneal Venous Shunts 1023
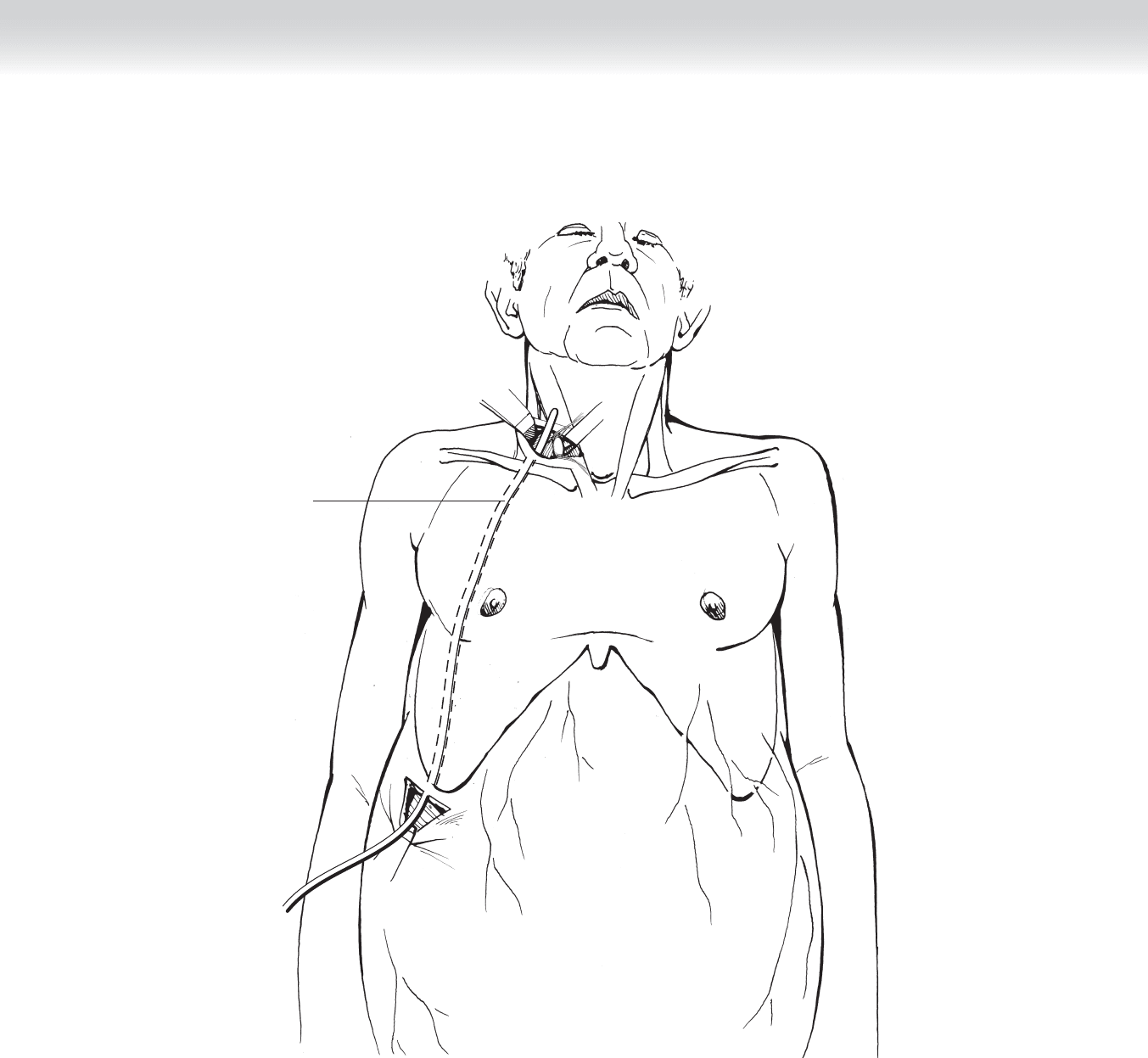
Shunt tubing in
subcutaneous
tunnel
FIGURE 92 –3

1024 Section XII • Vascular
◆ The muscle in the abdomen should be split to expose the peritoneum. A purse-string with a
radius of 1 cm should be made in the peritoneum. Permanent suture is advised. Incision of
the peritoneum within the purse-string is made with electrocautery or scissors. While the
ascites is draining, place the intra-abdominal end of the shunt into the opening and thread
the tubing into the peritoneal cavity. Secure the purse-string around the shunt. If using the
LeVeen shunt, thread the entire catheter in until the disc is fl ush with the peritoneum. Con-
nect the tubing running toward the neck incision to the port on the side of the abdominal
disc. Secure the tube to the disc with a large tie. If using the Denver shunt, thread the cath-
eter in until the “valve/pump” can be positioned over ribs 9 to 11. The subcutaneous tissue
will have to be dissected to create a cavity to support the pump. The pump should be
secured to the underlying tissue to avoid migration (Figure 92-4, A).
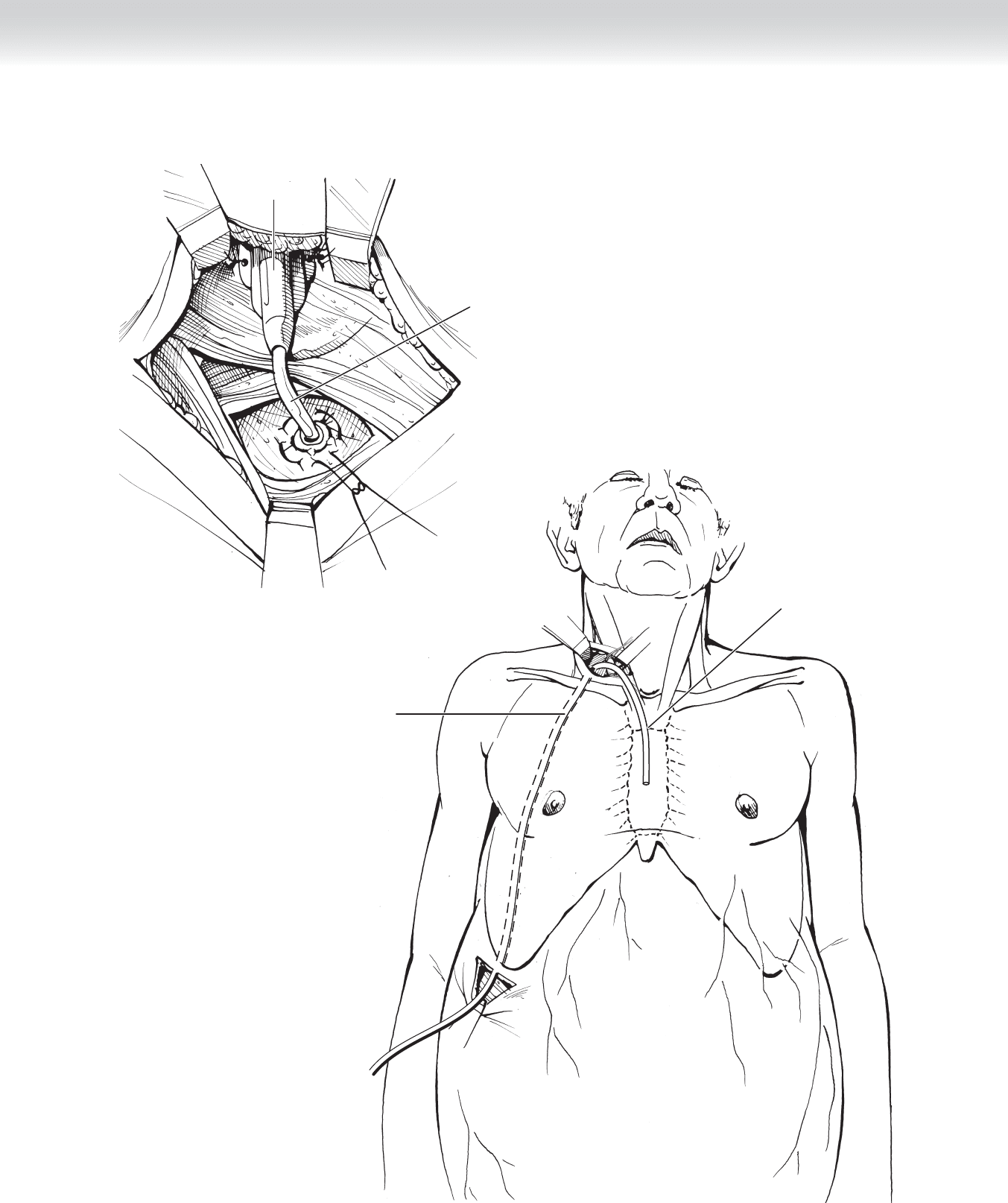
◆ Prime the tubing by aspirating at the venous end until there are no bubbles in the tubing. If
using the Denver shunt, press the pump several times until the fl uid comes out the end of
the shunt. Clamp the tubing at the site where it enters the neck incision from below. Esti-
mate the length of the venous end of the shunt by placing the tubing onto the sternum. Cut
the tube at the point where it crosses the manubrium. Do not cut the tube at an angle,
because the tube may push against the side wall of the vein and obstruct the fl uid fl ow
(Figure 92-4, B).
CHAPTER 92 • Insertion of Peritoneal Venous Shunts 1025
B
Shunt tubing in
subcutaneous
tunnel
Site of transection
of catheter
Shunt valve
Peritoneal
catheter
A
FIGURE 92 –4
1026 Section XII • Vascular
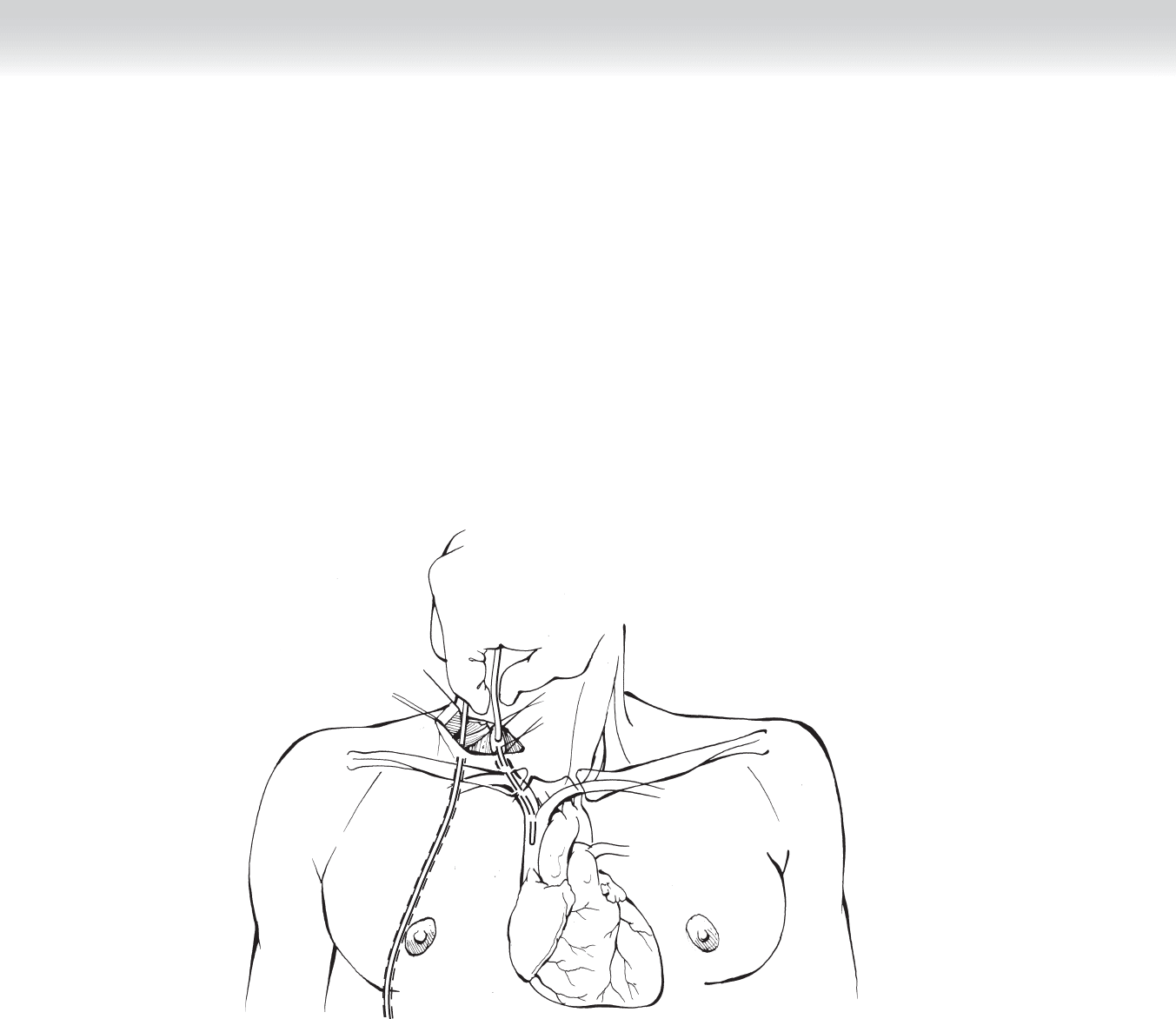
◆ Place a purse-string suture in the anterior wall of the jugular vein with Prolene suture
(3-0 or 4-0). Occlude the vein with the elastic loops. Incise the vein within the purse-string.
Raise the head of the patient to approximately 35 degrees. Keep the tubing clamped at skin
level and tubing distal to the clamp fi lled with the ascitic fl uid or heparinized saline (2500
U heparin in 250 mL normal saline).
◆ Hold the edge of the incised vein and insert the tubing. Take tension off the lower elastic
loop to allow the tube to be advanced into the thorax. Secure the purse-string around the
tubing (Figure 92-5).
FIGURE 92 –5
CHAPTER 92 • Insertion of Peritoneal Venous Shunts 1027
3. CLOSURE
◆ The course of the shunt should be from the peritoneal cavity, exiting out the abdomen and
coursing along the lateral chest wall, across the clavicle to enter into the internal jugular
vein, ending at the junction of the superior vena cava and right atrium. All wounds should
be closed in two layers over the foreign body (the shunt) (Figure 92-6).
Peritoneal
catheter
Venous catheter
Denver
shunt valve
FIGURE 92 –6

1028 Section XII • Vascular
STEP 4: POSTOPERATIVE CARE
◆ The patient should be admitted for an overnight stay. The potential problems are fever, fl uid
overload, and disseminated intravascular coagulation (DIC). Fever is usually transient and
treated symptomatically. The identifi cation of infection occurs in approximately 5% of those
patients with fever and warrants treatment. Pulmonary edema occurs in approximately 10%
of the patients but usually can be handled with diuretics. DIC is usually subclinical and can
be treated expectantly. The worst case scenario is fulminant bleeding, which requires re-
moval of the shunt. The bleeding may be related to exposure of the systemic circulation to
fi brin split products (FSP)–rich ascitic fl uid that may activate the coagulation mechanism.
Bleeding complications do not appear to be related to the severity of the post-shunt coagu-
lopathy but rather to the severity of liver dysfunction and presence of preoperative DIC,
probably caused by the liver disease.
STEP 5: PEARLS AND PITFALLS
◆ The contraindications for shunt insertion should include pseudomyxoma peritonei, recent
or current infection, preoperative coagulopathy, liver failure, and loculated ascites. Relative
contraindications include positive cytologic fi ndings in ascitic fl uid and concurrent cardiac
failure. Bloody ascites and ascitic fl uid protein content greater than 4.5 g/L are also consid-
ered contraindications to shunting, secondary to increased risk of shunt blockage from clot
or fi brin plugs.
◆ If a patient has had episodes of variceal bleeding, the risk of rebleeding postshunt is great
secondary to the risk of postshunt coagulopathy and increased intravascular volume.
SELECTED REFERENCES
1. Smith EM, Jayson GC: The current and future management of malignant ascites. Clin Oncol
(R Coll Radiol) 2003;15:59-72.
2. Becker G, Galandi D, Blum HE: Malignant ascites: Systematic review and guideline for treatment.
Eur J Cancer 2006;42:589-597.
3. Suzuki H, Stanley AJ: Current management and novel therapeutic strategies for refractory ascites and
hepatorenal syndrome. QJM 2001;94:293-300.

1030
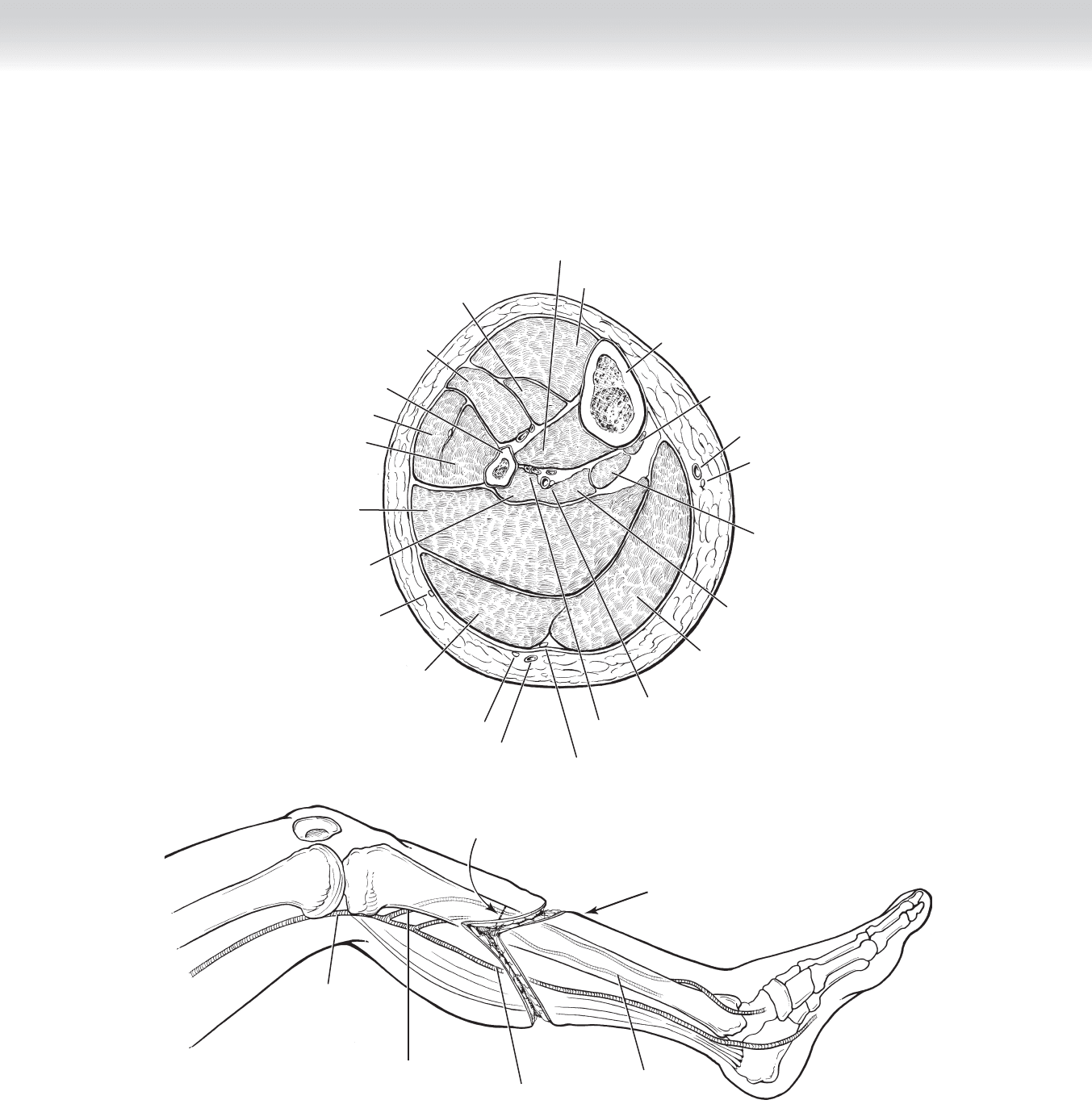
STEP 1: SURGICAL ANATOMY
◆ Cross-sectional anatomy of the lower leg is shown in Figure 93-1, A.
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Selection of level for amputation depends on the underlying pathology and the need to
ascertain effi cient wound healing of the amputation stump.
◆ Below-knee amputation stumps do not rely on a symmetrical fl ap closure, but rather the
posterior fl ap with extensive musculature is to be brought anteriorly.
◆ Use of a tourniquet is at the discretion of the surgeon.
STEP 3: OPERATIVE STEPS
1. INCISION
◆ Planning the level of incision begins by determining the bony structures to preserve,
typically 2 to 3 fi ngerbreadths below the tibial tuberosity (Figure 93-1, B).
◆ From this landmark, skin fl aps are developed, typically the midpoint of the leg in an
anterior to posterior plane is identifi ed, just below this level.
◆ The anterior fl ap is incised anteriorly.
◆ The posterior fl ap is incised as a semicircle, at its apex with a length equal to the distance
to reach the anterior margin of the wound.
CHAPTER
93
Below-Knee Amputation
Arthur P. Sanford
CHAPTER 93 • Below-Knee Amputation 1031
Tibialis anterior muscle
Extensor hallucis
longus muscle
Extensor digitorum
longus muscle
Peroneus longus muscle
Peroneus brevis muscle
Gastrocnemius muscle
(medial head)
Gastrocnemius muscle
(lateral head)
Tibia
Tibialis posterior muscle
Popliteus muscle
Great saphenous vein
Saphenous nerve
Soleus muscle
(tibial head)
Flexor digitorum
longus muscle
Soleus muscle
(fibular head)
Lateral sural
cutaneous nerve
Flexor hallucis
longus muscle
Sural nerve
Small saphenous vein
A
Peroneal artery and vein
MC
Medial sural cutaneous nerve
Posterior tibial artery, vein, and nerve
Fibula
Division of anterior
and posterior skin flaps
and deep tissue
Level of bone division
Popliteal artery
Anterior tibial artery
Posterior tibial artery
Peroneal artery
LS
B
FIGURE 93 –1