Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 90 • Hemodialysis Access Procedures 1001
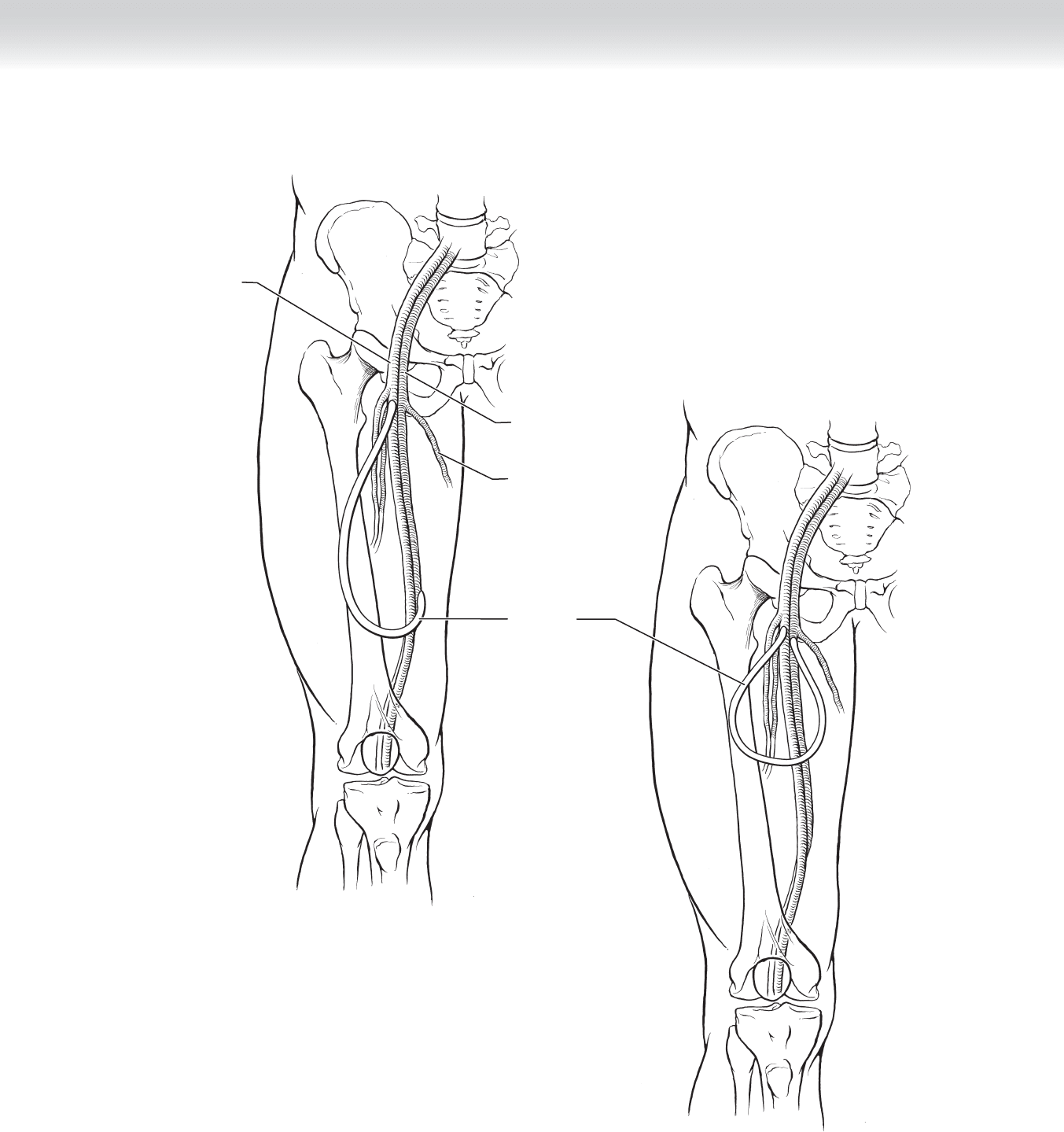
Femoral artery
PTFE graft
Femoral vein
Saphenous vein
FIGURE 90 –21

1002 Section XII • Vascular
2. DISSECTION
◆ Arterial infl ow and venous outfl ow are isolated. Proximal and distal control of both vessels
is obtained.
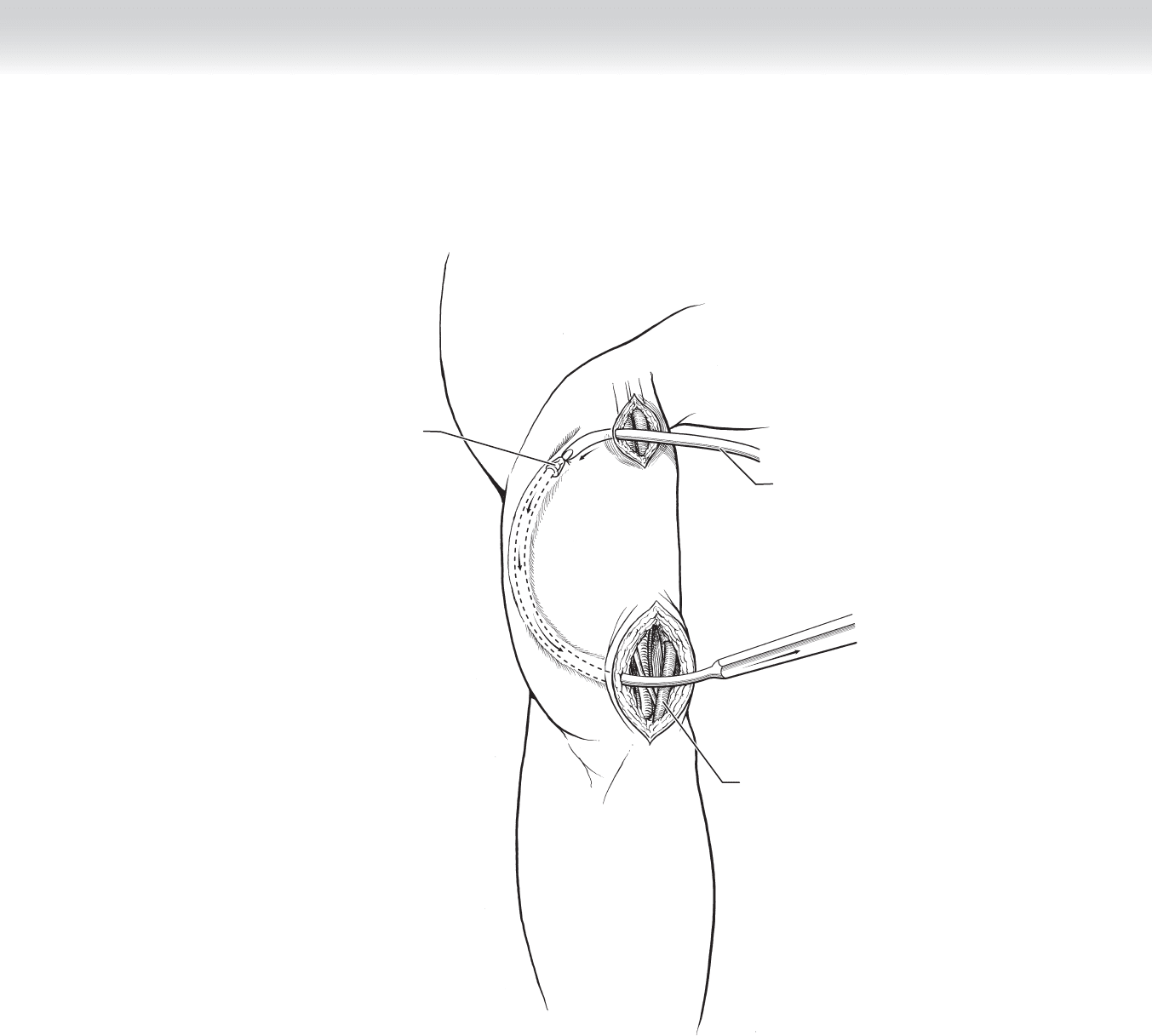
◆ The graft is tunneled, with care taken to keep the graft untwisted and to maintain a proper
depth (approximately 4 mm). A counter-incision may be required, depending on the ana-
tomic location (Figure 90-22).
◆ Once the tunnel is completed, the patient is heparinized. A small hood is cut in each end of
the graft, which is oriented according to the direction of fl ow. The vessels are clamped, and
end-to-side anastomoses are performed to the target artery and vein with 6-0 Prolene su-
ture. If the graft has a pre-existing (i.e., manufactured) venous hood, the venous anastomo-
sis should be performed fi rst to size the length of the graft appropriately.
◆ The clamps are removed, with the distal arterial clamp removed last. The graft is palpated
for a thrill. Revision may be necessary if a thrill is not readily palpable. If the graft twisted
in the tunnel, the anastomosis may need to be taken down and the vein retunneled. If the
graft is pulsatile without a thrill, a distal obstruction may be present. A venogram can be
performed to assess for stenotic lesions.
3. CLOSURE
◆ The wound is closed in two layers with interrupted 3-0 Vicryl subcutaneous sutures and a
running 4-0 Monocryl subcuticular layer.
CHAPTER 90 • Hemodialysis Access Procedures 1003
PTFE graft
Basilic vein
Tunneler
FIGURE 90 –22

1004 Section XII • Vascular
STEP 3: OPERATIVE STEPS—GRAFT REVISION: THROMBECTOMY
1. INCISION
◆ Most commonly, a small incision is made over the fi stula or graft a few centimeters down-
stream from the arterial anastomosis.
2. OPERATIVE APPROACH
◆ Proximal and distal control of the fi stula or graft is obtained. The patient is heparinized.
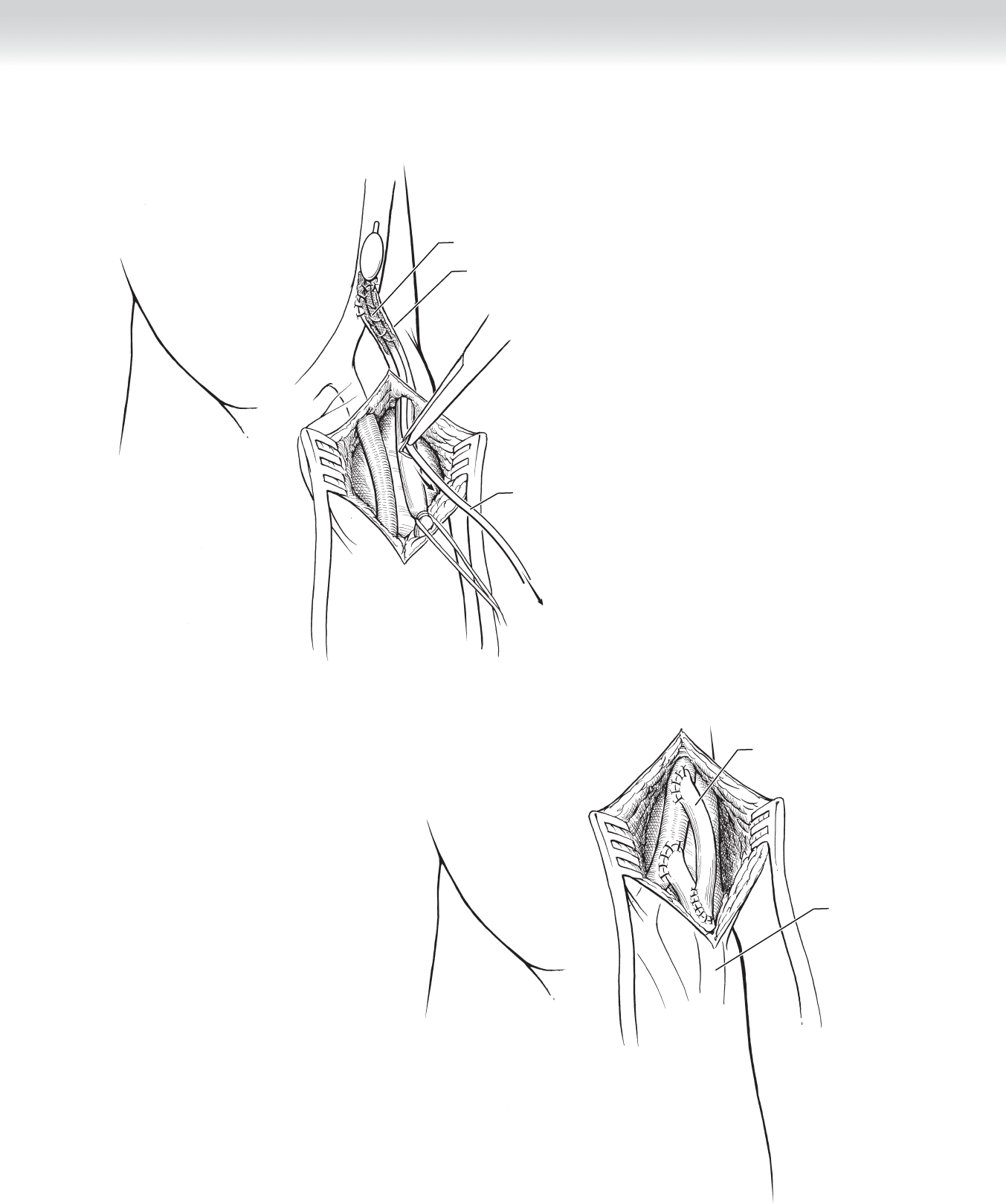
◆ A transverse incision is made in the conduit. A balloon thrombectomy catheter is passed
up the venous limb fi rst, and the clot is removed. The process is repeated for the arterial
limb. There should be the return of strong, pulsatile fl ow on removal of the arterial clot
(Figure 90-23).
◆ A fi stulogram or shuntogram is performed to assess for anatomic causes of the thrombosis.
The central veins should be assessed as part of this venogram to evaluate for central
stenoses. Peripheral or central stenoses may require balloon angioplasty or stenting.
◆ Short jump grafts or patch angioplasties are required for persistent anastomotic strictures
(Figure 90-24).
3. CLOSURE
◆ The wound is closed in two layers with interrupted 3-0 Vicryl subcutaneous sutures and a
running 4-0 Monocryl subcuticular layer.
CHAPTER 90 • Hemodialysis Access Procedures 1005
Balloon catheter
removing embolus
Thrombus
PTFE graft
FIGURE 90 –23
PTFE graft
PTFE graft
revision
FIGURE 90 –24

1006 Section XII • Vascular
STEP 4: POSTOPERATIVE CARE
◆ Patients should be examined again in the recovery room, and regularly until discharge, for a
thrill and a bruit in the access.
◆ Fistulae require a minimum of 6 weeks to mature before cannulation. Most grafts require a
minimum of 2 weeks before cannulation.
◆ Long-term catheters should be removed promptly once the fi stula or graft has matured and
has been used successfully for hemodialysis.
◆ Arm swelling that persists beyond the second postoperative week and does not respond to
arm elevation should be investigated further with imaging.
◆ Fistulae often have venous side branches that prevent adequate maturation. If these are
found, selective ligation of the branches can allow for maturation of the fi stula. Imaging
should be obtained of fi stulae that do not mature by the sixth postoperative week.
◆ Mature fi stulae (greater than 6 weeks after placement) are more likely to be usable if they
meet the Rule of 6s criteria: fl ow greater than 600 mL/min, diameter larger than 6 mm,
depth less than 6 mm, and discernable margins.
◆ Patients should be instructed in isometric hand exercises and in daily examination of the
access for a thrill or signs of infection.
STEP 5: PEARLS AND PITFALLS
◆ Nondistendable veins are sclerotic and usually will not mature. Noncompressible veins are
thrombosed. A history of intravenous drug use, chemotherapy, or multiple intravenous
catheters at the site may indicate the presence of such veins.
◆ When a fi stula or graft thromboses or has consistently high venous pressures, a fi stulogram
or shuntogram should be performed, which includes a central venogram. Because many of
these patients have had multiple catheters, they are at risk for subclavian vein stenoses. If
such a stenosis is found, it may be amenable to angioplasty and stenting. If the subclavian
vein is actually occluded, the other arm should be assessed for access sites.
◆ Most of the arterial targets course near major nerves. Care should be taken to avoid traction
injury or other damage to these nerves, especially in redo operations, where the anatomy
may not be as well demarcated as usual.
◆ Steal syndrome, defi ned as ischemia of the hand, is more common with artifi cial conduit
than autologous fi stula, probably because the slower maturation of the fi stula allows accli-
mation and collateralization to develop. Steal symptoms are also more common when the
anastomosis is above the elbow or the patient is diabetic. These symptoms may occur
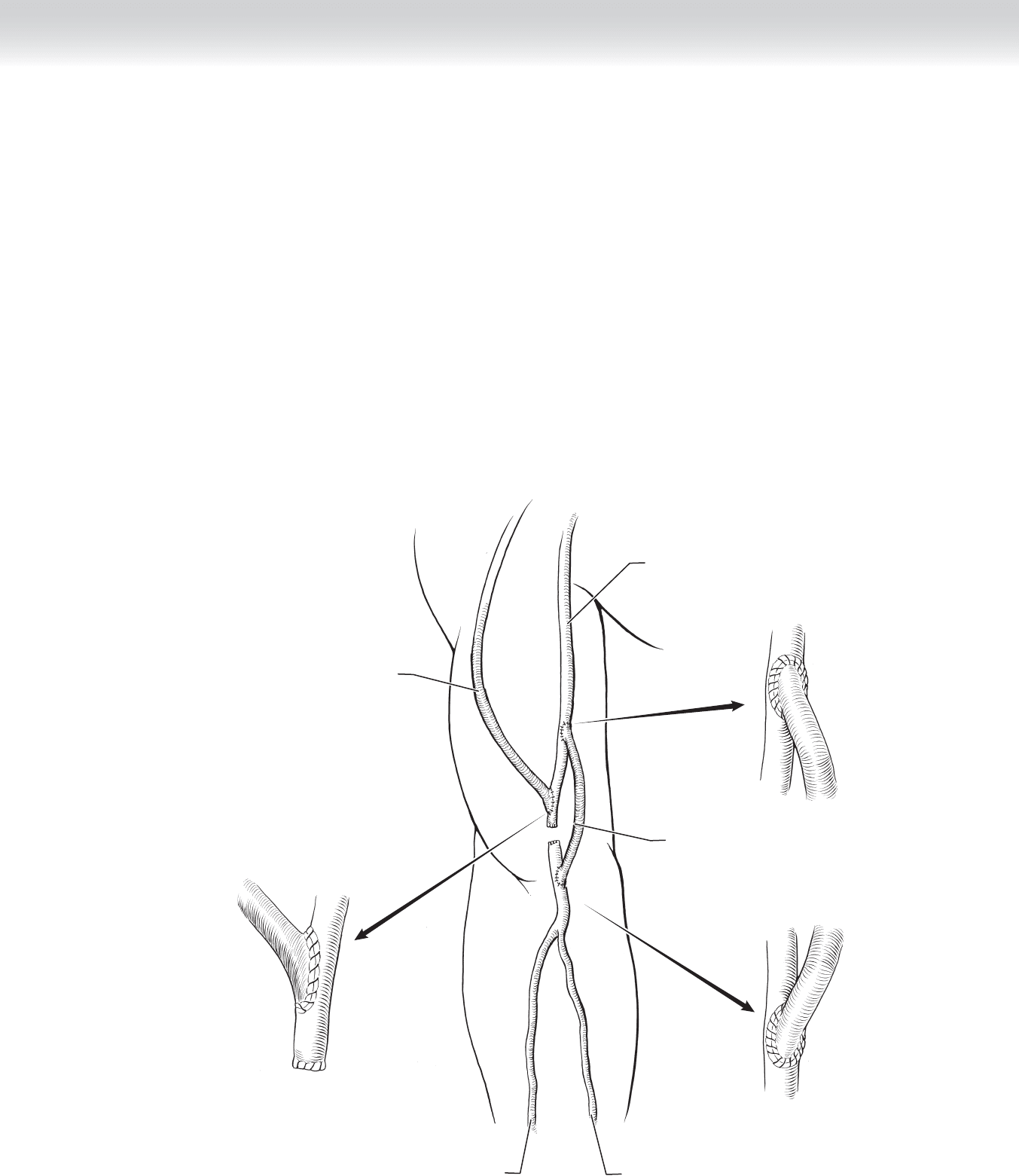
CHAPTER 90 • Hemodialysis Access Procedures 1007
sporadically, when the patient is on hemodialysis, or may be continuous. Any such symp-
toms require prompt evaluation. The access may need to be ligated or other procedures,
such as a distal revascularization with interval ligation (DRIL), may be required to prevent
hand loss and salvage the graft (Figure 90-25).
◆ Potential future access sites should be preserved, with the patient counseled to avoid blood
draws and catheters at those sites.
◆ Large aneurysmal dilations often indicate a downstream stenosis, especially if they occur
away from cannulation sites, and should be investigated further.
◆ The patient’s dialysis center should be sent a diagram of the access detailing the conduit,
course, and anastomotic sites, as well as any fi ndings of importance (e.g., angioplasty or
stent sites).
Brachial artery
Radial artery
Interposition graft
Ulnar artery
Dialysis access
(vein or PTFE)
FIGURE 90 –25

1008 Section XII • Vascular
SELECTED REFERENCES
1. National Kidney Foundation: KDOQI clinical practice guidelines and clinical practice recommendations
for 2006 updates: Hemodialysis adequacy, peritoneal dialysis adequacy, and vascular access. Am J Kidney
Dis 2006:48: S1-S322.
2. Haisch CE, Parker FM, Brown PM Jr: Access and ports. In Townsend CM Jr (ed): Sabiston Textbook of
Surgery: The Biological Basis of Modern Surgical Practice, 17th ed. Philadelphia, Elsevier Saunders, 2004,
pp 2081-2094.
3. Bohannon WT, Silva MB: Venous transpositions in the creation of arteriovenous access. In Rutherford RB (ed):
Vascular Surgery, 6th ed. Philadelphia, Elsevier Saunders, 2005, pp 1677-1684.
4. Lumsden AB, Bush RL, Lin PH, Peden EK: Management of thrombosed dialysis access. In Rutherford RB (ed):
Vascular Surgery, 6th ed. Philadelphia: Elsevier Saunders, 2005, pp 1684-1692.
5. Knox RC, Berman SS, Hughes JD, et al: Distal revascularization-interval ligation: A durable and effective
treatment for ischemic steal syndrome after hemodialysis access. J Vasc Surg 2002;36:250-255.
1009
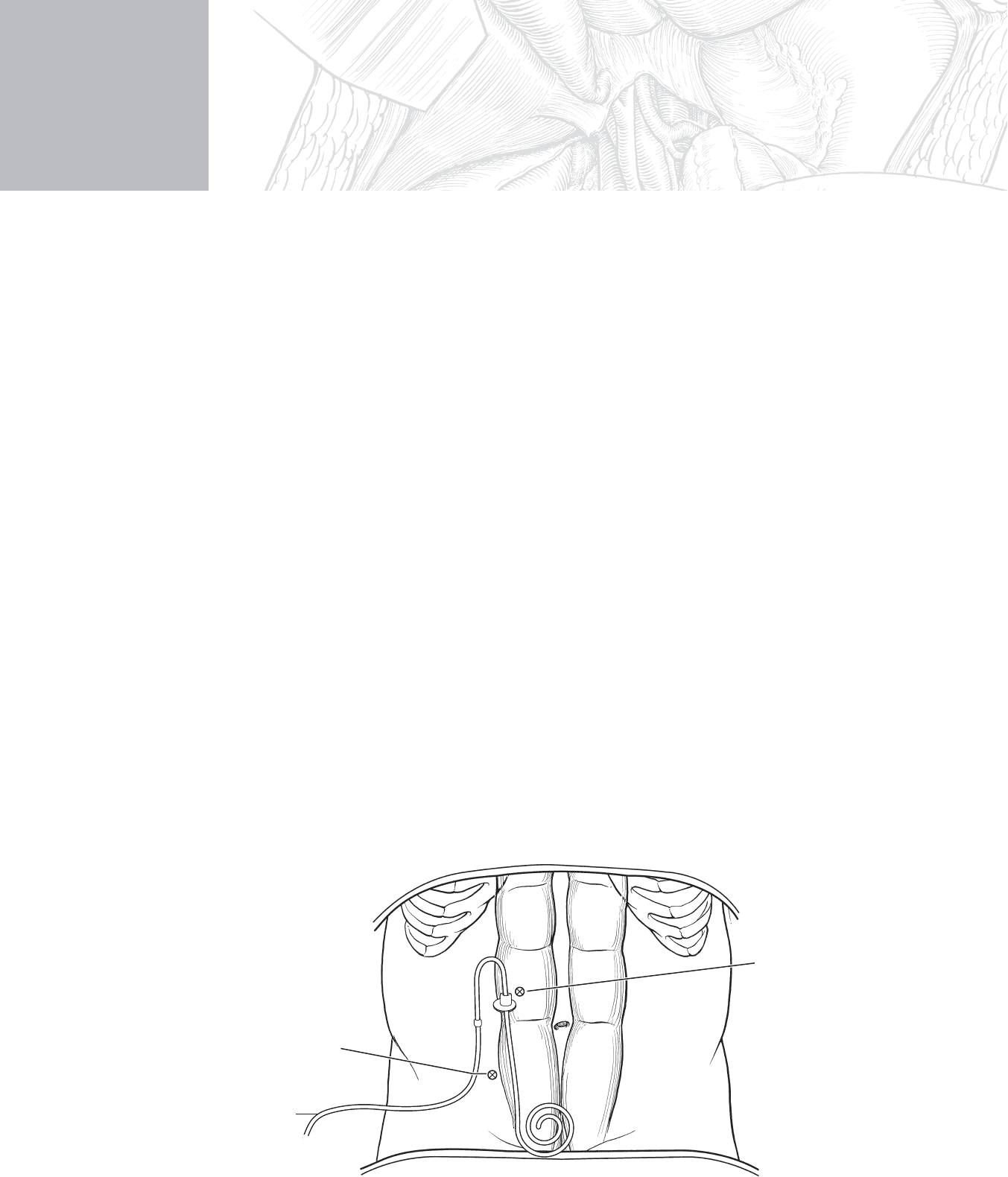
STEP 1: SURGICAL ANATOMY
◆ Place the uppermost trocar or the incision in a paramedian position. This allows for burial
of the cuff of the catheter under the muscle and decreases the incidence of cuff erosion
through the incision. Make the optimal placement by placing the catheter on the abdomen
in a position where the end of the catheter or the bottom of the cuff is situated on the sym-
physis pubis and the fi rst cuff lies over the rectus muscle. Place the incision where the fi rst
cuff lays on the abdomen. The exit site is usually lateral to the fi rst trocar. Use this site for
the second trocar (Figure 91-1).
◆ Achieve the optimal placement of the exit site with the aid of a home dialysis nurse. This
provider can meet with the patient preoperatively to design the exit site that is most func-
tional for the patient. Functionality is predicated by the handedness of the patient (usually
more comfortable when the catheter is placed on the same side as the dominant hand) and
body habitus (different placement for a patient with a large panniculus versus a thin
patient; patient comfort in having the catheter below the belt line or above).
CHAPTER
91
Insertion of Tenckhoff
Catheter
Kristene K. Gugliuzza
Catheter on
skin before
incision
Site for incision
or trocar
Site for exit of
catheter or trocar
MC
FIGURE 91–1

1010 Section XII • Vascular
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Twenty million Americans, one in nine adults, have chronic kidney disease (CKD), and
20 million more are at increased risk. The peritoneal dialysis (PD) catheter is one of the
three options for treatment of stage 5 CKD (glomerular fi ltration rate [GFR] ⬍ 15 ml/min).
The other options are hemodialysis and transplantation. Fifteen percent of the population
dependent on dialysis chooses the option of PD.
◆ There are four methods to place a PD catheter. One is an emergent, temporary catheter at
the bedside. Use this method only in a patient who requires immediate dialysis and cannot
be moved from the intensive care unit (ICU). The second method is an open placement
usually performed in the operating room with the patient under local or general anesthesia.
The third and fourth methods are placed laparoscopically, either as an assist to open surgery
or as the primary technique for placement of the catheter.
◆ Use the emergent and the laparoscopic-only procedures when there is no fear of adhesions
that increase the risk of perforation of bowel through the blind insertion of the trocar or
needle.
◆ The emergent placement of a PD catheter is similar to the procedure of diagnostic perito-
neal lavage (DPL). The Seldinger technique (using a blunt-tipped fl exible guidewire inside a
fi nder needle to introduce a sheath or a catheter into the peritoneal space) is a safe method
to place the catheter. You can accomplish this technique with an incision through the skin
down to the peritoneum or as a puncture through the skin.
◆ It is helpful if the patient’s bowel is defl ated. Encourage the patient to ingest only liquids
the day before the procedure.
STEP 3: OPERATIVE STEPS—OPEN PROCEDURE
◆ Patient positioning
◆ Place the patient supine.
◆ The surgical preparation should include the skin from the nipples to the symphysis pubis
and laterally from the mid-anterior axillary line to the anterior axillary line.
1. INCISION
◆ To estimate the correct position of the incision for the fi rst cuff of the catheter, lay the cath-
eter on the abdomen with the bottom of the curl placed on the symphysis pubis. The fi rst
cuff will lay lateral to the umbilicus on the side of the exit site mark that has been placed
preoperatively by the dialysis nurse. Make the incision approximately 1 cm above and
below the area of the cuff (see Figure 91-1).