Johnson J., Keogh J. Pediatric Nursing Demystified: A Self-Teaching Guide
Подождите немного. Документ загружается.

CONCLUSION
The kidneys and the urinary tract comprise the urinary system. Contained within
the kidneys are nephrons, which is the site where urine is formed. Nephron
tubules filter waste fluid (urine) from blood and flows urine into the urinary tract.
The urinary tract consists of ureter (tubes connecting the kidney to the bladder),
the bladder (a pouch to contain urine), and the urethra (the tube connecting the
bladder to outside the body). Urine in the bladder causes the micturition reflex,
which signals the brain that it is time to voluntarily urinate. The micturition
reflex develops around 3 years of age.
The kidneys also regulate the production of red blood cells, electrolytes,
fluid volume, and blood pressure.
Microorganisms can enter the urinary tract causing a urinary tract infec-
tion, which if left untreated can cause glomerulonephritis, inflammation of
the glomerulus, or pyelonephritis, which is a kidney infection.
Bacterial infections can also cause hemolytic uremic syndrome where glomeru-
lar arterioles are damaged that can lead to renal failure. Renal failure is a sudden
or progressive decrease in renal function. There are two types of renal failure.
Acute renal failure is reversible once the underlying condition is treated. Chronic
renal failure is irreversible because the underlying condition damaged the kidney.
Damage to the glomerular filtration membrane can result in nephritic syn-
drome where the kidneys release albumin into the urine, resulting in edema
due to a fluid switch in the body.
Pediatric Nursing Demystified
272
Interpretation: A streptococcal infection normally precedes acute
glomerulonephritis by up to 6 weeks. During that time the bacteria infects
the glomerulus, causing the kidneys to malfunction temporarily, resulting
in hematuria, proteinuria, and elevated creatinine and BUN. Urine output
is decreased, resulting in a high specific gravity of the urine. Proteinuria
causes a fluid switch to the third space, resulting in edema.
Nursing intervention: Strict intake and output, daily weights, place the
patient in a quiet environment. Place the patient on a low-salt, low-protein
and fluid-restricted diet. Administer antibiotics to resolve the infection;
diuretics to reduce edema, and corticosteroids to reduced inflammatory
response as ordered. Monitor for renal failure. Instruct Mrs. Miller to
administer the complete round of antibiotics and not to stop when Judy
begins to feel better.
Evaluation: Assess Judy’s temperature and urine output a week follow-
ing treatment to determine the success of treatment.
The urinary tract can also be affected by congenital anomalies, resulting in
abnormal structure of components of the urinary tract. These are typically
resolved by surgery.
Wilms tumor is another congenital disorder. Wilms tumor is a cancerous
growth that can go unnoticed until the child reaches 4 years of age. At first the
tumor is encapsulated, but the capsule can rupture, resulting in the tumor
metastasizing to other areas of the body.
CHAPTER 12 / Genitourinary Conditions
273
FINAL CHECKUP
1. The mother of a child diagnosed with Wilms tumor asks why they must be care-
ful when touching their child’s abdomen. What is the best response?
a. To prevent unnecessary pain to the child.
b. They might inadvertently injure the child.
c. The tumor is soft and encapsulated. Pressure on or near the tumor might rupture
the capsule.
d. The tumor may metastasize to the lung.
2. A parent of a child who is recently diagnosed with a urinary tract infection franti-
cally calls saying that her daughter’s infection has worsened since she started treat-
ment. Her urine is orange when before it was cloudy. What is your best response?
a. This is a normal side effect of phenazopyridine.
b. Go to the Emergency Department immediately.
c. Bring the child to the health-care provider immediately.
d. This is a tinge of blood that will resolve itself in 7 to 10 days.
3. The mother of a child who has been diagnosed with ureter stenosis asks for you
to explain this disorder. What is your best response?
a. Ureters are tubes that connect each kidney to the bladder. These tubes are narrower
than normal.
b. Ureters are tubes that connect each kidney to the bladder. These tubes did not exist
at birth; however, they can be restored surgically.
c. Ureters are tubes that connect each kidney to the bladder. There is a duplication of
these tubes.
d. Ureters are tubes that connect each kidney to the bladder. Two ureters are joined
together prior to entering the bladder.
4. A patient experiences a sudden decrease in renal function as a result of
pyelonephritis. What category acute of renal failure is the patient experiencing?
a. Prerenal
b. Renal
c. Postrenal
d. None of the above
?
Pediatric Nursing Demystified
274
5. A patient being treated for glomerulonephritis is prescribed Kayexalate. His mother
asks why this medication is prescribed. What is the best response?
a. Increases potassium that has decreased due to chronic glomerulonephritis
b. Increases potassium that has decreased due to acute glomerulonephritis
c. Removes potassium that has increased due to acute glomerulonephritis
d. Removes potassium that has increased due to chronic glomerulonephritis
6. The parents of a child with a recently diagnosed with Wilms tumor asks why
must the health-care provider stage the tumor. What is your best response?
a. To assess if the tumor has metastasized and if so where it has metastasized
b. To determine the child’s level of discomfort
c. To determine the best course of treatment
d. To prevent the tumor from spreading
7. A parent of a child who is diagnosed with hemolytic uremic syndrome asks why
her child’s kidney became enlarged. What is your best response?
a. A tumor developed on the kidney
b. Blood vessels within the kidneys became blocked by lesions
c. The child has a bacterial infection
d. The child has injected too much fluid
8. The health-care provider asks the patient’s mother to collect a urine sample
from the patient so the sample can be sent for a culture and sensitivity study. The
mother asks you why this is done. How would you respond?
a. Explain that the culture and sensitivity study identifies microorganism that causes
the infection
b. Explain that the culture and sensitivity study identifies RBC and WBC in the
urine
c. Explain that the culture and sensitivity study identifies microorganism that causes
the infection and the antibiotic that kills the microorganism
d. Explain that the culture and sensitivity study identifies nitrites in the urine
9. A parent of a child diagnosed with renal failure overhears the health-care
provider saying that the child has signs of third spacing of fluids. She asks you
what this means. What is your best response?
a. I’ll ask the health-care provider to explain this to you.
b. There is a backup of fluid because the kidneys are not working properly.
c. Extracellular fluids are contained either in the interstitial compartment or the intravas-
cular compartment. Renal failure causes fluids to move into a third compartment
within the body.
d. Fluid that is outside the cell is stored in tissue or in the vascular system. Renal
failure causes fluid to enter other areas of the body other than tissue or the vascular
system, resulting in edema.
CHAPTER 12 / Genitourinary Conditions
275
10. Why could insertion of a urinary catheter cause a nosocomial urinary tract
infection?
a. The urinary catheter provides a pathway for microorganisms to enter the urinary
tract.
b. The health-care provider used poor aseptic technique when inserting the urinary
catheter.
c. The patient was not administered prophylactic antibiotics.
d. All of the above.
ANSWERS
Routine checkup 1
1. b
2. a
Routine checkup 2
1. c
2. b
Final checkup
1. c 2. a 3. a 4. b
5. d 6. a 7. b 8. c
9. d 10. d
This page intentionally left blank
CHAPTER
Musculoskeletal
Conditions
13
Learning Objectives
At the end of the chapter, the student will be able to
1 Understand the structure and function of the musculoskeletal system.
2 Treat soft tissue injury.
3 Know how traction is used realign fractures.
4 Assess for compartment syndrome.
5 Explain hip dysplasia.
6 Identify scoliosis.
7 Care for a child with juvenile rheumatoid arthritis.
8 Teach parents about the treatment for a clubfoot.
OVERVIEW
The musculoskeletal system consists of bones, muscles, tendons, ligaments,
and fascia and provides support for soft tissue and protection for organs within
the body. The musculoskeletal system is also a reservoir for calcium and phos-
phorus and the site where red blood cells are produced.
Bones provide the rigid framework for the body and are moved when skele-
tal muscles contract. Skeletal muscles are connected to bones by bands of
fibrous connective tissue called tendons. Bones are connected to each other
to form a joint by fibrous connective tissue called a ligament.
Bones, muscles, and other structures in the body are covered by an
uninterrupted web of tissues called fascia that maintains the body’s structural
integrity.
BONES
Bones are covered by the periosteum, a double layer of connective tissue that
covers all bone except for joints. The periosteum nourishes the bone. Chil-
dren have a thick vascular periosteum that provides nourishment for bone
growth and faster healing.
Bones develop from tissues during the ossification process where osteoblasts
provide the structure for bone cells. Deposits of calcium and phosphorus, regulated
by the thyroid and parathyroid glands, form salt that strengthens the framework
for new bone. Placing bones under stress results in increased deposits in bone;
periods of no stress results in resorption of deposits by the body.
Long bones have a growth end called the epiphysis. At the epiphysis there
is the epiphyseal plate commonly referred to as the growth plate. The epiphy-
seal plate is composed of cartilage, dense connective tissue that does not con-
tain blood vessels. As the child grows, the epiphyseal plate is replaced by
1
Pediatric Nursing Demystified
278
Cartilage
Comminuted fracture
Compartment syndrome
Contusion
Epiphyseal line
Epiphyseal plate
Fascia
Greenstick fracture
Hairline fracture
Ligaments
Pavlik harness
Periosteum
RICE
Sprain
Strain
Synovial joints
Tendons
Traction
KEY WORDS
bone. Once the child stops growing, the epiphyseal plate transforms into the
epiphyseal line, which provides a smooth surface for articulating bones.
Nursing alert Damage to a child’s epiphysis might impede the child’s growth.
CHAPTER 13 / Musculoskeletal Conditions
279
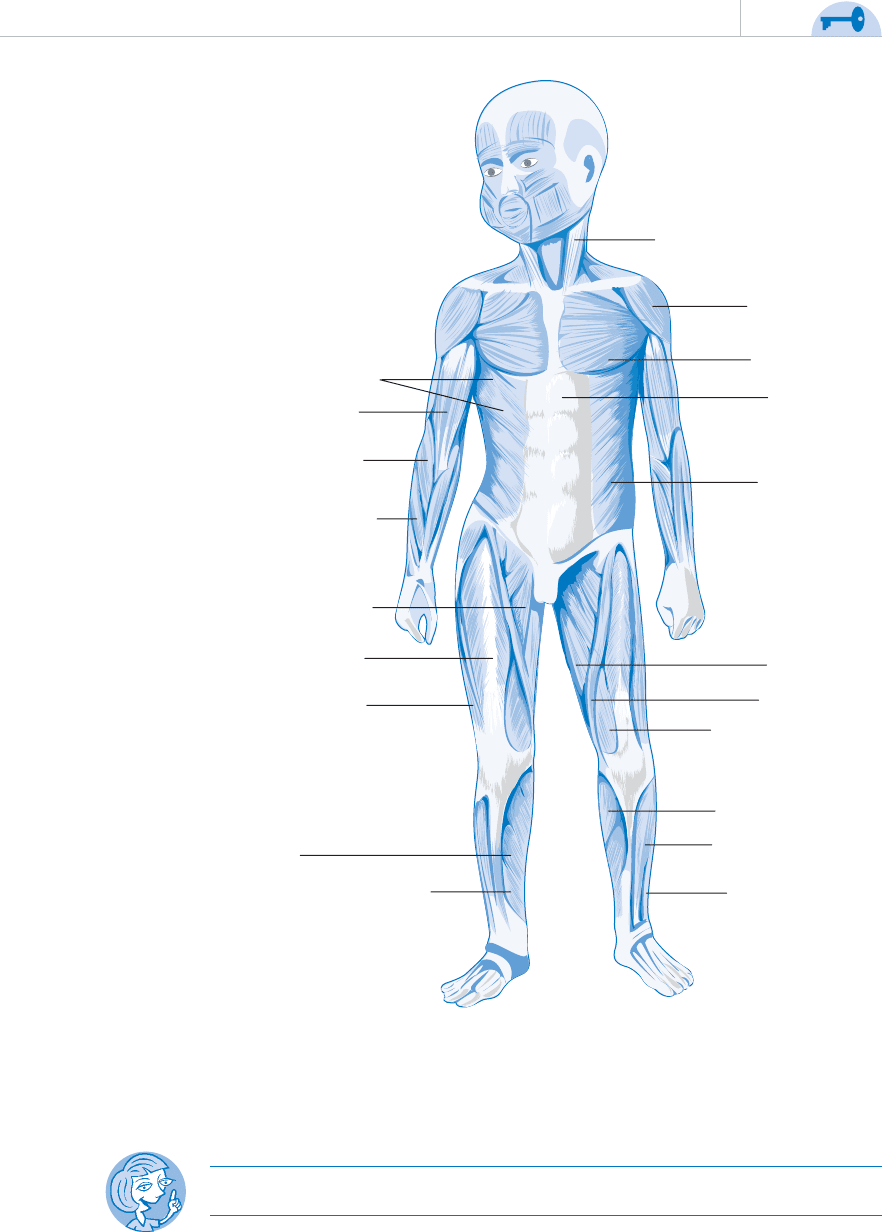
M. Sternocleidomastoideus
M. Deltoideus
M. Pectoralis
major
M. Rectus
abdominis
M. Obliquus
externus
abdominis
M. Gracilis
M. Sartorius
M. Vastus medialis
M. Gastrocnemius
M. Tibialis anterior
M. Extensor
digitorum longus
M. Flexor digitorum longus
M. Soleus
M. Vastus lateralis
M. Rectus femoris
M. Adductor longus
M. Extensor radialis
brevis
M. Brachioradialis
M. Biceps brachii
M. Serratus anterior
FIGURE 13-1 A
JOINTS
A joint is where two articulated bones come together. Joints are held together by
ligaments, and cartilage cushions the surface area between each bone.
Joints are classified by movement:
Pediatric Nursing Demystified
280
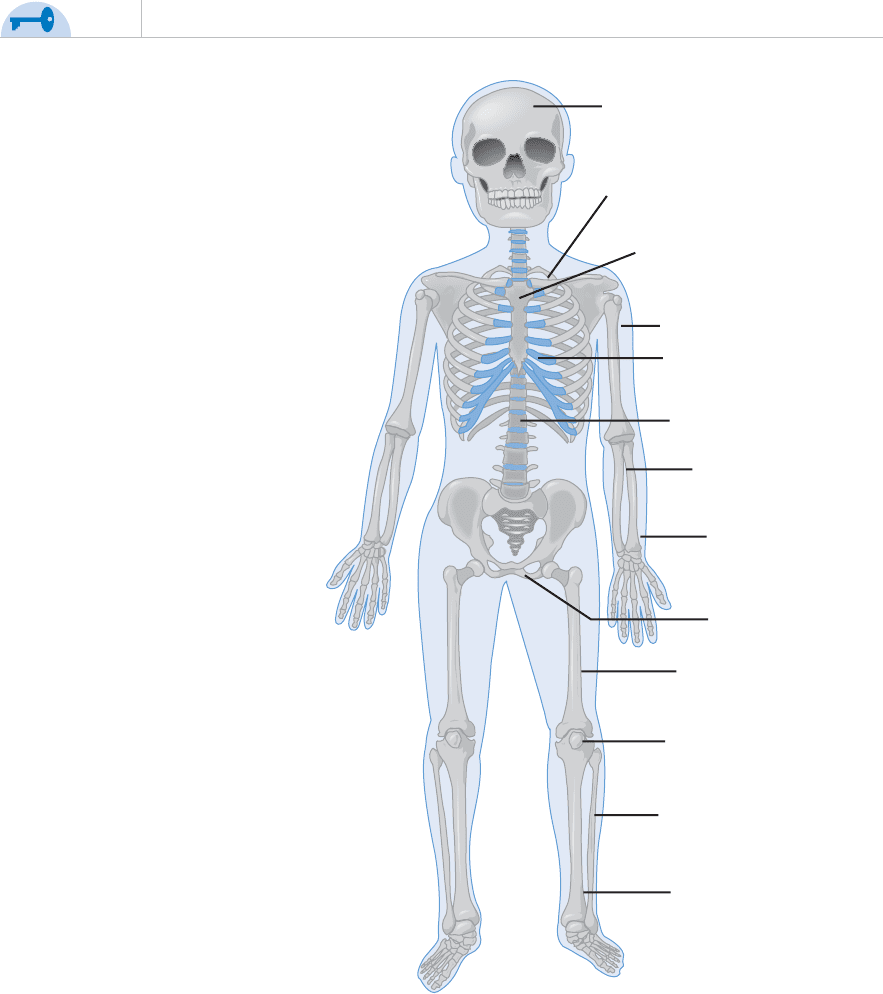
Cranium
Clavicle
Sternum
Humerus
Rib
Column
Ulna
Radius
Pelvis
Femur
Patela
Fibula
Tibia
FIGURE 13-1 B
䊋 Synarthrodial: Immovable such as the skull.
䊋 Amphidiarthrodial: Semimovable such as between the vertebras.
䊋 Diarthrodial (synovial joints): Freely movable such as the knees. These
are encapsulated joints that contain synovial fluid to lubricate the joint.
SKELETAL MUSCLES
Skeletal muscles are striated fibrous bundles covered with connective tissue
that contract when stimulated by an electrical impulse. During a contraction,
the muscle shortens, called flexing, causing the attached bone to be pulled in
the direction of the contraction.
Sets of opposing muscles are used to articulate a bone. One set of muscles
contracts while the opposing muscles relax, called extending, resulting in bone
movement. The opposing muscle contracts to return the bone to the original
position.
CHAPTER 13 / Musculoskeletal Conditions
281
Which of the following takes longer to heal if damaged?
a. Muscles
b. Tendons
c. Ligaments
d. Cartilage
Answer:
✔ ROUTINE CHECKUP 1
SOFT TISSUE INJURY
What Went Wrong?
Soft tissue injury is a sprain, strain, or contusion that affects the soft tissue of
the musculoskeletal system.
䊋 A strain is the tearing, twisting, or stretching of a muscle or tendon.
䊋 A sprain is injury to a ligament as a result of stretching or tearing the lig-
ament and is commonly the result of an automobile accident, fall, or
sports injury.
䊋 A contusion, commonly known as a bruise or hematoma, occurs when
a blood vessel ruptures beneath the skin and bleeds into the tissue and
causes discoloration.
Nursing alert Most ankle injuries in children are sprains.