Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.


have been used most widely and have been shown to
be safe should be preferred to anything new or
untested. Small doses of simple analgesic drugs such
as aspirin and acetaminophen (paracetamol) appear
to be safe, as do common cold remedies, which often
have these drugs as their active contents.
0028 No problems have been reported with the use of
homeopathic remedies in pregnancy. There has been
much interest in possible therapeutic benefit from the
consumption of oil of evening primrose in pregnancy.
It has been hypothesized that the linoleic acid and
g-linoleic acid in the compound may stimulate pro-
duction of vasodilatory prostaglandins and be of
benefit in lowering blood pressure in abnormal states
of pregnancy such as preeclampsia. The limited stud-
ies so far reported do not support this hypothesis.
0029 Recent reports have compared women who are on
diets rich in natural fish oil, the Faroese, with women
on the Danish mainland whose diets contain much
less fish oil. The Faroese had fewer premature babies,
fewer problems with blood pressure, and heavier
babies than the mainlanders. Unfortunately, these
studies cannot be interpreted as showing uniform
benefit from fish oil supplements as the Faroese also
lost more babies as stillbirths. A further report, com-
paring women in Aberdeen with women in the North
Sea Orkney Islands, showed the latter to have average
birth weights 250 g higher. After correction, a small
but significant proportion of the difference was found
to be related to genetic or environmental factors. The
latter included a diet in Orkney containing 30% more
fish than in Aberdeen.
0030 Ginger root may act as an antiemetic by a local
effect in the stomach. Evidence of benefit in preg-
nancy nausea exists.
0031 Garlic is widespread in the human diet. There has
always been a recognition of possible benefits of
garlic supplements on a wide range of disorders,
including hypertension, hyperlipidemia, and throm-
bosis. No studies of supplementation in pregnancy
have been reported.
Vitamin and Mineral Supplementation
0032 Some pregnant women benefit from iron and/or folic
acid supplements when dietary deficiency provokes
anemia. Although self-medication with vitamin and
mineral supplements is widespread, there is a good
case during pregnancy to restrict such supplements to
those prescribed by doctors or preparations contain-
ing less than 100% of the recommended dietary
allowance. Vitamin A in the form of retinol and its
analogs can cause congenital malformations in mega-
dosage, and vitamin D supplementation is thought to
have been the cause of idiopathic hypercalcemia. This
was a congenital syndrome consisting of abnormal
facial features, mental retardation, and abnormal
calcium metabolism. It was common in the UK in
the late 1950s and early 1960s when vitamin D sup-
plementation of a variety of foods was practiced. (The
relationship of periconceptional multivitamins to
NTDs is discussed elsewhere.)
0033It seems clear that some members of dark-skinned
races are at risk of vitamin D deficiency when resident
in temperate climates. Their newborns may be at
risk of hypocalcemia, a cause of convulsions in the
newborn period. These children may also have
delayed growth in the first year of life. Both problems
may be corrected by vitamin D supplementation in
pregnancy.
0034At various times, maternal zinc deficiency has been
proposed as a cause of both congenital malformation
and retarded fetal growth. No valid evidence has yet
emerged of any benefit derived from maternal zinc
supplementation with regard to either outcome in
humans.
Food Safety in Pregnancy
0035Pregnant women share the concerns of the general
public about food poisoning but there is a great deal
of confusion in the mind of the public and the
clinicians treating them about which foods are safe
to eat during pregnancy.
Listeria monocytogenes
0036This organism is widely distributed in the environ-
ment and the low incidence of infection suggests that
infection requires the ingestion of a large dose by a
susceptible individual. Listeriosis is a significant
problem in pregnancy because infection of the mother
can cause fetal death following transmission of the
organism across the placenta. It is not certain at the
present time whether the apparent increase in fetal
loss from this infection represents improved ascer-
tainment or a genuine increase in disease frequency.
0037Most women do not realize that the symptoms of
Listeria infection are not the same as those for some
other foodborne pathogenic organisms: Listeria symp-
toms are often described as mild ‘flu-like symptoms‘
rather than diarrhea and vomiting. The perceived risk
of Listeria infection in pregnancy for many women
appears to be much greater than the actual risk.
0038During pregnancy the following foods should be
avoided to reduce the risk of Listeria infection:
.
0039Mold-ripened cheese and some types of sheep and
goats’ milk cheese
.
0040Pa
ˆ
te
´
– meat, fish, and vegetable (unless canned or
ultra heat-treated)
PREGNANCY/Safe Diet 4735

.0041 Cook–chill foods that have not been thoroughly
reheated
However, many health professionals advise women
to avoid ‘unpasteurized soft cheeses‘ which, to most
pregnant women, means avoiding all types of cream
and cottage cheese together with yogurt and fromage
frais. In fact, it is only mold-ripened cheeses with
either a skin such as that found on Brie and Camem-
bert or a mold inside such as Danish blue that should
be avoided, together with sheep and goats‘ milk
cheese that has not been made with pasteurized
milk. Unnecessary avoidance of these dairy foods
will substantially decrease calcium intake.
Toxoplasmosis
0042 Toxoplasma is a protozoan organism which can cross
the placenta when primary infection occurs in preg-
nancy. It can lead to fetal death, mental handicap,
and/or blindness in an estimated 30% of offspring
of infected mothers. To reduce the risk of infection
during pregnancy women are advised to:
.
0043 Avoid eating raw and undercooked meat.
.
0044 Always wash vegetables and salads well to remove
soil.
.
0045 Wear gloves when gardening.
.
0046 Avoid unpasteurized sheep and goats’ milk.
.
0047 Wash hands after contact with cats and kittens and
avoid contact with stray cats.
.
0048 Wear rubber gloves when cleaning out cat litter
trays or get somebody else to do this job if possible.
(See Vegetarian Diets.)
Salmonellosis
0049 Salmonella bacteria are one of the most common
causes of food poisoning in the UK, giving rise to
sickness and diarrhea. Steering clear of raw eggs and
products containing uncooked egg and exercising ap-
propriate food hygiene can reduce this risk.
Campylobacteriosis
0050 The main source of Campylobacter infection is raw
milk and poultry but a large number of foods have
been implicated in outbreaks. Again, campylobacter
may not have any direct effect on the fetus, but the
Department of Health advises women in the UK to
avoid this distressing illness.
Shellfish
0051 Pregnant women are advised not to eat oysters and
other shelled seafood, such as prawns, mussels, and
crab, unless they are part of a hot meal and have been
thoroughly cooked. When raw these foods may be
contaminated with harmful bacteria and viruses.
Bovine spongiform encephalopathy
0052In 1996 evidence of a new variant of Creutzfeldt–
Jacob disease (CJD) began to be observed, which is
most probably the result of eating beef infected with
bovine spongiform encephalopathy (BSE). A particu-
lar source of concern at the moment is vertical trans-
mission which, although common in cattle, has not
been shown to occur in humans. However, there has
recently been a possible case reported in the media of
mother to child infection.
0053Other concerns of pregnant women in the area of
food safety include the hazards of fungicide and pesti-
cide residues. and possible harmful effects of natural
food toxicants. At present it seems unlikely that there
are toxic residues on foods which can be associated
with harm in pregnancy, but this observation should
not be taken as grounds for complacency. One of the
main difficulties for scientists wishing to explore this
matter is the limited availability of reproducible
assays for the minute quantities to be studied. Simi-
larly, the study of natural food toxicants for possible
harmful effects on the fetus is in its infancy.
Conclusions
0054It is important to monitor continuously any effects
our dietary habits may be having on child-bearing
and child development, but we should be able to
achieve this without causing unnecessary scares.
Most women who consume a good general diet, and
are not addicted to tobacco, alcohol, or other drugs,
can contemplate pregnancy without concern that
their dietary habits can ‘harm the baby‘.
See also: Caffeine; Campylobacter: Campylobacteriosis;
Cholecalciferol: Properties and Determination;
Physiology; Coffee: Physiological Effects; Folic Acid:
Properties and Determination; Physiology; Food
Intolerance: Food Allergies; Food Poisoning:
Classification; Food Safety; Garlic; Listeria: Properties
and Occurrence; Detection; Listeriosis; Retinol:
Properties and Determination; Physiology
Further Reading
Department of Health (2001) Committee on Toxicity of
Chemicals in Food, Consumer Products and the Envir-
onment. Statement on the Reproductive Effects of Caf-
feine 2001/06. London: HMSO.
Department of Health and Social Security (1990) Vitamin A
and Pregnancy. PL/CMO (90) 11, PL/CNO (90).
London: Stationery Office.
Department of Health and Social Security (2000) Folic Acid
and the Prevention of Disease. London: Stationery Office.
Frisch RE and McArthur JW (1974) Menstrual cycles: fat-
ness as a determinant of minimum weight for height
4736 PREGNANCY/Safe Diet
necessary for their maintenance and onset. Science 185:
949–951.
Jensen KT, Hjollund NH and Henriksen TB (1998) Does
moderate alcohol consumption affect fertility? Follow
up study among couples planning first pregnancy. British
Medical Journal 317: 505–510.
Karen G (ed.) (1990) Maternal–Fetal Toxicology. A Clin-
ician’s Guide. New York: Marcel Dekker.
Maternal Diet, Vitamins, and
Neural Tube Defects
M L Watkins, National Center on Birth Defects and
Developmental Disabilities, Atlanta, GA, USA
S L Carmichael, March of Dimes/California Birth
Defects Monitoring Program, Oakland, CA, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Background
0001 The most interesting work relative to neural tube
defect (NTD) etiology and prevention in the last few
years has focused on nutritional factors. This chapter
summarizes what is known about the relation
between NTDs and various nutritional factors,
with particular emphasis on folate, and includes a
discussion of the methodologic challenges inherent
in identifying such associations.
Neural Tube Defects
0002 NTDs result from failure of normal closure of the
embryonic neural tube at one or more of five separate
closure sites. Complex forces are involved, with vary-
ing closure mechanisms at different sites within the
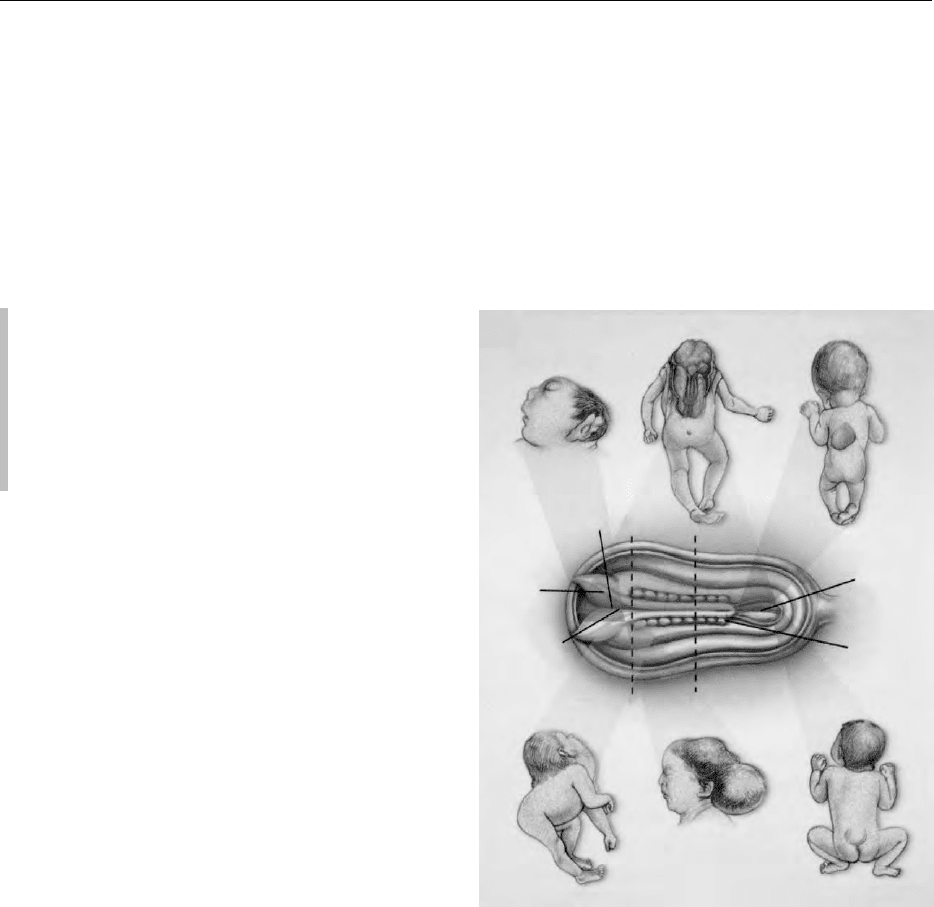
neural tube. Of the several NTD types (Figure 1),
spina bifida is the most common. The extent of phys-
ical disability (e.g., paralysis, bowel and bladder dys-
function) associated with spina bifida depends on the
lesion level, size, and extent of spinal nerve involve-
ment. Developmental, learning, and social problems
are common. Most children born with spina bifida in
developed countries now survive because of extensive
medical and surgical treatment. Many of these
children, however, face lifelong physical and deve-
lopmental disabilities. The death rate for affected
infants in the USA is about 10%, but the rate is
much higher in countries with less accessible medical
care. Clinical deterioration and secondary conditions
occur in many affected children in a variety of body
systems, resulting in complex medical and surgical
care. Because of a lack of information about the
natural history of untreated children, a lack of ran-
domized trials, and a lack of diagnostic criteria for
neurologic complications, there are controversies
about optimal care. The economic costs of spina
bifida are huge. The role and effectiveness of intra-
uterine myelomeningocele repair is controversial;
clinical trials have been recommended.
0003NTDs affect at least 300 000 newborns worldwide
each year. NTD rates vary considerably around the
world, with northern China reporting some of the
Anencephaly
Cranial
neuropore
Neural
fold
Neural
groove
AB
Iniencephaly
Encephalocele
Caudal
neuropore
Somite
Closed spina bifida
Craniorachischisis Open spina bifida
fig0001Figure 1 Neural tube defects. Schematic view (from above) of a
neural tube. Main clinical types of neural tube defects. Anenceph-
aly (lateral view): the absence of the brain and skull can be total
or partial, always fatal. Craniorachischisis (posterior view):
anencephaly occurs with contiguous bony defect of the spine
and exposed neural tissue. Open spina bifida (posterior view):
bony defect of the vertebrae (in this case, of the lower thoracic
vertebrae), accompanied by exposure of neural tissue and men-
inges that are not covered by skin. Closed spina bifida (posterior
view): bony defect of the vertebrae and, if present, the herniated
meninges and neural tissue, are covered by skin. Extent of the
disability associated with spina bifida related to the level and
size of the lesion and the extent of spinal nerve involvement.
Encephalocele (lateral view): the brain and meninges herniate
through a skull defect. Iniencephaly (lateral view): the dysraphic
process in the occipital region is accompanied by severe retro-
flexion of the neck and trunk. Spina bifida and anencephaly are
more common than encephalocele, craniorachischisis, or inien-
cephaly. Adapted from Botto LD, Moore CA, Khoury MJ and
Erickson JD (1999) Neural-tube defects. New England Journal of
Medicine 341: 1509–1519, with permission.
PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects 4737
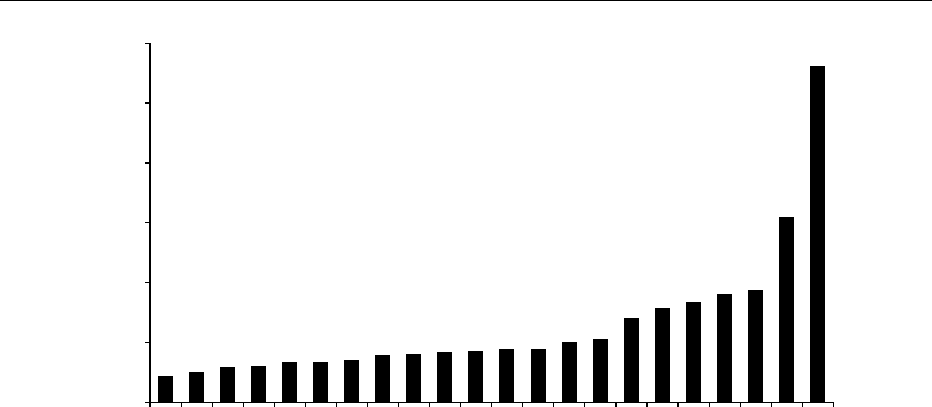
highest rates (Figure 2). Both environmental and gen-
etic factors likely explain the variation in rates. Of
NTDs, 80% are thought to be ‘multifactorial,‘ mean-
ing that they are influenced by both genetic and en-
vironmental factors. A minority of NTDs are caused
by chromosomal abnormalities, single gene muta-
tions and teratogens. Risk factors include maternal
diabetes, use of folic acid antagonists, fever or hyper-
thermia in early pregnancy, low socioeconomic
status, and obesity. In the USA, NTD rates are higher
among Hispanic whites than non-Hispanic whites;
blacks have the lowest rates. NTD-rate monitoring
is complicated by the increasing use of prenatal diag-
nosis and selective termination, which results in lower
birth prevalence. Because the neural tube develops
very early in pregnancy (closure by 28 days postcon-
ception) before most women are aware they are preg-
nant, prevention efforts are challenging, especially in
populations with high unplanned pregnancy rates.
Approximately 95% of all NTD-affected pregnancies
occur in women with no previous history, which is
referred to as ‘occurrence.‘ However, women who
have already had an NTD-affected pregnancy have
a 10-fold greater risk for having an NTD-affected
subsequent pregnancy than women who have not.
Having more than one NTD-affected pregnancy is
referred to as ‘recurrence.‘
0004The increased prevalence of NTDs in lower socio-
economic groups, decreasing NTD rates, and sea-
sonal patterns of occurrence are consistent with a
dietary etiology for NTDs. Certain nutrients (specif-
ically folic acid) were thought to be involved because
of their role in human growth and because birth
defects occurred with maternal use of folic acid an-
tagonists (e.g., aminopterin, when used as an aborti-
facient, induced fetal NTDs). Also, animal data have
demonstrated NTD inducement resulting from vari-
ous nutritional deficiencies and excesses, suggesting
the plausibility of nutritional causes of NTDs.
Methodologic Issues in the Study of
Nutrition and NTDs
0005However plausible the link between nutrition and
NTDs, studying these associations presents inherent
challenges. Approaches to measuring nutritional
status can be broadly classified as dietary, bio-
chemical, anthropometric, or genetic. Many of the
0
Switzerland
Rate per 10 000 births
Denmark
Netherlands
Italy
Japan
Belgium
Czech Republic
Ireland, Northern Ireland
United states
France
Norway
Uruguay
China (South)
Spain
British Isles
Australia
Brazil
Chile
Argentina
Venezuela
Mexico
China (North)
10
20
30
40
50
60
fig0002 Figure 2 Rates of spina bifida and anencephaly by country. Cases reported in pregnancy terminations are included, where
available. Rates for Latin-American countries and Japan are estimated from hospital-based registries. Rates for other locations are
based on data from birth defects registries that usually monitor only part of a country’s birth population. The following countries and
registries are included: Switzerland (selected counties), Denmark (Odense), The Netherlands (North), Italy (Campania, Emilia-
Romagna, Toscana), Belgium (Hainaut-Namur), Czech Republic, Ireland (Dublin, Belfast), United States (Atlanta, Hawaii), France
(Bouches-du-Rhone, Paris, Strasbourg, Central East France), Norway, Spain (Basque country), UK (Glasgow, North Thames),
Australia (Victoria, South Australia), and China (selected counties). Data from the International Center for Birth Defects and the
European Registration of Congenital Anomalies (1998) World Atlas of Birth Defects, pp. 20–31. Geneva: World Health organization.
4738 PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects

difficulties in studying nutrition and birth defects
stem from the fact that most studies are retrospective
in nature, resulting from the relatively low prevalence
of NTDs. This limitation has varied implications,
depending on the particular approach used to meas-
ure nutritional status.
0006 The food-frequency questionnaire is a tool com-
monly used to assess dietary intake retrospectively.
This method produces reasonably valid and reliable,
comprehensive, and semiquantitative data on usual
or average intake of foods and nutrients. The validity
of the data depends, however, on several factors,
including the appropriateness of the food list for the
study population; the accuracy of the nutrient data-
base; and variability in individual nutrient require-
ments and in the bioavailability and absorption of
nutrients from foods (which are affected by, for
example, food processing, fiber intake, alcohol con-
sumption, cigarette smoking, and infection). Chal-
lenges related to the analysis of dietary data include
whether to analyze intake from foods and supple-
ments separately or together; foods versus nutrients;
or single versus multiple nutrients simultaneously.
The high correlation that exists between nutrients
makes it particularly difficult to isolate the independ-
ent effects of individual nutrients.
0007 Depending on the particular nutrient, biochemical
measures of nutritional status may vary by time of
day, by the tissue from which the measurement is
made (serum and toenail zinc, for instance, reflect
more short-term versus long-term zinc status, respect-
ively), and by various host factors (e.g., genes, behav-
iors such as smoking and alcohol consumption,
health status, physical activity, stress, and medica-
tions). Furthermore, pregnancy itself is a time of
changing nutritional requirements and absorption.
These factors must be taken into consideration
when interpreting results from individual studies
and when comparing results across studies.
0008 Anthropometric measurements (e.g., height and pre-
pregnancy weight) can be recalled reasonably well.
Whether retrospectively collected data on more com-
plex measures (e.g., skinfold thickness and waist-to-hip
ratio) can serve effectively as proxies for these param-
eters around the time of conception is questionable.
0009 Genetic material is most commonly obtained from
blood samples or buccal smears. The challenge is in
discovering functionally relevant polymorphisms and
in having sample sizes large enough to detect mean-
ingful differences in risk. Recent advances in tech-
nology are enabling more rapid identification and
analysis of polymorphisms, and innovative appro-
aches to epidemiologic study design are being dev-
eloped that enable smaller numbers of subjects for
examination of certain types of genetic hypotheses.
Folic Acid and NTDs
0010In 1930, Dr. Lucy Wills discovered a factor that cured
the nutritional deficiency anemia of pregnancy
among women in India. This factor was later isolated
from spinach and named ‘folic acid‘ (folium is Latin
for ‘leaf‘). Because humans are unable to synthesize
folate, they must depend solely upon dietary sources.
Folate-rich food sources include green leafy vege-
tables, grains, legumes, certain fruits, and liver. Be-
cause heat, ultraviolet light, and air inactivate food
folate, food processing, preparation, and cooking can
reduce the amount of food folate ingested by an esti-
mated 50–95%. Bioavailability, the extent to which
folates are available for use at the cellular level, varies
widely across foods. The bioavailability of synthetic
folic acid (monoglutamate form), which is used in
cereal grain fortification and multivitamin/mineral
supplements, is estimated to be about twice that of
food folate (polyglutamate form).
0011Studies in the mid-twentieth century linked nutri-
tion and NTDs. Lower vitamin C and folate levels in
one study and poorer diet quality (in terms of macro-
nutrient and fresh fruit and vegetable intake) in an-
other were found among women with NTD-affected
children. Intervention and observational studies
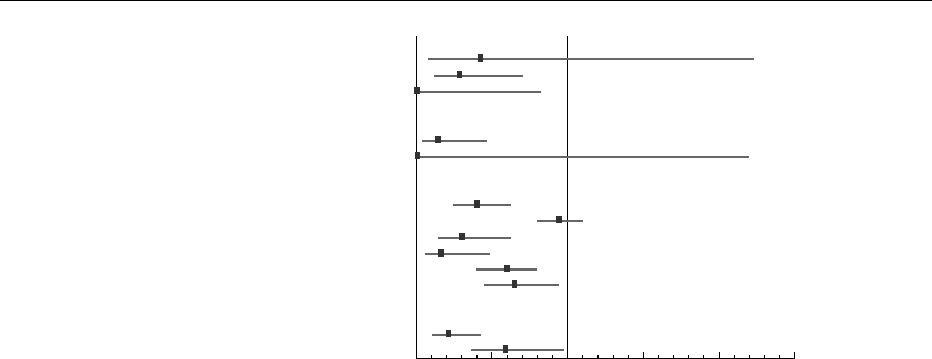
followed (Figure 3). The most convincing and solid
evidence for a preventive effect of folate is provided
by two intervention trials. The international Medical
Research Council (MRC) trial, a large UK-sponsored
recurrence prevention trial, was conducted at 33 sites
in seven countries. Women who had a previous NTD-
affected pregnancy were randomized to one of four
vitamin-use groups. Among 1195 pregnancies with
known outcomes, folic acid (alone or with other vita-
mins) was associated with a 72% reduction in risk.
0012In 1992, a Hungarian randomized trial pro-
vided strong evidence for the efficacy of folic acid-
containing multivitamin supplementation to prevent
NTD occurrence. Results from this trial, combined
with results from several observational studies
(Figure 3) provided convincing evidence that occur-
rence is preventable. As a result, several countries
recommended in 1992 that women of childbearing
potential consume periconceptional folic acid daily
(most commonly 400 mg) to prevent NTDs. The rec-
ommendation was made for all women capable of
becoming pregnant (not just those planning a preg-
nancy), because these birth defects occur before many
women are aware that they are pregnant, and because
many pregnancies are unplanned. Since then, a large,
nonrandomized community intervention in China
demonstrated significant NTD reductions associated
with the use of a 400-mg supplement containing only
folic acid. Risk reductions were greater (85%) in the
PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects 4739
high-prevalence northern countries than in the lower-
prevalence southern counties (40%). Additional
evidence for the efficacy of folic acid comes from
another study that found that periconceptional ex-
posure to folic acid antagonist medications more
than doubles the risk for NTDs and that folic acid
supplementation reduced the risk elevation associ-
ated with certain folic acid antagonists.
Efficacy Issues
0013 Based on the risk reduction observed in several stu-
dies, estimates are that at least 50% of NTDs could
be prevented by the use of folic acid. The proportion
of NTDs that are preventable may be less in low-
prevalence areas than in high-prevalence areas.
Some studies also suggest a smaller reduction in risk
for NTDs associated with folic acid use for Hispanics
than for non-Hispanic whites or blacks, and for obese
women compared with average weight women. These
observations require more study. The minimum daily
effective dose of folic acid for NTD prevention is
unknown; it may be < 400 mg for occurrence preven-
tion, but determining the effectiveness of lower
dosages is difficult because of the size and cost of
studies necessary to assess the relative efficacy of
various dosages.
0014The reasons for variability in folate efficacy are
unknown, largely because the biologic mechanism
by which periconceptional folic acid use protects
against NTDs is unknown. Folic acid plays a role in
transfer of methyl groups in the amino acid methyla-
tion cycles, a process essential for recycling homo-
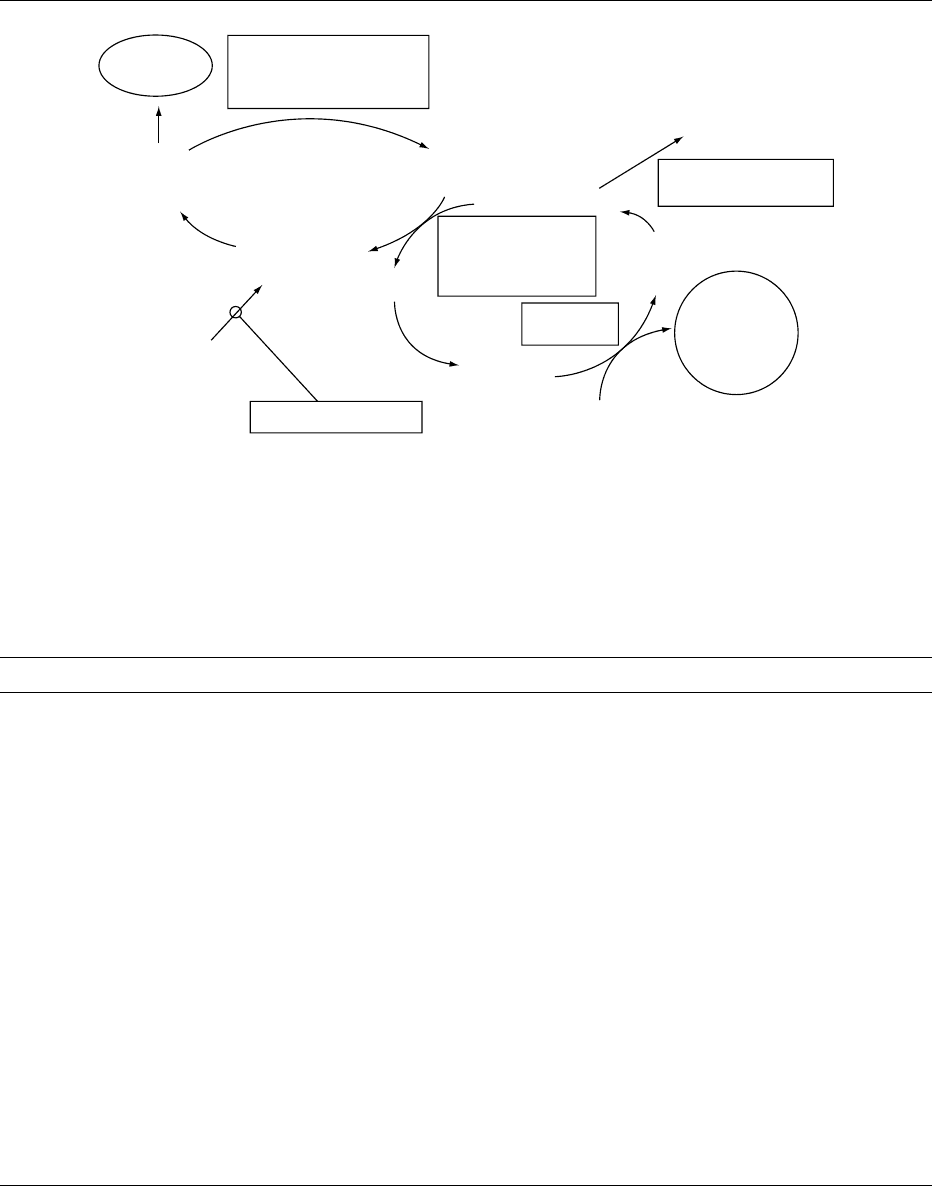
cysteine back to methionine (Figure 4). It is also a
cofactor for enzymes involved in DNA and RNA
synthesis, providing single carbon units for the
synthesis of nucleotide bases, a process that is essen-
tial to the rapid cell division that occurs in early fetal
development. Extrinsic folic acid may work by in-
creasing tissue folate levels enough to override a fail-
ure in folate metabolism, or it may compensate for
deficiency or metabolic defects related to other nutri-
ents closely related to folate metabolism. Recent re-
search has focused on the role of mutations in the
genes that code for enzymes involved in folic acid
metabolism.
Approaches to Increasing Folic Acid Consumption
0015Although the mechanism is unknown, a significant
proportion of NTDs can be prevented with folic acid.
The challenge is in how to translate science into public
health policy and practice. Table 1 summarizes three
approaches for increasing folic acid consumption.
Randomized trials
U.K. '81 (recurrence)
U.K. '83 (recurrence)
Cuba '90 (recurrence)
Observational studies
U.S. '88
U.S. '89
U.S. '89b
Australia '89
U.S. '93
U.S. '95
Community interventions
China '99 (North)
China '99 (South)
0 0.5 1 1.5
Estimated relative risk and 95% confidence intervals
2 2.5
U.K.-International MRC '91 (recurrence)
Hungary '92 (occurrence)
Non-randomized trials
fig0003 Figure 3 Risk of neural tube defects and use of folic acid or multivitamin supplements: summary of studies 1980–95, by country and
year of publication. The figure shows risk estimates (boxes) and 95% confidence intervals. Risk estimates < 1 indicate a reduction in
risk among the ‘exposed‘ mothers (periconceptional use of folic acid or multivitamins). If the upper limit of confidence intervals is > 1,
the risk estimate is not statistically significant. Some studies used folic acid (varying doses); some used multivitamins. Two
randomized controlled trials (UK’ 81 and UK-international-MRC’91) and two nonrandomized trials (UK’83 and Cuba’90) examined
the efficacy of folic acid with or without other vitamins among women with a previously affected pregnancy (recurrence). One
randomized trial (Hungary’92) assessed the efficacy of a multivitamin containing folic acid among women without a previously
affected pregnancy (occurrence). Of the observational studies, five (US’88, US’89, Australia’89, US’93, US’95,) were case-control
studies, whereas one (US’89b,) was an observational cohort. The community intervention study (China’99) was conducted in two
areas, one in Northern China and one in Southern China; it assessed the effectiveness of 0.4-mg folic acid supplements (without other
vitamins) among women without a previously affected pregnancy in areas of high (North) and low (South) occurrence rates of neural
tube defects. From Botto LD, Moore CA, Khoury MJ, and Erickson JD (1999) Neural-tube defects. New England Journal of Medicine 341:
1509–1519, with permission.
4740 PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects
Fortification of a food staple provides wide population
coverage at low cost without requiring behavior
change. The optimal fortification level is controver-
sial. Some experts had concerns that daily folic acid
intakes in excess of 1 mg could adversely affect some
persons, particularly persons with untreated cobala-
min deficiency. Folic acid can ameliorate the anemia
associated with cobalamin deficiency, possibly leading
to a failure to detect and treat the cobalamin
deficiency, which could result in the initiation or
Nucleotide
biosynthesis
5,10 methylene
tetrahydrofolate reductase
MTHFR
5,10 methylene
tetrahydrofolate
5 methyl
tetrahydrofolate
Tetrahydrofolate
Folic acid
Folic acid receptors
Methionine
Homocysteine
Methionine synthase
plus vitamin B
12
,
methionine synthase
reductase
Methyl
transferases
S-adenosyl
methionine
(SAM)
S-adenosyl
homocysteine
DNA, proteins, lipids
Methylated
DNA, proteins
lipids
Cystathionine synthase
plus vitamin B
6
Cystathionine
fig0004 Figure 4 Metabolic roles of folic acid and related dietary factors. Simplified schematic of some of the metabolic processes that
involve folic acid and other related factors. Folic acid (bottom left), after entering the cell (aided by folate receptors), participates in the
transfer of carbon units used for the synthesis of nucleotides (top left) or, through the conversion of homocysteine to methionine
(center), for methylation purposes. These processes are regulated by many factors including enzymes (in rectangular boxes) and
vitamins other than folic acid (e.g., vitamins B
6
and B
12
). The activity of some enzymes (e.g., methionine synthase) may be influenced
by other enzymes (e.g., methionine synthase reductase). Adapted from Botto LD, Moore CA, Khoury MJ, and Erickson JD (1999)
Neural-tube defects. New England Journal of Medicine 341: 1509–1519, with permission.
tbl0001 Table 1 Ways to increase folic acid/folate consumption to prevent neural tube defects
Approach Advantages Disadvantages Status
Fortify staple foods Proven to increase blood
folate level
Reaches almost all women
Behavior change not
necessary unless
higher intakes needed
Inexpensive
All consumers (not just target
population) increase intake;
concern that some will have
excess intake
Variable staple consumption
results in variable folic acid
intake
Sustained behavior change
required for consumption of
higher amounts
Mandatory fortification
in the USA, Canada, and several
Central and South American
and eastern European
countries; proposed in the UK
Increase use of
supplements
Efficacy proven by clinical
trials
Proven to increase blood
folate level
Relatively inexpensive
Requires sustained behavior
change
Reservations of some medical
and nutritional professionals
Varies by country and survey
question (e.g., in the USA, 30% of
reproductive-age women report
regular use; in The Netherlands,
54% of women report
‘any periconceptional use‘
and 21% ‘appropriate use‘)
Increase consumption of
foods with high levels
of natural folates (e.g.,
fruits and vegetables)
Other benefits of healthy
diet that includes
fruits and vegetables
Efficacy not proven
Much smaller increases in
blood folate levels than
supplements or fortified foods
Requires significant and
sustained behavior change
May be expensive
Various healthy diet campaigns
under way
PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects 4741

progression of neuropathy. Although some experts in
the study of birth defects advocated a higher fortifica-
tion level, the US Food and Drug Administration ruled
that, effective January 1, 1998, all flour, corn meal,
pasta, and rice labeled as ‘enriched‘ be fortified with
folic acid at 140 mg per 100 g of cereal grain product.
Canada and several Central and South American and
eastern European countries also have mandated forti-
fication of wheat flour. The fortification level in some
countries (e.g. Chile) was established at a higher level,
with the goal of achieving a higher average daily intake
of folic acid. In 2000, the UK Committee on Medical
Aspects of Food and Nutrition Policy recommended
folic acid fortification at 240 mg per 100 g of flour. At
the time of writing, this proposal is under review but
not yet approved, although voluntary optional fortifi-
cation is allowed in the UK. Serum and red blood cell
folate levels among reproductive aged women in the
USA have more than doubled since fortification of
cereal grain products. In addition, preliminary ana-
lyses suggest an approximate 20% decline in NTD
rates postfortification.
0016 Although multivitamin supplements containing
folic acid are of proven efficacy in preventing NTDs,
their use requires a sustained behavior change by
most women. Educational campaigns in the USA
have increased awareness and knowledge about folic
acid more than they have increased actual supplement
use. In 2001, although 80% of childbearing aged
women in the USA had heard of folic acid, only
29% took a daily vitamin containing folic acid, up
only slightly from 25% in 1995. In the UK and in The
Netherlands, public-awareness campaigns signifi-
cantly increased both knowledge about, and use of,
folic acid. For example, after a 1995 campaign in
The Netherlands, use of folic acid for ‘any period
around conception‘ increased from 25% before the
campaign to 54% after, and ‘appropriate‘ use in-
creased from 5 to 21%. Whether increases in supple-
ment use can be sustained and whether levels of use
plateau at a certain level is unknown. Supplement use
is less common among younger women, less educated
women, and those with lower incomes – populations
that are often harder to reach through health educa-
tion efforts.
0017 Attempts to increase population consumption of
folate-rich foods (e.g., fruits and vegetables) through
programs like the ‘Five-a-Day‘ campaign in the USA
have generally resulted in only modest increases. One
small study found that neither dietary advice nor
folate-rich foods significantly increased women’s red
cell folate levels, whereas supplements and fortified
foods did. This could result from the lower bioavail-
ability of food folate and/or the challenges of making
dietary behavior changes.
Folate-related Nutrients
0018As noted previously, the preventive effects of folate
supplementation are more likely to result from its
compensation for metabolic errors closely related to
folate metabolism, rather than overt folate deficiency.
Folate is involved in an intricate network of reactions
that include many enzymes, nutrients, and other sub-
strates that could affect NTD risk through a variety of
mechanisms (Figure 4). The conversion of 5-methyl
tetrahydrofolate to tetrahydrofolate produces the
substrate necessary for the transmethylation of
homocysteine to methionine; the enzyme methionine
synthase (MS) catalyzes the reaction, and vitamin B
12
is a cofactor for this enzyme (Figure 4). Homocysteine
may also be metabolized to cystathionine via
cystathionine b synthase (CBS), of which vitamin B
6
is a cofactor.
0019Hyperhomocysteinemia, which has been shown to
cause NTDs in animal models, may reflect impaired
metabolism of folate, B
12
,B
6
, or homocysteine, may
reflect a defect in the enzymes 5,10-methylenetetra-
hydrofolate reductase (MTHFR), MS, or CBS, or
may be harmful on its own. Several studies have
reported an increased NTD risk associated with
high homocysteine levels in humans, in the amniotic
fluid of mothers carrying affected fetuses, in maternal
serum during pregnancy and postpartum, and among
children with NTDs, although results have not been
entirely consistent.
0020Animal models indicate that methionine is also
important to neural tube closure. Although the mech-
anism is unknown, methionine is necessary for
protein synthesis and transmethylation reactions.
Two population-based, case-control studies have
reported a 30–50% reduction in risk for NTDs with
increasing quartiles of methionine intake. Other stud-
ies have been inconsistent: some have demonstrated
higher levels of methionine in the amniotic fluid of
mothers carrying NTD-affected fetuses, whereas an-
other study reported no difference in maternal serum
methionine post-partum.
0021Several studies have indicated lower levels of vita-
min B
12
in the amniotic fluid and serum of women
with affected pregnancies. Studies of methyl malonic
acid (an indicator of B
12
deficiency or a defect in B
12
metabolism) and B
12
carrier proteins also suggest a
defect in B
12
metabolism among case mothers. Other
studies have not supported these differences or have
been inconsistent in their findings depending on the
timing of and tissues used for measurement. Although
the results are mixed, they do not seem to provide
strong evidence for a relation between B
12
deficiency
and NTD risk. Few studies have examined the asso-
ciation between vitamin B
6
and risk for NTDs;
4742 PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects

significant differences have not been observed, but
studies have involved only small sample sizes.
0022 There is some evidence that polymorphisms in the
genes for MTHFR, MS, and CBS contribute to altered
levels of these nutrients and to NTD risk, but again,
results have been mixed.
0023 The individual contributions of each of these indi-
cators of metabolic disturbances to NTD risk, and
their interdependence, are unclear at this point.
Folic acid supplementation might play a role in over-
coming the negative effects of many of these disturb-
ances. However, until the exact causes of NTDs are
determined, the understanding of the implications of
these findings and the way in which they should be
used for prevention purposes remains limited.
Other Nutrients
0024 At least 30–50% of NTDs are folate-resistant; there-
fore, other nutrients have been implicated as possible
causes of these cases. The evidence for the role of
vitamin A, zinc, and inositol in NTD etiology is
reviewed here. Other nutrients – including vitamin
C, riboflavin, iron, calcium, magnesium, selenium,
lead, and copper – also may be associated with
increased NTD risk, but evidence is very limited.
0025 The finding that isotretinoin, a synthetic derivative
of vitamin A, is teratogenic led to investigations of
whether naturally derived vitamin A is associated
with increased risk for NTD-affected pregnancy.
Most studies have found no evidence of an associ-
ation of high vitamin A levels with NTD risk, based
on intake from foods and supplements and on serum
samples taken during the first trimester of pregnancy
or postpartum. The safe level of vitamin A intake is
still debatable, in part because of its potential associ-
ation with other types of malformations and its
association with other negative health outcomes.
The effects of deficient vitamin A intake on NTD
have not been explored.
0026 Zinc is important to cellular growth and differenti-
ation and to folate absorption. Various experimental
studies in animals and case reports of women with
specific disturbances of zinc metabolism have sug-
gested an association between zinc and increased
risk for NTD-affected pregnancy. Results for analytic
studies of zinc and NTDs in humans are inconsistent.
Postpartum studies have reported NTD case mothers
to have levels of zinc in the hair that were higher,
lower, or the same as those in control mothers, higher
levels in toenails, and the same as control mothers
in serum levels. Studies of pregnant women have
reported that mothers with NTD-affected pregnan-
cies have higher levels of zinc in serum, lower levels in
white blood cells, and lower dietary intakes, whereas
other studies have reported no difference in serum
or amniotic fluid. Despite the number of studies,
inference is limited by the wide variability in zinc
measurement and by the limited understanding of
the relationships between these measures.
0027Inositol is a 6-carbon polycyclic alcohol that is
present in all cells, with especially high levels in
nerve cells. It protects against NTDs in the curly-
tailed mouse, a folate-resistant NTD model, leading
some researchers to recommend supplementation
with a combination of folate and inositol. However,
the applicability of these findings to humans has not
been studied.
Limitations
0028In general, the proposed associations reviewed here
are biologically plausible and supported by animal
models. Unfortunately, systematically testing these
associations in humans is difficult, and most existing
evidence is clinical or experimental and speculative.
Sample sizes for many of the studies have been small
(often involving < 20 case-patients). Study population
characteristics and selection methods have been
highly variable; very few have been population-
based. Few studies have adjusted for potential con-
founding or effect modification by other maternal
characteristics, including status with respect to other
nutritional factors or individual nutrients.
0029The ability to measure maternal nutritional status
is also limited. Because pregnancy is a time of tremen-
dous metabolic change, the ability of measurements
taken later in pregnancy to represent the status during
the time of neural tube closure is questionable. For
example, the fetal contribution to levels of nutrients
in amniotic fluid is uncertain and may vary by timing
of measurement and by nutrient. Also, many women
begin taking multivitamin/mineral supplements soon
after the time of neural tube closure.
0030The cause of observed variability in nutrient
levels is usually unknown, limiting the understanding
of how to use such information for preventive
measures. Nutrient metabolism is highly complex,
and many reactions are interdependent. For example,
depending on their cause, high homocysteine levels
could be remedied with supplementation of B
12
, me-
thionine, folate, or B
6
; low calcium intake may result
in increased bioavailability of lead, reduced bioavail-
ability of vitamin B
12
, and, accordingly, reduced me-
thionine synthase activity; and calcium, fiber, protein,
and methionine are all important to zinc bioavailabil-
ity. Therefore, it is critical that future studies examine
interrelationships, including nutrient–nutrient inter-
actions as well as gene–nutrient interactions, when-
ever possible.
PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects 4743
Other Nutritional Factors
0031 Evidence for a link between tea and NTDs is weak. A
study in England and Wales showed an excess of
anencephaly among women drinking three or more
cups of tea per day, but no dose–response effect was
observed, and the relation was observed only in
regions with higher NTD prevalence rates. Further-
more, a study in Boston, Philadelphia, and Toronto
found no elevated risk for NTDs associated with tea
drinking. Nor is the link between coffee and NTDs
strong. In the Boston study, no significant differences
in coffee consumption were observed between the
mothers of NTD-affected infants and control
mothers. Also, no association with decaffeinated
coffee or cola drinks has been found. A Finnish
study found no association between central nervous
system defects and coffee intake. Although there are
case reports of NTDs occurring among infants of
mothers who consumed significant amounts of
alcohol during pregnancy, epidemiologic studies
have provided little evidence for a link between
NTDs and alcohol, especially for mothers consuming
minimal or moderate amounts.
0032 Some food contaminants have been proposed to
be NTD teratogens. Potato blight, caused by a fungus
(Phytophthora infestans) that rots potatoes, was
hypothesized to cause NTDs in the early 1970s,
although most evidence does not support this hypoth-
esis. Fumonisin, a potent mycotoxin prevalent in corn
and a carcinogen and cause of various animal diseases
has been suggested as a possible cause of high NTD
rates among persons living along the Texas–Mexico
border who commonly consume corn products.
Recent research suggests that fumonism may be
involved in NTD formation by inhibiting folate
uptake by cells. Also, fumonisins have been shown
to produce NTDs in mouse whole embryo cultures;
folic acid has ameliorated this teratogenic effect.
More research is needed to establish the link between
fumonisin consumption and NTD risk in humans.
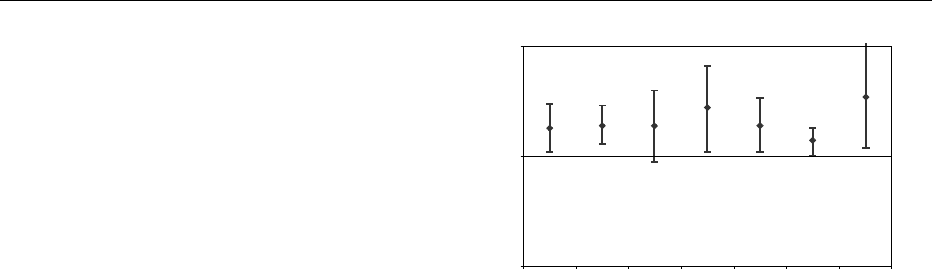
0033 About one-fourth of childbearing age women in the
USA and almost as many such women in Canada, the
UK, and Continental Europe, are obese, and obesity
prevalence is increasing rapidly. Studies consistently
find a twofold elevated risk for NTDs among children
of obese women compared with mothers of average
weight, although risk estimates vary with the body
mass index cutoffs and referent groups used
(Figure 5). Most studies found a higher risk estimate
for spina bifida than anencephaly and found no risk
elevation for encephalocele. Reasons for the increased
risk are unknown. Potential explanations include
teratogenic metabolic abnormalities associated with
obesity including elevated levels of glucose, insulin,
uric acid, and endogenous estrogens. Obese women
may be more likely to be nutritionally deficient be-
cause of a self-imposed diet restriction, poor choice of
foods, or increased requirement for folate or other
nutrients. More studies are needed to help elucidate
the mechanism. The population burden of NTDs as-
sociated with obesity is substantial and increasing.
Conclusion
0034There is still much to be learned about the complex
link between nutrition and birth defects. Evidence is
emerging regarding the role of nutritional factors in
the etiology of birth defects other than NTDs (e.g.,
heart defects and orofacial clefts). Despite the chal-
lenges in studying nutritional causes of birth defects,
the prevention potential is substantial and worthy of
pursuit.
See also: Cobalamins: Properties and Determination;
Folic Acid: Properties and Determination; Physiology;
Food Fortification; Nutritional Assessment:
Importance of Measuring Nutritional Status;
Anthropometry and Clinical Examination; Biochemical
Tests for Vitamins and Minerals; Functional Tests;
Obesity: Epidemiology; Retinol: Properties and
Determination; Physiology; Vitamins: Determination;
Zinc: Properties and Determination; Physiology;
Deficiency
Further Reading
Anonymous (2000) Folic acid and the prevention of disease.
Report of the Committee on Medical Aspects of Food
0.1
US, BMI > 31
Odds ratio
US, BMI > 29
US, BMI > 28-32
US, BMI > 32
US, BMI > 29
Sweden, BMI > 26
US, BMI > 30
1
1.8
1.9 1.9
2.8
1.9
1.4
3.5
10
fig0005Figure 5 Risk of neural tube defects in offspring of obese
women, odds ratios, and 95% confidence intervals. All studies
except one (Sweden) were performed in the USA. The body
mass index (BMI) used to define obesity varied (see x-axis).
The referent group was average-weight or nonobese women.
4744 PREGNANCY/Maternal Diet, Vitamins, and Neural Tube Defects