Caballero B. (ed.) Encyclopaedia of Food Science, Food Technology and Nutrition. Ten-Volume Set
Подождите немного. Документ загружается.

0010 The discovery of fluoride (known to act as a proto-
plasmic poison in some circumstances) as the causa-
tive agent in mottling of the teeth was a cause of
concern to the US Public Health Service. In response
they appointed a dentist, H Trendley Dean, to investi-
gate the condition. Dean devised a six-point scale of
severity of dental fluorosis which is still used today.
Dean’s index facilitates regional and international
comparisons of dental fluorosis as well as
temporal comparisons. However the index is rela-
tively subjective and the appearance of enamel varies
according to lighting conditions, drying of the
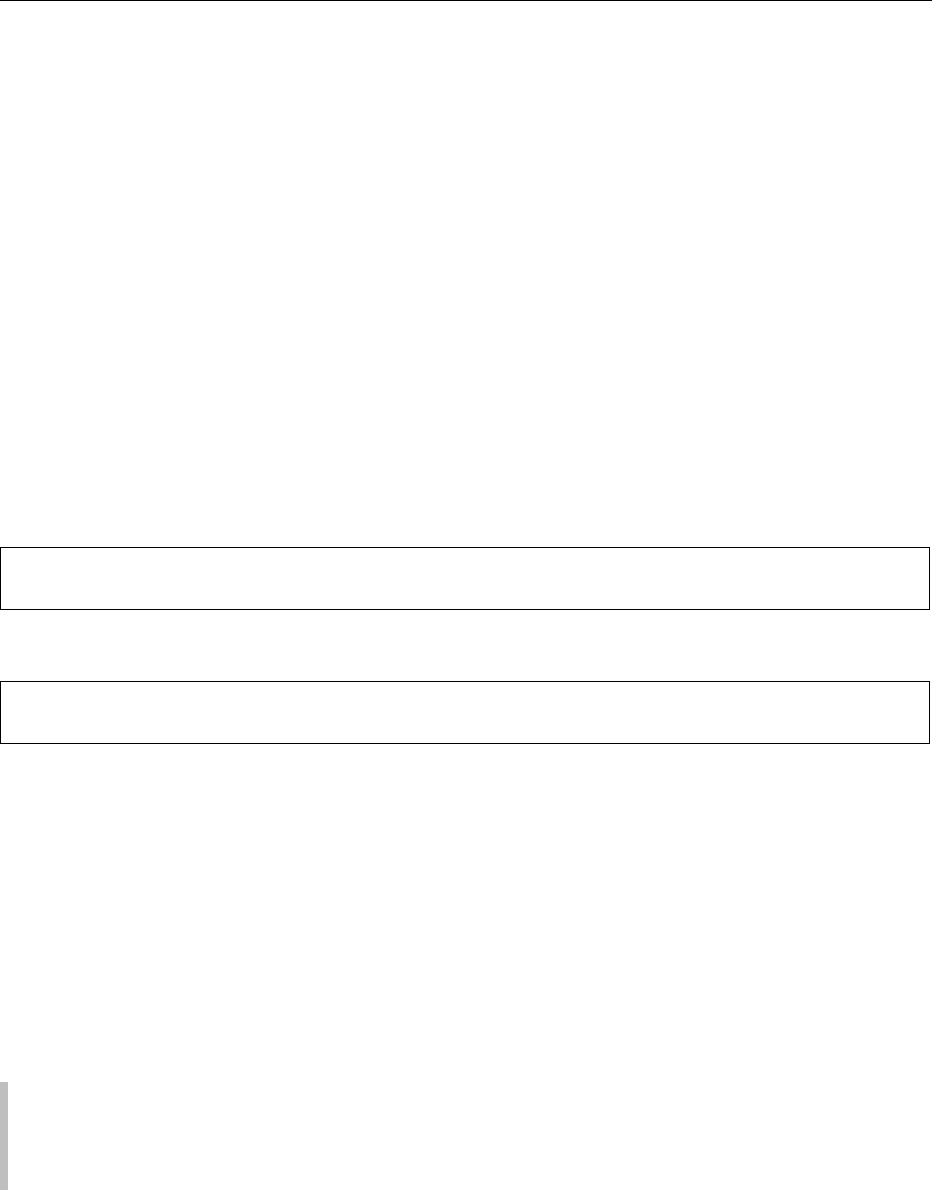
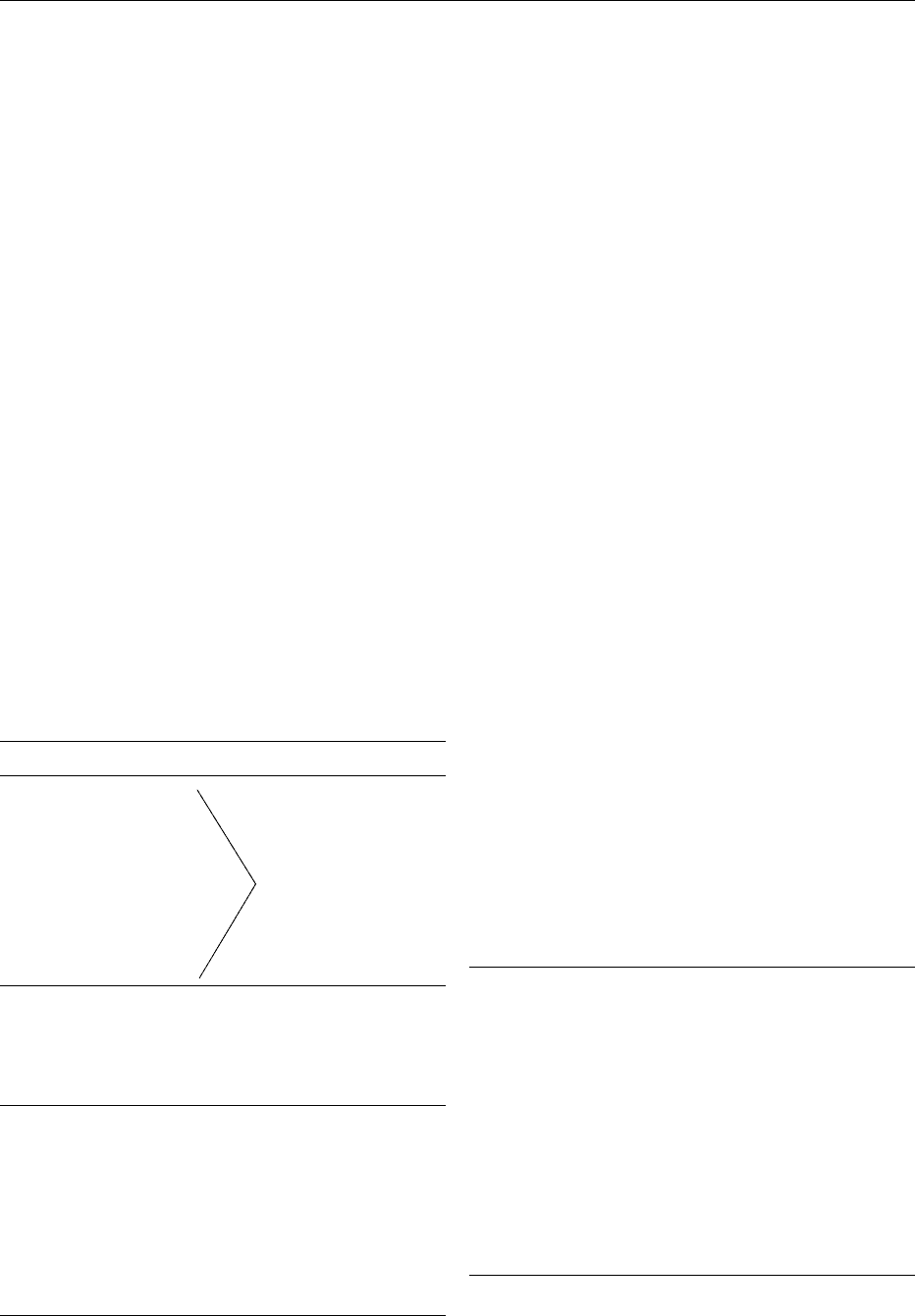
enamel, and angulation of viewing. Dean’s index cat-
egorizes the enamel into normal, questionable, very
mild, mild, moderate, and severe (Figure 1). Some of
the limitations of Dean’s index have since been over-
come by the development of a standardized photo-
graphic method for the recording of dental fluorosis.
0011 Dean combined measurement of the condition of
the enamel with analysis of the drinking water
throughout the USA. He then set out to identify the
water fluoride levels, which represented the best com-
promise between low caries experience and a level of
fluorosis, which could be deemed acceptable. The
resulting study became known as the ‘21 cities’
study. Dean recorded the level of dental caries and
dental fluorosis in 7257 12–14-year-old children who
had been lifetime residents of 21 cities with varying
levels of natural fluoride in their water supplies from
0.0 to 2.6 ppm.
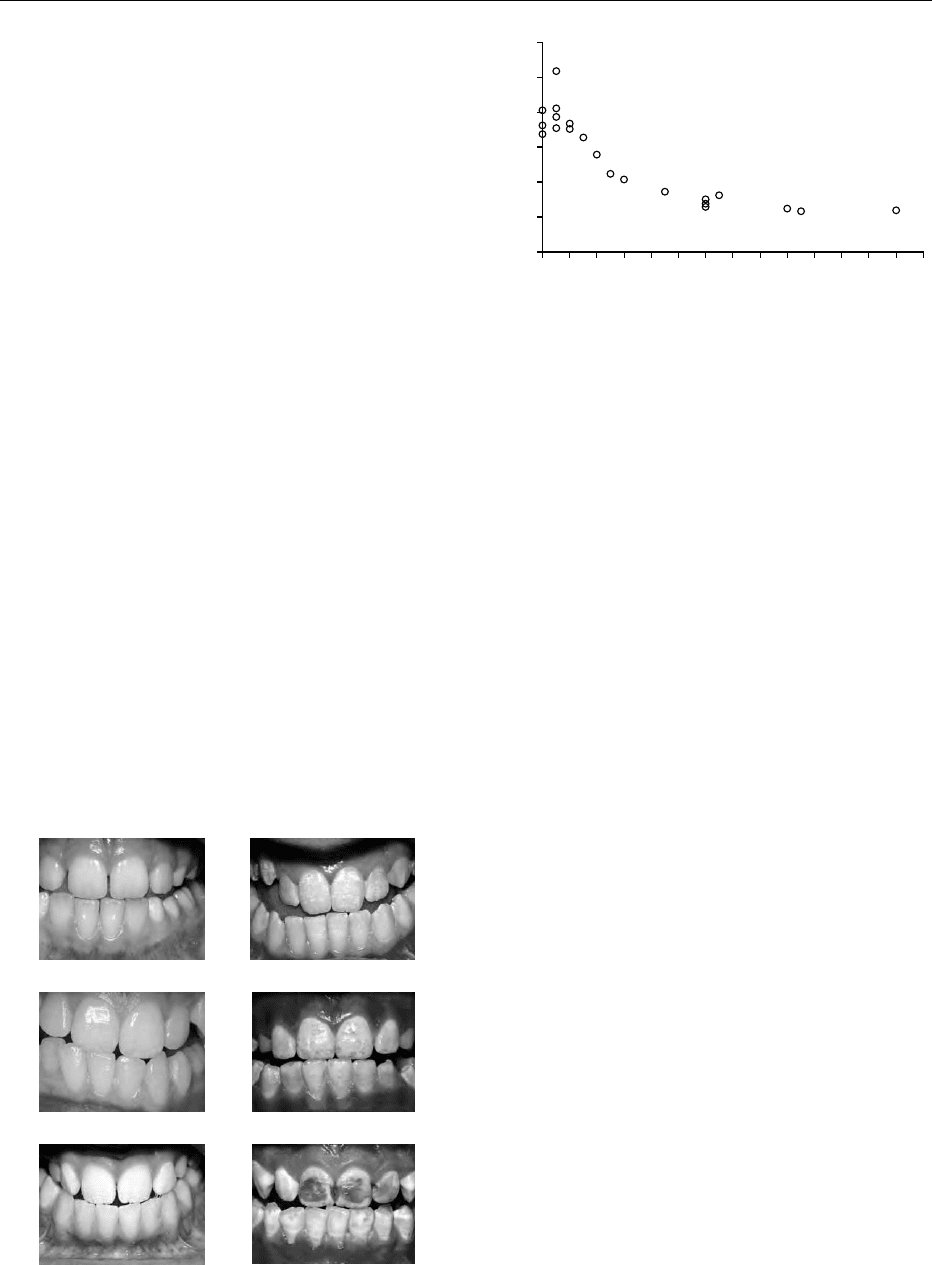
0012 The marked inverse association between the fluor-
ide content of the drinking water and the experience
of caries in the population is shown in Figure 2. This
study showed that, above a concentration of 1 ppm
fluoride in the water, very little further reduction in
caries was obtained. Dean also illustrated the dose–
response relationship between water fluoride levels
and dental fluorosis in the ‘21 cities study.’ He
found that, where the fluoride concentration exce-
eded 1.0 ppm, undesirable mottling would be seen
in about 10% of the population.
0013In 1945 and 1946 four cities in the USA and
Canada began to add fluoride to their water supplies
at a concentration of 1 ppm as part of the first con-
trolled field trials of water fluoridation. The fluorid-
ation of water to 1 ppm reduced the number of
carious teeth per child by on average 60% relative
to children in nonfluoridated cities.
Fluoridation Worldwide
0014Throughout the world it is estimated that about 317
million people drink artificially fluoridated water and
that a further 40 million drink water in which the
natural fluoride level is high enough to provide a
significant degree of protection against tooth decay.
Countries with fluoridation schemes include the
USA, Canada, Mexico, Argentina, Ireland, UK, Spain,
Australia, New Zealand, Hong Kong, and Singapore.
0015The USA is the most extensively fluoridated coun-
try in the world, with some 135 million people – over
half the population – currently receiving artificially
fluoridated water and another 10 million receiving
naturally fluoridated water. The national health pro-
motion and disease prevention objectives in Healthy
People 2010 call for increasing the percentage of
Normal
Questionable
Very mild
Mild
Moderate
Severe
fig0001 Figure 1 (see color plate 46) Categories of dental fluorosis
according to Dean’s index.
0
0
2
4
6
8
10
12
0.2 0.4 0.6 0.8 1 1.2
Fluoride content of the public water supply (ppm)
Mean number of teeth decayed,
missing and filled due to caries
1.4 1.6 1.8 2 2.2 2.4 2.6 2.8
fig0002Figure 2 The relation between caries levels observed in 7257
selected 12–14-year-old white school children of 21 cities of four
states and the fluoride content (ppm, horizontal scale) of
public water supply. Open circles, DMFT (mean number of
teeth decayed, missing, and filled due to caries). (Reproduced
from F.J. McClure (ed.) (1962) Fluoride Drinking Waters, by kind
permission of the National Institute of Dental and Craniofacial
Research).
1756 DENTAL DISEASE/Fluoride in the Prevention of Dental Decay

Americans on public water supplies drinking fluorid-
ated water from 62 to 75%.
0016 Within the European Community (EC), the UK,
Ireland, and Spain are currently operating fluorid-
ation schemes. In Ireland, fluoridation of public water
supplies is mandatory. An EC directive relating to the
quality of water intended for human consumption (98/
83/EC) sets a maximum admissible concentration
(MAC) for fluoride at 1.5 parts of fluoride per million
parts of water, irrespective of climate.
0017 Some countries, such as France, Switzerland, and
Germany, have implemented salt fluoridation.
Fluoride Ingestion and Absorption
0018 Approximate estimates for daily dietary fluoride
intake are shown in Table 1. It is estimated that 75–
90% of daily fluoride intake is absorbed. Of that
absorbed, the amount excreted varies; it is estimated
that on average approximately 50% of absorbed
fluoride is excreted, primarily by the kidneys in
urine. In the very young more fluoride is retained.
Most retained fluoride is deposited in bone because
of its strong affinity for calcium.
0019 Assessing fluoride levels in plasma, ductal saliva, or
in urine can help monitor recent total fluoride expos-
ure of individuals or populations. Research is ongoing
into the use of fingernail clippings as a biomarker for
fluoride intake some weeks prior to clipping. Dental
fluorosis is a convenient biomarker for fluoride
intake; however it is relevant only to the first 6 years
of life. Dental fluorosis is a convenient biomarker for
fluoride intake, however it is relevant only to the first
6 years of life. Dental hard tissues provide a marker
for fluoride exposure during defined developmental
periods. Bone provides information on the accumu-
lated body burden of fluoride over a lifetime.
Fluoride Toothpastes
0020 Studies of the effectiveness of fluoride toothpaste in
the 1940s and early 1950s failed to demonstrate a
caries-preventive effect. It is now believed that the
sodium fluoride was not bioavailable due to a reac-
tion with the calcium carbonate or calcium orthopho-
sphate abrasive in the formulation. Since the 1950s
studies of 2–3 years’ duration have reported that
fluoride toothpaste reduces caries experience among
children by a median of 15–30%. A dose–response
relationship has been demonstrated showing greater
caries-preventive effects for higher-dose fluoride
toothpaste. The two most commonly used forms of
fluoride added to toothpaste are sodium fluoride
(NaF) and sodium monofluorophosphate (MFP).
There are many different formulations of fluoride
toothpaste on the market. The concentration of fluor-
ide in toothpastes varies from 250 to 2800 ppm. The
most commonly sold toothpastes contain 1000–1500
ppm. In the European Union the maximum permis-
sible concentration in fluoride toothpaste to be sold
over the counter is 1500. Hence toothpaste formula-
tions with greater than 1500 ppm fluoride are avail-
able at pharmacies only.
0021Manufacturers commonly list fluoride levels in
toothpaste as a percentage. Table 2 shows the com-
mon percentages of NaF and NaMFP found in tooth-
pastes, expressed as ppm in toothpaste.
0022Fluoride toothpaste contributes to the risk of
enamel fluorosis because the swallowing reflex of
children aged under 6 years and especially in those
aged under 3 years is not well controlled. Early use of
fluoride toothpaste by children is associated with the
development of dental fluorosis. Ingestion of exces-
sive amounts of toothpaste during the period of
enamel formation can cause fluorosis. Enamel forma-
tion for all of the anterior teeth and most of the
posterior teeth is complete by age 7. The critical
window of vulnerability for anterior teeth to develop
fluorosis from ingested fluoride has been reported to
be 15–24 months for boys and 21–30 months for
girls. The amount of toothpaste used accounts
for an estimated 60% of the variation in the amount
of toothpaste swallowed by children under age 7. It
takes 0.75–1.0 g of toothpaste to cover a full head of a
child-sized toothbrush. For a 1000 ppm toothpaste,
this represents 0.75–1.0 mg fluoride. To minimize
toothpaste ingestion up to age 7, manufacturers
advise supervision and use of only a pea-sized amount
of toothpaste (0.25 g). Many experts also recommend
that toothpaste should not be used when brushing
children’s teeth up to the age of 2 years. The risk of
ingesting fluoride toothpaste has led to the develop-
ment of low-fluoride pediatric toothpastes with 250
or 550 ppm fluoride. These toothpastes have not been
shown to be as effective in preventing caries as the
tbl0001 Table 1 Estimated daily fluoride intake from dietary sources
Fluoridated area Nonfluoridatedarea
Adults 1.0–3.0 mg 1.0 mg
Children 0.5 mg 0.25 mg
tbl0002Table 2 NaF and NaMFP found in toothpastes, expressed as
percentages and as ppm in toothpaste
NaF (%) NaMFP(%) ppm
0.32 1.14 1500
0.22 0.76 1000
0.11 0.38 500
DENTAL DISEASE/Fluoride in the Prevention of Dental Decay 1757

1000 ppm formulation. Over the age of 7 years, when
there is little risk of swallowing toothpaste, children
who are able to expectorate the toothpaste properly
may be allowed to use a greater quantity of tooth-
paste with up to 1500 ppm fluoride.
Other Fluoridated Products
0023 Many other vehicles for the delivery of fluoride for
the prevention of dental caries have been shown to
be effective. Under the appropriate circumstances,
fluoridated salt (250 ppm) has been shown to be as
effective as water fluoridation. Fluoridated domestic
salt is available in Switzerland, France, and Germany.
Fluoridated milk and sugar have been tested on a pilot
basis. Among the other products available are fluoride
tablets for daily use, drops, mouth rinses for daily
(0.05% NaF, 230 ppm) or fortnightly (0.2% NaF,
910 ppm) use, and products for application by dental
professionals, including topically applied gels and var-
nishes. Applying fluoride gel (2.72% NaF, 12 300
ppm) or other products containing a high concentra-
tion of fluoride to the teeth leaves a temporary layer of
calcium fluoride-like material on the enamel surface.
The fluoride in this material is released when the pH
drops in the mouth in response to acid production and
is available to promote enamel remineralization.
Dental filling materials have also been developed
which release fluoride over time; however, fluoride
release is limited to a relatively short period after
placement. Other products have also been developed
for placement in the mouth which would slowly release
fluoride over months, if not years. Human clinical trial
data on the effectiveness of these products are not yet
available. Fortnightly school-based fluoride mouth
rinse programs for the prevention of dental caries
have been shown to be successful for the duration of
the program. However in programs that cease at age
12, the effects have been shown to fade after 4 years.
Mechanism of Action of Fluoride in the
Prevention of Dental Caries
0024 Dental enamel is a highly mineralized tissue made up
of 96% mineral and 4% organic material and water.
The inorganic content of enamel consists of a crystal-
line calcium phosphate known as hydroxyapatite.
The dissolution of these crystals by acid is the start
of the caries process. Fortunately, enamel can remi-
neralize as well as demineralize and the enamel sur-
face is in a constant seesaw between demineralization
and remineralization. Saliva provides a supersatur-
ated solution of ions and acts as an ion reservoir
during this process. When the equilibrium is dis-
turbed, caries can progress.
0025In the early days scientists thought that the anti-
caries activity of fluoride was a preeruptive systemic
effect as a result of its incorporation into the enamel
crystal to form fluorapatite during the time of enamel
formation. This crystal is more stable and resistant to
acid demineralization than hydroxyapatite. However,
investigators have failed to show a consistent correl-
ation between anticaries activity and the specific
amounts of fluoride incorporated into the enamel.
The theory of preeruptive fluoride incorporation as
the sole or principal mechanism of caries prevention
has been largely discounted. Another theory was that
fluoride inhibits bacterial metabolism; however, the
low levels of fluoride found in the mouth after tooth-
brushing with fluoride-containing dentifrices are in-
effective in interfering with processes of growth and
metabolism of bacteria. The current theory is that the
caries-preventive effect of fluoride is mainly attrib-
uted to the effects on demineralization/remineraliza-
tion at the tooth–oral fluids interface. Levels well
under 1 ppm of fluoride in saliva are effective in
shifting the balance from demineralization, leading
to caries, to remineralization. This is attributed to
the fluoride-enhanced precipitation of calcium phos-
phates, and the formation of hydroxyfluorapatite in
the dental tissues.
Benefits and Risks of Fluorides in
Contemporary Society
0026In the 1950s and 1960s dental caries was an over-
whelming problem in many countries. For example,
in Ireland prior to the introduction of water fluorid-
ation, in the early 1960s 12-year-old children had
on average five teeth with decay. In the 1990s 12-
year-old children whose domestic water supplies
were fluoridated had on average one decayed tooth,
and those without water fluoridation had on average
two decayed teeth. The dramatic decline in the level of
caries both in fluoridated and nonfluoridated areas
reflects changes seen in the other established market
economies.
0027Whilst early studies reported up to a 60% reduc-
tion in caries with water fluoridation, more recent
estimates of effectiveness are lower with an 18–40%
difference in caries levels. This apparent reduction in
effectiveness is probably due to the widespread use of
fluoridated toothpaste in both fluoridated and
nonfluoridated communities. In addition, the con-
sumption of foods and drinks manufactured using
fluoridated water and consumed in nonfluoridated
areas may confer some protection against dental
caries to populations in nonfluoridated areas. This is
known as the halo effect. Thus, where nonfluoridated
communities are exposed to fluoride from sources
1758 DENTAL DISEASE/Fluoride in the Prevention of Dental Decay

other than water, the observed effectiveness of water
fluoridation is reduced. In Ireland water fluoridation
was introduced in the 1960s and the use of fluorid-
ated toothpastes became widespread in the 1970s.
Whilst the level of caries has declined, the prevalence
of fluorosis amongst Irish children appears to have
increased since the 1980s when it was first measured.
The alteration in the pattern of caries, the changes in
the severity of the disease, and the use of multiple
sources of fluoride have prompted a number of
reviews of the risks and benefits of fluoridation. In
2000 the University of York presented a systematic
review of the evidence on the positive and negative
effects of population-wide drinking-water fluoridat-
ion strategies to prevent caries. The review summ-
arized the best available and most reliable evidence
on the safety and efficacy of water fluoridation. Of all
the studies found in the literature search, 214 satisfied
the inclusion criteria for consideration in the ap-
praisal of the evidence. Outcomes for the five object-
ives of the review are shown in Table 3.
0028 The reviewers were critical of the lack of high-
quality research on water fluoridation. They recom-
mended: ‘the evidence of a benefit of a reduction in
caries should be considered together with the
increased prevalence of dental fluorosis.’
0029 Those who oppose water fluoridation do so on
three main grounds:
1.
0030 the effectiveness of water fluoridation in prevent-
ing caries in contemporary society
2.
0031 the safety of water fluoridation. Concerns around
the general health effects of fluoride have been
raised. For example, fluoride has a high affinity for
calcium and most fluoride, which is absorbed and
not excreted, is deposited in bones, hence, the effect
of fluoride on bone health has been questioned
3.
0032the ethics of administering fluoride through the public
water supply and removal of the right to choose
whether one’s water supply is fluoridated or not
With regard to effectiveness, the current evidence con-
tinues to demonstrate a positive protective effect of water
fluoridation against dental caries. Concerning safety,
studies have failed to find harmful effects of water fluorid-
ation at 1 ppm. Finally, the ethical debate is a philosoph-
ical one and is outside the scope of this paper.
Conclusion
0033Fluoride has been shown to be effective in the control
of dental caries. Its effect is mainly topical at the
plaque–enamel interface. The aim of fluoride therapy
is to maintain the ambient level of the fluoride ion in
the saliva at a constant optimum level. The evidence
suggests that the effects of fluoridated water and
fluoride toothpaste are additive. However, the risk
associated with excessive ingestion and absorption
of fluoride is the development of dental fluorosis.
See also: Fluoride; Water Supplies: Chemical Analysis
Further Reading
Evans RW and Darvell BW (1995) Refining the estimate of
the critical period for susceptibility to enamel fluorosis
in human maxillary central incisors. Journal of Public
Health Dentistry 55(4): 238–249.
tbl0003 Table 3 Objectives and conclusions of the systematic review of public water fluoridation conducted by the NHS Centre for Reviews
and Dissemination, University of York, 2000
Objective Number of studies
includedinreview
Conclusion
The effects of
fluoridation of drinking water supplies
on the incidence of caries
26 The best available evidence
suggests that fluoridation of
drinking water supplies
does reduce caries prevalence
The effect over and above that offered by
the use of alternative interventions
and strategies
9 Water fluoridation has an
additional beneficial effect
The effect of water fluoridation on
levels of caries across social groups and
between geographical locations
15 Inconclusive evidence
Negative effects
Fluorosis 88 Yes, dose–response relationship with
water fluoridation
Bone fracture and bone
development problems
29 No association found
Cancer 26 No association found
Other negative effects 33 No clear association found
Differences in the effects of
natural and artificial water fluoridation
Not enough evidence to draw conclusions
DENTAL DISEASE/Fluoride in the Prevention of Dental Decay 1759
Fejerskov O, Ekstrand J and Burt BA (1996) Fluoride in
Dentistry, 2nd edn. Copenhagen: Munksgaard.
Fluorine in web elements. http://www.webelements.com.
Holland TJ, Whelton H, O’Mullane DM and Creedon P
(1995) Evaluation of a fortnightly school-based sodium
fluoride mouthrinse 4 years following its cessation.
Caries Research 29(6): 431–434.
Mascarenthas AK and Burt BA (1998) Fluorosis risk from
early exposure to fluoride toothpaste. Community
Dental and Oral Epidemiology 26(4): 241–248.
Murray JJ, Rugg-Gunn AJ and Jenkins AN (1991) Fluorides
in Caries Prevention, 3rd edn. Oxford: Wright.
NHS CRD (2000) A systematic review of public water
fluoridation. Report 18. York: NHS Centre for Reviews
and Dissemination, University of York.
Taves DR (1983) Dietary intake of fluoride ashed (total
fluoride) v. unashed (inorganic fluoride) analysis of indi-
vidual foods. British Journal of Nutrition 49: 295–301.
ten Cate JM (1999) Current concepts on the theories of the
mechanism of action of fluoride. Acta Odontologica
Scandinavica 57: 325–329.
US Department of Health and Human Services (2000)
Healthy People 2010. Washington: US Department of
Health and Human Services.
US Department of Health and Human Services (2000) Oral
Health in America: A Report of the Surgeon General.
Rockville, MD: US Department of Health and Human
Services, National Institute for Dental and Craniofacial
Research, National Institute of Health.
US Department of Health and Human Services Center for
Disease Control and Prevention (2001) Morbidity and
Mortality Weekly Report 50: no. RR-14.
Wang NJ, Gropen AM and Ogaard B (1997) Risk factors
associated with fluorosis in a non-fluoridated popula-
tion in Norway. Community Dental and Oral Epidemi-
ology 25(6): 396–401.
Whitford GM (1996) The Metabolism and Toxicity of
Fluoride, 2nd edn. Basel: Karger.
World Health Organization (1994) Report of a WHO
Expert Committee on Oral Health Status and Fluoride
Use. Fluorides and Oral Health. Geneva: WHO.
Detergents See Cleaning Procedures in the Factory: Types of Detergent; Types of Disinfectant; Overall
Approach; Modern Systems
Detoxification See Toxins in Food – Naturally Occurring; Alkaloids: Properties and Determination;
Toxicology
DEVELOPMENTAL DISABILITIES AND
NUTRITIONAL ASPECTS
Contents
Down Syndrome
Prader–Willi Syndrome
Down Syndrome
B Lucas and S Feucht, University of Washington,
Seattle, WA, USA
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Etiology
0001 Down syndrome (DS) (Trisomy 21) is one of the most
common chromosomal abnormalities, affecting one
in 600 live births. DS results from the presence of
extra genetic material (a third copy) on chromosome
21. It occurs during the prenatal period and affects all
races. The incidence of DS increases with maternal
age, although 80% of children with DS are born to
mothers less than 35 years of age due to increased
fertility of younger women. Current knowledge de-
scribes three types of genetic changes in chromosome
21 that cause DS:
.
0002nonfamilial trisomy 21, occurring in 95% of
individuals;
1760 DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Down Syndrome

.0003 unbalanced translocation between chromosome
21 and another chromosome, in 3–4%; of these,
approximately 25% result from a familial balanced
translocation, and parents may be at increased risk
of having another child with DS;
.
0004 mosaicism, in 1–2% of individuals with DS,
resulting from two present cell lines – one normal
and one trisomy 21; these individuals are usually
affected less severely than the other types.
Recent research has studied the role of folate and
homosysteine metabolism in women who had
children with DS. Although no conclusions could be
drawn from the small numbers, more work is needed.
It is possible that both genotype and nutrition may
play a role in the etiology of DS, as it does with neural
tube defects.
Features and Characteristics
0005 Individuals with DS demonstrate physical features
and other characteristics that define the syndrome
and determine the extent of health care, special edu-
cation, therapies, and vocational planning needed.
Developmental delay, hypotonia (reduced muscle
tone), and short stature are seen in all individuals
with DS. Cognitive levels usually range from mild
to moderate mental retardation. See Table 1 for
common characteristics.
0006 Overweight and obesity are frequently seen in indi-
viduals with DS, resulting from a variety of factors.
Other health concerns occurring less frequently, but
impacting nutrition, feeding, or physical activity,
include congenital heart disease, hearing problems,
vision problems, cervical spine abnormalities, seizure
disorders, and thyroid disease.
0007 Down syndrome is associated with premature
aging, often beginning in the fourth and fifth decades
of life. Along with this aging, there is reported to be
an increased incidence of Alzheimer’s disease, senility,
autoimmune diseases, and cataracts. Preliminary
studies had documented in vitro chronic oxidative
stress in persons with DS compared with their control
siblings, but the role of this or other biomarkers in
accelerated aging is controversial.
0008Services for individuals with DS are primarily com-
munity-based, compared with the past when most of
this population would be found in residential insti-
tutions. Currently, the diagnosis is made at, or shortly
after, birth, and early intervention services and
therapies are begun in early infancy. Full inclusion
in social, educational, and work environments is
supported in most all communities and countries. As
adults, many people with DS live in the community
(with family, in group or individual homes) and are in
vocational programs or gainfully employed.
Growth
0009Individuals with DS grow more slowly and are
shorter in final stature than those without the syn-
drome of the same age and sex. The growth differ-
ences begin in the prenatal period. By puberty,
children with DS are typically 1–2 inches (2.5–5 cm)
shorter than their peers. The onset of the growth spurt
may be delayed 6–12 months in adolescents with DS,
and some may never have a growth spurt. Specific
medical conditions such as congenital heart disease
may also impact growth and weight gain for a child
with DS. Since the onset of overweight can begin in
late infancy or the preschool period, appropriate
prevention strategies by the health care team should
begin early.
Specialized Growth Charts
0010Specialized growth charts have been published for
children with DS from birth to 36 months of age
and from 2 to 18 years of age. They provide a better
picture of length or stature in relation to other chil-
dren with DS. These DS charts reflect small sample
numbers (longitudinal data for weight and length/
height for 400 males and 300 females), and include
some children with congenital heart disease. The data
were collected from 1960 to 1986 on children living
at home, and they reflect a tendency to overweight. It
is essential to use these specialized charts in combin-
ation with standard growth charts, such as the Center
for Disease Control Growth Charts: United States
2000. The DS charts do not include head circumfer-
ence data for younger children, nor do they compare
weight/length or height in younger children or body
mass index for children over the age of two.
Overweight and Obesity
0011Increasing rate of weight gain is a risk in persons with
DS due to physical characteristics, medical condi-
tions, and environment (see Table 2). With wellness
tbl0001 Table 1 Characteristics of persons with Down syndrome
Hypotonia
Mental retardation
Short stature
Flat facial profile
Eye features (upward slanting eyelids; skinfolds in corners of
eyes)
Dental hypoplasia and irregular tooth placement
Increased risk of overweight and obesity
Accelerated aging process, i.e., Alzheimer-like brain changes,
cataracts
Increased incidence of congenital heart disease, thyroid disease,
leukemia
DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Down Syndrome 1761
programs for this population and their families/care-
givers, however, obesity can be prevented. A 1992
study of 30 sibling pairs, aged 2–14, found no signifi-
cant differences between the DS children and their
siblings in terms of BMI. The children with DS were
less active than their siblings. Although children with
DS who grow up with their own families have less
overweight and obesity than their institutionalized
peers, adults with DS living in the community are
more likely to be overweight or obese than those in
institutional settings. In 1995, Prasher reported on an
assessment of overweight and obesity in 201 adults
with DS living in the UK. Using BMI values, 31%
of males were overweight, and 48% were obese
(BMI > 30). For females, 22% were overweight, and
47% were obese; they also had the more severe
forms of obesity. This study found no association
between overweight/obesity and the severity of learn-
ing disability. Of note was the decreasing fall in BMI
with increasing age, but it is unclear if this is an
effect of the precocious aging or other related medical
conditions.
0012 For children, weight should be closely monitored
on standard growth charts to prevent rapid or exces-
sive gain that may not be as clearly seen on the DS
charts. Overall, the velocity of growth and weight
gain is more important than the actual percentile on
either growth chart (see Table 3). For adults, regular
health assessment should include weight and BMI
monitoring. Adults with DS and their older parents
may not have had the benefit of early intervention
programs and may not be as enthusiastic about phys-
ical fitness and healthy diet plans as younger persons.
Regardless of the etiology, the hazards of obesity
make prevention and intervention important.
0013Inclusion in social, educational, and vocational
environments brings new dietary challenges. Food
choices, from vending machines and fast food outlets,
typically favor high-fat, high-energy, nutrient-poor
foods and beverages. Nutrition education is required
to assist individuals with DS to make healthy food
choices for themselves in their communities.
Nutrition and Feeding Issues
0014Individuals with DS require the same nutrients and a
varied healthy diet as anyone else. However, the syn-
drome characteristics may make them more at risk for
nutrition and feeding problems. Owing to early de-
velopment delays, some feeding issues can arise that
affect the overall nutrient intake. Some infants may
be poor feeders due to hypotonia. As the child grows,
delays may be seen in the introduction of textured
foods and the transition to feeding themselves table
foods. Concerns have also been raised about low
energy intake, which may result from efforts to pre-
vent excessive weight gain. This low energy intake
may lead subsequently to a low nutrient intake.
With adequate monitoring and teamwork with the
family, issues around feeding and nutrition can be
identified early and appropriate interventions con-
sidered. Table 4 provides some general guidance to
support positive development of food habits and
prevention of excessive weight gain.
tbl0002 Table 2 Risk factors for overweight and obesity in individuals
with Down syndrome
Risk factors Effect
Hypotonia
Short stature
Low resting metabolic rate Easily tired
Hypothroidism Excess energy intake
Decreased pulmonary function Poor food choices
Cardiac malformations
Premature aging
Limited instruction in wellness
Food used as a reward
Limited physical activity
Preference for indoor
activities
Disinterest in physical
exercise
Adapted from Pipes P and Powell J (1996) Preventing obesity in children
with special health care needs. Nutrition Focus Newsletter 11(6): 1–8.
tbl0003 Table 3 Guidelines for growth monitoring and obesity
prevention in children with Down syndrome
Use standard growth charts for assessing weight for length,
weight for height, and/or body mass index (BMI)
Down syndrome-specific growth charts may be used with parents
to compare their children with their peers for length/height
Height and activity level should be used to determine individual
energy requirements (a baseline for children 5–11 years of age
is 16.1 kcal (67 kJ) per centimeter of height for males and
14.3 kcal (60 kJ) per centimeter of height for females)
Physical exercise is an important adjunct to an appropriate diet to
increase lean body mass and, if needed, decrease fat tissue
tbl0004Table 4 Nutrition recommendations for children with Down
syndrome
Establish early acceptance of a variety of foods
Develop a predictable eating pattern, i.e., three meals a day and
snacks, if needed
Eat together as a family as often as possible; do not expect the
child to eat alone
To establish good food habits early, limit access to non-nutritious
foods
Carry low-energy foods, e.g., vegetable juice, fruit, when away
from home
Have water readily available to drink
Avoid the use of food reinforcers in educational settings or for
behavior management
Physical activity limits excessive snacking while increasing
energy expenditure. (Note: To prevent aspiration, children
should not be engaged in physical activity while eating.)
Adapted from Pipes P and Powell J (1996) Preventing obesity in children
with special health care needs. Nutrition Focus Newsletter 11(6): 1–8.
1762 DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Down Syndrome

Energy and Nutrient Intake
0015 Since body mass and rate of growth determine basal
energy expenditure, individuals with DS require less
energy than their peers. Several studies of 5–11-year-
old children, living either in an institution or at home,
reported less energy intake than what is recom-
mended for their age groups, or compared with the
intake of their typically developing siblings. Obese
teenagers with DS consumed 12–13 kcal (50–54 kJ)
per cm (between the 10th and 50th percentile of
energy intake for typically developing teens).
0016 Over the years, nutrients of concern in children
with DS have included calcium, iron, copper, zinc,
and vitamins A, C, and E. Some reports have shown
the overall intake of vitamins and minerals to be
lower in children with DS compared with their con-
trols. This is a concern for those children with a lower
weight/height ratio and may be related to food/energy
restriction. Earlier vitamin A studies demonstrated a
lower intake, decreased absorption, and decreased
plasma levels of retinol. How this might relate to
abnormal immune response remains speculative.
0017 A recent study by Hopman of 44 children (birth to
4 years) with DS indicated that, while there was
delayed introduction of solid foods, the overall nutri-
ent intake was adequate. Iron was the exception, and
was low for both the subjects and controls. Energy
intake was 27% below the RDA, but when assessed
using energy per kilogram of body weight, this group
reached the recommended level (102 kcal (427 kJ)
per kg). These young children with DS as a group
weighed less than their controls and were younger
than those previously studied. With concerns about
low energy intake and the risk of inadequate nutrient
intake, a nutrition referral is appropriate for children
with Down syndrome, especially in the early months
and years of life.
Feeding Problems
0018 Feeding difficulties and concern about related nutri-
ent intake occur most often during the infant, toddler,
and preschool years. If feeding issues continue into
older childhood, they may have multiple causes and
be more severe. Early feeding problems may include
difficulties with coordination of suck and swallow.
Most infants with DS are not ready for semisolids by
the usual 4–6 months of age. They are usually not
able to sit without support due to the hypotonia, and
immature oral motor abilities make eating from a
spoon difficult, if not unpleasant. If solids are not
offered when the child is developmentally ready,
however, subsequent feeding problems can occur.
Delays in introducing solid foods due to oral motor
issues sometimes can lead to a refusal to progress and/
or chew more textured foods when the child is
developmentally able to do so.
0019Because of the delayed development, parents often
do not have adequate guidance or cues regarding
when and how to progress in food textures and self-
feeding skills. Feeding problems can also develop from
negative experiences and interactions around feeding,
i.e., choking or gagging, force-feeding. Infants and
children with DS benefit from periodic screening to
assess feeding development with subsequent referral
to therapists or a feeding team if concerns are present.
This screening should begin in infancy.
Supplement Use in Down Syndrome
0020The use of alternative treatments, such as supplemen-
tal vitamins and minerals, is relatively common in
individuals with developmental disabilities. Vitamin
supplements, with varying formulations and some-
times at high levels, have been promoted for persons
with Down syndrome for at least 60 years. Related to
the theory of increased oxidative stress, there have
been various studies using individual nutrient supple-
ments, i.e., zinc, vitamin A, selenium, and vitamin B
6
.
The results of these studies were inconsistent, and
most had major methodological limitations.
0021The current popular approach is ‘targeted nutrition
intervention.’ The supplement promoted promises to
‘alleviate certain harmful symptoms of Down syn-
drome (e.g., the susceptibility to infections), and at-
tempt to keep other harmful effects of the syndrome
(e.g., mental retardation) from getting worse.’ It
contains vitamins and minerals for which there is a
dietary reference intake (DRI) or a recommended
dietary allowance (RDA), amino acids, and other
compounds such as coenzyme Q10 and papain,
which have no established dietary requirement.
When provided as recommended for a child’s weight,
the supplement does not provide excessive doses of
fat-soluble vitamins, which could lead to toxicity.
However, some of the water-soluble vitamins are ex-
cessively high for infants, i.e. 60 times the dietary
reference intake for vitamin B
12
. Although such high
levels are not reported to be deleterious in adults,
studies in infants and young children are virtually
nonexistent. Therefore, monitoring of these supple-
ments is indicated, as well as education and counsel-
ing for families regarding recommended nutrient
intakes for infants and children.
0022Anecdotal reports and testimonials of the benefits
of these and similar supplements are widely distrib-
uted in lay publications and on the Internet, but no
controlled studies have been conducted on these
supplements.
0023When a similar supplement was popular in the
1980s, several double-blind, controlled studies using
DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Down Syndrome 1763

the same protocol were conducted with children with
DS. There was no difference in the health, develop-
ment, and cognition between the children receiving
the supplements and those who received the placebo.
All groups showed improvements in all areas, as
would be expected over time.
0024 Health and education professionals working with
families who are using such supplements need to be
supportive and open, yet make sure that the practice
does no harm. They should ask: Is the product safe?
Does it work? What is the cost to the family? Are diet,
feeding, and growth concerns being addressed at the
same time? Is the child still obtaining education and
needed therapies?
Other Nutrition-related Issues
Constipation
0025 Constipation is a frequent problem due to hypotonia
and decreased motor activity. The colon may retain
stool longer leading to loss of water and result in
hard, dry stools and long periods between stooling.
Typical interventions include increasing the amount
of fiber-containing foods and fluids in the diet and
participating in appropriate exercise. If feeding prob-
lems are present, dietary treatment may be a challenge.
Behavior-management techniques are sometimes help-
ful. Additional medical management may be needed
with the use of stool softeners or addition of medical
fiber products. Generally, the use of laxatives, supposi-
tories, etc. is not appropriate for children, unless the
child’s primary care provider is consulted.
0026 Children with DS have an increased incidence of
Hirschsprung disease. In this condition, nerve endings
are missing in the colon, so stools are not pushed
along in the large intestine. This condition is usually
identified early in life with subsequent surgical inter-
vention.
Celiac Disease
0027 Celiac disease may occur in 7–16% of children with
DS, mostly documented from European sources.
Individuals with DS may be predisposed to this
condition because of the known increased incidence
of autoimmune disorders. Symptoms usually resolve
following institution of a gluten-free diet.
Dental Issues
0028 Persons with DS often have smaller jaws and palates.
Protruding of the lower jar can lead to poor align-
ment, which can affect chewing. The tongue also may
be increased in size (or the jaw may be too small to
support the tongue) and be more furrowed, leading to
crevices that retain food and plaque. This can foster
bacteria growth and/or bad breath. Dry mouth
(xerostomia) is common and is believed to be due to
reduced saliva as well as an open mouth and mouth
breathing due to the tongue and jaw size.
0029Tooth eruption is delayed in children with DS until
12 and 18 months of age. There is also a risk for
enamel abnormalities that can cause pitting and re-
tention of food and plaque. Gum disease also occurs
with greater frequency.
0030These problems can impact the individual’s ability to
eat and chew. With the increased risks of dental prob-
lems that can impact food intake, early and regular
tooth and gum care is essential. For children with DS,
the first visit to the dentist is recommended immedi-
ately after the first teeth erupt or by the first birthday.
Physical Activity
0031Individuals with DS are known to be less active than
peers and to spend significantly more time indoors.
Hypotonic children tire easily and use movement
patterns requiring the least expenditure of energy.
However, hypotonia tends to improve with age and
therapy. The low level of physical fitness is partially
explained by findings such as blood pressure, which
does not rise regularly with the workload increment.
The Health Care Guidelines for Individuals with
Down Syndrome recommend establishing regular
exercise and recreational programs early in the child’s
life. Enrollment in an early intervention program,
which includes a focus on gross motor activities, is
usually recommended within the first months of life.
0032Many children with DS have few restrictions in
physical activity and should be encouraged to be active
to increase their function, improve fitness, expend
energy for weight management, and have fun. Sports
should be limited to noncontact sports that challenge
development, coordination, balance, and agility, and
are fun to encourage life-long participation. The
Special Olympic programs fosters life-long participa-
tion in physical activity and has many social rewards.
0033Approximately 10–40% of individuals with DS
have atlantoaxial dislocation (ligaments in the cer-
vical vertebra are more relaxed) resulting from hypo-
tonia. This instability may increase the risk for spinal
cord compression and injury. Activities that cause or
require significant flexion of the neck, such as high
jumping, gymnastics, diving and the butterfly stroke,
should be avoided or done under medical supervision.
Promotion of Health and Nutrition
0034Optimal nutrition and growth, a healthy weight, and
overall wellness are positive goals for persons with DS
1764 DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Down Syndrome

and their families/caregivers. These are achieved not
only by appropriate health care, but also by health
and nutrition curricula in educational settings, and
wellness programs in vocational and work sites. Key
elements in a comprehensive wellness program for
individuals with DS throughout the life span include:
.
003 5 access to accurate and consistent nutrition, well-
ness, and fitness information and anticipatory
guidance;
.
003 6 interdisciplinary health care teams who develop
trusting relationships with families and support
access to scientific information and interpretation
of that information;
.
003 7 focus on good food choices and appropriate
physical activity (beginning in infancy) to prevent
overweight and obesity;
.
003 8 practical nutrition education (appropriate to cog-
nitive level) related to good food choices, basic
food preparation, and physical activity for older
children and adults with DS in the community.
Seealso: Developmental Disabilities and Nutritional
Aspects:Prader–WilliSyndrome; Gene Expression and
Nutrition; Pregnancy:MaternalDiet,Vitamins,and
NeuralTubeDefects; Slimming:MetabolicConseqences
ofSlimmingDietsandWeightMaintenance
Further Reading
American Academy of Pediatrics (1994) Health supervision
for children with Down syndrome. Pediatrics 93:
855–859.
Ani C, Grantham-McGregor S and Muller D (2000) Nutri-
tional supplementation in Down syndrome: theoretical
considerations and current status. Developmental
Medicine and Child Neurology 42: 207–213.
Cohen WI (ed.) (1996) Health Care Guidelines for Individ-
uals with Down Syndrome (Down Syndrome Preventive
Medical Check List). Down Syndrome Quarterly 1: 2
(available at http://denison.edu/dsq).
Cronk CE, Crocker AC, Pueschel SM et al. (1988) Growth
charts for children with Down syndrome 1 month to 18
years of age. Pediatrics 81: 102. (Note: the birth to 36
month chart for males and females has errors in the
weight increments).
Hobbs CA, Sherman SL, Yi P et al. (2000) Polymorphisms
in genes involved in folate metabolism as maternal risk
factors for Down’s syndrome. American Journal of
Human Genetics 67: 623–630.
Hopman E, Cszimadia CG, Bastiani WF et al. (1998) Eating
habits of young children with Down syndrome in The
Netherlands: Adequate nutrient intakes but delayed
introduction of solid food. Journal of the American
Dietetic Association 98: 790–794.
James SJ, Pogribna M, Pogribny IP et al. (1999) Abnormal
folate metabolism and mutation in the methylenetetra-
hydrofolate reductase gene may be maternal risk factors
for Down syndrome. American Journal of Clinical
Nutrition 70: 495–501.
Luke A, Sutton M, Schoeller DA and Roizen NJ (1996)
Nutrient intake and obesity in prepubescent children
with Down syndrome. Journal of the American Dietetic
Association 96: 1262–1267.
National Down Syndrome Congress. Atlanta, GA
(www.ndscenter.org).
Prasher VP (1995) Overweight and obesity amongst
Down’s syndrome adults. Journal of Intellectual Disabil-
ity Research 39: 437–441.
Sharar T and Bowman ST (1992) Dietary practices, physical
activity, and body-mass index in selected population of
Down syndrome children and their siblings. Clinical
Pediatrics 31: 341–344.
Prader–Willi Syndrome
M S N Gellatly, Chelmsford, Essex, UK
Copyright 2003, Elsevier Science Ltd. All Rights Reserved.
Prevalence and Incidence
0001Prader-Willi Syndrome (PWS) is a complex genetic
disorder.
0002In early 2002, the best estimate of incidence is 1 in
38 000–40 000. Increased awareness of the syndrome
and improved diagnostic procedures should not be
confused with an increase in prevalence.
0003PWS occurs in all races and across all ethnic
groups.
Characteristics
0004The documented characteristics of PWS are summar-
ized in Table 1. The range and severity of these vary
considerably.
Body Composition
0005People with PWS have an abnormal body compos-
ition. Part of the explanation can be attributed to
lowered gonadal hormones and their contribution to
normal development. The most significant abnormal-
ity is a peculiarly high fat to fat-free mass ratio. Bone
composition irregularities include lower mineral
density, which contributes to the increased risk of
osteoporosis, while bone age may be advanced if the
child is significantly obese. Hypotonia (poor muscle
tone) is primarily caused through central nervous
system abnormalities; muscle abnormalities may be
observed, such as size variations in type 1 and defi-
ciencies in type 2B fibers.
DEVELOPMENTAL DISABILITIES AND NUTRITIONAL ASPECTS/Prader–Willi Syndrome 1765