Townsend Courtney M.Jr., Evers B. Mark. Atlas of General Surgical Techniques: Expert Consult
Подождите немного. Документ загружается.

CHAPTER 105 • Subclavian Artery Stab 1167
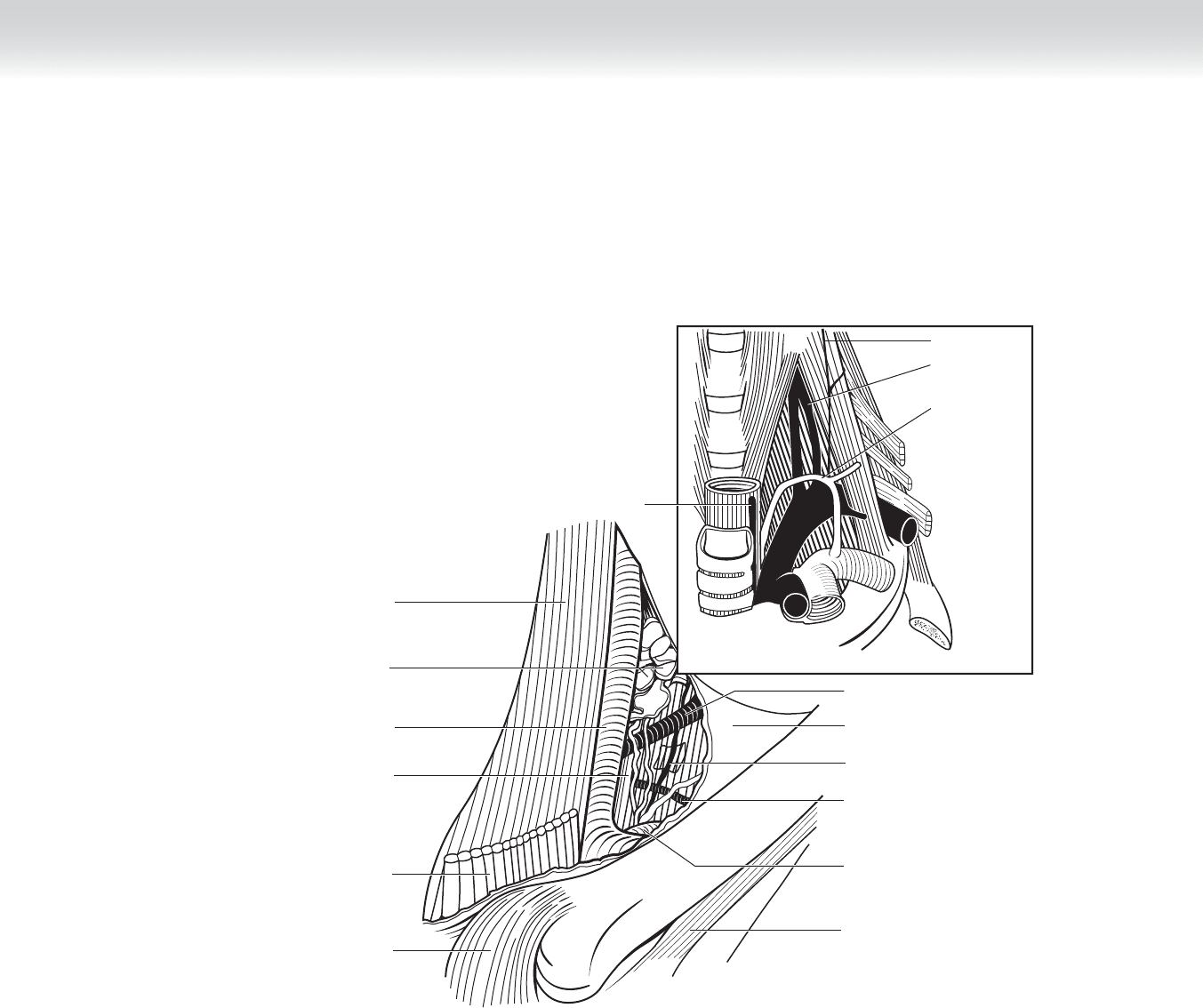
Anterior sternoclavicular
ligament
Sternohyoid muscle
Thoracic duct
Internal jugular
vein
Deep cervical
lymph nodes
Sternothyroid muscle
C6
Recurrent
laryngeal nerve
Phrenic nerve
Inferior thyroid
artery
Thoracic
duct
Contents of carotid sheath
Subclavius muscle
Subclavian vein
Suprascapular artery
Phrenic nerve
Omohyoid fascia
Transverse cervical artery
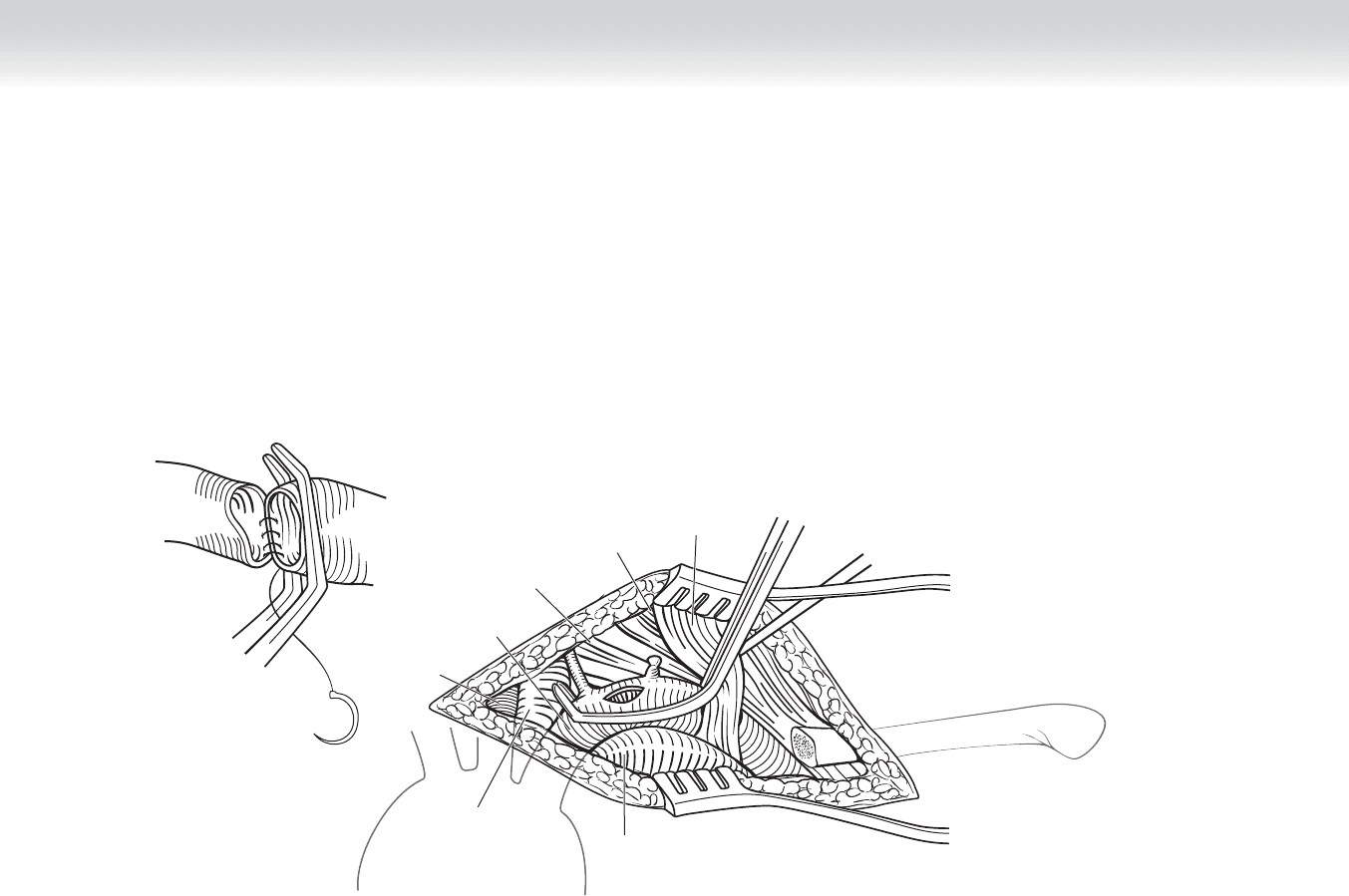
FIGURE 105 –1

1168 Section XVI • Operations—Elective and Trauma
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Operative approach to stab wounds of the subclavian vessels is based on the patient’s clinical
(i.e., hemodynamic) status. In patients who present with massive bleeding in extremis, initial
attempts at digital compression through the wound or a limited second intercostal anterior
thoracotomy with compression of the vessels by insertion of two fi ngers may allow tempo-
rary control, permitting resuscitation and surgical exposure.
◆ In patients with near normal vital signs or who stabilize with initial resuscitation, imaging
studies, either angiogram or computed tomography (CT) angiogram that provides anatomic
defi nition, can guide decisions on surgical approach. Both the right and left subclavian
vessels can be approached by medial clavicular resection. If it is suspected that proximal
control at either the innominate or aortic junction will be needed, a median sternotomy
may be required.
STEP 3: OPERATIVE STEPS
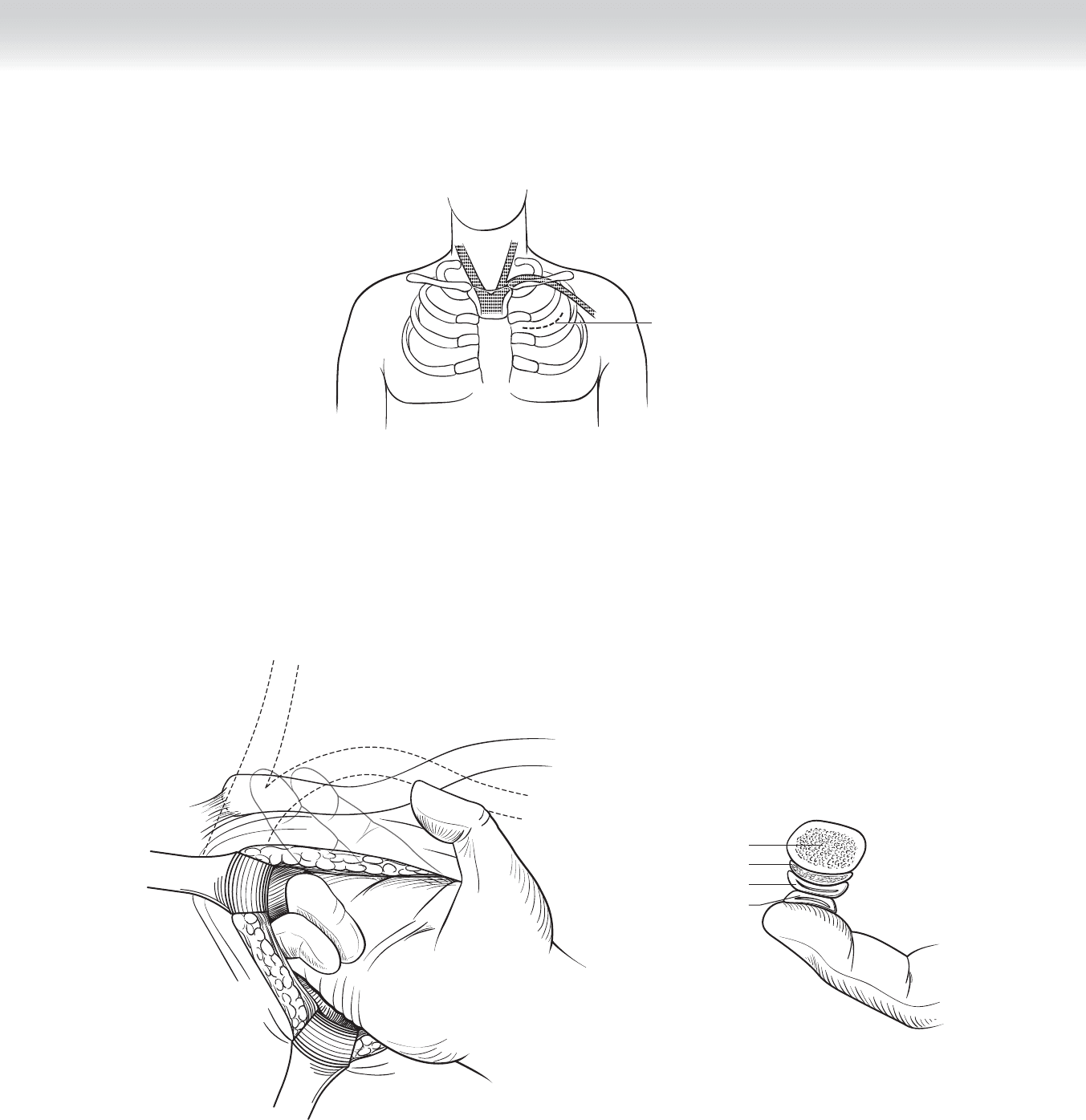
◆ The incision is at the second interspace.
◆ A curvilinear incision 5 to 7 cm in length is rapidly created, beginning at the lateral
border of the sternum through the pectoralis into the pleura (Figure 105-2).
◆ The right second and third fi ngers are inserted and used to apply pressure superiorly and
medially to compress the subclavian artery and vein against the clavicle (Figure 105-3).
◆ After the hemorrhage is controlled, the subclavian vessels can be exposed by resecting
the medial clavicle.
CHAPTER 105 • Subclavian Artery Stab 1169
Incision at second
interspace
A
Clavicle
B
Subclavius muscle
Subclavian vein
Subclavian artery
FIGURE 105 –3
FIGURE 105 –2
1170 Section XVI • Operations—Elective and Trauma
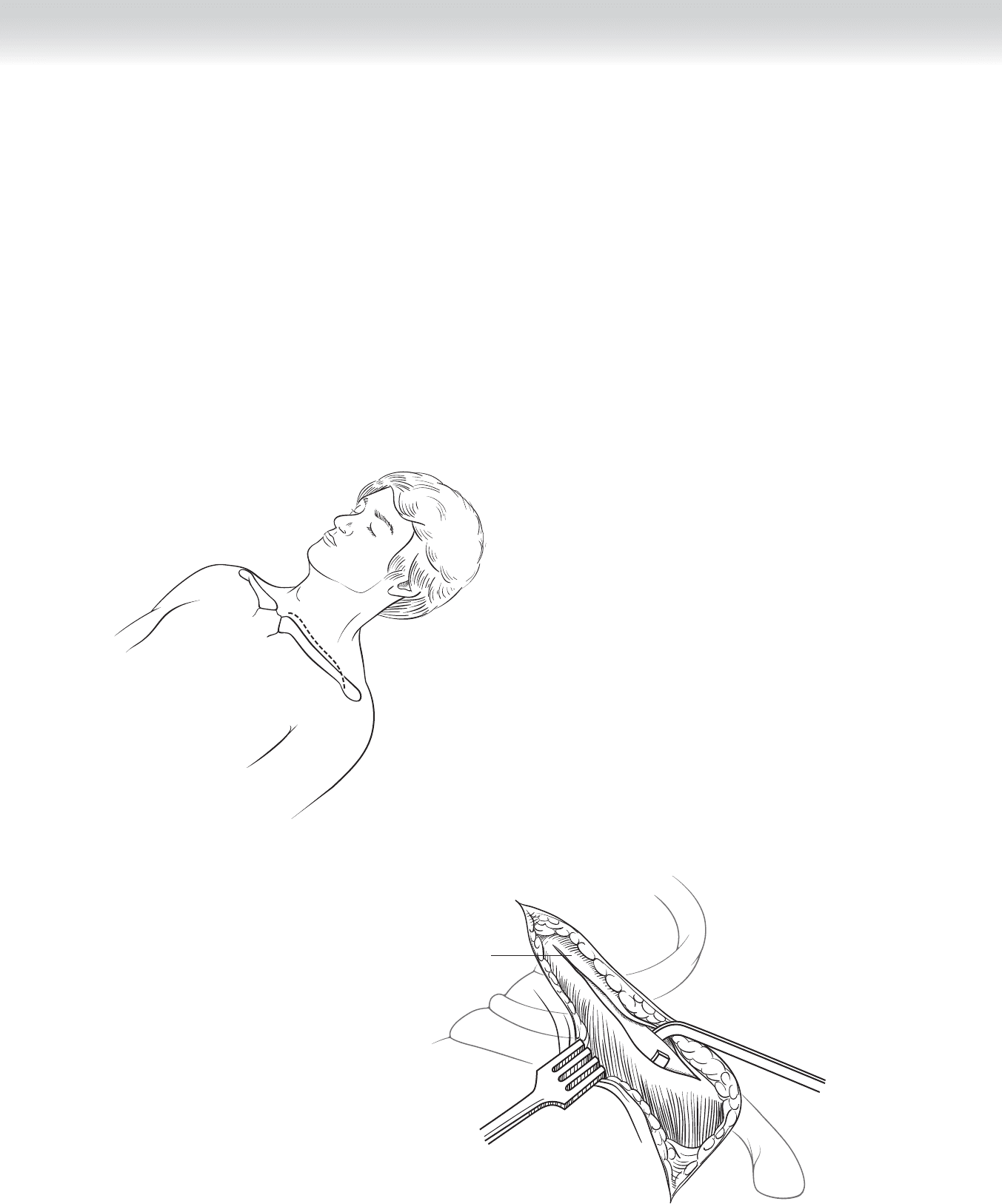
◆ Clavicular resection
◆ The incision is begun at the midline and extended laterally, directly over the clavicle to
the deltopectoral groove (Figure 105-4, A). Subcutaneous tissue and the anterior perios-
teum can be quickly dissected with electrocautery.
◆ The periosteum is separated from the clavicle circumferentially using periosteal elevators
(Figure 105-4, B).
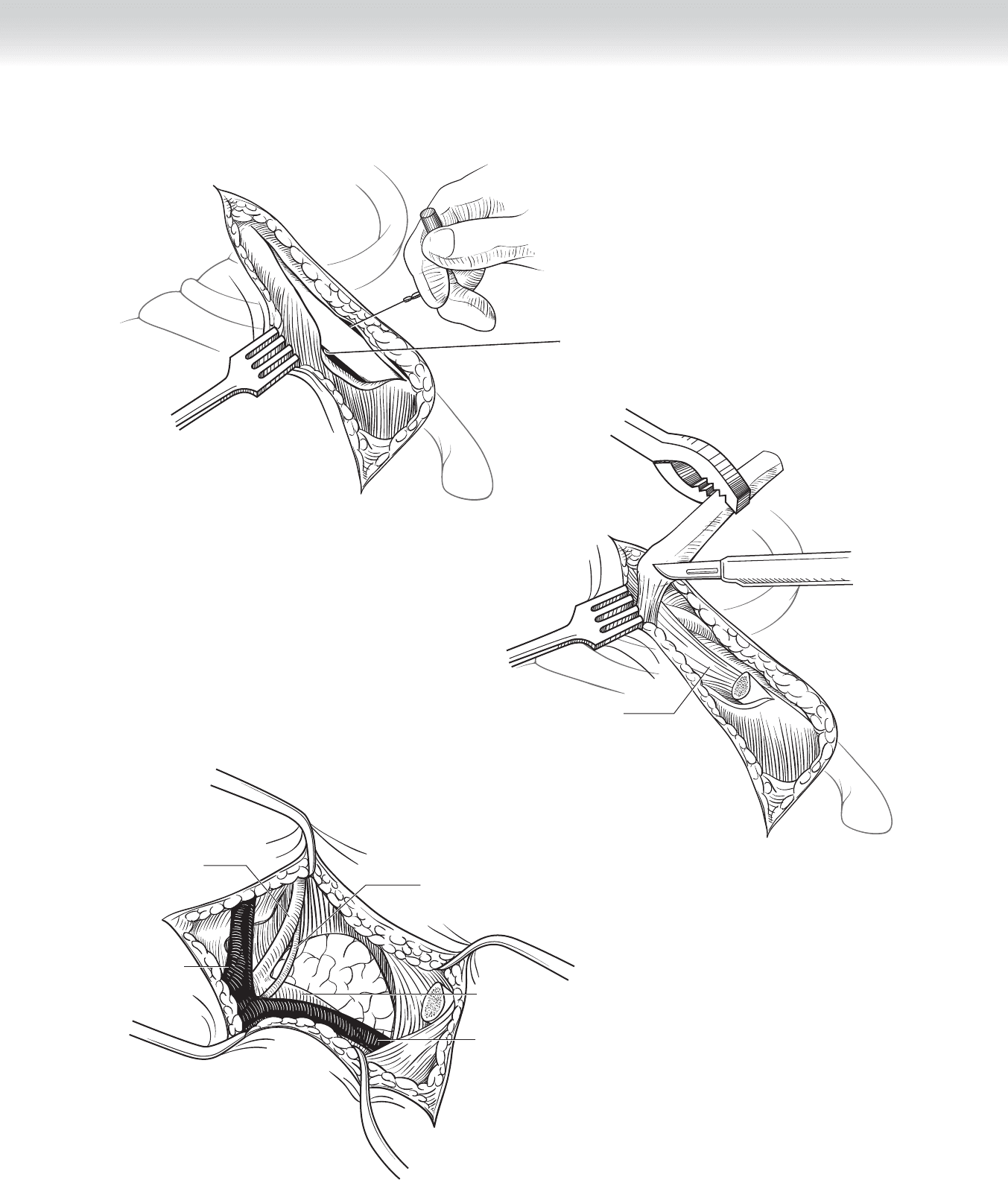
◆ The clavicle is then transected at the lateral aspect of the exposure using a Gigli saw
(Figure 105-4, C).
◆ The medial aspect is retracted medially and superiorly, allowing separation of the
sternoclavicular joint with sharp dissection or electrocautery.
◆ The posterior periosteum is incised at the lateral aspect of the incision and extended
medially (Figure 105-4, D).
◆ Placing two self-retaining retractors beneath the incised periosteum will allow dissection
of the subclavian artery and vein, permitting proximal and distal vascular control in
preparation for vascular repair (Figure 105-4, E-F).
A
Periosteum
B
FIGURE 105 –4
CHAPTER 105 • Subclavian Artery Stab 1171
D
Posterior periosteum
C
E
Thoracic duct
Subclavian artery
Vertebral artery
Subclavian vein
Internal
jugular vein
FIGURE 105 –4, cont’d
1172 Section XVI • Operations—Elective and Trauma
Left jugular vein
F
Left
subclavian vein
Left subclavian
artery
Sternocleido-
mastoid muscle
Phrenic
nerve
Anterior scalene
muscle
Left common
carotid artery
FIGURE 105 –4, cont’d

CHAPTER 105 • Subclavian Artery Stab 1173
STEP 4: POSTOPERATIVE CARE
◆ Patient should wear a shoulder immobilizer.
STEP 5: PEARLS AND PITFALLS
◆ Although numerous references suggest replacement and reconstruction of the clavicle, it
may be unnecessary. If the patient’s condition allows, replacement of the medial clavicle
with internal fi xation should be attempted to reduce long-term morbidity.
SELECTED REFERENCE
1. Thal ER, Weigelt JA, Carrico CJ: Operative Trauma Management: An Atlas, 2nd ed. New York,
McGraw Hill, 2002, pp 110-114.

1174
STEP 1: SURGICAL ANATOMY
The following structures must be observed:
◆ Xiphoid process
◆ Fifth intercostal space
◆ Latissimus dorsi muscle
◆ Sternum
◆ Clavicles
◆ Pericardium
◆ Phrenic nerves
◆ Lungs
◆ Intercostal muscles
◆ Intercostal vessels
◆ Internal mammary vessel
CHAPTER
106
Thoracotomy for Trauma
William J. Mileski
CHAPTER 106 • Thoracotomy for Trauma 1175
STEP 2: PREOPERATIVE CONSIDERATIONS
◆ Patients with combined cardiac and pulmonary injuries or bilateral thoracic injuries may
require a bilateral anterior lateral thoracotomy, or “clamshell thoracotomy,” which provides
exposure of bilateral hemithoraces, the pulmonary hila, and the mediastinum.
◆ Emergent thoracotomy requiring extension from left anterior lateral thoracotomy to right
thoracotomy is infrequently needed but may be necessary when penetrating injuries
unexpectedly require exposure of both right and left hemithoraces. Median sternotomy
would be preferred for treating penetrating cardiac injuries.
◆ There is generally insuffi cient time for formal preparation. Rapid painting with povidone-
iodine (Betadine) is generally performed. The neck, entire thorax, abdomen, and upper
thighs should be included. The incision of the thigh may facilitate use of mechanical
cardiopulmonary support.
STEP 3: OPERATIVE STEPS
1. INCISION
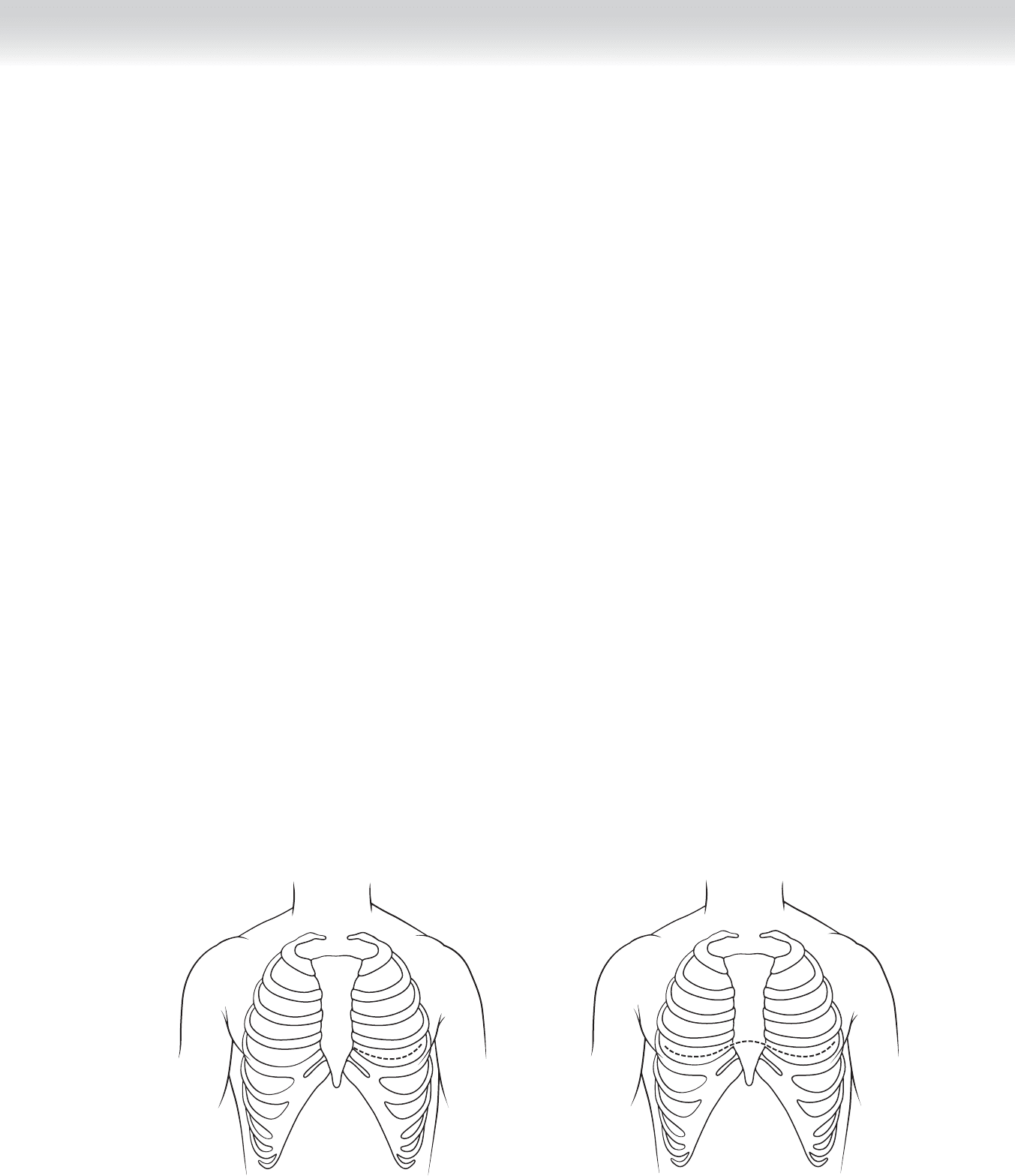
◆ The incision begins at the junction of the xiphoid process and sternum and is extended
laterally in a curvilinear fashion to the anterior border of the latissimus dorsi
(Figure 106-1).
◆ The incision should be carried down to the intercostal muscles on the superior aspect of
the fi fth or sixth rib, with care given not to cut through the intercostals into the underlying
pulmonary parenchyma (Figure 106-2).
FIGURE 106 –1
FIGURE 106 –2

1176 Section XVI • Operations—Elective and Trauma
2. DISSECTION
◆ The intercostal muscles and pleura are best taken down using a curved Mayo scissors,
partially opened, pressed on the superior aspect of the rib, and advanced lateral to medial.
At the medial aspect, the internal mammary vessels are often transected and require ligation
if resuscitation is successful.
◆ A rib spreader is inserted and retracted.
◆ The pericardium is inspected if indicated, and pericardiotomy is performed in a
longitudinal fashion, anterior to the phrenic nerve.
◆ In the absence of a source of hemorrhage in the left hemithorax or a cardiac injury and
suspected hemorrhage in the right hemithorax, the incision may be rapidly extended to the
right hemithorax in a mirrored fashion.
◆ The xiphisternal junction may be transected with an osteotome, Lebsche knife, or
sternal saw.
◆ Again, the internal mammary vessels are transected and ligated (Figure 106-3).
◆ The superior thoracic cage can then be retracted cephalad, exposing the anterior medias-
tinum and bilateral hemithoraces and the pulmonary hila (Figure 106-4).
3. CLOSING
◆ If resuscitation is successful and a treatable injury is identifi ed and repaired, thoracic closure
should be rapidly accomplished.
◆ Bilateral 36F thoracostomy tubes are placed, the ribs are approximated with interrupted
#1 Vicryl suture, the subcutaneous tissue is reapproximated with absorbable suture, and
the skin is closed with staples.
STEP 4: POSTOPERATIVE CARE
◆ Pain control and respiratory therapy are critical to recovery.
STEP 5: PEARLS AND PITFALLS
◆ Care must be exercised to avoid damage to the phrenic nerve when pericardiotomy is
performed.