Cui Dongmei. Atlas of Histology: with functional and clinical correlations. 1st ed
Подождите немного. Документ загружается.

CHAPTER 15
■
Digestive Tract
285
Epithelium
Lamina propria
Muscularis mucosae
4. Serosa / adventitia
4. Serosa
1. Mucosa
Longitudinal
muscle
Circular
muscle
Oblique
muscle
1. Mucosa
2. Submucosa
2. Submucosa
3. Muscularis
externa
3. Muscularis
externa
Inner circular muscle
Outer longitudinal muscle
Epithelium
Lamina propria
Muscularis mucosae
2. Submucosa
1. Mucosa
3. Muscularis
externa
Circular muscle
Longitudinal muscle
band (teniae coli)
4. Serosa/adventitia
Small intestine
Stomach
Large intestine
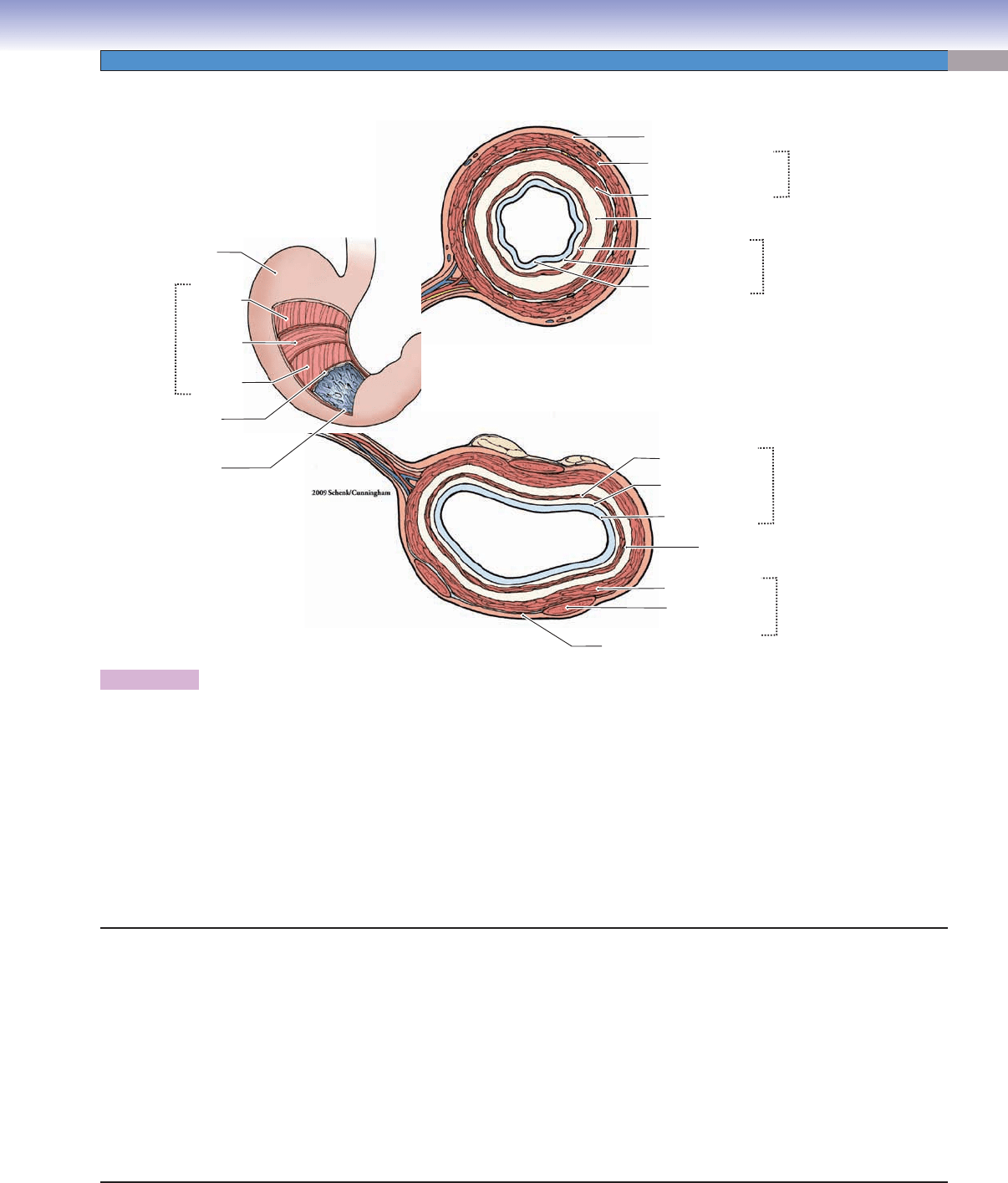
Figure 15-3. General structure of the wall of the digestive tract.
The wall of the digestive tract can be divided into several basic tunics (layers) based on histologic organization. (1) Mucosa: epithelium,
lamina propria, and muscularis mucosae. The epithelium is composed of simple columnar cells in most of the digestive tract, except
for stratifi ed squamous cells in the esophagus and anal canal. The lamina propria is a layer of loose connective tissue beneath the
epithelium. The muscularis mucosae is a thin layer of smooth muscle; it marks the boundary between the mucosa and the submucosa.
(2) Submucosa: dense irregular connective tissue with blood vessels, lymphatic vessels, and submucosal plexuses (Meissner plexuses).
Mucous glands may be present in this layer. (3) Muscularis externa: two or three layers of smooth muscle. It may also include skeletal
muscle as in the esophagus. There are blood vessels and myenteric (Auerbach) plexuses that lie between the muscle layers. (4) Serosa/
adventitia: The outermost layer is called serosa if it is composed of loose connective tissue with blood vessels and nerves passing
through and is covered by mesothelium. It is called adventitia if covered by a layer of connective tissue without mesothelium lining.
The serosa covers organs within the abdominal or pelvic cavities (intraperitoneal), whereas the adventitia covers organs and serves
as a capsule and attachment between the organs or between an organ and the body wall (retroperitoneal).
1. Mucosa
Epithelium
Lamina propria
Muscularis mucosae
2. Submucosa
Mucous glands and lymphatic nodules may be present
3. Muscularis Externa
Inner circular muscle layer
Outer longitudinal muscle layer
Oblique muscle layer (stomach)
4. Serosa/Adventitia
Serosa: outermost layer composed of connective tissue
covered by mesothelium
Adventitia: outermost layer composed of connective tissue
without mesothelium covering
Tunics (Layers) of the Digestive Tract
CUI_Chap15.indd 285 6/2/2010 3:23:38 PM
286
UNIT 3
■
Organ Systems
Esophagus
Submucosa
Muscularis
externa
Mucosa
Mucosa
Mucosa
Lumen
Lumen
Lumen
Esophageal
glands
Muscularis
mucosae
A
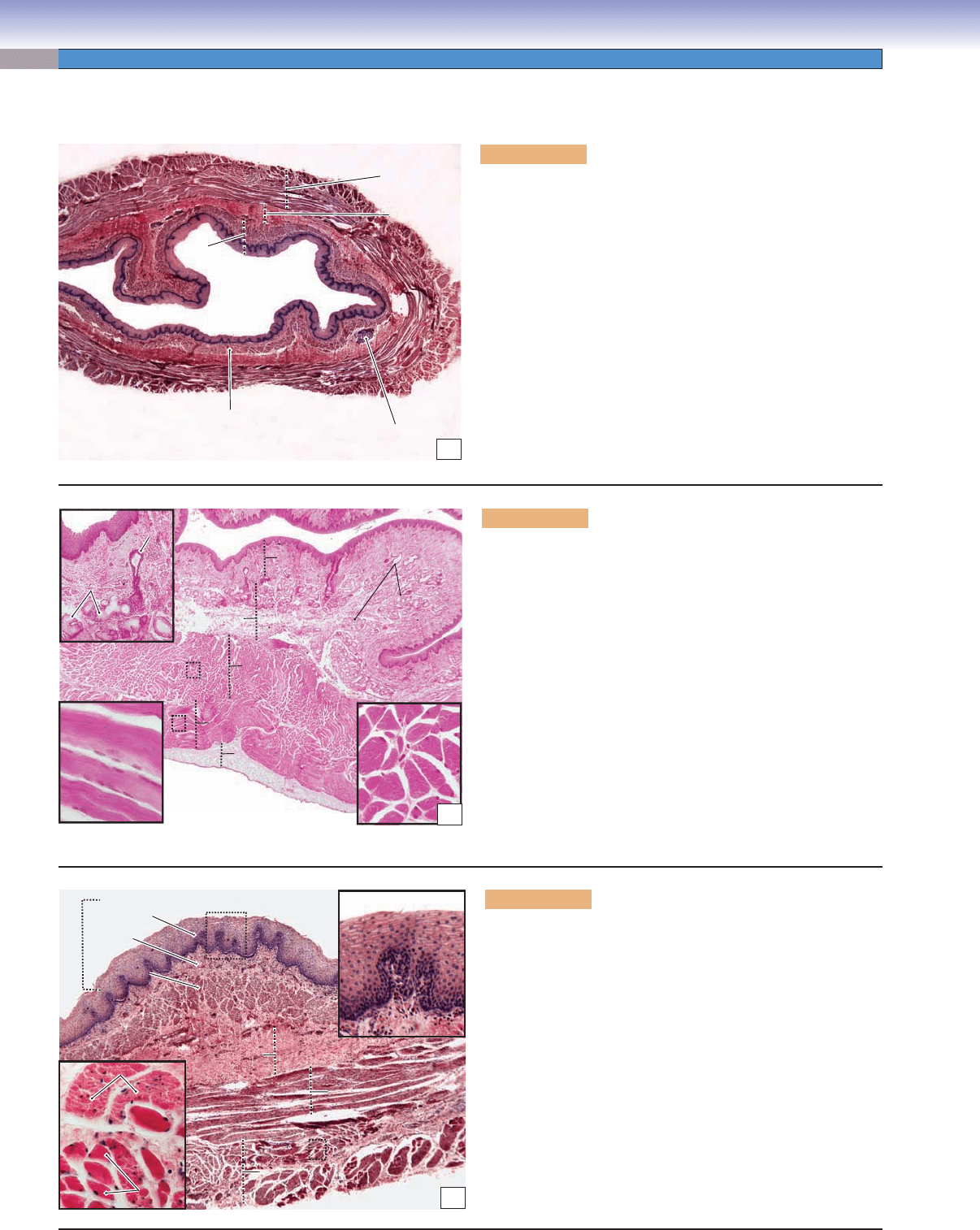
Figure 15-4A. Overview of the esophagus. H&E, 11
The esophagus can be divided into three regions: the upper,
middle, and lower esophagus. The esophagus is a long tube
that connects the oropharynx to the stomach. Like other parts
of the digestive tract, the esophagus has mucosa, submucosa,
muscularis externa, and adventitia/serosa. (1) The mucosa is
composed of epithelium, lamina propria, and muscularis muco-
sae. The mucosa of the esophagus has folds extending into the
lumen. Stratifi ed squamous epithelium covers the inner surface of
the esophagus. The muscularis mucosae is composed of a single
layer of longitudinal smooth muscle. (2) The submucosa contains
mucous glands called esophageal glands, which secrete mucus and
provide lubrication that aids in swallowing. (3) The muscularis
externa is composed of two layers of muscle organized into inner
circular and outer longitudinal layers. (4) The outermost wall of
the esophagus is commonly covered by adventitia (Fig. 15-4B),
but the lower esophagus is covered by serosa.
Inner circular
Inner circular
(skeletal) muscle
(skeletal) muscle
Inner circular
(skeletal) muscle
Outer longitudinal
Outer longitudinal
(skeletal) muscle
(skeletal) muscle
Outer longitudinal
(skeletal) muscle
Esophageal
Esophageal
glands
glands
Esophageal
glands
Esophageal
Esophageal
glands
glands
Inner circular muscle
Inner circular muscle
Outer longitudinal muscle
Outer longitudinal muscle
Adventitia
Adventitia
Mucosa
Mucosa
Submucosa
Submucosa
Duct of
Duct of
glands
glands
Duct of
glands
B
Esophageal
glands
Inner circular muscle
Outer longitudinal muscle
Adventitia
Mucosa
Submucosa
Figure 15-4B. Upper esophagus. H&E, 17; (upper inset)
40; (lower insets) 216
The upper esophagus, connecting to the oropharynx, is the fi rst
segment of the esophagus. The muscularis externa of the upper
esophagus contains two layers of skeletal muscle. The skeletal
muscle is a voluntary muscle that helps to initiate swallowing.
This muscle is innervated by the glossopharyngeal nerve. The
muscularis externa of the esophagus has distinguishable muscle
components, which vary in different regions. The upper esopha-
gus has skeletal muscle, the middle esophagus has mixed skeletal
and smooth muscles, and the lower esophagus has only smooth
muscle in the muscularis externa. The muscularis externa plays
an important role in producing contractions of the esophagus
that transport food from the oral cavity to the stomach. The
major movement of the esophagus is peristalsis (waves of invol-
untary contraction), as in other parts of the digestive tract. The
initiation of swallowing is voluntary because the upper esophagus
contains only skeletal muscle fi bers in the muscularis externa.
Epithelium
Epithelium
Epithelium
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
Epithelium
Epithelium
Epithelium
Lamina
Lamina
propria
propria
Lamina
propria
Mucosa
Mucosa
Mucosa
Inner circular muscle
Inner circular muscle
Inner circular muscle
Outer longitudinal muscle
Outer longitudinal muscle
Outer longitudinal muscle
Submucosa
Submucosa
Submucosa
Smooth muscle
Smooth muscle
Smooth muscle
Skeletal
Skeletal
muscle
muscle
Skeletal
muscle
C
Figure 15-4C. Middle esophagus. H&E, 34; insets (left)
208, (right) 116
The mucosa of the esophagus is covered by a thick layer of
nonkeratinized stratifi ed squamous epithelium, which refl ects
its function in resisting abrasion and friction. The epithe-
lium of the esophagus is continuously renewed by basal cells
that migrate and differentiate from the basal layer. Most of
the digestive tract is covered by simple columnar epithelium;
only the two ends (esophagus and anal canal) are covered by
stratifi ed squamous epithelium. The muscularis externa of the
middle esophagus contains mixed skeletal and smooth muscle
fi bers, which are organized in inner circular and outer longitu-
dinal muscle bundles. Each skeletal muscle fi ber is larger, has
multiple nuclei positioned peripherally, and stains darker than
the smooth muscle fi ber. Each smooth muscle fi ber has a single
nucleus located in the center of the muscle fi ber.
CUI_Chap15.indd 286 6/2/2010 3:23:41 PM
CHAPTER 15
■
Digestive Tract
287
Submucosa
Submucosa
Submucosa
Submucosa
Submucosa
Submucosa
Lamina
Lamina
propria
propria
Lamina
propria
Esophageal
Esophageal
cardiac glands
cardiac glands
Esophageal
cardiac glands
epithelium
epithelium
epithelium
Mucosa
Mucosa
Mucosa
Simple
Simple
columnar epithelium
columnar epithelium
Simple
columnar epithelium
Stratified squamous
Stratified squamous
epithelium
epithelium
Stratified squamous
epithelium
Muscularis
Muscularis
externa
externa
Muscularis
externa
Mucosa
Mucosa
Mucosa
A
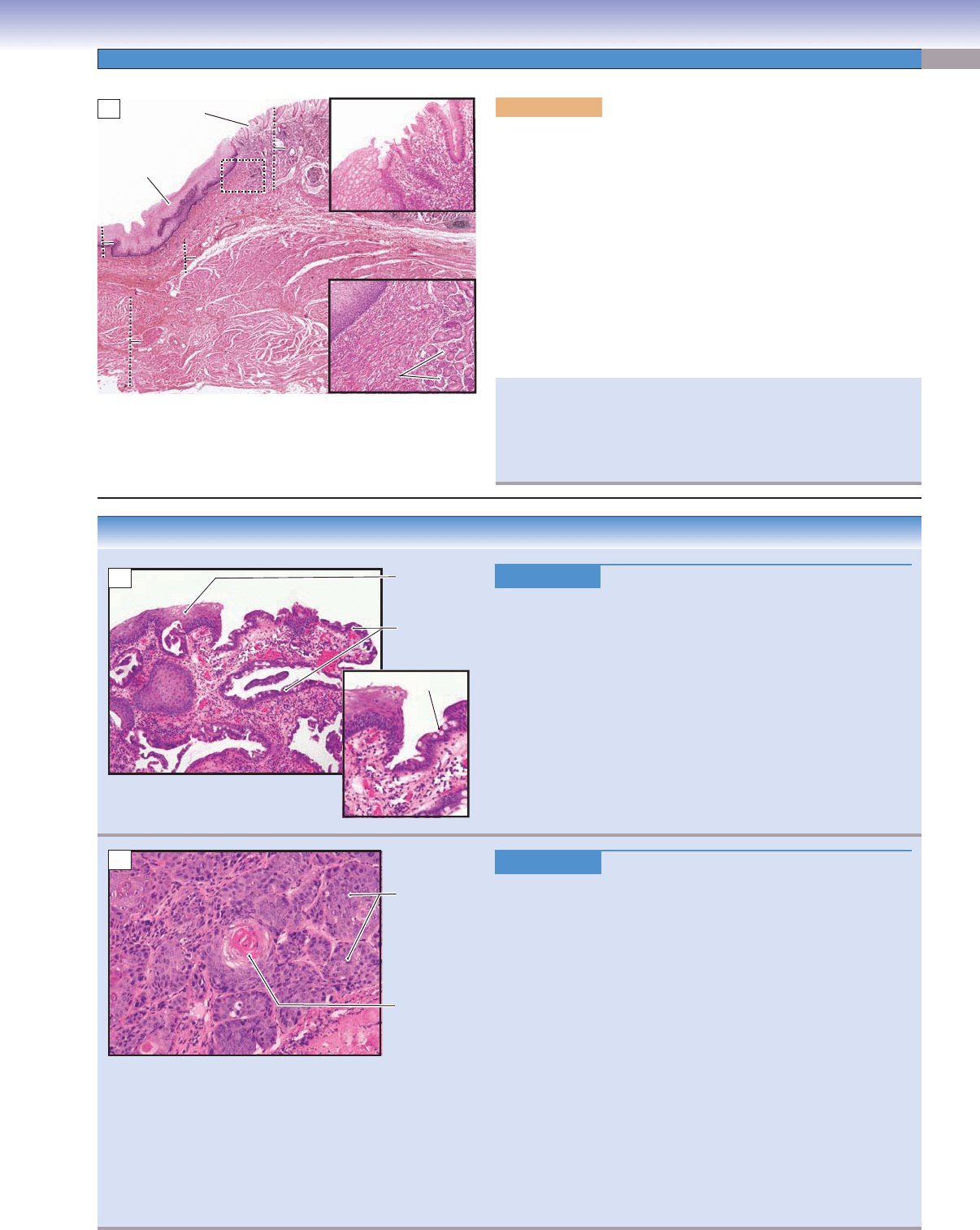
Figure 15-5A. Lower esophagus, esophagogastric junction
(esophagus on left; stomach on right of illustration). H&E, 11;
insets (upper) 57; (lower) 45
The lower esophagus meets the stomach at the esophagogastric junction.
The esophagus is lined by stratifi ed squamous epithelium, and the car-
diac region of the stomach is lined by simple columnar epithelium. The
change in the lining epithelium refl ects the change in function from a
conduit for food transport to an organ of digestion. The muscularis
externa of the lower esophagus is composed of two layers of smooth
muscle fi bers, which are controlled by the vagus nerve. Mucous glands
are also found in the lamina propria of the lower esophagus (right
inset). These glands are called esophageal cardiac glands. They pro-
duce mucus to protect the epithelial wall of the esophagus from the
refl ux of acidic gastric juices coming from the stomach.
In some patients, the epithelium of the lower esophagus (stratifi ed
squamous epithelium) changes to stomachlike epithelium (simple
columnar epithelium). This pathologic change is called metaplasia.
It is due to the long-term chemical irritation caused by gastroesopha-
geal refl ux.
CLINICAL CORRELATIONS
Figure 15-5B.
Barrett Esophagus. H&E, 48; inset 82
Barrett esophagus is a chronic complication of gastroesophageal
refl
ux disease (GERD), characterized by metaplasia of the strati-
fi ed squamous epithelium of the lower esophagus into a special-
ized glandular epithelium with goblet cells. Patients with Barrett
esophagus have an increased risk of developing adenocarcinoma
(cancer of the esophagus) of the distal esophagus. Common symp-
toms include heartburn, trouble swallowing, and weight loss.
Endoscopically, Barrett esophagus appears as salmon-colored
“tongues” of mucosa extending proximally from the gastroe-
sophageal junction. This photomicrograph shows the metaplastic
glandular epithelium with goblet cells that have replaced the
normal squamous epithelium and the infl ammatory cells (mainly
lymphocytes and plasma cells) infi ltrating the connective tissue.
Figure 15-5C.
Esophageal Carcinoma. H&E, 97
Esophageal carcinoma is a malignant neoplasm that stems
from the epithelial cells lining the inner surface of the esopha-
gus. W
orldwide, squamous cell carcinoma is the most common
type of esophageal cancer, and it is associated with alcohol and
tobacco use in the United States and Europe and with mutagenic
substances and nutritional defi ciencies in less-well-developed
parts of the world. In the United States, adenocarcinoma of the
lower esophagus is becoming more frequent, representing about
50% of esophageal cancers. The major known risk factor for
the development of adenocarcinoma is chronic GERD causing
Barrett esophagus, a metaplastic change in the squamous mucosa
of the distal esophagus to a glandular type of epithelium with
goblet cells. Esophageal cancer is characterized by progressive
diffi culty in swallowing, loss of weight, fatigue, and chest pain.
Pathological changes include ulcerations, exophytic masses, and
thickening and narrowing of the lumen. Treatment includes sur-
gery (esophagectomy) and chemotherapy. This photomicrograph
shows a moderately differentiated squamous cell carcinoma with
focal keratin production in the center, called a keratin pearl.
Metaplastic
Barrett
epithelium with
goblet cells
Squamous
epithelium
Goblet cell
B
Keratin pearl
Squamous cell
carcinoma
C
CUI_Chap15.indd 287 6/2/2010 3:23:49 PM
288
UNIT 3
■
Organ Systems
Stomach
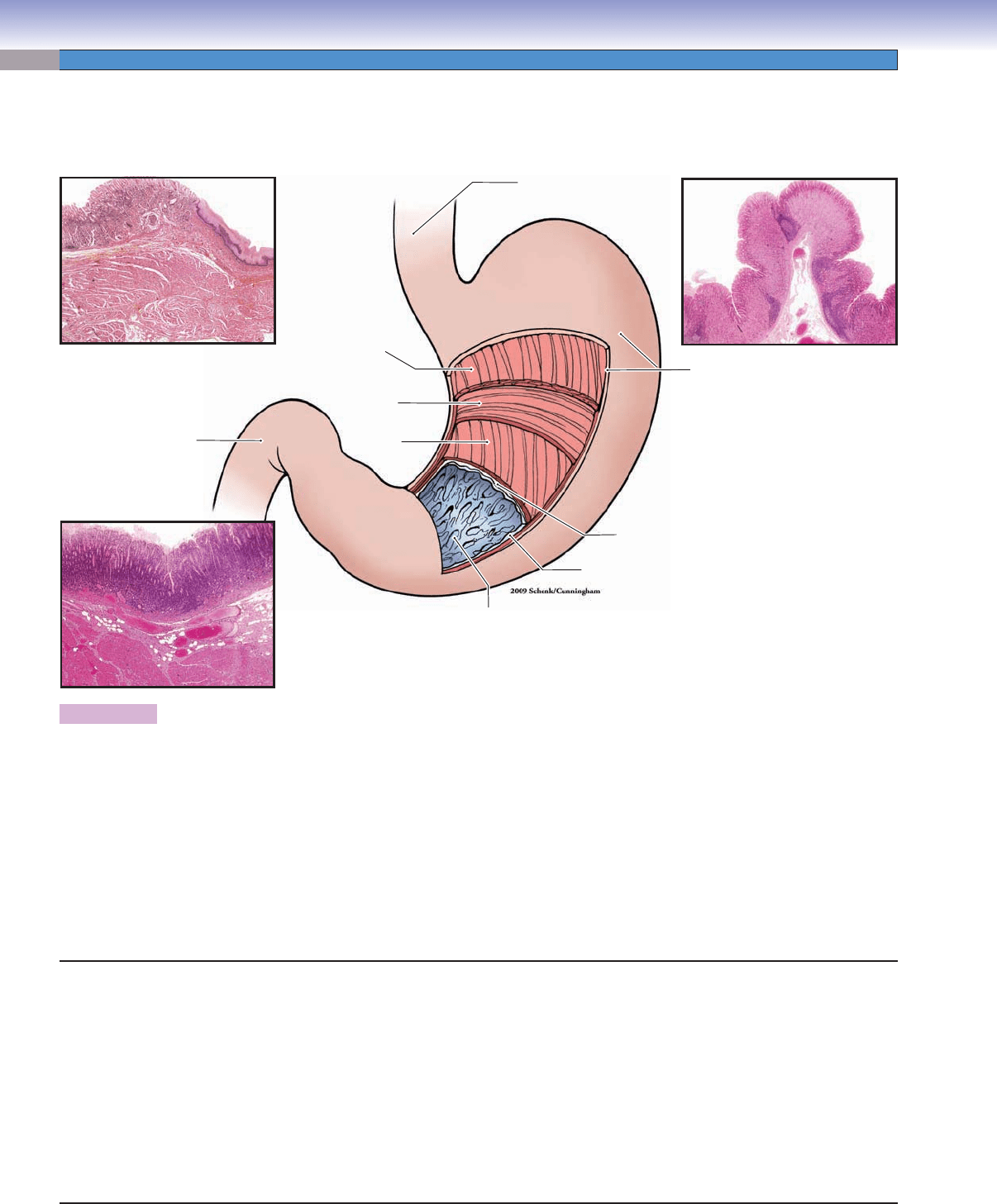
Figure 15-6. Overview of the stomach. H&E, insets (upper left) 5; (lower left) 9; (right) 7.
The stomach is a “J”-shaped hollow organ. It connects the esophagus and duodenum of the small intestine. The stomach initiates
digestion of food and temporarily stores food. It can be divided into four parts: the cardia, fundus, body, and pylorus. Histologically,
stomach tissue can be distinguished by its mucosal glands (glands in the mucosa). (1 and 2) The cardia connects to the esophagus,
and the pylorus connects to the duodenum. These two ends of the stomach have similar histological characteristics. The mucosal
glands of the cardia and pylorus are called cardiac glands and pyloric glands, respectively. Both contain many mucus-secreting
cells and produce mucus, which is a thick, gel-like material that coats the surface of the stomach and protects it from acidic gastric
fl uid. Mucus-secreting cells contribute a small volume to the gastric juices. (3 and 4) The fundus and body of the stomach form the
largest part of the stomach (about two thirds). The mucosal glands in this region are called fundic (gastric) glands. These glands
are composed mainly of parietal and chief cells, which produce large volumes of gastric juices. A small number of various types of
enteroendocrine cells are found at the base of the gastric glands. The gastric juices contain primarily water, HCl, mucus, pepsin, IF,
rennin, and lipase. This is a highly acidic fl uid and plays an important role in digesting food.
Fundus of stomach
Pylorus of stomach
Esophagus
Fundus
Body
Gastric
rugae
Serosa
Submucosa
Mucosa
Oblique
muscle
Circular
muscle
Cardia
Longitudinal
muscle
Pylorus
Duodenum
Esophagogastric
junction
Stomach
I. Cardia
A. Cardiac glands
B. Mucus-secreting cells (produce mucus and lysozyme)
II. Fundus and Body
A. Fundic (gastric) glands
B. Mucous neck cells (secrete mucus)
C. Parietal cells (secrete HCl and gastric IF)
D. Chief cells (secrete pepsinogen, rennin, and lipase)
E. Enteroendocrine (diffuse neuroendocrine) cells (release,
e.g., gastrin, histamine, and serotonin)
III. Pylorus
A. Pyloric glands
B. Mucus-secreting cells (produce mucus and lysozyme)
C. Enteroendocrine cells
D. G cells (secrete gastrin)
E. D cells (release somatostatin)
CUI_Chap15.indd 288 6/2/2010 3:23:54 PM
CHAPTER 15
■
Digestive Tract
289
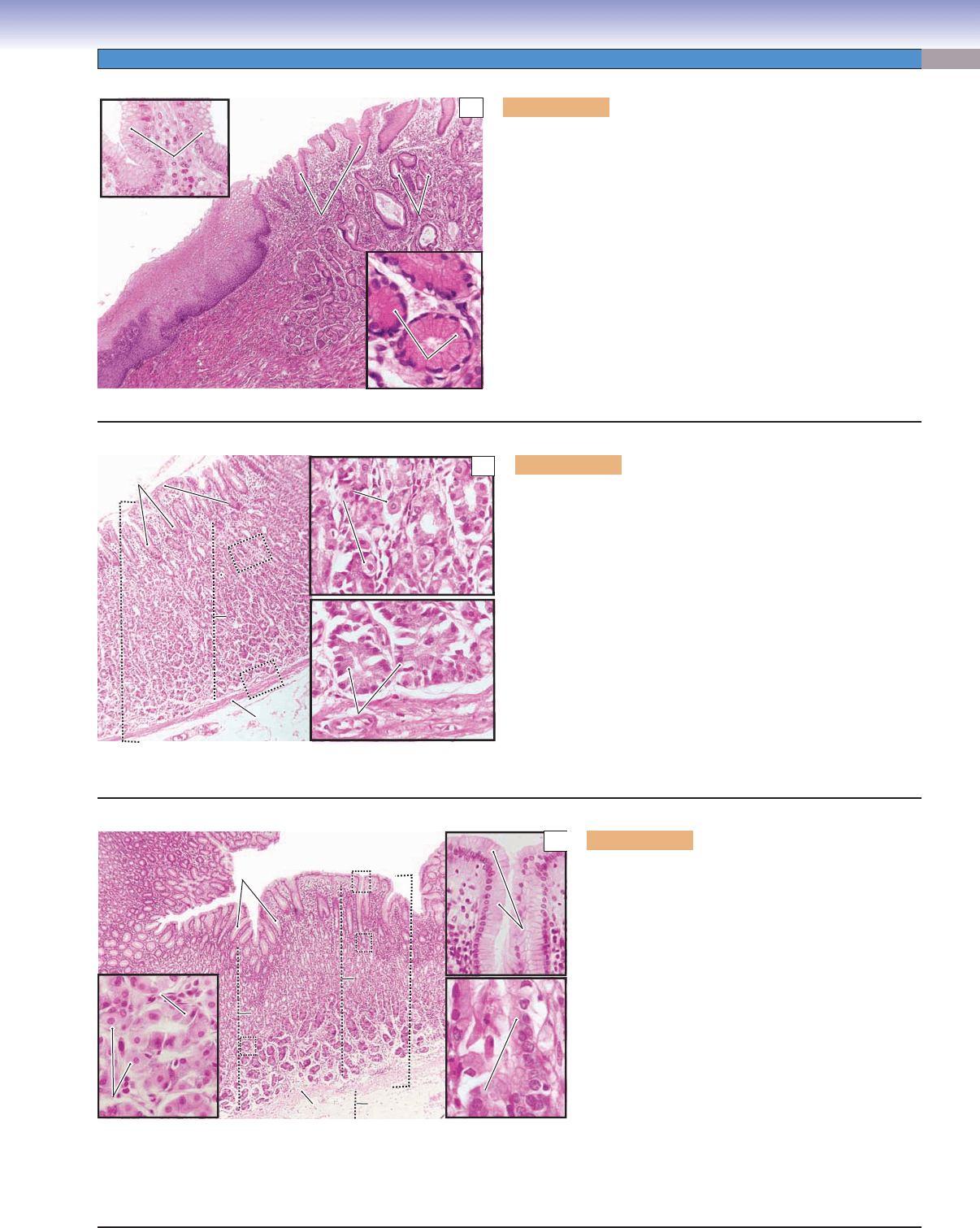
Figure 15-7A. Cardiac region, esophagogastric junction. H&E,
34; insets (left) 192, (right) 331
The inner surface of the stomach is lined by columnar epithelium,
which forms a secretory sheath and is composed of mucus- secreting
cells called surface mucous cells. These cells cover the entire inner
surface of the stomach and also line the surface of the gastric pits.
The gastric pits are invaginations of the epithelium and are sur-
rounded by the lamina propria. This is an example of the cardiac
region of the stomach at the esophagogastric junction. The lamina
propria (loose connective tissue) contains cardiac glands. These
glands are branched tubular glands (see Fig. 3-22A,B) and are
composed of mucus-secreting cells. The secretions of the cardiac
glands empty directly into the gastric pits. The cardiac glands con-
sist of mucous cells, which are similar in appearance to the surface
mucous cells. They have basally positioned nuclei and lightly stain-
ing cytoplasm.
Mucus-secreting cells
Mucus-secreting cells
of cardiac glands
of cardiac glands
Mucus-secreting cells
of cardiac glands
E
E
s
s
o
o
p
p
h
h
a
a
g
g
u
u
s
s
Esophagus
Gastric
Gastric
pits
pits
Gastric
pits
Cardiac
Cardiac
glands
glands
Cardiac
glands
Surface
Surface
mucous cells
mucous cells
Surface
mucous cells
S
S
to
to
m
m
a
a
c
c
h
h
Stomach
A
Figure 15-7B. Fundic region of the stomach. H&E, 51;
insets 245
The surface of the fundus region of the stomach is covered by
surface mucous cells, which produce mucus to protect the epi-
thelium from the acidic gastric juice. The fundic glands in the
lamina propria are different from the cardiac glands but similar
to the glands in the body of the stomach. Fundic glands con-
tain stem cells, mucous neck cells (Fig. 15-7C), parietal cells, and
chief cells. The stem cells can differentiate into other types of
cells in the glands. The parietal cells are large, round cells with
centrally positioned nuclei (“fried-egg” appearance). Their cyto-
plasm stains paler than that of chief cells. The parietal cells are
more numerous in the superior half of the fundic glands (upper
inset). The chief cells are small, columnar cells and have darkly
stained cytoplasm. Their nuclei are commonly located at the base
of the cells. The chief cells are more numerous in the inferior half
of the fundic glands (lower inset).
Muscularis
Muscularis
mucosae
mucosae
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
Muscularis
mucosae
Chief cells
Chief cells
Chief cells
M
M
u
u
c
c
o
o
s
s
a
a
Mucosa
Fundic
Fundic
glands
glands
Fundic
glands
Gastric
Gastric
pits
pits
Gastric
pits
Epithelium
Epithelium
(mucous
(mucous
surface cells)
surface cells)
Epithelium
(mucous
surface cells)
Parietal
Parietal
cells
cells
Parietal
cells
B
Figure 15-7C. Body region of the stomach. H&E,
34; insets (left) 232; (right upper) 164; (right
lower) 394
Histologically, the body and fundus of the stomach are
similar to one another, and their glands are identical.
They are called fundic (gastric) glands. The mucous
neck cells are commonly found between the parietal
cells at the neck region of the gastric glands. They secrete
acidic mucus. The parietal cells secrete large quanti-
ties of HCl and gastric IF. The parietal cells are also
called oxyntic (acid-forming) cells. The chief cells are
often called zymogenic or peptic cells; their cytoplasm
contains zymogen granules. They secrete pepsinogen
and precursors of rennin and lipase. Enteroendocrine
cells may also be found at the neck and base of the
gastric glands. They release endocrine molecules (e.g.,
serotonin, gastrin, histamine). These cells are similar
in appearance to the enteroendocrine cells in the small
intestine (see Fig. 15-13B). Stem cells may also be
found at neck regions of the gastric glands.
Submucosa
Submucosa
Submucosa
Lamina
Lamina
propria
propria
Lamina
propria
M
M
u
u
c
c
o
o
s
s
a
a
Mucosa
Fundic
Fundic
glands
glands
Fundic
glands
Muscularis mucosae
Lumen
Lumen
Lumen
Gastric
Gastric
pits
pits
Gastric
pits
Surface
Surface
mucous cells
mucous cells
Surface
mucous cells
Mucous neck cell
Mucous neck cell
Mucous neck cell
Parietal cells
Parietal cells
Parietal cells
Chief cellChief cell
Chief cell
Chief cell
C
CUI_Chap15.indd 289 6/2/2010 3:23:57 PM
290
UNIT 3
■
Organ Systems
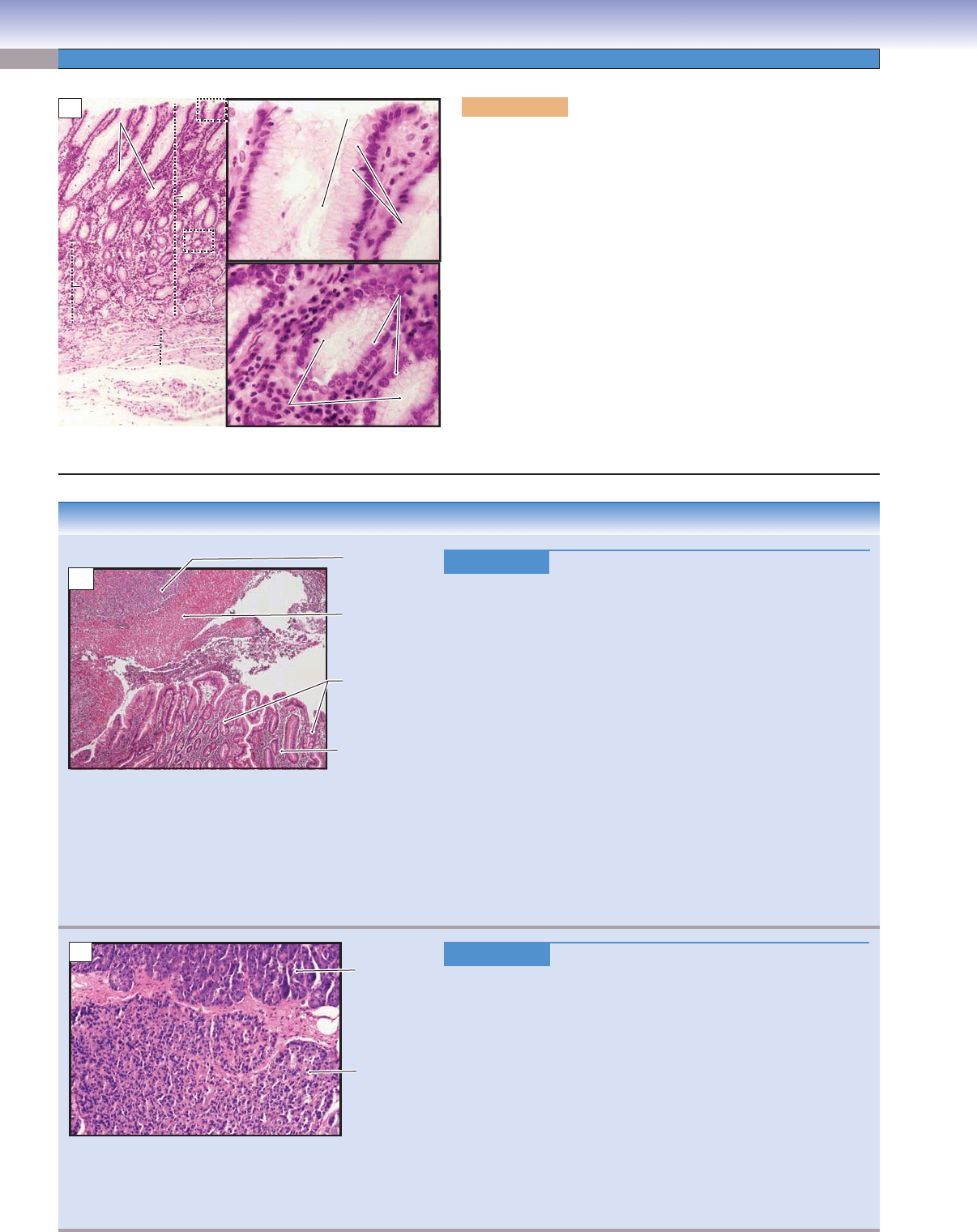
CLINICAL CORRELATIONS
Figure 15-8B.
Gastric Ulcer (Peptic Ulcer). H&E, 19
Peptic ulcers are chronic mucosal lesions that occur in the gastro-
intestinal tract. The duodenum and stomach are the most common
sites for ulcers. Causes of these ulcers include Helicobacter pylori
infection, long-term use of nonsteroidal anti-infl ammatory
drugs
and corticosteroids, and cigarette smoking. Epigastric burning or
pain, bleeding, and even perforation are the common signs and
symptoms of the peptic ulcers. Morphologically, peptic ulcers are
usually small, round to oval in shape, less than 4 cm in diameter with
well-defi ned margins without elevation, and have a clean, smooth
base. Histologically, a thin layer of necrotic fi brinoid debris with
neutrophil infi ltration is seen, beneath which lies granulation tis-
sue. Treatments include using H
2
receptor antagonists; antibiotics;
proton pump inhibitors; and surgery for severe, refractory cases.
Care must be taken to differentiate benign ulcers from malignant
adenocarcinomas, which may appear ulcerated. This image shows
the transition from gastric mucosa to ulcer, showing a fi brinopuru-
lent surface with underlying granulation tissue. The gastric mucosa
shows chronic gastritis with plasma cells within the lamina propria
and intestinal metaplasia (note the goblet cells).
Figure 15-8C.
Gastrinoma (Zollinger-Ellison Syndrome). H&E, 97
Gastrinomas, also called Zollinger
-Ellison syndrome, are neoplasms
producing the hormone gastrin, which commonly arise in the duo-
denum and pancreas. Hypersecretion of gastrin by the tumor leads
to hypergastrinemia, resulting in excess production of gastric acid.
Patients have symptoms of peptic ulcers, with clinical fi ndings, such
as epigastric tenderness, bleeding, and perforation. Pathologic fi nd-
ings include hyperplasia of the parietal cells that produce gastric
acid within the mucosa of the stomach. Tumor cells resemble pan-
creatic endocrine cells, are well differentiated, and contain gastrin
peptides within the secretory granules. Proton pump inhibitors and
surgical removal of the tumor are the fi rst treatment choice for this
syndrome. This image shows normal pancreatic parenchyma (upper
portion) and a well-circumscribed gastrinoma (lower portion). Note
the relatively uniform neoplastic cells within the gastrinoma.
Gastric mucosa
(with intestinal
metaplasia)
Chronic gastritis
Granulation
tissue
Fibrinopurulent
exudate (ulcer)
B
Normal
pancreatic
parenchyma
Gastrinoma
C
Figure 15-8A. Pyloric region of the stomach. H&E, 68;
insets 283
The pylorus is the last region of the stomach and connects to the
duodenum. The mucosa of the pylorus has deep gastric pits. Pyloric
glands, composed primarily of mucus-secreting cells, empty their
secretory products into the base of the gastric pits. These mucus-
secreting cells are pale staining and have basally located nuclei, as
do the cells of the cardiac glands. They produce mucus to protect the
epithelium of the pylorus from acidic gastric secretions. Two types
of enteroendocrine cells are found at the base of the pyloric glands.
G cells release gastrin, which stimulates parietal cells to secrete HCl.
Another type of enteroendocrine cell, called the D cell, releases
somatostatin, which inhibits the release of gastrin by G cells. These
two types of enteroendocrine cells are also found in the mucosa of
the duodenum (see Fig. 15-13B). The upper inset shows a gastric
pit and surface mucous cells in the superior portion of the mucosa.
The lower inset shows pyloric glands and mucus-secreting cells in
an inferior portion of the mucosa. Both cell types have basally posi-
tioned nuclei and clear cytoplasm containing secretory granules.
Pyloric
Pyloric
glnads
glnads
Pyloric
glands
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
Submucosa
Submucosa
Submucosa
Pyloric
Pyloric
glnads
glnads
Pyloric
glands
Surface
Surface
mucous cells
mucous cells
Surface
mucous cells
Mucus-secreting
Mucus-secreting
cells
cells
Mucus-secreting
cells
Gastric pits
Gastric pits
Gastric pits
Mucosa
Mucosa
Mucosa
Gastric pits
Gastric pits
Gastric pits
A
CUI_Chap15.indd 290 6/2/2010 3:24:05 PM
CHAPTER 15
■
Digestive Tract
291
Small Intestine
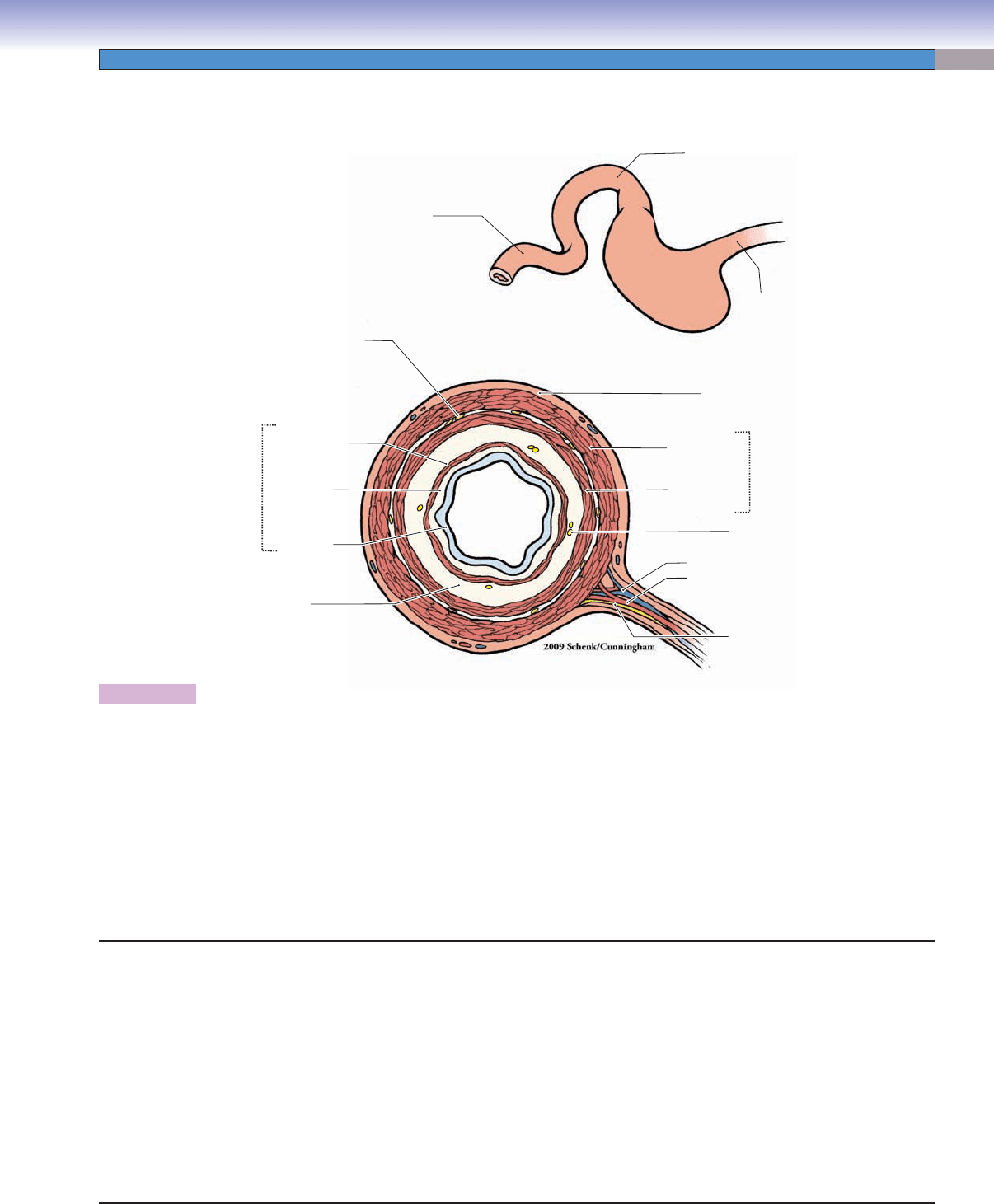
Figure 15-9. Overview of the small intestine.
The small intestine is a very long, tubular organ, about 6 to 7 m long, with a relatively small diameter. It connects the stomach to the
large intestine and can be divided into three regions based on anatomy and function. (1) The duodenum, the most proximal region
of the small intestine, is a short, C-shaped segment about 20 to 25 cm long. Mucous glands called Brunner glands are present only
in the duodenum. Bile and pancreatic secretions enter the duodenum through their duct systems. (2) The jejunum makes up about
two fi fths of the rest of the small intestine. It has a larger diameter and thicker wall than the ileum. The jejunum has long villi and
has neither Brunner glands nor Peyer patches. (3) The ileum is the most distal portion of the intestine, and it makes up about three
fi fths of the small intestine. The ileum has a thinner wall and fewer villi than the jejunum, and it has clusters of lymphatic nodules,
called Peyer patches, in the lamina propria. This illustration shows the general tunics (layers) of the small intestine. Like the other
parts of the digestive tract, the small intestine consists of a mucosa (epithelium, lamina propria, and muscularis mucosae), submu-
cosa, muscularis externa, and serosa/adventitia. Several myenteric (Auerbach) plexuses are illustrated between the two layers of the
muscularis externa; submucosal (Meissner) plexuses are located in the submucosal layer.
Mucosa
Myenteric (Auerbach) plexus
Jejunum
Submucosa
Epithelium
Lamina
propria
Muscularis
mucosae
Vein
Submucosal
(Meissner) plexus
Artery
Nerve
Muscularis
externa
Serosa/adventitia
Esophagus
Stomach
Inner circular
muscle
Outer
longitudinal
muscle
Duodenum
Small Intestine
I. Duodenum
A. Mucosa
B. Submucosa (Brunner glands)
C. Muscularis externa
D. Serosa/adventitia
II. Jejunum
A. Mucosa
B. Submucosa
C. Muscularis externa
D. Serosa
III. Ileum
A. Mucosa (Peyer patches)
B. Submucosa (Peyer patches may extend into this layer)
C. Muscularis externa
D. Serosa
Cell Types in the Small Intestine
Villi: columnar absorptive cells and goblet cells
Glands (crypts) of Lieberkühn: absorptive cells, goblet cells,
Paneth cells, enteroendocrine cells, and stem cells
CUI_Chap15.indd 291 6/2/2010 3:24:09 PM
292
UNIT 3
■
Organ Systems
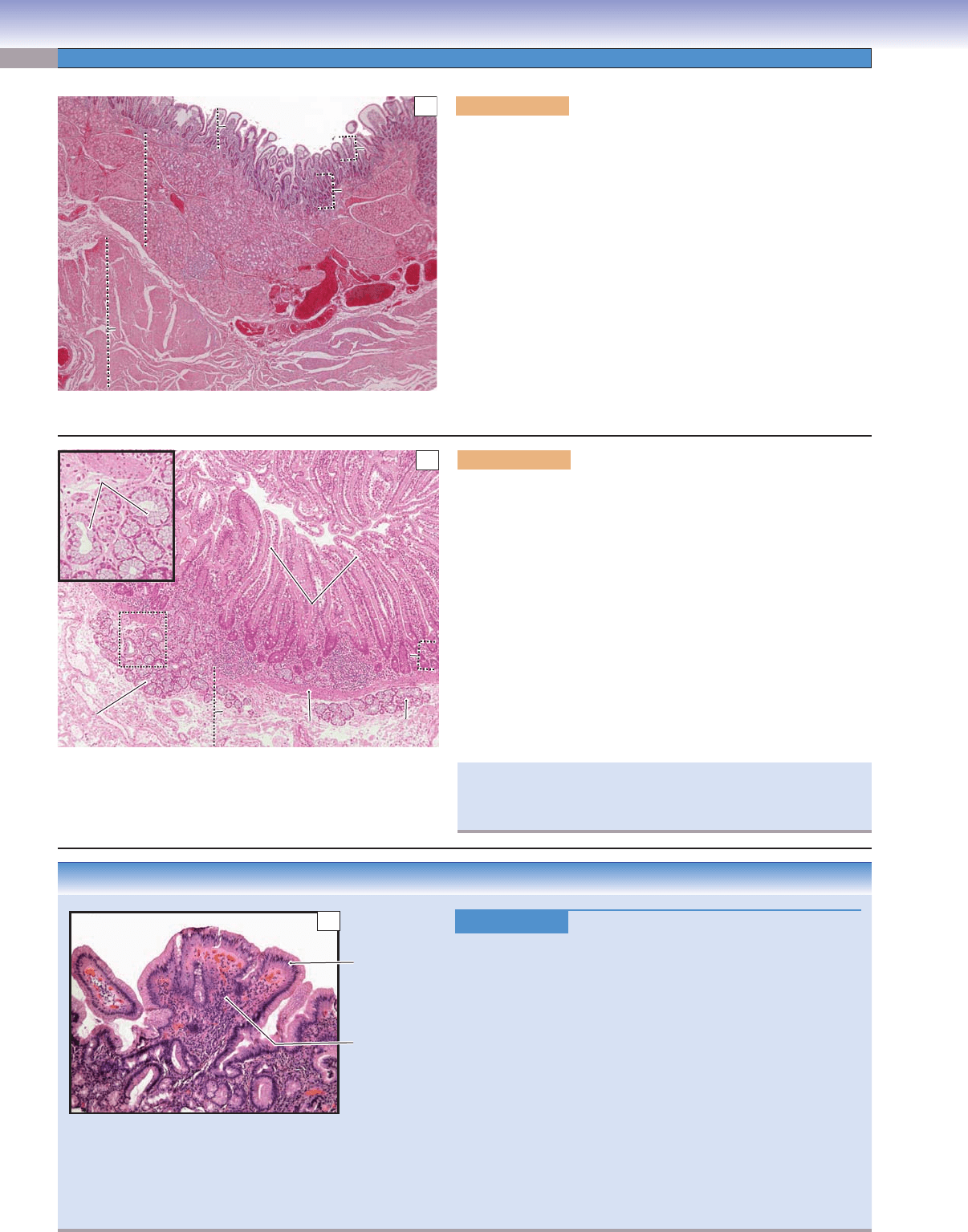
CLINICAL CORRELATION
Figure 15-10C.
Peptic Duodenitis. H&E, 48
Peptic duodenitis is an infl
ammatory process caused by chronic
exposure of the duodenal mucosa to increased levels of gastric
acid and is usually found in the fi rst portion of the duodenum, the
duodenal bulb. Symptoms of peptic duodenitis include epigas-
tric pain and dyspepsia. Histologic features include fl attening, or
blunting, of the normally fi ngerlike villi, increased infl ammatory
cells within the lamina propria, Brunner gland hyperplasia, crypt
hyperplasia, and gastric foveolar metaplasia of the epithelium.
Metaplasia to a gastric foveolar type of epithelium is an adaptive
protective response to the increased levels of acid. H. pylori may
be found in the metaplastic mucosa as seen in the stomach. In
time, a duodenal ulcer may result from peptic duodenitis. This
photomicrograph shows duodenal mucosa with complete replace-
ment of the normal epithelium with goblet cells by gastric foveo-
lar epithelium. Note the widened, distorted villi and increased
infl ammatory cells within the lamina propria.
Metaplastic
gastric mucosa
with loss of
goblet cells
Blunt, widened
villous with
inflammation
C
Figure 15-10A. Duodenum, small intestine. H&E, 14
The duodenum connects to the stomach. The mucosa of the duode-
num is composed of simple columnar epithelium, lamina propria,
and muscularis mucosae. Epithelial cells lining the surface of the villi
and the glands of Lieberkühn include absorptive cells, goblet cells,
Paneth cells, enteroendocrine cells, and stem cells. The lamina pro-
pria is a layer of loose connective tissue, which forms the core of the
villus and contains various types of connective tissue cells includ-
ing fi broblasts, plasma cells, macrophages, and some leukocytes
(see Fig. 4-3A). The muscularis mucosae is a thin layer of smooth
muscle (Fig. 15-10B). The submucosa is a layer of dense connec-
tive tissue containing mucous glands called Brunner glands, which
produce mucus to protect the duodenal wall from acidic gastric juice
from the stomach. The muscularis externa consists of two layers of
smooth muscle: an inner circular layer and an outer longitudinal
layer. The outer layer of the duodenum is mostly covered by serosa;
areas where it is attached to other organs are covered by adventitia.
Villi
Villi
Villi
Glands of
Glands of
Lieberkühn
Lieberkühn
Glands of
Lieberkühn
Submucosa
Submucosa
Submucosa
Mucosa
Mucosa
Mucosa
Brunner
Brunner
gland
gland
Brunner
gland
Muscularis
Muscularis
externa
externa
Muscularis
externa
A
Figure 15-10B. Duodenum, small intestine. H&E, 45; inset
112
An example of the mucosa and submucosa of the duodenum is
shown. A thin layer of muscularis mucosae lies between the lamina
propria and the submucosa. Fingerlike villi project into the lumen
(Fig. 15-11B). Brunner glands are distributed in the submucosa
and extend into the lamina propria of the mucosa. Brunner glands
produce mucus that protects the epithelium from HCl secreted in
the stomach. They also secrete large numbers of bicarbonate ions,
which neutralize acidic gastric juice from the stomach. Two types
of enteroendocrine cells associated with the regulation of gastric
secretion are also found in the glands of Lieberkühn of the duode-
num: (1) G cells that release gastrin, which stimulates parietal cell
secretion of HCl and (2) D cells that release somatostatin, which
inhibits gastrin release. G cells and D cells are predominantly found
in the pylorus of the stomach but are also found in the duodenum.
L
L
u
u
m
m
e
e
n
n
Lumen
Glands of
Glands of
Lieberkühn
Lieberkühn
Villi
Villi
Glands of
Lieberkühn
Villi
Brunner
Brunner
glands
glands
Brunner
glands
Muscularis
Muscularis
mucosae
mucosae
Muscularis
mucosae
Submucosa
Submucosa
Submucosa
Brunner
Brunner
glands
glands
Brunner
glands
Brunner
Brunner
glands
glands
Brunner
glands
B
If Brunner cells are not able to produce enough mucus and bicar-
bonate ions over the long term, a duodenal (Brunner) ulcer may
develop.
CUI_Chap15.indd 292 6/2/2010 3:24:11 PM
CHAPTER 15
■
Digestive Tract
293
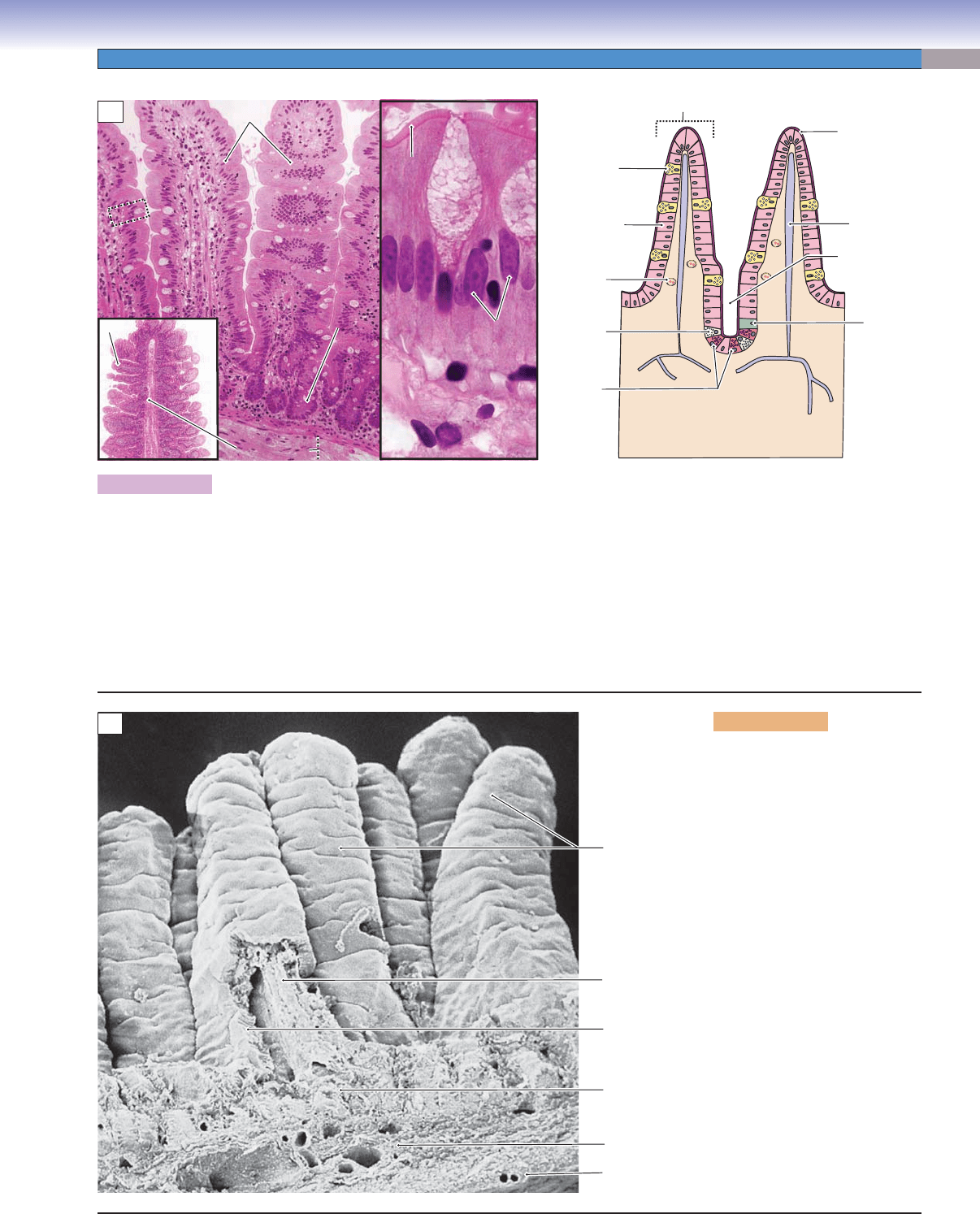
Figure 15-11A.
Plicae circulares, villi, and microvilli. H&E, 124; inset (left) 15, (right) 882
The small intestine is a long tube with three levels of folds that increase the surface area for absorption. (1) Plicae circulares (valves
of Kerckring) are gross folds involving the mucosa and submucosa that project into the lumen (left inset). (2) Villi are smaller folds
than the plicae circulares and involve only mucosa. The central core of each villus is formed by the lamina propria; the nutrients
absorbed from the lumen by absorptive cells are transported into the lamina propria. The lamina propria contains a central lacteal (a
blind-ended lymphatic vessel) and many capillaries involved in the transport of absorbed nutrients. (3) Microvilli (see Fig. 15-12B)
are at the apical surfaces of columnar absorptive cells, increasing the surface area at the cellular level. They appear as a pink border
in light microscopy and form a brush border. The drawing on the right shows various types of cells arranged in the epithelium of
the mucosa. These cells include column-shaped absorptive cells (enterocytes), goblet cells, Paneth cells, and enteroendocrine cells.
The central lacteals are also illustrated.
T. Yang
Lacteal
Microvilli
(brush border)
Stem
cell
Goblet
cell
Capillary
Paneth
cells
Columnar
absorptive
cell
Entero-
endocrine
cell
Goblet
Goblet
cell
cell
Goblet
cell
Columnar
Columnar
absorptive cells
absorptive cells
Columnar
absorptive cells
Lamina propria
Lamina propria
Lamina propria
Microvilli
Microvilli
Microvilli
Villus
Plicae circulare
Plicae circulare
Plicae circulare
Villus
Submucosa
Submucosa
Submucosa
Gland (crypt)
Gland (crypt)
of Lieberkühn
of Lieberkühn
Gland (crypt)
of Lieberkühn
Lumen of the
gland (crypt)
of Lieberkühn
Lamina
Lamina
propria
propria
Lamina
propria
Villi
Villi
Villi
A
Villi
Lamina propria
Submucosa
Epithelium
Serosa
Muscularis
externa
B
Figure 15-11B. Villi of the
small intestine. SEM, 170
An example of a scanning electron
microscopy image showing fi n-
gerlike villi extending from the
intestinal wall and projecting into
the lumen is shown. Each villus is
composed of mucosa (epithelium
and lamina propria). The lamina
propria (connective tissue) forms
the central core of the villus. Epi-
thelium with microvilli forms the
outer layer of the villus. The villi
are unique structures in the small
intestine; they are found neither
in the stomach nor in the large
intestine. The villi are tallest in
the duodenum and shortest in the
ileum. They gradually reduce in
height and size from the proximal
regions to the distal regions of the
small intestine. The submucosa
and muscularis externa are also
shown here. The outermost layer
of the intestinal wall is serosa.
CUI_Chap15.indd 293 6/2/2010 3:24:17 PM
294
UNIT 3
■
Organ Systems
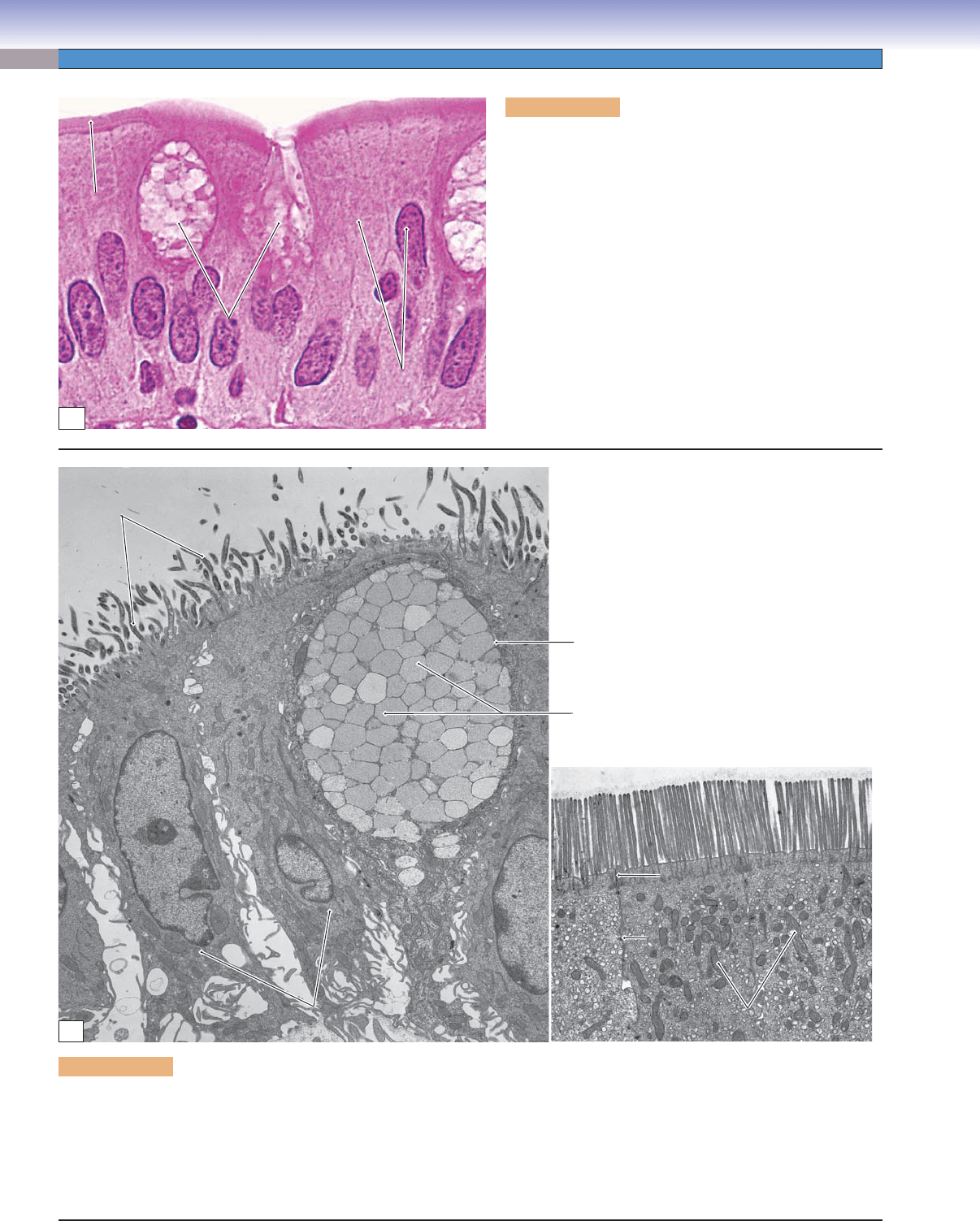
Figure 15-12B. Goblet cells, columnar absorptive cells, and microvilli. EM, (left, large intestine) 4,831, (right, small intestine)
6,906
There are numerous mitochondria in the apical cytoplasm of the columnar absorptive cells. Junction complexes are located between
neighboring cells near the lumen, and microvilli are present on the apical surfaces of the absorptive cells. A goblet cell with many
mucus-secretory granules in the cytoplasm is also shown here. These granules contain mucinogen and are released onto the surface
of the epithelium by exocytosis. During exocytosis, mucinogen becomes hydrated and forms mucin, which expands greatly in
volume after it is released from the goblet cell.
Mucus (mucinogen) granules
Goblet cell
Microvilli
Microvilli
Microvilli
Tight junctions
Tight junctions
Tight junctions
Desmosome
Desmosome
Desmosome
Mitochondria
Mitochondria
of absorptive cells
of absorptive cells
Mitochondria
of absorptive cells
Absorptive cells
Absorptive cells
Absorptive cells
Microvilli
Microvilli
Microvilli
B
Goblet
Goblet
cells
cells
Goblet
cells
Columnar
Columnar
absorptive
absorptive
cells
cells
Columnar
absorptive
cells
Microvilli
Microvilli
Microvilli
A
Figure 15-12A. Columnar absorptive and goblet cells of
the small intestine. H&E, 1,422
The columnar absorptive cells of the small intestine are also
called enterocytes or intestinal absorptive cells. They are tall
and columnar in shape; oval-shaped nuclei lie in the basal
region of the cells. The columnar absorptive cells are the
predominant cells in the epithelium of the small intestine.
The apical surfaces of the cells are covered by microvilli,
which are coated with glycocalyx. The microvilli increase
the cellular surface area for absorption. Goblet cells are
interspersed among the absorptive cells. These are unicellu-
lar glands (see Fig. 3-20A,B) with a distinctive goblet shape.
The goblet cells are mucus-secreting cells, and their numbers
gradually increase from the proximal (duodenum) to the dis-
tal (ileum) portions of the small intestine.
CUI_Chap15.indd 294 6/2/2010 3:24:21 PM