Мир М.Афзал Атлас клинического диагноза
Подождите немного. Документ загружается.

8
ATLAS
OF
CLINICAL
DIAGNOSIS
152
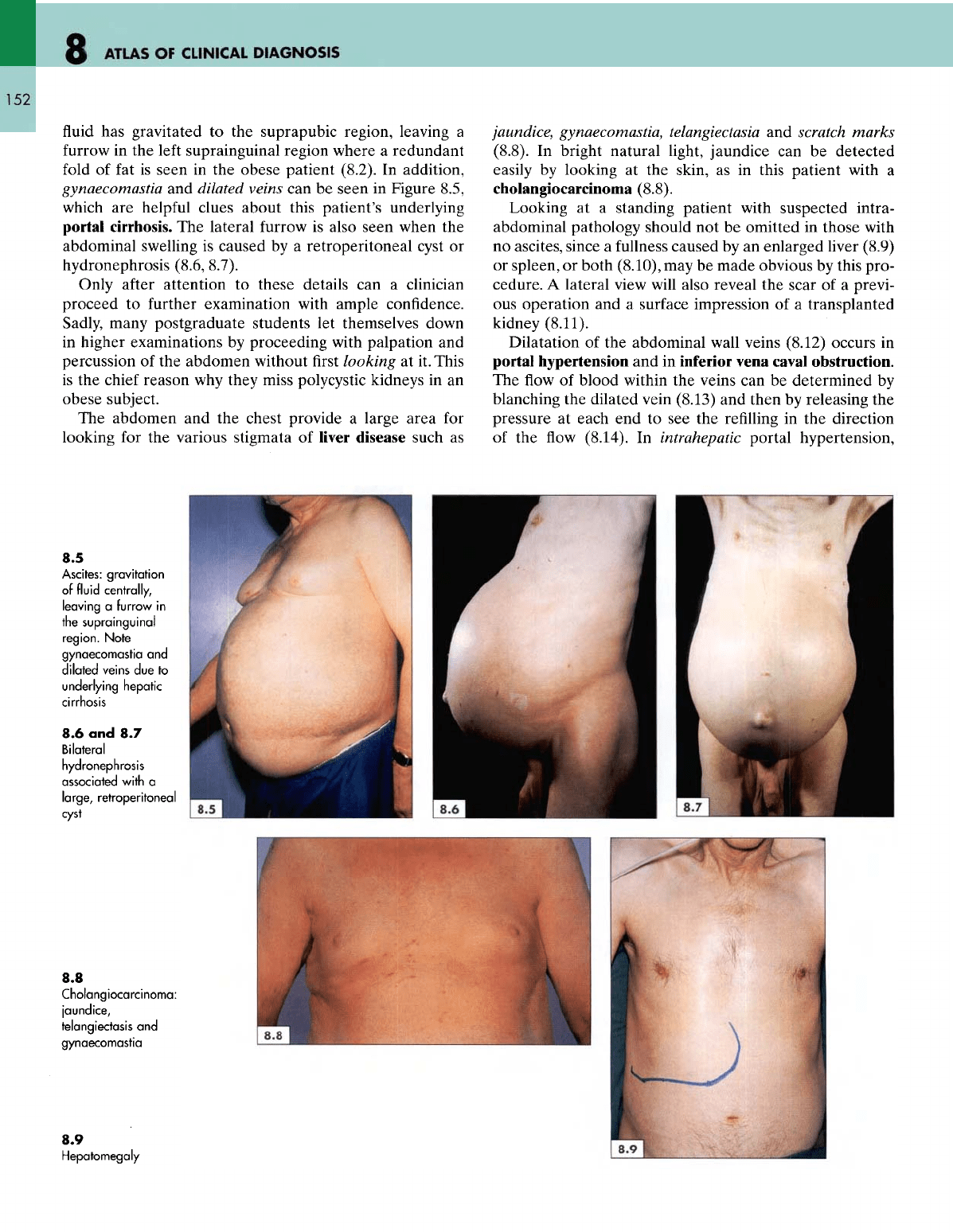
fluid has
gravitated
to the
suprapubic region, leaving
a
furrow
in the
left
suprainguinal region where
a
redundant
fold
of fat is
seen
in the
obese patient (8.2).
In
addition,
gynaecomastia
and
dilated veins
can be
seen
in
Figure 8.5,
which
are
helpful
clues about this patient's underlying
portal
cirrhosis.
The
lateral
furrow
is
also
seen
when
the
abdominal swelling
is
caused
by a
retroperitoneal cyst
or
hydronephrosis
(8.6, 8.7).
Only after attention
to
these details
can a
clinician
proceed
to
further
examination with ample confidence.
Sadly,
many postgraduate students
let
themselves down
in
higher examinations
by
proceeding with palpation
and
percussion
of the
abdomen without
first
looking
at it.
This
is
the
chief reason
why
they miss polycystic kidneys
in an
obese subject.
The
abdomen
and the
chest provide
a
large area
for
looking
for the
various stigmata
of
liver
disease such
as
jaundice, gynaecomastia, telangiectasia
and
scratch marks
(8.8).
In
bright natural light, jaundice
can be
detected
easily
by
looking
at the
skin,
as in
this patient with
a
cholangiocarcinoma
(8.8).
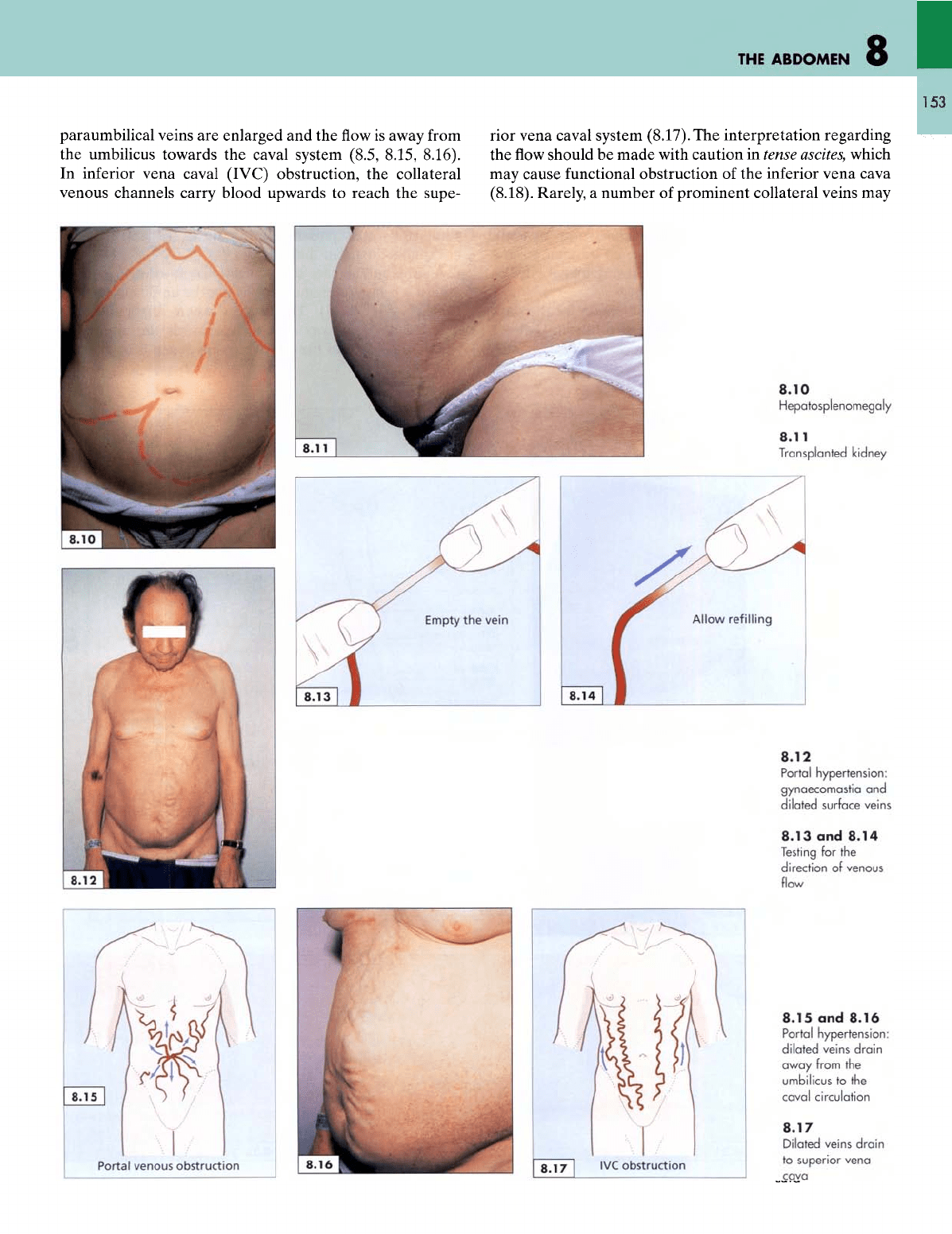
Looking
at a
standing patient with suspected intra-
abdominal pathology should
not be
omitted
in
those with
no
ascites, since
a
fullness
caused
by an
enlarged liver (8.9)
or
spleen,
or
both
(8.10),
may be
made obvious
by
this pro-
cedure.
A
lateral view
will
also reveal
the
scar
of a
previ-
ous
operation
and a
surface impression
of a
transplanted
kidney
(8.11).
Dilatation
of the
abdominal wall veins
(8.12)
occurs
in
portal
hypertension
and in
inferior
vena
caval
obstruction.
The flow of
blood within
the
veins
can be
determined
by
blanching
the
dilated vein (8.13)
and
then
by
releasing
the
pressure
at
each
end to see the
refilling
in the
direction
of
the flow
(8.14).
In
intrahepatic
portal hypertension,
8.5
Ascites:
gravitation
of
fluid centrally,
leaving
a
furrow
in
the
suprainguinal
region.
Note
gynaecomastia
and
dilated
veins
due to
underlying
hepatic
cirrhosis
8.6 and 8.7
Bilateral
hydronephrosis
associated
with
a
large,
retroperitoneal
cyst
8.8
Cholangiocarcinoma:
jaundice,
telangiectasis
and
gynaecomastia
8.9
Hepatomegaly
THE
ABDOMEN
153
paraumbilical
veins
are
enlarged
and the flow is
away
from
the
umbilicus towards
the
caval
system (8.5, 8.15, 8.16).
In
inferior vena caval
(IVC)
obstruction,
the
collateral
venous channels carry blood upwards
to
reach
the
supe-
rior vena caval system
(8.17).
The
interpretation regarding
the flow
should
be
made with caution
in
tense
ascites,
which
may
cause functional obstruction
of the
inferior vena cava
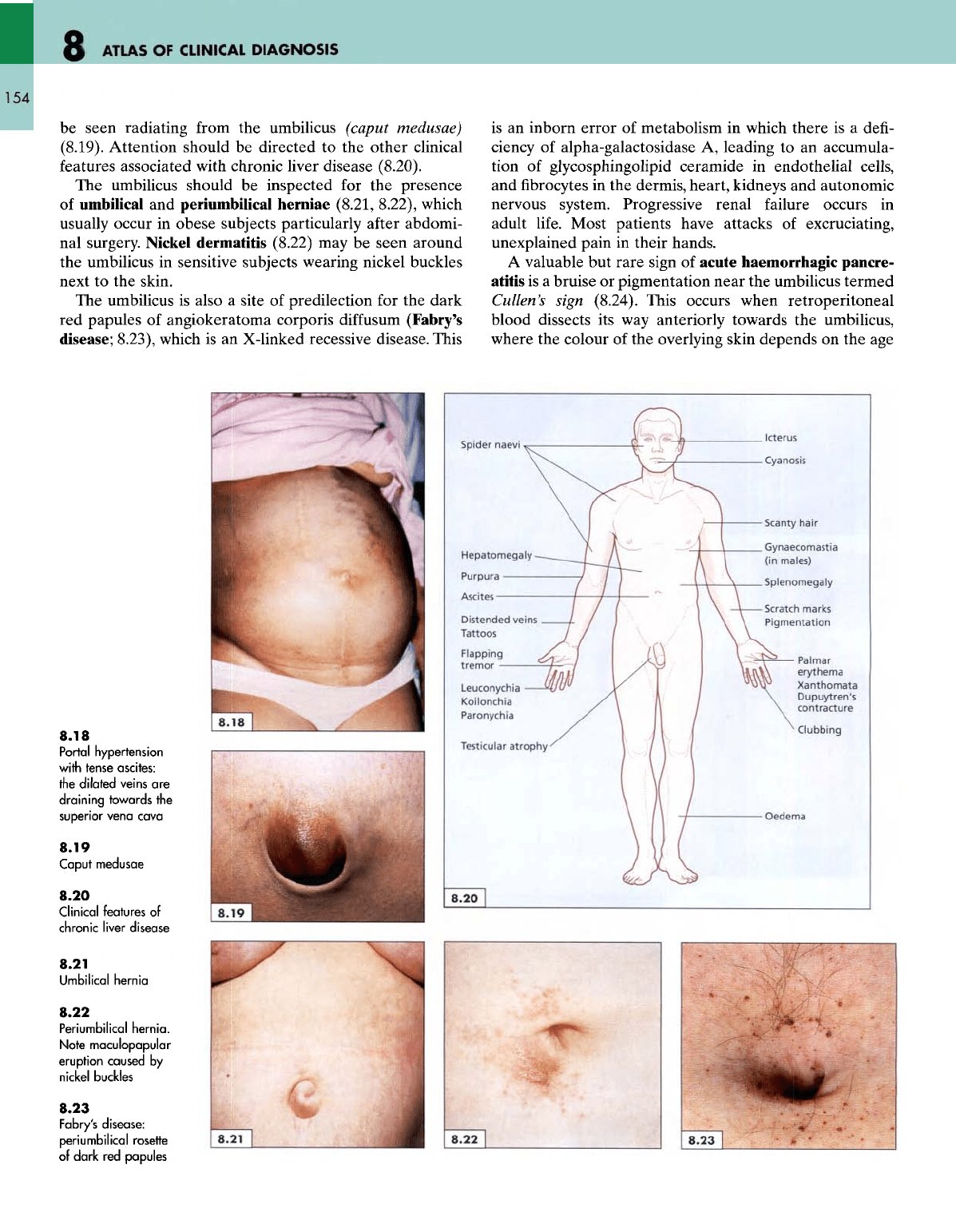
(8.18). Rarely,
a
number
of
prominent collateral veins
may
8.10
Hepatosplenomegaly
8.11
Transplanted kidney
8.12
Portal hypertension:
gynaecomastia
and
dilated
surface veins
8.13
and
8.14
Testing
for the
direction
of
venous
flow
8.15
and
8.16
Portal hypertension:
dilated
veins
drain
away
from
the
umbilicus
to the
caval circulation
8.17
Dilated
veins
drain
to
superior vena
cava
8
ATLAS
OF
CLINICAL
DIAGNOSIS
154
be
seen radiating
from
the
umbilicus
(caput
medusae)
(8.19). Attention should
be
directed
to the
other clinical
features
associated
with chronic liver
disease
(8.20).
The
umbilicus should
be
inspected
for the
presence
of
umbilical
and
periumbilical herniae (8.21, 8.22), which
usually
occur
in
obese subjects particularly
after
abdomi-
nal
surgery. Nickel dermatitis (8.22)
may be
seen around
the
umbilicus
in
sensitive subjects wearing nickel buckles
next
to the
skin.
The
umbilicus
is
also
a
site
of
predilection
for the
dark
red
papules
of
angiokeratoma corporis
diffusum
(Fabry's
disease;
8.23), which
is an
X-linked
recessive disease. This
is
an
inborn error
of
metabolism
in
which there
is a
defi-
ciency
of
alpha-galactosidase
A,
leading
to an
accumula-
tion
of
glycosphingolipid
ceramide
in
endothelial
cells,
and fibrocytes in the
dermis, heart, kidneys
and
autonomic
nervous system. Progressive renal failure occurs
in
adult
life.
Most patients have attacks
of
excruciating,
unexplained pain
in
their hands.
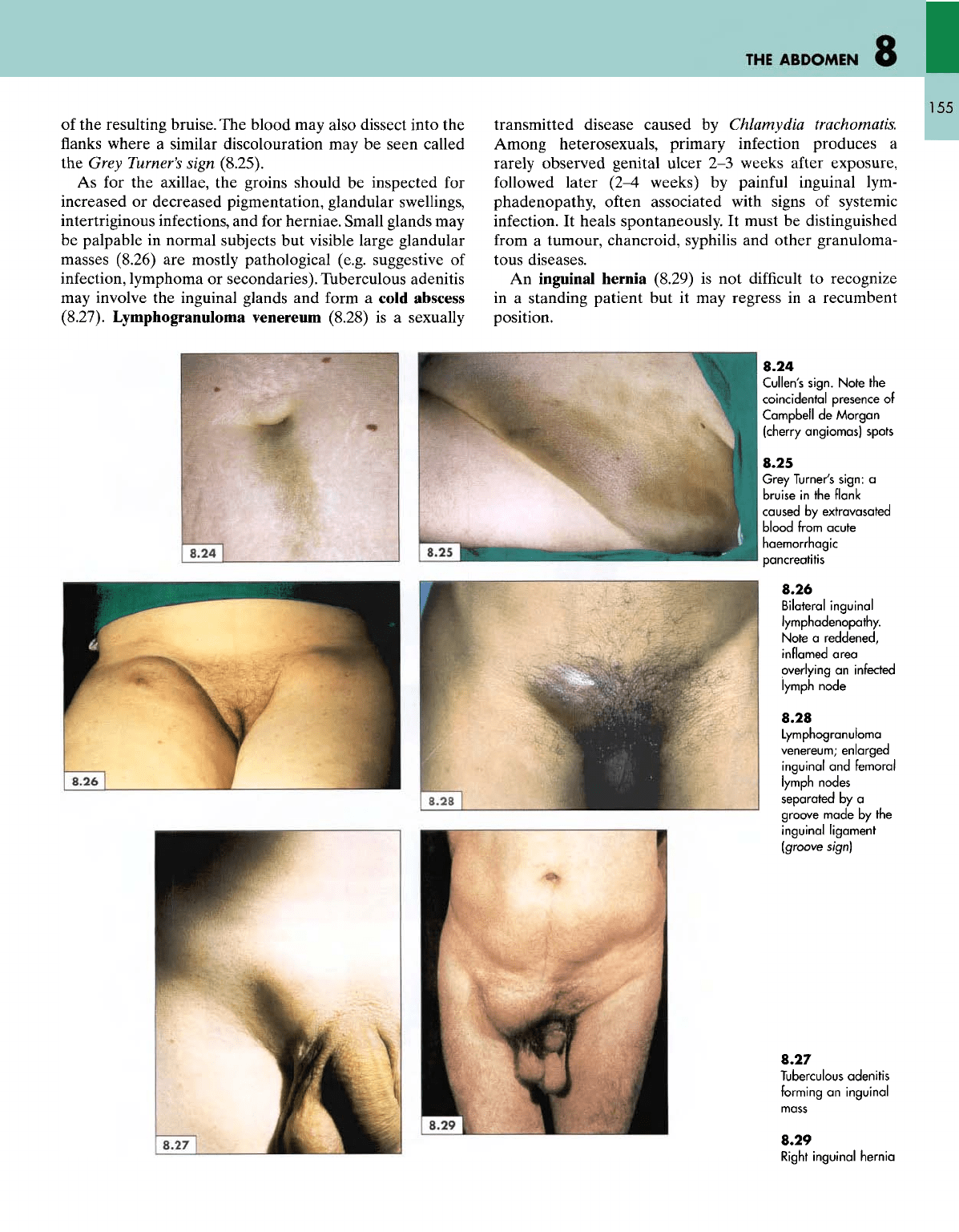
A
valuable
but
rare sign
of
acute haemorrhagic pancre-
atitis
is a
bruise
or
pigmentation near
the
umbilicus termed
Cullen's
sign (8.24). This occurs when retroperitoneal
blood dissects
its way
anteriorly towards
the
umbilicus,
where
the
colour
of the
overlying skin depends
on the age
8.18
Portal
hypertension
with
tense ascites:
the
dilated
veins
are
draining
towards
the
superior
vena
cava
8.19
Caput
medusae
8.20
Clinical
features
of
chronic
liver
disease
8.21
Umbilical
hernia
8.22
Periumbilical
hernia.
Note
maculopapular
eruption
caused
by
nickel buckles
8.23
Fabry's
disease:
periumbilical
rosette
of
dark
red
papules
Spider
naevi
Hepatomegaly
Purpura
Ascites
Distended
veins
Tattoos
Flapping
tremor
Leuconychia
Koilonchia
Paronychia
Testicular
atrophy
Oedema
8.20
8.22
THE
ABDOMEN
8
155
of
the
resulting bruise.
The
blood
may
also dissect into
the
flanks
where
a
similar discolouration
may be
seen called
the
Grey
Turner's
sign (8.25).
As for the
axillae,
the
groins should
be
inspected
for
increased
or
decreased pigmentation, glandular swellings,
intertriginous
infections,
and for
herniae.
Small glands
may
be
palpable
in
normal subjects
but
visible large glandular
masses (8.26)
are
mostly pathological (e.g. suggestive
of
infection,
lymphoma
or
secondaries). Tuberculous adenitis
may
involve
the
inguinal glands
and
form
a
cold abscess
(8.27). Lymphogranuloma
venereum
(8.28)
is a
sexually
transmitted
disease caused
by
Chlamydia trachomatis.
Among heterosexuals, primary infection produces
a
rarely observed genital ulcer
2-3
weeks after exposure,
followed
later
(2-4
weeks)
by
painful
inguinal
lym-
phadenopathy,
often
associated with signs
of
systemic
infection.
It
heals spontaneously.
It
must
be
distinguished
from
a
tumour, chancroid, syphilis
and
other granuloma-
tous diseases.
An
inguinal hernia (8.29)
is not
difficult
to
recognize
in
a
standing patient
but it may
regress
in a
recumbent
position.
8.24
Cullen's sign.
Note
the
coincidental presence
of
Campbell
de
Morgan
(cherry angiomas) spots
8.25
Grey
Turner's sign:
a
bruise
in the
flank
caused
by
extravasated
blood
from acute
haemorrhagic
pancreatitis
8.26
Bilateral
inguinal
lymphadenopathy.
Note
a
reddened,
inflamed
area
overlying
an
infected
lymph
node
8.28
Lymphogranuloma
venereum;
enlarged
inguinal
and
femoral
lymph
nodes
separated
by a
groove
made
by the
inguinal
ligament
(groove
sign)
8.27
Tuberculous
adenitis
forming
an
inguinal
8.29
Right
inguinal
hernia
8
ATLAS
OF
CLINICAL
DIAGNOSIS
156
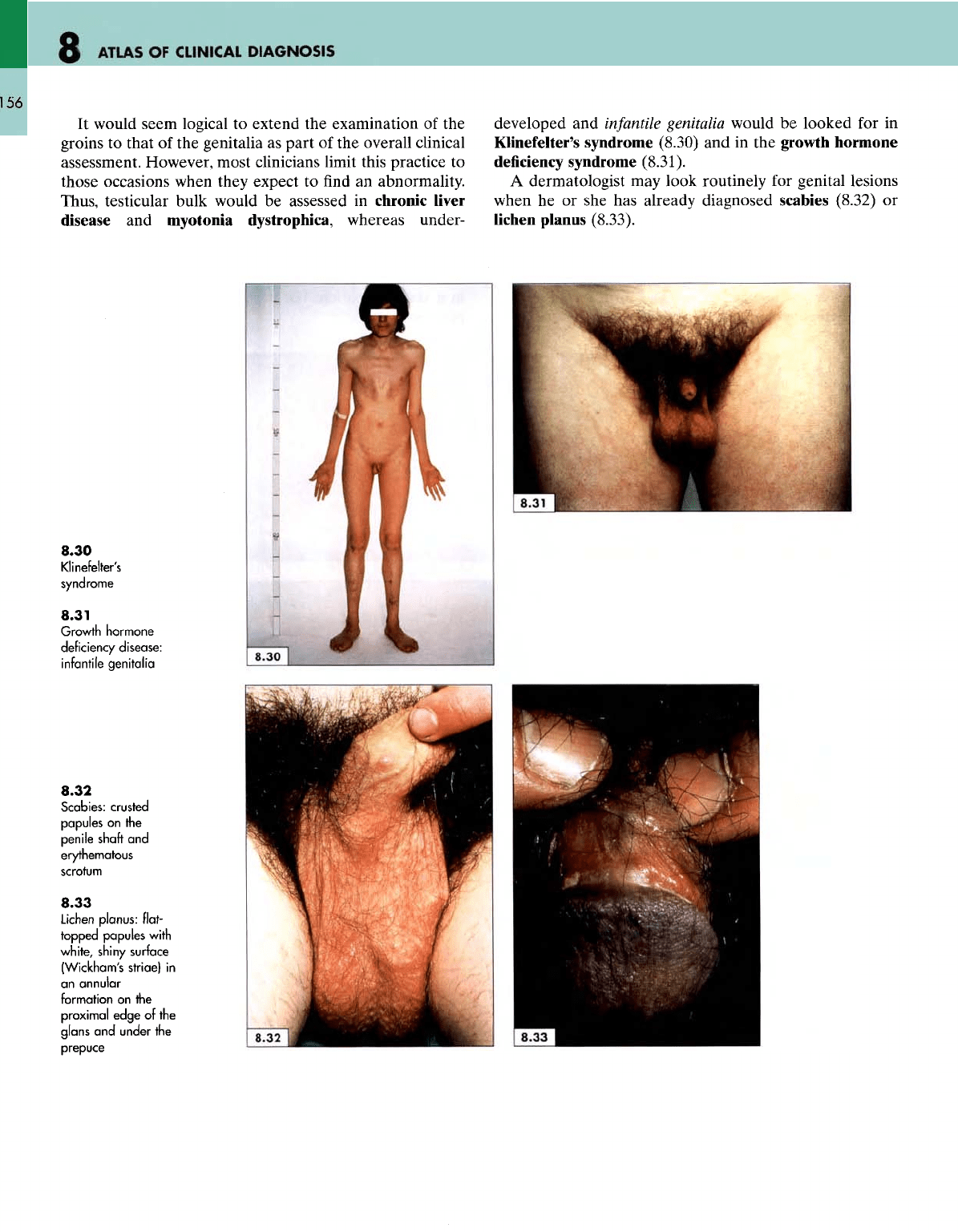
It
would seem logical
to
extend
the
examination
of the
groins
to
that
of the
genitalia
as
part
of the
overall clinical
assessment. However, most clinicians limit this practice
to
those
occasions
when they
expect
to find an
abnormality.
Thus, testicular bulk would
be
assessed
in
chronic
liver
disease
and
myotonia dystrophica, whereas under-
developed
and
infantile
genitalia would
be
looked
for in
Klinefelter's
syndrome (8.30)
and in the
growth hormone
deficiency
syndrome
(8.31).
A
dermatologist
may
look routinely
for
genital
lesions
when
he or she has
already diagnosed scabies (8.32)
or
lichen planus (8.33).
8.30
Klinefelter's
syndrome
8.31
Growth
hormone
deficiency disease:
infantile
genitalia
8.32
Scabies: crusted
papules
on the
penile
shaft
and
erythematous
scrotum
8.33
Lichen
planus:
flat-
topped
papules
with
white,
shiny surface
(Wickham's striae)
in
an
annular
formation
on the
proximal
edge
of the
glans
and
under
the
prepuce
9
THE
HANDS
157
Inspection
of the
hands
is
next only
to
that
of the
face
in
yielding
a
plethora
of
useful
clinical signs.
The
task
of
clinically
scrutinizing
the
hands
is
vast
and
needs
a
logical
approach.
The
visual survey should address
five
questions.
1. Is
there
an
arthropathy?
(e.g.
rheumatoid,
osteoarthrosis, gout, psoriasis, septic);
2.
Is
there
a
skin lesion?
(e.g.
dermatoses, systemic
disorders);
3.
Is
there
a
neuromuscular
disorder?
(e.g.
wasting,
deformity,
fasciculation);
4.
Is
there
a
sign supporting
those
found elsewhere?
(e.g.
ulcers,
erythema, cyanosis, pigmentation, acropachy,
etc.);
5.
Is
there
a
fundamental sign suggesting
a
systemic
disorder?
(e.g.
clubbing, xanthomata, erythema
nodosum, etc.).
These
questions
can be
summarized
as
looking
for
swelling,
deformity,
wasting,
skin
lesions,
and
normal
and
abnormal
movements.
A
diagnostic hypothesis
can be
syn-
thesized
from
any one or a
combination
of
these signs
as
illustrated
in the
following
five
sections.
Arthropathies
The
hands should
be
looked
at for any
signs
of
arthritis
such
as
swelling, deformity, wasting, subluxation
or
anky-
losis
of the
joints. Rheumatoid arthritis
is by far the
com-
monest
of the
arthritides
(1-5%)
afecting females
at
least
three
times more often than males,
and
with
a
peak inci-
dence between
the
fourth
and
sixth decade, although
it
may
develop
for the first
time
in
patients even
in
their
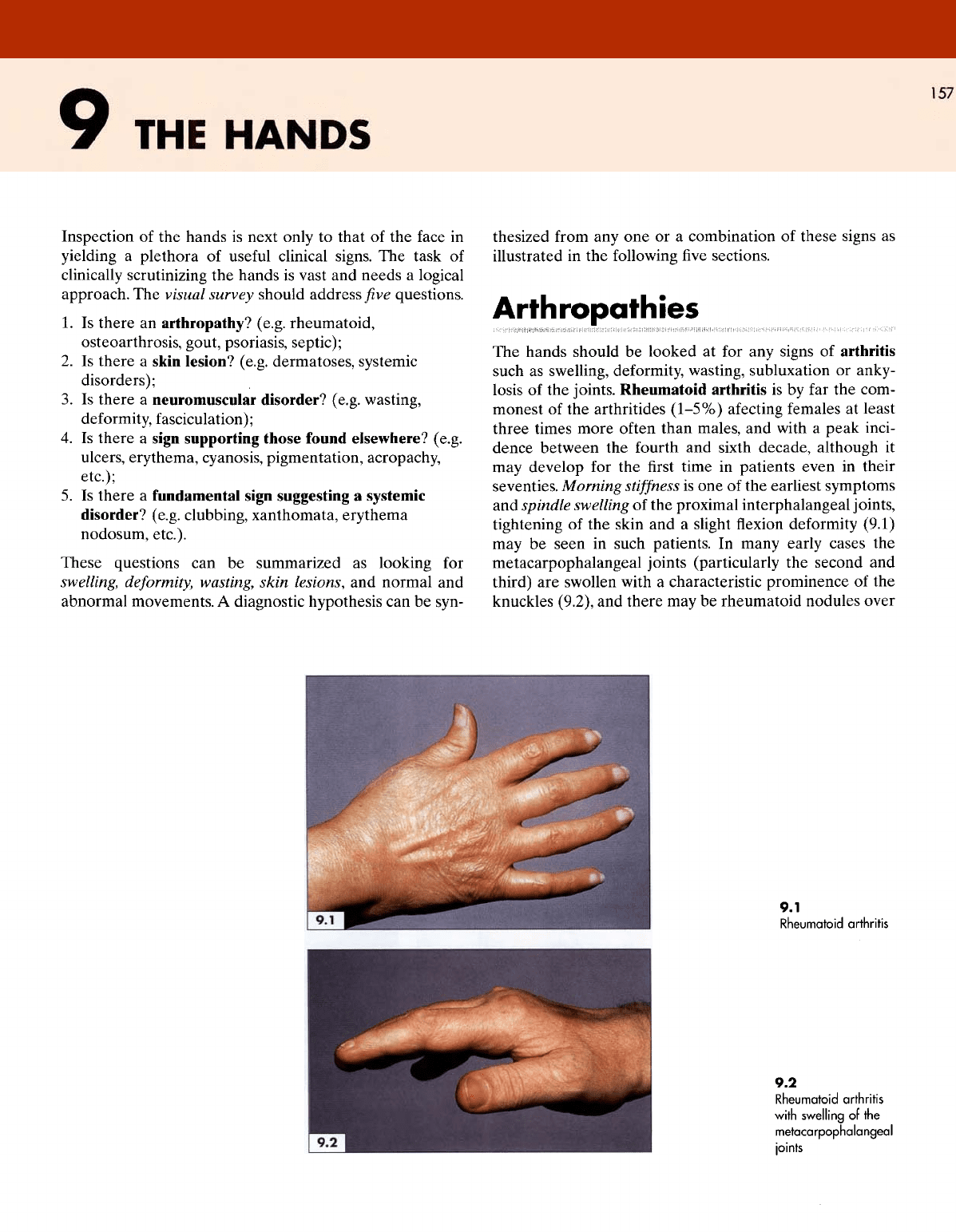
seventies. Morning
stiffness
is one of the
earliest symptoms
and
spindle swelling
of the
proximal interphalangeal joints,
tightening
of the
skin
and a
slight
flexion
deformity
(9.1)
may
be
seen
in
such patients.
In
many early cases
the
metacarpophalangeal joints (particularly
the
second
and
third)
are
swollen with
a
characteristic prominence
of the
knuckles (9.2),
and
there
may be
rheumatoid nodules over
9.1
Rheumatoid
arthritis
9.2
Rheumatoid
arthritis
with
swelling
of the
metacarpophalangeal
joints
ATLAS
OF
CLINICAL
DIAGNOSIS
158
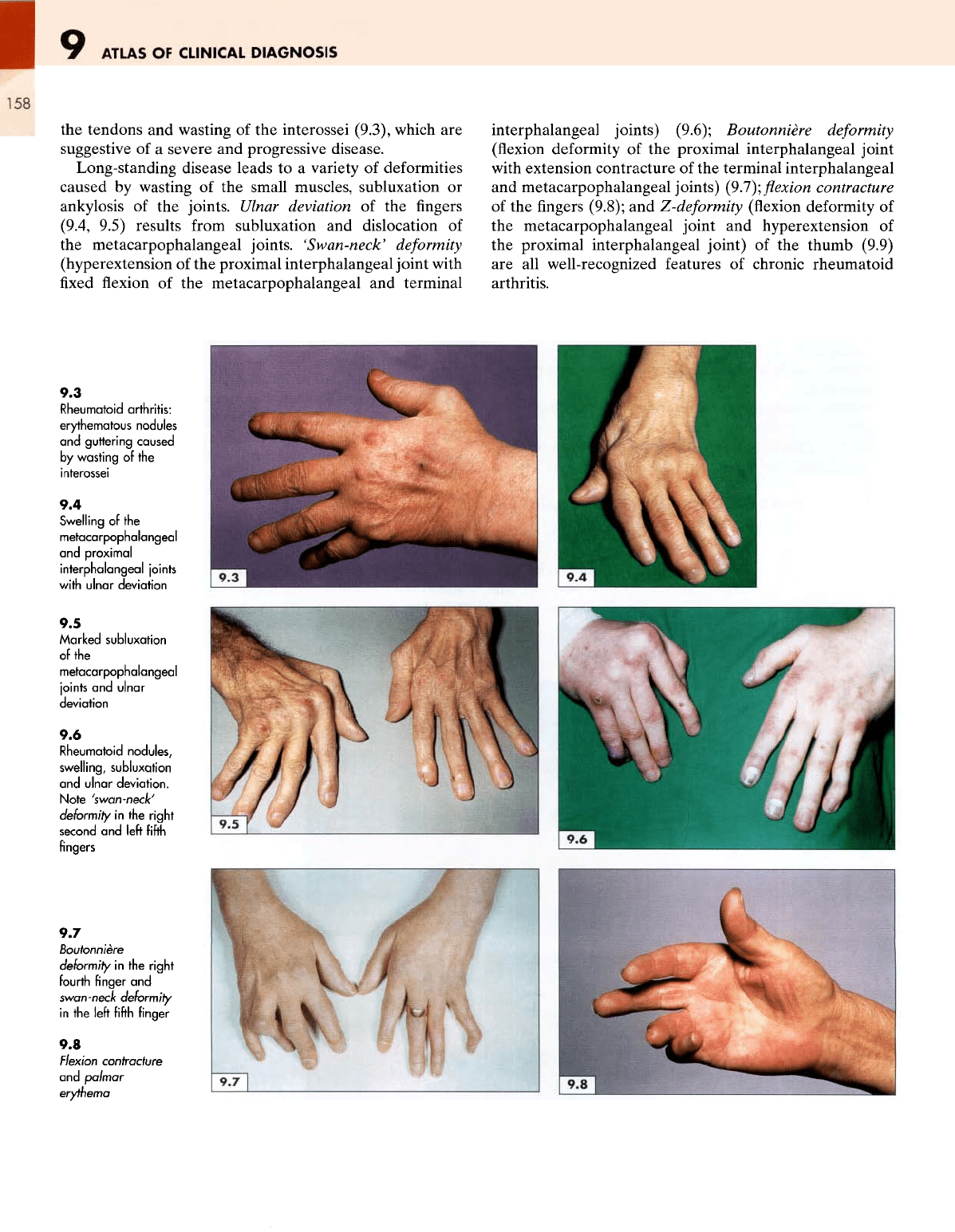
the
tendons
and
wasting
of the
interossei (9.3), which
are
suggestive
of a
severe
and
progressive disease.
Long-standing disease leads
to a
variety
of
deformities
caused
by
wasting
of the
small muscles, subluxation
or
ankylosis
of the
joints.
Ulnar
deviation
of the
fingers
(9.4,
9.5) results
from
subluxation
and
dislocation
of
the
metacarpophalangeal joints.
'Swan-neck'
deformity
(hyperextension
of the
proximal interphalangeal joint with
fixed
flexion
of the
metacarpophalangeal
and
terminal
interphalangeal joints) (9.6); Boutonniere
deformity
(flexion
deformity
of the
proximal interphalangeal joint
with
extension contracture
of the
terminal interphalangeal
and
metacarpophalangeal joints)
(9..7);
flexion
contracture
of
the
fingers
(9.8);
and
Z-deformity
(flexion
deformity
of
the
metacarpophalangeal joint
and
hyperextension
of
the
proximal interphalangeal joint)
of the
thumb (9.9)
are all
well-recognized features
of
chronic rheumatoid
arthritis.
9.3
Rheumatoid
arthritis:
erythematous
nodules
and
guttering
caused
by
wasting
of the
interossei
9.4
Swelling
of the
metacarpophalangeal
and
proximal
interphalangeal
joints
with
ulnar
deviation
9.5
Marked
subluxation
of
the
metacarpophalangeal
joints
and
ulnar
deviation
9.6
Rheumatoid
nodules,
swelling,
subluxation
and
ulnar
deviation.
Note
'swan-neck'
deformity
in
the
right
second
and
left fifth
fingers
9.7
Boutonniere
deformity
in the
right
fourth
finger
and
swan-neck
deformity
in
the
left fifth
finger
9.8
Flexion
contracture
and
palmar
erythema
THE
HANDS
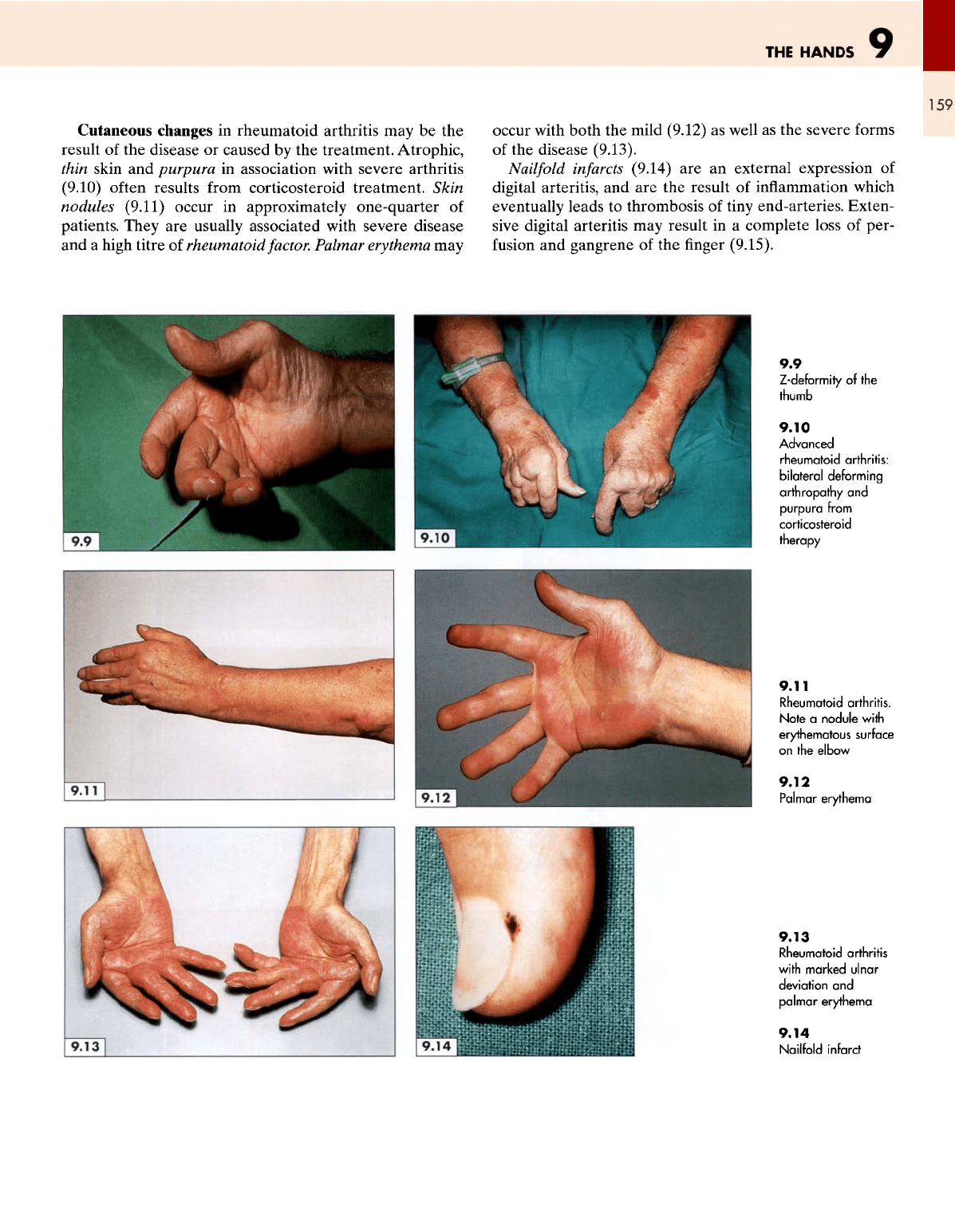
Cutaneous
changes
in
rheumatoid arthritis
may be the
result
of the
disease
or
caused
by the
treatment. Atrophic,
thin
skin
and
purpura
in
association with severe arthritis
(9.10)
often
results
from
corticosteroid treatment.
Skin
nodules
(9.11)
occur
in
approximately one-quarter
of
patients. They
are
usually associated with severe disease
and a
high titre
of
rheumatoid
factor.
Palmar erythema
may
occur with both
the
mild (9.12)
as
well
as the
severe
forms
of
the
disease (9.13).
Nailfold
infarcts
(9.14)
are an
external expression
of
digital
arteritis,
and are the
result
of
inflammation
which
eventually
leads
to
thrombosis
of
tiny
end-arteries. Exten-
sive
digital arteritis
may
result
in a
complete loss
of
per-
fusion
and
gangrene
of the
finger
(9.15).
9.9
Z-deformity
of
the
thumb
9.10
Advanced
rheumatoid
arthritis:
bilateral
deforming
arthropathy
and
purpura
from
corticosteroid
therapy
9.11
Rheumatoid arthritis.
Note
a
nodule
with
erythematous
surface
on
the
elbow
9.12
Palmar
erythema
9.13
Rheumatoid arthritis
with
marked
ulnar
deviation
and
palmar
erythema
9.14
Nailfold
infarct
ATLAS
OF
CLINICAL
DIAGNOSIS
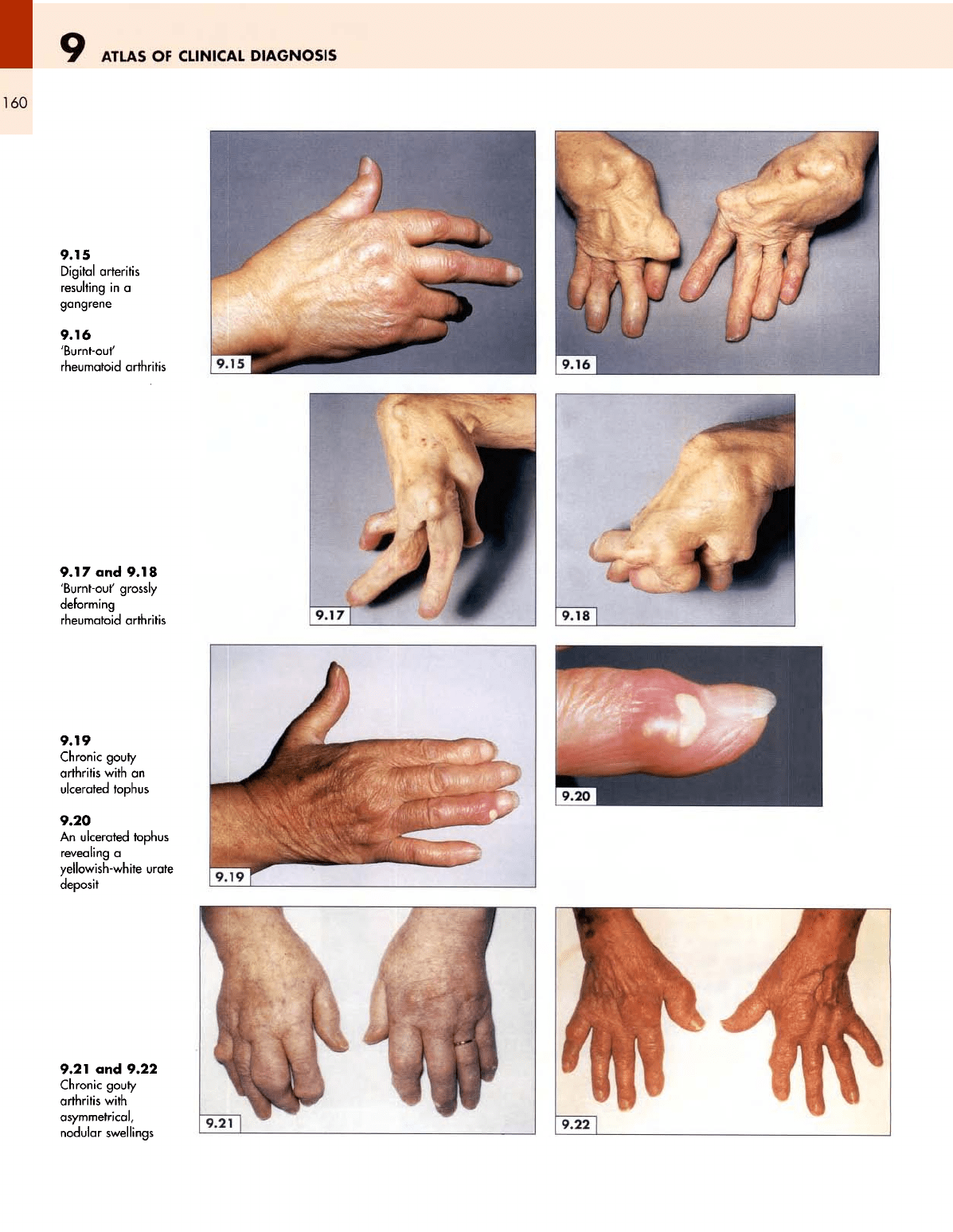
160
9.15
Digital
arteritis
resulting
in a
gangrene
9.16
'Burnt-out'
rheumatoid arthritis
9.17
and
9.18
'Burnt-out'
grossly
deforming
rheumatoid arthritis
9.19
Chronic gouty
arthritis with
an
ulcerated
tophus
9.20
An
ulcerated tophus
revealing
a
yellowish-white urate
deposit
9.21
and
9.22
Chronic gouty
arthritis with
asymmetrical,
nodular
swellings
THE
HANDS
161
Unlike
in a
neuromuscular
disorder, many patients with
rheumatoid arthritis, even with gross muscular wasting,
retain
a
reasonable degree
of
power
and
function
in the
hands. Nevertheless, end-stage
or
'burnt-out'
arthritis
severely distorts
the
hands
(9.16,9.17),
and
sometimes only
short
and
disfigured
stumps
of
fingers
(9.18)
remain, with
very
little
useful function.
Chronic gouty
arthritis
(9.19) sometimes resembles
rheumatoid arthritis
at first
sight
but it may be
betrayed
by
the
presence
of
tophaceous
urate
deposits,
which
may
produce
a
yellowish-white, hard swelling
on one or
more
of
the fingers
(9.20).
As a
result
of
these tophaceous
deposits,
the
joint deformities
in
gout, unlike
those
in
rheumatoid arthritis,
are
neither predictable
nor
sym-
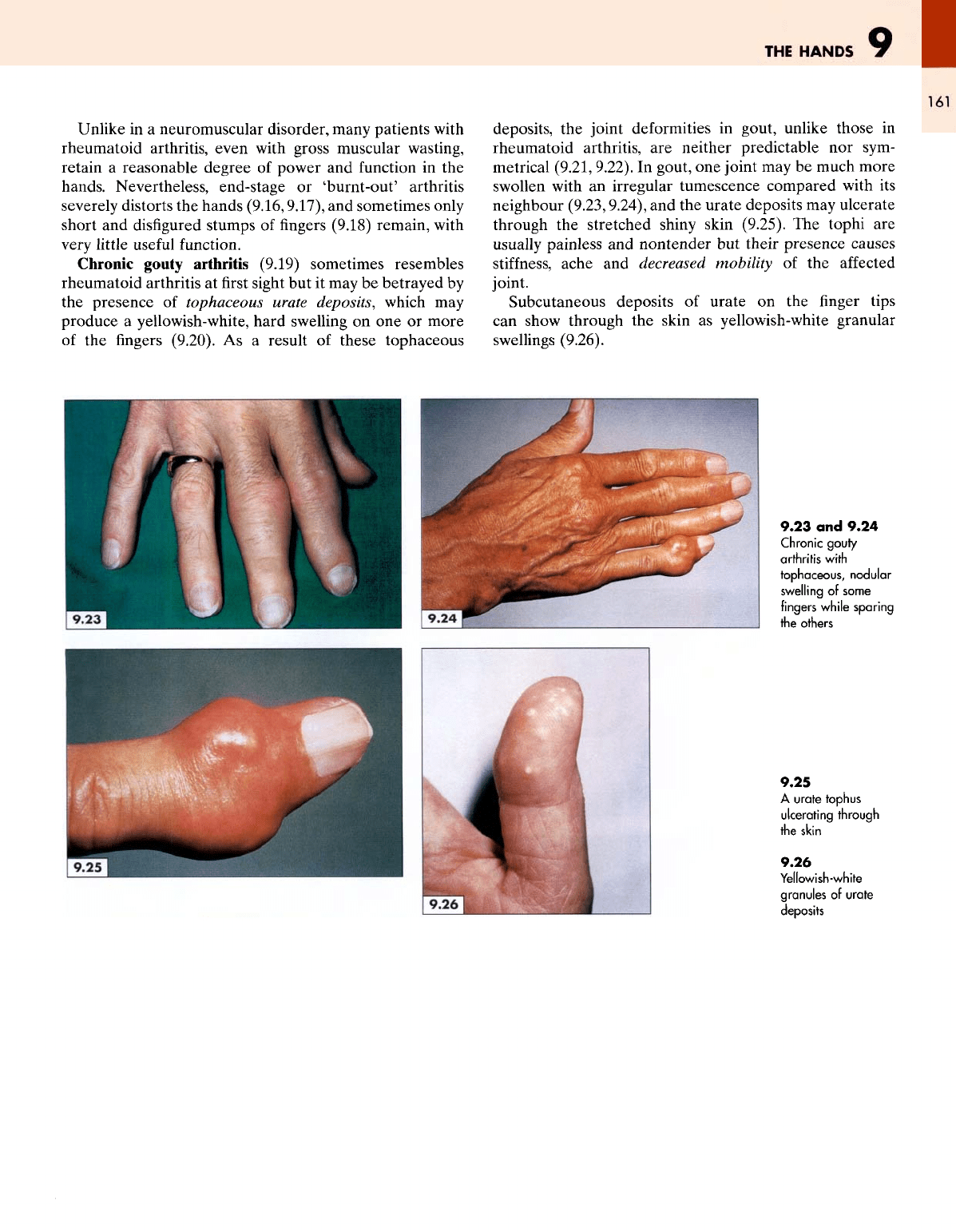
metrical (9.21, 9.22).
In
gout,
one
joint
may be
much more
swollen
with
an
irregular tumescence compared with
its
neighbour
(9.23,9.24),
and the
urate deposits
may
ulcerate
through
the
stretched shiny skin (9.25).
The
tophi
are
usually
painless
and
nontender
but
their
presence
causes
stiffness,
ache
and
decreased mobility
of the
affected
joint.
Subcutaneous deposits
of
urate
on the finger
tips
can
show through
the
skin
as
yellowish-white granular
swellings
(9.26).
9.23
and
9.24
Chronic
gouty
arthritis
with
tophaceous,
nodular
swelling
of
some
fingers
while
sparing
the
others
9.25
A
urate tophus
ulcerating
through
the
skin
9.26
Yellowish-white
granules
of
urate
deposits