Мир М.Афзал Атлас клинического диагноза
Подождите немного. Документ загружается.

ATLAS
OF
CLINICAL
DIAGNOSIS
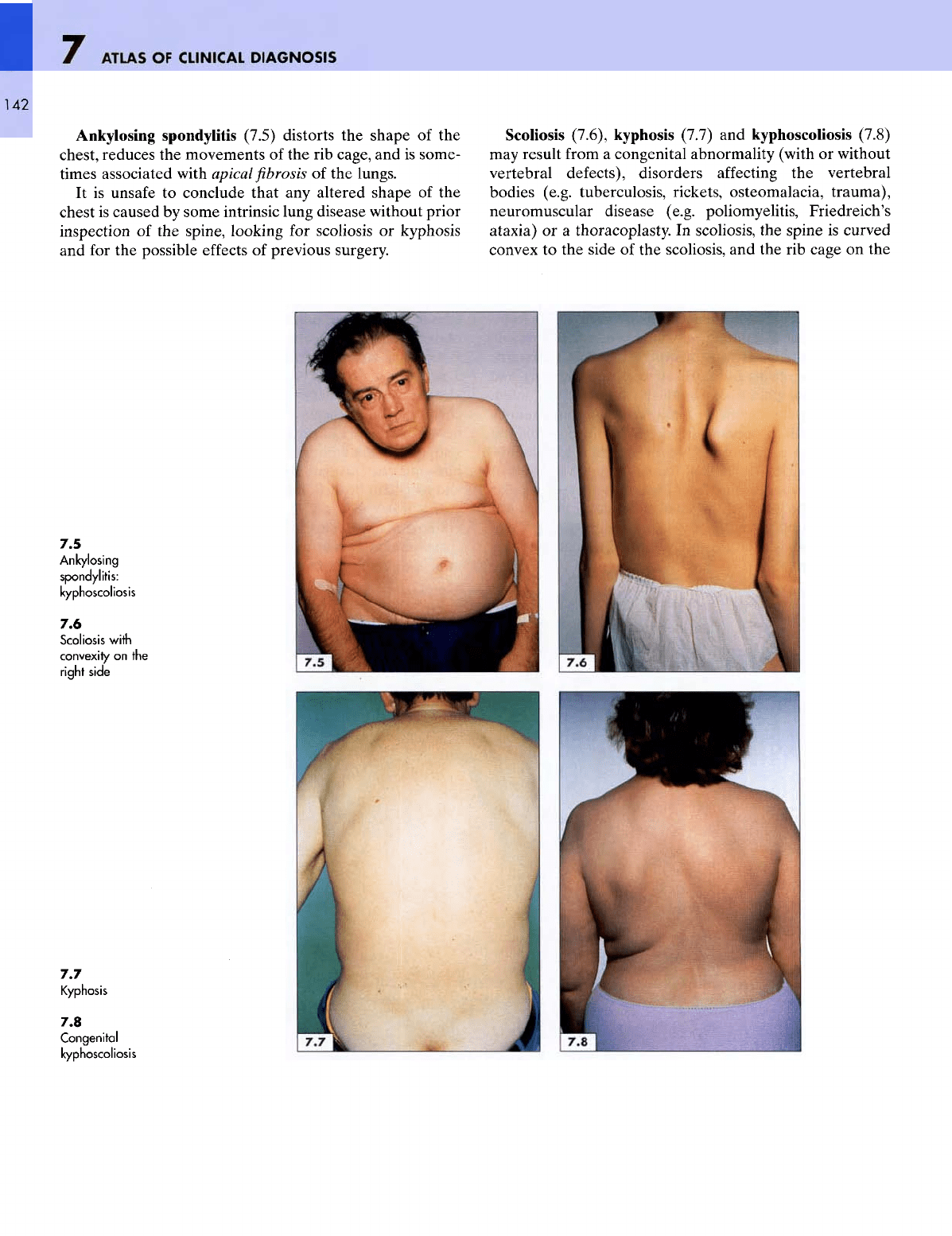
Ankylosing spondylitis (7.5) distorts
the
shape
of the
chest, reduces
the
movements
of the rib
cage,
and is
some-
times associated with
apical
fibrosis of the
lungs.
It is
unsafe
to
conclude that
any
altered shape
of the
chest
is
caused
by
some intrinsic lung disease without prior
inspection
of the
spine, looking
for
scoliosis
or
kyphosis
and for the
possible
effects
of
previous surgery.
Scoliosis (7.6), kyphosis (7.7)
and
kyphoscoliosis (7.8)
may
result
from
a
congenital abnormality (with
or
without
vertebral defects), disorders
affecting
the
vertebral
bodies (e.g. tuberculosis, rickets, osteomalacia, trauma),
neuromuscular disease (e.g. poliomyelitis, Friedreich's
ataxia)
or a
thoracoplasty.
In
scoliosis,
the
spine
is
curved
convex
to the
side
of the
scoliosis,
and the rib
cage
on the
7.5
Ankylosing
spondylitis:
kyphoscoliosis
7.6
Scoliosis
with
convexity
on the
right
side
7.7
Kyphosis
7.8
Congenital
kyphoscoliosis
THE
CHEST
7
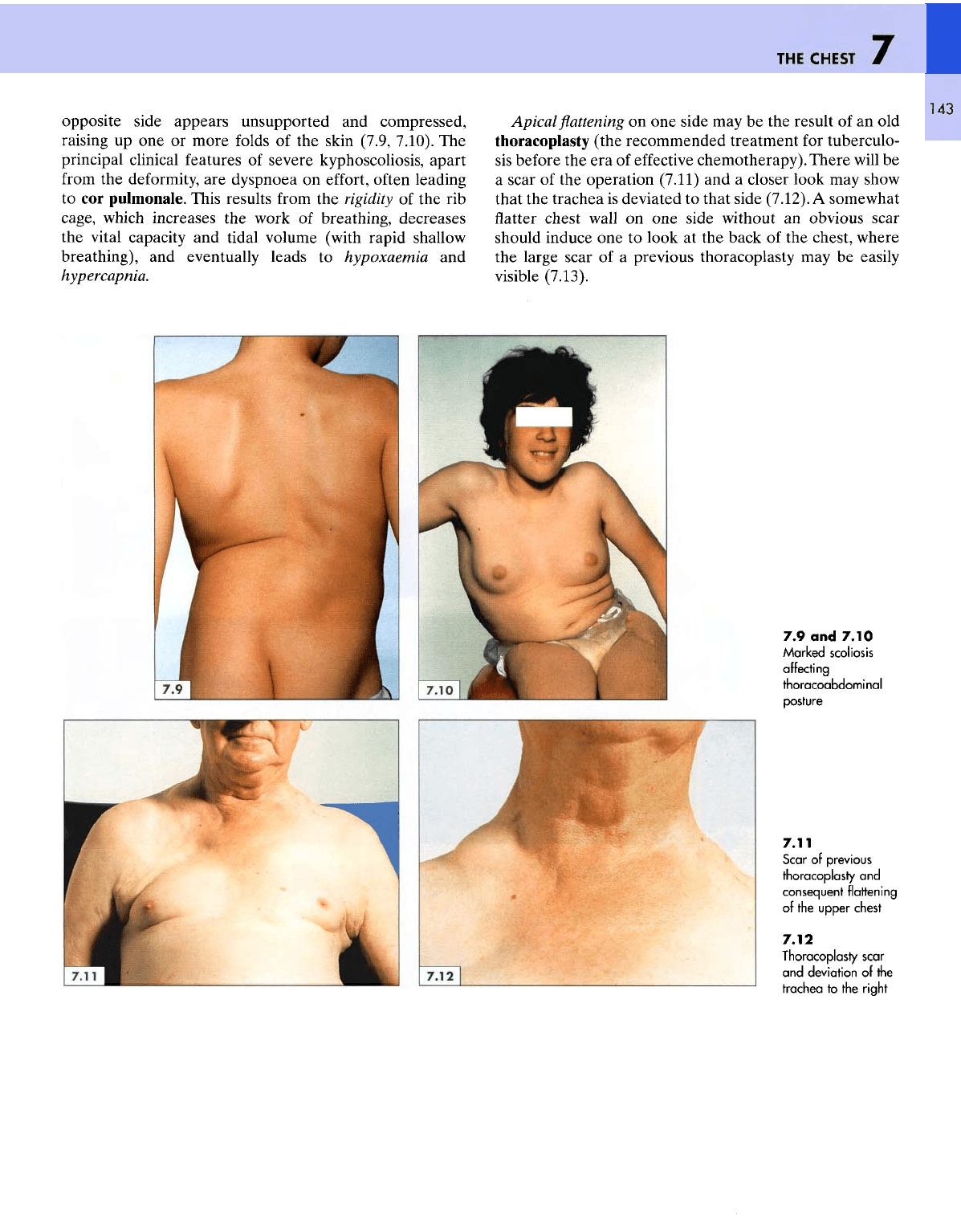
opposite side appears unsupported
and
compressed,
raising
up one or
more
folds
of the
skin (7.9, 7.10).
The
principal clinical features
of
severe kyphoscoliosis, apart
from
the
deformity,
are
dyspnoea
on
effort,
often
leading
to cor
pulmonale. This results
from
the
rigidity
of the rib
cage, which increases
the
work
of
breathing,
decreases
the
vital capacity
and
tidal volume (with rapid shallow
breathing),
and
eventually leads
to
hypoxaemia
and
hypercapnia.
Apical
flattening on one
side
may be the
result
of an old
thoracoplasty
(the recommended treatment
for
tuberculo-
sis
before
the era of
effective
chemotherapy).
There
will
be
a
scar
of the
operation
(7.11)
and a
closer look
may
show
that
the
trachea
is
deviated
to
that side (7.12).
A
somewhat
flatter
chest
wall
on one
side without
an
obvious scar
should induce
one to
look
at the
back
of the
chest, where
the
large scar
of a
previous thoracoplasty
may be
easily
visible
(7.13).
7.9 and
7.10
Marked
scoliosis
affecting
thoracoabdom
i
nal
posture
7.11
Scar
of
previous
thoracoplasty
and
consequent flattening
of the
upper
chest
7.12
Thoracoplasty scar
and
deviation
of the
trachea
to
the
right
ATLAS
OF
CLINICAL
DIAGNOSIS
144
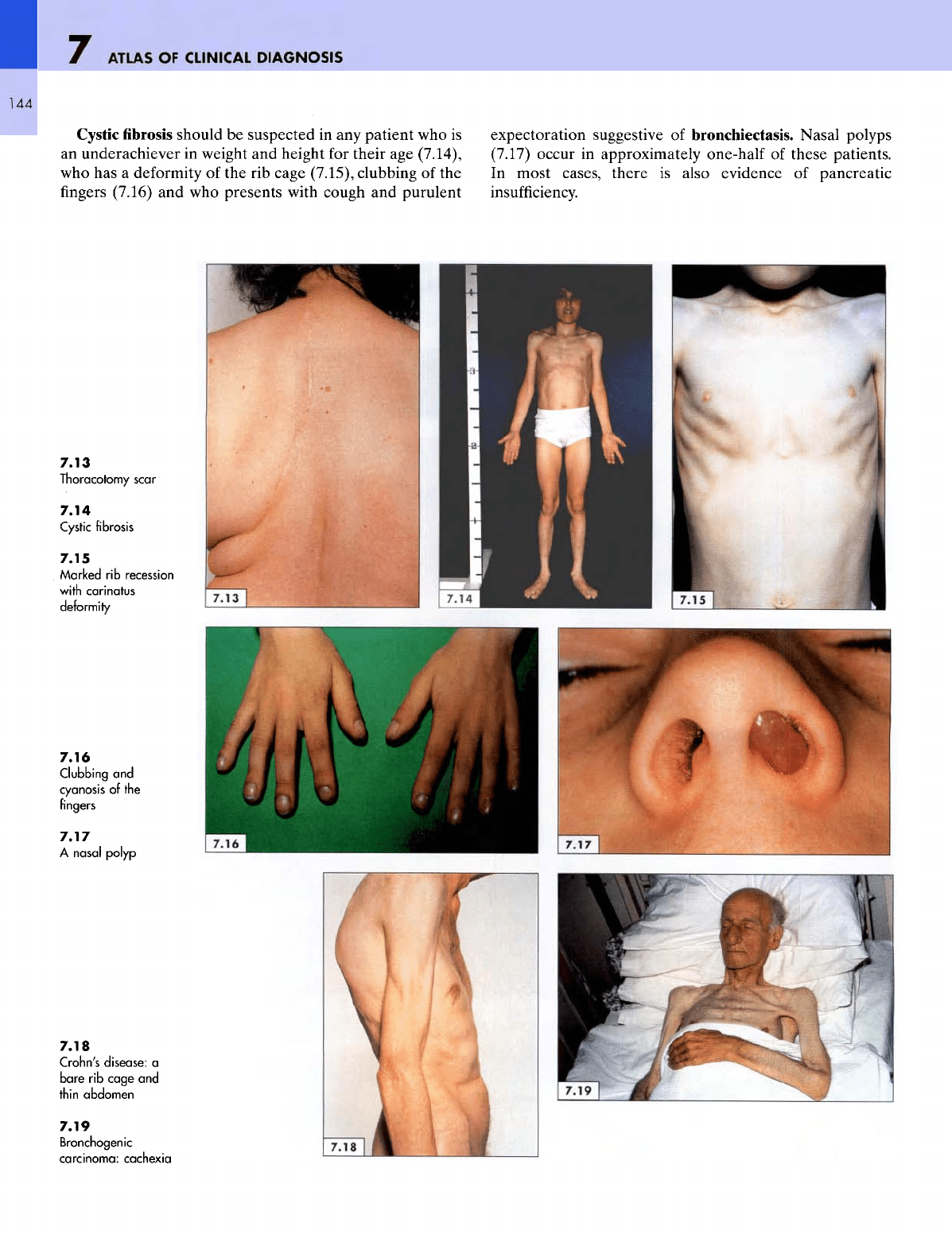
Cystic
fibrosis
should
be
suspected
in any
patient
who is
an
underachiever
in
weight
and
height
for
their
age
(7.14),
who
has a
deformity
of the rib
cage (7.15), clubbing
of the
fingers
(7.16)
and who
presents with cough
and
purulent
expectoration suggestive
of
bronchiectasis. Nasal polyps
(7.17)
occur
in
approximately one-half
of
these patients.
In
most cases,
there
is
also evidence
of
pancreatic
insufficiency.
7.13
Thoracotomy
scar
7.14
Cystic
fibrosis
7.15
Marked
rib
recession
with
carinatus
deformity
7.16
Clubbing
and
cyanosis
of the
fingers
7.17
A
nasal
polyp
7.18
Crohn's
disease:
a
bare
rib
cage
and
thin
abdomen
7.19
Bronchogenic
carcinoma:
cachexia
THE
CHEST
The
overall nutritional status
of a
patient
can be
assessed
by
looking
at the
chest.
In
wasting disorders,
the
loss
of
muscle bulk
and
subcutaneous
fat
makes
the
nor-
mally
rounded
rib
cage look square,
as in
this patient with
Crohn's disease
(7.18).The
ribs become prominent
and the
rib
spaces show marked guttering,
as
seen
in
this
man
with
a
carcinoma
of the
lung (7.19).
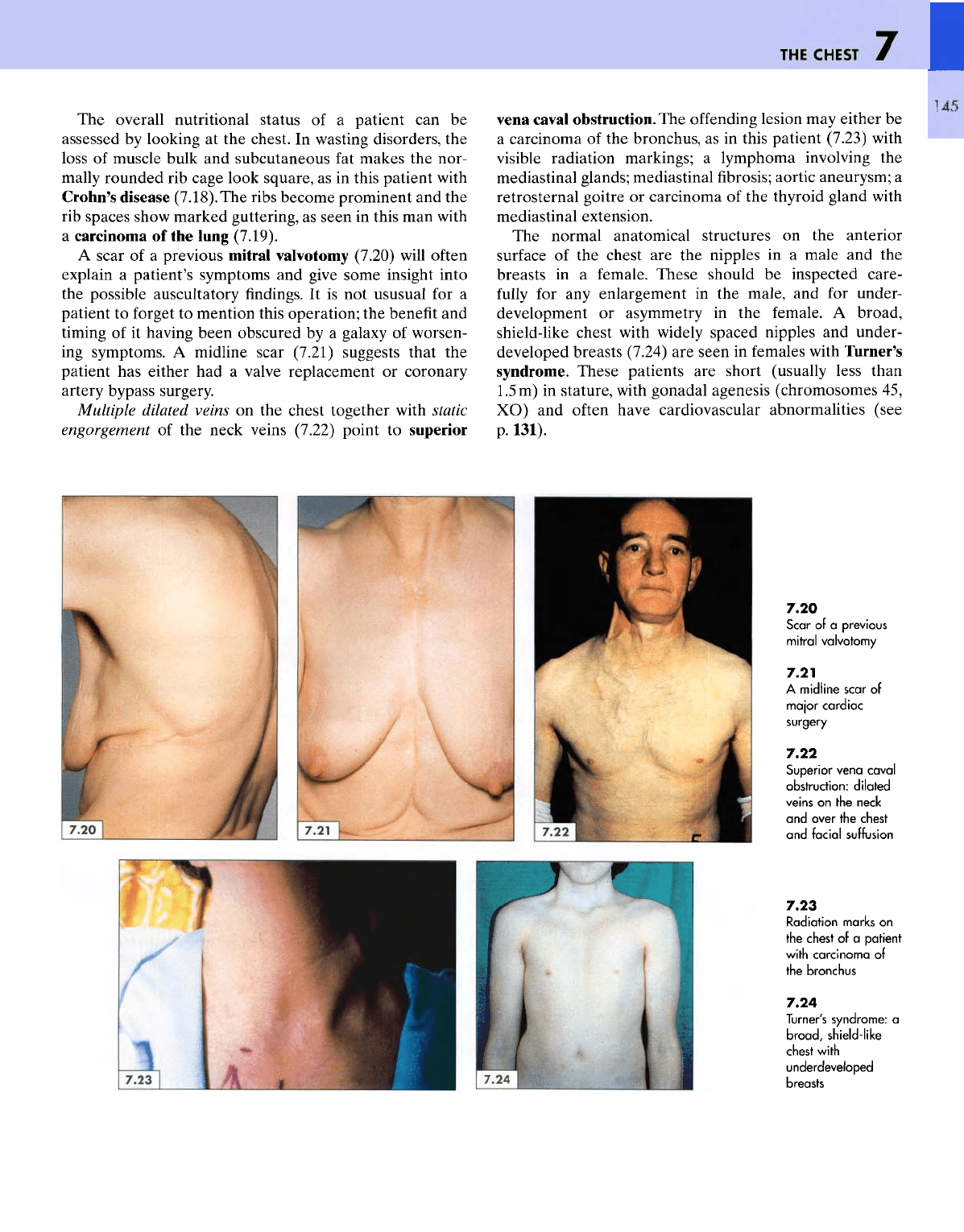
A
scar
of a
previous
mitral
valvotomy (7.20)
will
often
explain
a
patient's symptoms
and
give
some
insight into
the
possible auscultatory
findings.
It is not
ususual
for a
patient
to
forget
to
mention this operation;
the
benefit
and
timing
of it
having been obscured
by a
galaxy
of
worsen-
ing
symptoms.
A
midline scar (7.21) suggests that
the
patient
has
either
had a
valve replacement
or
coronary
artery
bypass surgery.
Multiple
dilated veins
on the
chest together with static
engorgement
of the
neck veins (7.22) point
to
superior
vena
caval
obstruction.
The
offending
lesion
may
either
be
a
carcinoma
of the
bronchus,
as in
this patient (7.23) with
visible
radiation markings;
a
lymphoma involving
the
mediastinal
glands; mediastinal
fibrosis;
aortic aneurysm;
a
retrosternal goitre
or
carcinoma
of the
thyroid gland with
mediastinal extension.
The
normal anatomical structures
on the
anterior
surface
of the
chest
are the
nipples
in a
male
and the
breasts
in a
female.
These
should
be
inspected care-
fully
for any
enlargement
in the
male,
and for
under-
development
or
asymmetry
in the
female.
A
broad,
shield-like
chest
with
widely spaced nipples
and
under-
developed breasts (7.24)
are
seen
in
females with Turner's
syndrome.
These
patients
are
short (usually less than
1.5m)
in
stature, with gonadal agenesis (chromosomes
45,
XO) and
often
have cardiovascular abnormalities (see
p.
131).
7.20
Scar
of a
previous
mitral
valvotomy
7.21
A
midline
scar
of
major
cardiac
surgery
7.22
Superior
vena
caval
obstruction:
dilated
veins
on
the
neck
and
over
the
chest
and
facial
suffusion
7.23
Radiation
marks
on
the
chest
of a
patient
with
carcinoma
of
the
bronchus
7.24
Turner's
syndrome:
a
broad,
shield-like
chest
with
underdeveloped
breasts

ATLAS
OF
CLINICAL
DIAGNOSIS
146
Gynaecomastia
associations:
(7.25,
7.26)
has
many causes
and
•
Age-related (e.g. puberty, senile
-
rise
in
oestrogens
and
fall
in
androgens);
•
Endocrine (e.g. thyrotoxicosis, hypothyroidism,
pituitary
disease,
Addison's
disease, testicular tumours,
adrenal carcinoma, isolated gonadotrophin deficiency);
•
Chromosomal (e.g. Klinefelter's syndrome
-
47,
XXY);
•
Metabolic (e.g. hepatic failure);
•
Neoplastic (e.g. carcinoma
of the
lung);
•
Drug-induced (e.g. oestrogen therapy, aldactone,
digoxin,
alkylating agents, griseofulvin, methyldopa,
phenothiazines, tricyclics, anabolic
and
adrenocortical
steroids, isoniazid,
etc.).
Approximately
5% of
patients with carcinoma
of the
lung
develop gynaecomastia, sometimes associated with
hypertrophic pulmonary osteoarthropathy.
The
presence
of
gynaecomastia must
not be
accepted
on
inspection
alone, particularly
in an
obese
subject.
The
swelling must
be
palpated
for the
presence
of
glandular
tissue,
thereby
distinguishing
it
from
adipose tissue.
Puckering
and
indrawing
of a
part
of the
breast (7.27),
with
or
without apparent induration,
is a
serious sign
and
suggests
the
presence
of a
neoplasm.
Almost
all of the
skin disorders
can
involve
the
chest,
although
in
some cases
the
lesions
are
missed because
of
inadequate undressing before clinical examination
of the
patient.
Telangiectasia
are by far the
most important
of the
cutaneous lesions
to
look for, since these
are
seldom
found
below
the
transnipple line. Sometimes they occur
in
crops
on the
upper chest,
as in
this patient with
the
Budd-Chiari
syndrome
(7.28).
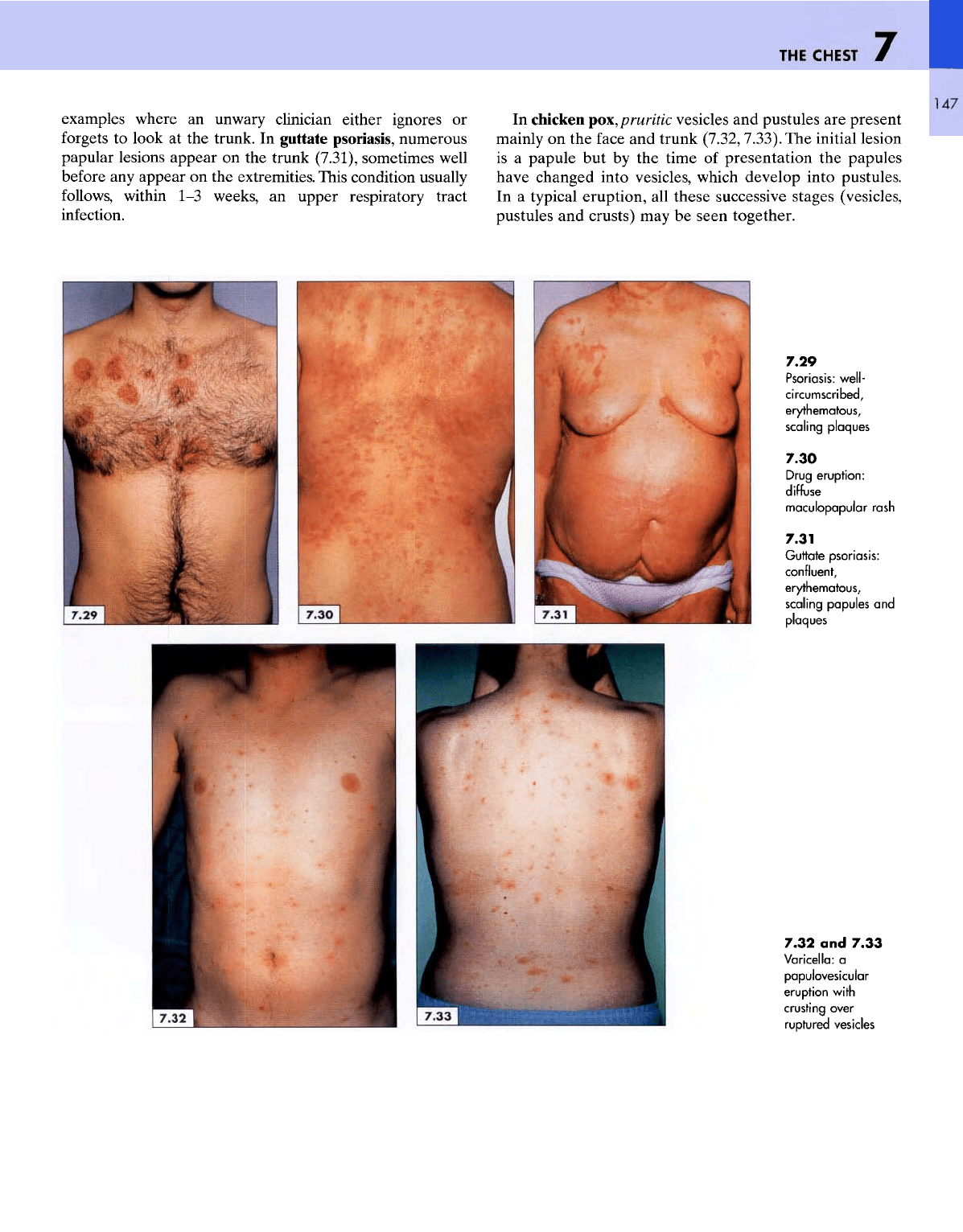
Psoriasis
(7.29)
and
drug eruptions (7.30)
are two
good
7.25
Gynaecomastia
7.26
Gynaecomastia
with
prominent
breasts
and
unassociated
with
confounding
obesity
7.27
Malignancy:
puckering
and
indrawing
of the
left
breast
7.28
Diffuse
telangiectasis
THE
CHEST
147
examples where
an
unwary clinician either ignores
or
forgets
to
look
at the
trunk.
In
guttate psoriasis, numerous
papular lesions appear
on the
trunk (7.31), sometimes
well
before
any
appear
on the
extremities. This condition usually
follows,
within
1-3
weeks,
an
upper respiratory tract
infection.
In
chicken
pox,
pruritic
vesicles
and
pustules
are
present
mainly
on the
face
and
trunk
(7.32,7.33).
The
initial lesion
is
a
papule
but by the
time
of
presentation
the
papules
have
changed into vesicles, which develop into pustules.
In a
typical eruption,
all
these successive stages (vesicles,
pustules
and
crusts)
may be
seen together.
7.29
Psoriasis:
well-
circumscribed,
erythematous,
scaling plaques
7.30
Drug
eruption:
diffuse
maculopapular
rash
7.31
Guttate
psoriasis:
confluent,
erythematous,
scaling papules
and
plaques
7.32
and
7.33
Varicella:
a
papulovesicular
eruption
with
crusting
over
ruptured
vesicles
ATLAS
OF
CLINICAL
DIAGNOSIS
148
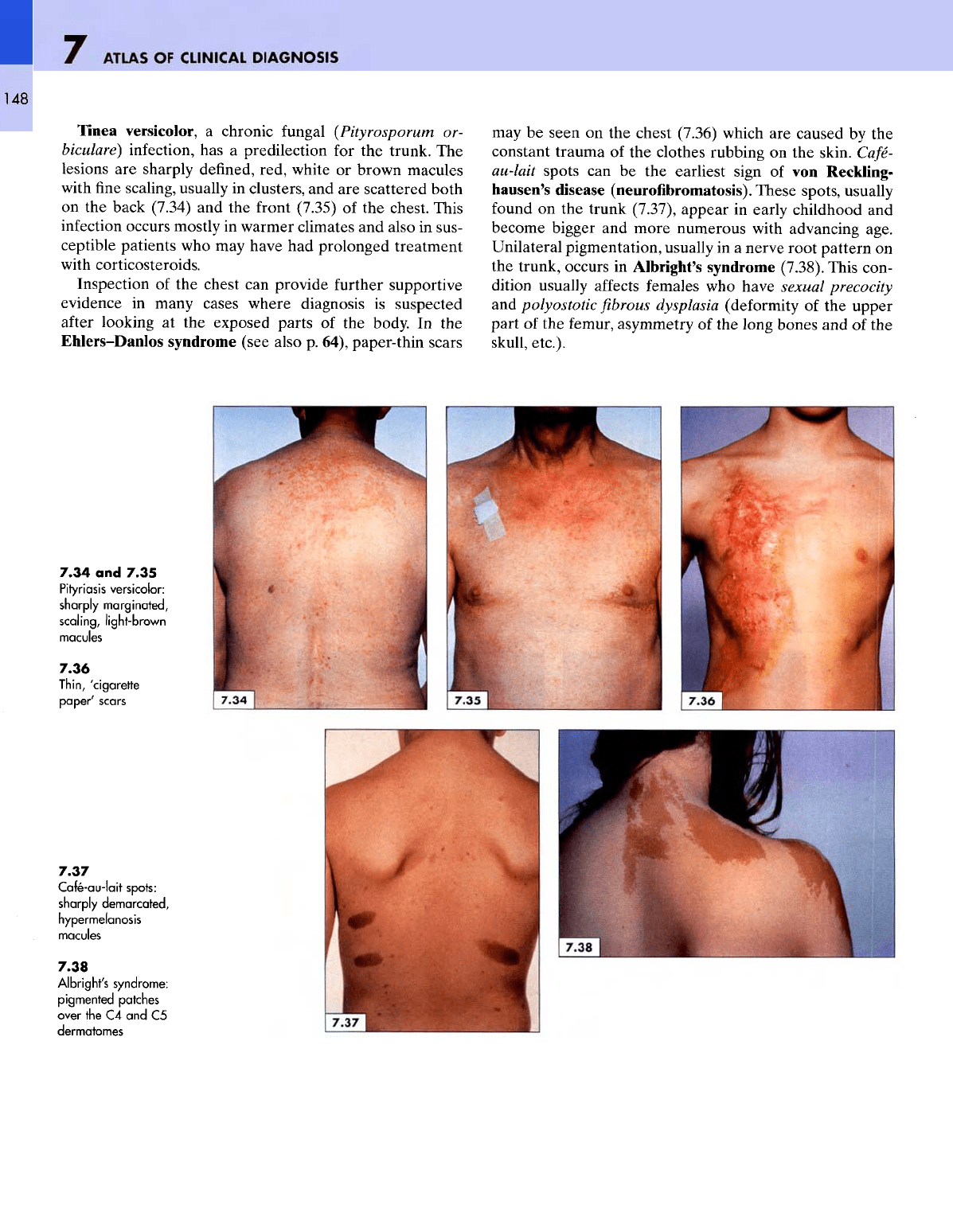
Tinea versicolor,
a
chronic
fungal
(Pityrosporum
or-
biculare)
infection,
has a
predilection
for the
trunk.
The
lesions
are
sharply defined, red, white
or
brown macules
with
fine
scaling, usually
in
clusters,
and are
scattered both
on the
back (7.34)
and the
front (7.35)
of the
chest. This
infection
occurs mostly
in
warmer climates
and
also
in
sus-
ceptible patients
who may
have
had
prolonged treatment
with
corticosteroids.
Inspection
of the
chest
can
provide
further supportive
evidence
in
many cases where diagnosis
is
suspected
after
looking
at the
exposed
parts
of the
body.
In the
Ehlers-Danlos syndrome (see also
p.
64), paper-thin scars
may
be
seen
on the
chest (7.36) which
are
caused
by the
constant trauma
of the
clothes rubbing
on the
skin.
Cafe-
au-lait
spots
can be the
earliest sign
of von
Reckling-
hausen's disease
(neurofibromatosis).
These
spots, usually
found
on the
trunk (7.37), appear
in
early childhood
and
become bigger
and
more numerous with advancing age.
Unilateral pigmentation, usually
in a
nerve
root
pattern
on
the
trunk, occurs
in
Albright's syndrome (7.38). This con-
dition usually affects females
who
have sexual precocity
and
polyostotic
fibrous
dysplasia
(deformity
of the
upper
part
of the
femur, asymmetry
of the
long
bones
and of the
skull,
etc.).
7.34
and
7.35
Pityriasis
versicolor:
sharply
marginoted,
scaling,
light-brown
macules
7.36
Thin,
'cigarette
paper'
scars
7.37
Cafe-au-lait
spots:
sharply
demarcated,
hypermelanosis
macules
7.38
Albright's
syndrome:
pigmented
patches
over
the C4 and C5
dermatomes
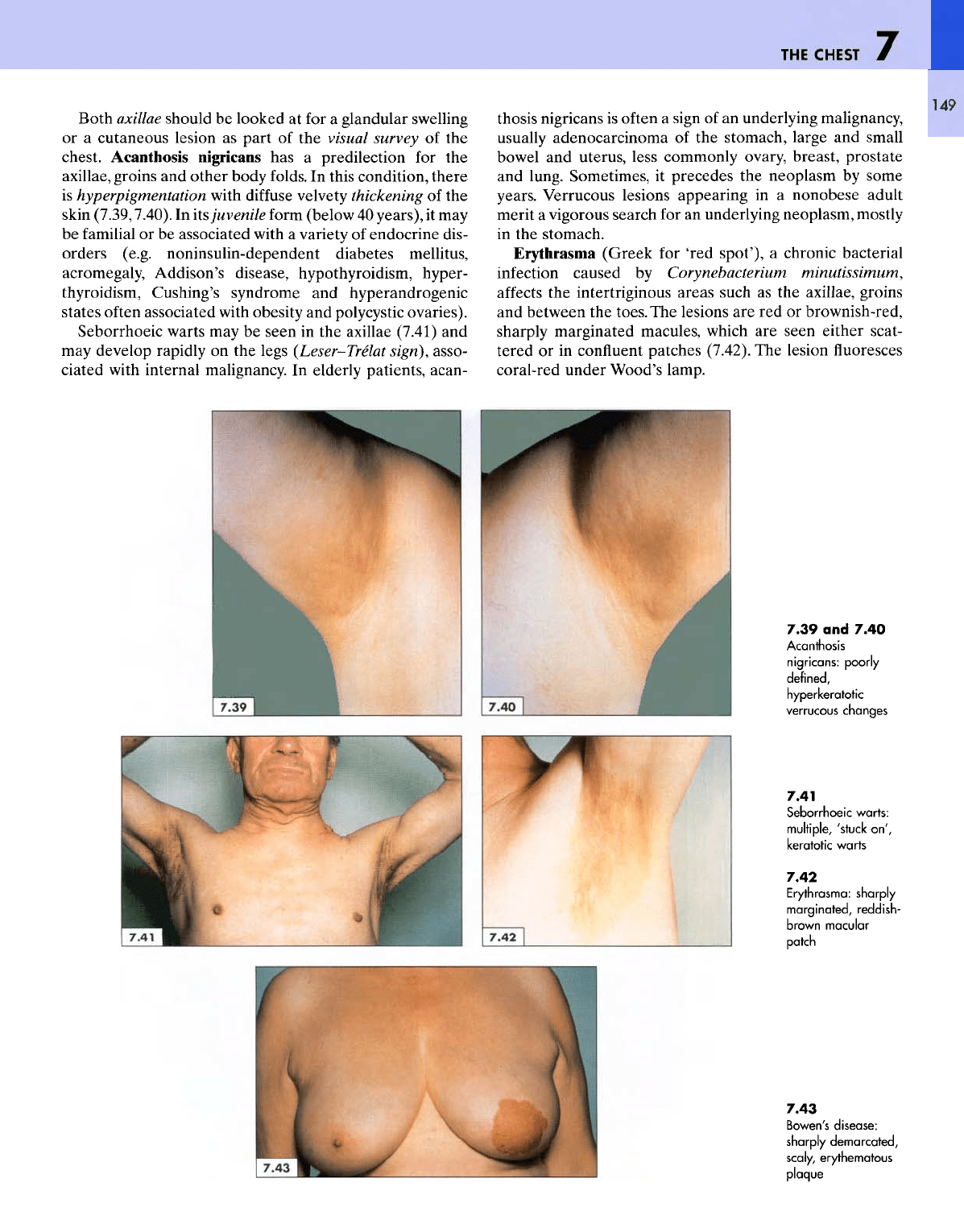
Both axillae should
be
looked
at for a
glandular swelling
or a
cutaneous lesion
as
part
of the
visual survey
of the
chest. Acanthosis nigricans
has a
predilection
for the
axillae,
groins
and
other body folds.
In
this condition, there
is
hyperpigmentation with
diffuse
velvety thickening
of the
skin
(7.39,7.40).
In
its
juvenile form (below
40
years),
it may
be
familial
or be
associated with
a
variety
of
endocrine dis-
orders (e.g. noninsulin-dependent diabetes mellitus,
acromegaly,
Addison's disease, hypothyroidism, hyper-
thyroidism,
Cushing's
syndrome
and
hyperandrogenic
states
often
associated with obesity
and
polycystic ovaries).
Seborrhoeic warts
may be
seen
in the
axillae (7.41)
and
may
develop rapidly
on the
legs
(Leser-Trelat
sign),
asso-
ciated with internal malignancy.
In
elderly patients, acan-
thosis nigricans
is
often
a
sign
of an
underlying malignancy,
usually
adenocarcinoma
of the
stomach, large
and
small
bowel
and
uterus, less commonly ovary, breast, prostate
and
lung. Sometimes,
it
precedes
the
neoplasm
by
some
years. Verrucous lesions appearing
in a
nonobese adult
merit
a
vigorous search
for an
underlying neoplasm, mostly
in
the
stomach.
Erythrasma
(Greek
for
'red
spot'),
a
chronic bacterial
infection
caused
by
Corynebacterium
minutissimum,
affects
the
intertriginous
areas
such
as the
axillae, groins
and
between
the
toes.
The
lesions
are red or
brownish-red,
sharply
marginated macules, which
are
seen either scat-
tered
or in
confluent
patches (7.42).
The
lesion
fluoresces
coral-red under Wood's lamp.
149
7.39
and
7.40
Acanthosis
nigricans:
poorly
defined,
hyperkeratotic
verrucous
changes
7.41
Seborrhoeic
warts:
multiple,
'stuck
on',
keratotic warts
7.42
Erythrasma: sharply
marginated,
reddish-
brown
macular
patch
7.43
Bowen's disease:
sharply
demarcated,
scaly,
erythematous
plaque
ATLAS
OF
CLINICAL
DIAGNOSIS
150
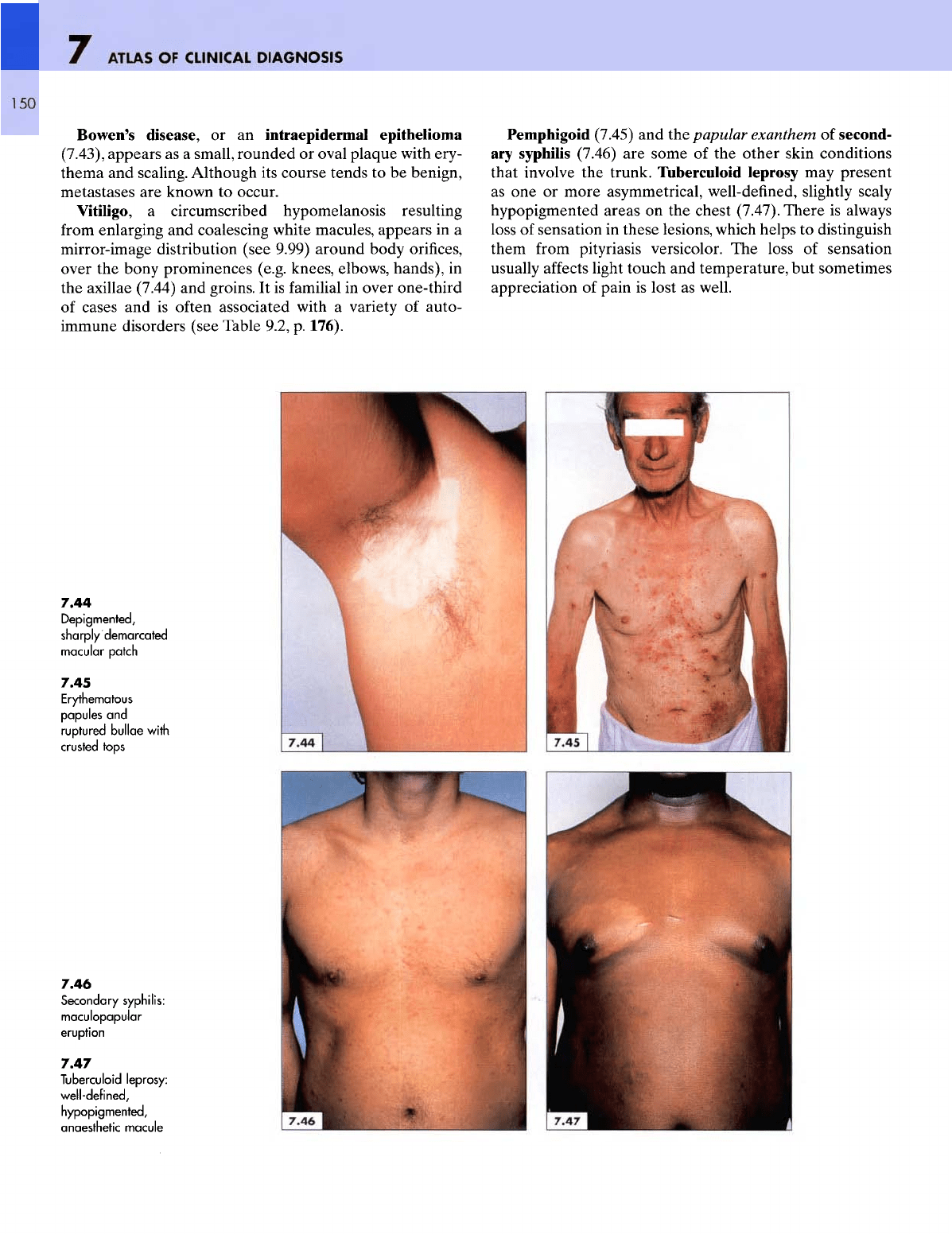
Bowen's
disease,
or an
intraepidermal epithelioma
(7.43),
appears
as a
small, rounded
or
oval plaque with ery-
thema
and
scaling. Although
its
course tends
to be
benign,
metastases
are
known
to
occur.
Vitiligo,
a
circumscribed hypomelanosis resulting
from
enlarging
and
coalescing white macules, appears
in a
mirror-image
distribution (see 9.99) around body
orifices,
over
the
bony prominences (e.g. knees, elbows, hands),
in
the
axillae (7.44)
and
groins.
It is
familial
in
over one-third
of
cases
and is
often associated with
a
variety
of
auto-
immune disorders (see Table 9.2,
p.
176).
Pemphigoid (7.45)
and the
papular exanthem
of
second-
ary
syphilis (7.46)
are
some
of the
other skin conditions
that involve
the
trunk. Tuberculoid leprosy
may
present
as
one or
more asymmetrical, well-defined, slightly scaly
hypopigmented
areas
on the
chest (7.47).
There
is
always
loss
of
sensation
in
these
lesions, which helps
to
distinguish
them
from
pityriasis versicolor.
The
loss
of
sensation
usually
affects
light touch
and
temperature,
but
sometimes
appreciation
of
pain
is
lost
as
well.
7.44
Depigmented,
sharply
demarcated
macular patch
7.45
Erythematous
papules
and
ruptured
bullae
with
crusted
tops
7.46
Secondary syphilis:
maculopapular
eruption
7.47
Tuberculoid
leprosy:
well-defined,
hypopigmented,
sthetic
jle
8
THE
ABDOMEN
151
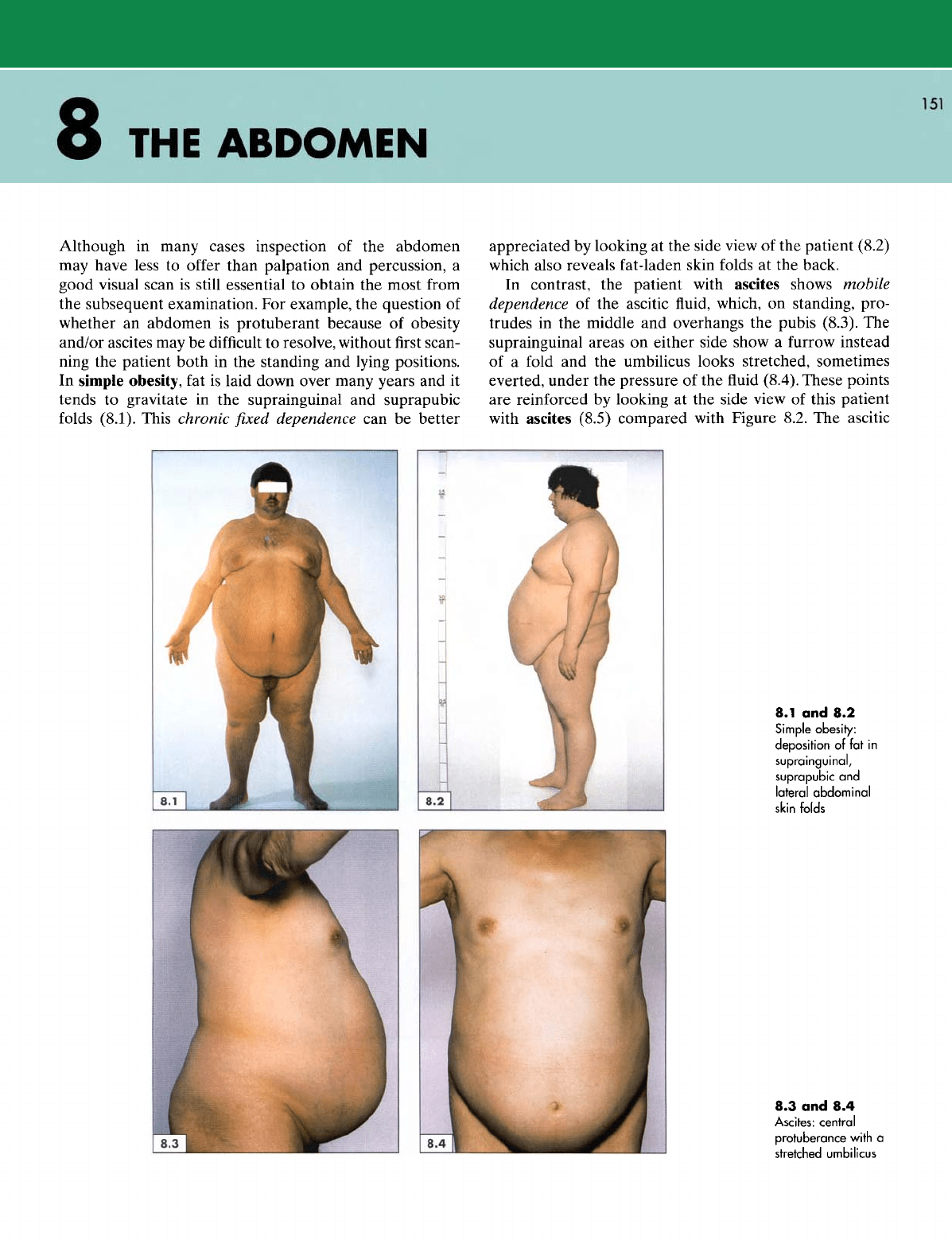
Although
in
many cases inspection
of the
abdomen
may
have less
to
offer
than palpation
and
percussion,
a
good visual scan
is
still essential
to
obtain
the
most
from
the
subsequent examination.
For
example,
the
question
of
whether
an
abdomen
is
protuberant because
of
obesity
and/or
ascites
may be
difficult
to
resolve, without
first
scan-
ning
the
patient both
in the
standing
and
lying positions.
In
simple obesity,
fat is
laid down over many years
and it
tends
to
gravitate
in the
suprainguinal
and
suprapubic
folds
(8.1).
This chronic
fixed
dependence
can be
better
appreciated
by
looking
at the
side view
of the
patient (8.2)
which
also reveals fat-laden skin
folds
at the
back.
In
contrast,
the
patient with ascites shows mobile
dependence
of the
ascitic
fluid,
which,
on
standing, pro-
trudes
in the
middle
and
overhangs
the
pubis (8.3).
The
suprainguinal
areas
on
either side show
a
furrow
instead
of
a
fold
and the
umbilicus looks stretched, sometimes
everted,
under
the
pressure
of the fluid
(8.4).
These
points
are
reinforced
by
looking
at the
side view
of
this patient
with
ascites (8.5) compared with Figure 8.2.
The
ascitic
8.1
and 8.2
Simple obesity:
deposition
of
fat
in
suprainguinal,
suprapubic
and
lateral
abdominal
skin
folds
8.3 and 8.4
Ascites:
central
protuberance
with
a
stretched umbilicus