Marshall L. Stoller, Maxwell V. Meng-Urinary Stone Disease
Подождите немного. Документ загружается.

Chapter 33 / Open Stone Surgery 639
639
From: Current Clinical Urology, Urinary Stone Disease:
A Practical Guide to Medical and Surgical Management
Edited by: M. L. Stoller and M. V. Meng © Humana Press Inc., Totowa, NJ
33
Open Stone Surgery
Elizabeth J. Anoia, MD and Martin I. Resnick, MD
CONTENTS
INTRODUCTION
INDICATIONS FOR OPEN STONE SURGERY
SURGICAL TECHNIQUE
RESULTS
COMPLICATIONS
CONCLUSIONS
REFERENCES
Key Words: Nephrolithiasis; surgery; anatrophic nephrolithotomy;
open surgery.
INTRODUCTION
Urinary lithiasis is a disease process that predates the Hippocratic Oath (1). It afflicts
males three times more frequently than females with a peak age incidence occurring in
the twenties to forties. Most cases of stone disease are not linked to a specific genetic
defect and their development is related to multiple external factors, including diet. The
main types of stones are composed of calcium, struvite, uric acid, and cystine; the com-
position of each stone is unique owing to the variety of etiology and patient response to
the different therapies available (2). Medical, as well as surgical therapies, are both used
as effective forms of treatment. This chapter will focus specifically on the role of open
stone surgery in the treatment of patients with urinary lithiasis.
The surgical treatment of urolithiasis has undergone a rapid evolution over the past
25 yr. Before the introduction and refinement of extracorporeal, endourologic, and
percutaneous techniques, urinary stones required major open surgical procedures, which
had a significant morbidity and potential for renal loss. The advent of these newer less
invasive techniques has resulted in a shift in the manner in which all types of stones are
managed.

640 Anoia and Resnick
One open surgical treatment option is termed anatrophic nephrolithotomy. Anatrophic
nephrolithotomy is a procedure that has been used by urologists for over 30 yr for the
removal of staghorn renal calculi. The original description was by Smith and Boyce in
1968 and was based on the principle of placing the nephrotomy incision through a plane
of the kidney that is relatively avascular—between the anterior and posterior segmental
arteries. This approach avoids damage to the renal vasculature and subsequent atrophy
of the renal parenchyma, hence the term anatrophic (3).
Other types of open stone surgery include radial nephrotomies, pyelolithotomy,
extended pyelolithotomy, and ureterolithotomy. Pyelolithotomy refers to the incision
of the renal pelvis. Radial nephrotomy describes a procedure in which multiple paren-
chymal incisions are made over the calculus to effect its removal. A simple pyelolitho-
tomy can be used for partial staghorn stones or multiple 1–2 cm stones that extend into
the calyces. An extended pyelolithotomy, also referred to as the Gil-Vernet approach,
is indicated for more complex stones that extend into infundibula (4). Ureterolitho-
tomy can be performed throughout the entire length of the ureter when extracorporeal
shockwave lithotripsy (SWL) or endoscopic techniques fail. The surgical approach
depends on the location of the stone—at the ureteropelvic junction, in the proximal
half, or in the distal half.
INDICATIONS FOR OPEN STONE SURGERY
Struvite stones are often associated with urinary tract infections, and the coexistence
of these two conditions makes it difficult to eradicate either. Definitive treatment of these
stones is generally advocated because of the significant morbidity and mortality asso-
ciated with untreated infected calculi. Blandy and Singh found that patient survival is
reduced with untreated staghorn calculi, with a mortality rate of 28% at 10 yr (5). The
American Urologic Association Nephrolithiasis Clinical Guidelines Panel in 1994 rec-
ommends a percutaneous procedure with or without SWL as an initial treatment for
complex staghorn calculi (6). However, in specific situations anatrophic nephrolitho-
tomy remains the optimal treatment option for renal calculi and thus has maintained an
important, albeit smaller, role in the treatment of these large complex stones. Anatrophic
nephrolithotomy involves not only removal of the stone but also reconstruction of the
intrarenal collecting system to eliminate anatomic obstruction. Thus, this procedure
would improve urinary drainage, thereby reducing the likelihood of urinary tract infec-
tion, which would prevent recurrent stone formation.
The indications for all open stone surgeries have changed somewhat with advances
in minimally invasive methods of treating stones; however, the inability to successfully
eradicate a stone with less invasive methods remains an important indication. In 1994,
Assimos (7) outlined specific anatomic clinical scenarios for open renal or ureteral
surgery. Calyceal diverticular stones can be difficult to treat percutaneously when the
diverticula are intimately associated with the hilar vessels or have an extrarenal exten-
sion. Open surgical pyelolithotomy and pyeloplasty has been recommended in kidneys
with stones and a ureteropelvic junction obstruction if there is a large redundant pelvis
that necessitates tapering, a high ureteral insertion, a long segment of stricture, if the
obstruction is associated with an aberrant lower pole artery, and in patients with solitary
kidneys. Patients with other forms of nephroureteral obstruction which require stone
treatment in conjunction with anatomic correction are often better served with an open
definitive procedure.

Chapter 33 / Open Stone Surgery 641
Ureteral stones associated with ureterocele, ectopic ureters, obstructing congenital
megaureter, or kidney with severe infundibular stenosis are examples that could be
treated with a ureterolithotomy (7). Stones in the presence of an ileal conduit present a
treatment challenge, especially if there is a Wallace ureterointestinal anastomosis (8).
Overall, less than 3% of all upper ureteral stones will require an open procedure. Char-
acteristics more common to this group are moderate to severe hydronephrosis and larger
stone size (9).
Emphysematous pyelonephritis associated with stones that have been unsuccessfully
treated percutaneously is another indication for an open approach. Ectopic kidneys or
pelvic horseshoe kidneys may require an open surgery if the major stone burden is in
extremely anterior pelvis that limits adequate shockwave focusing or percutaneous
access. A preoperative abdominal angiogram is recommended as the blood supply can
vary (7).
Certain stone compositions (calcium oxalate monohydrate and brushite) may not be
as effectively treated with SWL therapy, and open procedures may be required if they
are refractory after multiple attempts. Impacted stones may also require an open salvage
procedure (2,7,9).
Anatrophic nephrolithotomy or other open procedures can also be the first line treat-
ment in patients requiring stone removal but have a body habitus that makes the less
invasive procedures difficult to impossible (7,10). The presence of limb contractures,
stones in a transplant kidney (11), and obesity often present challenges for positioning
and access. These include an inability to reach stones with traditional instruments, the
risk of severe tissue necrosis secondary to positioning, and technical issues. SWL can
only be performed in patients in whom the stone–skin distance equals the approximate
focal length of the specific machine. Percutaneous nephrolithotomy (PCNL) also requires
adequate fluoroscopic penetration to visualize the stone.
Despite the need for open surgery, these procedures come with their own set of risks.
There can be difficulty in identifying anatomic landmarks and inadvertent incisions have
been made above the 10th rib. Other problems are awkward positions for the surgeons,
well-vascularized subcutaneous tissue leading to excessive bleeding from skin inci-
sions, intraoperative rhabdomyolysis resulting in temporary renal failure, and wound
infection (10).
Other relative indications include select cases of complex stone disease, previous
renal surgery, comorbid disease, and patient preference (12,13). Before deciding on a
treatment strategy, the above factors, the urologist’s preference and access to equipment,
and the patient’s individual situation must be considered.
If a patient’s clinical presentation does not mandate open surgery, other important
variables in deciding between open procedures and other less invasive modalities must
be considered. Each option has its own advantages, disadvantages, and different stone
free rate. Studies have compared the cost and morbidity of percutaneous vs open flank
procedures. Percutaneous procedures involved less anesthesia time, less duration of
hospitalization, less recuperative time, decreased transfusion requirements, less post-
operative need for narcotics, and less total cost without an increased risk for renal
parenchymal damage (14,15). However this may not be the case when unsuccessful
percutaneous procedures are considered, demonstrating the importance of the learning
curve and the stone burden (15). Larger stones require more manipulation, longer pro-
cedures, and often multistage approaches.

642 Anoia and Resnick
SURGICAL TECHNIQUE
Incisions
There are several approaches for open stone surgery, depending on the location of the
stone and patient and physician preferences previously described: the commonly used
flank approach, the posterior approach, and the most invasive transperitoneal approach.
The basic surgical principles of stone extraction are similar; the difference lies in how
access to the kidney and ureter is obtained. The flank approach may be subcostal or
intercostal; this approach provides better access to the renal hilum and the upper pole
(16). The posterior approach is an excellent procedure for pyelolithotomy and upper
third ureterolithotomy with decreased postoperative pain and shorter hospital stay (17).
The transabdominal approach is reserved for patients that are difficult to position or for
patients who have undergone multiple previous surgical procedures (16). In any case
after the administration of appropriate preoperative intravenous antibiotics and induc-
tion of general anesthesia, a Foley catheter is placed in the bladder.
For the flank approach the patient is placed in the standard flank position with eleva-
tion of the kidney rest and flexion of the operating table to achieve adequate spacing
between the lower costal margin and the iliac crest. Three-inch-wide adhesive tape
applied at the shoulders and hips is often used to secure the patient to the table. Adequate
padding should be used to protect pressure points. The incision can be placed through
the bed of either the 11th or 12th rib, depending on the estimated position of the kidney
and the location of the stone, and can be extended as far medially as the lateral border
of the rectus sheath. If a previous flank incision has been made for renal surgery, it is
preferable to place the incision above the old scar, ensuring that access to the kidney can
be achieved through unscarred tissue. After rib identification and resection when access
has been gained into the retroperitoneal space, Gerota’s fascia is visualized overlying the
kidney (16).
The technique for the posterior approach is as follows. The patient is placed in the
lateral position with the table flexed to extend the lumbar region. A vertical lumbar
incision along the lateral margin of the sacrospinalis muscle is made starting superiorly
at the upper margin of the 12th rib extending laterally to the iliac crest inferiorly. The
incision is carried down through the lumdodorsal fascia to the sacrospinalis and quadra-
tus lumborum muscles. These are then medially retracted to approach the renal fossa,
avoiding the morbidity of a muscle-splitting incision. If greater superior exposure is
needed, the 12th rib can be resected or the costovertebral attachment of this rib severed.
A selfretaining retractor is then inserted, being careful to avoid injury to the pleura and
subcostal vessels. After Gerota’s fascia is incised, excellent exposure is gained to the
renal pelvis and upper ureter for simple or extended pyelolithotomy or ureterolitho-
tomy (17).
Anatrophic Nephrolithotomy
In the classic description of anatrophic nephrolithotomy (3) Gerota’s fascia is incised
in a cephalad–caudal direction, which facilitates returning the kidney to its fatty pouch
at the end of the operation. The kidney is fully mobilized and the perinephric fat is
carefully dissected off the renal capsule with care taken not to disrupt the capsule. Should
the capsule become inadvertently incised, it can be closed at that time with fine chromic
catgut sutures. The kidney is now free to be suspended in the operative field by utilizing
Chapter 33 / Open Stone Surgery 643
a broad umbilical tape at each pole. At this point a preliminary portable plain radiograph
is obtained to identify the position and size of the stone(s).
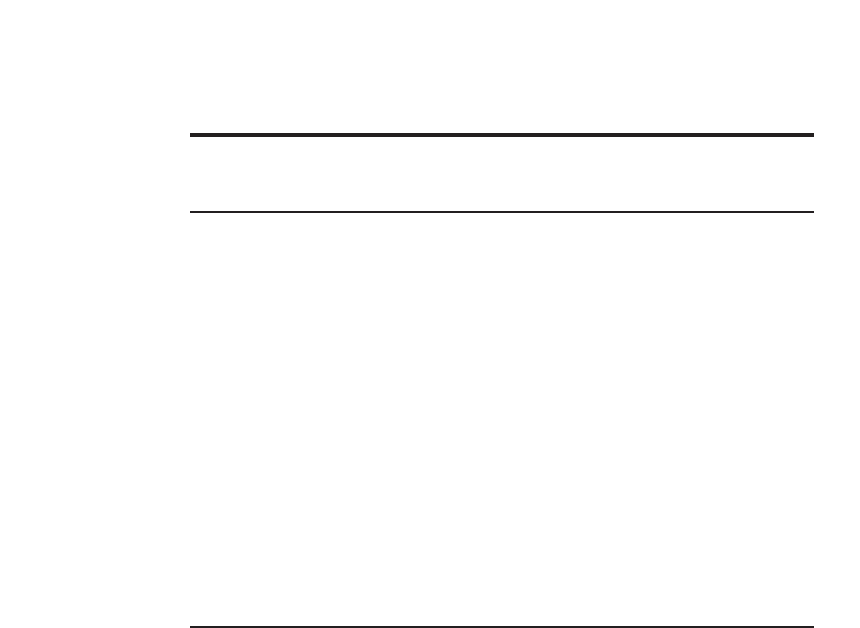
For the renal hilar dissection, the main renal artery and the posterior segmental branch
are approached posteriorly, carefully identified, and dissected (Fig. 1A). The renal pel-
vis and ureter should be identified, but not dissected. The avascular plane is identified
by temporarily clamping the posterior segmental artery and injecting 20 mL of methy-
lene blue intravenously. This results in the blanching of the posterior renal segment
while the anterior portion turns blue, allowing identification and marking of the avascu-
lar plane (Fig. 1B) (18). Placing the nephrotomy incision through this plane will achieve
maximal renal parenchymal preservation and minimize blood loss. The avascular plane
can also be identified with the use of a Doppler to localize the area of the kidney with
minimal blood flow.
More extensive renal hilar dissection can be avoided by utilizing a modification of the
original procedure described by Smith and Boyce. Redman and associates relied on the
relatively constant segmental renal vascular supply in the identification of Brodel’s line.
They advocated placing the incision at the expected location of the avascular plane after
clamping the renal pedicle with a Satinsky clamp, in an effort to prevent vasospasm of
the renal artery and warm ischemia (19). This modification can be time-saving and spare
extensive dissection of the renal hilum.
More recently, McAninch et al. have added another modification to this classic descrip-
tion in an attempt to maximally preserve renal function. In their description the renal
capsule is incised over the lateral convex surface of the kidney and a parenchymal
incision is made 1–2 cm posterior to the capsulotomy. This location approximates the
“avascular plane” and allows access to the collecting system directly over the stone
burden. The two potential advantages are avoiding overlying suture lines and ready
access to the collecting system (20).
Just before occluding the renal artery, 25 g of intravenous mannitol is administered.
This promotes a postischemic diuresis and prevents the formation of intratubular ice
Fig. 1. Anatrophic nephrolithotomy. (A) Main renal artery and branches are isolated. (B) The
posterior segmental artery is occluded, and methylene blue is administered intravenously. The
resulting demarcation between pale ischemic and bluish perfused parenchyma defines a rela-
tively avascular nephrotomy plane.
644 Anoia and Resnick
crystals by increasing the osmolarity of the glomerular filtrate. The main renal artery is
occluded with an atraumatic bulldog vascular clamp. A bowel bag is quickly placed
around the kidney, and it is insulated from the body wall and peritoneal contents with dry
packs. Hypothermia is then initiated with iced saline slush covering the kidney. The
kidney should be cooled for 10–15 min before the nephrotomy incision is made. This
should allow achievement of a core renal temperature of 15–20°C, which will allow safe
ischemic times from 60 to 75 min and minimizes renal parenchymal damage (21). The
ice slush should be continuously reapplied as needed throughout the procedure.
The renal capsule is incised sharply over the previously identified line, being careful
to avoid extension into the upper and lower poles. The renal parenchyma is bluntly
dissected with the back of the scalpel handle which minimizes injury to the intrarenal
arteries that are traversed. Small bleeding vessels can be controlled with 4-0 or 5-0
chromic catgut figure-eight suture ligature. If renal back bleeding continues to be a
problem despite these measures, the main renal vein can be occluded.
As the nephrotomy incision proceeds toward the renal hilum, the ideal location to
enter the collecting system is at the base of the posterior infundibula. The intraoperative
radiograph can be used as a guide to the pelvis and the base of the calyx. Occasionally,
with large posterior calyceal calculi, a dilated posterior calyx will be entered initially.
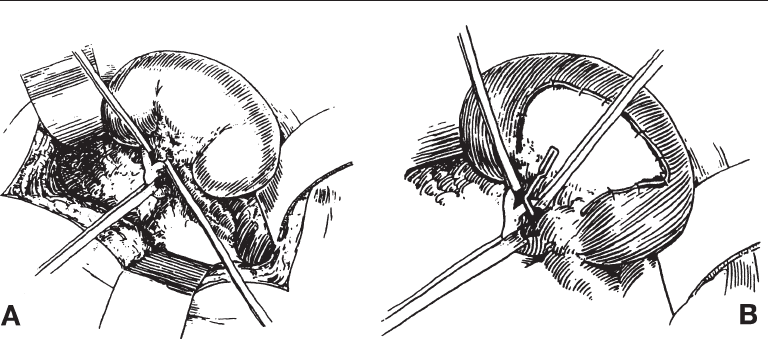
The remainder of the collecting system is identified with a probe and opened. If a
posterior infundibulum is entered first, the incision is then carried toward the renal
pelvis (Fig. 2). The stone is visualized and all ramifications of the stone are exposed by
opening adjacent infundibula into the calyces. In order to minimize stone fragmentation
and retained calculi, the stone should not be manipulated or removed until all of the
calyceal and infundibular extensions are appropriately identified and incised. This
allows for complete visualization and mobilization of the collecting system and calculi.
Ideally, the stone or stones should be removed without fragmentation; however, often
it is inevitable that there will be some piecemeal extraction. If this is necessary, a
ureteral stent can be inserted to prevent stone migration down the ureter during manipu-
lation. Each calyx should usually be inspected for stone fragments. After removal of all
stone fragments, the renal pelvis and calyces are copiously irrigated with cold saline and
the irrigant is aspirated. A nephroscope can be used to look for residual fragments. A
Fig. 2. The collecting system is carefully incised.
Chapter 33 / Open Stone Surgery 645
plain radiograph or ultrasonography are also options. At this time, a “double-J” ureteral
stent is passed from the renal pelvis into the bladder if this was not done at the time of
stone manipulation. The routine use of internal ureteral catheters is encouraged. They
provide good urinary drainage, protect the freshly reconstructed collecting system, and
minimize postoperative urinary extravasation.
The next step in the procedure is the reconstruction of the intrarenal collecting system
with correction of coexistent anatomic abnormalities that may be present. Infundibular
stenosis or stricture, which results in obstruction promoting urinary stasis and recurrent
stone formation, should be corrected with caliorrhaphy or calicoplasty. All intrarenal
reconstructive suturing is accomplished with 5-0 or 6-0 chromic catgut sutures. When
suturing the mucosal edges, it is important to avoid incorporation of underlying inter-
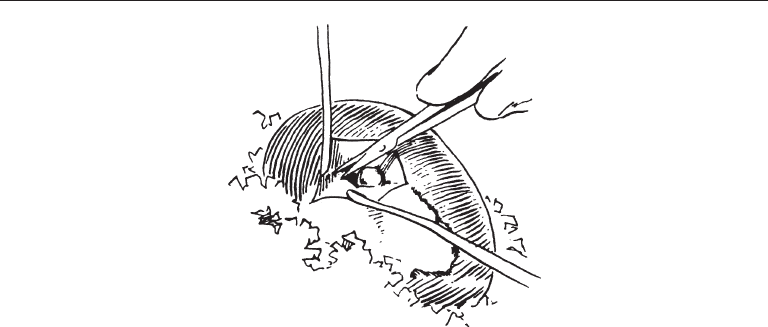
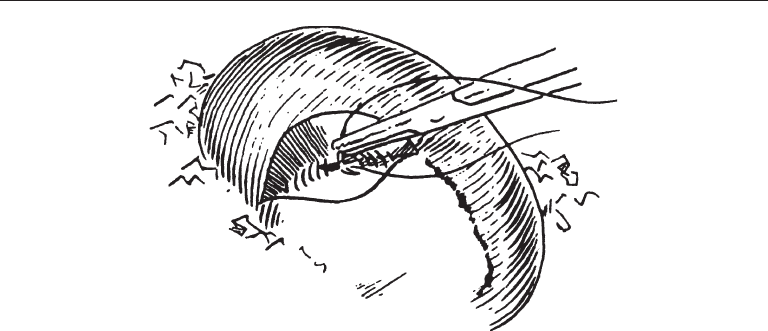
lobular arteries, thus preventing ischemia. The renal pelvis is then closed, first with
reinforcing corner sutures and then with a running 6-0 chromic catgut suture (Fig. 3).
Before closing the renal capsule bleeding points are identified and ligated with 4-0 or 5-
0 chromic figure-eight sutures. The renal capsule is closed with a running lock stitch of
4-0 chromic catgut suture or mattress sutures over bolsters can be used.
McAninch et al. have also created a modification involving renal reconstruction after
nephrolithotomy. Traditionally, the infundibula are reconstructed and the collecting
system is formally closed. The modification simplifies this closure by not reconstruct-
ing the infundibula; instead, the capsular and parenchymal staggered incisions are
closed with nonoverlapping suture lines forming a watertight renal closure. When
postoperative renal function results are compared there is a slight decrease in renal
function in McAninch’s series; however, overall findings are comparable to Smith and
Boyce (20).
After the capsule is closed and adequate hemostasis has been achieved, the renal
artery is unclamped and the kidney is observed for good hemostasis and return of pink
color and turgor. It is then returned into Gerota’s fascia, and the kidney and proximal
ureter are covered with some perirenal fat to minimize postoperative scar formation. If
Gerota’s fascia is unavailable because of previous surgery, omentum can be mobilized
through a peritoneal opening and wrapped around these structures. The peritoneal open-
ing should be sutured to the omentum to prevent herniation of the abdominal viscera.
Fig. 3. The renal pelvis is closed with a running 6-0 chromic suture.

646 Anoia and Resnick
A Penrose or suction-type drain is placed within Gerota’s fascia and brought out
through a separate stab incision. This drain is left in place until minimal drainage occurs,
usually by the third or fourth postoperative day. Nephrostomy tubes are generally avoided
because of their potential for causing infection or further renal damage. The flank mus-
culature and skin are closed in the standard fashion.
Pyelolithotomy
A pyelolithotomy also begins with mobilization of the kidney after Gerota’s fascia is
incised. The degree of mobilization is dependent on the size of the stone. If a smaller,
more centrally located renal pelvis stone is anticipated, it is not necessary to dissect the
renal artery. The renal pelvis and upper ureter are identified and the pelvis is approached
posteriorly to avoid injury to the renal vein. Two stay sutures are placed in the renal
pelvis using 4-0 chromic suture and a longitudinal incision made. Care must be taken to
avoid extension into the ureteropelvic junction so as to reduce the risk of subsequent
scarring and the development of ureteropelvic junction obstruction. After the successful
removal of all stones, the renal pelvis is closed with a 4-0 chromic continuous suture.
Drainage of the system is performed as described previously (16).
Extended Pyelolithotomy
In an extended pyelolithotomy described by Gil-Vernet (4), the dissection is more
extensive. The thin layer of connective tissue that extends from the renal capsule onto
the renal pelvis must be carefully incised in order to gain access to the renal hilum and
infundibula. The dissection is carried subparenchymally to expose the renal pelvis and
the infundibula. A curvilinear pyelotomy incision is made over the stone and then
extended to the superior and inferior calyces. The stone is freed from the mucosa and
removed. Once one is confident that all fragments have been removed with the aid of
radiographs and nephroscopy, the collecting system is closed with a continuous 4-0
chromic catgut suture as described above. The infundibular incisions will be covered by
the renal parenchyma; therefore it is not necessary to completely close them (22).
Drainage of the flank is again performed.
Ureterolithotomy
Ureterolithotomy can be performed via multiple approaches. The flank or posterior
lumbotomy incision can be used for the upper ureter, an anterior extraperitoneal muscle-
splitting incision can adequately expose the mid-ureter, and the lower ureter can be
accessed via a Gibson, Pfannenstiel, or midline suprapubic incision (8). Once the
approach is decided, radiographs are obtained to confirm stone position. For an upper
ureterolithotomy Gerota’s fascia is opened and the upper ureter is identified. A Babcock
forceps or vessel loop is placed on the ureter above the stone for traction and to prevent
stone migration. Dissection is carried downward to provide adequate exposure, being
careful not to devascularize the ureter or injure the muscularis layer. A vertical uretero-
tomy is made over the stone without injuring the posterior ureteral wall. After careful
stone extraction the entire ureter is irrigated and a double J stent may be placed. The
incision is closed longitudinally with simple interrupted 5-0 sutures placed 1–2 mm
apart. A Penrose or suction drain is used to drain the area of the ureterotomy. The
principles of stone extraction remain the same in a distal ureterolithotomy; however,
exposure of the ureter requires certain other maneuvers. Identifying the iliac vessels

Chapter 33 / Open Stone Surgery 647
and dividing the obliterated umbilical vessels can help. The bladder is reflected medi-
ally and kept decompressed with a Foley catheter (8,23).
Postoperative Management
Postoperative management after anatrophic nephrolithotomy, pyelolithotomy, or ure-
terolithotomy should follow the same principles that guide management after other
major operations. Intravenous fluids are maintained to achieve brisk urine output and
until the patient is able to tolerate a clear liquid diet. Broad-spectrum intravenous anti-
biotics are administered perioperatively and continued postoperatively for 5–7 d. Anti-
biotic coverage is guided by preoperative urine culture and sensitivity findings. The
ureteral stent is removed cystoscopically at approx 7 d postoperatively in uncomplicated
cases. A urine culture is checked for persistence of infection. At 1–2 mo a follow-up
intravenous pyelogram is obtained.
RESULTS
Stone free rates with staghorn calculi show that 21% of percutaneous procedures
required additional procedures to clear the stone burden. In contrast only 4% of patients
required further intervention after anatrophic nephrolithotomy. Residual stone disease
leading to multiple procedures is one of the significant drawbacks of PCNL (14). Less
than 10 yr after its development SWL monotherapy was found to have a 61% stone-free
rate at 8 mo of follow-up (24). PCNL or PCNL–SWL sandwich therapy stone free rates
were reported as 54–95% depending on stone volume and collecting system dilatation
(7). Endoscopic therapy of renal and ureteral stones with the Holmium:YAG laser is
reported to have an overall stone free rate of 95% when combined with other types of
lithotripsy (25). Overall, anatrophic nephrolithotomy stone free rates range from 80–
100% depending on collecting system dilatation and stone burden (12,26).
Open pyelolithotomy has a stone-free rate that approaches 100% if there is a single
stone. However if a staghorn stone is present or if there are multiple calyceal stones, the
stone-free rate decreases to approx 90% (16). A retrospective study by Paik et al. in 1998
reported an initial stone free rate of 93% in patients with large renal pelvic stones
undergoing simple or extended pyelolithotomy (13).
In 1997, the American Urologic Association published a meta-analysis on the cur-
rently available methods for treating ureteral calculi. Stone free rates for ureterolitho-
tomy vary from 84–100% depending on stone size and location (9,27). SWL had a 57%
stone-free rate with one-third of patients requiring second procedures. Endoscopic pro-
cedures were more successful with an initial stone-free rate of 74% and a final clearance
rate of 95% after additional procedures (9). Overall, the goals of open stone surgery
should be to remove all calculi and fragments, to improve urinary drainage of any
obstructed intrarenal collecting system, to eradicate infection, to preserve and improve
renal function, and to prevent stone recurrence (28).
As open stone surgery accounts for <5% of treatment modalities for staghorn and
other complex stones, there are now other less invasive techniques either alone or in
combination that have replaced these procedures. Despite impressive advances with the
less invasive techniques, anatrophic nephrolithotomy, pyelolithotomy, or ureterolitho-
tomy remain viable treatment options for large or staghorn calculi not expected to be
eliminated with a reasonable number of less invasive procedures. Staghorn stones asso-
ciated with anatomic abnormalities also require open surgical correction.

648 Anoia and Resnick
COMPLICATIONS
Complications resulting from open stone surgery are similar to other forms of open
surgery, for example wound infections and postoperative fevers. Pulmonary compli-
cations are common including atelectasis, pneumothorax, and pulmonary embolism.
Patients with a history of pulmonary disease should likely undergo preoperative evalu-
ation with pulmonary function testing and initiation of vigorous pulmonary toilet
before surgery. Postoperatively, patients should be encouraged to breathe deeply, and
use of an incentive spirometer should be routine to prevent atelectasis. Early ambulation
will also be beneficial.
Pneumothorax should occur in fewer than 5% of patients (28). A patient with a history
of pyelonephritis or previous renal surgery is at increased risk. Inadvertent opening of
the pleura, usually during incision and resection of a rib, should be identified and
repaired intraoperatively with a running chromic catgut suture. The lung is hyperinflated
just before the final suture is placed to ensure re-expansion of the lung. Chest tubes are
not routinely used but may be necessary if any question remains regarding the reliability
of the pleural closure. A chest radiograph should be obtained in the recovery room for
any patient who undergoes repair of a pleural defect. Pulmonary embolism remains a
potential complication of any major surgery. Routine use of support hose and sequen-
tial-compression stockings can lower the risk of deep venous thrombosis. Encourage-
ment of early ambulation is also an important preventive measure.
Significant postoperative renal hemorrhage after anatrophic nephrolithotomy should
occur in fewer than 10% of patients. Assimos and associates reported an incidence of
6.4%. Bleeding usually occurs immediately or approx 1 wk postoperatively. Extensive
intrarenal reconstruction, older age, impaired renal function, and presence of blood dys-
crasias were found to be significant risk factors. Slow bleeding will usually resolve on
its own; management includes correction of any bleeding abnormalities and replacement
with blood products as necessary. Oral aminocaproic acid can be successful in certain
cases. Bleeding that is brisk or cannot be adequately treated conservatively will require
a more aggressive approach. A renal arteriogram can help identify the lesion, and an
attempt at arteriographic embolization should be considered. Re-exploration may be
required in the remainder of the cases, with reinstitution of hypothermia and suture
ligation of the bleeding vessel(s). Persistent hematuria 1–4 wk postoperatively should
alert the clinician to the possibility of renal arteriovenous fistula formation or a false
aneurysm (29). Other possible complications that can result from arterial clamping
include renal injury and hypertension.
Urinary extravasation with any procedure should occur infrequently with the routine
use of perinephric drains and ureteral catheter drainage. Should drainage recur or persist
following removal of the drain and/or ureteral stent, replacement of the ureteral stent
should be considered to decompress the system and relieve any obstruction. Flank
abscess as a result of extravasation is an unusual complication that can usually be
managed conservatively with percutaneous drainage or may require open drainage (15).
Open ureterolithotomy has a complication rate ranging from 17–34% via the posterior
lumbotomy and flank approaches, respectively (9). A few complications that are unique
to this procedure include loss of the stone intraoperatively, fistulas, and strictures (8).
Preoperative localization and immobilization of the stone can decrease the risk of stone
loss. Fistulas, although uncommon, can occur with ureteral damage or infection. In 1993
a ureterofallopian fistula, manifesting as complete urinary incontinence, occurred after