Marshall L. Stoller, Maxwell V. Meng-Urinary Stone Disease
Подождите немного. Документ загружается.


588 Gettman and Segura
57. Segura JW, Preminger GM, Assimos DG, et al. Nephrolithiasis clinical guidelines panel summary
report on the management of staghorn calculi. J Urol 1994; 151: 1648–1651.
58. Elashry OM, DiMeglio RB, Nakada SY, McDougall EM, Clayman RV. Intracorporeal electrohy-
draulic lithotripsy of ureteral and renal calculi using small caliber (1.9F) electrohydraulic litho-
tripsy probes. J Urol 1996; 156:1581–1585.
59. Grasso M. Experience with the holmium laser as an endoscopic lithotrite. Urology 1996; 48: 199–
206.
60. Grasso M, Conlin M, Bagley D. Retrograde ureteropyeloscopic treatment of 2 cm. or greater upper
urinary tract and minor staghorn calculi. J Urol 1998; 160: 346–351.
61. Rudnick DM, Bennett PM, Dretler SP. Retrograde renoscopic fragmentation of moderate-size
(1.5–3.0-cm) renal cystine stones. J Endourol 1999; 13: 483–485.
62. Grasso M, Ficazzola M. Retrograde ureteropyeloscopy for lower pole caliceal calculi. J Urol 1999;
162: 1904–1908.
63. Kourambas J, Munver R, Preminger GM. Ureteroscopic management of recurrent renal cystine
calculi. J Endourol 2000; 14: 489–492.
64. Hollenbeck BK, Schuster TG, Faerber GJ, Wolf JS Jr. Flexible ureteroscopy in conjunction with
in situ lithotripsy for lower pole calculi. Urology 2001; 58: 859–863.
65. Lee DI, Bagley DH. Long-term effects of ureteroscopic laser lithotripsy on glomerular filtration
rate in the face of mild to moderate renal insufficiency. J Endourol 2001; 15: 715–717.
66. Lingeman JE, Siegel YI, Steele B, Nyhuis AW, Woods JR. Management of lower pole nephroli-
thiasis: a critical analysis. J Urol 1994; 151: 663–667.
67. Kourambas J, Delvecchio FC, Munver R, Preminger GM. Nitinol stone retrieval-assisted ureter-
oscopic management of lower pole renal calculi. Urology 2000; 56: 935–939.
68. Schuster TG, Hollenbeck BK, Faerber GJ, Wolf JS. Ureteroscopic treatment of lower pole calculi:
comparison of lithotripsy in situ and after displacement. J Urol 2002; 168: 43–45.
69. Elbahnasy AM, Clayman RV, Shalhav AL, et al. Lower-pole caliceal stone clearance after shock-
wave lithotripsy, percutaneous nephrolithotomy, and flexible ureteroscopy: impact of radiologic
spatial anatomy. J Endourol 1998; 12: 113–119.
70. Landman J, Monga M, El-Gabry EA, et al. Bare naked baskets: ureteroscope deflection and flow
characteristics with intact and disassembled ureteroscopic nitinol stone baskets. J Urol 2002; 167:
2377–2379.
71. Albala DM, Assimos DG, Clayman RV, et al. Lower pole I: a prospective randomizd trial of
extrcorporeal shock wave lithotripsy and percutaneous nephrostolithotomy for lower pole neph-
rolithiasis-initial results. J Urol 2001; 166: 2072–2080.
72. Dretler SP. Ureteroscopic fragmentation followed by extracorporeal shock wave lithotripsy: a
treatment alternative for selected large or staghorn calculi. J Urol 1994; 151: 842–846.
73. Mugiya S, Ohhira T, Un-No T, Takayama T, Suzuki K, Fujita K. Endoscopic management of upper
urinary tract disease using a 200-µm holmium laser fiber: initial experience in Japan. Urology
1999; 53: 60–64.
Chapter 30 / Ureteroscopy 589
589
From: Current Clinical Urology, Urinary Stone Disease:
A Practical Guide to Medical and Surgical Management
Edited by: M. L. Stoller and M. V. Meng © Humana Press Inc., Totowa, NJ
30
Ureteroscopy
Technical Aspects
Assaad El-Hakim, MD, Beng Jit Tan, MD,
and Arthur D. Smith, MD
CONTENTS
INTRODUCTION
ACCESS
INSTRUMENTATION
PEARLS/TRICKS
SUMMARY
REFERENCES
Key Words: Ureter; nephrolithiasis; instrumentation; ureteroscope.
INTRODUCTION
Ureteroscopy has gained widespread use for diagnosis and treatment of diseases of the
upper urinary tract. Ureteroscopy came as an extension of cystoscopy and was based to
a large extent on technologic advances in instrumentation. In 1912, Young and McKay
passed a rigid cystoscope into the dilated ureter of a boy with posterior urethral valves
(1). Since then, vast alterations in the concept and design of endoscopes occurred. Min-
iaturization of both rigid and flexible ureteroscopes was made possible mainly by
fiberoptic imaging technology. Ancillary instruments for ureteral access, stone frag-
mentation and retrieval, and other diagnostic and therapeutic applications have also been
developed. In this chapter, we review the technical aspects of ureteroscopy, including
ureteral access and instrumentation available for endoscopic stone management.
ACCESS
A complete patient history, physical examination, laboratory tests, and upper tract
imaging should be obtained in preparation for either diagnostic or therapeutic uretero-
590 El-Hakim, Tan, and Smith
scopy. The procedure must be planned appropriately depending on the collecting system
anatomy and the pathology in question. Previous pelvic surgery, radiation therapy, or
trauma may lead to anatomical abnormalities of the upper tracts. Likewise, a urethral
stricture or significant prostatic enlargement may make access difficult. An in-depth dis-
cussion of how to overcome a difficult access is presented in the Pearls and Tricks section
at the end of this chapter. We routinely administer preoperative prophylactic antibiotics
and use pneumatic compressive sleeves on the lower extremities to prevent deep venous
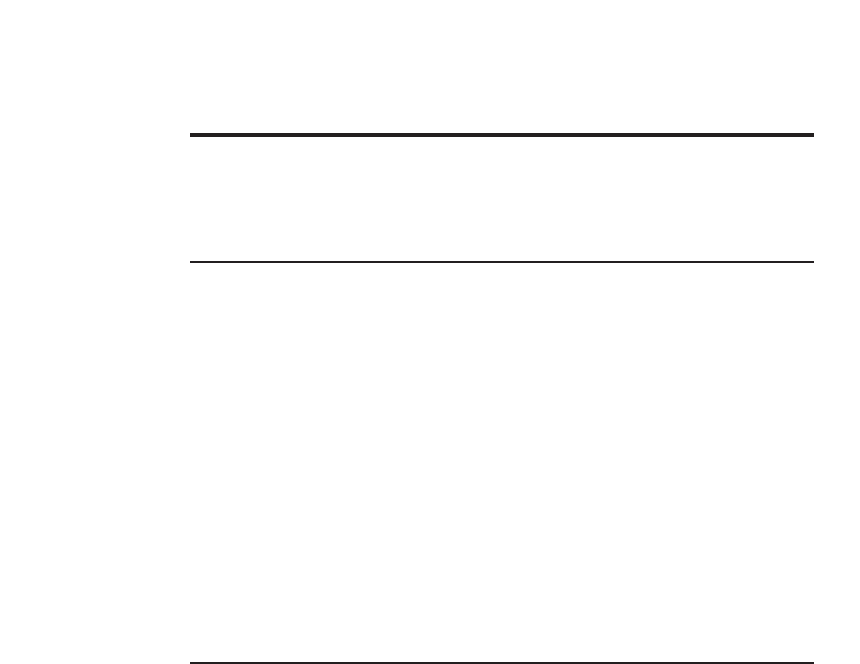
thrombosis. Basic requirements to obtain ureteral access include a cystoscopy table, cam-
era/video equipment, and a fluoroscopy unit (Fig. 1). The operating table must be radiolu-
cent, equipped with stirrups, and allow for a drainage system. Occasionally, the position
of the table must be altered to achieve better access to the ureter. A camera/video system
allows the surgeon to operate in a comfortable position with the advantage of a magnified
view. The assistant surgeon can follow the procedure simultaneously, and mentoring is
likewise facilitated. Fluoroscopy is mandatory to obtain access and perform adequate
tasks. All of the following maneuvers require fluoroscopic guidance, including retrograde
pyelography, insertion of guidewires, stents, and balloon dilation. We do not recommend
carrying out the procedure in a cystoscopy suite with overhead fluoroscopy, as this results
in exposure of the urologist to excessive radiation. The use of an appropriately positioned
C-arm allows the majority of the radiation to be absorbed by the patient.
The patient is positioned in dorsal lithotomy. All pressure points must be padded
carefully. The leg ipsilateral to the ureter to be explored is slightly extended, lowered,
and abducted. This position enhances maneuverability by straightening the distal ureter.
General or regional anesthesia is preferred for therapeutic ureteroscopy, although deep
sedation may be an option in selected cases. Access to the ureter begins by identifying
the ureteral orifice. A rigid cystoscope with a 30° lens, or alternatively a flexible cysto-
scope, is introduced into the bladder. Once the ureteral orifice has been located, a
guidewire is introduced gently (Fig. 2A). An open-ended ureteral stent is used to stabi-
lize the wire and guide its entrance into the orifice. At this point, a retrograde pyelogram
can be performed if necessary, using open ended or olive tip ureteral catheter.
Fig. 1. Video/Camera equipment and portable C-arm
fluoroscopy unit.
Chapter 30 / Ureteroscopy 591
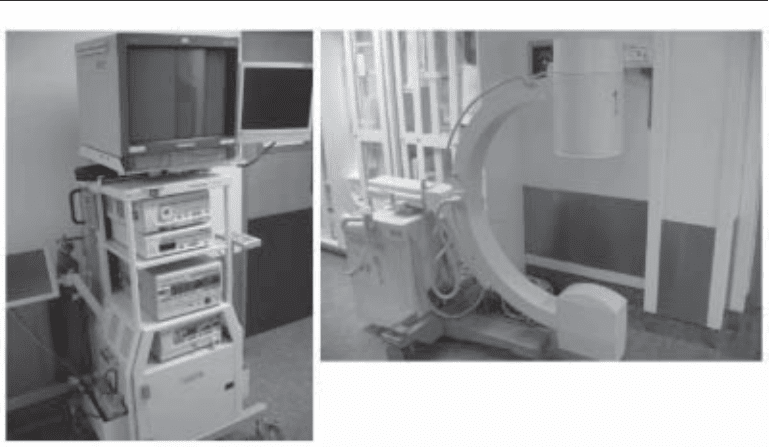
Fig. 2. (A) The ureteral orifice is located cystoscopically and a regular guidewire is introduced.
(B) The ureter is engaged with the rigid ureteroscope with the wire at 12-o’clock position tenting
up the ureteral orifice. Note that the ureteral orifice was not dilated in this case. (C) The distal
ureteral stone is visualized. (D) The holmium-laser fiber is placed on the stone surface before
activating the laser. (E) The stone is vaporized and fragmented in small pieces. (F) Fragments
that are less likely to pass spontaneously are removed using a stone basket. (G,H) The distal ureter
and the ureteral orifice at the end of the procedure; notice that minimal trauma to the urothelium
was sustained.
592 El-Hakim, Tan, and Smith
Ureteral Dilation
Today, technologic breakthroughs allow us to use very small ureteroscopes that per-
mit easy access to the ureter without prior dilation (Fig. 2B). However, this is not always
possible, and in many cases ureteral dilation is required. In general, dilation up to 15 or
18 Fr is more than sufficient (2). Before proceeding with dilatation, a retrograde pyelo-
gram must be obtained to clearly outline the anatomy of the ureter (Fig. 3).
Dilation should be simple, efficient, fast, and cause minimal or no iatrogenic trauma.
General indications include dilation of the ureteral orifice and intramural ureter before
ureteroscopy, and dilation of a ureteral stricture or narrowing.
Balloon dilators are the most preferred and probably the most used dilating devices.
They are available in different sizes, raging from 3 to 30 Fr in diameter and from 1 to
20 cm in length. The shaft length ranges from 30 cm for urethral dilation up to 150 cm
for ureteral dilation. Quality balloons allow for even distribution of pressure along the
entire length of the balloon, while keeping the external diameter constant. Each balloon
dilator has a recommended safe inflation pressure that ranges from 8 to 17 atm.
Balloon dilators accept a regular (0.035- or 0.038-in.) guidewire over which they can
be advanced. In the deflated state, the balloon collapses to essentially the size of the catheter
shaft to allow for smooth advancement and withdrawal from the urinary tract. After mul-
tiple inflations and deflations the balloon will not collapse to its initial deflated size and its
surface becomes somewhat irregular, which makes it more difficult to advance the balloon
forward. For this reason, it is easier to start dilating at the most proximal point of the ureter
and after deflation, pulling the balloon backward. If multiple dilations are required this
maneuver is repeated as necessary to the ureteral orifice. Two radiopaque markers are
located at each end of the balloon and thus indicate its proper position. In addition, balloon
dilators have various tip designs. Longer-tip dilators have a more tapered balloon shape
once inflated, whereas shorter tip dilators allow for a more complete expansion of the distal
end of the balloon, flush with the tip of the dilator.
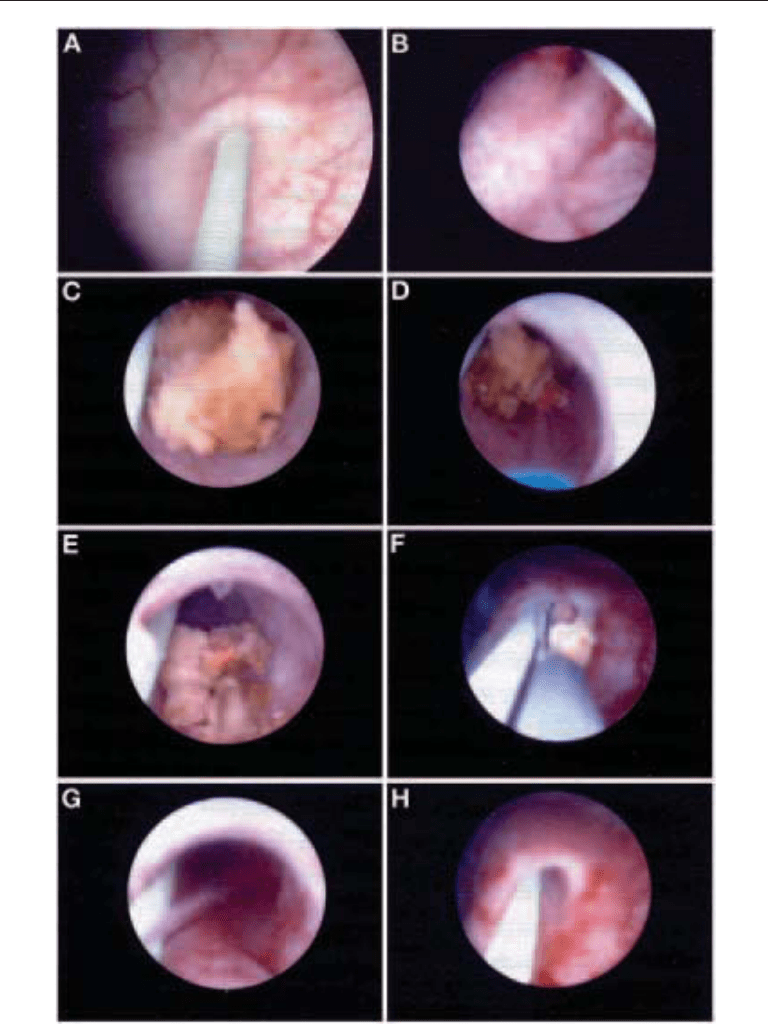
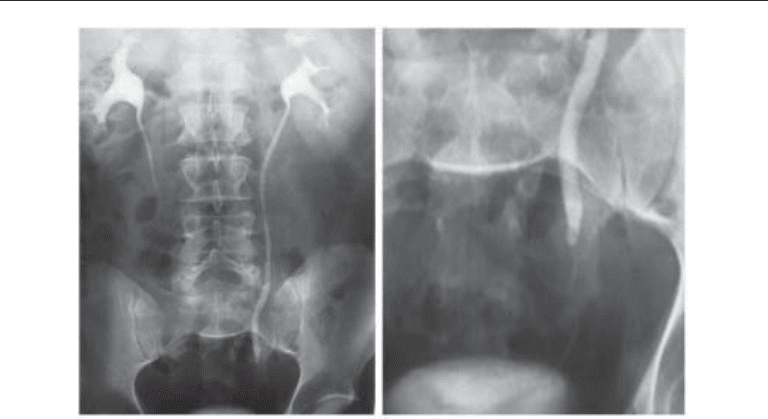
Fig. 3. Intravenous pyelogram (15 min) of a 45-year-old man with left distal ureteral stone. This
patient underwent left rigid ureteroscopy and holmium-laser lithotripsy as shown in Fig. 2.

Chapter 30 / Ureteroscopy 593
Various types of inflation devices are available. The LeVeen device (Boston Scien-
tific, Microvasive) is a 10-mL syringe with a spiral piston that allows gradual and
controlled inflation, and avoids pressure fluctuations. The addition of a pressure manom-
eter gauge permits constant monitoring of the balloon pressure, which must remain
within manufacturer’s range.
After retrograde pyelogram, the radiopaque markers of the balloon are positioned
using fluoroscopy around the desired location. The balloon dilator must be held tightly
in position to prevent it from migrating during inflation. Diluted contrast material is used
to fill the balloon and inflation is monitored fluoroscopically. We use a 6-Fr/65-cm long
shaft with an 18-Fr/4-cm long balloon. The maximum pressure of this balloon is 16 atm.
Inflation is maintained for approx 1–2 min. At the point of narrowing, a circumferential
constriction of the balloon, called a waist, can occur under low pressure, and then dis-
appears. If the waist persists then further dilation is required and it is preferable to deflate
the balloon and repeat the procedure after moving the balloon 0.5–1 cm either proximally
or distally. Inflation pressures of less than 15 atm are usually sufficient in more than 90%
of cases (3). Balloon dilation should never be performed at the level of a ureteral stone.
This may result in ureteral perforation and stone extrusion.
Early in ureteroscopic experience, the distal ureter was routinely dilated to 24 Fr to
facilitate passage of larger rigid ureteroscopes. Although such dilation is considered
excessive nowadays, Garvin and Clayman demonstrated that no distal ureteral stric-
tures occurred on excretory urogram obtained in 86 out of 131 patients who underwent
aggressive ureteral dilation (24 Fr) and ureteral stent insertion after ureteroscopic stone
extraction. A follow-up cystogram in 30 patients showed low-grade vesicoureteral
reflux in 20% of the patients and none of these individuals was symptomatic. However,
mucosal tears and extravasation of contrast were seen in 52% and 19% of patients,
respectively (4).
If balloon dilation is not successful, a backup form of dilation should be available. The
following are alternative mechanical dilating devices, but none are equivalent to balloon
dilators: Teflon or polyethylene dilators, telescoping metal ureteral dilators, metal bou-
gies, and multibeaded, acorn metal dilators. Finally, another system of ureteral dilation
is hydraulic pump dilation. We will discuss briefly each of these options.
Teflon or polyethylene dilators are graduated individual dilators from 6 to 18 Fr that
are passed over a regular guidewire through the cystoscope sheath (by increments of
2 Fr). Also available is a single 14-Fr Teflon dilator with the tip tapering down to 6 Fr
over the distal 4 cm. Dilation is accomplished in one passage with the latter. Lesions of
the ureteral wall secondary to linear shearing can occur with both types of dilators, and
their use is not recommended in the presence of distal stones or steinstrasse (5).
Telescoping metal dilators are coaxial hollow tubes that follow the same principle as
percutaneous renal access dilation. This technique has been abandoned owing to the high
associated rate of iatrogenic injuries. Metal bougies are flexible olive- or acorn-shaped
9–15-Fr dilators. They are passed over a guidewire through a cystoscope sheath. A
modification of this system consists of five individual olive-shaped dilators ranging
from 8.5 Fr to 15 Fr, strung together on a spring wire. The advantage of this method is
single passage of the dilator (6).
In contrast to mechanical-type dilators, the hydraulic Ureteromat (Karl Storz, Cul-
ver City, CA) system involves a pressure irrigation pump connected to the ureteroscope
that provides a controlled pulsatile flow of irrigant at the tip of the instrument. It has
a maximum flow of 400 mL/min and a maximum pressure of 200 mmHg. The irrigant
594 El-Hakim, Tan, and Smith
is directed at the center of the ureteral orifice, stretching its edges and dynamically
dilates it. The system is activated throughout the procedure for enhanced visibility.
The underlying rationale is to achieve temporary inversion of the ureteral peristaltic
waves (7).
Access Sheaths
Ureteral access sheaths and peel-away introducers are coaxial systems composed of
an external Teflon sheath over a polyurethane introducer that are passed over a guidewire.
Internal sheath diameter varies from 9.5 Fr to 14Fr and length from 20 cm to 60 cm. The
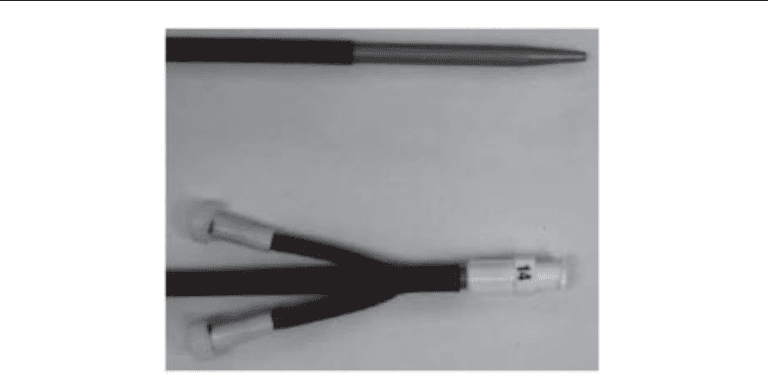
dilator tip tapers to 6 Fr to provide one-step gradual dilation (Fig. 4). The access sheath
provides a continuous working channel for the introduction of ureteroscopes and instru-
ments. The main advantage is to facilitate repeated instrument exchanges while protect-
ing the ureter from potential trauma. The sheath may minimize damage to the flexible
ureteroscope. Potential drawbacks include ureteral wall injury during initial introduc-
tion and access sheath kinking in the prostatic urethra of male patients. In addition, the
sheath may not be very useful for distal ureteral stones.
There has been a recent resurgence in the use ureteral of access sheaths. Preminger’s
group randomized 62 ureteroscopic procedures to 12/14 Fr ureteral access sheath vs no
access sheath. The access sheath appeared to facilitate semirigid and flexible uretero-
scopy by decreasing operative time and costs. There was no significant difference in
postoperative symptoms, early complication rate or stone-free status in the access sheath
and nonaccess sheath groups in patients not requiring additional balloon dilatation (8).
In another report of 71 ureteroscopic procedures using the access sheath the ureteral
stricture rate was 1.4% at 3 mo follow-up or greater (9).
Using an in vitro cadaveric model, application of the ureteral access sheath during
flexible ureteroscopy or percutaneous nephrolithotomy resulted in decreased intra-
renal pressures and increased irrigant flow (10,11). Another potential advantage of the
access sheath is that it facilitates retrograde balloon hot wire incision of ureteropelvic
junction obstruction, and allows direct vision assessment of the incision depth with a
ureteroscope afterwards (12).
Fig. 4. Ureteral access sheath.

Chapter 30 / Ureteroscopy 595
We have found ureteral access sheaths particularly useful in flexible ureteroscopy for
upper ureteral and intrarenal stones. Repeated access is greatly facilitated and stone
fragments can be easily extracted while the ureter is constantly protected.
Safety Wires
Use of safety guidewires is imperative to obtain access to the ureter. The 0.035-in. or
0.038-in. guidewires are standard for most ureteroscopic procedures. Other wires such
as the hydrophilic Teflon wire should also be available. During ureteroscopy the
guidewire plays a very important role. It is needed to gain and secure access, to pass
instruments and scopes, and to insert a ureteral stent. It also serves for reorientation
during surgery, either under direct vision or with fluoroscopy. The guidewire helps to
straighten ureteral kinks and tortuosities, and to align the ureteral orifice with the bladder
neck. Basically, a guidewire is for ureterorenoscopy what a retractor is for open surgery.
It is always preferable to have a safety wire in place during the whole procedure, regard-
less of whether flexible or rigid scopes are being used. For a more detailed description
of the composition and various designs of guidewires please refer to the Instrumentation
section.
Incision
To obtain access to the upper tract beyond the ureteral meatus an endoscopic incision
of the ureter may be required. In the case of an impacted stone at the level of the ureteral
orifice, a direct vision incision of the ureteral orifice can be performed at the 12-o’clock
position. This is achieved using a cold knife urethrotome or the Holmium:yttrium-
aluminum-garnet (YAG) laser. A guidewire can then be inserted past the stone to secure
access.
Other indications for endoureterotomy include ureteral strictures, ureteropelvic junc-
tion obstruction, ureterovesical junction obstruction, and ureteral anastomotic strictures
(uretero-intestinal stricture, ureteral reimplantation stricture, and renal transplant anas-
tomotic stricture). Cold knife, Holmium:YAG laser, and controlled cutting balloon cath-
eter (Acucise catheter) have all been used for the various indications of endoureterotomy,
in either a retrograde or antegrade manner (13). It is, however, beyond the scope of this
chapter to discuss the outcomes of all these techniques.
INSTRUMENTATION
Ureteroscopes
RIGID URETEROSCOPE
Initial exploration of the ureter was performed using rigid pediatric cystoscopes (1,14).
Modern rigid ureteroscopes are miniaturized instruments, which have either fiberoptic
light bundles or rod-lens optical system. The rod-lens system provides excellent optical
quality but does not allow torquing of the scope as that may result in a dark crescent area
appearing on the side of the image. The fiberoptic imaging bundles take up less space
than the rod lens system and have no image artifacts. Most modern rigid ureteroscopes
use this optical technology. Along with the advent of smaller working instruments,
newer ureteroscope diameters range from 6.9 to 9.4 Fr and are equipped with one or two
separate working channels ranging from 2.1 to 5.4 Fr in size. The angle of view is usually
0–5°. These ureteroscopes thus have a larger working channel than instruments of a
596 El-Hakim, Tan, and Smith
similar outer diameter with rod lens imaging systems. Their smaller size allows for easier
access to the upper urinary tract, less trauma to the urothelium (Fig. 2G, H), and possibly
less postoperative pain (15). The standard eyepiece design is in line with the shaft of the
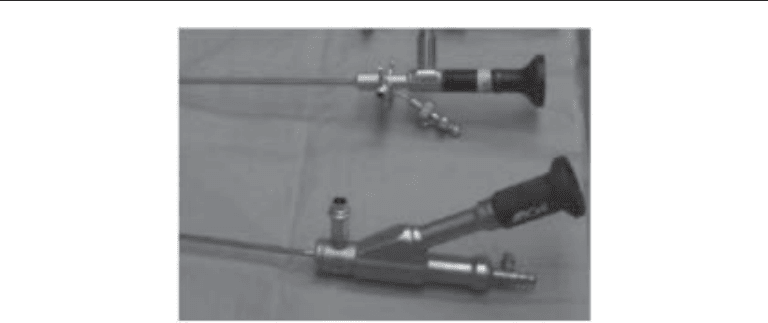
scope; however, most companies have developed ureteroscopes with an offset eyepiece
when rigid ultrasound probes were first introduced for ureteroscopic lithotripsy (Fig. 5).
The offset eyepiece can be fixed or movable. The tip of the ureteroscope is usually
beveled for smoother excursion. As mentioned previously, ureteroscopes with one or
two working channels are available. The advantage of having two separate working
channels is the minimal impact on irrigant flow during insertion of instruments. How-
ever single channels usually have a larger diameter. With the introduction of laser lithot-
ripsy, large working channels are probably less needed and a 3.4 Fr channel is probably
adequate for most procedures. These small-caliber instruments can be inserted without
dilatation of the ureteral orifice in the majority of cases, and are useful for most diagnos-
tic and therapeutic procedures.
During rigid ureteroscopy, the ureteroscope is passed in the urethra alongside the
safety guidewire up to the bladder. The ureter is carefully engaged with the wire at
12-o’clock position tenting up the ureteral orifice (Fig. 2B). Alternatively, the ureter can
be accessed with the wire at 6 o’clock position and the scope inverted 180 so that the
tip elevates the ureteral orifice initially. Under both direct and fluoroscopic guidance, the
ureteroscope is advanced up the ureter keeping the wire in view at all times. If difficulty
is encountered, a second guidewire can be passed through the working channel of the
ureteroscope up to the level of the kidney. This facilitates directing the tip of the scope
and controlled progression over the wire. The initial safety wire will serve to gently open
the ureteral lumen. Other correctable causes should be thought out when encountering
difficulty advancing the ureteroscope, such as an over-distended bladder, inadequate
dilation of the distal ureter, or anatomic abnormalities such as the presence of a large
prostatic median lobe or intrinsic or extrinsic narrowing of the ureter.
Continuous irrigation is very important to ensure adequate visibility during either
rigid or flexible ureteroscopy. Gravity irrigation is often insufficient owing to the narrow
and long working channels of ureteroscopes. Several irrigation devices are available that
generate higher flow at the tip of the instrument. We prefer pressurized irrigation using
Fig. 5. Straight, working–channel, rigid ureteroscope with an offset eyepiece as compared to a
standard rigid ureteroscope.

Chapter 30 / Ureteroscopy 597
a pneumatic sleeve applied around the normal saline bag. The hydraulic Ureteromat
system used for ureteral dilation also provides effective irrigation throughout the proce-
dure. Two 60-mL syringes attached to a Y connector can be used in alternation to
manually inject irrigation solution by the operator assistant.
F
LEXIBLE URETEROSCOPE
Marshall described the first clinical use of a flexible ureteroscope in 1964 (16). By the
1980s, the flexible fiberoptic ureteroscope had evolved from a passive diagnostic tool
to an active therapeutic instrument (17). With continued improvement of endoscopic
instrumentation and development of new energy sources, modern flexible ureteroscopes
now have the ability to access the entire collecting system and have become indispens-
able in the treatment of upper tract calculi, strictures, and tumors. The newest generation
of flexible ureteroscopes have even greater active tip deflection and narrower shaft
diameters; both factors facilitate passage of scopes into the upper tract and access to
lower calyceal pathologies (18).
Image and light transmission in flexible ureteroscopes uses fiberoptic technology.
The light cord can either be separate and plug onto the ureteroscope, or be incorporated
into the scope as an integral cord. Both types of light connection transmit more than
enough light to the internal ureteroscopic fiberoptic system. The depth of image (or field
of view) is limited in most flexible ureteroscopes; thus, flexible ureteroscopes are
equipped with focusing mechanisms and image magnification to compensate for that
loss. In addition to the active tip deflection, flexible ureteroscopes possess secondary
passive deflection. Secondary passive deflection is possible by an additional flexible
segment of the ureteroscope shaft located just proximal to the active deflection level.
This allows access to most parts of the collecting system (19). The principal advantage
of this segment is to allow advancement of the tip of the endoscope in the lower infun-
dibulum. The point of deflection can be effectively moved more proximally along the
shaft of the ureteroscope to give equivalent lengthening of the tip.
Currently available flexible ureteroscopes have a tip diameter from 6 to 8.4 Fr and a
shaft diameter from 7.2 to 9.9 Fr in size. Most ureteroscope working channels are 3.6 Fr
in diameter, although larger channels, up to 4.5 Fr, exist. Many instruments, including
stone baskets, graspers, and biopsy forceps are now available in sizes 3 Fr or less.
Active tip deflection is possible in two directions (down/up), and ranges from 160
to 185 for the downward direction and from 120 to 180 for the upward direction.
Recently, two manufacturers (ACMI, Santa Barbara, CA and Storz, Culver City, CA)
introduced a newer generation of flexible ureteroscopes (DUR-8 Elite and 11278 AU,
respectively) with enhanced active tip deflection (down/up: 310/170 and 270/270,
respectively). The DUR-8 Elite has a second lever to control an additional point of
deflection (130) located more proximally on the shaft (Fig. 6), and the Storz 11278AU
has a single lever that provides maximal deflection. Active tip deflection and irrigant
flow rate are invariably decreased by the introduction of instruments in the working
channel of flexible ureteroscopes. In a comparison of the newer models with their pre-
decessors Chiu et al. found that although the tip deflections of all ureteroscopes were
compromised by the insertion of endoscopic tools, new ureteroscopes were less affected.
However, the irrigant flow rate of these new scopes was decreased compared to their
respective older models (20).
Flexible and rigid ureteroscopes are used in a complementary fashion to access the
entire upper urinary tract. A flexible ureteroscope is introduced into the ureter over a