Elder K. Human preimplantation embryo selection
Подождите немного. Документ загружается.

HUMAN PREIMPLANTATION EMBRYO SELECTION
with the sequential Bonferroni procedure. The out-
come of these analyses is indicated in the tables.
The highest implantation and pregnancy rates
were indeed obtained following transfer of embryos
with 0–5% fragmentation. The embryos in this
group had significantly more cells on average than
the embryos in all other groups, demonstrating an
association between fragmentation and total cell
number (Table 6.2).
The original study
21
had also shown a general
decline in implantation and pregnancy rates when
the majority of the transferred embryos had type I,
type II, type III, or type IV fragmentation, but
the largest decrease in implantation rate occurred
when embryos with fragmentation type IV were
transferred. Embryos with type IV fragmentation
also showed the highest degree of fragmentation,
on average about 25%, which is likely to have
contributed to their low viability.
An updated analysis of transfers in which all
embryos were in the same category with respect to
the pattern of fragmentation (1263 transfers and
2703 transferred embryos) (Tables 6.3 and 6.4; same
statistical analyses as described above) showed that
the highest implantation rate was achieved follow-
ing exclusive transfer of embryos with type I frag-
mentation, while the poorest implantation and
pregnancy outcomes were obtained with embryos
with type IV fragmentation. Embryos with type II
fragmentation implanted as frequently as those with
type III fragmentation. On average, these two pat-
terns showed similar degrees of fragmentation, but
type II embryos had significantly fewer cells than
type III embryos (5.4 ⫾ 1.5 vs 6.1 ⫾ 1.3 cells,
Table 6.3 Pregnancy and implantation outcome in homogeneous transfer groups, including oocyte recipients
Fragmentation
pattern transfer No. of embryos Implantation
group No. of procedures No. of pregnancies Pregnancy rate
a
(%) transferred No. of FHB rate
b
(%)
(1) Type I 130 72 55.4 242 101 41.7
(2) Type II 76 25 32.9 133 37 27.8
(3) Type III 840 412 49.0 1957 613 31.3
(4) Type IV 217 50 23.0 371 61 16.4
FHB, fetal heart beat.
a
Pair-wise contrasts of pregnancy results in groups 1–4 show statistically significant differences between all except group 1 vs group 3; and group 2 vs
group 4.
b
Pair-wise contrasts of implantation results in groups 1–4 show statistically significant differences in all except group 2 vs 3.
Table 6.4 Other characteristics of embryos in the homogeneous fragmentation pattern transfer groups
Average day-3
Fragmentation Average day-3 Average day-3 Average day-3 fragmentation
b
pattern transfer cell number
a
fragmentation
a
cell number
a
(transferred
group (all embryos) ⫾SD (all embryos) (%) ⫾SD (transferred embryos) ⫾SD embryos) (%) ⫾SD
(1) Type I 6.5 1.4 13.1 9.3 7.5 1.3 5.3 2.7
(2) Type II 5.4 1.5 21.7 13.6 6.6 1.7 13.5 6.2
(3) Type III 6.1 1.3 20.5 10.7 7.3 1.3 13.3 5.7
(4) Type IV 5.2 1.4 30.1 15.0 6.3 1.3 24.6 10.9
a) Differences among the groups are significant at the 0.05 significance level (Newman–Kuels multiple comparisons test).
b) Difference in average day 3 fragmentation in transferred embryos in group 2 vs group 3 is not significant.
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 56
respectively, overall; 6.6 ⫾ 1.7 vs 7.3 ⫾ 1.3 cells,
respectively, in transferred embryos). Pregnancy rate,
however, was significantly lower following transfer
of type II embryos than type III embryos (32.9 vs
49%, respectively).
Compared to embryos with all other patterns of
fragmentation, those with type IV fragmentation
had fewer cells (5.2 ⫾ 1.4) on day 3 and led to far
fewer implantations and pregnancies. Fluorescence
in situ hybridization (FISH) analysis has shown a
significantly higher incidence of chromosomal
abnormality in embryos with type IV fragmenta-
tion than those with types I, II, or III fragmentation
(M Alikani, G Tomkin and S Munné, unpublished
data).
The same fragmentation pattern classification
system
21
was adopted by others
29
who studied the
incidence of different patterns among transferred
embryos in pregnant and non-pregnant cycles.
Prior to embryo transfer, the zona pellucida in all
embryos was partially opened with acidified
Tyrode’s solution but fragments were not removed.
The degree of fragmentation was not noted in these
embryos. The results showed that in pregnancy
cycles, 48% of transferred embryos had type I frag-
mentation, while in non-pregnant cycles, a gener-
ally lower incidence of type I and a generally higher
incidence of type II fragmentation had occurred.
Implantation failed in seven cases in which embryos
with fragmentation types III and IV were transferred
exclusively. The latter outcome is not consistent
with our own experience with these fragmenta-
tion patterns, but the discrepancy may be partly
explained by the very low number of observations
in the study of Desai et al.
29
Moreover, since the
classification of the patterns still has an element of
subjectivity, observer variation may also account for
these differences.
In another interesting study,
27
embryos with more
than 25% fragmentation showed very low viability
(0.8%). When cell number, degree of fragmenta-
tion, and cell asymmetry (the latter defined as ‘none,
some, and severe’) were considered together, there
was a measurable negative impact of asymmetry on
viability of 8-cell embryos, regardless of the degree
of fragmentation (⬍10% or 10–25%). Transfer of
7-cell and ⬍7-cell embryos with severe asymmetry
led to complete failure of implantation.
27
Collectively, these data point to a definition of
‘top quality’ embryos as those with less than 20%
fragmentation, at least seven blastomeres on day 3
of development
30,31
, little asymmetry (attributable
to asynchronous division of cells), and no major
size discrepancy attributable to fragmentation or
uneven division of cells.
21,27,32
The impact of fragmentation on neonatal out-
come is less clear. One study
33
has suggested that
transfer of embryos with 25% to ⬎50% fragmenta-
tion leads to significantly higher rates of fetal abnor-
malities than transfer of embryos with ⬍25%
fragmentation. Four minor malformations occurred
among the 180 children born following 309 transfers
in the ⬍25% fragmentation group. In another group
consisting of 75 transfers that included embryos
with 25–50% fragmentation, one case of trisomy 21
and one of fibroma were seen among 13 newborns.
Among 19 children born following 76 transfers that
included embryos with ⬎50% fragmentation, two
cases of trisomy 18, one of hydrocephalus with anal
atresia, and one of hydrocele were found.
33
Several aspects of this study are puzzling. For
example, the large proportion of transfers that
reportedly included embryos with ⬎50% fragmen-
tation (75/460 or 16%) brings into question the
accuracy of the fragmentation estimates. In our data-
base of 3322 transfers homogeneous with respect to
the degree of fragmentation, only 1.3% (43/3322)
had embryos with ⬎35% fragmentation. The total
number of embryos with 50% or more fragmenta-
tion within this group was 25. When the entire
database was considered, 96 of 25 372 (0.38%)
transferred embryos had 50% or more fragmenta-
tion. These figures reflect the deliberate exclusion of
such embryos from transfer and the relatively low
frequency with which such extensive fragmentation
occurs in the first 2–3 days of culture (5893/79 936
or 7.4%).
Another point of debate is the implied associa-
tion of aneuploidy – in this case, trisomies – with
fragmentation. So far, such an association has not
been established by chromosomal analysis of
large numbers of IVF embryos. The incidence of
ORIGINS AND CONSEQUENCES OF FRAGMENTATION
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 57

HUMAN PREIMPLANTATION EMBRYO SELECTION
aneuploidy (single chromosome loss or gain) does
not seem to be related to embryo morphology, but
to maternal age; the predominant abnormalities
among fragmented embryos are polyploidy and
extensive mosaicism which are often incompatible
with development to term.
34–37
The question of a potential relationship between
early embryo morphology and structural abnor-
malities in fetuses should perhaps be more carefully
examined in larger series of cases where several
morphological parameters have been well defined
and thoroughly examined. In the study of Ebner
et al.,
33
the embryos were evaluated by one static
observation on day 2 of development, at a magnifi-
cation of ⫻200.
We have not systematically studied neonatal
outcome following transfer of fragmented embryos.
Although it has been suggested that embryo mor-
phology on the day of transfer does not predict first
trimester pregnancy loss,
38
our data indicate a high
incidence of early pregnancy loss in cases where
extensively fragmented embryos were transferred.
Among 43 cases in which all embryos had ⬎35%
fragmentation at the time of evaluation (before
fragment removal), 13 pregnancies resulted, but
only three babies were born (two male and one
female). Seven pregnancies were classified as bio-
chemical, having shown at least three consecutive
rises in hCG levels but having failed to show a
gestational sac with or without fetal heart activity.
Three other pregnancies were lost between 7 and 9
weeks of gestation, after detection of a gestational
sac. This is an early loss rate of 77% in an IVF pro-
gram where the overall loss rates after a positive
hCG pregnancy test and detection of cardiac
activity are approximately 25% and 11%, respec-
tively. Such an extraordinarily high loss rate is an
argument against transfer of embryos with exten-
sive fragmentation (as also argued in ref. 33).
Cytogenetic analysis was not performed on the
aborted fetuses, so it is not known for certain
whether chromosomal or other abnormalities were
the cause of spontaneous abortion. However, such
abnormalities have been found in 50–65% of very
early pregnancy losses following IVF.
39,40
Moreover,
transcervical embryoscopy (direct visualization of
the fetus) combined with cytogenetic analysis of
missed abortions has shown chromosomal abnor-
malities in 75%, and normal karyotype but structural
defects in 18% of the cases.
41
The observed incidence of implantation failure
of embryos with extensive fragmentation reflects a
persistent negative effect of fragmentation on
embryo development in utero associated with frag-
mentation. The question is whether these effects are
manifested during prolonged culture in vitro?
THE IMPACT OF FRAGMENTATION ON
PREIMPLANTATION DEVELOPMENT
The relationship between embryo morphology
and viability has become more evident following
assessment of embryos in elective single embryo
transfers.
38
It is also of interest that a large study
including a data set of 10 000 embryo transfers
42
recently concluded that embryo quality (assessed on
day 2) is the best predictor of pregnancy (following
day 2 transfer) even when considered together with
16 other possible treatment cycle variables that
included maternal age, duration and type of infer-
tility, ovarian stimulation protocol, number of IVF
attempts, progesterone level at hCG administration,
sperm count, motility and morphology, number of
retrieved and mature oocytes, number of embryos,
and number of transferred embryos. The highest
embryo quality score was assigned to 4-cell embryos
with no fragmentation or fragmentation ⬍20% and
evenly sized cells. Thus the suggestion that embryo
morphology, including fragmentation, has no cor-
relation with blastocyst formation or quality during
extended culture
43,44
seems both counter intuitive
and generally unsupported.
Our assessment of the impact of fragmentation
on blastulation in over 1200 surplus embryos
45
showed that with increasing fragmentation (0–15%
vs ⬎15%), fewer embryos compacted, cavitated,
and formed normal blastocysts. When fragmenta-
tion exceeded 35%, all processes were severely
compromised, even though in some cases, fragments
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 58
ORIGINS AND CONSEQUENCES OF FRAGMENTATION
were excluded in the perivitelline space by the
embryo (see Figure 6.4). When the origin of all the
blastocysts that were selected for transfer (i.e. the
best available embryos) was considered, we found
that nearly 90% had developed from embryos
with ⱕ15% fragmentation on day 3.
Interestingly, fragmentation has been found to
influence allocation of cells during differentiation.
46
According to this study, increasing fragmentation
resulted not only in reduced blastocyst formation
but also in lower cell numbers when blastocysts did
form. Moreover, in the case of minimal to moderate
fragmentation, the reduction in cell number was
apparently confined to the trophectoderm, while a
steady number of inner cell mass cells was main-
tained. However, when fragmentation exceeded
25%, cell numbers in both lineages were reduced.
46
These results are difficult to reconcile with the
suggestion that blastocyst viability on day 5 is not
affected by the degree of fragmentation on day 3 of
development.
27
Perhaps this can be partly attributed
to the relatively small groups of patients and
embryos examined.
27
In the case of embryos with
⬎25% fragmentation, for instance, only five blasto-
cysts (two of which implanted) and possibly two
patients were included in the study.
27
Thus the
study’s conclusion cannot be considered definitive.
Observational studies also suggest that the pat-
tern of fragmentation has an influence on blastula-
tion. The presence of large scattered fragments in
embryos with uneven cell size is associated with a
significant reduction in normal blastocyst forma-
tion compared with the other patterns.
45
The
reduced ability to form morphologically normal
blastocysts often becomes obvious at compaction,
which normally occurs on day 4 of development in
the human.
47
‘Regional’ or partial compaction,
with exclusion of a number of cells and fragments
from the morula, occurs frequently in fragmented
embryos (Figure 6.4).
In our study,
45
nearly half of normally compact-
ing embryos formed blastocysts, but this incidence
was reduced to only one third in regionally com-
pacted embryos and to 10% in embryos that did
not show compaction on day 4 in culture. These
data demonstrate that evidence of compaction on
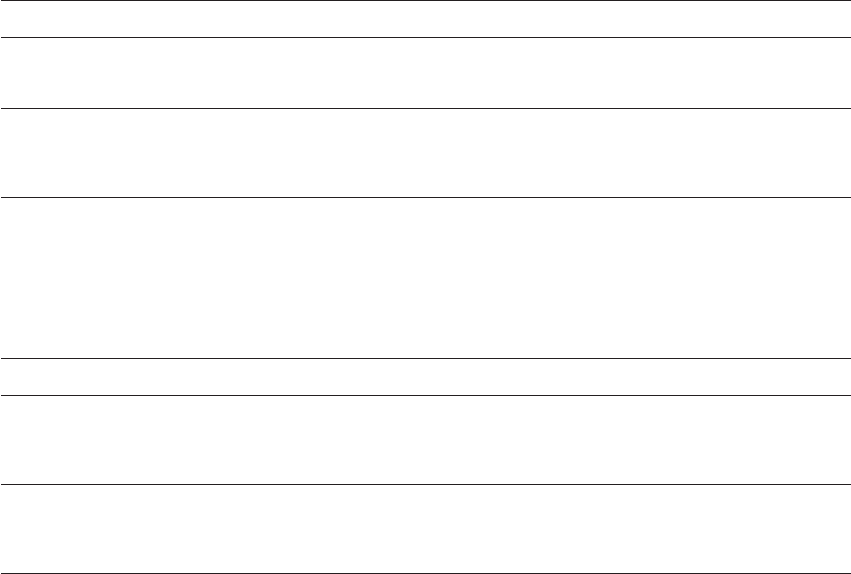
ABCDE
FGHI
M
J
Figure 6.4 Serial 4 micron thick optical sections through a day 5 human embryo, obtained on the laser scanning confocal
microscope, showing ‘regional’ compaction. The excluded cells and fragments (A)–(E) as well as a small morula (M in (I)) are visible.
The embryo has been stained with antibodies against E-cadherin (green). The nuclei are stained with propidium iodide (red).
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 59
HUMAN PREIMPLANTATION EMBRYO SELECTION
day 4 is highly prognostic for normal blastocyst
formation.
The relationship between fragmentation pat-
tern and blastocyst formation was assessed in
another study,
48
in which the progress of 1566
surplus embryos was monitored until day 5 of
development. Embryos with no fragmentation, or
with type I fragmentation
21
had a higher blastocyst
formation rate than embryos with type II or III
fragmentation, while embryos that were assessed
to have type IV fragmentation failed to form any
normal blastocysts.
48
Based on the fragmentation patterns described
by Antczak and Van Blerkom,
22
the majority of
cleavage stage embryos with types II (multiple layers
of fragments with cell size reduction) or III (com-
plete fragmentation of one blastomere) fragmenta-
tion continued to divide beyond the 4-cell stage,
and about half reached the blastocyst stage, albeit in
some cases with a delay of 12–24 hours. It was also
observed that fragmentation at the 8-cell stage did
not preclude development to the blastocyst stage,
suggesting that the occurrence of fragmentation
early in development was more likely to be detri-
mental to development. How does fragmentation
interfere with normal embryonic development in
vitro or in vivo?
THE IMPACT OF FRAGMENTS ON THE
FRAGMENTING BLASTOMERE AND
ITS SISTER BLASTOMERES
Cytoplasmic blebs that emerge often during the
process of division can become ‘reincorporated’
into blastomeres.
19,49
Furthermore, evidence sug-
gests that small apical fragments may lyze, while
larger fragments may swell and burst, possibly due
to depletion of mitochondria and ATP stores in
these structures.
19
However, most fragments, once
they are clearly formed, obviously persist through-
out the early cleavage stages and it would be incor-
rect to imply that all fragments are transitory
structures.
Fragments may be excluded during compaction
or even found in the blastocoel cavity of the
blastocyst. According to one study, they are not
static and can ‘move in concert’ with the underlying
blastomeres.
19
Clearly, fragmentation can affect the size of the
fragmenting blastomeres, albeit not always appre-
ciably. It has been shown that mean blastomere size
decreases significantly with increasing degree of
fragmentation.
50
Highly fragmented embryos show
a 43–67% reduction in blastomere volume. It is
possible that the reduction in size, if substantial
can lead to arrest of the affected blastomeres.
21
Examination of individual ‘cells’ from fragmented
embryos suggests that ‘cells’ ⬍45 m in diameter
in day 2 embryos and those ⬍40 m in day 3
embryos should be considered fragments since they
never contain a nucleus and only seldom contain
chromosomal DNA.
51
It has been suggested that certain patterns of
fragmentation can result in ‘partial or near total
loss’ of several regulatory proteins from specific
blastomeres, with developmental consequences for
both the affected blastomere and the embryo as a
whole.
22
The products of cell lysis or degeneration might
cause deterioration of neighboring blastomeres or
interfere otherwise in normal embryo development.
This appears to be the case in the mouse, since the
presence of deliberately lyzed cells among other
viable cells reduces the incidence of blastocyst
hatching, and removal of the lyzed cells restores
hatching ability.
52
At the same time, preliminary
evidence suggested that removal of cryo-damaged
cells from frozen-thawed human embryos was not
only feasible but potentially beneficial.
52
This tech-
nique has since been shown in clinical trials to
improve pregnancy outcome.
53,54
We investigated the question of fragment ‘toxic-
ity’ in a mouse model,
55
taking advantage of mouse
blastomere totipotency at first cleavage.
56
Two-cell
embryos were dissociated (generating two blas-
tomeres), and each blastomere (or half-embryo)
was placed in a host zona pellucida (ZP; mouse,
bovine, or human) either alone or aggregated with
mouse or human egg/embryo fragments. The
development of the half embryo-fragment aggre-
gates and the control half embryos was monitored
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 60
ORIGINS AND CONSEQUENCES OF FRAGMENTATION
over the course of the following 3–4 days in
culture. The fragments were not spontaneously
generated by the half embryos, and therefore the
experiments measured the impact of fragments or
the microenvironment created by their presence
on division of the original single blastomere (or
half embryo) and its descendent cells. The pres-
ence of large numbers of fragments (in bovine or
human ZP) appeared to be disruptive to develop-
ment in some cases, but the overall results suggest
that at least in the absence of an intact ZP, mouse
blastomeres are neither overtly sensitive to close
physical association with heterologous (often
degenerative) cytoplasmic fragments nor respon-
sive to the intrazonal microenvironment created
by them (Figure 6.5).
The loss of fragments through large slits in the
zona pellucida presented a problem in these experi-
ments and may have affected the outcome, and
therefore the results should be interpreted with
caution. However, mouse embryos are not nega-
tively affected by exposure to cytoplasts, either
removed from the zygote and reinserted in the
perivitelline space, generated by enucleation of two
blastomeres of an 8-cell embryo,
57
or by enucleation
of one or two blastomeres of a 2-cell embryo.
58
Thus,
in the mouse, there is no clear evidence of fragment
‘toxicity’ except under extreme circumstances.
In the human, the picture is somewhat different.
Clinical data suggest that removal of fragments
from some fragmented embryos prior to intrauter-
ine transfer leads to higher frequency of implanta-
tion. In the past 10 years, we have routinely used
microsurgery to remove the majority of cytoplasmic
fragments when fragmented embryos were to be
transferred. This was initially based on finding a 4%
overall increase in implantation rate when zona
drilling (assisted hatching) and fragment removal
were applied simultaneously, in comparison with
embryos which were zona-drilled only.
59
The analy-
sis of a larger series of cases provided more support
for the suggestion that the removal of the fragments
contributes to the survival of fragmented embryos
following intrauterine transfer: embryos with
10–35% fragmentation showed similar implanta-
tion rates, and a very low implantation rate (6%)
occurred only when fragmentation exceeded ⬎35%
before fragment removal.
21
In a more recent study,
60
327 non-donor cycles
in which embryos with ⬎10% fragmentation were
subjected to assisted hatching and microsurgical
fragment removal prior to transfer were retrospec-
tively evaluated. Three groups were identified:
74 cycles in which at least one embryo required
fragment removal, 39 cycles in which all embryos
were subjected to this procedure, and a control
group of 234 cycles that included embryos with
⬍10% fragmentation subjected to assisted hatching
only. The data showed that the rates of implanta-
tion, live birth, spontaneous abortion, and fetal
abnormalities in the first two groups were equiva-
lent to those in the control group, suggesting a
beneficial effect of fragment removal on pregnancy
outcome.
Thus it appears that the reduced viability of frag-
mented human embryos is at least partly attributa-
ble to the presence of the fragments per se. However,
the beneficial effects of fragment removal are obvi-
ously limited. A recent analysis of a larger set of
homogeneous transfers (described above) suggests
that even after removal of fragments, the implanta-
tion rate of embryos with ⬎15% but ⬍35% frag-
mentation is still lower than that of embryos with
0–15% fragmentation (32% vs 18%, respectively).
Moreover, removal of fragments from embryos with
minimal fragmentation (0–15%) or from those in
which fragmentation exceeds 35%, has little or no
influence on the transfer outcome in a majority of
cases. In the case of 0–15% fragmentation, viability is
not substantially reduced in the first place, and in
the case of ⬎35% fragmentation even though removal
of fragments may occasionally lead to survival of the
affected embryo (as mentioned above), it is unlikely
to address the underlying cause of the abnormality
or its associated developmental problems.
Further insight into the possible impact of frag-
ments on the neighboring cells was provided by
examining the developmental capacity of blasto-
meres isolated from fragmented embryos. This was
done either by individual culture of these
blastomeres
61,62
or their artificial aggregation in a
host zona pellucida.
61
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 61
HUMAN PREIMPLANTATION EMBRYO SELECTION
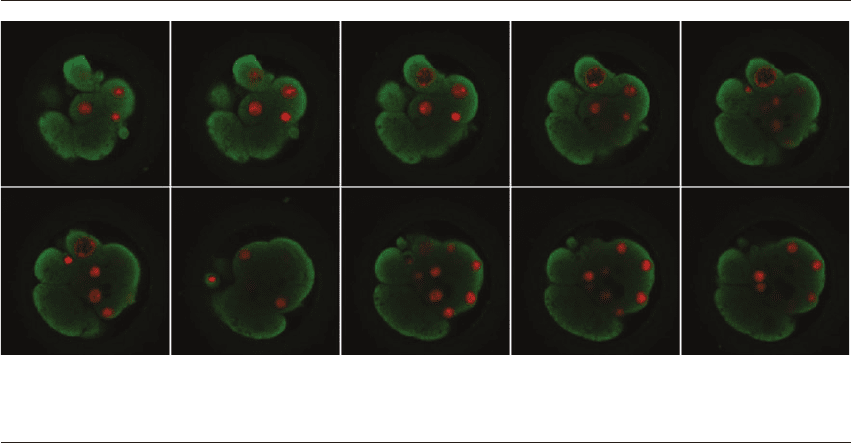
Day 2
Aa3a4a5
Bb3b4b5
Cc3c4c5
Dd3d4d5
Ee3e4e5
Day 3 Day 4 Day 5
Figure 6.5 (Continued)
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 62
In the first series of experiments, nucleated
blastomeres and fragments were biopsied from
discarded embryos with 1–10 cells and 20–75%
(primarily type IV) fragmentation on day 3 of
development. Roughly 40% of these arrested when
placed in culture in isolation but the remaining 60%
divided during the course of culture. Of those that
divided, a substantial proportion went on to form a
‘cavity’ and blastulate, albeit with fewer than four
cells. These observations suggest that the mixing of
potentially normal and abnormal cells and cell frag-
ments may reduce the development potential of the
normal cells by reducing the likelihood of normal
blastulation.
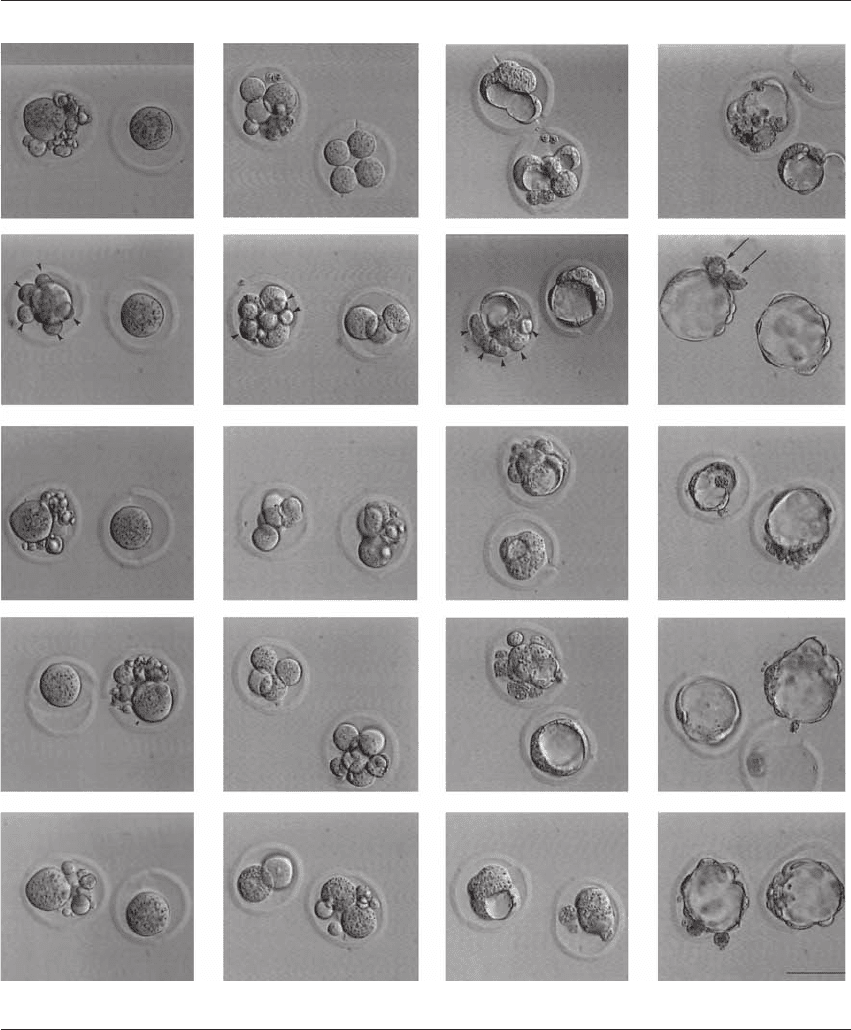
The second set of experiments lends support
to this proposal: non-viable embryos with exten-
sive fragmentation and other abnormalities were
disaggregated and blastomeres of normal appear-
ance from two or more embryos were combined
into ‘chimeric’ aggregates.
61
Roughly one-third of
these aggregates formed blastocysts with distinct
inner cell masses and relatively high cell numbers,
ranging from 31 to 56 cells (Figure 6.6). Of these
cells, 52–90% were diploid. Chaotic mosaicism was
the most common abnormality found in these
embryos. This outcome demonstrates the develop-
mental potential and regulatory capacity of a pro-
portion of cells derived from non-viable embryos,
again suggesting that poor development of the latter
is at least partly attributable to the presence of the
fragments and/or abnormal nucleated cells. Does
the presence of fragments influence other aspects of
early development?
THE IMPACT OF FRAGMENTS ON CELL–CELL
INTERACTIONS/EMBRYO ORGANIZATION
It has been speculated that disruption of the spatial
arrangement of cells through fragmentation may
be a cause for reduced cell–cell contact and com-
munication.
21
Transmission electron microscopy
does not support this proposal. According to Van
Blerkom et al.
19
(2001), although ‘lysed, ‘prelytic’
and intact fragments interposed between blasto-
meres seemed to prevent close apposition of adja-
cent plasma membranes’.
19
Serial section analysis of
images ‘demonstrated that these separated zones
were focal and that close contact between opposed
plasma membranes existed in other regions of these
blastomeres.’ Whether this is a general phenomenon
or one that is restricted to certain cases of fragmen-
tation remains to be seen.
It is nonetheless clear that during the course of
culture in vitro, fragmented human embryos
often fail to compact or they undergo abnormal
compaction, excluding a number of cells and frag-
ments (Figures 6.3–6.5).
45
We investigated this phenomenon further by
examining the localization of E-cadherin, a vital cell
adhesion protein, in a large number of non-viable
human embryos with normal and abnormal mor-
phology.
63
In all other mammalian species studied
so far, E-cadherin is actively relocated in the course
of embryogenesis.
64,65
Relocation first occurs at the
time of compaction, and involves the cells that
form the outer layer of the embryo. In these cells,
ORIGINS AND CONSEQUENCES OF FRAGMENTATION
Figure 6.5 The development of experimental and control half embryos from day 2 through day 5 in culture.In panel A, Cavitation
and blastulation appear to be abnormal in both control and the experimental half embryos. In panel B (second row from top), on
day 2 of development, five large fragments (arrowheads) aggregated with one blastomere are visible, while the sister blastomere from
the same 2-cell embryo is seen in a host zona pellucida alone. One day later, on day 3 of development (b3), the five fragments can be
seen surrounding three blastomeres (1⫻1/4 and 2⫻1/8). The control half embryo has exactly the same number of cells (1⫻1/4 and
2⫻1/8). On day 4 (b4), the fragments in the experimental half embryo have moved to one side of a compacted mass that has begun
to cavitate. The control half embryo has also compacted and cavitated but appears better organized. By day 5, both half embryos have
formed blastocysts. The fragments (arrows), now degenerated, are loosely attached to the experimental half embryo. Development of
control and experimental blastomeres depicted in panels C, D, and E is comparable. Scale bar is 50 m.
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 63
HUMAN PREIMPLANTATION EMBRYO SELECTION
E-cadherin is transported from the cytoplasm to the
cell membrane in areas of contact between cells.
This relocation is a preliminary to the formation of
junctional complexes between the trophectodermal
cells, which are responsible for the integrity of the
blastocyst.
It is therefore reasonable to expect that frag-
mentation may be associated with the failure of
proper expression, localization, or distribution of
E-cadherin, all of which are required for normal
compaction. Laser scanning microscopy (LSM)
images suggest that the characteristic distribution
pattern of E-cadherin is perturbed and erratic in
abnormally cleaving human embryos (Figure 6.7).
Although it is not clear whether the erratic distribu-
tion is a cause or an effect of abnormal develop-
ment, including fragmentation, these disturbances
can nonetheless lead to failure of compaction,
which in turn leads to failed or abortive blastula-
tion. Moreover, the presence of non-interacting cells
and fragments and interactive cells in the same
embryo may contribute to the problem by disrupt-
ing cell signaling processes that are mediated by E-
cadherin.
It is therefore plausible that fragmentation,
regardless of its underlying cause, disrupts early
development via a mechanism that involves cell–cell
interaction or communication.
A
DE
BC
A⬘ B⬘ C⬘
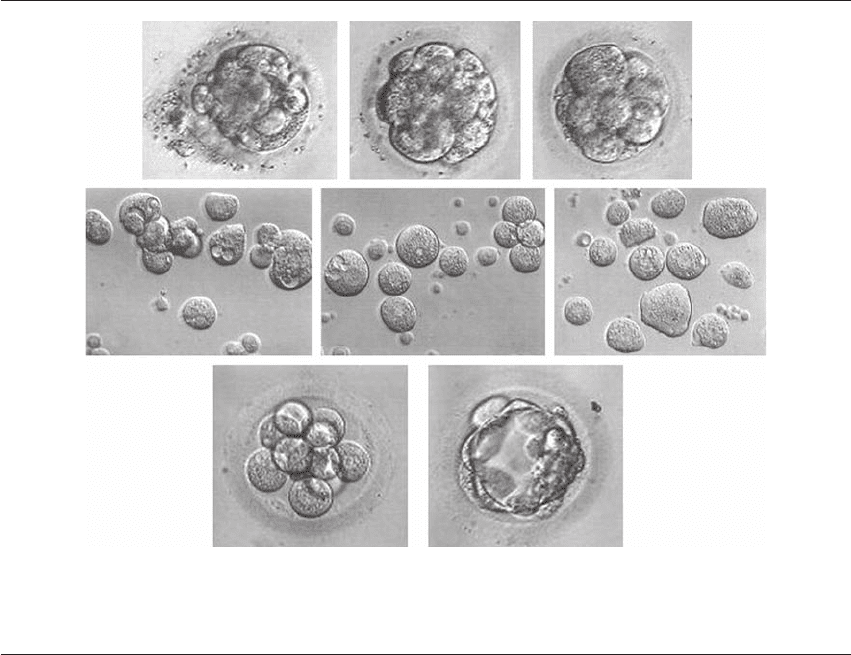
Figure 6.6 Development of a human aggregate. (A–C) Three discarded non-viable embryos on day 3 of development. (A⬘–C⬘)
Dissociated cells of the respective non-viable day 3 human embryos in A–C, comprising mononucleated, multinucleated, and
anucleate blastomeres/fragments. (D) Eleven of the mononucleated cells from the three embryos were used on day 3 to construct an
aggregate. (E) Following 2 days of culture, the aggregate formed a blastocyst.
HPE_Chapter06.qxp 7/13/2007 4:46 PM Page 64
ORIGINS AND CONSEQUENCES OF FRAGMENTATION
A
ab
cd
ab
cd
B
C
M
D
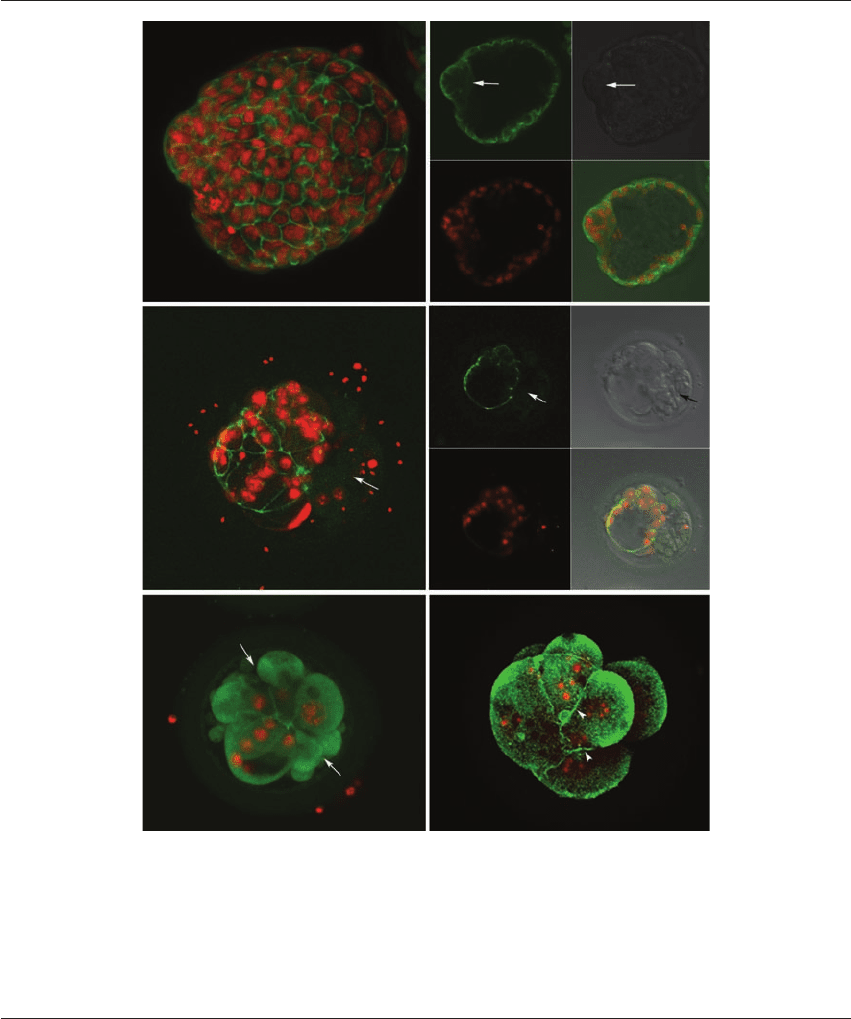
Figure 6.7 The distribution of E-cadherin (green) in human embryos at different stages of development. (A) Hatched day 7 blasto-
cyst from a normally fertilized egg. The cells of the trophectoderm (both polar and mural) show an intense ‘belt’ of fluorescence
indicating localization of E-cadherin in the membranes. Cells within the inner cell mass (arrows in panels a and b) show diffuse cyto-
plasmic E-cadherin. (B) An embryo showing abnormal blastulation and ‘belt’ staining of trophoectoderm cell membranes; many
excluded cells and fragments which do not show any staining are visible (arrows in panels B, a, and b). (C) A day 5 human embryo
with excluded cells and fragments (arrows) and a small morula (M) consisting of about 6 cells. (D) Compacting 8-cell embryo show-
ing weak staining in areas of cell–cell contact (arrowheads). The images in A–D are projections of multiple 4–5 m thick optical
sections obtained on the laser scanning confocal microscope. Images in a–d are single optical sections.
HPE_Chapter06.qxp 7/13/2007 4:47 PM Page 65