Columbia. Accident investigation board
Подождите немного. Документ загружается.


1 0
R e p o r t V o l u m e I A u g u s t 2 0 0 3
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 1
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
R e p o r t V o l u m e I A u g u s t 2 0 0 3
The Columbia Accident Investigation Boardʼs independent
investigation into the tragic February 1, 2003, loss of the
Space Shuttle Columbia and its seven-member crew lasted
nearly seven months and involved 13 Board members,
approximately 120 Board investigators, and thousands
of NASA and support personnel. Because the events that
initiated the accident were not apparent for some time,
the investigationʼs depth and breadth were unprecedented
in NASA history. Further, the Board determined early in
the investigation that it intended to put this accident into
context. We considered it unlikely that the accident was a
random event; rather, it was likely related in some degree
to NASAʼs budgets, history, and program culture, as well
as to the politics, compromises, and changing priorities of
the democratic process. We are convinced that the manage-
ment practices overseeing the Space Shuttle Program were
as much a cause of the accident as the foam that struck the
left wing. The Board was also inuenced by discussions
with members of Congress, who suggested that this nation
needed a broad examination of NASAʼs Human Space Flight
Program, rather than just an investigation into what physical
fault caused Columbia to break up during re-entry.
Findings and recommendations are in the relevant chapters
and all recommendations are compiled in Chapter 11.
Volume I is organized into four parts: The Accident; Why
the Accident Occurred; A Look Ahead; and various appendi-
ces. To put this accident in context, Parts One and Two begin
with histories, after which the accident is described and then
analyzed, leading to ndings and recommendations. Part
Three contains the Boardʼs views on what is needed to im-
prove the safety of our voyage into space. Part Four is refer-
ence material. In addition to this rst volume, there will be
subsequent volumes that contain technical reports generated
by the Columbia Accident Investigation Board and NASA,
as well as volumes containing reference documentation and
other related material.
PART ONE: THE ACCIDENT
Chapter 1 relates the history of the Space Shuttle Program
before the Challenger accident. With the end looming for
the Apollo moon exploration program, NASA unsuccess-
fully attempted to get approval for an equally ambitious
(and expensive) space exploration program. Most of the
proposed programs started with space stations in low-Earth
orbit and included a reliable, economical, medium-lift
vehicle to travel safely to and from low-Earth orbit. After
many failed attempts, and nally agreeing to what would
be untenable compromises, NASA gained approval from the
Nixon Administration to develop, on a xed budget, only
the transport vehicle. Because the Administration did not ap-
prove a low-Earth-orbit station, NASA had to create a mis-
sion for the vehicle. To satisfy the Administrationʼs require-
ment that the system be economically justiable, the vehicle
had to capture essentially all space launch business, and to
do that, it had to meet wide-ranging requirements. These
sometimes-competing requirements resulted in a compro-
mise vehicle that was less than optimal for manned ights.
NASA designed and developed a remarkably capable and
resilient vehicle, consisting of an Orbiter with three Main
Engines, two Solid Rocket Boosters, and an External Tank,
but one that has never met any of its original requirements
for reliability, cost, ease of turnaround, maintainability, or,
regrettably, safety.
Chapter 2 documents the nal ight of Columbia. As a
straightforward record of the event, it contains no ndings or
recommendations. Designated STS-107, this was the Space
Shuttle Programʼs 113th ight and Columbiaʼs 28th. The
ight was close to trouble-free. Unfortunately, there were no
indications to either the crew onboard Columbia or to engi-
neers in Mission Control that the mission was in trouble as
a result of a foam strike during ascent. Mission management
failed to detect weak signals that the Orbiter was in trouble
and take corrective action.
Columbia was the rst space-rated Orbiter. It made the Space
Shuttle Programʼs rst four orbital test ights. Because it was
the rst of its kind, Columbia differed slightly from Orbiters
Challenger, Discovery, Atlantis, and Endeavour. Built to an
earlier engineering standard, Columbia was slightly heavier,
and, although it could reach the high-inclination orbit of the
International Space Station, its payload was insufcient to
make Columbia cost-effective for Space Station missions.
Therefore, Columbia was not equipped with a Space Station
docking system, which freed up space in the payload bay for
longer cargos, such as the science modules Spacelab and
SPACEHAB. Consequently, Columbia generally ew sci-
ence missions and serviced the Hubble Space Telescope.
STS-107 was an intense science mission that required the
seven-member crew to form two teams, enabling round-
the-clock shifts. Because the extensive science cargo and
its extra power sources required additional checkout time,
the launch sequence and countdown were about 24 hours
longer than normal. Nevertheless, the countdown proceeded
as planned, and Columbia was launched from Launch Com-
plex 39-A on January 16, 2003, at 10:39 a.m. Eastern Stan-
dard Time (EST).
At 81.7 seconds after launch, when the Shuttle was at about
65,820 feet and traveling at Mach 2.46 (1,650 mph), a large
piece of hand-crafted insulating foam came off an area
where the Orbiter attaches to the External Tank. At 81.9
seconds, it struck the leading edge of Columbiaʼs left wing.
This event was not detected by the crew on board or seen
by ground support teams until the next day, during detailed
reviews of all launch camera photography and videos. This
foam strike had no apparent effect on the daily conduct of
the 16-day mission, which met all its objectives.
The de-orbit burn to slow Columbia down for re-entry
into Earthʼs atmosphere was normal, and the ight prole
throughout re-entry was standard. Time during re-entry is
REPORT SYNOPSIS

1 2
R e p o r t V o l u m e I A u g u s t 2 0 0 3
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 3
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
R e p o r t V o l u m e I A u g u s t 2 0 0 3
measured in seconds from “Entry Interface,” an arbitrarily
determined altitude of 400,000 feet where the Orbiter be-
gins to experience the effects of Earthʼs atmosphere. Entry
Interface for STS-107 occurred at 8:44:09 a.m. on February
1. Unknown to the crew or ground personnel, because the
data is recorded and stored in the Orbiter instead of being
transmitted to Mission Control at Johnson Space Center, the
rst abnormal indication occurred 270 seconds after Entry
Interface. Chapter 2 reconstructs in detail the events lead-
ing to the loss of Columbia and her crew, and refers to more
details in the appendices.
In Chapter 3, the Board analyzes all the information avail-
able to conclude that the direct, physical action that initiated
the chain of events leading to the loss of Columbia and her
crew was the foam strike during ascent. This chapter re-
views ve analytical paths – aerodynamic, thermodynamic,
sensor data timeline, debris reconstruction, and imaging
evidence – to show that all ve independently arrive at the
same conclusion. The subsequent impact testing conducted
by the Board is also discussed.
That conclusion is that Columbia re-entered Earthʼs atmo-
sphere with a pre-existing breach in the leading edge of its
left wing in the vicinity of Reinforced Carbon-Carbon (RCC)
panel 8. This breach, caused by the foam strike on ascent,
was of sufcient size to allow superheated air (probably ex-
ceeding 5,000 degrees Fahrenheit) to penetrate the cavity be-
hind the RCC panel. The breach widened, destroying the in-
sulation protecting the wingʼs leading edge support structure,
and the superheated air eventually melted the thin aluminum
wing spar. Once in the interior, the superheated air began to
destroy the left wing. This destructive process was carefully
reconstructed from the recordings of hundreds of sensors in-
side the wing, and from analyses of the reactions of the ight
control systems to the changes in aerodynamic forces.
By the time Columbia passed over the coast of California
in the pre-dawn hours of February 1, at Entry Interface plus
555 seconds, amateur videos show that pieces of the Orbiter
were shedding. The Orbiter was captured on videotape dur-
ing most of its quick transit over the Western United States.
The Board correlated the events seen in these videos to
sensor readings recorded during re-entry. Analysis indi-
cates that the Orbiter continued to y its pre-planned ight
prole, although, still unknown to anyone on the ground or
aboard Columbia, her control systems were working furi-
ously to maintain that ight prole. Finally, over Texas, just
southwest of Dallas-Fort Worth, the increasing aerodynamic
forces the Orbiter experienced in the denser levels of the at-
mosphere overcame the catastrophically damaged left wing,
causing the Orbiter to fall out of control at speeds in excess
of 10,000 mph.
The chapter details the recovery of about 38 percent of the
Orbiter (some 84,000 pieces) and the reconstruction and
analysis of this debris. It presents ndings and recommenda-
tions to make future Space Shuttle operations safer.
Chapter 4 describes the investigation into other possible
physical factors that may have contributed to the accident.
The chapter opens with the methodology of the fault tree
analysis, which is an engineering tool for identifying every
conceivable fault, then determining whether that fault could
have caused the system in question to fail. In all, more than
3,000 individual elements in the Columbia accident fault
tree were examined.
In addition, the Board analyzed the more plausible fault sce-
narios, including the impact of space weather, collisions with
micrometeoroids or “space junk,” willful damage, ight crew
performance, and failure of some critical Shuttle hardware.
The Board concludes in Chapter 4 that despite certain fault
tree exceptions left “open” because they cannot be conclu-
sively disproved, none of these factors caused or contributed
to the accident. This chapter also contains ndings and rec-
ommendations to make Space Shuttle operations safer.
PART TWO: WHY THE ACCIDENT OCCURRED
Part Two, “Why the Accident Occurred,” examines NASAʼs
organizational, historical, and cultural factors, as well as
how these factors contributed to the accident.
As in Part One, Part Two begins with history. Chapter 5
examines the post-Challenger history of NASA and its
Human Space Flight Program. A summary of the relevant
portions of the Challenger investigation recommendations
is presented, followed by a review of NASA budgets to indi-
cate how committed the nation is to supporting human space
ight, and within the NASA budget we look at how the
Space Shuttle Program has fared. Next, organizational and
management history, such as shifting management systems
and locations, are reviewed.
Chapter 6 documents management performance related to
Columbia to establish events analyzed in later chapters. The
chapter begins with a review of the history of foam strikes on
the Orbiter to determine how Space Shuttle Program managers
rationalized the danger from repeated strikes on the Or-
biterʼs Thermal Protection System. Next is an explanation
of the intense pressure the program was under to stay on
schedule, driven largely by the self-imposed requirement to
complete the International Space Station. Chapter 6 then re-
lates in detail the effort by some NASA engineers to obtain
additional imagery of Columbia to determine if the foam
strike had damaged the Orbiter, and how management dealt
with that effort.
In Chapter 7, the Board presents its view that NASAʼs or-
ganizational culture had as much to do with this accident
as foam did. By examining safety history, organizational
theory, best business practices, and current safety failures,
the report notes that only signicant structural changes to
NASAʼs organizational culture will enable it to succeed.
This chapter measures the Shuttle Programʼs practices
against this organizational context and nds them wanting.
The Board concludes that NASAʼs current organization
does not provide effective checks and balances, does not
have an independant safety program, and has not dem-
onstrated the characteristics of a learning organization.
Chapter 7 provides recommendations for adjustments in
organizational culture.
1 2
R e p o r t V o l u m e I A u g u s t 2 0 0 3
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 3
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
R e p o r t V o l u m e I A u g u s t 2 0 0 3
Chapter 8, the nal chapter in Part Two, draws from the
previous chapters on history, budgets, culture, organization,
and safety practices, and analyzes how all these factors con-
tributed to this accident. The chapter opens with “echoes of
Challenger” that compares the two accidents. This chapter
captures the Boardʼs views of the need to adjust manage-
ment to enhance safety margins in Shuttle operations, and
reafrms the Boardʼs position that without these changes,
we have no condence that other “corrective actions” will
improve the safety of Shuttle operations. The changes we
recommend will be difcult to accomplish – and will be
internally resisted.
PART THREE: A LOOK AHEAD
Part Three summarizes the Boardʼs conclusions on what
needs to be done to resume our journey into space, lists
signicant observations the Board made that are unrelated
to the accident but should be recorded, and provides a sum-
mary of the Boardʼs recommendations.
In Chapter 9, the Board rst reviews its short-term recom-
mendations. These return-to-ight recommendations are the
minimum that must be done to essentially x the problems
that were identied by this accident. Next, the report dis-
cusses what needs to be done to operate the Shuttle in the
mid-term, 3 to 15 years. Based on NASAʼs history of ignor-
ing external recommendations, or making improvements
that atrophy with time, the Board has no condence that the
Space Shuttle can be safely operated for more than a few
years based solely on renewed post-accident vigilance.
Chapter 9 then outlines the management system changes the
Board feels are necessary to safely operate the Shuttle in the
mid-term. These changes separate the management of sched-
uling and budgets from technical specication authority,
build a capability of systems integration, and establish and
provide the resources for an independent safety and mission
assurance organization that has supervisory authority. The
third part of the chapter discusses the poor record this na-
tion has, in the Boardʼs view, of developing either a comple-
ment to or a replacement for the Space Shuttle. The report is
critical of several bodies in the U.S. government that share
responsibility for this situation, and expresses an opinion on
how to proceed from here, but does not suggest what the next
vehicle should look like.
Chapter 10 contains ndings, observations, and recom-
mendations that the Board developed over the course of this
extensive investigation that are not directly related to the
accident but should prove helpful to NASA.
Chapter 11 is a compilation of all the recommendations in
the previous chapters.
PART FOUR: APPENDICES
Part Four of the report by the Columbia Accident Inves-
tigation Board contains material relevant to this volume
organized in appendices. Additional, stand-alone volumes
will contain more reference, background, and analysis ma-
terials.
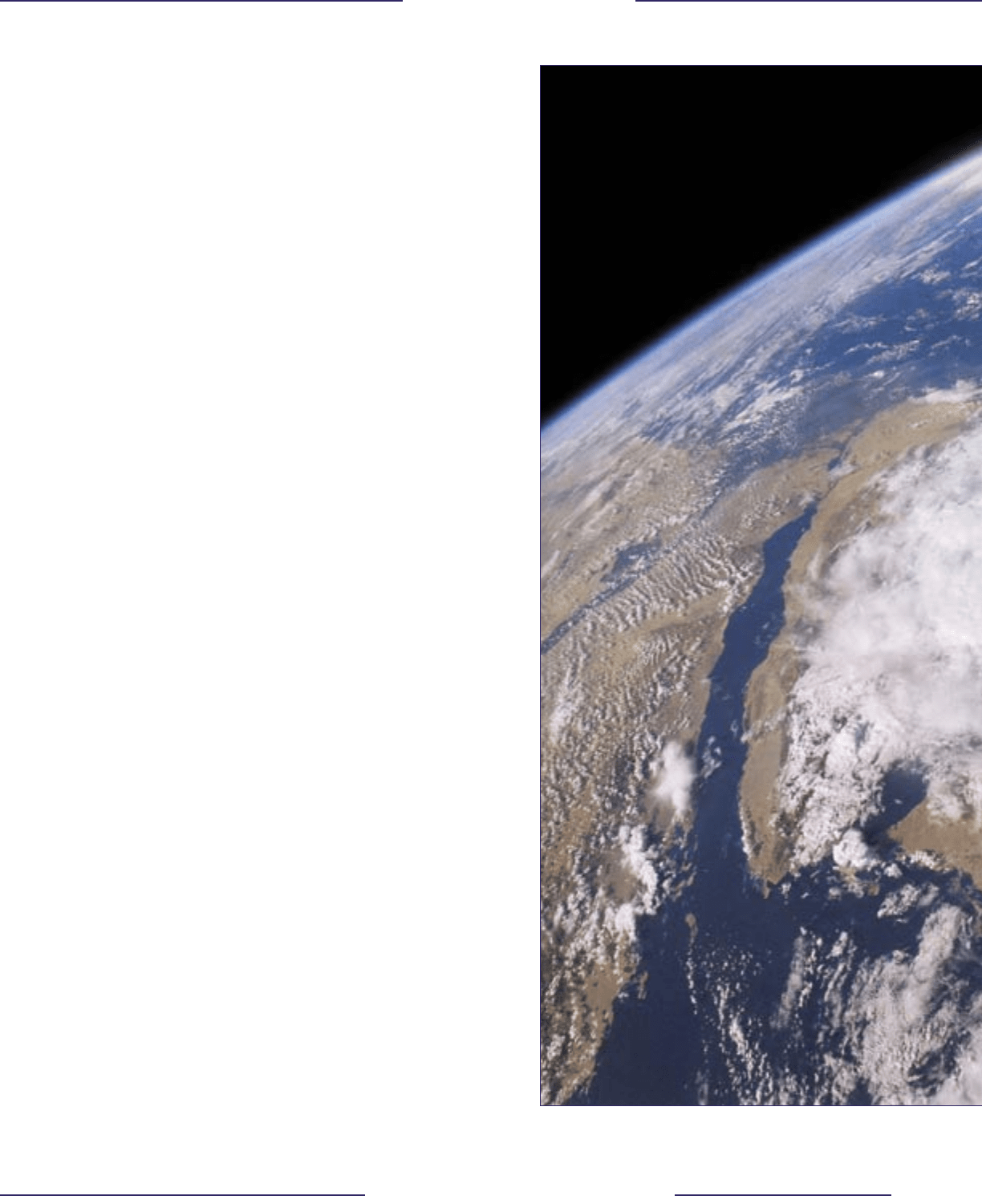
This Earth view of the Sinai Peninsula, Red Sea, Egypt, Nile River,
and the Mediterranean was taken from Columbia during STS-107.
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 4
R e p o r t V o l u m e I A u g u s t 2 0 0 3
1 5
R e p o r t V o l u m e I A u g u s t 2 0 0 3
AN INTRODUCTION TO THE SPACE SHUTTLE
The Space Shuttle is one of the most complex machines ever
devised. Its main elements – the Orbiter, Space Shuttle Main
Engines, External Tank, and Solid Rocket Boosters – are assembled
from more than 2.5 million parts, 230 miles of wire, 1,060 valves,
and 1,440 circuit breakers. Weighing approximately 4.5 million-
pounds at launch, the Space Shuttle accelerates to an orbital
velocity of 17,500 miles per hour – 25 times faster than the speed
of sound – in just over eight minutes. Once on orbit, the Orbiter
must protect its crew from the vacuum of space while enabling
astronauts to conduct scientic research, deploy and service
satellites, and assemble the International Space Station. At the end
of its mission, the Shuttle uses the Earthʼs atmosphere as a brake to
decelerate from orbital velocity to a safe landing at 220 miles per
hour, dissipating in the process all the energy it gained on its way
into orbit.
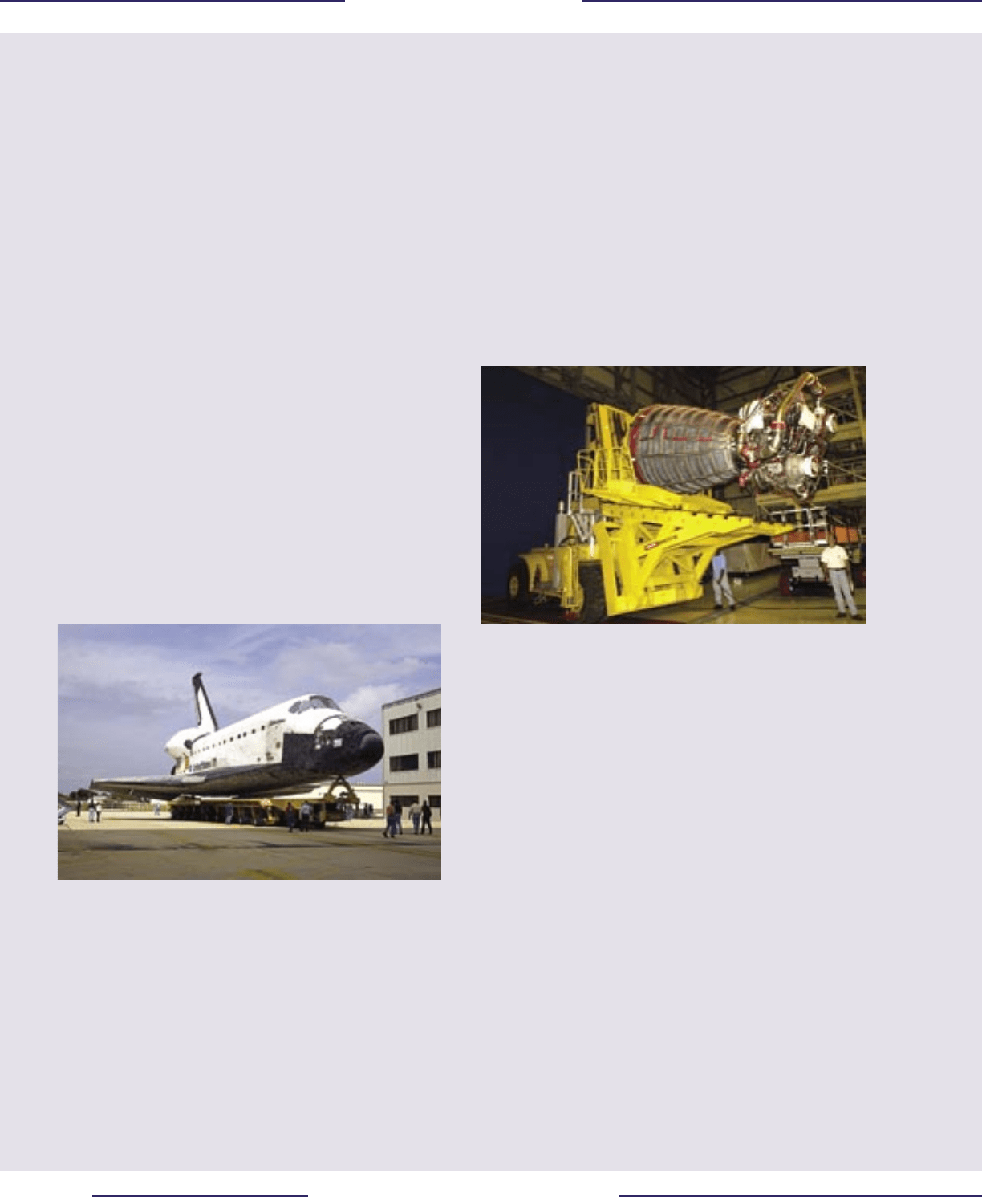
THE ORBITER
The Orbiter is what is popularly referred to as “the Space Shuttle.”
About the size of a small commercial airliner, the Orbiter normally
carries a crew of seven, including a Commander, Pilot, and ve
Mission or Payload Specialists. The Orbiter can accommodate a
payload the size of a school bus weighing between 38,000 and
56,300 pounds depending on what orbit it is launched into. The
Orbiterʼs upper ight deck is lled with equipment for ying and
maneuvering the vehicle and controlling its remote manipulator
arm. The mid-deck contains stowage lockers for food, equipment,
supplies, and experiments, as well as a toilet, a hatch for entering
and exiting the vehicle on the ground, and – in some instances – an
airlock for doing so in orbit. During liftoff and landing, four crew
members sit on the ight deck and the rest on the mid-deck.
Different parts of the Orbiter are subjected to dramatically different
temperatures during re-entry. The nose and leading edges of the
wings are exposed to superheated air temperatures of 2,800 to 3,000
degrees Fahrenheit, depending upon re-entry prole. Other portions
of the wing and fuselage can reach 2,300 degrees Fahrenheit. Still
other areas on top of the fuselage are sufciently shielded from
superheated air that ice sometimes survives through landing.
To protect its thin aluminum structure during re-entry, the Orbiter
is covered with various materials collectively referred to as the
Thermal Protection System. The three major components of the
system are various types of heat-resistant tiles, blankets, and the
Reinforced Carbon-Carbon (RCC) panels on the leading edge of
the wing and nose cap. The RCC panels most closely resemble a
hi-tech berglass – layers of special graphite cloth that are molded
to the desired shape at very high temperatures. The tiles, which
protect most other areas of the Orbiter exposed to medium and
high heating, are 90 percent air and 10 percent silica (similar to
common sand). One-tenth the weight of ablative heat shields,
which are designed to erode during re-entry and therefore can only
be used once, the Shuttleʼs tiles are reusable. They come in varying
strengths and sizes, depending on which area of the Orbiter they
protect, and are designed to withstand either 1,200 or 2,300 degrees
Fahrenheit. In a dramatic demonstration of how little heat the tiles
transfer, one can place a blowtorch on one side of a tile and a bare
hand on the other. The blankets, capable of withstanding either
700 or 1,200 degrees Fahrenheit, cover regions of the Orbiter that
experience only moderate heating.
SPACE SHUTTLE MAIN ENGINES
Each Orbiter has three main engines mounted at the aft fuselage.
These engines use the most efcient propellants in the world
– oxygen and hydrogen – at a rate of half a ton per second. At 100
percent power, each engine produces 375,000 pounds of thrust,
four times that of the largest engine on commercial jets. The large
bell-shaped nozzle on each engine can swivel 10.5 degrees up and
down and 8.5 degrees left and right to provide steering control
during ascent.
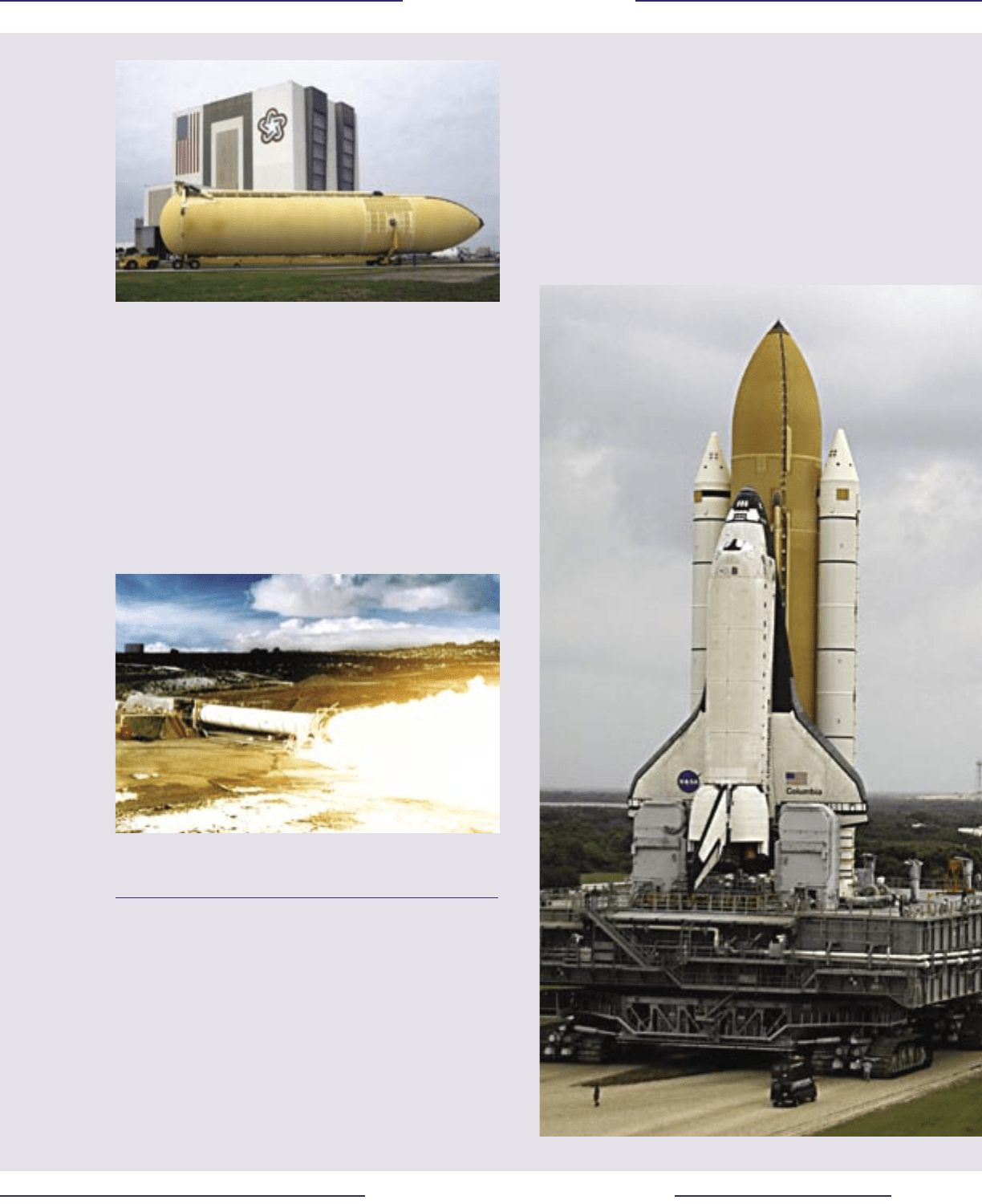
EXTERNAL TANK
The three main engines burn propellant at a rate that would drain
an average-size swimming pool in 20 seconds. The External
Tank accommodates up to 143,351 gallons of liquid oxygen and
385,265 gallons of liquid hydrogen. In order to keep the super-cold
propellants from boiling and to prevent ice from forming on the
outside of the tank while it is sitting on the launch pad, the External
Tank is covered with a one-inch-thick coating of insulating foam.
This insulation is so effective that the surface of the External Tank
feels only slightly cool to the touch, even though the liquid oxygen
is stored at minus 297 degrees Fahrenheit and liquid hydrogen
at minus 423 degrees Fahrenheit. This insulating foam also
protects the tankʼs aluminum structure from aerodynamic heating
during ascent. Although generally considered the least complex
of the Shuttleʼs main components, in fact the External Tank is a
remarkable engineering achievement. In addition to holding over
1.5 million pounds of cryogenic propellants, the 153.8-foot long
tank must support the weight of the Orbiter while on the launch pad
and absorb the 7.3 million pounds of thrust generated by the Solid
Rocket Boosters and Space Shuttle Main Engines during launch and
ascent. The External Tanks are manufactured in a plant near New
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 4
R e p o r t V o l u m e I A u g u s t 2 0 0 3
1 5
R e p o r t V o l u m e I A u g u s t 2 0 0 3
Orleans and are transported by barge to the Kennedy Space Center
in Florida. Unlike the Solid Rocket Boosters, which are reused, the
External Tank is discarded during each mission, burning up in the
Earthʼs atmosphere after being jettisoned from the Orbiter.
SOLID ROCKET BOOSTERS
Despite their power, the Space Shuttle Main Engines alone are not
sufcient to boost the vehicle to orbit – in fact, they provide only 15
percent of the necessary thrust. Two Solid Rocket Boosters attached
to the External Tank generate the remaining 85 percent. Together,
these two 149-foot long motors produce over six million pounds of
thrust. The largest solid propellant rockets ever own, these motors
use an aluminum powder fuel and ammonium perchlorate oxidizer
in a binder that has the feel and consistency of a pencil eraser.
Each of the Solid Rocket Boosters consists of 11 separate segments
joined together. The joints between the segments were extensively
redesigned after the Challenger accident, which occurred when hot
gases burned through an O-ring and seal in the aft joint on the left
Solid Rocket Booster. The motor segments are shipped from their
manufacturer in Utah and assembled at the Kennedy Space Center.
Once assembled, each Solid Rocket Booster is connected to the
External Tank by bolts weighing 65 pounds each. After the Solid
Rocket Boosters burn for just over two minutes, these bolts are
separated by pyrotechnic charges and small rockets then push the
Solid Rocket Boosters safely away from the rest of the vehicle. As
the boosters fall back to Earth, parachutes in their nosecones deploy.
After splashing down into the ocean 120 miles downrange from the
launch pad, they are recovered for refurbishment and reuse.
THE SHUTTLE STACK
The rst step in assembling a Space Shuttle for launch is stacking
the Solid Rocket Booster segments on the Mobile Launch
Platform. Eight large hold-down bolts at the base of the Solid
Rocket Boosters will bear the weight of the entire Space Shuttle
stack while it awaits launch. The External Tank is attached to
the Solid Rocket Boosters, and the Orbiter is then attached to the
External Tank at three points – two at its bottom and a “bipod”
attachment near the nose. When the vehicle is ready to move out of
the Vehicle Assembly Building, a Crawler-Transporter picks up the
entire Mobile Launch Platform and carries it – at one mile per hour
– to one of the two launch pads.
A Solid Rocket Booster (SRB) Demonstration Motor being tested
near Brigham City, Utah.
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 6
R e p o r t V o l u m e I A u g u s t 2 0 0 3
1 7
R e p o r t V o l u m e I A u g u s t 2 0 0 3
AN INTRODUCTION TO NASA
“An Act to provide for research into the problems of ight within
and outside the Earthʼs atmosphere, and for other purposes.” With
this simple preamble, the Congress and the President of the United
States created the National Aeronautics and Space Administration
(NASA) on October 1, 1958. Formed in response to the launch of
Sputnik by the Soviet Union, NASA inherited the research-oriented
National Advisory Committee for Aeronautics (NACA) and several
other government organizations, and almost immediately began
working on options for manned space ight. NASAʼs rst high
prole program was Project Mercury, an early effort to learn if hu-
mans could survive in space. Project Gemini followed with a more
complex series of experiments to increase manʼs time in space and
validate advanced concepts such as rendezvous. The efforts con-
tinued with Project Apollo, culminating in 1969 when Apollo 11
landed the rst humans on the Moon. The return from orbit on July
24, 1975, of the crew from the Apollo-Soyuz Test Project began
a six-year hiatus of American manned space ight. The launch of
the rst Space Shuttle in April 1981 brought Americans back into
space, continuing today with the assembly and initial operations of
the International Space Station.
In addition to the human space ight program, NASA also main-
tains an active (if small) aeronautics research program, a space
science program (including deep space and interplanetary explora-
tion), and an Earth observation program. The agency also conducts
basic research activities in a variety of elds.
NASA, like many federal agencies, is a heavily matrixed organiza-
tion, meaning that the lines of authority are not necessarily straight-
forward. At the simplest level, there are three major types of entities
involved in the Human Space Flight Program: NASA eld centers,
NASA programs carried out at those centers, and industrial and
academic contractors. The centers provide the buildings, facilities,
and support services for the various programs. The programs, along
with eld centers and Headquarters, hire civil servants and contrac-
tors from the private sector to support aspects of their enterprises.
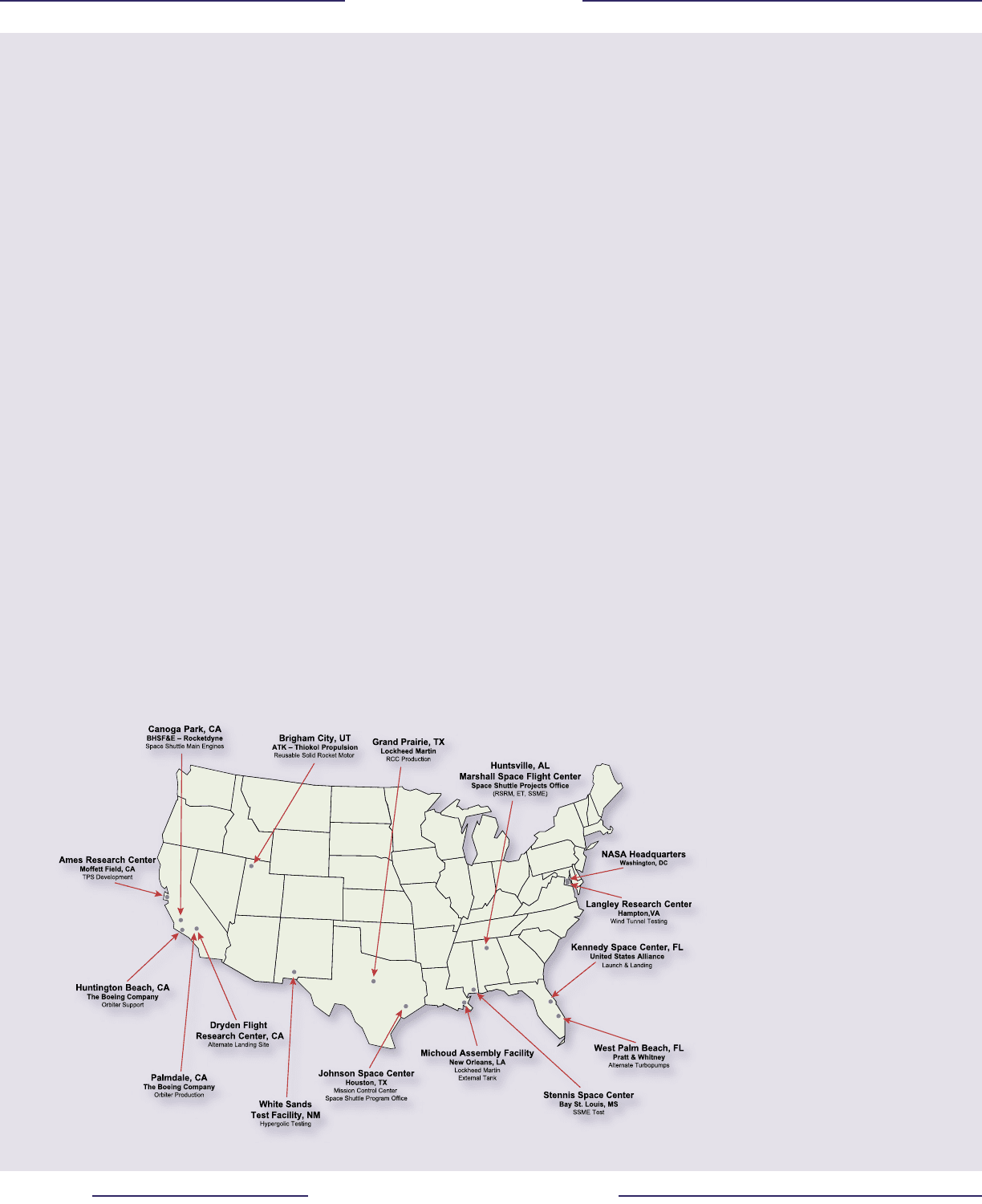
THE LOCATIONS
NASA Headquarters, located in Washington D.C., is responsible for
leadership and management across ve strategic enterprises: Aero-
space Technology, Biological and Physical Research, Earth Science,
Space Science, and Human Exploration and Development of Space.
NASA Headquarters also provides strategic management for the
Space Shuttle and International Space Station programs.
The Johnson Space Center in Houston, Texas, was established in
1961 as the Manned Spacecraft Center and has led the development
of every U.S. manned space ight program. Currently, Johnson is
home to both the Space Shuttle and International Space Station Pro-
gram Ofces. The facilities at Johnson include the training, simula-
tion, and mission control centers for the Space Shuttle and Space
Station. Johnson also has ight operations at Ellington Field, where
the training aircraft for the astronauts and support aircraft for the
Space Shuttle Program are stationed, and manages the White Sands
Test Facility, New Mexico, where hazardous testing is conducted.
The Kennedy Space Center was created to launch the Apollo mis-
sions to the Moon, and currently provides launch and landing facili-
ties for the Space Shuttle. The Center is located on Merritt Island,
Florida, adjacent to the Cape Canaveral Air Force Station that also
provides support for the Space Shuttle Program (and was the site
of the earlier Mercury and Gemini launches). Personnel at Ken-
nedy support maintenance and overhaul services for the Orbiters,
assemble and check-out the integrated vehicle prior to launch, and
operate the Space Station Processing Facility where components of
the orbiting laboratory are packaged for launch aboard the Space
Shuttle. The majority of contractor personnel assigned to Kennedy
are part of the Space Flight Operations Contract administered by
the Space Shuttle Program Ofce at Johnson.
The Marshall Space Flight Center, near Hunstville, Alabama, is
home to most NASA rocket propulsion efforts. The Space Shuttle
Projects Ofce located at
Marshall—organization-
ally part of the Space
Shuttle Program Ofce
at Johnson—manages the
manufacturing and support
contracts to Boeing Rock-
etdyne for the Space Shut-
tle Main Engine (SSME),
to Lockheed Martin for the
External Tank (ET), and to
ATK Thiokol Propulsion
for the Reusable Solid
Rocket Motor (RSRM, the
major piece of the Solid
Rocket Booster). Marshall
is also involved in micro-
gravity research and space
product development pro-
grams that y as payloads
on the Space Shuttle.
The Stennis Space Center
in Bay St. Louis, Missis-
sippi, is the largest rocket
propulsion test complex in
the United States. Stennis
provides all of the testing
facilities for the Space
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 6
R e p o r t V o l u m e I A u g u s t 2 0 0 3
1 7
R e p o r t V o l u m e I A u g u s t 2 0 0 3
Shuttle Main Engines and External
Tank. (The Solid Rocket Boosters are
tested at the ATK Thiokol Propulsion
facilities in Utah.)
The Ames Research Center at Moffett
Field, California, has evolved from its
aeronautical research roots to become
a Center of Excellence for information
technology. The Centerʼs primary im-
portance to the Space Shuttle Program,
however, lies in wind tunnel and arc-jet
testing, and the development of thermal
protection system concepts.
The Langley Research Center, at Hamp-
ton, Virginia, is the agencyʼs primary
center for structures and materials and
supports the Space Shuttle Program in
these areas, as well as in basic aerody-
namic and thermodynamic research.
THE PROGRAMS
The two major human space ight ef-
forts within NASA are the Space Shut-
tle Program and International Space
Station Program, both headquartered at
Johnson although they report to a Dep-
uty Associate Administrator at NASA
Headquarters in Washington, D.C.
The Space Shuttle Program Ofce at
Johnson is responsible for all aspects
of developing, supporting, and ying
the Space Shuttle. To accomplish these
tasks, the program maintains large
workforces at the various NASA Cen-
ters that host the facilities used by the program. The Space Shuttle
Program Ofce is also responsible for managing the Space Flight
Operations Contract with United Space Alliance that provides most
of the contractor support at Johnson and Kennedy, as well as a small
amount at Marshall.
THE CONTRACTORS
The Space Shuttle Program employs a wide variety of commercial
companies to provide services and products. Among these are some
of the largest aerospace and defense contractors in the country, in-
cluding (but not limited to):
United Space Alliance
This is a joint venture between Boeing and Lockheed Martin that
was established in 1996 to perform the Space Flight Operations
Contract that essentially conducts the day-to-day operation of the
Space Shuttle. United Space Alliance is headquartered in Houston,
Texas, and employs more than 10,000 people at Johnson, Kennedy,
and Marshall. Its contract currently runs through 2005.
The Boeing Company, NASA Systems
The Space Shuttle Orbiter was designed and manufactured by
Rockwell International, located primarily in Downey and Palmdale,
California. In 1996, The Boeing Company purchased the aerospace
assets of Rockwell International, and later moved the Downey op-
eration to Huntington Beach, California, as part of a consolidation
of facilities. Boeing is subcontracted to United Space Alliance to
provide support to Orbiter modications and operations, with work
performed in California, and at Johnson and Kennedy.
The Boeing Company, Rocketdyne Propulsion & Power
The Rocketdyne Division of Rockwell International was responsi-
ble for the development and manufacture of the Space Shuttle Main
Engines, and continues to support the engines as a part of The Boe-
ing Company. The Space Shuttle Projects Ofce at Marshall man-
ages the main engines contract, with most of the work performed in
California, Stennis, and Kennedy.
ATK Thiokol Propulsion
ATK Thiokol Propulsion (formerly Morton-Thiokol) in Brigham
City, Utah, manufactures the Reusable Solid Rocket Motor seg-
ments that are the propellant sections of the Solid Rocket Boosters.
The Space Shuttle Projects Ofce at Marshall manages the Reus-
able Solid Rocket Motor contract.
Lockheed Martin Space Systems, Michoud Operations
The External Tank was developed and manufactured by Martin
Marietta at the NASA Michoud Assembly Facility near New Or-
leans, Louisiana. Martin Marietta later merged with Lockheed to
create Lockheed Martin. The External Tank is the only disposable
part of the Space Shuttle system, so new ones are always under
construction. The Space Shuttle Projects Ofce at Marshall man-
ages the External Tank contract.
Lockheed Martin Missiles and Fire Control
The Reinforced Carbon-Carbon (RCC) panels used on the nose
and wing leading edges of the Orbiter were manufactured by Ling-
Temco-Vought in Grand Prairie, Texas. Lockheed Martin acquired
LTV through a series of mergers and acquisitions. The Space Shuttle
Program ofce at Johnson manages the RCC support contract.
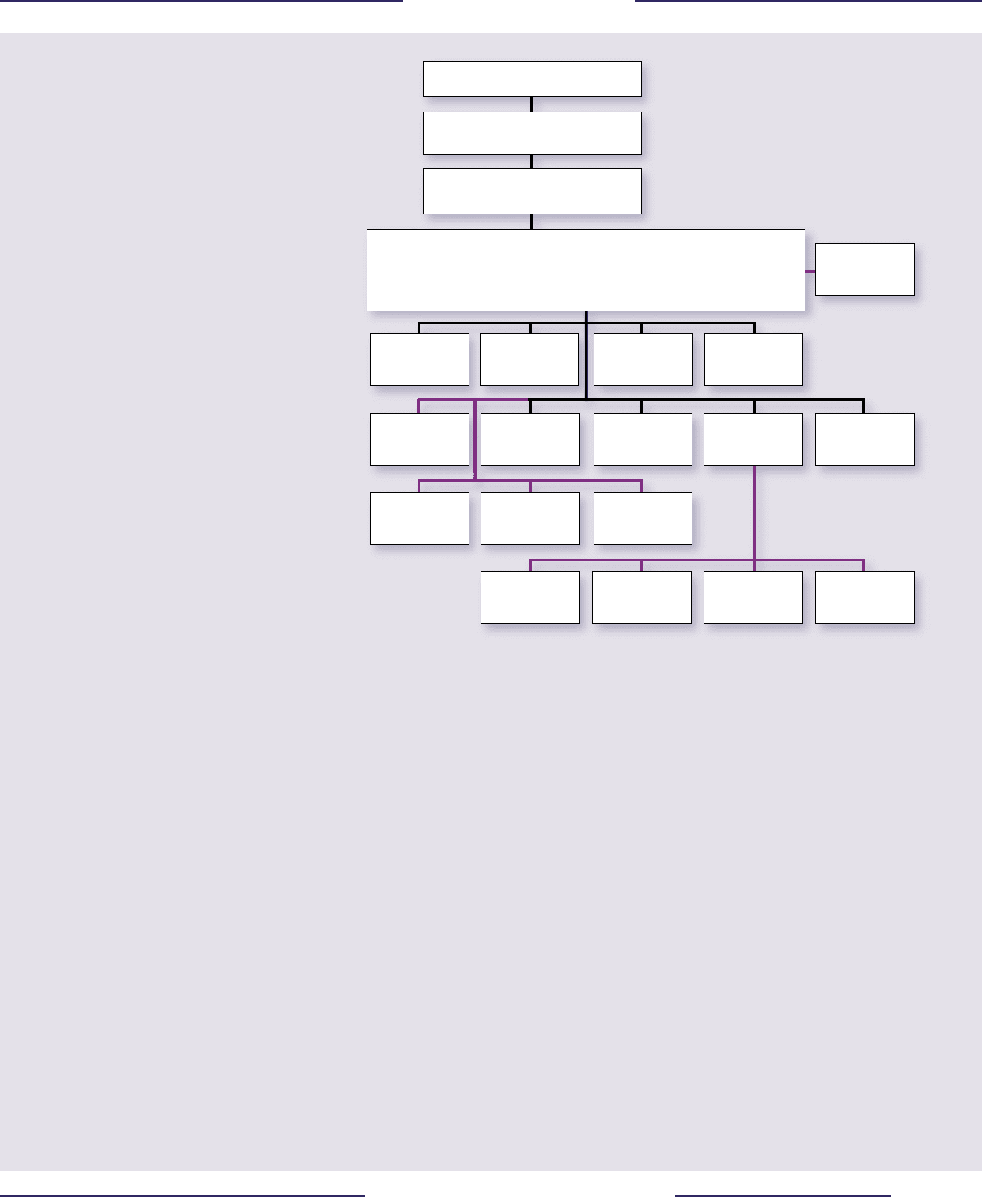
Human Exploration & Development of Space
Associate Administrator
International Space Station and
Space Shuttle Programs
Deputy Associate Administrator
Space Shuttle Program Office
Manager, Space Shuttle Program (SSP) Manager, SSP Safety and Mission Assurance
Manager, Launch Integration (KSC) Manager, SSP Development
Manager, Program Integration Manager, SSP Logistics (KSC)
Space Shuttle
S&MA Office
Space Shuttle
Administrative Office
S
p
a
c
e
S
h
ut
t
le
M
a
nag
e
m
ent
I
n
te
g
ra
t
i
o
n
Of
f
i
ce
Space Shuttle
Business Office
(SFOC COTR)
Space Shuttle
KSC Integration Office
Space Shuttle
Vehicle Engineering Office
Space Shuttle
Processing (KSC)
Space Shuttle
Systems Integration Office
Space Shuttle
Customer and Flight
Integration Office
Space Shuttle
Projects Office (MSFC)
Missions Operations
Directorate
Flight Crew Operations
Directorate
Extravehicular Activity
Solid Rocket Booster
(SRB) Office
Reusable Solid Rocket
Motor (RSRM) Office
Space Shuttle Main Engine
(SSME) Office
External Tank (ET)
Office
Administrator
Space Shuttle Program
NASA Organization

The launch of STS-107 on January 16, 2003.

A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
1 9
R e p o r t V o l u m e I A u g u s t 2 0 0 3
Part One
The Accident
“Building rockets is hard.” Part of the problem is that space
travel is in its infancy. Although humans have been launch-
ing orbital vehicles for almost 50 years now – about half the
amount of time we have been ying airplanes – contrast the
numbers. Since Sputnik, humans have launched just over
4,500 rockets towards orbit (not counting suborbital ights
and small sounding rockets). During the rst 50 years of
aviation, there were over one million aircraft built. Almost
all of the rockets were used only once; most of the airplanes
were used more often.
There is also the issue of performance. Airplanes slowly
built their performance from the tens of miles per hour the
Wright Brothers initially managed to the 4,520 mph that Ma-
jor William J. Knight ew in the X-15A-2 research airplane
during 1967. Aircraft designers and pilots would slightly
push the envelope, stop and get comfortable with where they
were, then push on. Orbital rockets, by contrast, must have
all of their performance on the rst (and often, only) ight.
Physics dictates this – to reach orbit, without falling back to
Earth, you have to exceed about 17,500 mph. If you cannot
vary performance, then the only thing left to change is the
amount of payload – the rocket designers began with small
payloads and worked their way up.
Rockets, by their very nature, are complex and unforgiving
vehicles. They must be as light as possible, yet attain out-
standing performance to get to orbit. Mankind is, however,
getting better at building them. In the early days as often
as not the vehicle exploded on or near the launch pad; that
seldom happens any longer. It was not that different from
early airplanes, which tended to crash about as often as they
ew. Aircraft seldom crash these days, but rockets still fail
between two-and-ve percent of the time. This is true of
just about any launch vehicle – Atlas, Delta, Soyuz, Shuttle
– regardless of what nation builds it or what basic congura-
tion is used; they all fail about the same amount of the time.
Building and launching rockets is still a very dangerous
business, and will continue to be so for the foreseeable fu-
ture while we gain experience at it. It is unlikely that launch-
ing a space vehicle will ever be as routine an undertaking as
commercial air travel – certainly not in the lifetime of any-
body who reads this. The scientists and engineers continu-
ally work on better ways, but if we want to continue going
into outer space, we must continue to accept the risks.
Part One of the report of the Columbia Accident Investiga-
tion Board is organized into four chapters. In order to set
the background for further discussion, Chapter 1 relates the
history of the Space Shuttle Program before the Challenger
accident. The events leading to the original approval of the
Space Shuttle Program are recounted, as well as an exami-
nation of some of the promises made in order to gain that
approval. In retrospect, many of these promises could never
have been achieved. Chapter 2 documents the nal ight of
Columbia. As a straightforward record of the event, it con-
tains no ndings or recommendations. Chapter 3 reviews
ve analytical paths – aerodynamic, thermodynamic, sensor
data timeline, debris reconstruction, and imaging evidence
– to show that all ve independently arrive at the same con-
clusion. Chapter 4 describes the investigation into other pos-
sible physical factors that might have contributed to the ac-
cident, but were subsequently dismissed as possible causes.
Sunrise aboard Columbia
on Flight Day 7.

A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
A C C I D E N T I N V E S T I G A T I O N B O A R D
COLUMBIA
2 0
R e p o r t V o l u m e I A u g u s t 2 0 0 3
2 1
R e p o r t V o l u m e I A u g u s t 2 0 0 3
The launch of STS-107 on January 16, 2003.